Aseptic Packaging. Content Introduction What is Aseptic? Aseptic Packaging Advantages Limitations.

CHHS18/137
Canberra Hospital and Health ServicesClinical ProcedureBrachytherapy Procedures for Nurses within Radiation Oncology (Adults Only)Contents
Contents....................................................................................................................................1
Purpose.....................................................................................................................................3
Alerts.........................................................................................................................................3
Scope........................................................................................................................................ 3
Section 1 – Vaginal Vault Brachytherapy..................................................................................4
Equipment............................................................................................................................4
Cleaning Equipment after CT................................................................................................4
Vaginal Vault Brachytherapy Treatment..............................................................................5
Section 2 – HDR Prostate Brachytherapy Volume Study...........................................................6
Equipment............................................................................................................................6
Day before procedure RO to contact the patient and advise the patient:...........................6
Day of procedure..................................................................................................................6
Commencing the HDR Prostate Brachytherapy Volume Study Procedure...........................8
On completion of the HDR Prostate Brachytherapy Volume Study Procedure....................8
Section 3 – Prostate Fiducial Marker Implant...........................................................................8
Equipment............................................................................................................................9
Pre procedure.....................................................................................................................10
Day before the procedure..................................................................................................10
Day of the procedure of the Fiducial Marker Implant........................................................10
At the end of the Fiducial Marker Implant Procedure........................................................13
Following the Fiducial Marker Implant Procedure.............................................................13
Section 4 – HDR Prostate Brachytherapy & Fiducial Marker Implant Insertion......................14
Equipment - Sterile stock...................................................................................................14
Equipment - Unsterile Stock...............................................................................................14
Pre HDR Prostate Brachytherapy procedure......................................................................15
Day 1.................................................................................................................................. 16
Day of the HDR Prostate Brachytherapy procedure........................................................16Doc Number Version Issued Review Date Area Responsible PageCHHS18/137 1 27/04/2018 01/03/2021 CACHS -
Brachytherapy1 of 27
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS18/137
Set up trolleys for end the HDR Prostate Brachytherapy procedure (outside the bunker)........................................................................................................................................ 19
At the end of the HDR Prostrate Brachytherapy procedure............................................20
Post-Operative HDR Prostate Brachytherapy Procedure/recovery performed by Radiation Oncology nurses..............................................................................................21
CT Planning Procedure pre HDR treatment.....................................................................22
Brachytherapy Treatment...............................................................................................22
Ward Management.........................................................................................................23
Day 2.................................................................................................................................. 23
Prostate Brachytherapy Treatment.................................................................................23
End of Day 2....................................................................................................................24
Implementation...................................................................................................................... 25
Related Policies, Procedures, Guidelines and Legislation.......................................................25
References.............................................................................................................................. 26
Abbreviations..........................................................................................................................26
Definition of Terms................................................................................................................. 27
Search Terms.......................................................................................................................... 27
Doc Number Version Issued Review Date Area Responsible PageCHHS18/137 1 27/04/2018 01/03/2021 CACHS -
Brachytherapy2 of 27
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS18/137
Purpose
This procedure provides nursing staff with the knowledge to assist medical officers (MOs) and radiation therapists (RTs) in performing the procedures that relate to Brachytherapy within the Radiation Oncology Department.
Brachytherapy is the insertion of radioactive sources intracavity and interstitially that emit a high dose of radiation. Patients may also have external beam radiation therapy (EBRT) before or after this procedure.
Back to Table of Contents
Alerts
Nursing staff assisting in the procedures must have undertaken the emergency/safety procedures provided by the appropriate RT.
Lead aprons must be worn for C-Arm fluoroscopy (X-Ray) in the Radiation Oncology Department during the prostate brachytherapy implant procedures. Personal radiation monitors are not required to be worn by nursing staff during the procedure.
Nursing staff scrubbing/scouting for the fiducial marker and prostate brachytherapy procedures must be credentialed annually for the assessment of Surgical Hand Antisepsis, Gowning and Gloving and Maintenance of an Aseptic Field.
Ensure patient privacy at all times by hanging a privacy notice on the entrance door and using the privacy screen placed at the entrance of the bunker.
For the Prostate Fiducial Marker Implant procedure and HDR Prostate Brachytherapy procedure never remove anything from the bunker after the initial count. All accountable items must remain in the bunker for surgical counting.
Back to Table of Contents
Scope
This document applies to: Registered Nurses (RNs) who have observed the procedure and are deemed competent
and credentialed against the Australian College of Perioperative Nurses (ACORN) Standards and working within their scope of practice. RNs must:o Be competent in the management of patients before, during and after the
procedures o Have attended the brachytherapy emergency training provided by RTso Have attended the three day peri operative course – this applies to RNs assisting with
fiducial marker insertion and HDR prostate brachytherapyo Be familiar with all theatre documentation - Pre-Operative checklist, Intra-Operative
Nursing Care Plan, Registered Nurses Theatre Report and Surgical safety checklisto Be familiar with Post-operative handover and Observations-Adult patients (first 24
hours). Doc Number Version Issued Review Date Area Responsible PageCHHS18/137 1 27/04/2018 01/03/2021 CACHS -
Brachytherapy3 of 27
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS18/137
Back to Table of Contents
Section 1 – Vaginal Vault Brachytherapy
Vaginal Vault Brachytherapy is high dose radiation (or internal radiation) delivered through an applicator. Vaginal Vault Brachytherapy is used to treat gynaecological cancers such as endometrial or vaginal vault.
Equipment Lignocaine gel syringe Three x sachets of KY jelly Two x 20 x 20cm combines Sterile Vaginal Vault Brachytherapy tray- provided by the RTs PPE
CT Planning Procedure1. RT will confirm patient identification (ID) and obtain patient’s informed consent prior to
the procedure. Refer to Consent and Treatment Policy and Patient Identification and Procedure Matching Policy for further information.
2. The Radiation Oncologist (RO) inserts the applicator following a vaginal examination. 3. Once the applicator is in place, the patient is instructed to lower their legs. Pen marks are
drawn on the patient’s inner thighs for marking purposes by the RTs. 4. Patient is advised not to wash these marks off between treatments.5. The patient will have a CT with the applicator insitu. The applicator should then be
removed following the CT procedure by the RO or RN.
Cleaning Equipment after CT1. Following each brachytherapy treatment, the applicator will be cleaned by an RN or RT. 2. RN to take the brachytherapy tray and applicator to pan room, don PPE, and wash the
applicator with soap and water or standard detergent wipes so that it is ready for use at the completion of the patients planning appointment.
3. Extreme care must be taken to ensure no fluid is introduced into the vaginal tube, or treatment channels during the cleaning process. The black sterilisation cap should be placed on the end of the tube (long plastic tube) prior to cleaning.
4. Take the cleaned brachytherapy tray, along with additional KY jelly to the brachytherapy bunker for the first brachytherapy treatment.
5. Individual brachytherapy tray number will be identified with Patient ID label on the brachytherapy tray sterilising form.
Doc Number Version Issued Review Date Area Responsible PageCHHS18/137 1 27/04/2018 01/03/2021 CACHS -
Brachytherapy4 of 27
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS18/137
Vaginal Vault Brachytherapy TreatmentPatients having vaginal vault brachytherapy are generally treated with an empty bladder.
1. RT will confirm patient ID and obtain patient’s informed consent prior to the procedure. 2. Ensure patient privacy at all times by hanging a privacy notice on the entrance door and
using the privacy screen placed at the entrance of the bunker. 3. RO will insert the cleaned applicator. Brachytherapy tray number to be matched against
patient ID label. 4. An RN must be present in the control room during the patient’s treatment.5. Brachytherapy treatment takes approximately 10 minutes (depending on the individual
plan and strength of the radioactive source). Following treatment, the applicator will be removed by the RO or the RN.
Note:Staff should not enter the room until all indicators show that the HDR source has returned to the treatment safe.
Post Vaginal Vault Brachytherapy Treatment1. RT to advise patient of their next appointment and patient will be escorted from the
brachytherapy treatment room by the RN.2. RN to provide patient with vaginal dilators and supporting documentation/education
after completing their final brachytherapy treatment. 3. Following each brachytherapy treatment, the equipment tray will be cleaned and
returned to pre-rinse for sterilisation by RN as follows: 3.1 Don PPE.3.2 The re-usable applicator sets will be taken to the pan room and disassembled by
unlocking the cylinder fixation piece and sliding the cylinder segments off the vaginal tube by the RN. Prior to cleaning, the black sterilisation cap must be placed on the end of the vaginal tube to prevent any fluid getting inside the applicator.
3.3 Applicator parts will be cleaned using soap and water, making sure that all visible soil is removed. Particular care must be taken not to lose any small pieces of equipment. Lost equipment will have to be replaced.
3.4 Applicator parts will be dried and returned to the applicator sterilisation tray. Two nurses must check and verify that all equipment is present on the tray and corresponds to the tray list.
3.5 Once the set components are checked off, a photocopy of the paperwork will be taken, which will be scanned to patient’s clinical notes on ARIA.
3.6 Cleaned re-usable applicators should be re-packaged with accompanying signed documentation and sent to pre rinse for sterilisation.
3.7 Wards person to collect and deliver tray to pre-rinse for sterilisation.
Back to Table of Contents
Doc Number Version Issued Review Date Area Responsible PageCHHS18/137 1 27/04/2018 01/03/2021 CACHS -
Brachytherapy5 of 27
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS18/137
Section 2 – HDR Prostate Brachytherapy Volume Study
The volume study procedure is performed to determine whether a patient is suitable to undergo HDR prostate brachytherapy. A volume study is a transrectal ultrasound procedure.
This procedure is usually done 6-8 weeks before the intended brachytherapy procedure and follows a flow study procedure that identifies that patient is suitable for brachytherapy, has adequate urine flow and minimal urine retention.
Equipment Dressing Trolley Dressing pack Two x 60mL luer lock syringes One x 3 way tap One x vial of 0.9% Sodium Chloride Three x tubes KY jelly Drawing up needle One x bladder syringe and one spare Sterile Gloves Clean gowns Safety glasses or goggles Sterile labels for fluid marking Sterile marking pen
RN to prepare trolley setup as close to patient’s arrival to the department as possible. This can be done in the Brachytherapy Bunker.
Day before procedure RO to contact the patient and advise the patient:1. To purchase a microlax enema from the chemist, which is available without prescription.2. Is required to use the enema the night before the procedure.3. Is required to fast from midnight and should not consume anything other than clear
fluids (e.g. water or black tea) until after the procedure.
Day of procedureOn the day of the procedure, the patient will generally arrive at 0820hrs with the aim to start the procedure at 0900hrs.1. Patient will get changed into a white gown.2. RT or RN to confirm consent and patient identification against clinical notes and stickers.3. RN to administer the charted microlax enema and encourage the patient to open their
bowels following the enema before the procedure begins.
Doc Number Version Issued Review Date Area Responsible PageCHHS18/137 1 27/04/2018 01/03/2021 CACHS -
Brachytherapy6 of 27
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS18/137
Setting up for procedure RN to perform the following: 1. Wash hands thoroughly before opening the dressing pack onto the cleaned and dry
dressing trolley.2. Open syringes, 3 way tap and drawing up needle onto the sterile field and the tray fill
with KY jelly.3. Open vials of 0.9% Sodium Chloride and place on the edge of the dressing trolley – not
on the sterile field.4. Don PPE including clean gown, safety goggles and sterile gloves as per Healthcare
Associated Infections Clinical Procedure.5. Fill the 60 mL luer lock syringe with approximately 50mL of KY jelly and 5mL 0.9% Sodium
Chloride. Sterile labels are used to identify items on the aseptic field as per National medication labelling.
6. Attach the 3-way tap to the syringe filled in step above and also an empty 60mL luer lock syringe.
7. Aerate the KY jelly/0.9% Sodium Chloride mixture by alternating filling and emptying of syringes until the mixture becomes opaque.
8. Add the mixture from the luer lock syringe to the bladder syringe by removing the plunger from the bladder syringe. Ensure the filled bladder syringe is kept in an angled position so the contents do not ooze out.
9. Keep the luer lock syringes attached to the 3-way tap on the sterile field in case another syringe with aerated KY jelly/0.9% Sodium Chloride is required to be made up.
10. Remove air bubbles from the bladder syringe by rolling the syringe in between your gloved hands.
11. Escort patient to the Brachytherapy bunker.12. Ensure patient privacy at all times by hanging a privacy notice on the entrance door and
using the privacy screen placed at the entrance of the bunker. 13. Set up the following on a second dressing trolley:
IDC pack 18fg catheter. Ensure that an extra catheter is available if required Two x KY jelly sachets Two x Lignocaine 2% gel Chlorhexidine One x spigot, and one spare Two x 30mL 0.9% Sodium Chloride, emptied into one of the trays as part of the
catheter pack or 0.9% Sodium Chloride Sterile labels for fluid marking Sterile marking pen Sterile gauze squares Extra gauze and combines under trolley to be opened if required Clamp Penile Thompson Walker (have one spare in case it is needed) Sterile gloves Sterile drapes Safety glasses or goggles and un sterile gown
Doc Number Version Issued Review Date Area Responsible PageCHHS18/137 1 27/04/2018 01/03/2021 CACHS -
Brachytherapy7 of 27
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS18/137
Commencing the HDR Prostate Brachytherapy Volume Study Procedure1. RT/RN to check patient identification, patient identification wrist band and consent
against clinical notes and stickers while verbally confirming with patient.2. Explain the procedure to the patient.3. Staff to don PPE.4. Patient is to be positioned in the lithotomy position using Yellowfin stirrups, which are
supplied by RTs. Legs to be placed into stirrups simultaneously.5. Penis and the surrounding area to be prepped with 0.9% Sodium Chloride and a sterile
drape to be placed around the perineal area, usually by MO or RO.6. RO or RN to insert Lignocaine Gel into the urethra.7. Use a Penile clamp to hold the penis in position to ensure lignocaine gel remains in the
urethra. 8. Encourage the patient to take deep breaths while RO or MO inserts the catheter. 9. RN to hold a collection tray while the catheter is being inserted for the urine to drain
into. Spigot is then placed on the end of the catheter by RN.10. Catheter balloon is not inflated for this procedure, as later in the procedure the catheter
will gently be pulled back as aerated KY jelly is injected into the urethra to highlight it on the ultrasound image.
11. RO will insert the transrectal ultrasound probe into the patient’s rectum. 12. RO will then inject approximately 10-20mL of 0.9% Sodium Chloride into the endocavity
balloon.13. RN to pass the sterile bladder syringe with the mixture of KY jelly/0.9% Sodium Chloride
(aerated gel) to the RO and hold the spigot. As aerated gel is inserted into the urethra, the RO slowly begins to partially slide out the catheter.
14. Using the ultrasound machine, the RO and the RT will take measurements and calculations to determine the prostate volume.
On completion of the HDR Prostate Brachytherapy Volume Study Procedure1. The transrectal ultrasound probe is removed by the RO.2. Urethral catheter is removed by RO or RN.3. Combines are used to clean the patient.4. Both legs to be taken out of the lithotomy position simultaneously.5. Encourage the patient to sit on the edge of the bed before completely getting up.6. Patient should be discharged from the unit following the procedure as per MO’s
instructions.7. All nursing notes should be entered into patient’s clinical record in ‘Encounters’ on ARIA.
Back to Table of Contents
Section 3 – Prostate Fiducial Marker Implant
Prostate Fiducial Marker Implant Procedure uses imaging guidance to place small metal objects called Fiducial Markers in the prostate in preparation for radiation therapy. The markers help to localise the prostate more accurately during daily pre-treatment imaging to improve the accuracy of the treatment.
Doc Number Version Issued Review Date Area Responsible PageCHHS18/137 1 27/04/2018 01/03/2021 CACHS -
Brachytherapy8 of 27
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS18/137
Equipment Two x Povidone-iodine solution 30mL Sterile gloves Three x Sterile gowns (STP 08). (Spare gowns should be available for the procedure) Sterile Urology pack STP 07 Sterile bowl set Sterile back table cover Sterile Urology Bundle (STP 07) Three x Combines 20x30cm Water for cleaning the patient at the end of the procedure Barrier-EasyWarm - Active self-warming blanket Safety glasses or goggles Procedure under pads e.g. Smart Barrier Touch Dry absorbent pads Ioban 6640 EZ One x Raytec swabs pack One x Rampley sponge holder forcep 25cm Sterile marking pen Sterile labels for fluid marking
Do Not Open (DNO) unless requested by the RO: 18Fg catheter and drainage bag 10mL syringe Two x Lignocaine 2% gel syringe Catheter pack Rectal tube KY Jelly Ioban 6640 EZ One x Raytec swabs One x Rampley sponge holder forcep 25cm
Theatre paperwork Progress Notes Observation chart Pre- Operative checklist Registered Nurses Theatre Report (RNTR) Intra- Operative Nursing Care Plan Canberra Hospital Operation Record Surgical Safety Checklist Canberra Hospital Anaesthetic Nurses’ Procedure report The Canberra Hospital Anaesthetic Assessment Intravenous Fluid and Additive Orders
Pre procedureRT will:
Doc Number Version Issued Review Date Area Responsible PageCHHS18/137 1 27/04/2018 01/03/2021 CACHS -
Brachytherapy9 of 27
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS18/137
1. Advise RN of the procedure date. 2. Organise brachytherapy bunker theatre clean for the day before procedure.3. Provide patient with a list of instructions prior to the procedure.
RN to:1. Book pre admission clinic (PAC) for patient at least two weeks prior to the fiducial marker
implant procedure.2. Ensure that all stock, sterile and non-sterile, is available for the procedure.3. Collect the pre admission paperwork and signed patient consent from pre admission
clinic.4. Check the trolley setup and ensure all stock is available for the procedure.5. Check that microlax enema has been charted by MO.
Day before the procedure1. RO will advise patient to purchase a microlax enema from the chemist, which is available
without prescription.2. Patient is required to use the enema the night before the procedure.3. Patient is required to fast from midnight and should not to consume any food or drink
until after the procedure (refer to Fasting Guidelines for Patients Requiring Sedation of Anaesthesia).
4. RN to set up the Radiation Oncology recovery bay area in order to receive the patient following the procedure and recover the patient from general anaesthetic, (inclusive of IV pole and patient monitoring equipment).
Day of the procedure of the Fiducial Marker Implant All staff entering the brachytherapy bunker on the day of the procedure must be dressed
in theatre scrubs. RTs will provide the shoe covers, hair covers, masks and eye protection so these items
are available for all staff to put on before entering the bunker. The patient will have a consultation with the Anaesthetic team prior to the procedure
and the Anaesthetic team will insert an IV cannula.
RN:1. Check patient identification, patient identification wrist band and consent against clinical
notes and stickers while verbally confirming with patient.2. Commence a Progress Note and complete Pre-Operative Checklist with the patient.3. Confirm the process and procedure to the patient.4. Measure baseline observations, usual systolic BP and MEWS score and weight and
complete Pre-Operative checklist.5. Secure patient’s belongings in the radiation oncology drug room.6. Assist patient to put on white gowns, the first one with the opening at the back and the
other with the opening at the front.7. Administer microlax enema as charted.
RN/Scrub nurse is to set up the brachytherapy bunker: Doc Number Version Issued Review Date Area Responsible PageCHHS18/137 1 27/04/2018 01/03/2021 CACHS -
Brachytherapy10 of 27
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS18/137
1. Clean trolley with detergent wipes.2. Check that all packaging is in date, intact and that sterility has not been compromised.3. Wash hands and open outer packaging of sterile gown, gloves, urology bundle and back
table cover. 4. Sterile gloves and gowns to be opened onto the cleaned and dry dressing trolley. 5. Open back table cover onto cleaned large trolley, discard outer plastic packaging and
open outer layer only.6. Place urology bundle on mayo table. Remove outer packaging and unwrap outer blue
layer only.7. Let the circulating nurse know that you are scrubbing.8. Perform five minute surgical scrub, in compliance with the ACORN standards, don sterile
gown and double sterile gloves. (Refer to ACORN Standards-2016/2017- Surgical Hand Antisepsis, Gowning and Gloving Standards and maintain a surgical aseptic field).
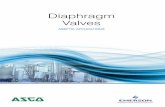
9. Prepare the surgical aseptic field and assemble the trolley with the sterile equipment that have been opened by the scout/circulating nurse – see figure 1 in section 4 below.
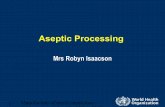
10. Assemble the template and equipment in an aseptic manner under the guidance of the RT (see figure 2 in section 4 below). (Refer to ACORN Standards – 2016/2017 – Asepsis).
Figure 1: Template and equipment to be assembled on trolley
Doc Number Version Issued Review Date Area Responsible PageCHHS18/137 1 27/04/2018 01/03/2021 CACHS -
Brachytherapy11 of 27
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS18/137
Figure 2: Assembled Template
RN/Circulating nurse:1. Walk patient to the brachytherapy bunker when the scrub nurse and anaesthetist are
ready.2. Circulating nurse and scrub nurse to perform initial count and record on the Registered
Nurse Theatre Report (RNTR) before the procedure is commenced.3. Ensure patient privacy at all times by hanging a privacy notice on the entrance door and
using the privacy screen placed at the entrance of the bunker. 4. Complete documentation on the RNTR and Intra Operative Nursing Care Plan during the
operative procedure.5. Perform first, second and final counts, on completion of the procedure, with the scrub
nurse and record on the RNTR.6. A team time out will be performed in the brachytherapy bunker. RO to go through and
complete the Surgical Safety Checklist. All staff in the room should participate, by pausing other activities and providing a verbal response to the RO. Patient will then be anaesthetised. (Refer to Surgical Safety Checklist Policy for further information).
7. Once patient is anaesthetised patients legs will be positioned simultaneously into lithotomy position using yellowfin stirrups, provided by RTs.
8. Scrub nurse to assist MOs with gowning and gloving once they have performed five minute surgical scrub.
9. Patient will then be prepped with Povidone-iodine solution, usually by MO. The skin prep procedure should include the patient’s perineum, genitals, medial thighs, lower anterior abdominal wall, anus and buttocks. (Refer ACORN standard 2016/2017 Preoperative Patient Skin Antisepsis).
10. Once the prepped skin is dry, the Ioban is positioned by MO. The MO applies the Ioban to push the penis and scrotum up towards the abdomen. The Ioban dressing is placed over the genitals to hold them in place and keep them out of the way.
11. Sterile urology drapes to be applied to the patient’s legs, pelvis and abdomen by the scrub nurse or scrubbed MO to create the aseptic field.
12. The RO inserts the rectal ultrasound probe into the rectum. 13. The RO attaches the stepper holder and the template in place against the patient’s skin.14. The RO will then insert three (3) fiducial markers aseptically into the prostate under
guided ultrasound.Doc Number Version Issued Review Date Area Responsible PageCHHS18/137 1 27/04/2018 01/03/2021 CACHS -
Brachytherapy12 of 27
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS18/137
At the end of the Fiducial Marker Implant ProcedureRN/ scrub nurse:1. Assist MO to remove Ioban from patient. 2. Wash the patient’s prepped area with water and dry with combines.3. Discard fiducial marker applicators, along with any other sharps, in sharps container
provided in the brachytherapy bunker.4. Place template and equipment in a kidney dish (it is important that all small pieces are
retained for sterilisation and not accidently discarded). All equipment is checked by RTs against the tray list.
5. Remove gown and outer gloves in brachytherapy bunker.6. Provide assistance lowering the patient’s legs simultaneously from the stirrups and
transferring the patient to their bed.7. Escort the patient to the recovery area of Radiation Oncology, receive a handover from
the anaesthetist and the patient is then recovered (refer to Post-operative handover and Observations – Adult patients – first 24 hours).
8. Review all theatre paperwork, sign on the RNTR to indicate that the final count is correct, and sign the bottom of form as the registered nurse.
9. Ensure that the RO who performed the procedure signs the RNTR.10. Post-Operative Observations are as follows:
10.1 10 minute observations for 30 minutes10.2 30 minute observations for two hours10.3 hourly observations for 4 hours10.4 4 hourly observations for the rest of the period10.5 Observations to be adjusted as the situation requires.
Following the Fiducial Marker Implant Procedure1. Patient can be discharged home from Radiation Oncology approximately 4 hours post
operatively following consent from the RO.2. Patient is able to eat and drink post procedure when fully recovered and as tolerated by
patient.3. Ensure that all theatre paperwork and ARIA documentation is completed and up to date.4. All theatre paperwork is to be photocopied. Original copies are to be sent to medical
records and the copies are to be placed in a tray at nurse’s station in Radiation Oncology to be scanned into the patient’s Aria notes.
5. Nursing documentation is to be entered in patient’s clinical recorder under ‘Encounters’ on ARIA.
6. All prostate brachytherapy equipment will be cleaned by the RTs.
Back to Table of Contents
Doc Number Version Issued Review Date Area Responsible PageCHHS18/137 1 27/04/2018 01/03/2021 CACHS -
Brachytherapy13 of 27
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS18/137
Section 4 – HDR Prostate Brachytherapy & Fiducial Marker Implant Insertion
HDR Prostate Brachytherapy involves temporarily inserting needles or tubes directly into the prostate to allow radiation to be delivered. HDR Brachytherapy involves the use of a radioactive source to treat men with intermediate to high risk prostate cancer.
Equipment - Sterile stock Four x Sterile gowns STP 08 Sterile Urology pack STP 07 Rampleys sponge holding forcep 25cm ( 1 x spare DNO) Back Table Cover Reinforced Sterile Bowl set Sterile Suture Tray Mayo needle holder Catheter Pack TWO x Lignocaine 2% Gel (10g) syringes Ioban 2 dressing (6640EZ) Liquid paraffin 3 way IDC 22FR/Ch (1 x spare) Four x spigots Two x 10mL syringes Two x bladder syringes Two x drawing up syringes Extra packets of Raytec swabs (DNO) Two x Suture (mersilk 0) or 2-0 Silk Reverse cutting needle (679) Mayo towel clips Sterile labels for fluid marking Sterile marking pen Magnetic sharps pad Two x Rectal tube (DNO) Urology Set Double Bag Spike – DUS4008 4L Urinary Drainage Bag Closed System – L153515
Equipment - Unsterile Stock Mepilex®Sacrum Three x Povidine-Iodine solution 30mLs Bottle of sterile water 90mLs 10mL vial of Urografin® 30% TED Stocking appropriate size Sequential Compression Devices (SCD’s) appropriate size 2000mL 0.9% Sodium Chloride irrigation fluid bags x 3 Boxes (For bladder irrigation post
procedure) Catheter retention strap – Flexi-Trak Naso-Fix
Doc Number Version Issued Review Date Area Responsible PageCHHS18/137 1 27/04/2018 01/03/2021 CACHS -
Brachytherapy14 of 27
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS18/137
Barrier-EasyWarm-Active self-warming blanket Antibiotics for the procedure to be available for the anaesthetist Ampicillen 1g,
Metronidazole 500mg/100mL and Gentamicin as requested Safety glasses or goggles Two x clean measuring jugs Procedure under pads e.g. Smart Barrier touch Dry absorbent pad
Pre HDR Prostate Brachytherapy procedure RT:1. Will advise RN of the procedure date. 2. Will organise brachytherapy bunker theatre clean for the day before procedure.3. Provide patients with a list of instructions about procedure, low residue diet and the
fasting for procedure.
RO:1. To advise patient fast from 2400hrs and not consume any food or drink until after the
procedure. (Refer to Fasting Guidelines for Patients Requiring Sedation of Anaesthesia). 2. Chart all medications required for the procedure along with fleet enema (for morning of
the procedure).
RN:1. Book pre admission clinic (PAC) for patient at least two weeks prior to HDR Prostate
Brachytherapy procedure.2. Fax RFA to bed management and admitting Ward. Patient will require admission for at
least two nights. 3. CNC to enter patient into Bed Management register on SharePoint.4. Ensure that all stock, sterile and non-sterile, is available for the procedure.5. Collect the pre admission paperwork and signed patient consent from pre admission
clinic.6. Fax the brachytherapy diet sheet to the Nutrition Department for a low-residue diet, at
least two days prior to the booked procedure. Fax number available through nutrition department.
7. Check the trolley setup and ensure all stock is available.8. Check that fleet enema and all medications required for the procedure has been charted
by MO.9. Take patient’s medication chart to pharmacy ensuring medications will be available for
the day of procedure.10. Contact admitting ward to confirm availability of patient’s bed for duration of treatment,
usually 2-3 nights. Procedure may be cancelled if no bed is available. In these circumstances the Medical Officer will notify patient and patient will be advised to stop fasting.
11. Contact the Nutrition Department to confirm delivery of lunches both days and breakfast on day two to the Radiation Oncology department. Also, confirm low residue diet to be delivered to the admitting ward both nights.
Doc Number Version Issued Review Date Area Responsible PageCHHS18/137 1 27/04/2018 01/03/2021 CACHS -
Brachytherapy15 of 27
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS18/137
Day 1Day of the HDR Prostate Brachytherapy procedure Two RNs will start work at 0700hrs to get the trolleys ready and ensure that everything is
organised for the arrival of the patient. All staff entering the brachytherapy bunker on the day of the procedure must be dressed
in theatre scrubs. RTs will provide the shoe covers, hair covers, masks and eye protection so these items are
available for all staff to put on before entering the bunker.
RN:1. Orientate the patient when they arrive in the department.2. Check patient identification, patient identification wrist band and consent against clinical
notes and stickers while verbally confirming with patient.3. Document baseline observations, usual systolic BP and MEWS score, weight and
complete Pre-Operative checklist. 4. Assist patient to put on white gowns, the first one with the opening at the back and the
other with the opening at the front.5. Administer the fleet enema as charted by MO. 6. Secure patient’s belongings in the radiation oncology drug room. 7. Commence writing Progress Note and complete Pre-Operative Checklist with the patient.8. Put TED stockings on the patient.9. Apply Mepilex®Sacrum to patient’s sacrum area prior to patient being anaesthetised.
RN/Scrub nurse is to set up the brachytherapy bunker:1. Clean and trolley with detergent wipes.2. Check that all packaging is in date, intact, and that sterility has not been compromised.3. Wash hands and open outer packaging of sterile gown, gloves, urology bundle and back
table cover. 4. Open sterile gloves and gowns onto the cleaned and dry dressing trolley. 5. Open back table cover onto cleaned large trolley, discard outer plastic packaging and
open outer layer only.6. Place urology bundle on mayo table. Remove outer packaging and unwrap outer blue
layer only.7. Put on lead apron before scrubbing. Lead aprons are located in the control room of the
brachytherapy bunker and are required to be worn for C-Arm fluoroscopy. Lead aprons should also be secured appropriately using the Velcro and clips provided.
8. Let the circulating nurse know that you are scrubbing.9. Perform five minute surgical scrub, in compliance with the ACORN standards, don sterile
gown and double sterile gloves. (Refer to ACORN Standards-2016/2017- Surgical Hand Antisepsis, Gowning and Gloving Standards and maintain a surgical aseptic field).
10. Prepare the large trolley, with the back table cover. This surgical aseptic field will be used to assemble the template (see figure 1 and 2 below)
11. Prepare the surgical aseptic field and assemble the trolley with the sterile equipment that have been opened by the scout/circulating nurse – see figure 1 in section 4 below. (Refer to ACORN Standards - 2016/2017 – Asepsis).
Doc Number Version Issued Review Date Area Responsible PageCHHS18/137 1 27/04/2018 01/03/2021 CACHS -
Brachytherapy16 of 27
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS18/137
12. Assemble the template and equipment in an aseptic manner under the guidance of the RT (see figure 2 in section 4 below).
13. Set up the Mayo table trolley for IDC insertion. Open IDC pack, sterile dish. Place the rampley sponge holder with counted raytec swabs onto this mayo table too.
14. Place sponge holders with counted, folded raytec swabs, onto the IDC insertion setup.
RN/circulating nurse:1. Open all the sterile equipment, for the template assemble, in accordance with the
ACORN standards, under the direct supervision of the scrub nurse.2. Open the outer packaging of all aseptically wrapped items and pass all the items needed
for the procedure abiding by the ACORN standards and ensuring that no contamination occurs.
3. Perform initial count with the scrub nurse and record on the Registered Nurse Theatre Report (RNTR) before procedure is commenced.
4. Pour Povidone-Iodine solution into the sterile dish for prepping. All fluids on sterile field are to be labelled as per labelling of medicines guidelines.
5. Walk patient to the brachytherapy bunker when the scrub nurse and anaesthetist are ready.
Figure 1: Template and equipment to be assembled on trolley
Figure 2: Assembled Template
Doc Number Version Issued Review Date Area Responsible PageCHHS18/137 1 27/04/2018 01/03/2021 CACHS -
Brachytherapy17 of 27
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS18/137
RN/Scrub nurse: 1. Draw up 90mL of sterile water in two bladder syringes and add 9mL of Urografin®30% to
one of those bladder syringes, this occurs on large aseptically draped trolley. 2. Draw up the 9mL of sterile water in a 10mL syringe with the remaining 1mL of Urografin.
10mLs of air to be drawn up in the other 10mL syringe.3. Ensure all medication/solutions on the aseptic field are clearly labelled as per ACORN
standards.
RN/circulating nurse:1. Open two spigots, 22Fr/Ch 3 way IDC and Lignocaine 2% gel.2. Ensure that Ampicillin, Metronidazole, Gentamicin and a 1 litre bag of 0.9% Sodium
Chloride are in the bunker for the anaesthetic staff.3. Walk the patient to the brachytherapy bunker once everything is set up and the scrub
nurse is ready.4. Ensure patient privacy at all times by hanging a privacy notice on the entrance door and
using the privacy screen placed at the entrance of the bunker. 5. Circulating nurse is responsible for completing RNTR and Intra Operative Nursing care
Plan during the procedure.6. Perform second and final counts, on completion of the procedure, with the scrub nurse
and record on the RNTR.
RO:To perform team time out in the brachytherapy bunker. The RO will go through and complete the Surgical Safety Checklist. All staff in the room should participate, by pausing from activities and providing a verbal response to the RO (refer to Surgical Safety Checklist Policy).
The patient will be met by Anaesthetic team and will have an IV cannula inserted. The patient will be positioned into lithotomy position using yellowfin stirrups, provided by RTs, once anaesthetised. Both legs to be positioned simultaneously then:
1. SCDs are attached to the patient’s legs and plugged in before the sterile drapes are applied.
Doc Number Version Issued Review Date Area Responsible PageCHHS18/137 1 27/04/2018 01/03/2021 CACHS -
Brachytherapy18 of 27
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS18/137
2. The Scrub nurse to assist the MO with gowning after they perform the surgical scrub.3. The patient is prepped with Povidone-Iodine solution include the patient’s perineum,
genitals, medial thighs, lower anterior abdominal wall, anus and buttocks as per ACORN guidelines. (Refer ACORN Standard 2016/2017 – Preoperative Patient Skin Antisepsis).
4. 10mLs of air will be injected into the catheter balloon followed by the combination of 9mLs of water and 1mL of Urografin® contrast. Urografin and water to be recorded on the Intra-Operative Nursing care Plan.
5. The gloved circulating nurse will then fill the bladder with 90mLs water and 10mLs of Urografin®30%, the catheter is then spigotted. Urografin and water to be recorded on the Intra-Operative Nursing Care Plan.
6. Once the prepped skin is dry the Ioban will be positioned. The MO will apply the Ioban to push the penis and scrotum up towards the abdomen. The Ioban dressing is placed over the genitals to hold them in place and keep them out of the way.
7. C-arm is draped and urology drapes will be applied to the patient’s legs, pelvis and abdomen by the scrub nurse or scrubbed MO to create the aseptic field.
8. Any soiled swabs and dishes are removed with the IDC trolley. The circulating nurse will ensure that swabs are put to the side for surgical counting later.
Alert: Never remove anything from the bunker after the initial count. All accountable items must remain in the bunker for surgical counting.
9. MO inserts the rectal ultrasound probe into the rectum.10. The RO will attach the stepper holder and the template will then place against the
patient’s skin.11. Three fiducial markers will be inserted by the RO into the prostate prior to commencing
the implant procedure. These will be inserted aseptically under ultrasound guidance. 12. Implants to be recorded on the Registered Nurse Theatre Report including Lot number
and expiry date.13. The implant needles will then be inserted through the template by the RO. C-arm
images are taken periodically throughout the implant procedure as requested by the RO and to determine the positioning of the needles.
14. Once needle positioning has been verified the template will be sutured to the patient’s perineum. This procedure takes around 60-90 minutes.
15. On completion of the procedure second and final counts are performed by the scrub and circulating nurses. This is to be recorded on the RNTR.
Set up trolleys for end the HDR Prostate Brachytherapy procedure (outside the bunker)RN/Circulating nurse:1. Continual bladder irrigation (CBI) is set up on an IV pole with 2 x 2L 0.9% Sodium Chloride
irrigation bags. Irrigation bags to be numbered. These are set up outside the bunker, along with a urology set double bag spike and a 4L urinary drainage bag closed system.
2. CBI is to be commenced on the completion of the procedure once the patient has been slid onto recovery bed. This bed will contain the hover mattress.
Doc Number Version Issued Review Date Area Responsible PageCHHS18/137 1 27/04/2018 01/03/2021 CACHS -
Brachytherapy19 of 27
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS18/137
3. Keep spare IDC, bladder syringes, kidney dishes, contrast, drawing up needles, swabs, scissors, forceps, and IDC drainage bag with integrated pump attached.
At the end of the HDR Prostrate Brachytherapy procedureRN/scrub nurse: Assist MO remove Ioban from the patient. Wash the patient’s prepped area with water and dry with combines. Discard all sharps in the provided sharps bin in the brachytherapy bunker (it is important
that all small pieces related to the prostate template sets are retained for sterilisation and not accidently discarded). All equipment is checked by RTs against the tray list.
Remove gown and top gloves in the brachytherapy bunker. Provide assistance putting the patient’s legs down simultaneously and transferring the
patient to their bed. Attach catheter bag, ensuring plug on tubing is pushed in prior to insertion. Naso-Fix tape is applied to the tip of the penis and wrapped around the IDC to prevent it
coming loose and ensure the indwelling catheter is secured with the appropriate device e.g. Flexi Track.
Commence CBI once the patient is transferred from treatment table to their bed (refer to Catheter Insertion and Management Bladder Irrigation, Nephrectomy and Trans Urethral Prostatectomy (TURP) Procedure).
RT: RT will prepare and position an implant protection cup which is positioned over the
implant needles to protect them before the patient leaves the brachytherapy bunker. Position and secure charnley pillow between the patient’s ankle and legs to keep legs
abducted. Clean the brachytherapy template and all other related equipment at the end of the
procedure.
RN/scrub nurse: Before the patient leaves the bunker, the “check out” section on the surgical safety
checklist should be completed. This includes checking that the surgical count is correct, and that the team members have expressed any key concerns for recovery.
Ensure SCDs and TED stockings are left insitu for the next two days. Escort the patient to the recovery area of Radiation Oncology, receive a handover from
the anaesthetist and the patient is then recovered (refer to relevant Canberra Hospital procedures for postoperative handover and observations).
Review all theatre paperwork and sign on the RNTR to indicate that the final count is correct, and sign the bottom of form as the registered nurse.
Ensure that the MO who performed the procedure signs the bottom of the RNTR.
Post-Operative HDR Prostate Brachytherapy Procedure/recovery performed by Radiation Oncology nurses1. RN to receive a clinical handover from the anaesthetist.2. Anaesthetised patient to be awake before anaesthetist leaves the department.
Doc Number Version Issued Review Date Area Responsible PageCHHS18/137 1 27/04/2018 01/03/2021 CACHS -
Brachytherapy20 of 27
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS18/137
3. Post-Operative Observations are as follows: 10 minute observations for 30 minutes 30 minute observations for two hours 1 hourly observations for 4 hours 4 hourly observations for the rest of the period, more often if clinically indicated Observations to be adjusted as the situation requires (refer to – Post Operative
Handover and Observations –Adult patients-first 24 hours).4. Observe the implantation site for ooze or blood loss.5. Patient is recovered by Radiation Oncology nursing staff. 6. Maintain patient privacy at all times.7. Ensure adequate and appropriate analgesia, especially prior to first planning CT scan.8. The patient must be rolled for pressure area care regularly and staff must ensure that
this information is handed over to ward staff. 9. If the patient has back pain they can have a pillow inserted behind their knees to take
pressure off their back.10. Hang irrigating fluid bags on portable IV pole, 60cm above the level of the bladder. Label
and number each bag when commencing.11. Maintain strict Bladder Irrigation Chart and Urine Output records. Ensure all output is
recorded on the fluid balance chart.12. The patient is able to eat once awake and sufficiently recovered. The low residue diet will
be delivered to the department for lunch time.13. Monitor bladder irrigation for clots. If not flowing properly then clamp off IDC below the
rubber ball until the line fills with urine. Gently squeeze the ball, pushing fluid back up into the catheter and then release clamp. This usually dislodges clots. If not, repeat the same process.
Note: penile tip pain could be an indication that the catheter balloon has been perforated by the implant needles and the catheter may need replacing. If this is the case, contact the Radiation Oncologist and set up a trolley for IDC insertion. The patient may require sedation and/or analgesia as ordered by the MO so this should be confirmed before set up for IDC insertion.
14. Continuous bladder irrigation (CBI) works by releasing the clamp on the first 2L bag of 0.9% Sodium chloride while the second bag is clamped. Ensure that the clamp on the IDC is open.
15. The roller clamp determines the flow of the 0.9% Sodium Chloride into the bladder, so it should be monitored and adjusted as necessary according to colour of urine return - rose or clear.
16. Heavily blood stained urine may require faster irrigation. Always keep two jugs at foot of patient’s bed to empty the bag if required. Record all output, input and colour of return on CBI chart. Refer to Urology – Catheter Insertion and Management, Bladder Irrigation, Nephrectomy and Trans Urethral Prostatectomy (TURP) Procedure
CT Planning Procedure pre HDR treatment
Doc Number Version Issued Review Date Area Responsible PageCHHS18/137 1 27/04/2018 01/03/2021 CACHS -
Brachytherapy21 of 27
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS18/137
At the completion of the HDR prostate brachytherapy implant procedure the patient will have a planning CT in Radiation Oncology.
Urografin® contrast is only used prior to CT but is not used prior to treatment.
RN: Administer analgesia to ensure patient comfortable during the CT procedure. Stop bladder irrigation. Drain the bladder and then re fill it with 100mL of solution (ratio
90mL water: 10ml Urografin® 30%) via the catheter. As this is uncomfortable for the patient, it should be completed as the last step before scanning. Injection of water and Urografin into bladder via the catheter to be recorded on the patient progress note.
Clamp off IDC as well or take bag off and spigot bag access. Escort patient to the CT scanner on their bed on the hover mat will be used to transfer
patient to CT bed. Ensure patient privacy at all times by hanging a privacy notice on the entrance and using
the privacy screen placed at the entrance of the bunker. Following the CT scan the RTs will replace the needle protection cup. Re position charnley pillow between the patient’s legs and re-start CBI. Pressure area care and skin integrity checks to be performed. Always replace TEDs, SCDs and charnley pillow following pressure area care. The patient
must be log rolled with charnley pillow insitu. Monitor the brachytherapy implant needles and the patient for penile tip pain and
rectal/anal pain.
Brachytherapy Treatment1. The patient commences treatment once the treatment plan is completed. The first
treatment will usually occur late in the afternoon (around 4:30pm) on the first day.2. Patients having treatment to the prostate are generally treated with 100mL of water in
their bladder.
RN: Stop bladder irrigation, drain the bladder and then fill it with 100mL of sterile water into
the bladder via the catheter. As this is uncomfortable for the patient, it should be completed as the last step before treatment.
Disconnect calf compressor pump for treatment. On completion of treatment fraction, bladder filling is released, CBI to be re connected
and commenced. Calf compressor pump to be reconnected and commenced. Patient will be transported back to the nursing bay in their bed. Photocopy the theatre paperwork, original paperwork to go to the admitting ward with
the patient, copied paperwork to be placed in a tray at nurse’s station in Radiation Oncology to be scanned into the patient’s Aria notes. Paper copies are destroyed after three months.
To record all nursing documentation in encounters on ARIA. Contact RMO to complete Medical admission in Radiation Oncology prior to patient
being transferred to admitting ward.Doc Number Version Issued Review Date Area Responsible PageCHHS18/137 1 27/04/2018 01/03/2021 CACHS -
Brachytherapy22 of 27
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS18/137
Complete Patient Care and Accountability Plan (PCAP) and action appropriately inclusive of indicating bladder irrigation.
Record in the patient’s clinical record, all post-operative nursing care provided and the patient’s response.
Accompany patient to the admitting ward in their Radiation Oncology bed, which they will remain in.
Transfer of care must reflect requirements as per the Clinical Handover Procedure.
Ward Management1. Check patient clinical records for medical orders.2. Maintain patent IV cannula.3. Maintain 4 hourly vital signs.4. Maintain CBI.5. Maintain strict Fluid Balance Chart.6. Monitor the implant insertion site for ooze or blood loss fourth hourly. 7. Patient to remain on their back, with charnley pillow insitu between their legs.8. Patient’s entire bed needs to be tilted for patient to eat. Patient is not to be sat up as this
may dislodge the prostate needles that must remain insitu.9. Ensure 2 hourly pressure area care and skin integrity checks are offered and performed.10. TEDs are to remain insitu.11. Patient to remain on low residue diet.12. Advise the ward staff to give the patient adequate analgesia before returning to clinic for
their second treatment the following morning. 13. Ensure that patient’s regular medications are sent down from the ward on the second
treatment day also (refer to relevant Canberra Hospital procedures for hand over and post- operative observations).
Day 2 Prostate Brachytherapy Treatment1. Patient brought to the Radiation Oncology Clinic at 0700hrs.
RN in Radiation Oncology: Check the medication chart to ensure adequate analgesia has been administered
prior to the patient going to CT. Set up water and Urografin®30% for CT. Clamp off and disconnect the CBI, IDC and spigot bag access. Insert a 100mL solution of contrast and sterile water into the bladder (ratio 90mLs
water: 10mLs Urografin®30%) via the catheter. Water and Urografin injected into the bladder via the catheter to be recorded on the patient progress note.
Escort the patient to the CT scanner on their bed and the hover mat will be used to transfer patient to CT bed. The calf compressor pump will be disconnected for the CT scan.
Staff to help roll the patient on left side while RN gently inserts tube using KY jelly as the lubricant. Leave in for 5-10 minutes then remove. Do not force rectal tube too far or hard as perforation could occur. This will help to relieve flatus which has accumulated overnight.
Doc Number Version Issued Review Date Area Responsible PageCHHS18/137 1 27/04/2018 01/03/2021 CACHS -
Brachytherapy23 of 27
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS18/137
Once CT is completed restart CBI and re-connect and commence calf compressor pump.
Patient will be transferred back to the nursing bay and set patient up for breakfast. Continue to monitor CBI and check to see if morning medications have been given. Ensure that the patient’s lunch arrives from the ward. Wash patient in bed and attend to pressure area care.
2. The patient will have two treatments while in clinic, one in the morning and one later that day – the treatments will be at least six hours apart. The patient requires 100mLs of water inserted into the bladder before both treatments.
3. If further CT scans are required, mix contrast into the water at the ratio of 90mL water: 10mL Urografin® 30%. Water and Urografin injected into the bladder via the catheter to be recorded in the patient progress note.
4. Patient will remain in the Radiation Oncology department for the day. Patient can have breakfast and lunch between treatments.
Alert:Please leave the IVC insitu as the patient may require sedation prior to the template removal. It also enables quick IV access if needed.
End of Day 21. Contact wards person to go up to the ward and bring a bed down for the patient. 2. Patient will remain in the Radiation Oncology department until the template is removed
after the final treatment is given.3. Prior to the final treatment, RN to set up a trolley for removal of the template with:
Stitch cutter Suture holder Gauze and combines Sedation/analgesia as per charted and Dr’s request
4. Following the patient’s final treatment, MO may give sedation/analgesia prior to the removal of the template.
5. At the completion of the final fraction of treatment, the sutures will be cut, and the template and needles will be removed by the RO.
6. All template and equipment to be placed in a kidney dish for the RTs (it is important that all small pieces are retained for sterilisation and not accidently discarded). All template equipment will be cleaned, and checked against the instrument tray list, by the RTs.
7. RN to don PPE8. After removal of the template the RN to apply combines to the perineum until the
bleeding stops. Check that all needles have been removed before applying pressure. Pressure to the perineum will minimise swelling and bruising.
9. RN to increase the flow rate on the CBI as the urine output will be frank blood return.10. Monitor the urine return and after it settles the patient can get up and walk around. 11. The IDC remains insitu until the following day and the CBI will continue.12. The patient will be transferred back to the ward once the MO is satisfied that the patient
is fit for transfer.Doc Number Version Issued Review Date Area Responsible PageCHHS18/137 1 27/04/2018 01/03/2021 CACHS -
Brachytherapy24 of 27
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS18/137
13. The patient will be reviewed by a RO the next morning prior to discharge. 14. If a problem arises with the IDC or there are clotting issues, staff must contact the RO
who performed the procedure.15. Patient is not discharged from the ward until they can urinate without a catheter and
until the urine is reasonably clear.
Back to Table of Contents
Implementation
This procedure will be communicated through an all of staff DDG email and implemented with in-services to wards and education to Radiation Oncology staff.
Back to Table of Contents
Related Policies, Procedures, Guidelines and Legislation
Policies Health Directorate Nursing and Midwifery Continuing Competence Policy Health Directorate Patient Identification Policy and Procedure CHHS Policy - Consent and treatment Patient Identification and Procedure Matching Policy Medication Handling Policy Surgical Safety Checklist Policy
Procedures Healthcare Associated Infections Clinical Procedure CHHS Radiation Therapy Operations Manual – Brachytherapy Patient Identification and Procedure Matching Procedure Clinical Handover Procedure Pressure Injury Prevention and Management Procedure Vital Signs and Early Warning Scores Procedure Urology – Catheter Insertion and Management, Bladder Irrigation, Nephrectomy and
Trans Urethral Prostatectomy (TURP) Procedure Aseptic Non Touch Technique Standard Operating Procedure
Guidelines Fasting Guidelines – Elective and Emergency Surgery patients
Standards ACORN Standards 2016/2017 - Asepsis ACORN Standards 2016/2017 – Preoperative Patient Skin Antisepsis ACORN Standards 2016/2017 – Surgical Hand Antisepsis, Gowning and Gloving Standards
and maintaining a Surgical Aseptic Field Radiation Oncology Practice Standards 2011
Doc Number Version Issued Review Date Area Responsible PageCHHS18/137 1 27/04/2018 01/03/2021 CACHS -
Brachytherapy25 of 27
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS18/137
Legislation Health Records (Privacy and Access) Act 1997 Human Rights Act 2004 Work Health and Safety Act 2011 Privacy Act 1988
Back to Table of Contents
References
1. 5 moments of Hand Washing- Hand Hygiene Australiahttp://www.hha.org.au/
2. Canberra Hospital and Health Services Radiation Therapy Operations Manual - Brachytherapy
3. World Health Organisation (WHO) Guidelines on Hand Hygiene in Healthcare 4. http://www.nursingmidwiferyboard.gov.au/Codes-and-Guidelines.aspx
Back to Table of Contents
Abbreviations
Indwelling catheter (IDC)Computerised Tomography (CT)Do not open (DNO)Pre admission clinic (PAC)Registered nurse theatre report (RNTR)Continual bladder irrigation (CBI)Patient care and accountability plan (PCAP)Radiation Oncologist (RO)Medical Officer (MO)Radiation therapist (RT)High Dose rate (HDR) Brachytherapy
Back to Table of Contents
Definition of Terms
Low residue diet: Is a diet that limits high-fibre foods, like whole-grain breads and cereals, nuts, seeds, raw or dried fruit, and vegetables.
Back to Table of Contents
Search Terms
Brachytherapy, Radiation Oncology, vaginal vault, fiducial markers, volume studies, radiotherapists, prostate brachytherapy, bunker, scout nurse, scrub nurse, bladder irrigation, CT, HDR and Urografin
Doc Number Version Issued Review Date Area Responsible PageCHHS18/137 1 27/04/2018 01/03/2021 CACHS -
Brachytherapy26 of 27
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS18/137
Disclaimer: This document has been developed by ACT Health, Canberra Hospital and Health Services specifically for its own use. Use of this document and any reliance on the information contained therein by any third party is at his or her own risk and Health Directorate assumes no responsibility whatsoever.
Policy Team ONLY to complete the following:Date Amended Section Amended Divisional Approval Final Approval 21/02/2018 New Document Denise Lamb CHHS Policy Committee
This document supersedes the following: Document Number Document Name
Doc Number Version Issued Review Date Area Responsible PageCHHS18/137 1 27/04/2018 01/03/2021 CACHS -
Brachytherapy27 of 27
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register