Br Heart ' Varicella
3
Br Heart_' 1993;70:93-95 Varicella zoster myocarditis progressing to cardiomyopathy and cardiac transplantation Andrew Tsintsof, Warwick J Delprado, Anne M Keogh Abstract The case of a 12 year old schoolgirl with heart failure due to varicella myocarditis is reported. Heart failure and cardio- genic shock were evident 21 days after the appearance of the rash, and cardiac transplantation was performed two weeks later. Myocarditis is a serious complication of varicella zoster infection and heart failure may be fulminant. Endomyocardial biopsy changes consis- tent with myocarditis were documented six days after the start of heart failure. The histological changes, however, developed into those of idiopathic dilated cardiomyopathy (with anisonucleosis and fibre width variation) over a seven day period. This case provides fiurther evidence for the link between viral myocarditis and idiopathic cardiomy- opathy and underlines the value of immediate endomyocardial biopsy in heart failure of recent onset. Cardiac transplantation led to a rapid and full recovery. (Br Heart J 1993;70:93-95) Primary infection with varicella zoster virus (chickenpox) is characterised by a generalised pruritic vesicular rash, usually without signifi- cant systemic illness. Serious complications such as encephalitis, pneumonitis, pancreati- tis, and nephritis may occur, however, partic- ularly in neonates, immunocompromised patients, and sometimes normal adults.' Myocarditis is an uncommon but serious complication. We report on a previously healthy child who developed biopsy-proven myocarditis after a primary infection with varicella zoster virus. This rapidly developed into a dilated cardiomyopathy (with histologi- cal changes consistent with this diagnosis) and the girl then needed cardiac transplanta- tion. Cardiopulmonary Transplant Unit, St Vincent's Hospital, Darlinghurst, Sydney, Australia A Tsintsof W J Delprado A M Keogh Correspondence to: Dr Anne Keogh, Cardiopulmonary Transplant Unit, St Vincent's Hospital, Darlinghurst, 2010, NSW, Sydney, Australia. Case report A 51 kg, 12 year old schoolgirl presented with a five day history of vomiting, exertional dys- pnoea, cough, and extreme lethargy that start- ed 21 days after the start of an itchy, vesiculopapular rash diagnosed as chicken pox. Initial treatment comprised salicylates and two weeks isolation. Previously the patient had experienced no major illness. There was no relevant family history of heart disease. On presentation she was pale, peripherally cool, unwell, and lethargic. Heart rate was 145 beats/minute, blood pressure was 95/60 mm Hg, and she was afebrile. Jugular venous pressure was elevated to the jaw, the apex beat was displaced laterally, and a third heart sound was audible. Lung fields were clear and there was no hepatomegaly or peripheral oedema. A chest radiograph showed cardiomegaly, pulmonary venous congestion, interstitial oedema, and small bilateral pleural effusions. The electrocardiogram showed sinus tachy- cardia, a nonspecific intraventricular conduc- tion defect, poor anterior R wave progression and inferolateral ST-T wave changes. The white cell count was 12-7 x 109/I (normal 4-11 x 109/I) with a neutrophilia (neutrophils 71%, lymphocytes 14%, monocytes 15%). Serum potassium (3-2 mmol/l) and magne- sium 074 mmol/l) concentrations were sub- normal. Serum albumin, creatinine, and urea concentrations, and hepatic transaminase activities were normal. Serological studies confirmed a recent primary varicella zoster infection with positive IgM and viral antibody titre of 32 (complement fixation test). Coxsackie, echo, influenza A and B, measles, cytomegalovirus, and Epstein Barr viral titres were all negative. Thyroid function testing was consistent with a sick euthyroid state. Echocardiography showed a considerably dilated, diffusely hypokinetic left ventricle with end diastolic diameter 73 mm (normal 35-56 mm) and dilated left atrium (47 mm, normal < 40 mm). There was moderate mitral regurgitation, mild tricuspid regurgita- tion, and a large apical thrombus. Left ventricular ejection fraction was 22% on radionuclide ventriculography. Endomyo- cardial biopsy performed 28 days after the start of the rash showed focal aggregates of mononuclear cells (> 5 lymphocytes/high power field), anisonucleosis, variation in fibre diameter and scattered necrotic myocytes with lymphocyte "cuffing" (fig). A diagnosis of varicella myocarditis was made. Fluid and salt restriction, frusemide, digoxin, captopril, and anticoagulation with heparin were started. In an attempt to limit myocardial destruction, 500 mg/day methyl- prednisolone was given intravenously for three consecutive days followed by a tapered dose of oral prednisolone (1 mg/kg/day reducing over 14 days to 02 mg/kg/day), and 1 mg/kg/day azathioprine orally was started. She also received acyclovir (500 mg eight hourly) intravenously. By 30 days after the 93 on November 18, 2021 by guest. Protected by copyright. http://heart.bmj.com/ Br Heart J: first published as 10.1136/hrt.70.1.93 on 1 July 1993. Downloaded from
Transcript of Br Heart ' Varicella

Br Heart_' 1993;70:93-95
Varicella zoster myocarditis progressing tocardiomyopathy and cardiac transplantation
Andrew Tsintsof, Warwick J Delprado, Anne M Keogh
AbstractThe case of a 12 year old schoolgirl withheart failure due to varicella myocarditisis reported. Heart failure and cardio-genic shock were evident 21 days afterthe appearance of the rash, and cardiactransplantation was performed twoweeks later. Myocarditis is a seriouscomplication of varicella zoster infectionand heart failure may be fulminant.Endomyocardial biopsy changes consis-tent with myocarditis were documentedsix days after the start of heart failure.The histological changes, however,developed into those of idiopathic dilatedcardiomyopathy (with anisonucleosisand fibre width variation) over a sevenday period. This case provides fiurtherevidence for the link between viralmyocarditis and idiopathic cardiomy-opathy and underlines the value ofimmediate endomyocardial biopsy inheart failure of recent onset. Cardiactransplantation led to a rapid and fullrecovery.
(Br Heart J 1993;70:93-95)
Primary infection with varicella zoster virus(chickenpox) is characterised by a generalisedpruritic vesicular rash, usually without signifi-cant systemic illness. Serious complicationssuch as encephalitis, pneumonitis, pancreati-tis, and nephritis may occur, however, partic-ularly in neonates, immunocompromisedpatients, and sometimes normal adults.'Myocarditis is an uncommon but seriouscomplication. We report on a previouslyhealthy child who developed biopsy-provenmyocarditis after a primary infection withvaricella zoster virus. This rapidly developedinto a dilated cardiomyopathy (with histologi-cal changes consistent with this diagnosis)and the girl then needed cardiac transplanta-tion.
CardiopulmonaryTransplant Unit, StVincent's Hospital,Darlinghurst, Sydney,AustraliaA TsintsofW J DelpradoAM KeoghCorrespondence to:Dr Anne Keogh,CardiopulmonaryTransplant Unit, StVincent's Hospital,Darlinghurst, 2010, NSW,Sydney, Australia.
Case reportA 51 kg, 12 year old schoolgirl presented witha five day history of vomiting, exertional dys-pnoea, cough, and extreme lethargy that start-ed 21 days after the start of an itchy,vesiculopapular rash diagnosed as chickenpox. Initial treatment comprised salicylatesand two weeks isolation. Previously the patienthad experienced no major illness. There was
no relevant family history of heart disease.
On presentation she was pale, peripherallycool, unwell, and lethargic. Heart rate was145 beats/minute, blood pressure was 95/60mm Hg, and she was afebrile. Jugular venouspressure was elevated to the jaw, the apexbeat was displaced laterally, and a third heartsound was audible. Lung fields were clearand there was no hepatomegaly or peripheraloedema.A chest radiograph showed cardiomegaly,
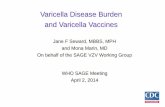
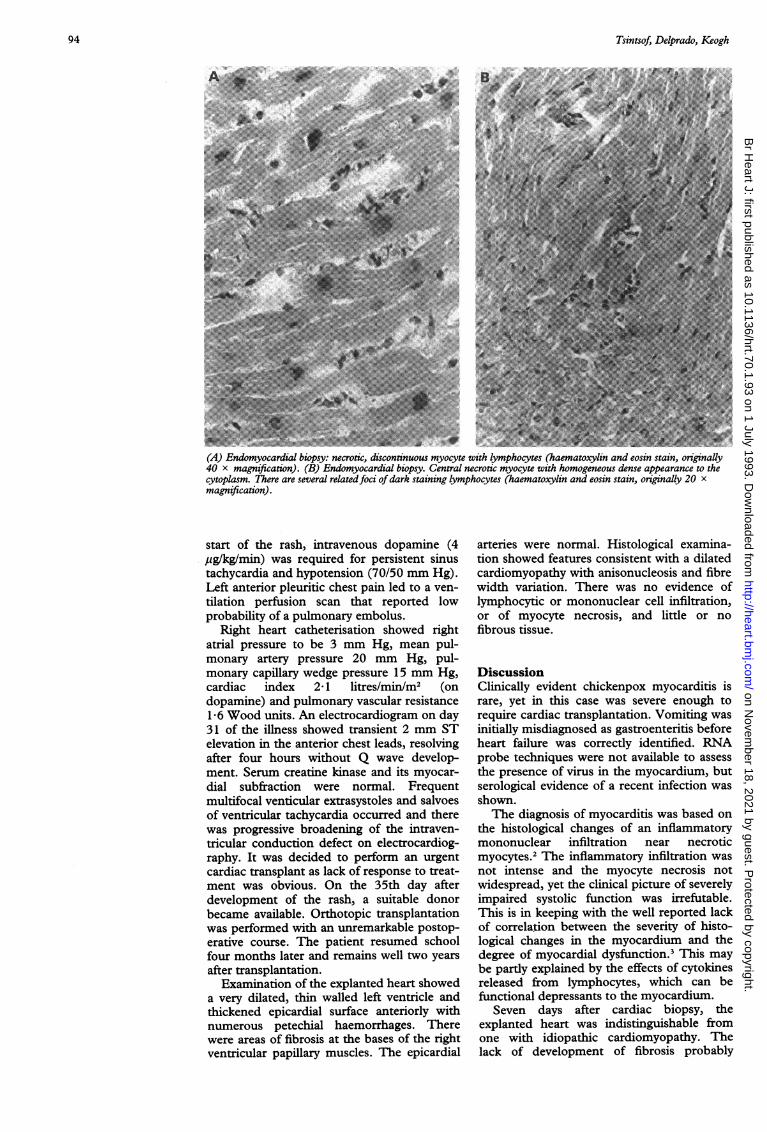
pulmonary venous congestion, interstitialoedema, and small bilateral pleural effusions.The electrocardiogram showed sinus tachy-cardia, a nonspecific intraventricular conduc-tion defect, poor anterior R wave progressionand inferolateral ST-T wave changes. Thewhite cell count was 12-7 x 109/I (normal4-11 x 109/I) with a neutrophilia (neutrophils71%, lymphocytes 14%, monocytes 15%).Serum potassium (3-2 mmol/l) and magne-sium 074 mmol/l) concentrations were sub-normal. Serum albumin, creatinine, and ureaconcentrations, and hepatic transaminaseactivities were normal. Serological studiesconfirmed a recent primary varicella zosterinfection with positive IgM and viral antibodytitre of 32 (complement fixation test).Coxsackie, echo, influenza A and B, measles,cytomegalovirus, and Epstein Barr viral titreswere all negative. Thyroid function testingwas consistent with a sick euthyroid state.Echocardiography showed a considerablydilated, diffusely hypokinetic left ventriclewith end diastolic diameter 73 mm (normal35-56 mm) and dilated left atrium (47 mm,normal < 40 mm). There was moderatemitral regurgitation, mild tricuspid regurgita-tion, and a large apical thrombus. Leftventricular ejection fraction was 22% onradionuclide ventriculography. Endomyo-cardial biopsy performed 28 days after thestart of the rash showed focal aggregates ofmononuclear cells (> 5 lymphocytes/highpower field), anisonucleosis, variation in fibrediameter and scattered necrotic myocyteswith lymphocyte "cuffing" (fig).A diagnosis of varicella myocarditis was
made. Fluid and salt restriction, frusemide,digoxin, captopril, and anticoagulation withheparin were started. In an attempt to limitmyocardial destruction, 500 mg/day methyl-prednisolone was given intravenously forthree consecutive days followed by a tapereddose of oral prednisolone (1 mg/kg/dayreducing over 14 days to 02 mg/kg/day), and1 mg/kg/day azathioprine orally was started.She also received acyclovir (500 mg eighthourly) intravenously. By 30 days after the
93
on Novem
ber 18, 2021 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.70.1.93 on 1 July 1993. D
ownloaded from
Tsintsof, Delprado, Keogh
(A) Endomyocardial biopsy: necrotic, discontinuous myocyte with lymphocytes (haematoxylin and eosin stain, originally40 x magnification). (B) Endomyocardial biopsy. Central necrotic myocyte with homogeneous dense appearance to thecytoplasm. There are several relatedfoci ofdark staining lymphocytes (haematoxylin and eosin stain, originally 20 xmagnification).
start of the rash, intravenous dopamine (44ug/kglmin) was required for persistent sinustachycardia and hypotension (70/50 mm Hg).Left anterior pleuritic chest pain led to a ven-
tilation perfusion scan that reported lowprobability of a pulmonary embolus.
Right heart catheterisation showed rightatrial pressure to be 3 mm Hg, mean pul-monary artery pressure 20 mm Hg, pul-monary capillary wedge pressure 15 mm Hg,cardiac index 2 1 litres/min/m2 (ondopamine) and pulmonary vascular resistance1 6 Wood units. An electrocardiogram on day31 of the illness showed transient 2 mm STelevation in the anterior chest leads, resolvingafter four hours without Q wave develop-ment. Serum creatine kinase and its myocar-dial subfraction were normal. Frequentmultifocal venticular extrasystoles and salvoesof ventricular tachycardia occurred and therewas progressive broadening of the intraven-tricular conduction defect on electrocardiog-raphy. It was decided to perform an urgentcardiac transplant as lack of response to treat-ment was obvious. On the 35th day afterdevelopment of the rash, a suitable donorbecame available. Orthotopic transplantationwas performed with an unremarkable postop-erative course. The patient resumed schoolfour months later and remains well two yearsafter transplantation.
Examination of the explanted heart showeda very dilated, thin walled left ventricle andthickened epicardial surface anteriorly withnumerous petechial haemorrhages. Therewere areas of fibrosis at the bases of the rightventricular papillary muscles. The epicardial
arteries were normal. Histological examina-tion showed features consistent with a dilatedcardiomyopathy with anisonucleosis and fibrewidth variation. There was no evidence oflymphocytic or mononuclear cell infiltration,or of myocyte necrosis, and little or nofibrous tissue.
DiscussionClinically evident chickenpox myocarditis israre, yet in this case was severe enough torequire cardiac transplantation. Vomiting wasinitially misdiagnosed as gastroenteritis beforeheart failure was correctly identified. RNAprobe techniques were not available to assessthe presence of virus in the myocardium, butserological evidence of a recent infection wasshown.The diagnosis of myocarditis was based on
the histological changes of an inflammatorymononuclear infiltration near necroticmyocytes.' The inflammatory infiltration wasnot intense and the myocyte necrosis notwidespread, yet the clinical picture of severelyimpaired systolic function was irrefutable.This is in keeping with the well reported lackof correlaion between the severity of histo-logical changes in the myocardium and thedegree of myocardial dysfunction.' This maybe partly explained by the effects of cytokinesreleased from lymphocytes, which can befunctional depressants to the myocardium.
Seven days after cardiac biopsy, theexplanted heart was indistinguishable fromone with idiopathic cardiomyopathy. Thelack of development of fibrosis probably
94
on Novem
ber 18, 2021 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.70.1.93 on 1 July 1993. D
ownloaded from

Varicella zoster myocarditis progressing to cardiomyopathy and cardiac transplantation
reflects the short time of illness. This rapidchange in histological appearance adds toother evidence linking acute myocarditis withidiopathic dilated cardiomyopathy.45 It alsoshows the potentially rapid transition ofmyocarditis to postmyocarditic cardiomyo-pathy and the need to biopsy as early as pos-sible in cases of heart failure of recent onset.Repeat endomyocardial biopsy has beenadvocated between three weeks and threemonths after the initiation of treatment formyocarditis.6 Other reports, however indicatethat early repeat endomyocardial biopsy(within four days) may show remarkablechanges in histopathology.5
Chickenpox affects 90% of children duringthe first decade of life.7 It seems possible thatsubclinical varicella myocarditis may underlieentities previously classified as idiopathic car-diomyopathy and such a myocardial insultcould leave the heart more prone to dysfunc-tion when stressed in later life.
Acyclovir was given after the varicelliformskin manifestations had resolved. We areaware of three reports in which acyclovir hasbeen used in varicella myocarditis.810 Thesepatients received acyclovir within five days ofthe start of exanthem. One patient recoveredfully, another was left with heart block andleft ventricular impairment, and third patientdied. It seems certain that our patient wouldhave died had a donor not become available.The use of acyclovir did not appear to bebeneficial. Acyclovir may be useful againstVaricella in normal adults," in preventing dis-semination in immunocompromised chil-dren'2 13 and in shortening the duration offever and skin manifestations in normal chil-dren when given orally within 24 hours ofdeveloping the rash.14 Acyclovir may thus bepotentially beneficial in varicella myocarditisif presentation occurs during the stage of viralreplication within the myocardium. This ismore likely early in the course of the illnesswhile new skin lesions are still appearing.
Steroid treatment and azathioprine werealso given in an attempt to prevent furthermyocardial destruction. The place of im-munosuppression, however, in the treatment
of myocarditis, particularly that mediated byviruses, remains controversial.6 1%17 In thiscase, there was deterioration in clinical statedespite reduction in inflammatory infiltrate.
In conclusion, the histopathologicalchanges seen in this case are evidence thatacute chickenpox myocarditis can progressrapidly to dilated cardiomyopathy. Such atransition may occur within a seven dayperiod. Chickenpox is a common conditionand it is conceivable that subclinical infectionor myocarditis may contribute to some casesof idiopathic dilated cardiomyopathy.
1 Straus S, Ostrove J, Inchauspe G, et al. Varicella-zostervirus infections. Ann Intern Med 1988;108:221-37.
2 Aretz H, Billingham M, Edwards W, et al. Myocarditis: ahistopathologic definition and classification. Am JCardiovasc Pathol 1986:1:3-14.
3 Schwarz F, Mall G, Zebe H, et al. Determinants of sur-vival in patients with congestive cardiomyopathy: quan-titative morphological findings and left ventricularhemodynamics. Circulation 1984;70:923-8.
4 Billingham M, Tazelaar H. The morphological progres-sion of viral myocarditis. Postgrad MedJ 1986;62:581-4.
5 Keogh A, Billingham M, Schroeder J. Rapid histologicalchanges in endomyocardial biopsy specimens aftermyocarditis. Br Heart _j 1990;64:406-8.
6 Hosenpud J, McAnulty J, Niles N. Lack of objectiveimprovement in ventricular systolic function in patientswith myocarditis treated with azathioprine and pred-nisone. _J Am Coll Cardiol 1985;6:797-801.
7 Guess H. Population-based studies of Vanrcella complica-tions. Paediatrics 1986;78:723-7.
8 Coppack S, Doshi R, Ghose A. Fatal Varicella in a healthyyoung adult. Postgrad MedJ 1985;61:529-31.
9 Ettedgui J, Ladusans E, Bamford M. Complete heartblock as a complication of Varicella. Int _7 Cardiol 1987;14:362-5.
10 Waagner D, Murphy T. Varicella myocarditis. PediatricInfections Diseases 1990;9:360-3.
11 Al-Nakib W, Al-Kandari S, El-Khalik D, El-Shirbiny A. Arandomised controlled study of intravenous acyclovir(Zovirax) against placebo in adults with chicken pox._l Infect Dis 1983;6(suppl 1):49-56.
12 Prober C, Kirk L, Keeney R. Acyclovir therapy of chick-enpox in immunosuppressed children: a collaborativestudy. J Paediatr 1982;101:622-5.
13 Nyerges G, Meszner Z, Gyarmati E, Kerpel-Fronius S.Acyclovir prevents dissemination of Varicella in im-munocompromised children. .7 Infect Dis 1988;157:309-13.
14 Balfour H, Kelly J, Suarez C, et al. Acyclovir treatment ofVaricella in otherwise healthy children. _7 Paediatr 1990;116:633-9.
15 Hobbs R, Pelegrin D, Ratliff N, et al. Lymphocyticmyocarditis and dilated cardiomyopathy: treatment withimmunosuppressive agents. Cleve Clin _7 Med 1989;56:628-35.
16 Latham R, Mulrow J, Virmani R, Robinowitz M, MoodyJ. Recently diagnosed idiopathic dilated cardiomyopa-thy: incidence of myocarditis and efficacy of prednisonetherapy. Am Heart.7 1989;117:876-82.
17 Salvi A, DiLenarda A, Dreas L, Silvestri F, Camerini F.Immunosuppressive treatment in myocarditis. Int .1Cardiol 1989;22:329-38.
95
on Novem
ber 18, 2021 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.70.1.93 on 1 July 1993. D
ownloaded from