
BPCO e Tubercolosi: un binomio pericoloso · Marco Contoli, MD, PhD [email protected] Sezione di...
28
BPCO e Tubercolosi: un binomio pericoloso Marco Contoli, MD, PhD [email protected] Sezione di Medicina Interna e Cardio-Respiratoria
-
Upload
truongdung -
Category
Documents
-
view
214 -
download
0
Transcript of BPCO e Tubercolosi: un binomio pericoloso · Marco Contoli, MD, PhD [email protected] Sezione di...

BPCO e Tubercolosi: un binomio pericoloso
Marco Contoli, MD, [email protected]
Sezione di Medicina Interna e Cardio-Respiratoria

BPCO e Tubercolosi: un binomio pericoloso
•BPCO
• Infezioni in BPCO
•TB (e micobatteri) & BPCO• RCTs• Studi coorte
•Meccanismi
COPD Definition
© 2017 Global Initiative for Chronic Obstructive Lung Disease
►Chronic Obstructive Pulmonary Disease (COPD) is a common, preventable and treatable disease that is characterized by persistent respiratory symptoms and airflow limitation that is due to airway and/or alveolar abnormalities usually caused by significant exposure to noxious particles or gases.

0
20
40
60
80
Remission
Pati
ents
(%)
Role of infections in chronic bronchitis
(Gump et al. Am Rev Resp Dis 1976)
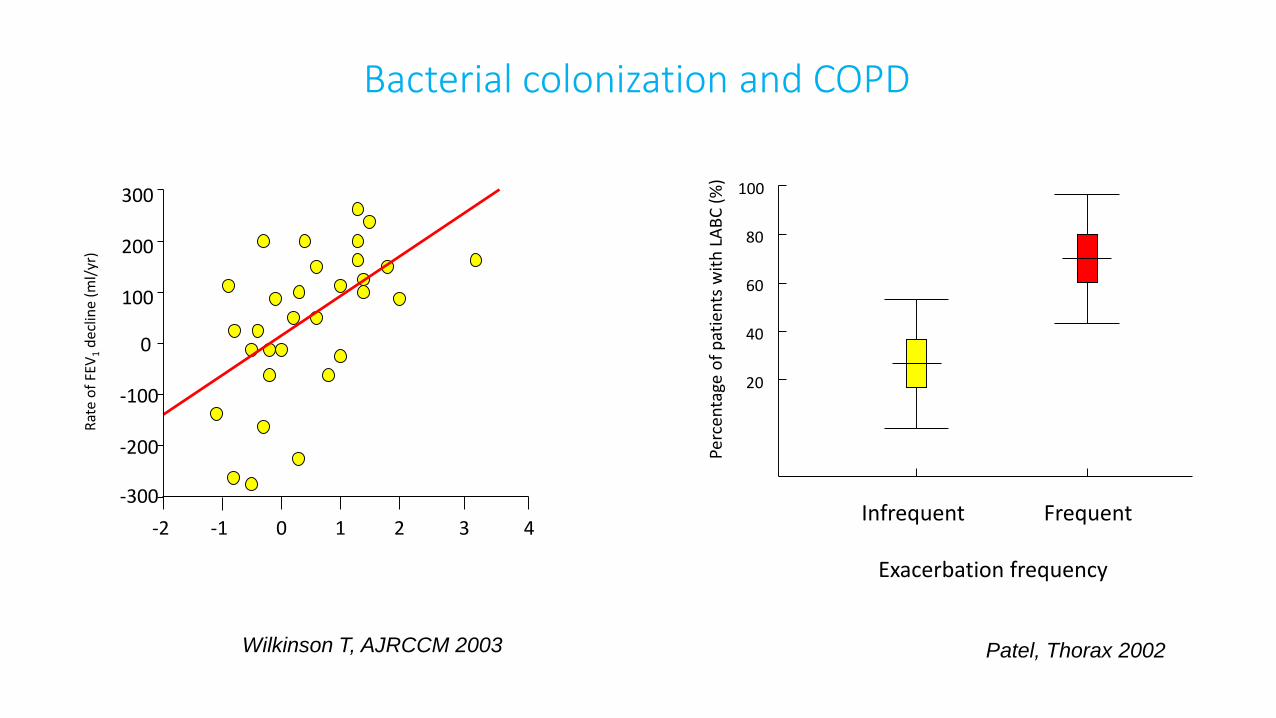
Bacterial colonization and COPD
-1 0 1 2 3 4
-300
-2
-200
-100
0
100
200
300
Rat
e o
f FE
V1
dec
line
(ml/
yr)
Wilkinson T, AJRCCM 2003
20
40
60
80
100
Perc
enta
geo
f p
atie
nts
wit
h L
AB
C (
%)
Exacerbation frequency
Infrequent Frequent
Patel, Thorax 2002
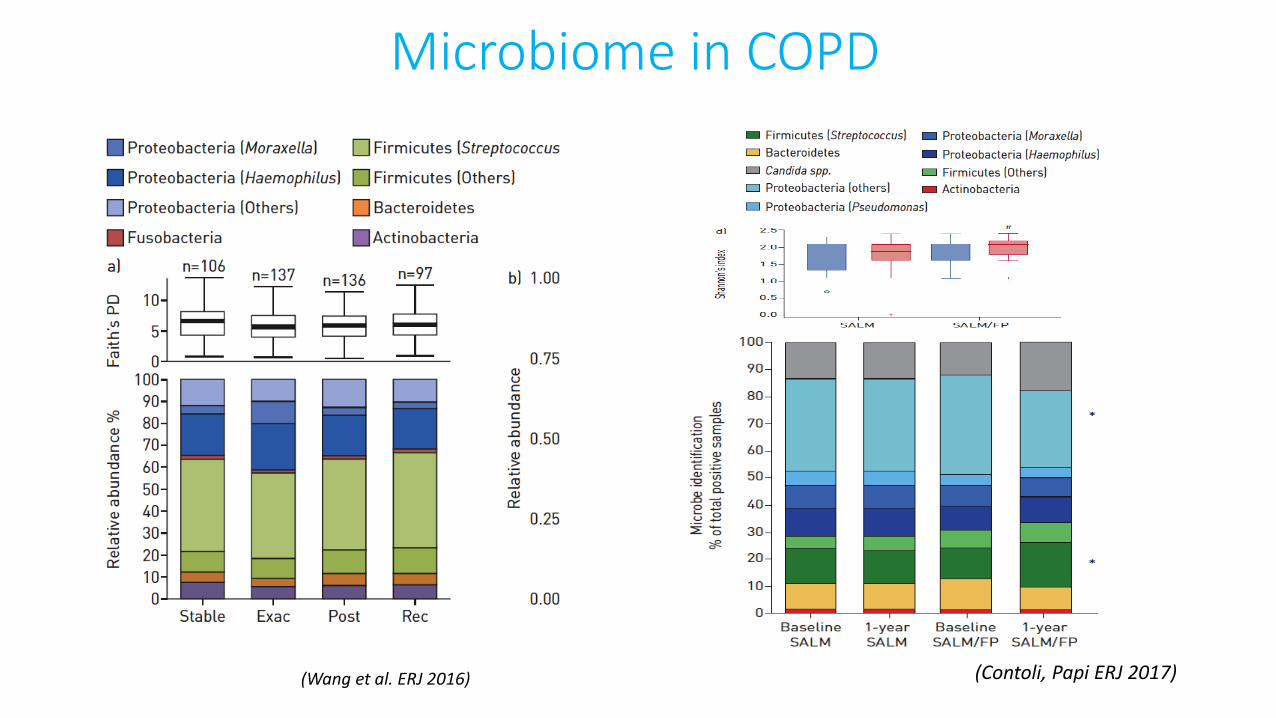
Microbiome in COPD
(Contoli, Papi ERJ 2017)(Wang et al. ERJ 2016)

0
20
40
60
80Exacerbation
Remission
Pa
tie
nts
(%
)
Role of bacterial infections in exacerbations
(Gump et al. Am Rev Resp Dis 1976)
Stable State Purulent
Exacerbation
0.0
1.0×1008
2.0×1008
3.0×1008
4.0×1008
Ba
cte
ria
l lo
ad
(cfu
/mL
)
(Stockley R et al. Chest 2000)

New Strains of Bacteria and Exacerbations of
COPD
0
10
20
30
40
50
60
Any Strain HI MC SP PA
New strain
No new strain
***
***
***
*
no
. o
f e
xa
ce
rba
tio
ns/
tota
ln
o. o
f vis
its
(%)
Sethi NEJM 2004

Detection of virus (rhinovirus) in induced sputumat exacerbation of COPD
(Seemungal et al. ERJ 2000)
0
5
10
15
20
25
%
0
10
20
30
40
50
%
(Rohde G et al. Thorax 2002)

0
1
2
3
4
5
6
-6 -4 -2 0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 38 40 420
1
2
3
4
5
6
COPD
HS
**
* *p<0.05
Study days
Dail
y L
RT
sym
pto
m s
core
s
BASE D5 D9 D12 D15 3/52 4/52 5/52 6/5285
90
95
100
105
110
115HSCOPD
Time
Po
st-
BD
PE
F (
% b
aselin
e)
(AJRCCM 2011)

(AJRCCM 2012)
D0 D5 D9 D12 D15 3/52 4/52 5/52 6/520
1
2
3
4
5
6
VIRUS
BACTERIA
0
1
2
3
4
5
6
Sp
utu
m v
iru
s l
oad
(lo
g1
0R
NA
co
pie
s/m
l)
Bacte
rial lo
ad
(log
10 C
FU
)
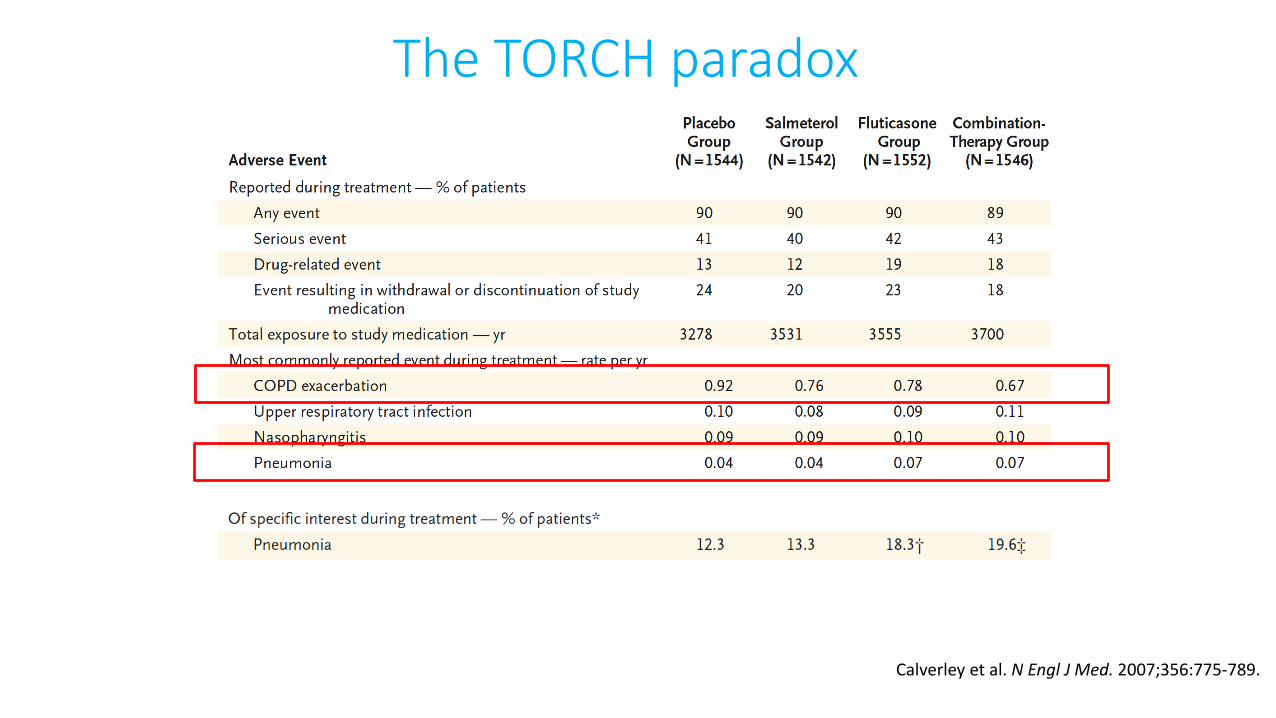
Calverley et al. N Engl J Med. 2007;356:775-789.
The TORCH paradox
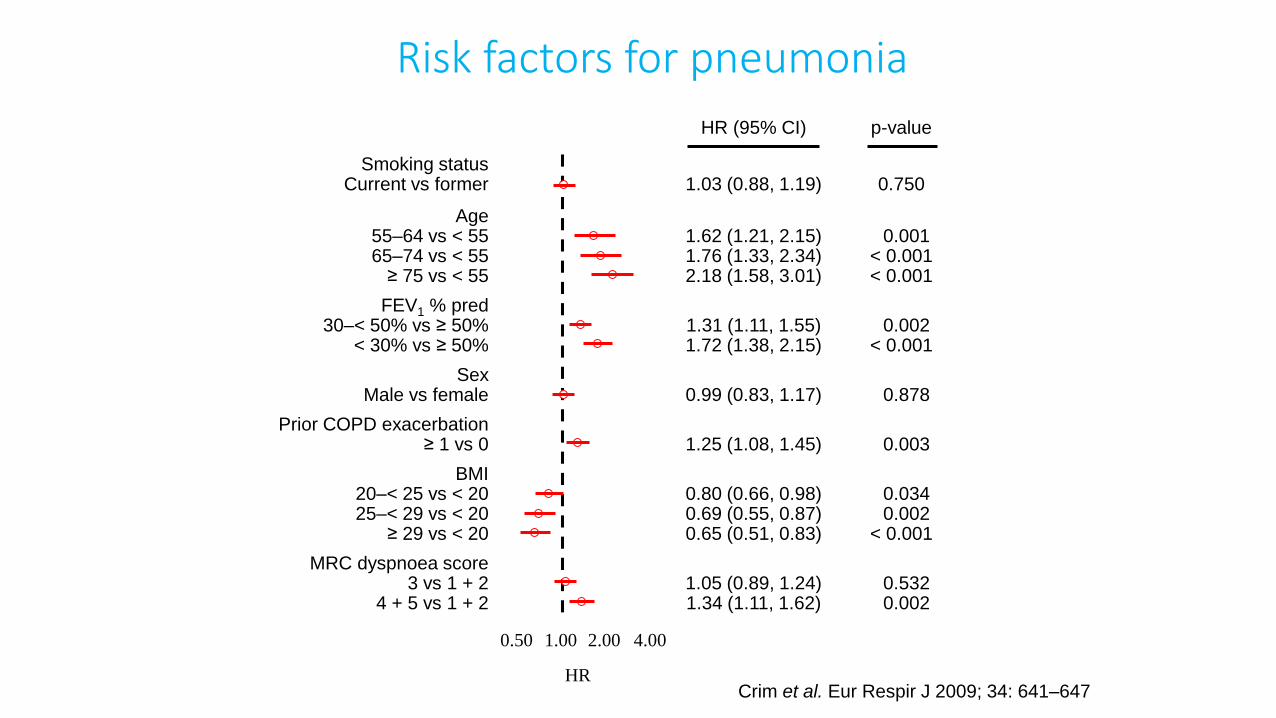
HR (95% CI) p-value
Smoking statusCurrent vs former 1.03 (0.88, 1.19) 0.750
Age55–64 vs < 5565–74 vs < 55
≥ 75 vs < 55
1.62 (1.21, 2.15)1.76 (1.33, 2.34)2.18 (1.58, 3.01)
0.001< 0.001< 0.001
FEV1 % pred30–< 50% vs ≥ 50%
< 30% vs ≥ 50%1.31 (1.11, 1.55)1.72 (1.38, 2.15)
0.002< 0.001
SexMale vs female 0.99 (0.83, 1.17) 0.878
Prior COPD exacerbation≥ 1 vs 0 1.25 (1.08, 1.45) 0.003
BMI20–< 25 vs < 2025–< 29 vs < 20
≥ 29 vs < 20
0.80 (0.66, 0.98)0.69 (0.55, 0.87)0.65 (0.51, 0.83)
0.0340.002
< 0.001
MRC dyspnoea score3 vs 1 + 2
4 + 5 vs 1 + 21.05 (0.89, 1.24)1.34 (1.11, 1.62)
0.5320.002
Risk factors for pneumonia
0.50 1.00 2.00 4.00
HRCrim et al. Eur Respir J 2009; 34: 641–647

Long-term effects of inhaled corticosteroids on sputumbacterial and viral loads in COPD
(Contoli, Papi et al. ERJ 2017)
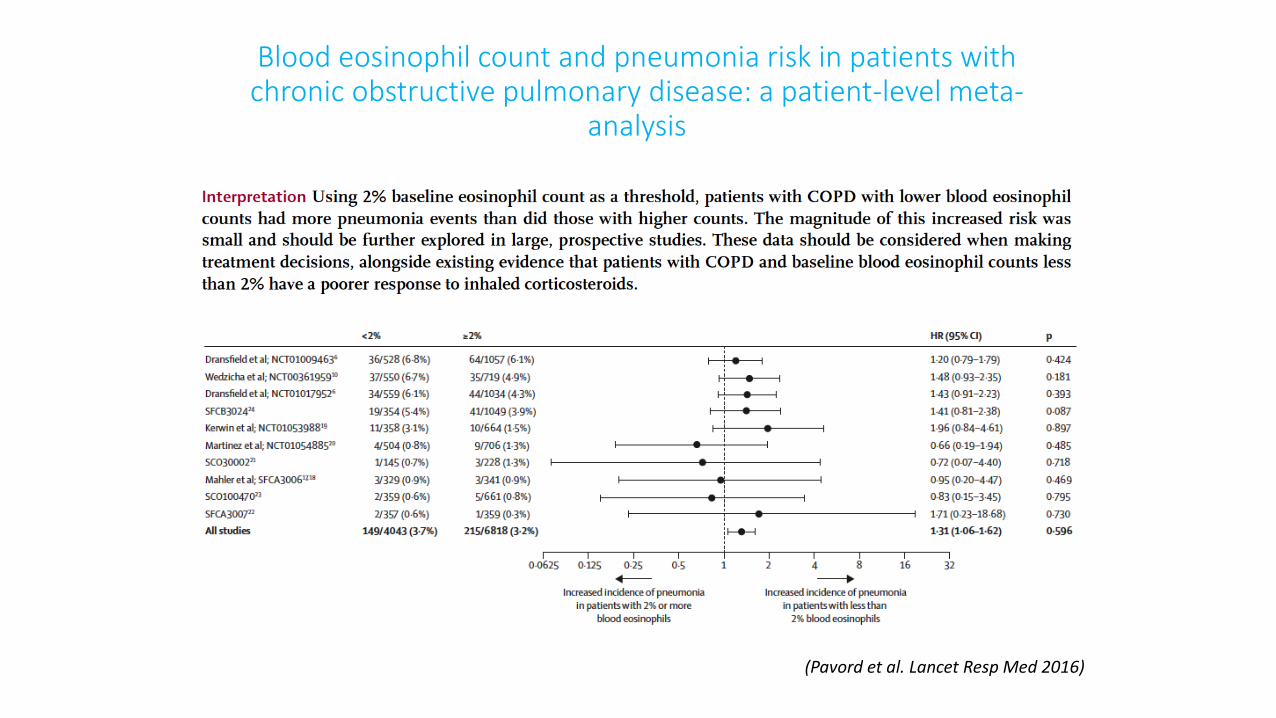
Blood eosinophil count and pneumonia risk in patients with chronic obstructive pulmonary disease: a patient-level meta-
analysis
(Pavord et al. Lancet Resp Med 2016)
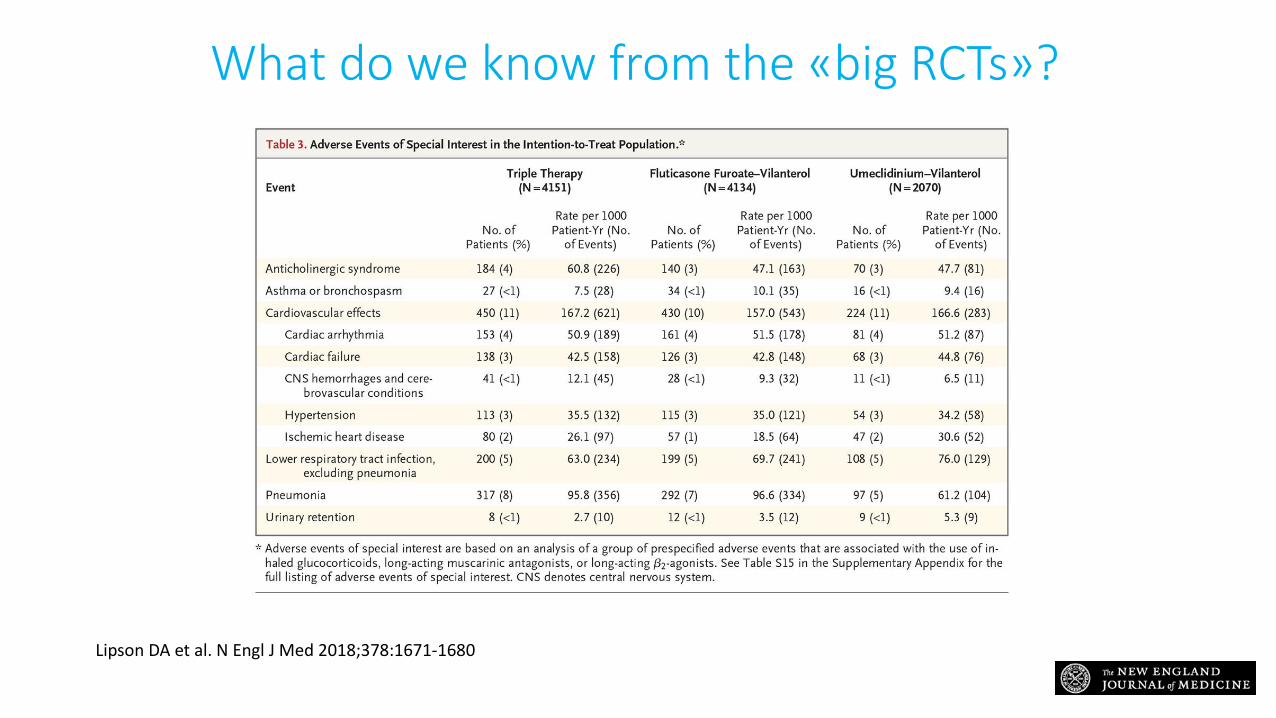
What do we know from the «big RCTs»?
Lipson DA et al. N Engl J Med 2018;378:1671-1680

(Songshi et al. J Thorac Dis 2014)
Five studies involving 4,851 cases and 28,477 controls
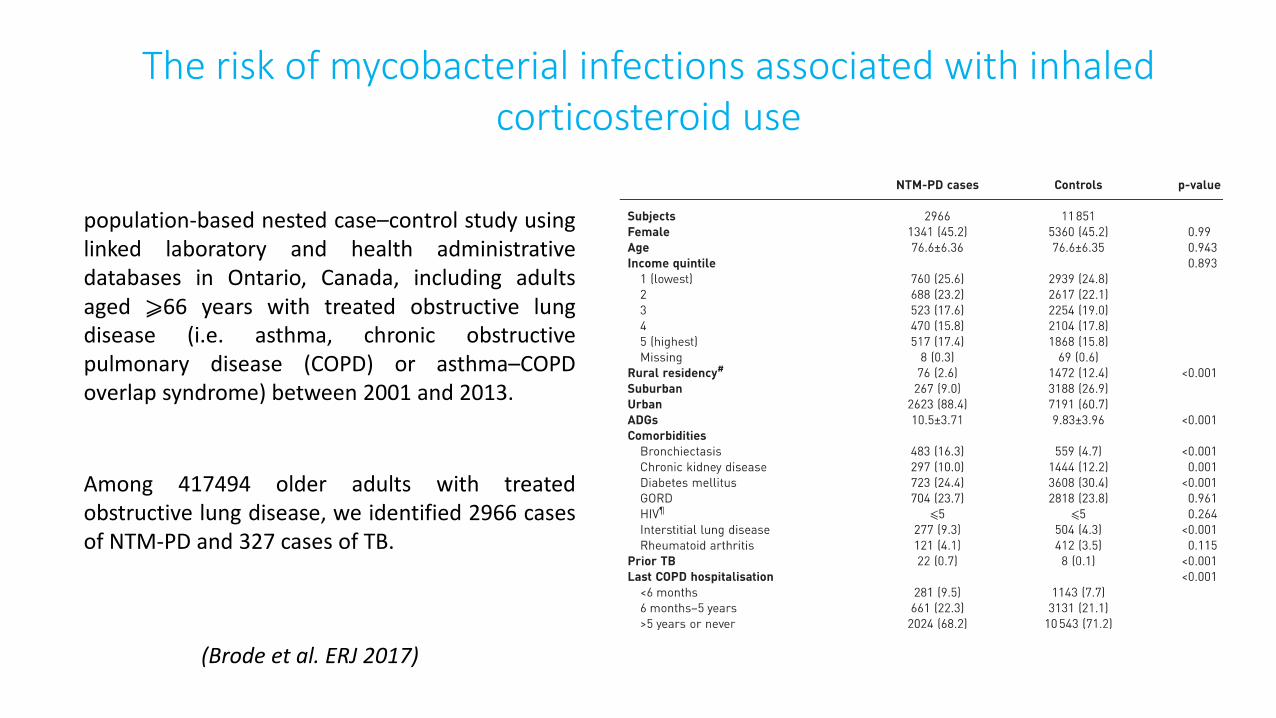
The risk of mycobacterial infections associated with inhaledcorticosteroid use
population-based nested case–control study usinglinked laboratory and health administrativedatabases in Ontario, Canada, including adultsaged ⩾66 years with treated obstructive lungdisease (i.e. asthma, chronic obstructivepulmonary disease (COPD) or asthma–COPDoverlap syndrome) between 2001 and 2013.
Among 417494 older adults with treatedobstructive lung disease, we identified 2966 casesof NTM-PD and 327 cases of TB.
(Brode et al. ERJ 2017)
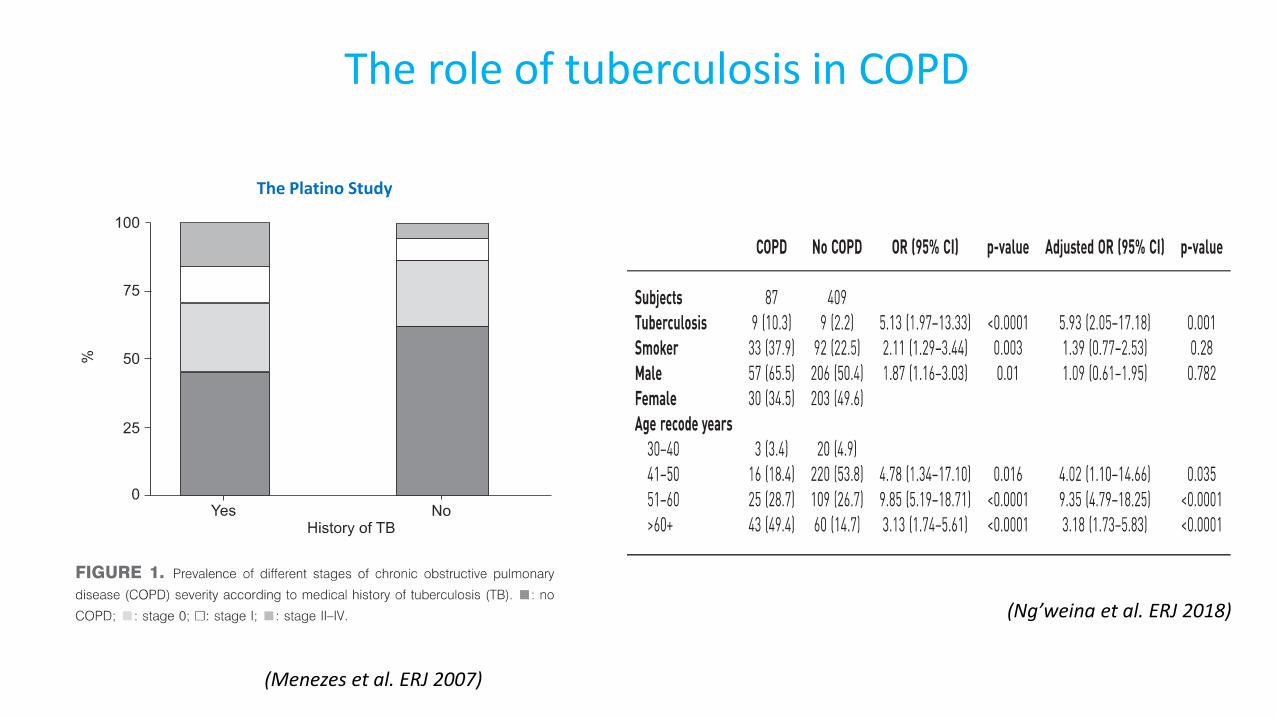
(Ng’weina et al. ERJ 2018)
The role of tuberculosis in COPD
The Platino Study
(Menezes et al. ERJ 2007)
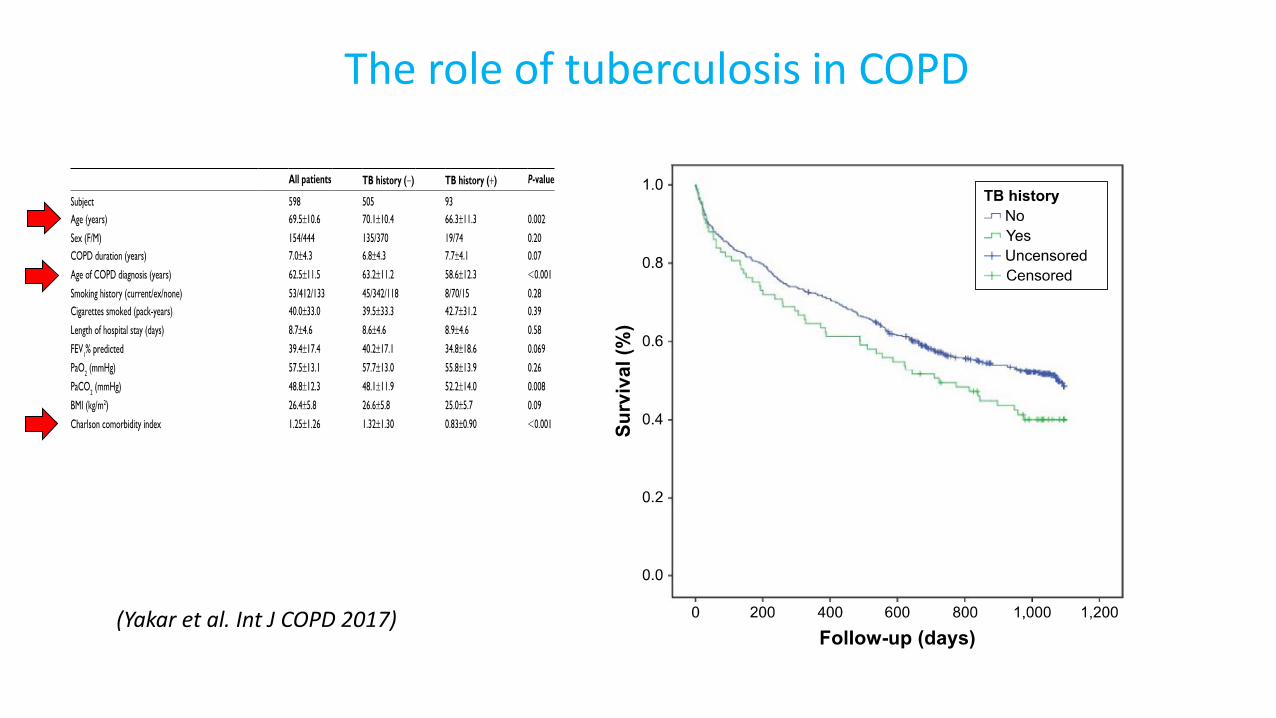
The role of tuberculosis in COPD
(Yakar et al. Int J COPD 2017)
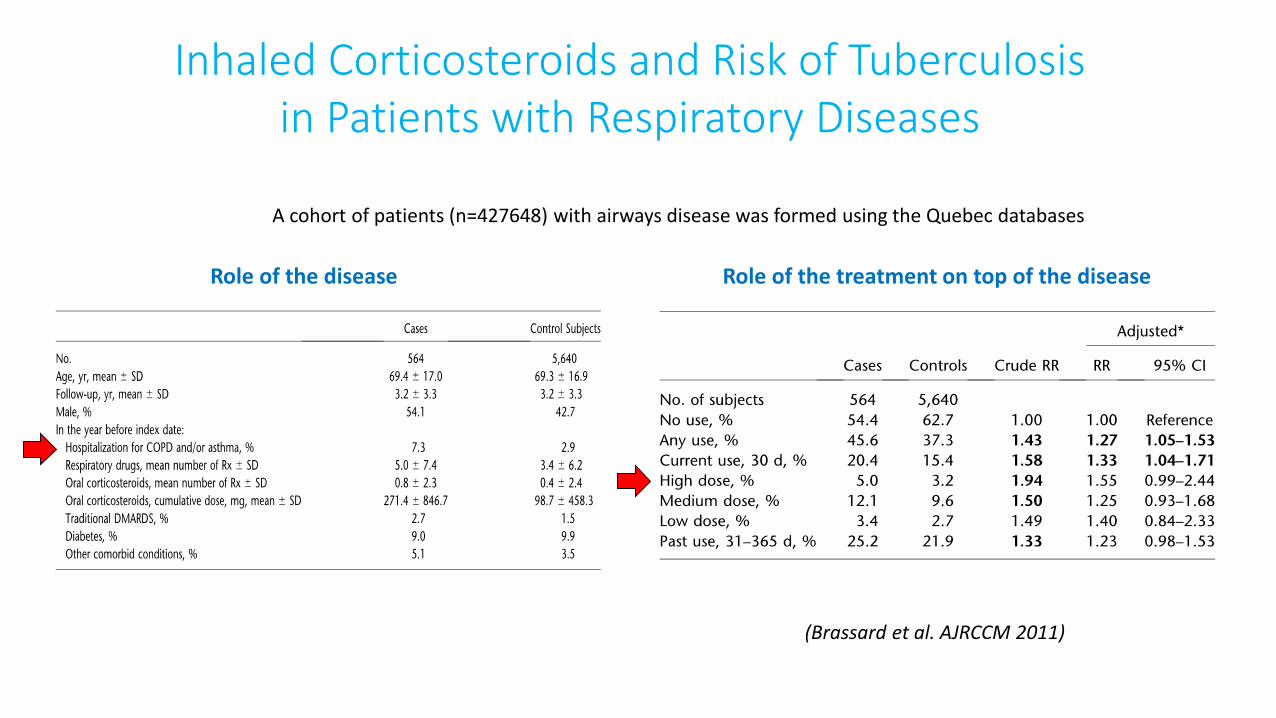
Inhaled Corticosteroids and Risk of Tuberculosisin Patients with Respiratory Diseases
(Brassard et al. AJRCCM 2011)
Role of the disease Role of the treatment on top of the disease
A cohort of patients (n=427648) with airways disease was formed using the Quebec databases

The eligible cohort consisted of 853439 new adult users in South Corea of inhaled respiratory medicationsbetween 1 January 2007 and 31 December 2010.
Use of inhaled corticosteroids and the risk of tuberculosis
(Lee et al. Thorax 2013)
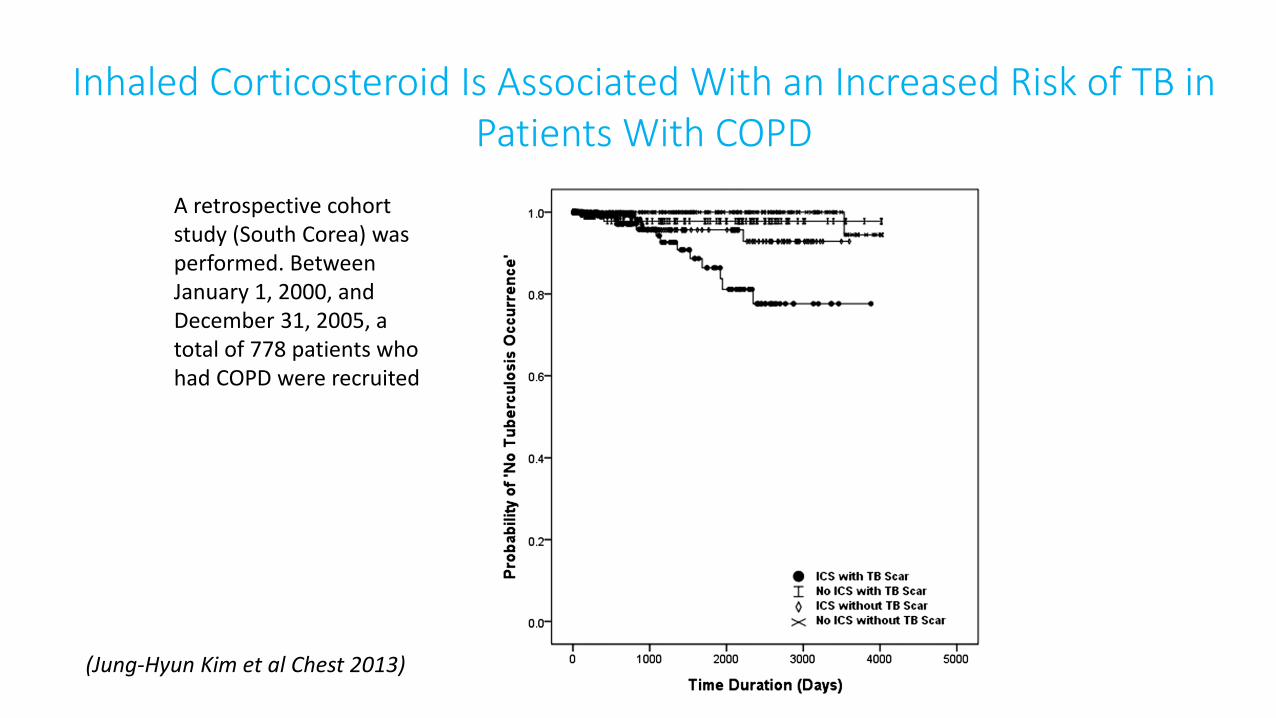
Inhaled Corticosteroid Is Associated With an Increased Risk of TB in Patients With COPD
A retrospective cohortstudy (South Corea) wasperformed. BetweenJanuary 1, 2000, and December 31, 2005, a total of 778 patients whohad COPD were recruited
(Jung-Hyun Kim et al Chest 2013)
BPCO e Tubercolosi: un binomio pericoloso
• BPCO
• Infezioni in BPCO
• TB (e micobatteri) & BPCO–RCTs
–Studi coorte
•Meccanismi

Effects of ICS on pulmonary host defence
1) inhibition of macrophage antimicrobial activity (Stolberg et al. J
Immunol 2015)
2) inhibition of the macrophage release of cytokines such asTNF and IP-10 (Patterson et al Respir Res 2012)
3) downregulation of the expression of MHC class II molecules in macrophages (Van de Garde et al. J Immunol 2012)
4) reduction of adaptive immune responses (Lee et al. FASEB 2012)
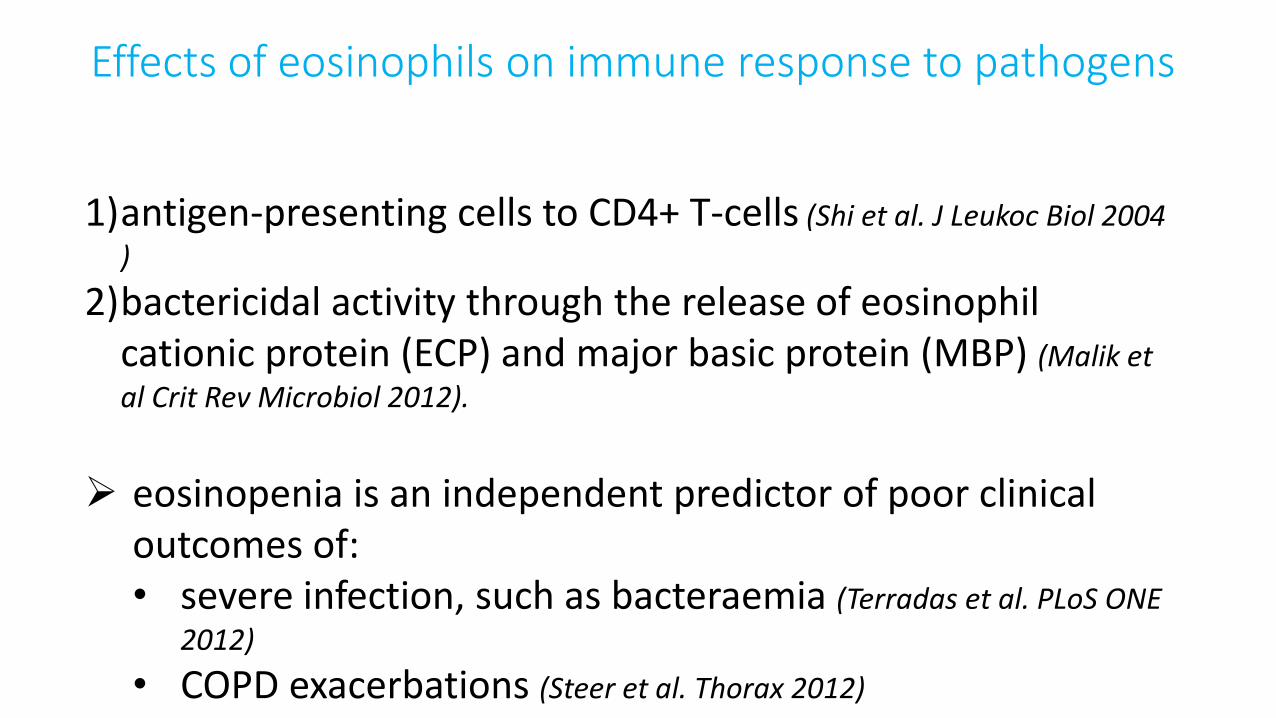
1)antigen-presenting cells to CD4+ T-cells (Shi et al. J Leukoc Biol 2004
)
2)bactericidal activity through the release of eosinophilcationic protein (ECP) and major basic protein (MBP) (Malik et
al Crit Rev Microbiol 2012).
eosinopenia is an independent predictor of poor clinicaloutcomes of:• severe infection, such as bacteraemia (Terradas et al. PLoS ONE
2012)
• COPD exacerbations (Steer et al. Thorax 2012)
Effects of eosinophils on immune response to pathogens
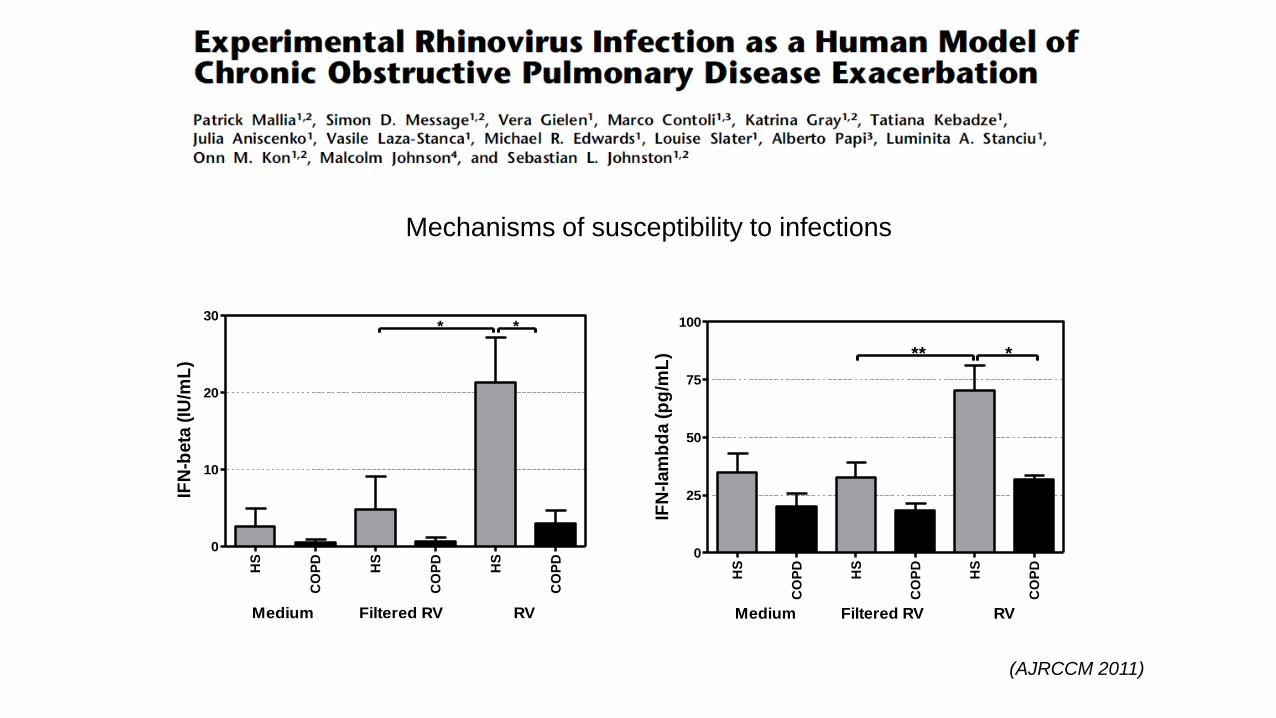
HS
CO
PD
HS
CO
PD
HS
CO
PD
0
10
20
30* *
Medium Filtered RV RV
IFN
-beta
(IU
/mL
)
HS
CO
PD
HS
CO
PD
HS
CO
PD
0
25
50
75
100
** *
Medium Filtered RV RV
IFN
-lam
bd
a (
pg
/mL
)
Mechanisms of susceptibility to infections
(AJRCCM 2011)

BPCO e Tubercolosi: un binomio pericoloso
Marco Contoli, MD, [email protected]
Sezione di Medicina Interna e Cardio-Respiratoria
Conclusioni
COPD & TB: YES
- Deranged innate immune response in COPD
PARTICULARLY IF:
• Elderly/comorbid patients• Previous history of TB• Low eos count• On high dose of ICS (Fluti)


















