Both Amiloride and Nebivolol Have a More Favourable Effect on Glucose Tolerance Than...
26
Both Amiloride and Nebivolol Have a More Favourable Effect on Glucose Tolerance Than Hydrochlorothiazide in the Treatment of Essential Hypertension Stears AJ, Woods SH, Watts MM, Graggaber J, Burton TJ, Brown MJ Department of Clinical Pharmacology, Addenbrookes’ Hospital, Cambridge
-
Upload
geraldine-glenn -
Category
Documents
-
view
216 -
download
1
Transcript of Both Amiloride and Nebivolol Have a More Favourable Effect on Glucose Tolerance Than...
Both Amiloride and Nebivolol Have a More Favourable Effect on Glucose
Tolerance Than Hydrochlorothiazide in the Treatment of Essential Hypertension
Stears AJ, Woods SH, Watts MM, Graggaber J, Burton TJ, Brown MJ
Department of Clinical Pharmacology, Addenbrookes’ Hospital, Cambridge

Disclosures
• This study is an investigator-led study supported by an unrestricted grant from Menarini

Evidence to support thiazide use
• Thiazide and thiazide-like diuretics have been used for treatment of essential hypertension since the 1950’s
• Evidence for their inclusion in clinical guidelines is based on 4 decades of cardiovascular outcome trials
• ALLHAT1,2 - 42,418 subjects comparing chlorthalidone with lisinopril, amlodipine and doxazosin
• Chlorthalidone was as beneficial as the comparator drugs in lowering blood pressure and preventing cardiovascular and renal outcomes
• Chlorthalidone was superior in preventing heart failure1ALLHAT Investigators. Major cardiovascular events in hypertensive patients randomized to doxazosin vs chlorthalidone: The Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT). JAMA. 2000;283;1967–1975.
2ALLHAT Investigators. Major outcomes in high-risk hypertensive patients randomized to angiotensin-converting enzyme inhibitor or calcium channel blocker vs diuretic: the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT). JAMA. 2002;288:2981–2997.

Thiazides and new onset diabetes• ALLHAT1,2
9.3% chlorthalidone 7.2% amlodipine 5.6% lisinopril
• ASCOT3 11.4% atenolol ± thiazide 8.0% amlodipine ± perindopril
• INSIGHT4 5.6% co-amilozide 4.3% nifedipine
3Bjorn Dahlof et al; Prevention of cardiovascular events with an antihypertensive regimen of amlodipine adding perindopril as required versus atenolol adding bendroflumethiazide as required, in the Anglo-Scandinavian Cardiac Outcomes Trial-Blood Pressure Lowering Arm (ASCOT-BPLA), Lancet 2005; 366: 895–9064Morris J Brown et al; Morbidity and mortality in patients randomised to double-blind treatment with a long-acting calcium-channel blocker or diuretic in the International Nifedipine GITS study: Intervention as a Goal in Hypertension Treatment (INSIGHT), Lancet • Vol 356 • July 29, 2000
New onset diabetes in ASCOT
Mechanism: thiazides and diabetes
• Mechanism underlying the association of thiazides with diabetes is not understood
• Not known if the principal defect is impaired insulin secretion or increased insulin resistance5
• Changes in plasma potassium concentration may affect glucose tolerance6
5Barry L. Carter et al; Thiazide-Induced Dysglycemia , Call for Research From a Working Group From the National Heart,
Lung, and Blood Institute, Hypertension 2008;52;30-366Zillich AJ; Thiazide diuretics, potassium, and the development of diabetes: a quantitative review. Hypertension. 2006;48:219 –224.

Potassium sparing diuretics
• Few studies of glucose metabolism7
• BP lowering efficacy of amiloride similar to thiazide in SALT8,9
• Cardiovascular outcome studies not available
7Boquist L. Effects of amiloride on insulin release, serum glucose and insulin, and glucose tolerance of mice. Med Biol. 1980 Apr; 58(2):109-11.8Susan J. Hood and Morris J. Brown ;The Spironolactone, Amiloride, Losartan, and Thiazide (SALT) Double-Blind Crossover Trial in Patients With Low-Renin Hypertension and Elevated Aldosterone-Renin Ratio,Circulation 2007;116;268-2759JP Thomas: Comparison of thiazides and amiloride in treatment of moderate hypertension, BMJ 286, 25 June 1983
.

β1-selective beta blockade
• Studies investigating metabolic effects of newer β1-selective selective β-blockers have found them to be neutral or beneficial10
• Outcome studies showing metabolic effects of atenolol used relatively high mean doses
• Our previous study showed no change in 2-hour glucose from baseline during an oral glucose tolerance test (OGTT) after 4 weeks treatment with atenolol11
10Basile JN; One size does not fit all: the role of vasodilating beta-blockers in controlling hypertension as a means of reducing cardiovascular and stroke risk. Am J Med.123(7 Suppl 1):S9-15.
11Stears AJ et al; Early Metabolic Changes with Thiazide or Beta Blocker Therapy for Essential Hypertension;, Poster Presentation BHS 2008

Study objectives
• Primary objective – What are the changes from baseline in an
OGTT after 4 weeks treatment with hydrocholorothiazide (HCTZ) compared with amiloride and nebivolol monotherapy and combination therapy with HCTZ/nebivolol?
• Secondary objective– What is the effect of each drug/drug
combination on blood pressure?

Inclusion/exclusion criteria
Inclusion criteria
• 18-75 years• BP untreated
>140/90 and <170/110mmHg
• BP treated with drugs other than beta blockers or diuretics and BP>140/85mmHg
Exclusion criteria
• Previous intolerance of study drugs
• Diabetes• Gout, asthma• Heart failure, liver failure,
renal failure, terminal illness
• Women of child bearing potential
• Inability to give informed consent

Study design
HCTZ - hydrochlorothiazideNeb - nebivololAmil - amiloride
Randomised, double blind, placebo controlled,cross-over study
BP, 75g OGTT, and electrolytes measured at 0, 2 and 4 weeks for each phase of study
Phase 1 Phase 2 Phase 3 Phase 4 Phase 5
Placebo washout
Placebo washout
Placebo washout
Placebo washout
0 2 4 8 10 12 16 18 20 24 26 28 32 34 36Weeks
Visit 1 Visit 2 Visit 3 Visit 4 Visit 5 Visit 6 Visit 7 Visit 8 Visit 9 Visit 10 Visit 11 Visit 12 Visit 13 Visit 14 Visit 15
Amil 10mg
Amil 20mg
Placebo PlaceboHCTZ 25mg
HCTZ 50mg
Neb 5mg
Neb 10mg
HCTZ 25mg+
Neb 5mg
HCTZ 50mg +
Neb 10mg

Baseline characteristics
Results are mean (sd), except for age which is median (range)
Male/Female 17/20 Age (years) 65 (41-75) BMI (kg/m2) 28.6 (4.2) Baseline SBP (mmHg) 144.3 (13.7) Baseline DBP (mmHg) 85.4 (9.9)

OGTT at baseline and 4 weeks Amiloride vs HCTZ
Amiloride
0 30 60 120
Time (mins)
4
5
6
7
8
9
10
11P
lasm
a gl
ucos
e (m
mol
/L)
HCTZ
0 30 60 120
Time (mins)
Baseline 4 weeks
p=0.006
Mean 2-hour glucose 6.70 mmol/l on amiloride vs 7.49 mmol/l on HCTZ
p <0.0001

OGTT at baseline and 4 weeks
Time (mins)
Baseline
0 30 60 1204
5
6
7
8
9
10
11
Pla
sma
gluc
ose
(mm
ol/L
)
Time (mins)
4 weeks
0 30 60 120
Amiloride Nebivolol Combination HCTZ Placebo
Mean 2-hour glucose 6.77 mmol/l on nebivolol vs 7.49 mmol/l on HCTZ
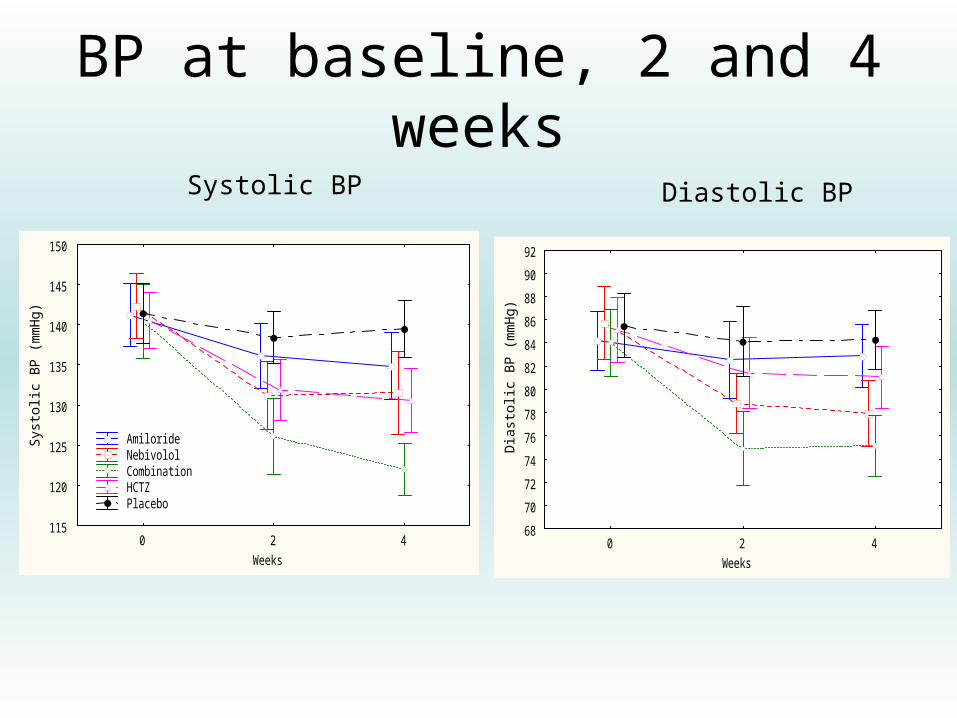
BP at baseline, 2 and 4 weeks
0 2 4
Weeks
115
120
125
130
135
140
145
150
Sys
tolic
BP
(m
mH
g)
Amiloride Nebivolol Combination HCTZ Placebo
0 2 4
Weeks
68
70
72
74
76
78
80
82
84
86
88
90
92
Dia
sto
lic B
P (
mm
Hg
)
Systolic BP Diastolic BP
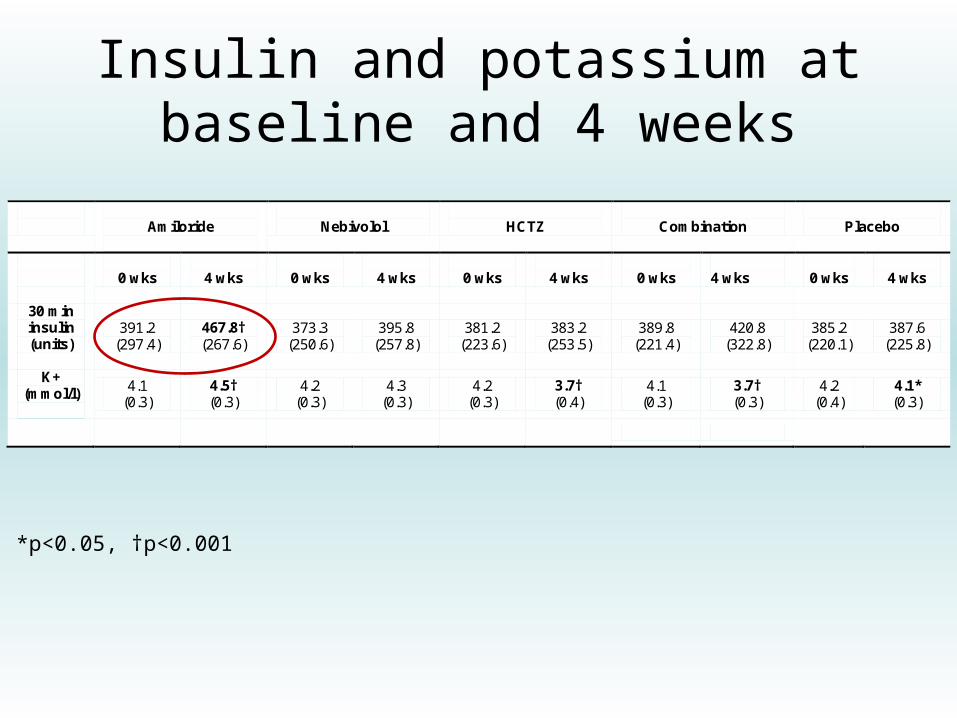
Insulin and potassium at baseline and 4 weeks
Amiloride
Nebivolol
HCTZ
Combination
Placebo
0 wks
4 wks
0 wks
4 wks
0 wks
4 wks
0 wks
4 wks
0 wks
4 wks
30 min insulin (units)
391.2 (297.4)
467.8† (267.6)
373.3 (250.6)
395.8 (257.8)
381.2 (223.6)
383.2 (253.5)
389.8 (221.4)
420.8 (322.8)
385.2 (220.1)
387.6 (225.8)
K+ (mmol/l)
4.1 (0.3)
4.5† (0.3)
4.2 (0.3)
4.3 (0.3)
4.2 (0.3)
3.7† (0.4)
4.1 (0.3)
3.7† (0.3)
4.2 (0.4)
4.1* (0.3)
*p<0.05, †p<0.001

Negative correlation between change in 2-hour glucose and change in potassium between
baseline and 4 weeks
r = -0.28, p<0.0001

Results summary
• Glucose tolerance significantly impaired with HCTZ compared with amiloride or nebivolol
• Similar BP lowering with HCTZ, nebivolol and amiloride
• Combination therapy with HCTZ/nebivolol has better BP lowering efficacy
• Combination therapy has similar metabolic effects to HCTZ monotherapy
• Negative correlation between change in 2-hour glucose and change in plasma potassium

Conclusions
• Should amiloride or an amiloride/thiazide combination replace thiazides as the diuretic of choice?– BHF funded ‘Pathway 3’ study - Does a
combination of HCTZ/amiloride have a metabolic advantage over HCTZ alone?
• β1-selective beta blockers appear to lack the deleterious effect on glucose tolerance previously reported for atenolol

Acknowledgments
• Study volunteers• Prof MJ Brown• Sarah Woods• Michaela Watts• Dr Johann Graggaber• Dr Swe Myint• Dr Fraz Mir• Dr Tim Burton• Staff on Clinical Investigation Ward

Questions?

Result (mean±sd)
Amiloride
Nebivolol
HCTZ
Combination
Placebo
0 wks
4 wks
0 wks
4 wks
0 wks
4 wks
0 wks
4 wks
0 wks
4 wks
Fasting glucose (mmol/l)
5.19 (0.47)
5.23 (0.55)
5.23 (0.52)
5.24 (0.59)
5.16 (0.52)
5.45† (0.55)
5.25 (0.63)
5.47* (0.64)
5.30 (0.71)
5.19 (0.52)
2-hour glucose (mmol/l)
7.07 (2.17)
6.70 (1.88)
7.21 (2.09)
6.79 (2.21)
7.00 (2.36)
7.55* (2.24)
7.39 (2.44)
7.65 (2.13)
7.38 (2.38)
6.65* (2.08)
Fasting insulin (units)
66.4 (46.6)
65.5 (31.5)
61.5 (38.1)
66.9 (44.6)
67.1 (38.3)
71.8 (39.7)
64.2 (47.2)
75.6* (48.4)
68.0 (43.0)
61.1 (34.9)
30 min insulin (units)
391.2 (297.4)
467.8† (267.6)
373.3 (250.6)
395.8 (257.8)
381.2 (223.6)
383.2 (253.5)
389.8 (221.4)
420.8 (322.8)
385.2 (220.1)
387.6 (225.8)
K+ (mmol/l)
4.1 (0.3)
4.5† (0.3)
4.2 (0.3)
4.3 (0.3)
4.2 (0.3)
3.7† (0.4)
4.1 (0.3)
3.7† (0.3)
4.2 (0.4)
4.1* (0.3)
SBP (mmHg)
139.1 (12.9)
132.3† (15.0)
142.3 (14.7)
131.2† (16.2)
140.6 (12.0)
129.8† (13.7)
140.6 (16.0)
121.6† (12.2)
141.0 (11.4)
137.0* (11.8)
DBP (mmHg)
82.8 (8.4)
81.2 (7.8)
84.4 (11.5)
77.4† (10.4)
84.1 (8.7)
80.7* (9.8)
83.8 (10.0)
74.7† (9.8)
85.6 (8.1)
83.1* (8.6)

Management of hypertension in adults in primary care NICE guideline 34, June 2006

Clinical management of hypertension in adults NICE clinical guideline 127, August 2011

Oral glucose tolerance test
Fasting glucose (mmol/l)
2 hour glucose(mmol/l)
Normal < 6.0 < 7.8
Impaired 6.1 - 7.0 7.8 - 11.1
Diabetes > 7.0 > 11.1

Diuretics for hypertension
• Diuretics inhibit sodium reabsorption from different parts of the nephron
• Thiazides - early distal tubule, inhibit sodium-chloride co-transporter (NCT)
• Amiloride - late distal tubule, inhibits epithelial sodium channel (ENaC)

Study Design
• Double-blind, placebo controlled, cross-over study
• Inclusion criteria: essential hypertension, BP >140/85mmHg, <170/110mmHg, no diabetes
• 5 active treatment phases, each phase separated by a 4-week placebo washout
• Patients supplied with home blood pressure monitor for duration of study