Bosnia: The War Against Public Health · To the outside world, the war in Bosnia has been...
17
T o the outside world, the war in Bosnia has been confusing, marked by appar- ent random violence and relentless tragedy. War evokes images of armies and battles, yet the pictures and stories from Bosnia are more often about civilian casual- ties and personal suffering, presented as the tragic by-products of conflict. Behind these confusing images, and beyond the complex question of which factions, ethnic groups, or nationalities have been responsible, there is a hidden logic to this conflict that emerges from an analysis of its effects on the health of the civilian population. This is a war on populations, not armies. The basic conditions that people need to pro- tect their health -- their physical, mental, and social well being -- are being systematically and ruthlessly undermined in Bosnia. The 130 Medicine & Global Survival 1994; Vol. 1, No. 3 Bosnia: The War Against Public Health Bosnia: The War Against Public Health Jonathan Mann, MD, MPH; Ernest Drucker, PhD; Daniel Tarantola, MD; and Mary Pat McCabe, BS At the time of publication JM was Francois- Xavier Bagnoud Professor of Health and Human Rights, Director of the Francois-Xavier Bagnoud Center for Health and Human Rights, Professor of Epidemiology and International Health at the Harvard School of Public Health; ED was Professor of Epidemiology and Social Medicine at the Albert Einstein School of Medicine; DT was Director of the International AIDS Program at the Francois-Xavier Bagnoud Center for Health and Human Rights and Lecturer in Population and International Health at the Harvard School of Public Health; MPMcC was Administrator of the Francois-Xavier Bagnoud Center for Health and Human Rights and a stu- dent in the Department of Population and International Health at the Harvard School of Public Health. © Copyright 1994 Medicine & Global Survival ❧ The health of the civilian population in Bosnia -- including the fundamentals for sur- vival such as food, water, and fuel, as well as the country's medical infrastructure -- has been a direct target of the current war. More than half a million people had been killed, wounded, or displaced as of September 1993, the end point of a detailed study that was conducted of each major condition for health and personal safety affected by the war. This report, culled from a wide range of sources and relying on data lim- ited in time and/or scope, has attempted to define the health vulnerabilities of the civil- ian population prior to the onset of the winter of 1993-94. Bosnia's crippled health sys- tem, the authors determined, could no longer meet even basic health needs, and a wide range of specific illnesses, including diarrhea, respiratory ailments, chronic dis- eases, premature and low birthweight babies, and vaccine preventable diseases pose an increasing threat. The fundamental means by which this war on public health has been conducted are denial of access and restriction of movement of people and goods. "Ethnic cleansing" has resulted in major population shifts that have increased vulnerability to sickness and death. External support to existing health authorities must be combined with accurate documentation and analysis of the war on health in Bosnia, to determine accountability. The experience of Bosnia should prompt a rethinking of the ways in which the impacts of collective violence on health are mea- sured and assessed. [M&GS 1994;1:130-146]
Transcript of Bosnia: The War Against Public Health · To the outside world, the war in Bosnia has been...
To the outside world, the war in Bosniahas been confusing, marked by appar-ent random violence and relentless
tragedy. War evokes images of armiesand battles, yet the pictures and stories fromBosnia are more often about civilian casual-ties and personal suffering, presented as thetragic by-products of conflict. Behind theseconfusing images, and beyond the complexquestion of which factions, ethnic groups, ornationalities have been responsible, there is ahidden logic to this conflict that emergesfrom an analysis of its effects on the health ofthe civilian population.
This is a war on populations, not armies.The basic conditions that people need to pro-tect their health -- their physical, mental, andsocial well being -- are being systematicallyand ruthlessly undermined in Bosnia. The
130 Medicine & Global Survival 1994; Vol. 1, No. 3 Bosnia: The War Against Public Health
Bosnia: The War Against Public Health
Jonathan Mann, MD, MPH; Ernest Drucker, PhD; Daniel Tarantola, MD;and Mary Pat McCabe, BS
At the time of publication JM was Francois-Xavier Bagnoud Professor of Health and HumanRights, Director of the Francois-Xavier BagnoudCenter for Health and Human Rights, Professorof Epidemiology and International Health at theHarvard School of Public Health; ED wasProfessor of Epidemiology and Social Medicineat the Albert Einstein School of Medicine; DTwas Director of the International AIDS Programat the Francois-Xavier Bagnoud Center forHealth and Human Rights and Lecturer inPopulation and International Health at theHarvard School of Public Health; MPMcC wasAdministrator of the Francois-Xavier BagnoudCenter for Health and Human Rights and a stu-dent in the Department of Population andInternational Health at the Harvard School ofPublic Health.
© Copyright 1994 Medicine & Global Survival
§
The health of the civilian population in Bosnia -- including the fundamentals for sur-vival such as food, water, and fuel, as well as the country's medical infrastructure --has been a direct target of the current war. More than half a million people had beenkilled, wounded, or displaced as of September 1993, the end point of a detailed studythat was conducted of each major condition for health and personal safety affectedby the war. This report, culled from a wide range of sources and relying on data lim-ited in time and/or scope, has attempted to define the health vulnerabilities of the civil-ian population prior to the onset of the winter of 1993-94. Bosnia's crippled health sys-tem, the authors determined, could no longer meet even basic health needs, and awide range of specific illnesses, including diarrhea, respiratory ailments, chronic dis-eases, premature and low birthweight babies, and vaccine preventable diseasespose an increasing threat. The fundamental means by which this war on public healthhas been conducted are denial of access and restriction of movement of people andgoods. "Ethnic cleansing" has resulted in major population shifts that have increasedvulnerability to sickness and death. External support to existing health authoritiesmust be combined with accurate documentation and analysis of the war on health inBosnia, to determine accountability. The experience of Bosnia should prompt arethinking of the ways in which the impacts of collective violence on health are mea-sured and assessed. [M&GS 1994;1:130-146]

war against the public health of Bosnia hasbeen powerful and ominously effective.Bosnia has been converted from a modern,industrialized country into one unable toensure even the basic elements of healthsecurity and protection for its people.
As of September 1993, an estimated150,000 people had been killed in the wars inthe former Yugoslavia; 300,000 people hadbeen wounded and an estimated 200,000 hadbeen displaced [1]. Yet beyond the extraordi-nary violence reported in the media, dis-placement and isolation of populations havebeen the central weapons of war. Lack ofaccess to food, fuel, medical supplies, andother material, compounded by the stressesof physical and emotional isolation -- onlypartially and intermittently relieved bycourageous humanitarian efforts -- are thefinal common pathway to the damage doneto public health in Bosnia.
The tragic success of aggression hasbeen abetted and intensified by three factors:increasing concentrations of vulnerable peo-ple, including the elderly, young children,the institutionalized and disabled, and peo-ple displaced by the conflict; the depletion ofmaterial and physical, mental and social"reserves" that occurs with the passage oftime; and the predictably damaging yet dif-fuse effect of winter.
This is a report on a war against thehealth of an entire population. Most, but notall, of the data presented here focus on cen-tral Bosnia. Conditions throughout Bosniavary greatly and continue to evolve. Thisreport will present data about a wide rangeof areas in Bosnia over the period leading upto the 1993-94 winter season.
To reveal and assess this dimension ofthe war in Bosnia, the report is divided intothree parts:
I. The war on public health: thecentral and major part of this report isan examination of the impact of thisconflict on public health, including anassessment of how winter intensifiesthe war on public health in a diffuseand apparently "natural" manner.
II. The defense of public health: abrief summary of how those chargedwith protecting the public health haveresponded to this broad assault.
III. Recommended action: basedon this analysis of the essential natureof the conflict, a set of broad recom-mendations is proposed to enhanceaccountability; to strengthen thecapacity of the public health response;and to mitigate the long term healthimpact of the conflict.
This analysis, although necessarilyincomplete, draws many fragments of infor-mation into a coherent picture. The authorshope that a clear understanding of this waron public health will contribute to a moreeffective response in Bosnia and helpstrengthen the world's resolve to prevent andprepare for this kind of war in the future.
The War Against HealthPublic health focuses on providing and
protecting those conditions that allow peopleto achieve physical, mental, and social wellbeing. For practical reasons, previous descrip-tions of the health threat to the Bosnian popu-lation have usually focused on individualmeasures of physical health, such as childmortality rates, nutritional status, or reportsof epidemic disease. It is important to movebeyond this approach, for several reasons:
* "health" cannot be viewed asphysical health alone; information onmental and
social dimensions of well beingshould also be considered;
* a focus on mortality data andlimited statistics on morbidity repre-sent only partial and incomplete mea-sures of physical health;
* several conditions are necessaryfor health that extend far beyond accessto medical care. The evaluation ofthreats to health should include condi-tions such as housing,nutrition, sanita-tion, personal security, education,employment, and systematic violationsof personal and collective dignity.
At this time, it is not possible to presenta full analysis or accounting of this war's bur-den on the physical, mental, and social wellbeing of the Bosnian population. The infor-mation needed to identify fully and measureadequately these health impacts does not yetexist -- in Bosnia or elsewhere. Nevertheless,since this war involves the systematic undermining and destruction of the full range ofconditions that people require to be healthy,and despite the limitations in available infor-mation, this report seeks to illustrate theprocess through which a more completeaccounting of suffering in Bosnia and, byextension, human suffering in conflicts andwar, could be approached.
Conditions Needed for HealthHealth -- physical, mental, and social
well being -- depends upon several basic,essential conditions. For this analysis, fivesuch conditions were selected; the availabili-ty and/or quality of: (1) food; (2) water; (3)fuel/energy; (4) health services; and (5) per-
Bosnia: The War Against Public Health Mann et al 131
sonal security. In a modern community inany developed country, these conditionsshare two characteristics: they are providedthrough complex systems beyond individualcontrol (food supply, water systems, fuel dis-tribution networks, private and governmen-tal health systems, and police/ justice sys-tems); and they are taken for granted. If theseessential conditions are not provided, indi-vidual and social life must be drastically reor-ganized. In Bosnia, the search for an ade-quate supply of food and safe water, fuel forheating and transport, health services (pre-ventive and curative), and a modicum of per-sonal security becomes not only a matter ofsurvival but a source of risk.
Winter can only lead to further deterio-ration of health in Bosnia. Cold weathertends to increase crowding, which may havea broad range of effects on personal and col-lective hygiene, heightens the risk of trans-mission or amplification of pathogenic agents(via personal contact, food, water, vector-borne, respiratory, and fecal-oral routes), andmay also have substantial impact on mentaland social well being. Winter creates newproblems, including cold-related injury. Tothe extent that availability of material andsupplies (including food, fuel, and medicalsupplies) is further con strained by trans-portation difficulties secondary to winterconditions, the damage to public health willbe increased.
Lack of AccessDenial of free and unconstrained access
is the fundamental method through whicheach of the essential conditions for healthhave been undermined and attacked. Themovements of people and goods to, from,and within Bosnia have been dramaticallyrestricted. The creation of "enclaves" is sym-bolic of the extent to which the civilian popu-lation of Bosnia have become a hostage peo-ple; isolation deprives them of practical andemotional support and provokes despair.
The damage to basic conditions forhealth and the exacerbation of specific healthproblems are intensified by three factors:geographical and demographic concentrationof the most vulnerable populations; deple-tion of physical, mental and social "reserves"due to the duration of the conflict; and thespecific conditions of winter.
The concept of vulnerability as applied topeople living in a war zone may seem super-fluous. Certainly in the current war in the for-mer Yugoslavia, in which an estimated 180200,000 people may have already died fromviolence, the principal hazards seem clear forboth civilian and military populations.
A focus on the civilian population, how-ever, reveals three critical facts:
1. New vulnerable populationshave been created, involving enclavesand other areas with lack of access tothe essential conditions needed forhealth.
2. Illness, disease! and death arenot randomly distributed. The greatesthealth burdens among non-combat-ants fall upon four groups: the veryyoung, the elderly, the chronicallysick, and the disabled. As a conse-quence of the current conflict, the vul-nerable populations mentioned abovehave been concentrated geographical-ly far beyond pre-war conditions.
3. Displaced people constituteanother new vulnerable population,created by warfare and the horror of"ethnic cleansing."
Therefore, the illness, suffering, anddeath of these three interrelated groups inBosnia is not "collateral" or incidental; rather,they are the frontlines of the war on publichealth.
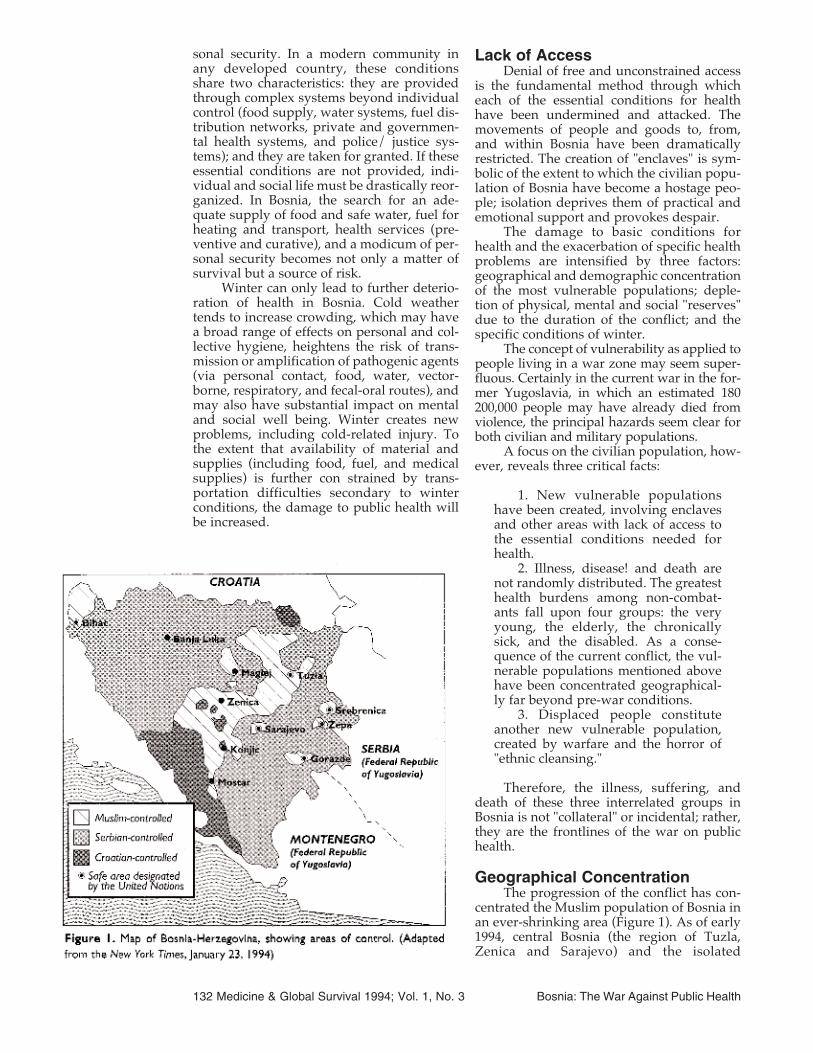
Geographical ConcentrationThe progression of the conflict has con-
centrated the Muslim population of Bosnia inan ever-shrinking area (Figure 1). As of early1994, central Bosnia (the region of Tuzla,Zenica and Sarajevo) and the isolated
132 Medicine & Global Survival 1994; Vol. 1, No. 3 Bosnia: The War Against Public Health
enclaves of Bihac and Tesanj/Maglaj in thewest; and Srebrenica, Zepa, and Gorazde inthe east constituted the area still under polit-ical control of the government of Bosnia. Thetotal population within these boundaries wasapproximately 2.7 million. Of these, an esti-mated 2.1 million were within areas wheremore than 90 percent of the population isMuslim.
The characteristics of the population areas important as the number of people in anygiven area. Vulnerability can be expressed indemographic terms (age, gender), by thepresence of certain conditions (pregnancy,chronic illness, disability), or in social terms(institutionalized populations, such as pris-oners, the mentally ill, the retarded,orphans).
A distinctive feature of the population ofBosnia is its shifting demographic structure.As the territory of Bosnia shrinks it includesan ever-increasing proportion of these vul-nerable populations (those too young, old orweak to escape). Limited available data forspecific areas suggest that the proportion ofchildren (under 14 years of age) in the popu-lation has increased along with the propor-tion of elderly (over 65 years of age). Thehealth status of these groups is precarious orhighly susceptible to a variety of external fac-tors such as lack of food, water, fuel/energy,and health services.
Displaced PopulationsAs a result of "ethnic cleansing" and
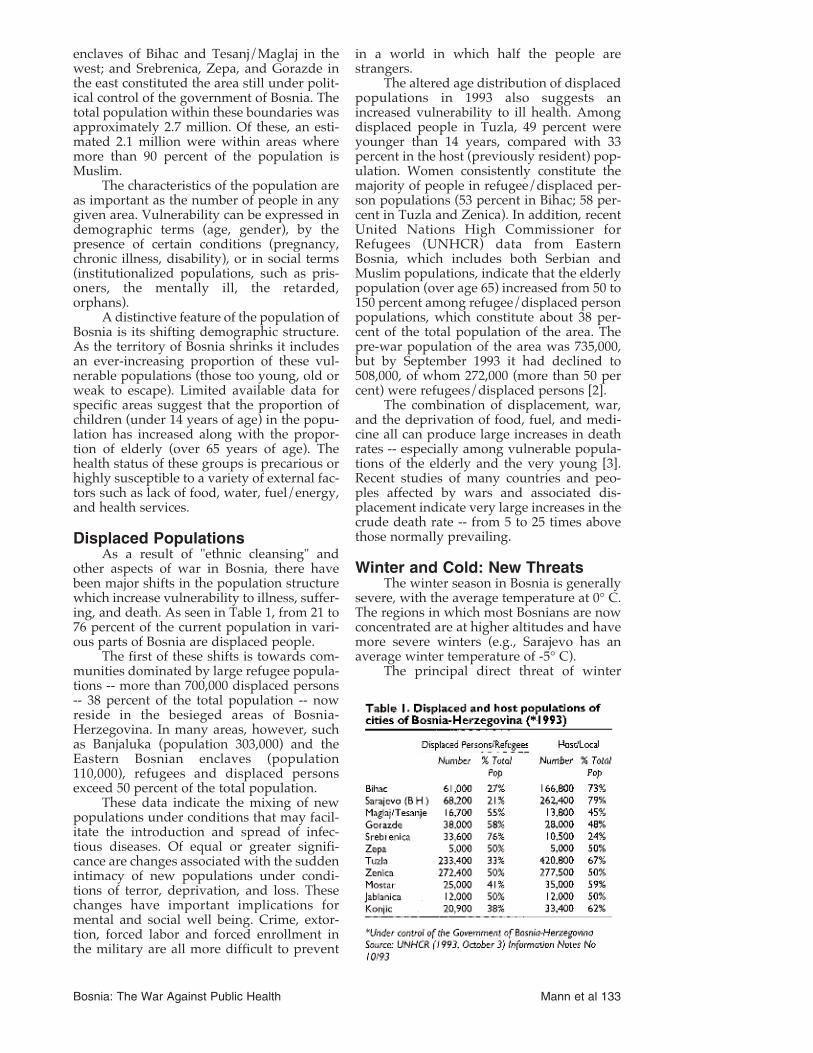
other aspects of war in Bosnia, there havebeen major shifts in the population structurewhich increase vulnerability to illness, suffer-ing, and death. As seen in Table 1, from 21 to76 percent of the current population in vari-ous parts of Bosnia are displaced people.
The first of these shifts is towards com-munities dominated by large refugee popula-tions -- more than 700,000 displaced persons-- 38 percent of the total population -- nowreside in the besieged areas of Bosnia-Herzegovina. In many areas, however, suchas Banjaluka (population 303,000) and theEastern Bosnian enclaves (population110,000), refugees and displaced personsexceed 50 percent of the total population.
These data indicate the mixing of newpopulations under conditions that may facil-itate the introduction and spread of infec-tious diseases. Of equal or greater signifi-cance are changes associated with the suddenintimacy of new populations under condi-tions of terror, deprivation, and loss. Thesechanges have important implications formental and social well being. Crime, extor-tion, forced labor and forced enrollment inthe military are all more difficult to prevent
in a world in which half the people arestrangers.
The altered age distribution of displacedpopulations in 1993 also suggests anincreased vulnerability to ill health. Amongdisplaced people in Tuzla, 49 percent wereyounger than 14 years, compared with 33percent in the host (previously resident) pop-ulation. Women consistently constitute themajority of people in refugee/displaced per-son populations (53 percent in Bihac; 58 per-cent in Tuzla and Zenica). In addition, recentUnited Nations High Commissioner forRefugees (UNHCR) data from EasternBosnia, which includes both Serbian andMuslim populations, indicate that the elderlypopulation (over age 65) increased from 50 to150 percent among refugee/displaced personpopulations, which constitute about 38 per-cent of the total population of the area. Thepre-war population of the area was 735,000,but by September 1993 it had declined to508,000, of whom 272,000 (more than 50 percent) were refugees/displaced persons [2].
The combination of displacement, war,and the deprivation of food, fuel, and medi-cine all can produce large increases in deathrates -- especially among vulnerable popula-tions of the elderly and the very young [3].Recent studies of many countries and peo-ples affected by wars and associated dis-placement indicate very large increases in thecrude death rate -- from 5 to 25 times abovethose normally prevailing.
Winter and Cold: New ThreatsThe winter season in Bosnia is generally
severe, with the average temperature at 0° C.The regions in which most Bosnians are nowconcentrated are at higher altitudes and havemore severe winters (e.g., Sarajevo has anaverage winter temperature of -5° C).
The principal direct threat of winter
Bosnia: The War Against Public Health Mann et al 133

involves cold-induced and cold-related dis-ease and injury. The concentration withinBosnia of segments of the population (theyoung, the chronically ill, and the elderly) aremore vulnerable to cold-related illnesses andinjury will intensify the damage to healthresulting from the winter.
The war and the conditions it has creat-ed in the besieged areas of Central Bosniainfluence the health of all groups. Elderlypeople and young children will be at specialrisk this winter due to cold, food shortages,and poor medical care. Under normal condi-tions, those over 65 years of age (approxi-mately 10 percent of the population of pre-war Yugoslavia) account for 65 percent of all"natural" deaths. Infants (younger than 1 yearold) are the other group that normallyaccount for a disproportionate number ofdeaths; they constitute one percent of thepopulation yet account for four percent ofdeaths. Therefore, the crude death rate willincrease as the proportion of the elderly risesin the Bosnian population. In addition, thedeath rate among the elderly will increasedue to winter conditions, exacerbated bypoor nutrition and sanitation, the absence ofmedications, and mental stress.
As many as 60 percent of all causes ofdeath observed in adults in industrializedcountries (e.g. respiratory, cardiovascular,injuries, etc.) are susceptible to substantialincreases through the effects of cold, hunger,and stress. In a country accustomed toWestern medicine, the lack of access tomodem medical care services is a hugechange and may portend a sharp rise in deathrates among vulnerable populations.
Winter months are routinely associatedwith increased mortality rates; generally theincrease is 20 to 35 percent over summerrates. In pre-war Yugoslavia excess winterdeaths were generally at the high end of thisrange, at 30 percent above the June-September figures. More developed andmore prosperous northern countries withbetter health care and infrastructure(Sweden, for example) show less increase(lower than 12 percent) in winter comparedto summer deaths [4].
The effects of winter on health havebeen studied for many years. In general, thecold acts on all organ systems, but cardiovas-cular and pulmonary diseases have beenmost closely studied. For both conditionsthere is an increase and a worsening in sever-ity and outcome in cold winter months. Inadults, 66 percent of the incremental deathsoccurring in winter are due to cardiovasculardiseases (especially myocardial infarctions)and 13 per cent are due to respiratory condi-tions (influenza and pneumonia). Winter's
effects on health are often visible as twopeaks of increased mortality -- one an"instantaneous effect of winter" on the car-diovascular system, the other a "delayed andmuch smaller effect" associated with respira-tory infections [5].
The 1992/93 winter brought news fromBosnia of multiple families huddled in oneroom trying to keep warm and of "whitedeath," as people looking for food traveledthrough the mountains in the winter, only todie from exposure. Though the winter wasrelatively mild, the lack of fuel forcedBosnians to use trees and wooden furniturefrom homes for heating [6]. In the secondwinter of the war, the weather was moresevere and there were few trees or pieces offurniture left to burn. Refugees/displacedpersons who left home in their summerclothes were totally dependent on humani-tarian aid for clothes, shelter and food [7].UNHCR alone has spent nearly $23 million inaid for fuel, clothing, stoves and other win-ter-related supplies to be distributed inBosnia.
During the 1992/93 winter in Sarajevo,UNHCR reported that the mortality rateamong the elderly in homes was double theusual December rate. The elderly in collectivecenters were observed to be sleeping on barefloors without adequate covering [8].
In hospitals, signs of hypothermia wereseen among bedridden, incontinent people."Hospitalized paraplegics, young men of 20years old, lay for days in their cold urine -- nowater, no washing, no linen changes, nocatheters..."[9]. Surgeons were unable tooperate with cold fingers, equipment failedand liquids froze.
In summary, despite the tragic nature ofdeath and injury from cold itself (hypother-mia), the major health impact of winterresults from: the stresses produced by theconstant struggle against cold weather, snow,and ice (with its associated burdens on dailyliving); pervasive deleterious effects on thebroad range of conditions needed for health(e.g., food, fuel, medical supplies); andamplification of health risk to the very youngand the elderly.
The influence of winter is insidious. Foras the arrival of winter and its severity areboth beyond human control, winter appearsto be neutral in this conflict. Tragically, how-ever, winter is aiding those seeking todestroy the health of the people of Bosnia.
FoodA modern analysis views severe food
shortages as a consequence of politicalactions or inactions, rather than simply amatter of insufficient food production.
134 Medicine & Global Survival 1994; Vol. 1, No. 3 Bosnia: The War Against Public Health

Population food needs are assessed as a com-bination of baseline caloric requirements(daily caloric requirements increase by 1% forevery degree drop in mean daily temperaturebelow 20° C.) as well as availability of criticalnutrients. Populations experiencing a wide-spread and sustained lack of food suffer awide range of impacts on physical, mental,and social well being, particularly when thefood deficit is of long duration.
Available evidence suggests that theBosnian population is experiencing a chronicfood deprivation whose severity varies wide-ly, over time and among different sub-groupsof the population.
Data from the spring of 1993 suggestthat the normal mechanisms of food produc-tion and distribution have been profoundlydisrupted in Bosnia. The rural areas have notbeen able to produce enough food to meet theneeds of the urban population, and foodshipments into and within Bosnia are severe-ly constrained [10]. The main UNHCR ware-house in Metkovic, which supplies the south-western portion of Bosnia, was empty inearly April 1993. During that month, 7,780metric tons (MT) of wheat flour werereceived but could not be moved into centralBosnia [11]. The port of Ploce had food aid forBosnia in June 1993 which could not be deliv-ered because there was no fuel for trucks;some of the perishable food spoiled and hadto be discarded [12]. The local Red Cross soci-ety estimated that as a result of these types ofdisruptions, 90 percent of the population ofBosnia was unable to meet its basic foodneeds as of October 1993 [13]. According toUNHCR, the World Food Program (WFP),and UNICEF, an estimated 50% of the foodneeds of the population of Bosnia must bemet through humanitarian aid [14]. In March1993, the WFP estimated that 2.3 millionrefugees and displaced persons were in needin Bosnia [15].
Humanitarian organizations have madeheroic efforts to feed the population ofBosnia. Particular nutritional needs of thepopulation in different areas have been docu-mented and the types of food delivered havebeen adjusted to alleviate health problemsthat may have arisen from malnutrition[13,16,10]. The basic foods supplied haveincluded high-protein biscuits, oil, beans,flour, cheese, dried milk, sugar, salt, and vit-amins [10].
These efforts have only been partiallysuccessful, for several reasons. Food stored inwarehouses has not been able to reach itsintended recipients due to shelling, closedroads, and the turning back of convoys [17].The total amount of additional food neededfor Bosnia in early 1993 was estimated to
range from 9,000 (UNHCR) to 17,000 metrictons per week (WFP) [18]. According to avail-able sources, need has far exceeded deliver-ies. UNHCR was able to deliver only 22,000metric tons (62 percent of need) in July and25,000 metric tons (69 percent) in August1993. In October 1993, UNHCR delivered 29to 35 percent of the food requirement to cen-tral Bosnia (exception: 62 percent to Tuzla)[2]. As of November 1993, UNHCR reportedthat due to weather and security problems,only about 50 percent of the food require-ment was able to be delivered [18].
In addition, the lack of fuel for cookinghas exacerbated the effects of the food short-age [17,12]. Much of the flour and rice couldnot be used because there was no water orfuel for cooking. The 1993 summer fruit har-vest in Tuzla was plentiful, but fresh fruitcould not be preserved due to lack of sugar.Similarly, because there was no fuel to runthe farm equipment, Tuzla was expected tohave a wheat harvest of only 2,200 MT com-pared with a potential yield of 20-25,000 MT[12,19].
Statistics on both the scope and impactof chronic food deprivation are only availablefor individual towns, neighborhoods, hospi-tals and collective centers (for refugees anddisplaced persons), and are generally notavailable for the most isolated and threat-ened communities. Yet the information thatcan be obtained reveals a picture of a suffer-ing population.
The Food Crisis and MalnutritionUNHCR, UNICEF, and the World
Health Organization (WHO) have carried outseveral nutritional surveys since the begin-ning of the conflict. While small surveys fromcollective centers in 1992 found a high per-centage of children to be malnourished, aWHO summary of 1993 data found only 1.8percent of children to be undernourished[20,21]. Nutritional studies of adults have uti-lized the Body Mass Index (BMI). InSrebenik, in November 1992, 35 per cent ofadults were found to be suffering from mal-nutrition (BMI below 18.5). In March 1993,WHO found that in two areas -- Sarajevo andZenica -- between four and 12 percent ofwomen surveyed were suffering from mal-nutrition. Strikingly, women belonging to theresident population in these areas were morelikely to be malnourished than womenamong refugee or displaced populations. Thesame survey found that more than one-thirdof children and mothers in Bihac and 13 per-cent of mothers in Sarajevo had some degreeof anemia (Table 2) [21].
In a survey conducted in October 1993,UNHCR found that adults in central Bosnia
Bosnia: The War Against Public Health Mann et al 135

had lost an average of 10 kilograms (22pounds) over the course of the war [22].Sources in Sarajevo have estimated theweight loss among adults in central Bosnia toaverage nine to 15 kilograms (19.8 to 33pounds) [23]. WHO reported that body fatreserves of much of the population had beenexhausted by the end of the 1992-93 winter,and that the population of central Bosnia wason the verge of chronic energy deficiency [7].
As the war continues, the food crisisbecomes more desperate. In March 1993,WHO reported a few cases of scurvy, suspect-ed pellagra, and other vitamin and nutritionaldeficiency syndromes among refugees/dis-placed persons. WHO estimated that therewere 20 to 30 additional deaths per day due tomalnutrition and related infections inSrebrenica in March 1993. The estimated pop-ulation of 60,000 people needed 60 metric tonsof food per day, but was totally cut off fromincoming convoys and supplies [24].
Mental and social well being are notonly threatened directly by lack of food, butthe struggle for limited food supplies cangenerate emotional distress and interperson-al conflict. The monotony of the diet has beenreported to cause depression and associatedlack of appetite even among the malnour-ished [24]. At Knin General Hospital, inCroatia near the Bosnian border, desperatemothers tried to leave their children in thecare of the Pediatric Department becausethey could no longer feed them [25].
In summary, food -- the single most fun-damental requirement for health -- is beingdenied to the population of Bosnia. A chron-ic food deficiency of variable severity andduration has been created in Bosnia, with itsensuing physical, mental, and social conse-quences. Winter can only aggravate this situ-ation, due to the combined result of dimin-ished/absent food production, increasedtransportation difficulties, and the higherenergy/caloric needs of a population in coldweather.
WaterWater -- clean and in sufficient quantity
-- is absolutely essential for health. In termsof availability of adequate and safe water,Bosnia has been reduced to a pre-moderncondition. Water can no longer be taken forgranted and its acquisition has become asource of risk. Paradoxically, the Bosnianpopulation, which has ample natural watersupplies, now lacks drinking water becausethe water supply infrastructure has been sys-tematically destroyed. Water treatmentplants have become largely non-functionaland water pumping and distribution systemshave collapsed, due to sabotage, vandalism,lack of power (also a result of sabotage andvandalism), and lack of maintenance andsupplies [16,2,26].
Pre-war consumption of water inSarajevo was about 200 liters per person perday. Sarajevo used a 6.2 megawatt electricalsystem to supply power to water pumpingstations that supplied 210,000 cubic meters ofwater daily to a 53-square-kilometer area[27]. Since the war began, however, electrici-ty has been available intermittently or not atall [28]. In Sarajevo, different factions controlparts of the electrical network that suppliespower to the pumping station, resulting in alimited and unpredictable water supply. Theshortage of electricity has severely hamperedwater pumping from the stations. Thus, inJuly 1993, there was virtually no power avail-able for water pumping; water was rationedat two to three liters per person per day [26].
Further, under pre-war conditions, anaver age of 5,000 leak repairs were performedon the water system in Sarajevo each year;during the past year, it was only possible torepair 300 leaks. As a result, the leakage fac-tor has doubled from a pre-war level of 30percent to 60 percent. The Sarajevo watercompany normally employs 1,300 people, butits work force has now been reduced to only300 [27].
An International Rescue Committee pro-ject has developed two new water treatmentplants for Sarajevo. Protection from shellinghas been achieved by installing one plant in atunnel and another under a concrete roofcovered with a meter of soil and junk carsintended to detonate mortars before impact.Thus, by early January 1994, 450,000 liters ofclean water were to have become available inSarajevo, which is sufficient to supply at leastone-third of the Sarajevo population [27].
In Srebrenica, destruction of the munici-pal water supply infrastructure has had sev-eral important consequences. People havebeen forced to obtain water from othersources, including untreated water fromwells, rivers and streams, or from humanitar-
136 Medicine & Global Survival 1994; Vol. 1, No. 3 Bosnia: The War Against Public Health
ian organizations which truck in water whenpossible [8,29]. In Srebrenica, before the war,there were 5,000 inhabitants and all rawsewage went into the Jelini River. BySeptember 1993, the number of inhabitantshad increased to 25,000, and raw sewage wasstill released into the river [29]. As the watertreatment plant was not operational, howev-er, untreated river water has been used fordrinking; this river is also known to havehigh levels of lead. Inadequate water flowhas also created dangerous sanitation prob-lems; without water, modern human wastedisposal systems cannot function. Sewagehas backed up into homes and low pressurein water lines has led to cross-contaminationwith sewage lines [27].
Scenes previously associated with poor-er developing countries have now become anintegral part of life in Bosnia. Standing in linefor water, and carrying water in small con-tainers for long distances, have become com-monplace. In addition to the logistical diffi-culties, container-related contamination, andadditional expenditure of energy, peoplemaking their trips for water are exposed tosniper fire. In Mostar, inhabitants have riskedtheir lives by crossing the front lines at nightto get water [30].
Humanitarian organizations firstattempted to provide Bosnia with adequateclean water and, when this was not possible,chlorine tablets were sent in an effort to makeavailable water safer to drink. Between April1992 and August 1993, the InternationalCommittee of the Red Cross (ICRC) supplied40 municipalities with spare parts, pumps,chlorinators, and more than 70 tons of watertreatment chemicals [31].
Fuel/EnergyFuel to produce electrical, thermal, and
mechanical energy is essential to ensure ade-quate supplies of food and water, to protectagainst cold, to provide modern medical andpreventive health services, and to ensure ade-quate sanitary and hygienic conditions.Insufficient supplies or distribution of fuelleads to serious direct and indirect threats tohealth.
The supply of fuel to Bosnia and its dis-tribution have both been seriously curtailed,so that fuel for heat and transport has becomea central focus of survival efforts. UNHCRestimated that Bosnia would need 17.3 mil-lion liters of diesel fuel for schools, hospitals,mines, and power plants during the 1993-94winter. In November 1993, the available stocktotalled 3 million liters, with another 10 mil-lion liters in the pipeline -- a shortfall of atleast 4.3 million liters [16].
Before the war, Sarajevo relied mainly
on natural gas from the Ukraine andHungary to heat buildings. During the war,the natural gas pipe lines have been shutdown. A project supported by outside aid hasreconnected 20,000 people in Sarajevo withthe natural gas pipeline. In November 1993,natural gas in Sarajevo was restored to theminimum pressure of 1 bar after having beenshut down since May 1993 (pre-war pressurewas 6-8 bar) [2]. In 1993, Sarajevo requested105,000 m3 of gas from Hungary. Only 50,000m3 were allowed, however, of which 30,000m3 was diverted, leaving only 20,000 m3 forSarajevo [32].
Given the difficulties of maintainingnatural gas supply and distribution infra-structure, coal is considered the optimal fuelfor Bosnia [33]. Humanitarian organizationshave been struggling to provide materials forenergy efficient stoves that burn wood or coal[34]. The ability to supply coal insufficientquantities has been the central problem[6,16].
Health ServicesBosnia's once well developed health sys-
tem has been crippled and is no longer capa-ble of meeting even the basic health careneeds of the population.
In general, health care personnel areavail able. Local health care workers -- whohave borne the brunt of more than two yearsof conflict -- have been supported by a steadyflow of international health personnel fromhumanitarian organizations. Major gaps havedeveloped, however, in the infrastructureand supplies needed to deliver health care.This is the result of destruction of institutions(including ongoing threats to basic security),lack of specific medical supplies, and lack offuel.
The lack of energy, food, and suppliesmeans that many hospitals have no heat,lights, medical supplies, or capacity to ensurehygienic precautions. In these settings, oper-ations may be performed by candlelight, without anesthesia, by surgeons with freezinghands. Hospitals report a lack of diagnosticreagents, bandages, medicines, prostheses,dialysis equipment/supplies, and radiologysupplies. Populations particularly vulnerableto deficiencies of health care include preg-nant women, infants, the elderly, and thechronically ill.
Mental health services appear to havebeen particularly vulnerable to destruction.Prior to the war, Kosevo Hospital (Sarajevo)had one of the major psychiatry departmentsin the former Yugoslavia. The hospital wasbombed in April 1992, resulting in closure ofthe psychiatry department, including its alco-hol and drug rehabilitation units. Anecdotal
Bosnia: The War Against Public Health Mann et al 137

reports suggest that institutions serving thementally retarded and men tally ill have beenamong the first to lose access to fuel andother supplies [9]. A household survey con-ducted in December 1993 in Sarajevo con-cluded that 9.5 percent of all households hadone or more members suffering from mentalhealth problems. Ninety seven percent ofpeople suffering from mental health prob-lems required professional assistance butonly about one-third of them were able togain access to professional help [35].
Humanitarian organizations and WHOhave been sending medical supplies toBosnia, including several types of medicalkits designed to meet the needs of an area forseveral months. As a result of these effortsand the ability of some hospitals to obtainminimal supplies, some hospitals are operat-ing under fair to good conditions. Others,however, overwhelmed with injuries result-ing from the conflict, are operating underhighly adverse conditions [36].
Personal SecuritySince the beginning of the war in the for-
mer Yugoslavia, an estimated 3,000 childrenhave been killed by snipers. The news mediahave estimated that during the course of thecurrent conflict, thousands of women havebeen raped. In Sarajevo alone, from April1992 to March 1993, 6,800 civilians died andapproximately 16,000 were wounded. Inshort, the war has deprived non-combatantsof basic security and has torn apart a society.
In November 1993, a psychiatrist inSarajevo described a phenomenon he calledpassive suicide: the act of walking in areasknown to be dangerous... "a more primitiveform of suicide, the emotion without theintellectual plan." "A great number of elderlyhospital inpatients seem to have lost the willto live. People are suffering from all modes ofsevere trauma: shells, freezing, hunger,grief...Usually in war there are two soldierskilled or wounded for every civilian, but inthis war there are eight to nine civilians forevery soldier. After the war, psychiatry willbe flooded" [37].
Specific Health ProblemsA wide range of specific health problems
result from the combined effects describedabove. The following were selected to illus-trate this connection: (1) vaccine preventablediseases; (2) diarrheal disease; (3) prematurityand low birthweight babies; (4) injuries (non-combat related); (5) respiratory tract infec-tions; (6) ectoparasites (lice, scabies) and relat-ed diseases; and (7) chronic diseases (heartdisease, diabetes, hypertension).
Measles and Other Vaccine-Preventable Diseases
Prior to the war, childhood immuniza-tion was a regular and highly successful partof maternal and child health services. Before1992, 95 percent of infants in the formerYugoslavia received measles immunization.As a result of the war, in the Bihac pocket, thevaccination level among 1-year-olds whoshould have received measles immunizationfell to 60 percent in 1992 [26].
The disruption of health services, theshort age of vaccines and cold chain equip-ment, and reduced access to services hasseverely affected the immunization programin Bosnia. In June to July 1993, a survey con-ducted in four sites in Bosnia found that theproportion of children fully immunized hadplummeted in some areas to nearly 30 per-cent (Table 3).
The high drop-out rates shown in Table4, indicating an inability to complete vaccina-tion series, were a further alarming sign ofdeclining performance of the child healthprotection system.
In Sarajevo, childhood vaccination cov-erage was estimated at 40 percent, decliningfurther to about 20 percent by September1993 [38]. In addition, while 96 percent ofchildren included in the survey in Bihac (June1993) had received BCG at birth, fewer thanone-third had received all childhood immu-nizations, including measles, by 13 months ofage [39].
Immunization coverage is at an all-timelow in comparison with the pre-war era. Alarge pool of children susceptible to a sud-den, large scale measles epidemics existedduring the winter months of 1993-94. Thelevel of immunization coverage is a measureof the status of public health. In Bosnia, theevidence is clear: public health services havedeteriorated to the point where basic protec-tions are not provided. This deficiency doesnot result from a lack of trained personnel,but reflects the paralysis of an entire infra-structure.
Low childhood immunization ratestranslate directly into adverse individual andcollective consequences. At the individuallevel, the preventable burden of morbidity,disability, and mortality will be borne dispro-portionately by the youngest, most vulnera-ble segment of the population. The sequelaeof tuberculous meningitis or poliomyelitis,added to the negative impact that vaccinepreventable diseases will have on the precar-ious nutritional status of children, will havelong-lasting effects.
On a collective level, the risk of trans-mission of vaccine preventable diseases willexpose the population of Bosnia -- and neigh-
138 Medicine & Global Survival 1994; Vol. 1, No. 3 Bosnia: The War Against Public Health

boring countries as well -- to an increasedrisk of epidemic disease spread. Diphtheria,already reported from several EasternEuropean countries [40], as well aspoliomyelitis, measles, and pertussis all findfertile ground in crowded situations.
Diarrheal DiseasesWhile measles, polio, diphtheria, and
pertussis vaccination coverage rates reflectthe adequacy of health services (immuniza-tion delivery capacity), diarrheal diseases area consequence and measure of sanitary con-ditions. Diarrheal diseases flourish underconditions of poor food and water hygiene,and most result from fecal-oral spread, whichis also enhanced by crowding and lack ofadequate facilities to dispose of human fecalwaste.
Therefore, it is not surprising that diar-rheal diseases and, more generally, food- andwater borne diseases, have increased inBosnia since the beginning of the conflict. Thehygienic infrastructure which was intendedto protect the Bosnian population againstenteric disease has virtually collapsed.
The fecal contamination of water andfood may have contributed to the spread ofhepatitis A virus (HAV) infection. In the com-munity of Sorck Bunar in Sarajevo (popula-tion 3,600) more than 10 percent of the popu-lation (364 people) were reported to havedeveloped HAV infection from July toOctober 1993 [41]. The epidemic had alsoaffected other communities as evidenced byreported HAV infections: in October 1993,the municipalities of Novi Grad, NovoSarajevo, and Stari Grad had reported 27, 32,and 118 cases respectively, and more com-munities were experiencing the furtherspread of the epidemic [42]. Despite difficul-ties with disease surveillance, the number ofreported hepatitis A cases increased morethan 20-fold in Sarajevo Center in the firstnine months of 1993. In Brizim, where 10 to20 cases of HAV infection were reported
annually before the war, more than 80 caseswere reported during the period August 1 toNovember 18, 1993; 21 of these casesoccurred in the first half of November [41].
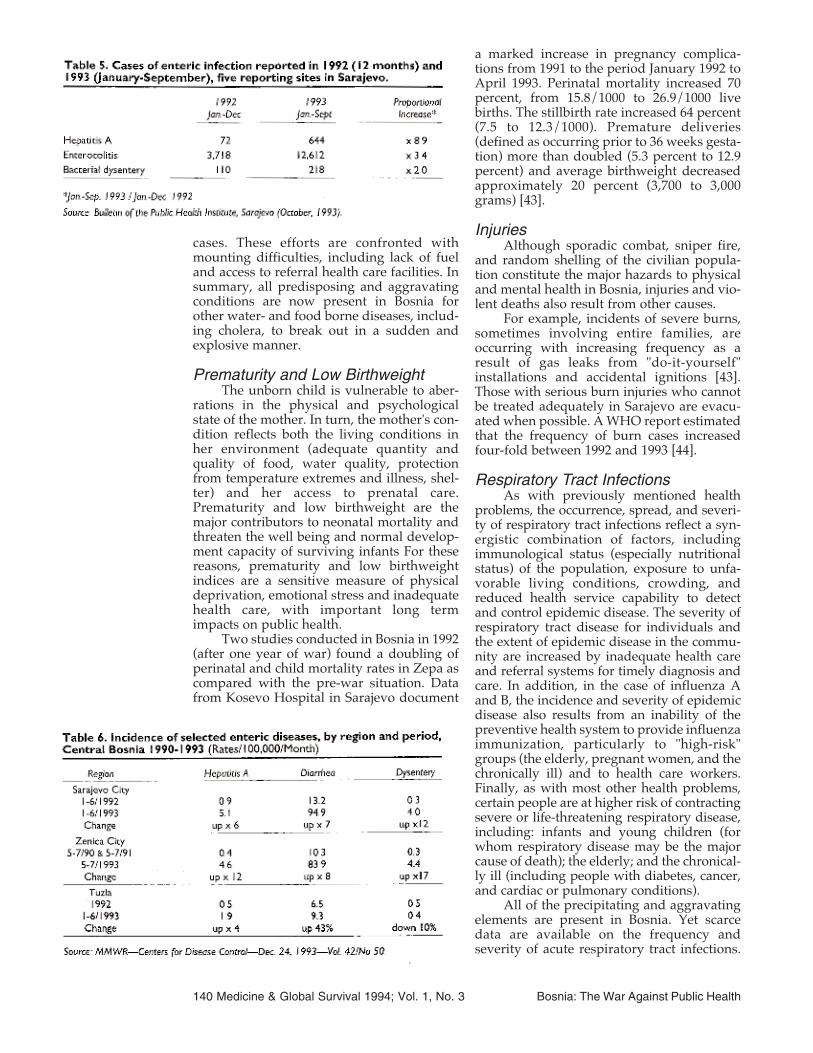
As shown in Table 5, the number ofreported cases of enteric infections inSarajevo increased 2 to 9 fold in the first ninemonths of 1993 compared with 1992. Othercommunities also reported steep increases inhepatitis A and two other notifiable entericinfections (diarrhea and dysentery) as shownin Table 6. In Sarajevo in 1992, 3,718 cases ofdiarrhea were reported (1,239 cases/100,000population) [38]. Thus, in 1993, based onreported cases for the first nine months, itcould be estimated that this rate wouldexceed a staggering 5,255/100,000 for thewhole year.
Diarrheal disease, in combination withthe lack of water and sewage, affects morethan physical health. The misery created bylack of sewage facilities in crowded quarterswith many sick people has a serious,although unmeasured, impact on mental andsocial well being. The drastic decline in per-sonal hygiene which accompanies diarrhealdisease in the absence of adequate water andsewage also diminishes personal dignity.
Local authorities and humanitarianrelief workers have made heroic efforts toimprove the quantity and quality of the watersupply, to promote better food hygiene,garbage and excreta disposal, and to rein-force early rehydration therapy for diarrheal
Bosnia: The War Against Public Health Mann et al 139
cases. These efforts are confronted withmounting difficulties, including lack of fueland access to referral health care facilities. Insummary, all predisposing and aggravatingconditions are now present in Bosnia forother water- and food borne diseases, includ-ing cholera, to break out in a sudden andexplosive manner.
Prematurity and Low BirthweightThe unborn child is vulnerable to aber-
rations in the physical and psychologicalstate of the mother. In turn, the mother's con-dition reflects both the living conditions inher environment (adequate quantity andquality of food, water quality, protectionfrom temperature extremes and illness, shel-ter) and her access to prenatal care.Prematurity and low birthweight are themajor contributors to neonatal mortality andthreaten the well being and normal develop-ment capacity of surviving infants For thesereasons, prematurity and low birthweightindices are a sensitive measure of physicaldeprivation, emotional stress and inadequatehealth care, with important long termimpacts on public health.
Two studies conducted in Bosnia in 1992(after one year of war) found a doubling ofperinatal and child mortality rates in Zepa ascompared with the pre-war situation. Datafrom Kosevo Hospital in Sarajevo document
a marked increase in pregnancy complica-tions from 1991 to the period January 1992 toApril 1993. Perinatal mortality increased 70percent, from 15.8/1000 to 26.9/1000 livebirths. The stillbirth rate increased 64 percent(7.5 to 12.3/1000). Premature deliveries(defined as occurring prior to 36 weeks gesta-tion) more than doubled (5.3 percent to 12.9percent) and average birthweight decreasedapproximately 20 percent (3,700 to 3,000grams) [43].
InjuriesAlthough sporadic combat, sniper fire,
and random shelling of the civilian popula-tion constitute the major hazards to physicaland mental health in Bosnia, injuries and vio-lent deaths also result from other causes.
For example, incidents of severe burns,sometimes involving entire families, areoccurring with increasing frequency as aresult of gas leaks from "do-it-yourself"installations and accidental ignitions [43].Those with serious burn injuries who cannotbe treated adequately in Sarajevo are evacu-ated when possible. A WHO report estimatedthat the frequency of burn cases increasedfour-fold between 1992 and 1993 [44].
Respiratory Tract InfectionsAs with previously mentioned health
problems, the occurrence, spread, and severi-ty of respiratory tract infections reflect a syn-ergistic combination of factors, includingimmunological status (especially nutritionalstatus) of the population, exposure to unfa-vorable living conditions, crowding, andreduced health service capability to detectand control epidemic disease. The severity ofrespiratory tract disease for individuals andthe extent of epidemic disease in the commu-nity are increased by inadequate health careand referral systems for timely diagnosis andcare. In addition, in the case of influenza Aand B, the incidence and severity of epidemicdisease also results from an inability of thepreventive health system to provide influenzaimmunization, particularly to "high-risk"groups (the elderly, pregnant women, and thechronically ill) and to health care workers.Finally, as with most other health problems,certain people are at higher risk of contractingsevere or life-threatening respiratory disease,including: infants and young children (forwhom respiratory disease may be the majorcause of death); the elderly; and the chronical-ly ill (including people with diabetes, cancer,and cardiac or pulmonary conditions).
All of the precipitating and aggravatingelements are present in Bosnia. Yet scarcedata are available on the frequency andseverity of acute respiratory tract infections.
140 Medicine & Global Survival 1994; Vol. 1, No. 3 Bosnia: The War Against Public Health

Accounts from Sarajevo and Modrica suggestan increased frequency of respiratory tractinfections; in displaced person centers, heat-ing by smoky wood stoves led to a largenumber of eye infections and exacerbation ofchronic respiratory diseases among the elder-ly [45,25]. Management of severe forms ofrespiratory tract infection has been affectedby the lack of oxygen in Sarajevo hospitals[451. Respiratory tract infections were report-ed to be the most common cause of mortalityin February-March 1993 in Volvodina. InSrebrenica, 20-30 deaths from pneumoniawere reported daily during this period, morethan 20 times the number recorded in pre-war times during the same period of the year.In 1992, respiratory diseases were the mostcommonly reported cause of morbidity inSarajevo [24]. In addition to pneumonia,which is a major cause of death among chil-dren living in precarious situations, the lowimmunization coverage among children (par-ticularly regarding pertussis and measles)increase the risk of outbreaks of respiratorytract infections.
Tuberculosis is a particularly complexproblem for health services, as its controlrequires both preventive and sustained casemanagement capacity. In contrast to the viralrespiratory diseases, treatment exists to pre-vent clinical tuberculosis in exposed people(such as household contacts with an activecase) and to treat active tuberculosis casesand render them non-infectious. The controlof tuberculosis is a useful indicator of the sta-tus of preventive health care services andinfrastructure. The tuberculosis situation inthe former Yugoslavia was assessed by aWHO team in June-July 1993 [46]. During thepre-war period, the former Yugoslavia had ahigh tuberculosis incidence (30/100,000 in1990); Bosnia had the highest incidence oftuberculosis in the country (85/100,000 in1990) [47]. The deterioration of the healthcare system currently does not allow for theprocurement of meaningful data on tubercu-losis. For example, 610 tuberculosis caseswere reported in 1991, but only 81 in 1992.Yet by January 1993, a WHO report suggest-ed that the number of tuberculosis cases hadincreased four-fold in Bosnia since the begin-ning of the war, a rise that was attributedpartly to the influx of refugees and displacedpersons [7]. Patient compliance with anti-tuberculous treatment is hampered by thediscomfort of having to stay in unheated hos-pitals, lack of medications, and pervasiveinsecurity that interferes with regular atten-dance at outpatient clinics. The risk of tuber-culosis spread both within and from Bosnia isaccentuated by the inability of the health caresystem to diagnose and treat cases early and
completely. It is further accentuated bycrowded living conditions and the move-ment of people in search of shelter, food, andsecurity.
Ectoparasites and related diseasesOutbreaks of vector-borne diseases
reflect the combined lack of medical, sani-tary, and preventive health services. Lice, thevector of epidemic typhus, propagate withmore intensity under crowded conditionsand where control measures are inadequateor absent.
Population concentration resulting fromthe conflict and the scarcity of topical agentsto treat infestation and prevent reinfestation,combined with the shortage of insecticidaldust to treat clothing and bedding, has led toa major increase in louse infestation.
By September 1993, WHO reported that,"...head and body lice infestations were out ofcontrol in many war-affected areas" [48]. Thepopulation is now highly vulnerable to epi-demic vector-borne disease, particularlyamong children and people living in institu-tions and communes.
Scabies, another ectoparasite, has spreadrapidly since the beginning of the conflict. Of109 children under the age of 5 years sur-veyed in Srebrenica in September 1993, 23percent had scabies and 20 percent had lice[29]. In the same area, reported scabies infes-tation declined in five clinics: from 2265 casesin June 1993 to 639 in August 1993. This pos-itive effect may have resulted from intensiveefforts supported by Medecins sansFrontieres to train local workers and supplyscabicidal treatment lotions [49].
Chronic DiseasesDespite remarkable work by local health
personnel and.humanitarian relief groups,the disruption of medical services in most ofBosnia [50] has created an immediate crisisand a longer-term threat to those with mani-fest, or not yet manifest, chronic diseases(diabetes, arthritis, cardiovascular disease,chronic pulmonary disease, cancer, chronicrenal disease, and mental disorders, includ-ing severe depression and schizophrenia).While sustained supplies of specific medica-tions are important, support of chronic illness(including attention to mental and social wellbeing) requires early diagnosis, complextreatments and counselling, support toenhance societal integration, good hygienicand dietary conditions, and close medical fol-low-up.
In Bosnia, these dimensions of care andsupport for people with chronic illnesses areprecarious, vulnerable, or absent. Specializeddrugs and medical equipment are lacking
Bosnia: The War Against Public Health Mann et al 141

(for example, insulin, cardiovascular andanti-cancer drugs, dialysis equipment andsupplies, and laboratory reagents) [51,7,45].In December 1992, 17 patients who couldhave benefitted from dialysis died from renalfailure [31]. Shortages of insulin for the treat-ment of diabetes have been reported to occurperiodically. No data are available on excessmortality due to inadequate treatment of car-diovascular diseases, which affect mostlyolder adults. Some patients with chronic dis-eases were evacuated from Bosnia to areaswhere better diagnosis and treatment wereavailable.
The impact of these deficiencies extendsfar beyond the individual patient to includefamilies struggling to protect the health oftheir chronically ill members. In September1993, a Centers for Disease Control reportconcluded: "there are severe unmet needs ofspecialized groups such as patients with can-cer, diabetes, glaucoma and renalfailure...war injuries and chronic diseasesaccount for most mortalities"
Conclusions andRecommendations
The Defense of Public HealthProtecting and promoting the health of
populations is a fundamental responsibilityof any legitimate governing authority. Whilethe conditions essential to protect healthextend far beyond the authority andresources of a Ministry of Health, thisMinistry is usually considered responsible, inthe first instance, for public health. The workof public health includes three distinct yetclosely related activities:
* assessment: data collection andanalysis to identify and describe thehealth problems facing a community;
* policy development: establish-ment of goals based on data, setting ofpriorities, and development of strate-gies to address priority health prob-lems; and
* assurance of services: design,implementation and evaluation of pro-grams to address priority health prob-lems.
Disruption of public health capabilitiesin Bosnia reflects the balance of assaults onthe people's health and the greatly dimin-ished capacity to respond to public healthchallenges. The war against public health iswinning, for two reasons.
First, the attack on the essential condi-tions for health involves societal and govern-mental sectors that cannot be controlled by
the Health Ministry (such as provision offuel, housing, and food). Until or unless thefundamental access problem is resolved, theessential conditions for health cannot berepaired and restored.
Second, the capacity of Bosnian publichealth authorities to fulfill each of the centralresponsibilities of public health is severelyhandicapped, due to the collapse of datagathering mechanisms and disruption of ser-vice delivery systems, directly resulting fromlack of access to, and free movement andcommunication within, Bosnia. As an exam-ple, the assessment function of public healthhas been seriously compromised. Since April1993, almost no data have been gatheredfrom local health posts, and data which doexist are considered unreliable. The disrup-tion of the population of Bosnia has includedmany of the professionals and othersinvolved in the public health system, as wellas those involved in clinical medicine, whothemselves may become refugees or dis-placed persons. Numerous hospitals andclinics have been shut down or destroyedsince the war began.
Staff from humanitarian organizationshave reported that their initial efforts to col-lect data were met with frustration.Desperate pleas for "help, not data; supplies,not analysis" reflect a society whose infra-structure has collapsed and whose majorstruggle is directed at survival. The difficul-ties in communication, the constant move-ment of the population, and the day-to daydisruptions caused by the war have madedata collection nearly impossible.
Nevertheless, the Director of theInstitute for Public Health in Sarajevoattempts to keep track of disease outbreaksand the availability of appropriate vaccinesand medications. The accuracy and timeli-ness of the information collected in this man-ner are limited, but the Institute strives tocarry out these functions.
Yet without accurate and timely infor-mation, specific problems and needs cannotbe appropriately identified and assessed;without the ability to possess and freelydeploy equipment, supplies, and staffaccording to public health need, critical pub-lic health services cannot be provided. Thiscollapse of health security is yet another bur-den on the mental and social well being of thepeople of Bosnia.
The Need for InformationFrom a health perspective, it is humane
and necessary, yet not sufficient, to focusupon individual tragedies, specific incidents,and immediate, urgent, and focal healthneeds. It is particularly tragic that a vocabu-
142 Medicine & Global Survival 1994; Vol. 1, No. 3 Bosnia: The War Against Public Health

lary is not available that would permit aclearer description and expression of what isnow occurring in Bosnia. For a massive effortis being made to destabilize the civilian pop-ulation, involving chronic and widespreaddeprivation, terror, psychological stress, anddestruction of societal coping mechanisms.This war is being carried out in a manner thatconceals its goals, yet threatens, in the end, tobe as effective as a military battle or overtgenocide. It is therefore essential to recognizethe essential nature of this conflict: a war onthe health of the people of Bosnia. The warmay be conducted by military forces, but thetarget is the physical, mental, and social wellbeing of an entire civilian population.
The authors of this report regret thatinsufficient data exist to identify -- for thosein Bosnia and for the entire world -- thenature, scope, and intensity of human suffer-ing now under way. If a more comprehensiveunderstanding and assessment of sufferingwere available, it could contribute to increas-ing international pressure for all parties toreach a settlement.
Recommended Action: Health andPeace
The central weapon in this war on pub-lic health is interference with the free andunconstrained movement of goods (particu-larly fuel, food, and medical supplies) andpeople, which together are essential for pro-tection of health in Bosnia. To the extent thatthis is a war on public health, it is impossibleto protect public health without peace.
If peace is not obtained, the health of thepeople of Bosnia will continue to deteriorate.Nevertheless, attempts must be sustainedand expanded to mitigate the impacts of thewar on health. External support to existinghealth authorities, in order to enhance theirability to perform the basic functions of pub-lic health to the maximum extent possibleunder extremely difficult conditions, couldbe critical. Yet while several measures couldbe helpful, it must be clear that none of thesewill adequately respond to the clear and pre-sent danger to public health in Bosnia.
Crimes Against Public Health:Documentation and Accountability
Documentation of this war against pub-lic health is essential. In the face of a massiveassault on the foundations of civilian health,those in public health have a moral responsi-bility to bear witness and to describe anddocument what is happening. The war strat-egy that targets the health of an entire popu-lation must be analyzed and documentedusing the full range of public health exper-tise. Only through this process can the actual
measure of damage to the Bosnian popula-tion begin to be understood and accountabil-ity determined. In addition, as future con-flicts may share this fundamental nature of awar on public health, systematic documenta-tion and analysis of the war in Bosnia mayhelp prevent such occurrences, amelioratetheir impact, and ensure account ability.
A New Public Health Challenge: TheEpidemiology and Health Impacts ofCollective Violence
The public health response to Bosniashould stimulate a rethinking of our ability topredict, measure, and assess the healthimpacts of collective violence. To be success-ful, such analyses must go far beyond the tra-ditional measures of damage to physicalhealth that have classically dominateddescriptions of the impact of war and conflicton the health of populations. Public healthcannot and should not avoid addressing theproblem of collective violence and its impactson physical, mental, and social well being.The study of the epidemiology of collectiveviolence, including a capacity to identifyearly warning signs of impending cata-strophic damage to public health, is urgentlyneeded.
Long-Term RehabilitationIt is essential to prepare now for identi-
fiable health needs once peace is restored toBosnia. Long-term medical and psychologi-cal support will be needed, including man-agement of post traumatic stress disorder, theimpact of "loss of childhood," and the long-term impact of rape. Expert groups shouldwork now to identify the range of such needs,which will require assessment, policy devel-opment, and planning for assurance of ser-vices. A firm commitment from the outsideworld to go beyond the reconstruction ofphysical infrastructure and to help addressrehabilitation needs when the war is overshould not await the final act in the Bosniantragedy, but must be made now.
References1. Judas M, Rados M, Loncar M, Kostovic 1.Medical center for human rights: war crimesand grave breaches of the Geneva convention.Croatian Medical Journal 1993;34:334-341.2. UNICEF. Consolidated situation report forOctober 1993. Zagreb: 1993. 3. Toole MJ, Waldman RJ. Refugees and dis-placed persons: war, hunger and public health.JAMA 1993;270:600-606. 4. McKee CM. Deaths in winter: can Britainlearn from Europe? European Journal ofEpidemiology 1989;5:178-182. 5. Mackenbach JP, Kunst AE, Looman CW.
Bosnia: The War Against Public Health Mann et al 143
§
Seasonal variation in mortality in theNetherlands. Journal of Epidemiology andCommunity Health 1992;46:261-265. 6.Edwards J. Mission to Sarajevo, August 3-5.Geneva: WHO 1993; unpublished. 7. WHO.Twelfth report from the office of the WHO spe-cial representative Zagreb Dec. 6-Jan. 2, Dec. 5-Jan. 12, 1993. Geneva: 1993; unpublished.8. UNHCR. Social services mission: draft report,former Yugoslavia (focus on Bosnia) November19, 1992-December 12,1992, and December 11,1992-January 1, 1993. Practical guidelines forimplementation (a community basedapproach). Geneva: 1993; unpublished. 9. Byers M. Interviewed by Jerry Paccione, M.D.Sarajevo. November 22, 1993. 10. World FoodProgramme. WFP in former Yugoslavia.Situation report 5. Zagreb: 1993; unpublished. 11. WFP. Situation report 3. Zagreb: 1993;unpublished. 12. WFP. Situation report 4. Zagreb: 1993;unpublished. 13. UNHCR. Information notes on formerYugoslavia. Zagreb:1993;10/93. 14. UNICEF. Summary report of nutritionalhealth surveys carried out in Bosnia-Herzegovina during June/July 1993. Zagreb:1993 WHO Nutrition Unit; unpublished. 15. WFP. Situation report 2. Zagreb: 1993;unpublished. 16. UNHCR. Report No. 11 /93. Zagreb:1993. 17. WFP. Report on food aid situation. Zagreb:November 12,1993; unpublished. 18. UNHCR.Refugees. Geneva:1993;91. 19. Mercado D Personal communication withBrent Burkholder, CDC. September 1993. 20. WHO. Thirteenth report on formerYugoslavia, from the office of WHO special rep-resentative, Zagreb, Jan. 13 to Feb 7, 1993.Geneva: 1993; unpublished. 21. WHO. Report from WHO nutrition unit,Zagreb. Bihac, Sarajevo, Zenica and Tuzla sur-veys. September 24,1993. Geneva: 1993; unpub-lished. 22. UNHCR. Information notes on formerYugoslavia. Zagreb:1993;10/93. 23. Beganovic M. Interviewed by JerryPaccione, M.D. Sarajevo. November 22,1993. 24. WHO. Fourteenth report from the office ofWHO special representative Zagreb, Feb-Mar13.1993. Geneva: 1993; unpublished. 25. WHO. Fifteenth report from the office ofWHO special representative Zagreb, 14thMarch-18th April, 1993. Geneva: April 20, 1993;unpublished. 26. WHO. Eighteenth report from the office ofWHO special representative Zagreb, July-Aug.1993. Geneva:1993; unpublished. 27. Stefatic I. Interviewed by Jerry Paccione,M.D. Sarajevo. November 22, 1993. 28. Nakos. Interviewed by Jerry Paccione, M.D.Sarajevo. November 22, 1993. 29. Robertson A.
Visit to Srebrenica: recommendations, WHO on9th-12th September 1993. Geneva: 1993; unpub-lished memorandum. 30. ICRC. Press releases and communications tothe press. Geneva: July 2, 1991-November4,1993. 31. ICRC. Bosnia-Herzegovina. Geneva: 1993;unpublished. 32. Vickland W. Interviewed by Jerry Paccione,M.D. Sarajevo. November 22,1993. 33. UNHCR. Winterization strategy for Soros.Zagreb: 1993; unpublished. 34. UNHCR. Updated UNHCR winterizationprogramme in the former Yugoslavia, 1993-1994. Geneva: 1993; unpublished. 35. Medecins Sans Frontieres-Holland. Health,water and heating in Sarajevo. Amsterdam:1993. 36. WHO. Health monitor 9. Geneva: 1993. 37. Ceric I. Interviewed by Jerry Paccione, M.D.Sarajevo. November 22, 1993. 38. Bulletin of thePublic Health Institute. Sarajevo: 1993;1 -40-134/93. 39. WHO. Monthly report, WHO field office,Tuzla. Geneva: October 28,1993. 40. WHO.Weekly epidemiological record 1993. Geneva:1993;68:133-140. 41. Action International Contre la Faim. Reporton hepatitis in Sarajevo. Geneva: 1993; unpub-lished. 42. Bulletin of the Public Health Institute.Sarajevo:1993;10-025/93. 43. Simic S. Interviewed by Jerry Paccione, M.D.Sarajevo. November 22, 1993. 44. Schroll C.Letter to MPMcC. Zagreb: Nov 22, 1993. 45. WHO. Thirteenth report on formerYugoslavia, from the office of WHO special rep-resentative, Zagreb, (Jan. 13 to Feb 7, 1993). Geneva: 1993;unpublished. 46. WHO. Summary report of nutritional healthsurveys carried out in Bosnia-Herzegovina dur-ing June/July 1993. Geneva: 1993; unpublished. 47. World Bank. World Development Report.New York:1993;199-225. 48. WHO. Monitoring of health in the waraffected areas. Health Monitor 8. Geneva: 1993;unpublished. 49. MSF-Holland. Report of a household surveyin Sarajevo, Bosnia Herzegovina, April 1993.Amsterdam: 1993; unpublished. 50. Toole MJ, Galson S, Brady W. Are war andpublic health compatible? Lancet.1993;341:1193-1196. 51. UNHCR. Bosnia and Herzegovina: benefi-ciaries by region as of March and September1993. Zagreb: 1993; unpublished. 52. Centers for Disease Control. US Departmentof Health and Human Services Status of publichealth -- Bosnia and Herzegovina, AugustSeptember 1993. Morbidity and MortalityWeekly Report. 1993;50:973-982.
144 Medicine & Global Survival 1994; Vol. 1, No. 3 Bosnia: The War Against Public Health

Methods and Data Sources: The main objective of the field team,
composed of Mr. Craig Sanders and Drs.Chuck Schroll and Jerry Paccione, was thecollection of data, both quantitative and qual-itative, that could be applied to the analyticalframe work developed by the project team.Given the time limitations, as well as the sit-uation in Bosnia, it was not considered feasi-ble to gather primary data. Rather, the dataused in this report was gathered from indi-vidual contacts (personal interview and tele-phone) and from organizations in the field.
To the greatest extent possible, key per-sons in the major humanitarian assistanceorganizations were identified and contactedby the project team and were asked to pro-vide information pertinent to the project.Where an interviewee had specializedknowledge of either a sector or a geographicarea, the project team attempted to pursue amore specific line of questioning. Reportsand data collected during the course of thismission were sent to the Cambridge office.
More than 150 reports and other docu-ments were collected in November 1993 andanalyzed in Cambridge by Dr. DanielTarantola and Ms. Mary Pat McCabe. Thefinal report was prepared by Drs. JonathanMann, Ernest Drucker, and Daniel Tarantolaand Mary Pat McCabe. The report wasreviewed by public health experts in theUnited States and in Europe, including sever-al with direct experience in Bosnia, and wasreleased in February 1994. This project wassupported through a grant from the OpenSociety Fund
Bosnia: The War Against Public Health Mann et al 145

146 Medicine & Global Survival 1994; Vol. 1, No. 3 Bosnia: The War Against Public Health