
BORDERNETwork Training on HIV and HBV Co-Infections Dr. med. Wolfgang Güthoff / Alexander Leffers,...
18
BORDERNETwork Training on HIV and HBV Co-Infections Dr. med. Wolfgang Güthoff / Alexander Leffers, M.A. www.bordernet.eu www.aidshilfe-potsdam.de
-
Upload
rashad-prophet -
Category
Documents
-
view
214 -
download
0
Transcript of BORDERNETwork Training on HIV and HBV Co-Infections Dr. med. Wolfgang Güthoff / Alexander Leffers,...
BORDERNETwork Training on
HIV and HBV Co-Infections Dr. med. Wolfgang Güthoff / Alexander Leffers, M.A.
www.bordernet.eu
www.aidshilfe-potsdam.de

This presentation arises from the BORDERNETwork project which has received funding from the European Union, in the framework of the Health Program, and co-funding of the Ministry of Environment, Health and Consumer Protection of the Federal State of Brandenburg. The sole responsibility of any use that may be made of the information lies with the authors (SPI, AIDS-Hilfe Potsdam e.V.)
Table of Contents
Epidemiology
HIV/HBV co-infection
Diagnostic
Treatment
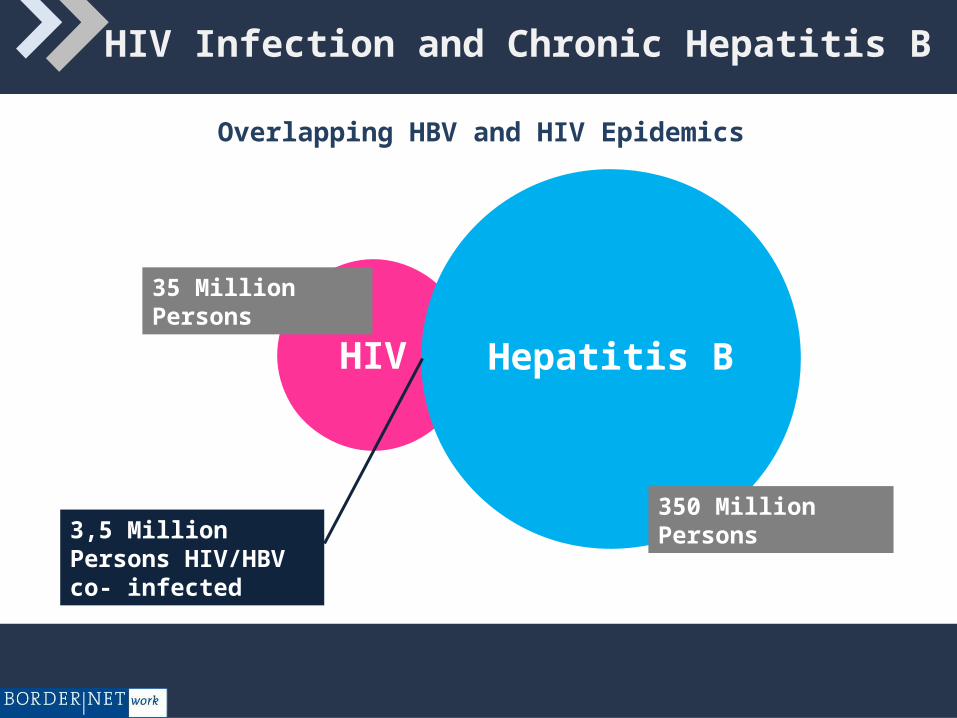
HIV Infection and Chronic Hepatitis B
Overlapping HBV and HIV Epidemics
Hepatitis BHIV
350 Million Persons
35 Million Persons
3,5 Million Persons HIV/HBV co- infected

HIV Infection and Chronic Hepatitis B
HBV/HIV Co-infection prevalence depends on HBV epidemic
5 - 7% co-infections in low prevalence countries
10 - 20% co-infections in high prevalence countries
Despite ART - increasing risk of liver related death in this group
the natural course of HBV - infection in HIV/HBV co-infected patients is different
> 8 % High
< 2 % Low 2 - 8 % Intermediate

Increased Liver Mortality in HIV /HBV Co-infected Patients
Increased rates of chronic hepatitis after infection
Higher levels of HBVDNA viraemia
Faster progression to liver cirrhosis
Increased rate of liver cancer development
HIV / HBV Co-infection
There are two main reasons for considering HBV therapy as a priority in HBV/HIV co-infected patients:
Liver disease may progress more rapidly in those patients and could lead to serious liver disease complications such as cirrhosis and liver cancer at younger ages.
There is a higher risk of developing hepatotoxicity following the initiation of antiretroviral therapy in HIV patients co-infected with HBV than in patients infected with HIV alone.
HIV / HBV Co-infection
Because HIV infection can accelerate progression of liver disease,
treatment of chronic hepatitis B is generally recommended in patients with:
HBV replication ( >2000 IU/ml )
Liver inflammation signs ( elevated ALAT )
Fibrosis ( liver biopsy Metavir 2, or high elastography )
HIV / HBV Co-infection
Patients without ART indication:
use only substances without HIV activity (Peg Ifn, Adefovir,
Telbivudine)
avoid Tenofovir, 3TC and FTC
avoid also Entecavir ( induction of HIV reverse transcriptase
mutation M184V is possible )

Treatment of Hepatitis B in co-infected patients without ART indication
Treatment with pegylated interferon should be considered in special circumstances:
HIV treatment is not needed (high number of CD4 cells)
HBe Ag positive
HBsAg genotype A
Elevated ALAT
Low level of HBVDNA
( poor data and no encouraging results )
Treatment of Hepatitis B in co-infected patients without ART indication
Alternatively to peg. Interferon patients can be treated with HBV polymerase inhibitors:
Telbivudine Adefovir
Telbivudine was preferred by most experts more than Adefovir (greater antiviral efficacy)
But always check possibility of early HAART including Tenofovir + FTC or 3TC (it is preferred - EACS 2011)

Treatment Algorithm for HBV in HIV Co-infected Patients
HIV/HBV coinfection
CD4 >500/µl orNo indication of HAART
CD4 <500/µl or symptomatic HIV or cirrhosis
HBV Rx indicated (b)
No HBV Rx indicated (b)
Lamivudine experienced
Lamivudine naive
a) Early HAART including TDF + FTC/3TC®
b) PEG-INF if genotype A, high ALT, low HBV DNA
Monitor closelyHAART including TDF ® + 3TC or
FTC
Add or substitute one NRTI with TDF ® as part of HAART
Source: EACS 2011

HIV / HBV Coinfection - Treatment Algorithm for HBV in Patients with ART
Indication for HIV treatment
>2000 IU/µl HBV DNAPatients with
cirrhosis
Patients without HBV-associated 3TC resistance
Patients with HBV-associated 3TC
resistance
HAART regimen of choice (in case of HBV polymerase
inhibitor maintain full suppression)
HAART including TDF + 3TC or FTC
HAART including TDF + 3TC or FTC
Substitute one NRTI with Tenofovir or add
Tenofovir
In case of liver decompensation
refer for evaluation for LT
<2000 IU/µl HBV DNA
Source: EACS 2011

Treatment of HIV / HBV Co-infection
Gold standard: ART contains Tenofovir +Emtricitabine or Lamivudine
There is a problem in patients with virological failure to this first line ART: if these patients are switched from Tenofovir / Emtricitabine to another
drug, they will be vulnerable for hepatitis B liver inflammation flare
Possibility: Continue Tenofovir and add Zidovudine

HIV / HBV Co-infection - Conclusions
Best solution: Early start of ART
If ART is not indicated: Limited treatment options with only
Adefovir and Telbivudine
(Alternative Interferon)
Treatment of choice with patients on ART: Tenofovir
3TC or FTC mono-therapy should never be considered
HIV / HBV Co-infection - Conclusions
Treatment of Hepatitis B follows the same rules as HIV:
full suppression of viral replication to avoid the development of drug resistance
successful therapy leads to inhibition of inflammation activity and reversion of fibrosis
final goal: immune control of infection
HIV / HBV Co-infection
Don‘t forget:
HIV patients not infected with Hepatitis B should be
vaccinated against HBV
successful response in 33% of patients with CD4 > 300/µl
successful response in 80% of patients with CD4 > 500/µl
Rey D et al. Vaccine 18,116182000)



















