Information Bulletin Do Not Resuscitate Confirmation Form (DNRC)
Upload
brandon-blakeCategory
view
215download
2
BONE LOSS &TRANSPORT
Discussant R N Mbuva

Priorities in open fractures
• ABCDE (resuscitate)• Restore blood supply• Debride adequately• Restore soft tissue envelope integrity• Restore skeletal stability• Rehabilitate

Bone loss initial treatment
• Antibiotic treatment• Tetanus toxoid• Irrigation and debridement• External fixation• Antibiotic bead spacers-availability• Soft tissue coverage• Sterilization and re-implantation

Reconstruction modalities
• Over joint surface -osteochondral allograft -total joint or hemi- arthroplasty -arthrodesis

Diaphyseal defects
1.Autogenous bone graft •cancellous•cortical•vascularized2.Allogeneic bone graft•cancellous•cortical•Demineralized bone matrix

diaphysis
3.Distraction osteogenesis•multifocal shortening/ lengthening•bone transport
4.Salvage procedures•shortening•one bone forearm

Bone grafting
• Osteogenesis - bone formation 1. Survival and proliferation of graft cells 2. Osteoinduction - host mesenchymal
cells• Osteoconduction• Structural Support

Graft incorperation
1.Hemorrhage2.Inflammation3.Vascular invasion4.Osteoclastic resorbtion/ Osteoblastic apposition5.Remodelling and reorientation
N/B cancellous graft fastest limited by size of graft

PAPINEAU TECHNIQUE
• Direct open cancellous grafting of granulation bed
• typically large metaphyseal defect

allograft
• Slower than autograft
• Cortical strut graft-structural support -weakly osteogenic -revascularize slowly
Cancellous allograft-same as autograft-rhBMP

Vascularized graft
1Pedicled ipsilateral fibula2Free bone flap -fibula -iliac crest -rib•Structural support, rapid healing, independent of host bed•will hypertrophy

classification
Depends on the site of loss
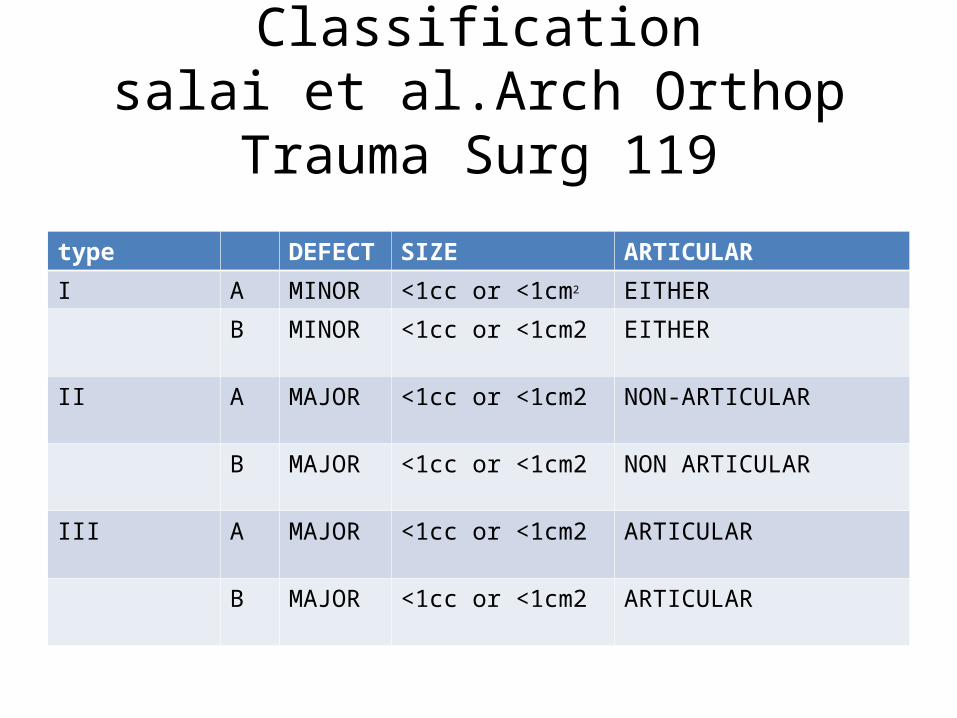
Classificationsalai et al.Arch Orthop Trauma Surg
119
type DEFECT SIZE ARTICULAR
I A MINOR <1cc or <1cm2 EITHER
B MINOR <1cc or <1cm2 EITHER
II A MAJOR <1cc or <1cm2 NON-ARTICULAR
B MAJOR <1cc or <1cm2 NON ARTICULAR
III A MAJOR <1cc or <1cm2 ARTICULAR
B MAJOR <1cc or <1cm2 ARTICULAR

classificationRobinson et al's classification of tibial bone loss.Grade Maximal bone loss (%) Maximum lengthof bone loss (cm)
1 Trivial Wedge < 25% 0
2 Minor Wedge 25% to 50% Wedge > 50% to < 100% < 2.5
3.Moderate Wedge > 50% but < 100% 2.5-10 Circumferential < 2.5
4.Severe Wedge > 50% but < 100% >10 Circumferential >2.5

Distraction osteogenesis
• Can be achieved using monoplanar or ring fixators

Ilizarov external fixator

• Hybrid(taylor) fixator

• Suv external fixator

• Joshi external stabilization system (JESS frame)

ilizarov
• Principles used in application -support- Control infection

Stages of ilizarov technique
1.fixator application and latency period 4-7 days2.distraction/compression1-4 or5/123.Period of immobility and fixation of the bone position-2x distraction4.Discontinuation of distraction-compression &frame dynamization-15-20/75.Period of immobilization-cast or brace-optional

CORTICOTOMY/COMPACTOTOMY
• Definitioni)corticotomy-cortical osteotomy with
transection of the bone cortex preserving periosteum and medullary canal
ii)latency-period of time after corticotomy and distraction

• iii)rate-1mm/day
• iv)rhythm-frequency of applied distraction 4xdaily
• v)Healing index-no. of months from operation to full unaided wt bearing

corticotomy
• Closed• Open
Ideal –long oblique -metaphyseal -without comminution -closed

corticotomy
• Level of corticotomy -avoid nutrient vessels metaphyseal segment suitable -local site: avoid old scars infection zone of sclerosis porosis cyst formation

corticotomy
monofocal• Lengthening upto 5cm• Bone fragment transport
upto 5-7cm• Stimulation of local blood
circulation and osteogenesis without significant lengthening
• Gradual correction of bone deformity
bifocal• 10-12cm• 10-16 cms
• Stimulation of osteogenesis in metabollic disease e.g pagets,OI,olliers disease
• Simultaneous lengthening at one level and correction of deformity at another level

Distraction
• Rate 1mm/day
• Indications for increased distraction 1.young patients 12-14yrs 2.premature bone consolidation 3.uncomplicated bone cut

• Indications for reduced distraction 1.severe pain after creating a gap of 3-4cm 2.neovascular problems 3.poor regeneration

Metaphyseal areas of corticotomy

Corticotomy in osteomyelitis

Distraction histogenesis of soft tissues
• 2 mechanisms -reorganization of collagen to stretch -neohistogenesis
Ilizarov -muscles respond by stretching without cell proliferation
Dyachkova-new schwann cells and active myelination seen in distraction

Docking
• Assesment – 1.when atleast three sites of contact 2.Callus is cylindrical 3.stress test doesn’t elicit pain

Docking
• Once edges dock healing improved by -bone grafting -tecerration -plug end into the medulla - compression -medical management-ultrasonic or pulsed
electromagnetic waves

Complications of ilizarov fixation
• Complications may arise -Preventable -Correctable -no interference with treatment

Classification of complications
1. General2. Specific3. inflammatory

general
a) immediate -neurologic compromise -vessel penetration -comminuted fracture of osteotomized bone -displacement of osteotomized fragment

General
b)Delayed -pain -compartment syndrome -muscle contracture -neurologic compromise -local edema -hypertension -joint subluxation

specific
a)Early complications -local skin tightness -local edema with circ,compromise -premature healing at corticotomy site -local pain with motion

specific
b)Delayed -break in wires -axial deviation of distracted fragments -joint stiffness -partial development of regenerate bone - delayed development of regenerate

specific
c) late iatrogenic complications -pseudoarthrosis -angulation of regenerate -fracture of regenerate -psychological incompatibility

inflammatory
• Any time in the course of treatment -pin tract infection -phlebitis -osteomyelitis

Conclusion
• Although the technique is labor intense and requires skill it is superior to monoplanar models in distraction osteogenesis