Boceprevir-based therapy adverse events : Case studies · 2014. 6. 20. · – W12 : HV RNA...
46
Boceprevir-based therapy adverse events : Case studies Marc Bourliere , MD International symposium Hôpital Saint Joseph 5-7 June 2014 Marseille, France St Petersburg
Transcript of Boceprevir-based therapy adverse events : Case studies · 2014. 6. 20. · – W12 : HV RNA...

Boceprevir-based therapy adverse events :
Case studies
Marc Bourliere , MD International symposium
Hôpital Saint Joseph 5-7 June 2014
Marseille, France St Petersburg

Disclosures
– Board member for : Schering-Plough, Merck, Janssen, Gilead, Boehringer Ingelheim, BMS, Novartis, Roche, Abbott, GSK, Vertex, Idenix
– Speaker for : Roche, Schering-Plough, Merck, Janssen, Gilead, BMS, Abbvie

Clinical Case
• Mr W 66 yo male, HCV cirrhosis genotype 1a, treatment failure in 2003, weight 85kg, BMI 29, type 2 diabetes
• Concomitant medication : Atorvastatin , metformin
• Prior treatment response : 2003 – Pegasys 180 µg / w + 1200mg/d Ribavirin
– W-4 : HCV RNA : 7,2 Log UI/ml
– W12 : HCV RNA positive (Cobas amplicor®)
– W24 : HCV RNA Positive : treatment was discontinued

Clinical Case
• No prior history of liver decompensation , no oesophageal varices
• Laboratory values : – AST : 90 IU/ml, ALT : 80 IU/ml, GGT: 75 IU/ml, AP: 60 IU/ml, Total
Bilirubin: 30 µmol/l , Albumin : 35g/l, PT: 85%, AFP : 50 ng/ml
– Platelets : 100,000, Hb : 11 g/dl WBC : 6000
– HCV RNA : 6.1 log10 IU/ml (MELD 9)
• FibroTest : A2F4, Fibroscan : 19 KpA IQR: 2 SR 85%
• Ultrasound : enlarge fatty liver , normal PV blood flow , splenomegaly, no ascites, no HCC

Do we need to treat this patients ?

Survival Outcomes in Patients With CHC and Advanced Hepatic Fibrosis With and Without SVR
Van der Meer AJ, et al. JAMA 2012

60
Cumulative development rate of HCC in HCV-infected patients treated with IFN
Retrospective cohort of 4302 Japanese patients treated with IFN-a followed for average 8.1 years
Cumulative incidence of HCC: 4.3% at 5 years, 10.5% at 10 years, 19.7% at 15 years
T2DM caused 1.73-fold increase in HCC
Arase Y et al, Hepatology 2013;57:964−973
0
10
20
30
40
50
0 10 20 30
Diabetes
Non-diabetes 24.5%
9.3%
HbA1c ≥7.0
HbA1c <7.0
27.9%
21%
60
0
10
20
30
40
50
0 10 20 30
p<0.001 p=0.015
Year of follow up Year of follow up
Cu
mu
lati
ve d
ev
elo
pm
en
t ra
te o
f H
CC
(%
)
Cu
mu
lati
ve d
ev
elo
pm
en
t ra
te o
f H
CC
(%
)
HCC, hepatocellular carcinoma; IFN, interferon;
SVR, sustained virological response; T2DM, type 2 diabetes
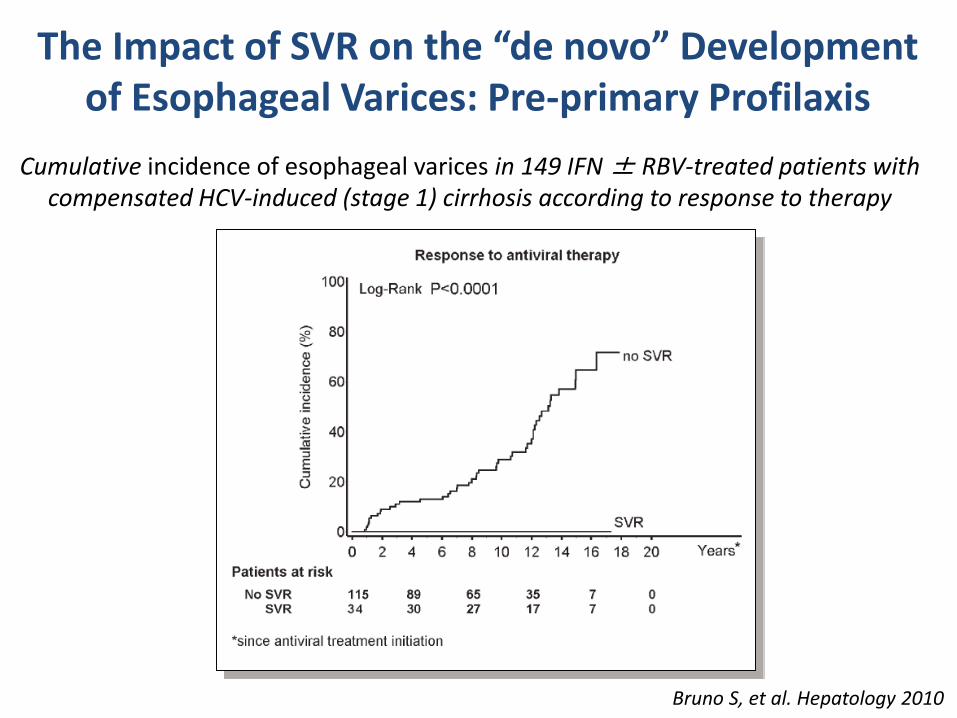
Cumulative incidence of esophageal varices in 149 IFN ± RBV-treated patients with compensated HCV-induced (stage 1) cirrhosis according to response to therapy
Bruno S, et al. Hepatology 2010
The Impact of SVR on the “de novo” Development of Esophageal Varices: Pre-primary Profilaxis

100
60
40
80
0 PRE-TREATMENT POST-TREATMENT
NU
MB
ER O
F PA
TIEN
TS (
%)
38 2 7
15
14 20
Cirrhosis Regression in 23 (61%) Patients
F4
F3
F2
F1
F0
D’Ambrosio R, et al. Hepatology 2012
Metavir
Rates of Cirrhosis Regression According to the METAVIR Scoring System
Post hoc analysis of the MIST study

Efficacy of triple therapy in treatment-experienced patients: clinical trials versus real life
Poordad F, et al. N Engl J Med 2011;364:1195–206 Calleja JL, et al. AASLD 2013. Abstract 1885
Fontaine H, et al. AFEF 2013
F0–4 F4 F0–4 F4 F0–4 F4
Clinical
EAP/cohort
RESPOND-2 CUPIC RESPOND-2 CUPIC PROVIDE CUPIC
BOC
F3/F4 F3/F4 F3/F4
Spanish
EAP
Spanish
EAP
Spanish
EAP
0
20
60
100
40
80
SV
R (
%)
Relapsers Partial responders Null responders
105 57 50 42 54 102 94 52 N=

Serious adverse events during triple therapy – clinical trials versus real life*
*Cross-comparison of studies cannot be carried out Proportion of cirrhotic patients in TARGET: TVR: 45%; BOC: 30% APRI: AST to platelet ratio index
1. Jacobson I, et al. N Engl J Med 2011;364:2405–16; 2. Poordad F, et al. N Engl J Med 2011;364:1195–206 3. Zeuzem S, et al. N Engl J Med 2011;364:417–28; 4. Bacon BR, et al. N Engl J Med 2011;364:1207–17
5. Fontaine H, et al. AFEF 2013; 6. Colombo M, et al. AASLD 2012. Abstract LB-15 7. Calleja JL, et al. AASLD 2013. Abstract 1885; 8. Di Bisceglie AM, et al. AASLD 2013. Abstract 41
9. Mauss S, et al. AASLD 2013. Abstract 1856; 10. Berg, et al. AASLD 2013. Abstract 1900
ADVANCE1 SPRINT-22 REALIZE3
Registration trials
RESPOND-24
Oc
cu
rre
nc
e o
f S
AE
s (
%)
CUPIC5
F0–4 F4 F3/F4 F0–F4 APRI >1.5
EAP and post-marketing cohorts
F0–4
TVR-EAP6 TARGET8 PAN9 TEPS10
Telaprevir
Boceprevir
Combined
0
20
40
60
9 12
54
12 12 14
12
16 18
44
F3/F4
35
BOC-EAP
(Spanish
patients)7

Adverse events with Boceprevir in phase II / III studies
Manns M et al. Liver Int 2014; 34: 707-719
PR BOC/PR

Patients, n
(% patients with at least one event)
Telaprevir n = 299 Boceprevir n=212
Serious adverse events (SAEs)* 161 patients
(53.8%)
94 patients
(44.3%)
Premature discontinuation /
due to SAEs
134 (44.8%) /
71 (23.8%)
95 (44.8%)/
37 (17.5%)
Death 8 (2.7 %) 3 (1.4%)
Infection (Grade 3/4) 29 (9.7 %) 8 (3.8%)
Hepatic decompensation
(Grade 3/4)
14 (4.7 %) 9 (4.2%)
Anemia (Grade ¾ : Hb < 8 g/dL) 38 (12.7 %) 19 (9%)
Rash (grade 3/SCAR) 16 (5.3 %)/ 0 (0 %) 2 (0.9%)/0
EPO use /
blood transfusion / RBV red or
disc
169 (57 %) /
53 (18 %) / 83 (28%)
119 (56.1%) /
25 (11.8%)/ 50(24%)
GCSF use 2 (0.7 %) 6 (2.8%)
* SAEs in patients; SCAR: severe cutaneous adverse reaction
SVR12 safety findings
Fontaine H , France, AFEF 2013,

SAE according to age
Hézode C, et al. AASLD 2013
Liver
Décompen
%
pati
en
ts
Grade 3/4
infection
0
5
10
15
20
2
4
9
12
4
6
<65 years
≥65 years
5/221 3/78 20/221 9/78 9/221 5/78
p=NS p=NS p=NS
Death
TELAPREVIR
Liver
Décompen
%
pati
en
ts
Grade 3/4
infection
0
5
10
15
20
2
0 3
7
2
14
<65 years
≥65 years
3/168 0/44 5/168 3/44 3/168 6/44
p=NS p=NS P=0.003
Death
BOCEPREVIR
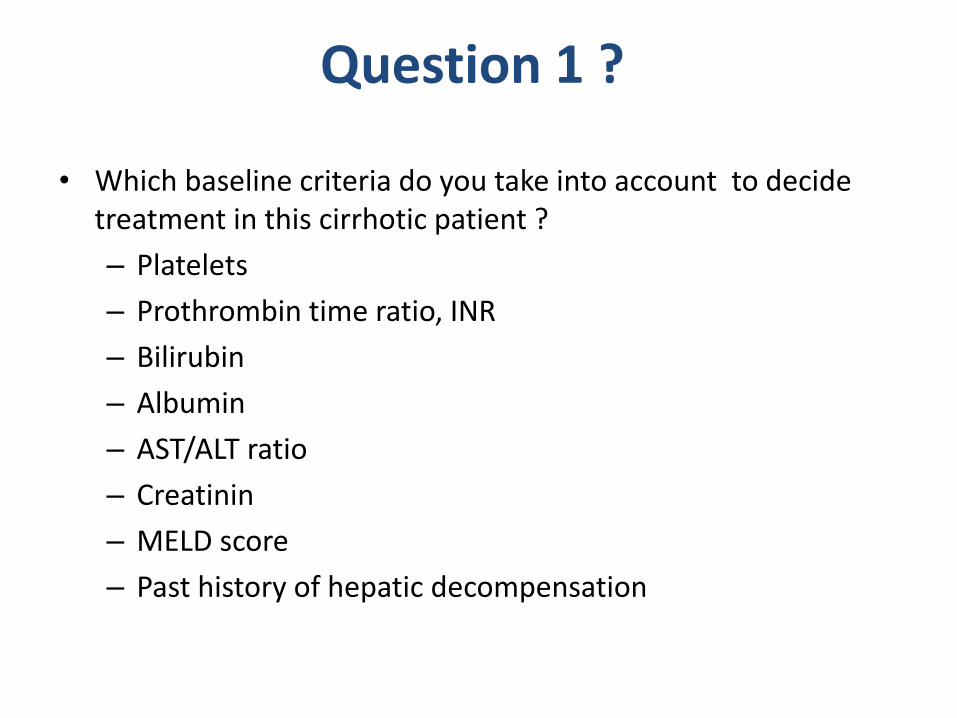
Question 1 ?
• Which baseline criteria do you take into account to decide treatment in this cirrhotic patient ?
– Platelets
– Prothrombin time ratio, INR
– Bilirubin
– Albumin
– AST/ALT ratio
– Creatinin
– MELD score
– Past history of hepatic decompensation
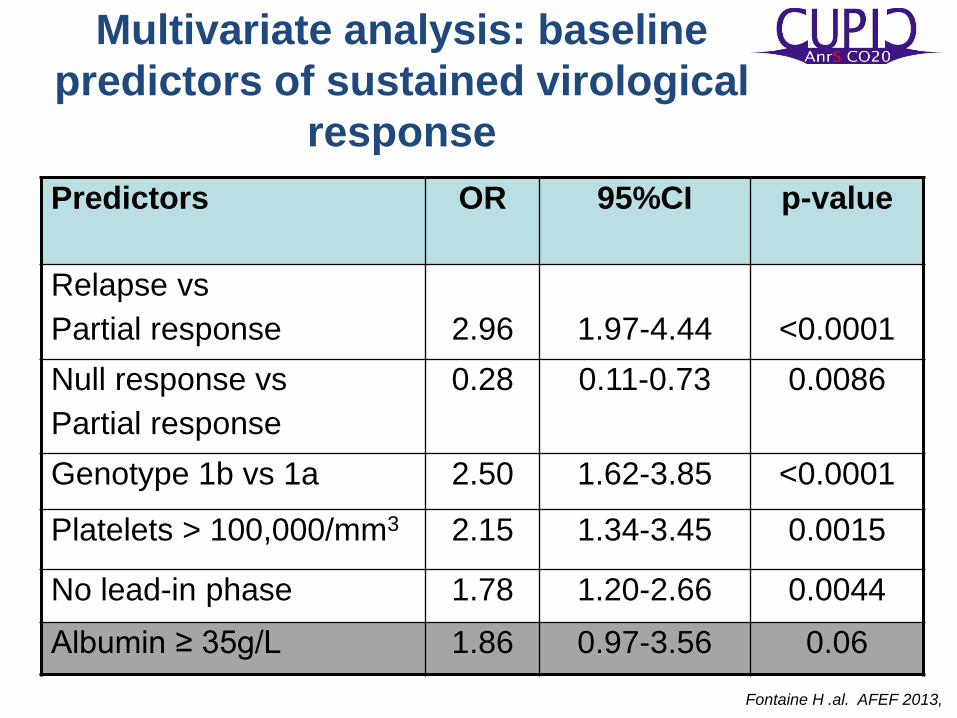
Multivariate analysis: baseline
predictors of sustained virological
response
Predictors
OR 95%CI p-value
Relapse vs
Partial response
2.96
1.97-4.44
<0.0001
Null response vs
Partial response
0.28 0.11-0.73 0.0086
Genotype 1b vs 1a 2.50 1.62-3.85 <0.0001
Platelets > 100,000/mm3 2.15 1.34-3.45 0.0015
No lead-in phase 1.78 1.20-2.66 0.0044
Albumin ≥ 35g/L 1.86 0.97-3.56 0.06
Fontaine H .al. AFEF 2013,

Sultanik P et al. EASL 2013
Baseline ApolipoproteinH (ApoH) is a predictor of early virologic response to triple therapy (ANRS-CO20-CUPIC)

Biomarkers in Hepatitis C – DAA1
CUPIC – ANRS CO20 plasma biomarkers
0
2
4
6
8
10
- Log
10 (
p)
AFP
TTR
apoH
apoCIMCSF
IL6rb
EVR
SVR
Cyt
okines
Chem
okines
Gro
wth
fact
ors
Tissu
e re
model
ing p
rote
ins
Apolip
oprote
ins
Met
abolic p
rote
ins
Horm
ones
Can
cer m
arke
rs
Oth
er p
lasm
a pro
tein
s
0.0 0.2 0.4 0.6 0.8 1.0 0.0
0.2
0.4
0.6
0.8
1.0
AUC = 0.77
Se = 66%, Sp = 72%
PPV = 68%, NPV =70%
ROC curve of apoH-based model for SVR
High basal Apolipoprotein H is associated with SVR
Sultanik & al., submitted

CUPIC: identifying high-risk patients
• CUPIC enrolled treatment-experienced patients with compensated cirrhosis and notable risk factors
– Patients achieved high rates of SVR with TVR or BOC in combination with PR
• Patients with cirrhosis who present with significant risk factors require careful monitoring when being treated with PR
Fontaine H, et al. AFEF 2013
Platelets count
≤100,000/mm3
Platelets count
>100,000/mm3
Albumin
<35 g/L
N
Complications, n (%)
SVR12, n (%)
37
19 (51.4%)
10 (27.0%)
31
5 (16.1%)
8 (29.0%)
Albumin
≥35 g/L
N
Complications, n (%)
SVR12, n (%)
74
9 (12.2%)
27 (36.5%)
306
19 (6.2%)
168 (54.9%)

CUPIC data confirmed in ongoing studies
Mauss S, et al. AASLD 2013. Abstract 1856
The risk of SAEs was 28.6% in patients with platelet count <100 x109/L and serum albumin <35 g/L, thus
confirming the findings from the CUPIC study
SAEs by platelets and albumin at baseline
This evaluation is part of a large,
ongoing German multi-centre
observational study including adults
with detectable HCV RNA
<100
<35
<100
≥35
≥100
≥35
≥100
<35
X109/L
g/L
Platelets:
Albumin:
SA
Es (
%)
4.8%
(n=1/21)
0%
(n=0/7)
8.5%
(n=4/47)
28.6%
(n=2/7)

HCV-TARGET: Risk Factors for Poor
Outcomes in PI-Treated Pts
• Risk factors for decompensation
among cirrhotic patients during
PI therapy identified[1]
• Pts with history of
decompensation at highest risk
for SAEs with PIs[2]
1. Afdhal N, et al. AASLD 2013. Abstract 1865. 2. Gordon S, et al. AASLD 2013. Abstract 1866.
Pa
tie
nts
(%
)
Baseline Characteristic
Odds Ratio Minimally Adjusted Estimates
P Value
CrCl (mL/min) 0.99 .03
Albumin (g/dL) 0.30 < .01
HCV RNA (log IU/mL)
0.76 < .01
Bilirubin (log mg/dL)
2.93 .02
100
80
60
40
20
0 SAE Decomp
AE Decomp
SAE Completed Treatment
Noncirrhotics (n = 639) Cirrhotics w/prior decomp’n (n = 49) Cirrhotics w/o prior decomp’n (n = 412)
10
33
12
1
24
7 0
10 1
71
43
55

Clinical Case
● June 2012: pegIFN /RBV 1200 mg/d was initiated ● HCV RNA : 1.5 106 IU/ml Hb: 12g/dl
● W2 : Hb : 11g/dl
● W4 : Hb : 10.1 g/dl, Albumin : 35 g/l, Bilirubin : 35 μmol/l , HCV RNA : 5 104 IU/ml

0
10
20
30
40
50
60
70
80
90
100
125/198 30/101
RVR
NO
RVR
63%
40%
P < 0.001
TELAPREVIR
0
10
20
30
40
50
60
70
80
90
100
62/99 29/113
HCV RNA
Decline
≥ 1log
W4
RVR
W8
63%
26%
BOCEPREVIR
Fontaine H , France, AFEF 2013,
SVR12 according to on-treatment response
HCV RNA
Decline
< 1log
W4
NO
RVR
W8
HCV RNA
Decline
< 3log
W8
58/81 33/131
72%
25%
4/63
6%
P < 0.001 P < 0.001

Question 2 ?
• How do you manage anemia at this stage ?
– EPO use
– Ribavirin dose reduction
– Both EPO and RBV dose reduction
– Peg-IFN dose reduction
– Nothing
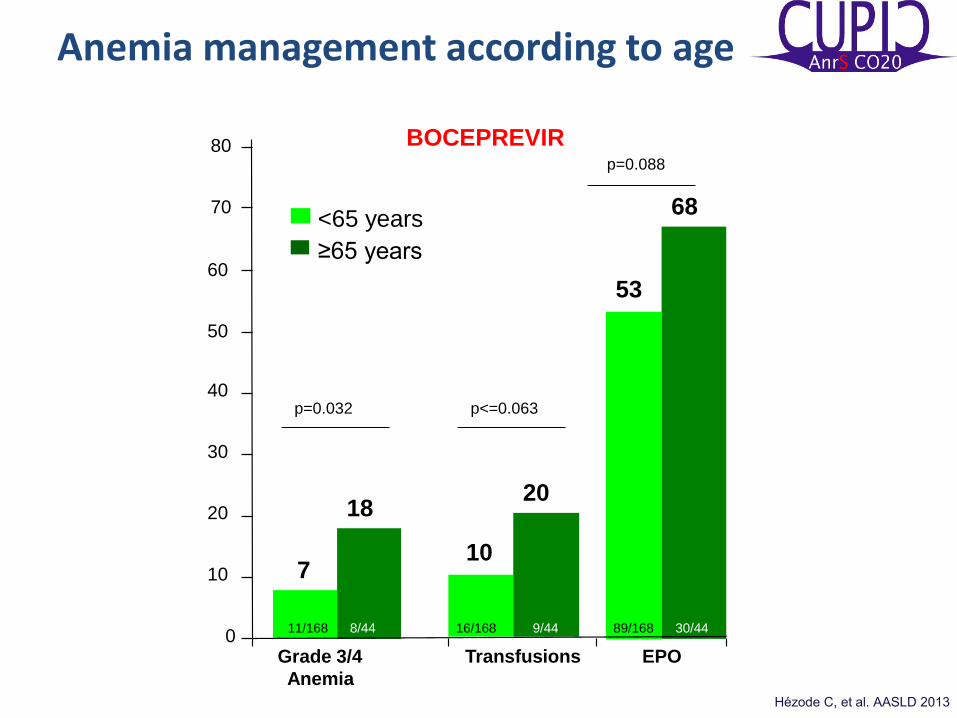
Anemia management according to age
Hézode C, et al. AASLD 2013
BOCEPREVIR
0
10
20
30
40
50
60
<65 years
≥65 years
7
18
10
20
53
68
p=0.032 p<=0.063
p=0.088
Grade 3/4 Transfusions EPO
Anemia
70
80
11/168 8/44 16/168 9/44 89/168 30/44

SVR according to time of first RBV dose reduction during first 4 weeks of treatment and HCV RNA status
Treatment-naïve patients in ADVANCE/ILLUMINATE (N=885) Sulkowski MS, et al. J Hepatol 2012;56(Suppl. 2):S459–60
Pati
en
ts w
ith
SV
R (
%)
Undetectable HCV RNA Detectable HCV RNA
40
45
347
405
120
176
168
259
Small sample sizes among previously treated patients limit interpretation of data in REALIZE,
however similar trends were observed

Boceprevir: similar SVR when RBV dose modification and EPO are used to manage anemia
178
249
178
251
Treatment-naïve G1 patients (n=687) received BOC-based therapy. Overall, 500
patients developed anemia (Hb ≤10 g/dL or were expected to reach that nadir
before next visit) and were randomized to have anemia managed with either
EPO (40 000 units/week SC), or RBV dose reduction (by 200–400 mg/day).
Transfusion in patients with Hb ≤8.5 g/dL was allowed to prevent study
discontinuation Poordad F, et al. EASL 2012. Abstract 1419

Genotype 1 cirrhosis and boceprevir : RBV dose reduction or EPO use ?
SVR according to
RBV DR or EPO use
RBV DR : RBV dose reduction
SV
R (
%)
SVR according to the need
of single or double strategy
57 64
RBV
DR
13/23
EPO
16/25 S
VR
(%
)
52
71
14/27
Do
ub
le
str
ate
gy
15/21
Sin
gle
str
ate
gy
Lawitz E, Etats-Unis, AASLD 2012, Abs. 50 actualisé

Predictors of severe anaemia < 8 g/dl or BT
Multivariate analysis: baseline factors related to anaemia<8g/dl or blood transfusion
Hezode et al AASLD 2012 Abs 51
Predictors OR 95%CI p-value
Gender: Female 2.19 1.11-4.33 0.023
No lead-in phase 2.25 1.15-4.39 0.018
Age ≥65 years 3.04 1.54-6.02 0.0014
Hemoglobin level ≤12 g/dL for female
≤13 g/dL for male
5.30 2.49-11.25 <0.0001

Clinical Case
● We reduced RBV dose down to 1000 mg/d add EPO W6: Hb : 10.5 g/dl , HCV RNA : 500 IU/mL
● W8: Hb : 9.5 g/dl, HCV RNA <12 IU/mL, albumin : 34 g/l , bilirubin: 35 μmol/l. Asthenia and anaemia were managed by EPO ( neorecormon 30.000 UI/w) and RBV dose reduction down to 800 mg/d

0
10
20
30
40
50
60
70
80
90
100
125/198 30/101
RVR
NO
RVR
63%
40%
P < 0.001
TELAPREVIR
0
10
20
30
40
50
60
70
80
90
100
62/99 29/113
HCV RNA
Decline
≥ 1log
W4
RVR
W8
63%
26%
BOCEPREVIR
Fontaine H , France, AFEF 2013,
SVR12 according to on-treatment response
HCV RNA
Decline
< 1log
W4
NO
RVR
W8
HCV RNA
Decline
< 3log
W8
58/81 33/131
72%
25%
4/63
6%
P < 0.001 P < 0.001

• Guidelines recommend BOC-based triple therapy
EASL guidelines: BOC treatment algorithm
*In the BOC SmPC label there is no response-guided therapy for treatment-experienced patients and patients with cirrhosis ER: early response; LR: late response EASL Clinical Practice Guidelines. J Hepatol 2014;60:392420
Detected LR
Undetected
Detected
<100 IU/mL
Detected
>100 IU/mL
Undetected
Undetected
Undetected
Detected
28 weeks of
therapy*
0 4 8 12 24 28
48 weeks of
therapy
Undetected
ER
PR PR + BOC
Week
HCV
RNA
Stop Stop

Interest of RGT for reducing adverse events
Manns M et al. Liver Int 2014; 34: 707-719

Clinical Case
● W12: Hb : 10.7g/dl , HCV RNA undetectable , albumin : 32 g/l , bilirubin: 37 μmol/l.
● W24 : Hb : 11g/dl, platelet count 60,000/μl, HCV RNA undetectable , albumin : 31 g/l, bilirubin 39 μmol/l.
● W36 : Hb : 10,7g/dl, platelet count 55,000/μl, HCV RNA undetectable , albumin : 30 g/l, bilirubin 39 μmol/l.
● W40 : Ascites, spontaneous bacterial peritonitis (caused by E. coli) and deep asthenia resulted in cessation of treatment
Clinical case
• SBP was cured by cefotaxim
• Ascites resolved with albumin and diuretic
• Patient did not relapsed
• MELD increase to 12
• Liver transplant assessment was done
Should we use prophylactic antibiotic in this setting ?

HCV decompensated cirrhosis treatment with PEG-
IFN / RBV : Usefulness of norfloxacin prophylaxis
Carrion JA et al. J Hepatol 2009; 50: 719-728.
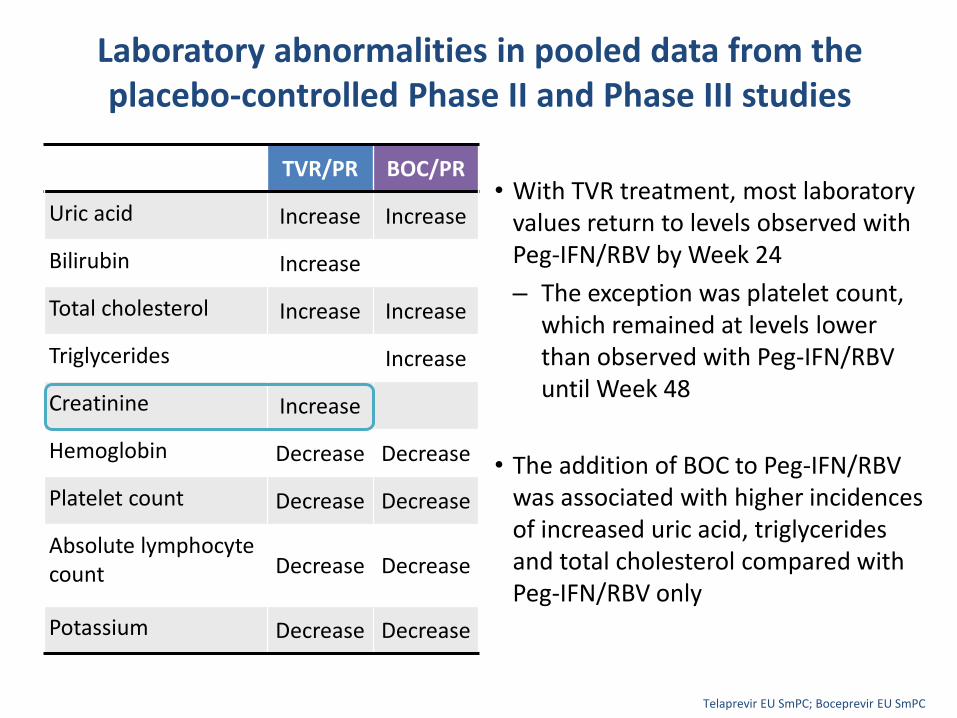
Laboratory abnormalities in pooled data from the placebo-controlled Phase II and Phase III studies
• With TVR treatment, most laboratory values return to levels observed with Peg-IFN/RBV by Week 24
– The exception was platelet count, which remained at levels lower than observed with Peg-IFN/RBV until Week 48
• The addition of BOC to Peg-IFN/RBV was associated with higher incidences of increased uric acid, triglycerides and total cholesterol compared with Peg-IFN/RBV only
Telaprevir EU SmPC; Boceprevir EU SmPC
TVR/PR BOC/PR
Uric acid Increase Increase
Bilirubin Increase
Total cholesterol Increase Increase
Triglycerides Increase
Creatinine Increase
Hemoglobin Decrease Decrease
Platelet count Decrease Decrease
Absolute lymphocyte count Decrease Decrease
Potassium Decrease Decrease

PAN cohort: decrease of eGFR in patients with >60 mL/min at baseline to ≤60 mL/min after 12 weeks
• Increased serum creatinine levels were observed in registration trials
eGFR: estimated glomerular filtration rate Telaprevir SmPC
Mauss S, et al. Hepatology 2014;59:46–8
Risk factors: age, arterial hypertension, diabetes mellitus, higher serum creatinine at baseline and triple therapy
TVR/PR BOC/PR PR
38/575 10/211 1/109
Pa
tie
nts
(%
)

Key learnings: a summary
• Anemia was commonly seen in real-life cohorts and should be managed early
with RBV dose reduction
– Does not impact SVR with TVR or BOC
– During TVR dosing, the timing of RBV dose reduction does not appear to impact SVR1
Older patients can still be effectively treated with TVR and BOC but are at greater
risk of anemia, rash and SAEs2,3
• Patients with risk factors for renal impairment receiving triple therapy are at greater risk of impaired renal function than patients receiving PR. Changes to renal function are typically temporary4
1. Bourliere M, et al. AASLD 2013. Abstract 1895; 2. Moreno C, et al. AASLD 1911 3. Hezode C, et al. AASLD 2013. Abstract 1845; 4. Mauss S, Hepatology 2014;59:46–8
Predictors of anemia and anemia management
Outcomes and management in elderly patients
Creatinine fluctuations on triple therapy

Telaprevir:1 Boceprevir:2
Counselling should be provided on potential adverse events that may occur
1. Telaprevir EU SmPC; 2. Boceprevir EU SmPC
Telaprevir:1 Boceprevir:2
Anemia
Nausea
Rash, pruritus
Anorectal signs/symptoms
Diarrhea
Anemia
Nausea
Dysgeusia
Neutropenia
Headache
Ribavirin doses should be reduced early to minimise the impact of anemia

Child-Pugh: A B C
Number of patients
Efficacy of treatment
Prevalence and severity of side effects
Efficacy of antiviral therapy and side effects in relation to severity of disease
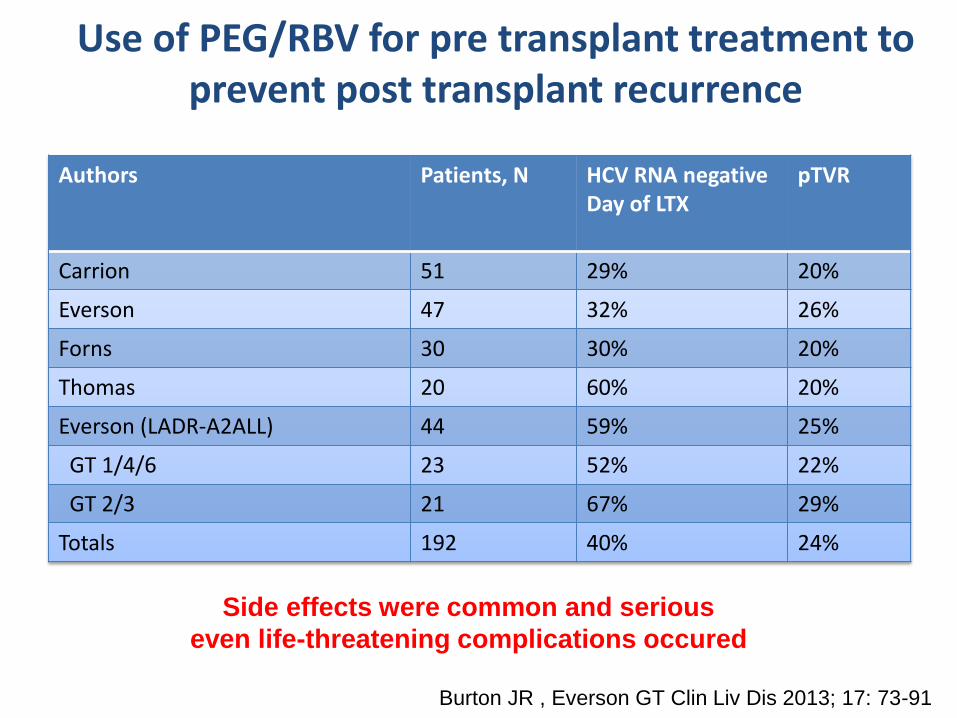
Use of PEG/RBV for pre transplant treatment to prevent post transplant recurrence
Authors Patients, N HCV RNA negative Day of LTX
pTVR
Carrion 51 29% 20%
Everson 47 32% 26%
Forns 30 30% 20%
Thomas 20 60% 20%
Everson (LADR-A2ALL) 44 59% 25%
GT 1/4/6 23 52% 22%
GT 2/3 21 67% 29%
Totals 192 40% 24%
Burton JR , Everson GT Clin Liv Dis 2013; 17: 73-91
Side effects were common and serious
even life-threatening complications occured

Likelihood of achieving pTVR is related to treatment duration
Everson GT, et al. Hepatology 2012

Protease-Inhibitor (PI) Triple Therapy (TT) in Cirrhotics with Compensated and Mildly Decompensated Disease:
Implications for Wait-Listed Patients
45 G1 HCV Cirrhotics
(7 wait-listed for OLT)
PR + BOC (24%)
PR + TPV (76%)
On-treatment VR:
≈40%
RVR associated with:
•Prev. Naive
•Prev. Relapser
•LVL
PI type: no prediction of
VR
Saxena V, et al. AASLD 2012

Summary and conclusions • DAAs have been shown to significantly improve SVR rates,
however there are patient management considerations
– AEs such as anemia and rash are common with triple therapy
– Effective management of these events is key to treatment success
• Early recognition of AEs through clinical monitoring is an important component of patient management
• The main components for these achievements are
– Doctor’s skill deriving from training and practice
– Patient’s awareness from practical guidance and counselling

Conclusion
• Cirrhotic patients are the most in needed for HCV treatment.
• Child Pugh A patients should be treated
• More advance cirrhosis should be treated with caution on a case by case basis
• Patients with platelets < 100,000 and albumin< 35g/l should not be treated