Effects of clonidine, prazosin and phentolamine on heart rate and ...
Upload
philip-morrisCategory
view
215download
0
Psychoneuroendocrinology 29 (2004) 269–278www.elsevier.com/locate/psyneuen
Blunted growth hormone response to clonidinein post-traumatic stress disorder
Philip Morris a,∗, Malcolm Hopwoodb, Kay Maguirec,Trevor Normanb, Isaac Schweitzerc
a Department of Psychiatry, University of Queensland, Brisbane, Australiab Department of Psychiatry, The Austin and Repatriation Medical Centre, University of Melbourne,
Heidelberg, Australiac The Melbourne Clinic, Department of Psychiatry, University of Melbourne, Richmond, Australia
Received 9 July 2002; received in revised form 9 September 2002; accepted 22 January 2003
Abstract
Hyperactivity of the sympathetic and noradrenergic systems is thought to be a feature ofpost-traumatic stress disorder (PTSD). Assessment of noradrenergic receptor function can beundertaken by measuring the growth hormone (GH) response to theα2-agonist clonidine. Theaim of this study was to examine whether subjects with combat-related PTSD (with or withoutco-morbid depression) have a blunted growth hormone response to clonidine, compared to acombat-exposed control group.
Twenty-three Vietnam veterans suffering from PTSD alone, 27 suffering from PTSD andco-morbid depression, and 32 veteran controls with no psychiatric illness were administered1.5 µg/kg clonidine i.v. Plasma growth hormone was measured every 20 min for 120 min.
The growth hormone response to clonidine was significantly blunted in the non-depressedPTSD group compared to both the depressed PTSD group and the control group as measuredby peak growth hormone, delta growth hormone and AUC growth hormone. Subjects withPTSD and no co-morbid depressive illness show a blunted growth hormone response to clonid-ine. This suggests that post-synapticα2-receptors are subsensitive. This finding is consistentwith other studies showing increased noradrenergic activity in PTSD. 2003 Elsevier Ltd. All rights reserved.
∗ Corresponding author. Address: 16 Riverbank Court, Ashmore, Qld 4214, Australia. Tel./fax:+61-7-55974011.
E-mail address: [email protected] (P. Morris).
0306-4530/$ - see front matter 2003 Elsevier Ltd. All rights reserved.doi:10.1016/S0306-4530(03)00027-1

270 P. Morris et al. / Psychoneuroendocrinology 29 (2004) 269–278
Keywords: Post-traumatic stress disorder; Depression; Growth hormone; Clonidine; Noradrenaline; Neuro-endocrine
1. Introduction
Historically there has been interest in the role of sympathetic nervous systemactivity in psychological disturbance following trauma. Early descriptions of syn-dromes analogous to what we now consider as post-traumatic stress disorder (PTSD)featured symptoms related to autonomic reactivity, including palpitations, fatigue,anxiety and an increased startle response which often generalised beyond directreminders of the traumatic experience.
More recently, investigators have made biological measurements of sympatheticactivity in patient groups with combat-related PTSD. The majority of studies havefocussed on indirect measures. Studies of 24-h urinary noradrenaline excretion haveyielded conflicting results. Some studies find increased noradrenergic levels (Kostenet al., 1987; Yehuda et al., 1992), while others find no difference between PTSDsubjects and controls (Pitman and Orr, 1990; Mellman et al., 1995). Plasma noradren-aline levels in PTSD subjects were not different to controls in two studies (McFallet al., 1990; Blanchard et al., 1991), but were increased in PTSD in one report,although only in patients without co-morbid secondary depression (Yehuda et al.,1998). An investigation of peripheral α2-adrenoceptors found a reduced number onplatelets taken from PTSD patients compared to controls (Perry et al., 1987), a find-ing consistent with increased noradrenergic activity. In the only direct study of cen-tral noradrenaline activity, serial CSF noradrenaline levels in PTSD subjects whowere not clinically depressed at the time, were found to be significantly increasedwhen compared to healthy controls (Geracioti et al., 2001).
Studies of central noradrenergic function using pharmacological probes(desipramine, clonidine and yohimbine) possessing α2-adrenergic receptor activityhave been reported. Two studies (Dinan et al., 1990; Yatham et al., 1996) examinedcentral α2-adrenoceptor function in non-combat PTSD using the growth hormone(GH) response to desipramine challenge. These studies found no significant differ-ence in growth hormone responses between the PTSD patients and age and sexmatched controls. There has been one single case report using clonidine, an α2-agonist, in PTSD (Hansenne et al., 1991). A clonidine growth hormone challengetest prior to psychiatric admission showed a blunted response that normalised aftersuccessful treatment of the patient with cognitive behavioural therapy.
In a series of investigations using yohimbine, an α2-antagonist, in combat-relatedPTSD, Southwick and colleagues demonstrated greater behavioural, cardiovascularand biochemical responses to yohimbine in PTSD subjects compared with controls(Southwick et al., 1993, 1997). In particular, Southwick et al. (1993) found a signifi-cantly greater increase in plasma levels of the noradrenaline metabolite, methoxy-hydroxy-phenyl-glycol (MHPG) in response to yohimbine challenge in Vietnam vet-erans with PTSD. Bremner et al. (1997), using positron emission tomography (PET),

271P. Morris et al. / Psychoneuroendocrinology 29 (2004) 269–278
found a significant decrease in cerebral metabolism in prefrontal, temporal, parietaland orbitofrontal cortices following yohimbine administration in PTSD patients com-pared to healthy subjects, a finding consistent with enhanced yohimbine-stimulatednoradrenaline release in the brain in PTSD. Another study from the same group(Rasmussen et al., 2000) found low baseline and blunted yohimbine-stimulatedplasma neuropeptide Y in combat-exposed PTSD subjects in comparison with heal-thy controls. Neuropeptide Y is co-localised with noradrenaline in most sympatheticnerves and in the locus coeruleus. The authors suggest that this neuropeptide maymediate, in part, the hyperreactivity in the noradrenergic system observed in studiesof combat-related PTSD.
Overall, the literature concerning noradrenergic function in PTSD is suggestiveof an increased reactivity of the noradrenergic system (Southwick et al., 1999). Notall studies support this hypothesis, but this may be in part related to a failure tocontrol for co-morbid depressive illness. Some studies indicate whether PTSDpatients have concurrent depressive diagnoses or symptoms, but in all but one study(Yehuda et al., 1998) the depressed subgroup has not been analysed separately. Inthe study by Yehuda et al. (1998), only the non-depressed PTSD subjects hadincreased plasma noradrenaline levels compared to controls and depressed PTSDsubjects.
In the present study, we evaluated central noradrenergic function in combat-relatedPTSD using the clonidine growth hormone challenge test. Subjects diagnosed withPTSD were also assessed for the presence of current depressive disorder. Since over-activity of the sympathetic nervous system and increased noradrenergic reactivityappear to be a feature of PTSD, we anticipated that patients with PTSD would showde-sensitised or down-regulated central noradrenergic receptors. Thus, we hypoth-esised that patients with PTSD would show a significantly blunted growth hormoneresponse to the α2-adrenergic agonist clonidine compared with controls.
2. Methods
2.1. Patient subjects
Male combat-exposed Vietnam war veterans were recruited from the AustinRepatriation Medical Centre Veterans’ Psychiatry Unit, the Vietnam Veterans’Association and the Returned and Servicemen’s League. Patient subjects were eli-gible if they had a current diagnosis of PTSD subsequent to war service and signifi-cant PTSD symptomatology (see below). Patient subjects were excluded if they had(i) other current psychiatric disorders other than major depression, (ii) acute or seri-ous medical illness (e.g. endocrine, cardiac, hepatic, renal or neurological disease),(iii) recent substantial changes in weight (i.e. �3 kg), or (iv) taken psychotropicmedications or cardiovascular medications (beta-blockers, anti-hypertensives) within2 weeks prior to testing.

272 P. Morris et al. / Psychoneuroendocrinology 29 (2004) 269–278
2.2. Control subjects
A control group of male combat veterans was recruited from the Vietnam Vet-erans’ Association and the Returned and Servicemen’s League. Control subjects werehealthy and did not suffer from psychiatric disorder.
Approval for the study was obtained from the Austin Repatriation Medical CentreHuman Ethics committee. All subjects provided written informed consent.
2.3. Clinical evaluation
All potential subjects underwent a structured interview with the ComprehensiveInternational Diagnostic Interview (CIDI, WHO, 1987). Details of demographic,marital, employment and military history were recorded. The diagnosis of PTSD wasmade on the basis of DSM III-R (APA, 1987) criteria for PTSD as identified byDavidson’s Interview for PTSD (Davidson et al., 1989) and the diagnosis of majordepression was made using DSM IIIR criteria and the CIDI. Self-reported PTSDsymptoms were assessed using the Impact of Events Scale (IES, Horowitz et al.,1979) and only patients with a score �30 were considered to have significant PTSDsymptomatology and included in the study (Aardal-Eriksson et al., 1999; Neal et al.,1994). As the IES version used did not contain a specific scale of arousal symptoms,we also assessed anxiety symptoms using the Hamilton Rating Scale for Anxiety(HARS, Hamilton, 1959). Depressive symptoms were assessed using the 21-itemHamilton Depression Scale (HDRS, Hamilton, 1960). PTSD subjects were dividedinto ‘depressed’ and ‘non-depressed’ groups based on the presence of a co-morbiddiagnosis of major depression and a HDRS score of �18.
Subjects were administered the Combat Exposure Scale (CES, Keane et al., 1989)as a measure of the level of wartime stressors experienced by combatants. For arating of cognitive function, subjects were administered the Mini Mental State Exam-ination (MMSE, Folstein et al., 1975).
2.4. Clonidine growth hormone challenge test
At 8:30 a.m., after an overnight fast, an intravenous line was inserted into a fore-arm vein of the reclining subject. Two 5 ml blood samples for growth hormoneestimation were collected 30 and 15 min prior to the clonidine infusion at 9:00a.m. Clonidine (1.5 µg/kg) dissolved in 10 ml of normal saline was administeredintravenously over a 10-min period. Subsequent blood samples were drawn every20 min for 120 min. Blood samples were centrifuged and stored at �20 °C untilassayed for plasma growth hormone by radioimmunoassay. A commercially availablekit (Orion Diagnostica, Finland) was used for the determination of growth hormoneconcentrations. The kit was a direct assay with a sensitivity of 0.6 mI U/l and anintra-assay precision (CV%) of 6.1% at 4.08 mI U/l and an intra-assay precision(CV%) of 13.7% at 2.19 mI U/l.

273P. Morris et al. / Psychoneuroendocrinology 29 (2004) 269–278
2.5. Data analysis
Neuroendocrine parameters measured included (i) the pre-dose (baseline) growthhormone (GH) concentration (mean of the two samples taken prior to administrationof clonidine), (ii) peak growth hormone concentration, (iii) time to reach the peak,and (iv) delta growth hormone (the change in growth hormone defined as the peakgrowth hormone concentration minus the pre-dose concentration). Area under thegrowth hormone versus time curve (AUC GH) was calculated using the trapezoidrule (summing areas between each time point) for each subject from the start of theinfusion to the time point where the growth hormone concentration returned to thepre-dose concentration. This takes into account diurnal rhythms. As the growth hor-mone variables were not normally distributed, they were log transformed before stat-istical testing. Statistical analysis included analysis of variance (one-way ANOVAand ANCOVA) with post hoc Student–Newman–Keuls (SNK) analysis.
3. Results
Eighty-two male combat-exposed subjects met the inclusion criteria for the study.Fifty subjects had a diagnosis of PTSD. Of this group, 23 were not depressed and27 were depressed. Thirty-two subjects were non-psychiatric controls. The means(±S.D.) of each group for age, body mass index (BMI), and clinical characteristicsare presented in Table 1.
There were no significant differences in age, BMI or cognitive function betweengroups. There were differences across groups for CES ratings. The controls demon-strated significantly less combat exposure than both of the PTSD groups (Table 1).There were differences between groups for IES scores. As expected, the controlsdemonstrated significantly fewer PTSD symptoms than both of the PTSD groups.
Table 1Mean (±S.D.), age, BMI and clinical rating scores for the three groups
Controls PTSD–non-depressed PTSD–depressed p-Value(N = 32) (N = 23) (N = 27)
Age (years) 48.2 ± 3.2 50.0 ± 3.9 48.5 ± 2.8 NSBMI 26.2 ± 4.2 24.2 ± 3.1 26.0 ± 4.2 NSMMSE 28.9 ± 1.1 28.6 ± 1.4 28.5 ± 1.3 NSCES 13.6 ± 9.9 24.7 ± 7.0 19.6 ± 9.9 0.0001a
IES 9.9 ± 10.4 46.9 ± 11.7 48.0 ± 8.8 �0.0001b
HARS 7.5 ± 6.3 17.7 ± 6.4 25.3 ± 8.2 �0.0001c
HDRS 6.7 ± 5.1 13.4 ± 3.4 25.4 ± 4.8 �0.0001d
a p � 0.001 controls vs. PTSD–non-depressed, p � 0.05 controls vs. PTSD–depressed.b p � 0.001 controls vs. PTSD–non-depressed, p � 0.001 controls vs. PTSD–depressed.c p � 0.001 all pairs.d p � 0.001 all pairs.

274 P. Morris et al. / Psychoneuroendocrinology 29 (2004) 269–278
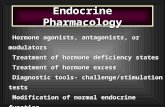
Fig. 1. The mean (±S.E.) of the GH concentration at each time point for the three groups. Top graph,control group; middle graph, PTSD-depressed group; bottom graph, PTSD-non-depressed group.
HARS scores differed between groups, with the PTSD–non-depressed group beingsignificantly more anxious than the controls but significantly less anxious than thePTSD–depressed group (Table 1). A similar pattern was observed in HDRS scores.
The mean (±S.E.) growth hormone concentrations at each time point for thePTSD–depressed, PTSD–non-depressed and the control group are presented in Fig.1. The PTSD–non-depressed subjects had a clearly blunted growth hormone responseto clonidine challenge compared to the other two groups.
The means (±S.D.) for the growth hormone parameters are presented in Table 2.There were no statistically significant differences across groups for the mean pre-dose GH concentration or for time to reach the peak GH response to clonidine. Therewere differences between the groups for peak GH (F = 4.08, p = 0.021). Peak GHresponses for the PTSD–non-depressed group were blunted in comparison to thecontrols and the PTSD–depressed group (both p � 0.05, post hoc SNK). There wasa similar pattern of differences between the groups for AUC GH (F = 3.52, p =
Table 2Mean (±S.D.) GH variables for the three groups
Controls PTSD–non-depressed PTSD–depressed p-Value(N = 32) (N = 23) (N = 27)
Pre-dose GH (mI U/l) 2.0 ± 1.2 1.6 ± 1.4 1.6 ± 0.7 NSa
Peak GH (mI U/l) 8.7 ± 8.8 3.9 ± 3.6 8.0 ± 9.4 0.021a,b
Time to peak (min) 41 ± 21 44 ± 29 39 ± 24 NSDelta GH (mI U/l) 6.6 ± 8.2 2.4 ± 3.1 6.4 ± 9.6 0.041a,c
AUC GH (mI 370 ± 603 90 ± 116 331 ± 633 0.034a,d
U/l/min)
a Log transformed values.b p � 0.05 controls vs. PTSD–non-depressed, p � 0.05 PTSD–non-depressed vs. PTSD–depressed.c p = 0.055 controls vs. PTSD–non-depressed, p = 0.05 PTSD–non-depressed vs. PTSD–depressed.d p � 0.05 controls vs. PTSD–non-depressed, p � 0.05 PTSD–non-depressed vs. PTSD–depressed.

275P. Morris et al. / Psychoneuroendocrinology 29 (2004) 269–278
0.034) and delta GH (F = 6.4, p = 0.041). AUC GH responses for the PTSD–non-depressed group were blunted in comparison to the controls and the PTSD–depressedgroup (both p � 0.05, post hoc SNK), and delta GH responses for the PTSD–non-depressed group were blunted in comparison to the controls (p � 0.05, post hocSNK) and approached significance in comparison with the PTSD–depressed group(p = 0.055, post hoc SNK). One significant association was found between CESscore and AUC GH (r = �0.24, p = 0.025). However, controlling for CES score(ANCOVA) did not alter the significant difference between groups on AUC GH.
4. Discussion
This is the first study of the growth hormone response to the α2-agonist clonidinein subjects with combat-related PTSD. The main finding of this study was a bluntedgrowth hormone response in non-depressed PTSD subjects when compared to sub-jects suffering from PTSD and concurrent depression and to a healthy control group.As clonidine stimulates growth hormone secretion via action on post-synaptic α2-receptors in the hypothalamus and pituitary axis (Matussek et al., 1980), the impli-cation of this result is that central α2-adrenergic receptors are subsensitive in PTSD.
The design of this study has several advantages over previous reports. First, weelected to use combat-exposed veterans as a control group to reduce the potentialfor confounding of the results by combat exposure. Second, subjects were dividedinto those with and without depression. Thus, the study examined three well definedcomparison groups: a combat-exposed control group with no PTSD, depression, orother psychiatric illness; a group with PTSD and no depression; and a group withboth PTSD and depression. Finally, the dose of clonidine was given on a µg/kg basisto minimise any effect of weight on the growth hormone response, and groups werematched on age and sex (all male).
The majority of previous studies indicate that PTSD is associated with an increasedresponsiveness in the noradrenergic system. Southwick et al. (1993) suggest thatpresynaptic α2-adrenergic autoreceptors are subsensitive in combat veterans withPTSD, which should lead to increased noradrenaline release in brain and increased24-h urinary excretion of noradrenaline. Our study infers that post-synaptic α2-adre-noceptors are also subsensitive in PTSD. A finding of subsensitive α2-adrenoceptorsis consistent with increased noradrenergic activity and agonist induced receptordown-regulation.
An attenuated growth hormone response after clonidine challenge has also beenfound in the majority of studies of major depressive illness (Matussek et al., 1980;Charney et al., 1982; Schittecatte et al., 1994) and was confirmed in the most recentreport involving a placebo-controlled clonidine challenge in over 70 patients with amajor depressive episode in comparison with healthy controls and other psychiatricpatients (Mokrani et al., 2000). The blunted response of growth hormone to clonidineinfers that post-synaptic α2-adrenoceptors are also subsensitive in depressive illness.However, not all reports are consistent, probably due to the many factors that mayinfluence the secretion of growth hormone. These include age (Mokrani et al., 2000),

276 P. Morris et al. / Psychoneuroendocrinology 29 (2004) 269–278
sex (Schittecatte et al., 1994), hormonal status (Schittecatte et al., 1994) and weight(Castro et al., 1990).
In contrast to the hyperactive noradrenergic state proposed for PTSD, receptorsubsensitivity in depression is thought to be due to a dysregulation of the norad-renergic system (Siever and Davis, 1985). Siever and Davis (1985) propose a modelof altered noradrenergic activity in which noradrenergic neuronal firing is increasedand erratic while noradrenaline released per nerve impulse is decreased. A recentstudy involving PET scanning during a clonidine challenge has found evidence ofattenuated noradrenergic function in the prefrontal cortex in depression (Fu et al.,2001), a finding consistent with this hypothesis.
Since attenuated growth hormone responses to clonidine have been found inpatients with major depression and in our non-depressed PTSD subjects, it mighthave been expected that the growth hormone response to clonidine in depressedPTSD subjects would show greater blunting than either of these two groups. Thiswas not observed. In fact, growth hormone response in our depressed PTSD subjectswas similar to controls. Our finding is congruent with the study of Yehuda et al.(1998), which found the noradrenergic abnormality to be confined to the subgroupof PTSD subjects without co-morbid depression. Yehuda et al. (1998) showed thatonly non-depressed PTSD subjects had increased plasma noradrenaline levels com-pared to normal controls, subjects with major depressive disorder, and subjects withPTSD and secondary depression. Other studies measuring urinary catecholamine lev-els and platelet α2-receptors have found a divergence in catecholamine function inmajor depressive disorder and PTSD (see Yehuda et al., 1998 for other references).A possible explanation is that abnormalities proposed for the noradrenergic systemin depression and PTSD do not compound but rather negate each other.
The blunted response of growth hormone in our PTSD–non-depressed group can-not be attributed to known confounding factors which can affect clonidine stimulatedgrowth hormone secretion (i.e. age, weight, sex) as they were controlled for in thisstudy. The two PTSD patient groups were similar in both combat exposure (asassessed by the CES) and PTSD symptomatology (as measured by the IES scale).Thus, the blunted response in the PTSD–non-depressed group appears to reflect aspecific subsensitivity of the post-synaptic α2-adrenoceptors. While we are unableto propose an explanation for the difference in growth hormone response to clonidinebetween the non-depressed and depressed PTSD subjects, this finding should encour-age further studies of this and other neurotransmitter systems in PTSD. Other neuro-transmitter alterations might differentiate PTSD from depression, as has beenobserved in studies of the hypothalamic–pituitary–adrenal axis (Yehuda et al., 1993).
Acknowledgements
The authors would like to thank Sophie Ignatiadis for recruiting the subjects andperforming the neuroendocrine challenge tests. Debbie Lynch assisted in the prep-aration of the manuscript. The study was funded by the Australian Department ofVeterans’ Affairs and the Weary Dunlop Research Foundation. We would like tothank all veterans for their typically generous participation.

277P. Morris et al. / Psychoneuroendocrinology 29 (2004) 269–278
References
Aardal-Eriksson, E., Eriksson, T.E., Holm, A.C., Lundin, T., 1999. Salivary cortisol and serum prolactinin relation to stress rating scales in a group of rescue workers. Biol. Psychiatry 46, 850–855.
American Psychiatric Association, Committee on Nomenclature and Statistics 1987. Diagnostic and Stat-istical Manual of Mental Disorders, third ed. revised. American Psychiatric Association, Wash-ington, DC.
Blanchard, E.B., Kolb, L.C., Prins, A., Gates, S., McCoy, G.C., 1991. Changes in plasma norepinephrineto combat-related stimuli among Vietnam veterans with post traumatic stress disorder. J. Nerv. Ment.Dis. 179, 371–373.
Bremner, J.D., Innis, R.B., Ng, C.K., Staib, L.H., Salomon, R.M., Bronen, R.A., Duncan, J., Southwick,S.M., Krystal, J.H., Rich, D., Zubal, G., Dey, H., Soufer, R., Charney, D.S., 1997. Positron emissiontomography measurement of cerebral metabolic correlates of yohimbine administration in combat-related post-traumatic stress disorder. Arch. Gen. Psychiatry 54, 246–254.
Castro, R.C., Vieira, J.G., Besser, G.M., Grossman, A.B., Lengyel, A.M., 1990. Pyridostigmine enhancesbut does not normalise the GH response to GH-releasing hormone in obese subjects. Acta Endocrinol.122, 385–390.
Charney, D.S., Heninger, G.R., Strenberg, D.E., Hafstad, K.M., Giddings, S., Landis, H., 1982. Adrenergicreceptor sensitivity in depression. Arch. Gen. Psychiatry 39, 290–294.
Davidson, J., Smith, R., Kudler, H., 1989. Validity and reliability of the DSM-III criteria for post-traumaticstress disorder — experience with a structured interview. J. Nerv. Ment. Dis. 177, 336–346.
Dinan, T.G., Barry, S., Yatham, L.N., Mobayed, M., Brown, I., 1990. A pilot study of a neuroendocrinetest battery in post-traumatic stress disorder. Biol. Psychiatry 28, 665–672.
Folstein, M.F., Folstein, S.E., McHugh, P.R., 1975. ‘Mini-mental state’ : a practical method for gradingthe cognitive state of patients for the clinician. J. Psychiatry Res. 12, 189–198.
Fu, C.H.Y., Reed, L.J., Meyer, J.H., Kennedy, S., Houle, S., Eisfeld, B.S., Brown, G.M., 2001. Norad-renergic dysfunction in the prefrontal cortex in depression: an [15O] H2O PET study of the neuromodul-atory effects of clonidine. Biol. Psychiatry 49, 317–325.
Geracioti, T.D., Baker, D.G., Ekhator, N.N., West, S.A., 2001. CSF norepinephrine concentrations inposttraumatic stress disorder. Am. J. Psychiatry 158, 1227–1230.
Hamilton, M., 1959. The assessment of anxiety states by rating. Br. J. Med. Psychol. 32, 50.Hamilton, M., 1960. A rating scale for depression. J. Neurol.-Neurosurg. Psychiatry 23, 56–62.Hansenne, M., Pitchot, W., Ansseau, M., 1991. The clonidine test in posttraumatic stress disorder. Am.
J. Psychiatry 148, 810–811.Horowitz, M., Wilner, N., Alvarez, W., 1979. Impact of events scale: a measure of subjective distress.
Psychosom. Med. 41, 209–218.Keane, T.M., Fairbank, J.A., Caddell, J.M., Zimmering, R.T., Taylor, K.L., Mora, C.A., 1989. Clinical
evaluation of a measure to assess combat exposure. Psychol. Assess. 1, 53–55.Kosten, T.R., Mason, J.W., Giller, E.L., Ostroff, R.B., Harkness, L., 1987. Sustained urinary norepi-
nephrine and epinephrine elevation in post traumatic stress disorder. Psychoneuroendocrinology 12,3–20.
Matussek, N., Ackenheil, M., Hippius, H., Muller, F., Schroeder, H.T., Schultes, H., Wasilewski, B.,1980. Effect of clonidine on growth hormone release in psychiatric patients and controls. PsychiatryRes. 2, 25–36.
McFall, M.E., Murburg, M.M., Ko, G.N., Veith, R.C., 1990. Autonomic responses to stress in Vietnamcombat veterans with posttraumatic stress disorder. Biol. Psychiatry 27, 1165–1175.
Mellman, T.A., Kumar, A., Kulick-Bell, R., Kumar, M., Nolan, B., 1995. Nocturnal/daytime urine norad-renergic measures and sleep in combat-related PTSD. Biol. Psychiatry 38, 174–179.
Mokrani, M.C., Duval, F., Diep, T.S., Bailey, P.E., Macher, J.P., 2000. Multihormonal response to clonid-ine in patients with affective and psychotic symptoms. Psychoneuroendocrinology 25, 741–752.
Neal, L.A., Busuttil, W., Rollins, J., Herepath, R., Strike, P., Turnbull, G., 1994. Convergent validity ofmeasures of post-traumatic stress disorder in a mixed military civilian population. J. Traumatic Stress7, 447–455.

278 P. Morris et al. / Psychoneuroendocrinology 29 (2004) 269–278
Perry, B.D., Giller, E.L., Southwick, S.M., 1987. Altered platelet α2-adrenergic binding sites in post-traumatic stress disorder. Am. J. Psychiatry 144, 1511–1512.
Pitman, R., Orr, S., 1990. Twenty-four hour urinary cortisol and catecholamine excretion in combat-related post-traumatic stress disorder. Biol. Psychiatry 27, 245–247.
Rasmussen, A.M., Hauger, R.L., Morgan, C.A., Bremner, J.D., Charney, D.S., Southwick, S.M., 2000.Low baseline and yohimbine-stimulated plasma neuropeptide Y levels in combat-related PTSD. Biol.Psychiatry 47, 526–539.
Schittecatte, M., Charles, G., Machowski, R., Dumont, F., Garcia-Valentin, J., Wilmotte, J., Papart, P.,Pitchot, W., Wauthy, J., Ansseau, M., Hoffman, G., Pelc, I., 1994. Effects of gender and diagnosison growth hormone response to clonidine for major depression: a large-scale multicentre study. Am.J. Psychiatry 151, 216–220.
Siever, L.J., Davis, K.L., 1985. Overview: toward a dysregulation hypothesis of depression. Am. J. Psy-chiatry 142, 1017–1031.
Southwick, S.M., Krystal, J.H., Morgan, C.A., Johnson, D.R., Nagy, L.M., Nicolaou, A., Heninger, G.R.,Charney, D.S., 1993. Abnormal noradrenergic function in post-traumatic stress disorder. Arch. Gen.Psychiatry 50, 266–274.
Southwick, S.M., Krystal, J.H., Bremner, J.D., Morgan, C.A., Nicolaou, A., Nagy, L.M., Johnson, D.R.,Heninger, G.R., Charney, D.S., 1997. Noradrenergic and serotonergic function in posttraumatic stressdisorder. Arch. Gen. Psychiatry 54, 749–758.
Southwick, S.M., Bremner, J.D., Rasmussen, A., Morgan, C.A., Arnsten, A., Charney, D.S., 1999. Norepi-nephrine: new vistas for an old neurotransmitter. Role of norepinephrine in the pathophysiology andtreatment of posttraumatic stress disorder. Biol. Psychiatry 46, 1192–1204.
World Health Organisation 1987. Composite International Diagnostic Interview. WHO, Geneva, Switzer-land.
Yatham, L.N., Sacamano, J., Kusumakoar, V., 1996. Assessment of noradrenergic functioning in patientswith non-combat-related post-traumatic stress disorder: a study with desmethylimipramine and ortho-static challenge. Psychiatry Res. 63, 1–6.
Yehuda, R., Southwick, S., Giller, E.L., Xiaowan, M.A., Mason, J.W., 1992. Urinary catecholamineexcretion and severity of PTSD symptoms in Vietnam combat veterans. J. Nerv. Ment. Dis. 180,321–325.
Yehuda, R., Southwick, S.M., Krystal, J.H., Bremner, D., Vharney, D.S., Mason, A.W., 1993. Enhancedsuppression of cortisol following dexamethasone administration in posttraumatic stress disorder. Am.J. Psychiatry 150, 83–86.
Yehuda, R., Siever, L.J., Teicher, M.H., Levengood, R.A., Gerber, D.K., Schmeidler, J., Yang, R.K.,1998. Plasma norepinephrine and 3-methoxy-4-hydroxyphenylglycol concentrations and severity ofdepression in combat posttraumatic stress disorder and major depressive disorder. Biol. Psychiatry 44,56–63.