Blunt Abdominal Trauma Jen Nicol PGY-2 Dr. Rob Lafreniere August 5 th, 2010.
80
Blunt Abdominal Trauma Jen Nicol PGY- 2 Dr. Rob Lafreniere August 5 th , 2010
-
Upload
milton-stevenson -
Category
Documents
-
view
217 -
download
1
Transcript of Blunt Abdominal Trauma Jen Nicol PGY-2 Dr. Rob Lafreniere August 5 th, 2010.

Blunt Abdominal Trauma
Jen Nicol PGY-2Dr. Rob LafreniereAugust 5th, 2010

Objectives
• Physical Exam in BAT• 3 important diagnostic modalities• Management goals in BAT• Hematuria in BAT• Common pitfalls


• Physical Exam in BAT
Objectives

Accuracy of physical exam in BAT is 55-65%

• In the alert patient–Pain– Tenderness with
guarding–Peritoneal findings
• High index of suspicion

Unreliable Findings• Equivocal exam• +/- normal physical
exam

Buckle up!

• Mesentery injury• Bowel perforation,
contusion• Rib & spine fractures• Diaphragm injury (rare)
Big Badness!


What is wrong with this picture?

Chance Fracture

Most common L1-3
50% con-current abdominal injuries

Objectives
• 3 important diagnostic modalities

If we all had these.....
It would be easy






Pain
Hematuria
Decreasing hematocrit levels
Negative FAST


FAST outcomes

CAT Scan


SN SP
Overall 92-98% 99%
Bowel / Mesentery
88% 99%
Diaphragm 54-73% 86-90%
pancreas 80%



Established need for laparotomy
Prior abdominal surgeryInfection
ObesityCoagulopathy
2/3rd trimester pregnancy

Sensitivity 87-95%Specificity 97-99%Accuracy 92-98%
Positive DPL In BAT:>10 mL aspirated blood
>100,000 RBC on lavage
Lavage output thorugh foley or chest tube
20,000-100,000 RBC indeterminite in BAT

DPL falsely negative in 25% of diaphragm injury

Objectives
• Management goals in BAT

Management Goals:
Stabilize the patient
Determine presence of intraperitoneal hemorrhage
Demonstrate organ injury requiring operative intervention
Don’t miss injuries!

Clinical Indications for laparotomy in BAT
Unstable VS, strongly suggestive abdominal injures
Unequivocal peritoneal irritation
Evidence of diaphragmatic injury
Significant GI bleeding

BAT
Hemodynamically Unstable?
Laparotomy
Yes
Clinical Indication for laparotomyYes
IPH?
+ve FAST / D
PL
IP injury?Source of bleeding?
CT scan, FAST, DPL Observe
No

BAT
Hemodynamically Unstable?
Clinical Indication for laparotomy
IPH?IP injury?
Reliable exam
No
Abdominal tenderness
Other serious injuries
No

Case 1
50 yo M rolled his dump truck while intoxicated
Prolonged extrication – 2 hrs+
Intubated for low GCS, STARS to FMC

78/48; 125; SaO2 96% 100%FiO2; temp 36.4;
FAST indeterminite
VBG pH 7.26, hbg90, lactate 3.5
↑ PTT/INR, low plts

DPA / PDL negative

No intra-abdominal hemorrhage, no hemothorax
Massive bleeding, exanguinating hematoma posterior torso.

Transfused copious amounts blood products
To interventional radiology
Arrests, dies on table

35 yo roofer falls of a 12 ft roof at work.
2min LOC, confused and disoriented, GCS 13 (E3V4M6).
Case 2

90 palp; HR 86; SaO2 100%2L; RR 18; temp 36.9
abdomen firm, mildly tender LUQ


Embolization by interventional radiology
Stabilises, no further transfusions
Unit 71, discharged a few days later

Case 3
4 yo F jumped out 2 story window
No VS abnormalities
Obviously deformed right femur
No abdominal tenderness

Insert XR here

More awake, less pain post femoral nerve block
Mild generalised abdominal pain
++++ RBC on urine cath dip
What to do now??

Objectives
• Hematuria in BAT

WHEN THE WHITE TURNS RED....

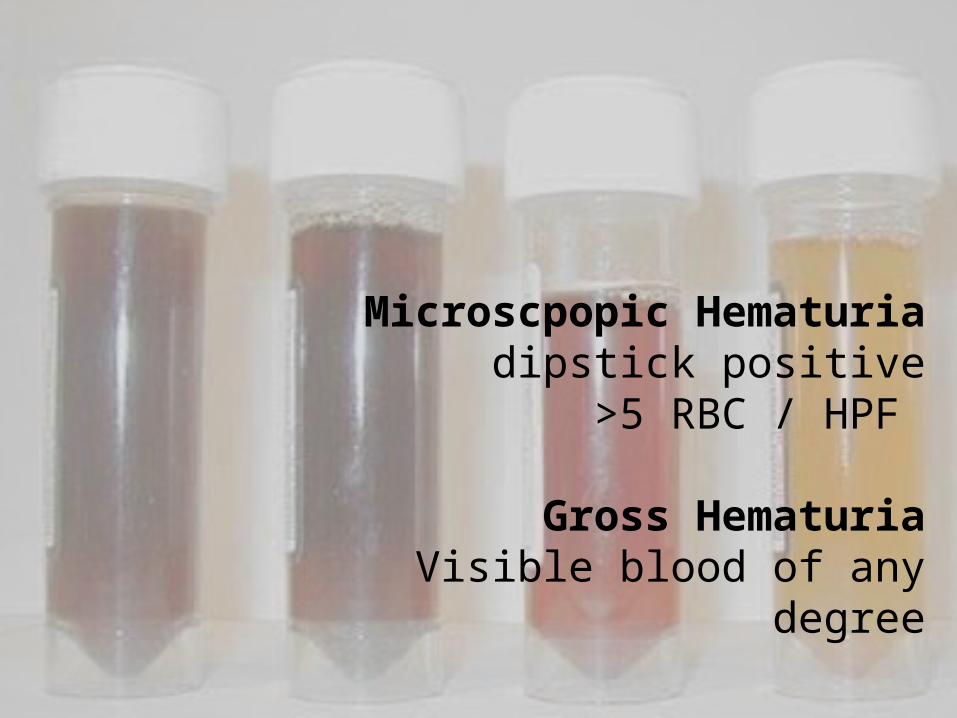
Microscpopic Hematuria dipstick positive
>5 RBC / HPF
Gross HematuriaVisible blood of any degree

Gross Hematuria
Microspcopic hematuria and shock (SBP<90)
Significant deceleration injury
Suspected intra-abdominal injuries
(J urol 1995;154:352)


Little Adults?

CT abdo / pelvis: •No acute injury•Kineys normal
Admitted to ortho fracture managment

22 year old M
Ran over by combine wheel near High River
STARS to FMC
Case 4

HR 123; BP 99/50; RR 20; SaO2 99 5L; temp 37
Grossly deformed pelvis
FAST negative x2 operators
3L NS 2U PRC’s - BP 90/48


Pelvic Fracture
Hemodynamically Stable?
FAST / DPL Positive?
Laparotomy
No
Angiography&
Pelvic fixation
Observation
Yes
No
IPH?
FAST, CT, DPL
Yes

FAST in pelvic fractures
SN 81% SP 87%
What does a negative FAST mean?

Rt internal iliac artery embolized with coil
Persistently tachycardic, hypotense
Taken to OR

17 yo M, aspiring Ducati racer
Flipped numerous times with bike before coming to stop
Wearing helmet, no leathers
Case 5

HR 119; BP 135/80; RR16; SaO2 99% 2L
Abdomen is +++tender – road rash over abdomen, torso, extremities
FAST negative

FAST negative
We decide to scan his abdo/pelvis
•Free fluid on 3 slices•no identifiable intra-abdominal organ damage

Free Fluid
Undetected solid organ injury
Bowel injury
Mesentery injury

Case 6
32 yo F assaulted with baseball bat by boyfriend
Intoxicated, Rt eye swollen shut
HR110; BP100/50; RR26; SaO2 96%RA, temp 37.4
Very tender LUQ – “he got a few good shots there”


CT scan normal, no free fluid, nil acute
Reassess frequently, more sober, still tender.
Observed until end of shift, tenderness dissipated, vital signs stable.

Negative CT scan
Discharge
Admit for observation
(J trauma 1998;44:273)
(Academic Emerg Med 2010;15:89

Discharged to Woman’s centre
Decides to press charges against her
boyfriend

• Common pitfalls
Objectives

False Negative Prediction
(Emerg Med Clin N Am 2010;28:1)

False attribution
(Emerg Med Clin N Am 2010;28:1)

Failure to assess the abdomen and plevis
(Emerg Med Clin N Am 2010;28:1)

Missed injuries
(Emerg Med Clin N Am 2010;28:1)