Blunt Abdominal Trauma

of 20
-
Upload
deusah-ezrah -
Category
Documents
-
view
21 -
download
0
description
pt
Transcript of Blunt Abdominal Trauma
-
BLUNT ABDOMINAL TRAUMA
-
OVERVIEWEvaluation of patients who have sustained blunt abdominal trauma (BAT) may pose a significant diagnostic challenge
Blunt trauma produces a spectrum of injury from minor, single-system injury to devastating, multi-system trauma.
-
OVERVIEWIntra-abdominal trauma may be missed in as many as 45% of patients
Exquisite judgment is required
Recognition of specific injury pattern is crucial for diagnosis
Standardization of operative and non-operative treatment
-
Several factors influence the selection of diagnostic testing: type of hospital - i.e., trauma center vs. non-trauma hospitalaccess to a particular technology at the surgeons institutionthe surgeons individual experience with a given diagnostic modality. As facilities evolve, technologies mature and surgeons gain new experience, it is important that any diagnostic strategy constructed be dynamic.
-
MOTOR VEHICLE COLLISIONSMOTORCYCLE CRASHESPEDESTRIANS STRUCK BY VEHICLESFALLSASSULTPATTERNS OF INJURY
-
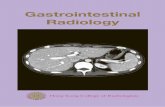
Algorithm for the initial evaluation of a patient with suspected blunt abdominal trauma
-
Algorithm for Evaluation of Blunt Abdominal TraumaBlunt Abdominal TraumaUltrasound POSITIVEEQIOVOCALNEGATIVEStableUnstableStableUnstableRepeat ultrasoundpositivenegativeCTLaparotomyCT or DPLDPL or Laparotomy
-
Level IExploratory laparotomy is indicated for patients with a positive DPL.CT is recommended for the evaluation of hemodynamically stable patients with equivocal findings on physical examination, associated neurologic injury, or multiple extra-abdominal injuries. Under these circumstances, patients with a negative CT should be admitted for observation.CT is the diagnostic modality of choice for nonoperative management of solid visceral injuries. In hemodynamically stable patients, DPL and CT are complementary diagnostic modalities.
-
Level IIFAST may be considered as the initial diagnostic modality to exclude hemoperitoneum. In the presence of a negative or indeterminate FAST result, DPL and CT have complementary roles.When DPL is used, clinical decisions should be based on the presence of gross blood on initial aspiration (i.e., 10 ml) or microscopic analysis of lavage effluent.In hemodynamically stable patients with a positive DPL, follow-up CT scan should be considered, especially in the presence of pelvic fracture or suspected injuries to the genitourinary tract, diaphragm or pancreas. Exploratory laparotomy is indicated in hemodynamically unstable patients with a positive FAST. In hemodynamically stable patients with a positive FAST, follow-up CT permits nonoperative management of select injuries.Surveillance studies (i.e., DPL, CT, repeat FAST) are required in hemodynamically stable patients with indeterminate FAST results.
-
Level IIIObjective diagnostic testing (i.e., FAST, DPL, CT) is indicated for patient with abnormal mentation, equivocal findings on physical examination, multiple injuries, concomitant chest injury or hematuria.Patients with seatbelt sign (SBS) should be admitted for observation and serial physical examination. Detection of intraperitoneal fluid by FAST or CT in a patient with SBS mandates either DPL to determine the nature of the fluid or exploratory laparotomy.CT is indicated for the evaluation of suspected renal injuries.A negative FAST should prompt follow-up CT for patients at high risk for intraabdominal injuries (e.g., multiple orthopedic injuries, severe chest wall trauma, neurologic impairment).Splanchnic angiography may be considered in patients who require angiography for the evaluation of other injuries (e.g., thoracic aortic injury, pelvic fracture).
-
Diagnostic Peritoneal Lavage
Rapid and accurate test used to identify intra-abdominal injuries after blunt trauma in the hypotensive or unresponsive patient without obvious indication for abdominal exploration. Standard criteria for a positive peritoneal lavage include : aspiration of at least 10 mL of gross blooda bloody lavage effluenta red blood cell count greater than 100,000/mm3a white blood cell count greater than 500/mm3, an amylase value greater than 175 IU/dLthe detection of bile, bacteria, or food fibers. This test is highly sensitive to the presence of intraperitoneal blood; however, specificity is low and because a positive test prompts surgical exploration, a significant number of explorations will be nontherapeutic
-
DPL Indications Equivocal pulmonary embolismUnexplained shock or hypotensionAltered sensorium (e.g., closed-head injury, drugs)General anesthesia for extra-abdominal proceduresCord injury
Contraindications Clear indication for exploratory laparotomy Previous exploratory laparotomy PregnancyObesity
-
UltrasoundThe objective of ultrasound evaluation is to search for free intraperitoneal fluid. It can be done expeditiously, and it is as accurate as diagnostic peritoneal lavage to detect hemoperitoneum. CT of the abdomen usually follows a positive ultrasound in a stable patient. The sensitivity ranges from 85% to 99%, and the specificity from 97% to 100%.[33]
- UltrasoundAdvantages NoninvasiveDoes not require radiationUseful in the resuscitation room or emergency departmentCan be repeatedUsed during initial evaluationLow costDisadvantages Examiner dependentObesityGas interpositionLower sensitivity for free fluid
-
Abdominal CT
CT is the most frequently used method to evaluate the stable patient with blunt abdominal trauma.The retroperitoneum is best evaluated by CTCT also evaluates solid organ injury, and in the stable patient with a positive ultrasound it is indicated to grade organ injury and to evaluate contrast medium extravasation.
-
Abdominal CTIndicationsBlunt traumaHemodynamic stabilityNormal or unreliable physical examinationMechanism: duodenal and pancreatic traumaContraindications Clear indication for exploratory laparotomyHemodynamic instabilityAgitationAllergy to contrast media
-
Abdominal CTAdvantages Adequate assessment of the retroperitoneumNonoperative management of solid organ injuriesAssessment of renal perfusionNoninvasiveHigh specificityDisadvantages Specialized personnelHardwareDuration: helical vs. conventionalHollow viscus injuriesCost
-
Blunt abdominal trauma initially is evaluated by FAST examinationFAST is not 100% sensitive, FAST is used to identify free intraperitoneal fluid (>250 ml)Morison's pouchthe left upper quadrant the pelvis.CT scanning to quantify injuriesInjury grading using the American Association for the Surgery of Trauma grading scale is a key component of non-operative management of solid organ injuries.
-
Additional findings noted on CT scan contrast extravasation (i.e., a "blush"),the amount of intra-abdominal hemorrhage,presence of pseudoaneurysms CT also is indicated for hemodynamically stable patients for whom the physical examination is unreliable.CT still has limited sensitivity for identification of intestinal injuries.Bowel injury is suggested by findings thickened bowel wall,"streaking" in the mesentery,free fluid without associated solid organ injury,free intraperitoneal air
-
Focused abdominal sonography for trauma right kidney and liver left kidney and spleen in the pelvis
*