
BLUE PRSRT STD - Health Insurance New Mexico · PRSRT STD U.S. POSTAGE PAID PERMIT NO. 581 CHICAGO,...
14
BLUE Review ISSUE 3 - 2006 (May/June) bcbsnm.com 2006 Provider Satisfaction Survey Our annual provider survey is an important tool used to develop plans for improving and maintaining provider satisfaction. This year’s provider survey will be mailed to you in May. You’ll have the opportunity to rate our performance in a number of areas such as timeliness of claims processing, frequency and effectiveness of provider visits, variety of drug list, the preauthorization process, and continuity and coordination issues. You will also be asked for general input on ways we can serve you better in the future. Several quality review committees analyze provider survey results and utilize provider responses to formulate improvement plans. We appreciate and encourage your continued feedback as a valued member of our provider community. BCBSNM’s behavioral health network is growing and stronger than ever. Mesa Mental Health (MMH) administers many of the BCBSNM/HMONM plans and maintains an extensive network of nearly 1,000 behavioral health providers throughout the state. Our behavioral health network has increased by nearly 150 practitioners in the past year to ensure the availability of services to meet members’ needs. A diverse group of independently licensed social workers, mental health therapists, substance abuse counselors, psychologists, psychiatrists, and other behavioral health specialists contract through MMH. BCBSNM and MMH partner on several proj- ects of special importance to New Mexicans. The Alcohol and Other Drug Project is designed to enhance aftercare for members needing ongoing chemical dependency services after discharge from a medical facility. It includes an innovative email notification system and new collaborative communications so that referrals are initiated prior to hospital discharge. Another valuable joint project of BCBSNM and MMH is the Post-Partum Depression Prevention Project. It identifies women with significant risk factors for serious depression and refers them for behavioral health services. To date, more than 500 prenatal women have been supplied with the PPD educational brochure. You may preview and print this brochure at mesamentalhealth.com/pdf/quality/ppd_ newsletter.pdf. MMH is now waiving the copay for initial assessments to the PPD program in order to remove any impediments for participants. Providers, how- ever, will be reimbursed 100% for the initial assessment by billing under CPT code 99420. For more information and a provider directory, visit bcbsnm.com. Customer Service staff are also available to answer questions about mental health benefits and assist in making appoint- ments with mental health providers by calling 816-6792 or toll-free at 800-583-6372. BCBSNM/HMONM behavioral health services
Transcript of BLUE PRSRT STD - Health Insurance New Mexico · PRSRT STD U.S. POSTAGE PAID PERMIT NO. 581 CHICAGO,...

PRSRT STDU.S. POSTAGE
PAIDPERMIT NO. 581
CHICAGO, IL
INSIDE this issue12006 Provider Satisfaction Survey1BCBSNM/HMONM behavioral health services 22006 BlueCard
®Program Satisfaction Survey
2Instant access online 2Blue News for Kids3Office Staff: COBC crossover update 3NPI updates now online4Claims filing corner: Boniva injections4Network Services contacts and related service areas4Coming soon! RBRVS updates/Blue Transitions 5-72006-2007 Clinical Practice Guidelines82006-2007 Adult Preventive Health Guidelines 9Altering medical records 9Reimbursement issue “letters of medical necessity” 9Attention ERAusers: We’re eliminating paper 10Medical policy updates10Blue Care Connection
SMDisease Management
10Special Beginnings®
prenatal program10New! Spanish PHGs112006 Drug List updates11Member rights and responsibilities
P.O. Box 27630Albuquerque, NM 87125-7630
ADivision of Health Care Service Corporation, a Mutual LegalReserve Company, an Independent Licensee of the Blue Crossand Blue Shield Association.
BLUEReviewISSUE 3 - 2006
ISSUE 3 - 2006 (May/June)bcbsnm.com
2006 Provider Satisfaction SurveyOur annual provider survey is an importanttool used to develop plans for improving andmaintaining provider satisfaction. This year’sprovider survey will be mailed to you in May.You’ll have the opportunity to rate our performance in a number of areas such astimeliness of claims processing, frequencyand effectiveness of provider visits, variety ofdrug list, the preauthorization process, and
continuity and coordination issues. You willalso be asked for general input on ways wecan serve you better in the future.
Several quality review committees analyzeprovider survey results and utilize providerresponses to formulate improvement plans.We appreciate and encourage your continuedfeedback as a valued member of our providercommunity.
Special InsertThe latest issue of Diabetes Resourcestitled “A1C: An Update on ClinicalRelevance” is a special insert in thisnewsletter. More diabetes informationis available at bcbsnm.comin theprovider area under DiabetesGuidelines and Reference.
BCBSNM’s behavioral health network isgrowing and stronger than ever. Mesa MentalHealth (MMH) administers many of the BCBSNM/HMONM plans and maintains anextensive network of nearly 1,000 behavioralhealth providers throughout the state. Ourbehavioral health network has increased bynearly 150 practitioners in the past year toensure the availability of services to meetmembers’ needs.
A diverse group of independently licensedsocial workers, mental health therapists, substance abuse counselors, psychologists,psychiatrists, and other behavioral healthspecialists contract through MMH.
BCBSNM and MMH partner on several proj-ects of special importance to New Mexicans.
The Alcohol and Other Drug Project isdesigned to enhance aftercare for membersneeding ongoing chemical dependency services after discharge from a medical facility. It includes an innovative email notification system and new collaborativecommunications so that referrals are initiatedprior to hospital discharge.
Another valuable joint project of BCBSNMand MMH is the Post-Partum DepressionPrevention Project. It identifies women with significant risk factors for serious depressionand refers them for behavioral health
services. To date, more than 500 prenatalwomen have been supplied with the PPD educational brochure. You may preview andprint this brochure at mesamentalhealth.com/pdf/quality/ppd_newsletter.pdf. MMH is now waiving thecopay for initial assessments to the PPD program in orderto remove anyimpediments forparticipants.Providers, how-ever, will bereimbursed 100%for the initialassessment bybilling underCPT code 99420.
For more information anda provider directory, visitbcbsnm.com.Customer Servicestaff are alsoavailable to answer questions about mentalhealth benefits and assist in making appoint-ments with mental health providers by calling 816-6792 or toll-free at800-583-6372.
BCBSNM/HMONM behavioral health services
bluereview3-2006.qxp 5/12/2006 2:56 PM Page 1

Brand-Name Medications moving to the Tier 3 Copayment Effective October 1, 2006THIRD-TIER BRAND SECOND-TIER ALTERNATIVES FIRST-TIER GENERIC ALTERNATIVES
Blood glucose test stripsFASTTAKE*ONE TOUCH II/BASIC/PROFILE*ONE TOUCH ULTRA*SURESTEP*
ACCU-CHEK AVIVA, ACCU-CHEK COMPACT, FRESTYLE, FRESTYLE FLASH, PRECISION QID, PRECISION XTRA blood glucose test strips
CAPITAL WITH CODEINECARBATROLCLOZAPINE 12.5mg, 50mg, 200mg tabletsDEXTROSTAT 10mgDILANTIN 100mg
acetaminophen and codeine oral sol 120 12mg/5ml
TEGRETOL XR 100mg, 200mg, 400mg carbamazepine immediate release tabletsclozapine 25mg, 100mg tabletsdextroamphetamine immediate release tabs phenytoin sodium, extended caps, 100mg
ELIXOPHYLLINFLEXERIL 5mgLITHIUM CARBONATE 150mg capsules
marketed by RoxaneLITHIUM CARBONATE 300mg tablets,
600mg capsulesMECLOFENAMATE
NAVANE 20mgORAMORPH SRPARNATEROCALTROLROXICET (oxycodone/acetaminophenoral solution 5-325mg/5 mL)
ZITHROMAX*ZYPREXA
ZYPREXA ZYDIS
theophylline elixircyclobenzapyrine tablets, 5mglithium carbonate 150mg capsules
lithium carbonate 300mg capsules
diclofenac sodium, ibuprofen, naproxen
thiothixene capsules, 2mg, 5mg, 10mg
morphine sulfate extended-release tabsNARDIL
calcitriol caps, oral solutionhydrocodone/acetaminophen elixir
7.5-325mg/15 mL
azithromycin tablets, 250mg, 500mg, 600mgGeodon, RISPERDAL, RISPERDAL
M-TAB, SEROQUELGeodon, RISPERDAL, RISPERDAL
M-TAB, SEROQUEL
ACTOPLUS MET FRESTYLE, FRESTYLE FLASH PARCOPACELONTIN blood glucose test strips PATANOLCHLORAL HYDRATE supp GEODON PRECISION QID, PRECISION XTRACODEINE PHOSPHATE sol tab KALETRA tablets blood glucose test stripsCYPROHEPTADINE syrup MESTINON syrup RENAGELDEXCHLORPHENIRAMINE MESTINON TIMESPAN SUBOXONE
MALEATE syrup METAPROTERENOL tab SUBUTEXDIAZEPAM oral sol, 1mg/mL MYFORTIC tablets TRAVATANEMTRIVA oral sol ORAP
Brand-Name Medications Added to Second-Tier Copay Effective April 1, 2006
* EFFECTIVE APRIL 1, 2006
The BCBSNM and Prime TherapeuticsPharmacy and Therapeutics Committee meton February 28, 2006, and recommended thefollowing changes and additions to the BCBSNM Drug List, effective October 1, 2006except where noted. The brand-name
prescription drugs listed will continue to beavailable to our members but members willpay the higher third-tier copayment effectiveOctober 1, 2006. In the table below, we’veincluded generic alternative medications thatare on our Drug List.
Drug List updates
Our health plan members have rights andresponsibilities that are listed in their BenefitBooklet or Member Handbook. Most members
can also access these documents on our web-site, bcbsnm.com.
Member rights and responsibilities
2006 BlueCard® Program Satisfaction Survey Our BlueCard program allows members of otherBlue Plans to obtain health care services while inanother plan’s service area. That means BCBS members visiting New Mexico can receive the benefits of the BCBS Plan listed on their insurancecard, and access our local BCBSNM provider network and savings.
As a participating BCBSNM provider, your satisfac-tion is a top priority to us. We value the care youprovide to our members. We conduct annual surveysto assess your satisfaction with the BlueCard pro-gram and your feedback allows us to identify waysto serve you more effectively. Last year’s surveynoted continued improvement in provider satisfac-tion with the program, specifically in these areas:
• Claims accuracy and timeliness• Satisfaction with resolving problem claims • Electronic eligibility verification • Customer service• Provider education
In 2005, we implemented the following initiatives tobetter serve you:
• Increased internal employee training resources to maximize quality of service
• Provided internal education to BCBSNM provider relations staff
• Featured ongoing articles in the Blue Review
To continue evaluating our performance, we haveasked The Response Center, an independentresearch company, to conduct telephone interviewson our behalf. They will contact a randomly selectedsample of providers who provided care for BlueCardmembers during 2005 and will ask to speak with the person in your office who is most knowledgeableabout filing BCBS claims and/or someone in thebilling department. The first set of telephone inter-views is currently in progress, and a second set willbe scheduled in the fall.
Thank you in advance for taking the time to provideus with your feedback.
If you have questions about the BlueCard Programor have suggestions for improvement, please emailus at [email protected]. Or, you may callthe BlueCard Provider Service Unit at 800-222-7992.
The 2006-2007 issue of Blue News for Kids has justbeen released. This 4-page newspaper addresseschildren’s health with fun, upbeat stories gearedfor kids and can supplement health care providers’preventive health education efforts. This issueincludes articles on: immunizations, dental care,growth and development, body image, hearing safety, eating disorder prevention, stress, bullies,gun safety, what to do in an emergency, sleep,nutrition, cooking, sun safety, and making physicalactivity fun.
Providers may receive free copies for their officesby contacting Network Services at 837-8800 or800-567-8540.
Blue News for Kids
Have you discovered how much BCBSNM has madeavailable online to provide better service to our net-work providers? Please visit the provider area atbcbsnm.com for the most complete and up-to-datenews and information on topics of concern to you.Among the resources you’ll find valuable: theProvider Library (with the current Blues ProviderReference Manual, medical policy information, and
forms), UM/QI Medical Management (with clini-cal guidelines, Blue Care Connection DiseaseManagement program information, and more),Provider Network, Pharmacy information,Medicaid Utilization Review information, BlueMedicare PPO page, Electronic Commerce andClaims Filing information, and a new NPI(National Provider Identifier) page.
Instant access online just for our network providers
bluereview3-2006.qxp 5/12/2006 2:56 PM Page 2

Medical policy updatesOnce approved, new or revised medical policies areposted on our website the first day of each month,with their effective dates indicated. You’ll find themost complete and up-to-date information on bothactive and pending medical policies in the provider
area of our websute, bcbsnm.com, under ProviderLibrary. New or revised medical policies developedsince the last Blue Review are summarized below.Please contact Health Services at (505) 816-2093with any questions.
OFFICE StaffIssue 3 - 2006 (May-June)bcbsnm.com
BCBSNM completed the first phase of the transi-tion to Centers for Medicare & Medicaid Services(CMS) consolidated Medicare crossover process lastNovember. The transition of Coordination ofBenefits Contractor (COBC) crossover on supple-mental claims used for calculating secondary payment liability was completed on April 3, 2006.We have appreciated your patience during theCOBC transition period. Here are a few highlightsof the COBC transition:
Enhancements: Under the new COBC process,supplemental claims will continue to cross over formembers in the BCBSNM eligibility files. Butclaims will now cross over to the supplementalinsurer from one party, the COBC contractor,rather than the various individual Medicare contractors.
Full Transition Date: Medicare Parts A and Bclaims processed on or after April 3, 2006, will crossover only after the claims have left Medicare payment floors. Please do not submit your supple-mental claims to BCBSNM prior to release of theMedicare payment floors:
• Electronic claims processed will be released to the supplemental insurer after a 14-day payment floor.
• Paper claims processed will be released after the new 29-day payment floor instituted under the Deficit Reduction Act (DRA).
Mass Adjustments: On February 10, 2006, CMSannounced that the DRA prevents payments forphysicians’ services delivered on or after January 1from being reduced by a negative update of 4.4 per-cent. January claims that have already been paidand have crossed over to the supplemental insurersare being adjusted by Medicare. All mass adjust-ments are expected to be completed by July 1, 2006.Since BCBSNM has elected to receive the massadjustments via the crossover files, please do notsubmit these adjustments on paper.
Medicare Claims with No Liability: Medicareclaims paid at 100% with no additional beneficiaryliability will not cross over. Medicare claims denied
at 100% with no additional beneficiary liability alsowill not crossover. In instances where there is noliability, please do not submit the claim to BCBSNM.
Although most claims will continue to seamlesslycross over, according to CMS, if claims fail to crossover due to claim data errors originating at theMedicare contractor site, the Medicare contractorswill send notification to the providers advisingthem that their claim did not cross over to thepatient's supplemental insurer due to claim dataerrors. If you receive this type of Medicare notifica-tion, please submit the supplemental claim elec-tronically to BCBSNM.
NPI updates now onlineThe Health Insurance Portability andAccountability Act of 1996 (HIPAA) mandated theadoption of standard unique identifiers for healthcare providers — the National Provider Identifier(NPI) — by May 23, 2007. The countdown to NPIimplementation is currently underway at BCBSNMand our goal is to make this transition as seamlessas possible for our providers. To assist you, a newlink, NPI (National Provider Identifier), has beenadded to the provider area of our website, bcbsnm.com. Information now available on our website includes:
• NPI overview• How to apply for your NPI• Links to other helpful websites• Contact information • Frequently Asked Questions• An NPI submission form (for providers who
currently have a BCBSNM provider number)
We will continue to provide updates on our websiteand in Blue Review. You will also receive notifica-tion by mail regarding how to submit your NPI tous. In the meantime, please do not begin usingyour NPI on electronic transactions untilBCBSNM has communicated an effective dateand instructions on how to proceed.
Coordination of Benefits Contractor (COBC) crossover updateEFF. DATE POLICY # POLICY NAME
06/01/2006 DME101.010 Wheelchairs and Accessories
06/01/2006 DME104.012 Lower Limb Prosthetics, Including Microprocessor Knees
06/15/2006 MED201.026 Surface Electrical Stimulation
06/15/2006 SUR712.004 Percutaneous Intervertebral Techniques to Treat Chronic Discogenic Back Pain
06/15/2006 THE801.006 Plasma Exchange (Plasmapheresis)
06/15/2006 DME104.001 Prosthetics, Except Lower Limb Prosthetics
07/15/2006 SUR706.009 Sleep Related Breathing Disorders, Medical and Surgical Management
07/15/2006 SUR702.009 Patient Controlled Analgesia
07/15/2006 MED207.104 Lyme Disease (Borrelia Burgdorferi) Management
07/15/2006 PSY301.014 Autism Spectrum Disorders (ASD)
07/15/2006 SUR716.017 Mastectomy for Gynecomastia
07/15/2006 DME101.001 Hospital Beds and Related Equipment
Special Beginnings® prenatalprogram supports your careBCBSNM provides our Special Beginnings prenatalprogram to members whose health plans includematernity coverage. This program provides additional support during pregnancy and includes educational materials, a 24-hour nurse line, healthrisk assessment, and case management for high-risk pregnancies. Members can receive informationonline via our website or through the mail.
Members are automatically referred to the SpecialBeginnings program when a provider’s office callsfor precertification for delivery or a referral to anOB specialist. Members are then contacted andoffered the option to participate. Members may alsoself-refer.
If you would like more information about SpecialBeginnings, please call the Health Services depart-ment at 800-325-8334.
Blue Care ConnectionSM DiseaseManagement programsBCBSNM continues to provide disease managementprograms for diabetes; asthma; COPD; and cardiacconditions such as CAD, CHF, and hypertension.For more information about our programs and making patient referrals, please call 816-2230 ortoll-free at 866-252-8106. Or, you may email us [email protected].
New! Spanish PHGsThe BCBSNM 2006-2007 Preventive HealthGuidelines for adults and children members arenow available in Spanish. Members and providerscan access ready-to-print versions in the memberand provider areas of our website, bcbsnm.com.
bluereview3-2006.qxp 5/12/2006 2:56 PM Page 3

PROVIDER REPRESENTATIVESThis team handles general questions for all areas
CENTRAL REGIONNetwork Contract Representative Michelle Quintero, (505) 816-2158
Lead Provider RepresentativeLiz Martinez, (505) 816-2161
SOUTHERN REGIONNetwork ContractRepresentative
Jill Billingsley, (505) 816-2143
Lead Provider RepresentativeJan Montoya, (505) 816-2303
NORTHERN REGIONNetwork Contract Representative
Joann Ireland, (505) 816-2159
Lead Provider RepresentativeGina Gutierrez, (505) 816-2156
PROFESSIONAL CONTRACTINGIncluding Allied Health Practitioners
HOSPITAL CONTRACTINGIncluding Acute Care, Behavioral Health,
and Specialty Hospitals
Network Contract Representative George Salaiz, (505) 816-2139
Lead Provider RepresentativeGina Gutierrez, (505) 816-2156
ANCILLARY CONTRACTINGDivided by Type of Ancillary Service Including
Vendors
Network Contract RepresentativeRick Bogle, (505) 816-2145
Lead Provider RepresentativeJan Montoya, (505) 816-2303
•DME, Home Health, Hospice, Home IV, and supplies (e.g., mastectomy, hearing, prosthetic/orthotic)
•Freestanding and Statewide Labs•Rehab. Hospitals (excluding Albuquerque Rehab.)•Air Ambulance•Radiology Providers•Freestanding Ambulatory Surgical Centers South of I-40•McKesson Specialty Pharmacy
Network Contract Representative Joyce Hamblet, (505) 816-2146
Lead Provider RepresentativeLiz Martinez, (505) 816-2161
•Skilled Nursing Facilities •Birthing Centers•Diabetes/Nutrition Centers •Sleep Study Centers•Cardiac Rehab. Facilities •Bone Density Centers •Dialysis Freestanding Facilities •Freestanding Ambulatory Surgical Centers North of I-40•Mesa Mental Health
Network Services and related service area contacts
Our Provider Representatives are available to assist you Monday - Friday, 8 a.m. to 5 p.m.General department telephone numbers: (505) 837-8800 or toll-free at 800-567-8540Our direct fax numbers: (505) 816-2688 or 866-290-7718
As the health care industry moves toward apaperless environment, payers have designedprograms to complement and/or be used withthe Electronic Remittance Advice (ERA). Thereare two products to assist you:
Electronic Payment Summary (EPS). BCBSNMhas designed an electronic format of the paperProvider Claim Summary, the EPS, which canbe used in coordination with the ERA. The EPSis an easy-to-read electronic print image of thepaper format you currently receive in the mail.You must enroll to receive the ERA and willthen automatically receive the EPS. For anERA enrollment form from BCBSNM, visitthinedi.com/enrollment.htm. The EPS filewill be placed in your electronic mailbox alongwith your ERA file.
Medicare Remit Easy Print. The Centers forMedicare & Medicaid (CMS) has designed aproduct called Medicare Remit Easy Print(MREP). If you are still receiving the StandardPaper Remittance Advice from Medicare (SPR),you can request cancellation of the paper and acopy of your remittance using the MREP soft-ware. For information on MREP, seewpsic.com/edi/pdf/mrep_overview.pdf, orcontact WPS Medicare at 877-567-7261.
Attention ERA users: We’re eliminating paper
Note: Paper remittances will eventually beeliminated. BCBSNM will discontinue thepaper after 30 days, and Medicare hasinformed our THIN Clearinghouse it will notmake the SPR available through the mail.
Altering medical recordsBCBSNM reviewers occasionally receive medical records with clinical information thathas been scribbled over, “whited out,” or other-wise altered. In a recently denied claim,records from a single visit were submittedtwice, with substantive changes made in whatappeared to be an effort to build criteria for aparticular medication, yet no initials, dates, orappropriate documentation accompanied therecord changes.
Altering medical records may have significantlegal implications, including medical fraud.While it is sometimes appropriate to make acorrection or change, such a change should bea made by a single line through the erroneousinformation, dated, and initialed or signed.The Fraud/Special Investigations Division of
BCBSNM and HCSC may become involvedwhen documents have been altered.
In the situation above, the BCBSNM medicaldirector contacted the provider who expressedsurprise and embarrassment about the matter.A support person in his office had made therecords change without his knowledge, and hewas very aware about the potential gravity ofaltering medical records. This was deemed anacceptable explanation and no further actionwas initiated by BCBSNM.
BCBSNM recommends that all medical per-sonnel train their staff on the correct way tochange medical documents and of the potentialimplications of inappropriately altering them.Providers are encouraged to consult their legaladvisors with any questions.
Reimbursement issue — “letters of medical necessity” Clinical documents — medical records thatestablish a relationship between the requestedproduct or service and the member's clinicalsituation — are generally required for determination of medical necessity. “Letters ofmedical necessity” — whether on template furnished by a product’s manufacturer or distributor or an original — are generally considered inadequate.
If you submit a “letter of medical necessity”with your request for approval of a product orservice without supporting clinical documents,
BCBSNM staff will likely request the medicalrecords, delaying processing, and potentiallydelaying your reimbursement. Or if medicalrecords are not furnished, the request may bedenied due to lack of adequate clinical documentation.
Note: The term,“letter of medical necessity,”is a misnomer. Medical necessity is notestablished by a letter, but by documentationin a contemporaneously produced medicalrecord. A “letter of medical necessity” is oftenextraneous.
Claims filing cornerBoniva injectionsBecause the injectable drug Boniva is new anddoes not yet have a published code, submit claimsusing the J3490 unclassified drug code, along withthe written description and NDC (National DrugCode) number. Boniva will be priced per AWP untila code and ASP are established and published.
Oral Boniva (non-injectable) should be submittedaccording to the member’s Pharmacy benefit.
Remember: Injectable Boniva requiresPrior Authorization because strict criteriamust be met in order for this drug to be covered by BCBSNM.
Coming soon!Annual RBRVS updates. All participatingproviders will soon receive a letter announcingupdates to the Maximum Allowable Fee Scheduleof the 2006 Resource Based Relative Value System(RBRVS) Relative Value Units (RVUs). Theseupdates will be effective for dates of service July 1,2006, and forward. Included are Medicare flat feesfor clinical laboratory and durable medical equip-ment, which will be used in our reimbursementmethodology. Please watch your mail.New plan: Blue Transitions. BCBSNM will soonbe offering a new health care plan, Blue Transitions,for New Mexicans who need a short-term policy fortransitional periods, such as between jobs, after gradua-tion, or recently moved to New Mexico. More detailscoming soon!
bluereview3-2006.qxp 5/12/2006 2:56 PM Page 4

The 2006-2007 BCBSNM/HMONM ClinicalPractice Guidelines are highly focused summariesof national recommendations designed for the busypractitioner. These CPGs have been approved bypracticing New Mexico physicians who serve on theBCBSNM Quality Improvement Professional ReviewCommittee. These reflect care that is appropriate formost persons with the disease, however they shouldnot substitute for clinical judgement in individualcases. Variations from the guidelines will be clinical-ly indicated in some patients.
Certain elements within these CPGs, however, areconsidered core elements and BCBSNM/HMONMannually measures how network physicians performin core elements as a basis for ongoing clinical quali-ty improvement and performance-based recognition.
Clinical Practice Guidelines are enclosed here andthe following two pages for the following five conditions:
• Treatment of ADHD in School-Age Children • Asthma• Diabetes• Hypertension• Initial Antidepressant Treatment of Adult Major
Depression
They can also be found in the provider area of bcbsnm.com, under the UM/QI/MedicalManagement heading. Additional information on BCBSNM Blue Care Connection DiseaseManagement is at bcbsnm.com/haw/haw_disease_mgt.htm.
2006-2007 Clinical Practice Guidelines
Treatment of ADHD in School-Age ChildrenEndorsedGuidelines
Clinical Practice Guideline: Treatment of the School-Aged Child with ADHD, AmericanAcademy of Pediatrics as published in: Pediatrics Oct 2001; 108(4):1033-1044
Guiding Principles 1. ADHD in children 6 through 12 years of age requires both a structured approach to diagnosis and the development of a specific treatment plan with concrete goals.
2. The treating clinician should work in collaboration with the child, parents, and school to implement the treatment plan.
3. Based on the available scientific evidence, stimulant medication, behavioral treatment, or both should form the basis of treatment to improve target symptoms.
4. Choice of medications should be tailored to the needs of the child.
5. Once adequate improvement in target symptoms is achieved, the child should be placed in an appropriate monitoring program.
6. Primary care providers should consider referral to behavioral health specialists when target symptoms are not improved despite therapy, or if other risk factors are present.
Core Elements 1. The diagnosis of ADHD is made objectively and is consistent with the American Academyof Pediatrics guideline for ADHD diagnosis. (Pediatrics May 2000; 105 (5):1158-1170)
2. The treating clinician formulates a treatment plan after consulting with the parents and school; and the treatment plan identifies specific target symptoms.
3. Once the diagnosis of ADHD is established, the treating clinician institutes a course of stimulantmedication or recommends formal behavioral therapy or both.
4. The treating clinician monitors children placed on stimulant medication for effectiveness and side-effects with a face-to-face office visit no less often than every six months.
5. If an adequate trial of stimulant therapy (including a second agent if needed) is not effective in improving target symptoms, consideration is given to referring the child to a behavioral healthspecialist.
To obtain the fullguideline and relat-ed practice tools
Internet:aap.org/policy/s0120.html
bluereview3-2006.qxp 5/12/2006 2:56 PM Page 5

Asthma DiabetesEndorsedGuidelines
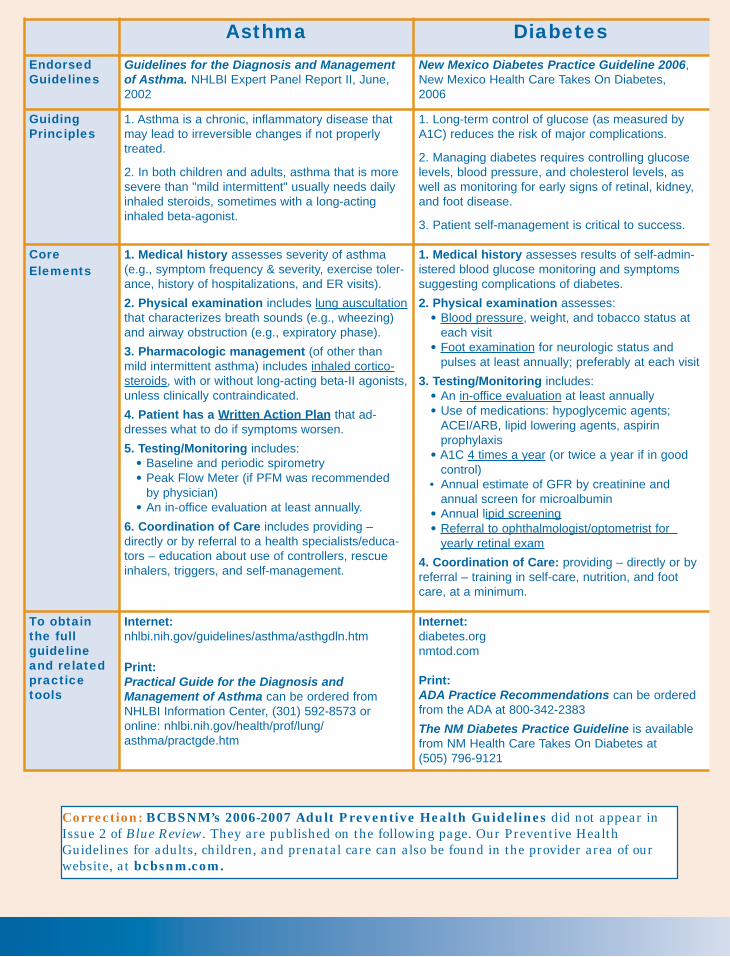
Guidelines for the Diagnosis and Managementof Asthma. NHLBI Expert Panel Report II, June,2002
New Mexico Diabetes Practice Guideline 2006,New Mexico Health Care Takes On Diabetes,2006
GuidingPrinciples
1. Asthma is a chronic, inflammatory disease thatmay lead to irreversible changes if not properlytreated.
2. In both children and adults, asthma that is moresevere than "mild intermittent" usually needs dailyinhaled steroids, sometimes with a long-actinginhaled beta-agonist.
1. Long-term control of glucose (as measured byA1C) reduces the risk of major complications.
2. Managing diabetes requires controlling glucoselevels, blood pressure, and cholesterol levels, aswell as monitoring for early signs of retinal, kidney,and foot disease.
3. Patient self-management is critical to success.
CoreElements
1. Medical history assesses severity of asthma(e.g., symptom frequency & severity, exercise toler-ance, history of hospitalizations, and ER visits).
2. Physical examination includes lung auscultationthat characterizes breath sounds (e.g., wheezing)and airway obstruction (e.g., expiratory phase).
3. Pharmacologic management (of other thanmild intermittent asthma) includes inhaled cortico-steroids, with or without long-acting beta-II agonists,unless clinically contraindicated.
4. Patient has a Written Action Plan that ad-dresses what to do if symptoms worsen.
5. Testing/Monitoring includes:• Baseline and periodic spirometry• Peak Flow Meter (if PFM was recommended
by physician)• An in-office evaluation at least annually.
6. Coordination of Care includes providing –directly or by referral to a health specialists/educa-tors – education about use of controllers, rescueinhalers, triggers, and self-management.
1. Medical history assesses results of self-admin-istered blood glucose monitoring and symptomssuggesting complications of diabetes.
2. Physical examination assesses:• Blood pressure, weight, and tobacco status at
each visit• Foot examination for neurologic status and
pulses at least annually; preferably at each visit
3. Testing/Monitoring includes:• An in-office evaluation at least annually• Use of medications: hypoglycemic agents;
ACEI/ARB, lipid lowering agents, aspirin prophylaxis
• A1C 4 times a year (or twice a year if in good control)
• Annual estimate of GFR by creatinine and annual screen for microalbumin
• Annual lipid screening• Referral to ophthalmologist/optometrist for
yearly retinal exam
4. Coordination of Care: providing – directly or byreferral – training in self-care, nutrition, and footcare, at a minimum.
To obtainthe fullguidelineand relatedpracticetools
Internet:nhlbi.nih.gov/guidelines/asthma/asthgdln.htm
Print: Practical Guide for the Diagnosis andManagement of Asthma can be ordered fromNHLBI Information Center, (301) 592-8573 oronline: nhlbi.nih.gov/health/prof/lung/asthma/practgde.htm
Internet:diabetes.org nmtod.com
Print:ADA Practice Recommendations can be orderedfrom the ADA at 800-342-2383
The NM Diabetes Practice Guideline is availablefrom NM Health Care Takes On Diabetes at (505) 796-9121
Essential Hypertension
Initial Antidepressant Treatmentof Adult Major Depression
EndorsedGuidelines
The Seventh Report of the Joint NationalCommittee on Prevention, Detection,Evaluation, and Treatment of High BloodPressure, National Heart, Lung, Blood Institute,NIH, 2003
Major Depression, Panic Disorder, and GeneralizedAnxiety Disorder in Adults in Primary Care, Institutefor Clinical Systems Improvement, 2001
Pharmacologic Treatment of Acute Major Depressionand Dysthymia, American College of Physicians, 2000
GuidingPrinciples
1. Treating essential hypertension greatly reducesrisk for MI, stroke, kidney failure, and prematuremortality. 2. The new Blood Pressure categories are:
3. Treat to goal: BP <140/90 or <130/80 ifdiabetes or chronic kidney disease.
4. The MAJORITY of patients will need TWOmedications to reach goal.
1. Major depression is a potentially life-threateningdisease that, in many cases, can be managed withantidepressant medication in a primary care setting.
2. Treatment of major depression requires that anti-depressants be used for a substantial initial period todetermine effectiveness.
3. Choice of antidepressants should be tailored to theindividual, based on the individual's behavioral andmedical condition and other medications.
4. Treatment of major depression requires follow-upvisits at least every month to check progress.
5. Referral to behavioral health specialists should bemade for atypical or high-risk cases, or cases unresponsive to trials of antidepressants.
CoreElements
1. When clinically indicated, the physician rulesout secondary hypertension.
2. The physician evaluates the patient at leastannually; more often if BP not controlled.
3. Treatment is consistent with JNC VIIrecommendations:
1. A diagnosis is made based on objective criteria, suchas DSM-IV. Clinical evaluation rules-out other medicaland psychiatric conditions that are similar to, or canmimic, major depression.
2. The patient with major depression is considered forantidepressant medication.
3. The choice of antidepressant is individualizedbased on concomitant medical and behavioral conditionsand known drug effects, side-effects, and drug-druginteractions.
4. An initial course of antidepressants is given for asufficient period, often up to twelve (12) weeks, toestablish efficacy.
5. The patient is evaluated at an office visit at leastmonthly during the initial course of therapy.
6. If antidepressant treatment is not successful, or ifthere are atypical or high-risk features, there is consulta-tion or referral to an appropriate mental health provider.
7. If the initial antidepressant therapy is successful,antidepressant treatment is continued for four totwelve months to reduce relapse risk.
To obtainthe fullguidelineand related practicetools
Internet:nhlbi.nih.gov/guidelines/hypertension/express.pdf
Print: JNC VII can be ordered from NHLBI InformationCenter (301) 592-8573 or online:nhlbi.nih.gov/guidelines/hypertension/jncintro.htm
Internet:icsi.org/guide/Anx.pdf acponline.org/sci-policy/depsummary.htm
Print:The ICSI guideline can be ordered at (952) 814-7060 or online: icsi.org/puborder.pdf
The ACP-ASIM guideline is published in Ann InternMed. 2000; 132:738-742
Category SBP mmhg DBP mmhgNormal <120 AND <80
Prehypertension 120-139 OR 80-89
Stage 1 HTN 140-159 OR 90-99
Stage 2 HTN >160 OR >100
ACEI: Angiotension Converting Enzyme Inhibitor
ARB: Angiotensin receptor blocker
BB: Beta blocker
CCB: Calcium channel blocker
BP Treatment
Pre HTN Lifestyle modification should be instituted
Stage 1 For most: Thiazide diuretic
Consider: ACEI, ARB, BB, CCB, or combination
Stage 2 For most: Two drug combinationUsual regimen: Thiazide diuretic PLUS ACEI, ARB,BB, or CCB
If not atgoal
If not <140/90 (or <130/80 if diabetes or kidney disease):
- Optimize doses
- Add additional medications
- If on diuretic + drugs at proper doses, consult with hypertension specialist
Correction: BCBSNM’s 2006-2007 Adult Preventive Health Guidelines did not appear inIssue 2 of Blue Review. They are published on the following page. Our Preventive HealthGuidelines for adults, children, and prenatal care can also be found in the provider area of ourwebsite, at bcbsnm.com.
bluereview3-2006.qxp 5/12/2006 2:56 PM Page 6
Asthma DiabetesEndorsedGuidelines
Guidelines for the Diagnosis and Managementof Asthma. NHLBI Expert Panel Report II, June,2002
New Mexico Diabetes Practice Guideline 2006,New Mexico Health Care Takes On Diabetes,2006
GuidingPrinciples
1. Asthma is a chronic, inflammatory disease thatmay lead to irreversible changes if not properlytreated.
2. In both children and adults, asthma that is moresevere than "mild intermittent" usually needs dailyinhaled steroids, sometimes with a long-actinginhaled beta-agonist.
1. Long-term control of glucose (as measured byA1C) reduces the risk of major complications.
2. Managing diabetes requires controlling glucoselevels, blood pressure, and cholesterol levels, aswell as monitoring for early signs of retinal, kidney,and foot disease.
3. Patient self-management is critical to success.
CoreElements
1. Medical history assesses severity of asthma(e.g., symptom frequency & severity, exercise toler-ance, history of hospitalizations, and ER visits).
2. Physical examination includes lung auscultationthat characterizes breath sounds (e.g., wheezing)and airway obstruction (e.g., expiratory phase).
3. Pharmacologic management (of other thanmild intermittent asthma) includes inhaled cortico-steroids, with or without long-acting beta-II agonists,unless clinically contraindicated.
4. Patient has a Written Action Plan that ad-dresses what to do if symptoms worsen.
5. Testing/Monitoring includes:• Baseline and periodic spirometry• Peak Flow Meter (if PFM was recommended
by physician)• An in-office evaluation at least annually.
6. Coordination of Care includes providing –directly or by referral to a health specialists/educa-tors – education about use of controllers, rescueinhalers, triggers, and self-management.
1. Medical history assesses results of self-admin-istered blood glucose monitoring and symptomssuggesting complications of diabetes.
2. Physical examination assesses:• Blood pressure, weight, and tobacco status at
each visit• Foot examination for neurologic status and
pulses at least annually; preferably at each visit
3. Testing/Monitoring includes:• An in-office evaluation at least annually• Use of medications: hypoglycemic agents;
ACEI/ARB, lipid lowering agents, aspirin prophylaxis
• A1C 4 times a year (or twice a year if in good control)
• Annual estimate of GFR by creatinine and annual screen for microalbumin
• Annual lipid screening• Referral to ophthalmologist/optometrist for
yearly retinal exam
4. Coordination of Care: providing – directly or byreferral – training in self-care, nutrition, and footcare, at a minimum.
To obtainthe fullguidelineand relatedpracticetools
Internet:nhlbi.nih.gov/guidelines/asthma/asthgdln.htm
Print: Practical Guide for the Diagnosis andManagement of Asthma can be ordered fromNHLBI Information Center, (301) 592-8573 oronline: nhlbi.nih.gov/health/prof/lung/asthma/practgde.htm
Internet:diabetes.org nmtod.com
Print:ADA Practice Recommendations can be orderedfrom the ADA at 800-342-2383
The NM Diabetes Practice Guideline is availablefrom NM Health Care Takes On Diabetes at (505) 796-9121
Essential Hypertension
Initial Antidepressant Treatmentof Adult Major Depression
EndorsedGuidelines
The Seventh Report of the Joint NationalCommittee on Prevention, Detection,Evaluation, and Treatment of High BloodPressure, National Heart, Lung, Blood Institute,NIH, 2003
Major Depression, Panic Disorder, and GeneralizedAnxiety Disorder in Adults in Primary Care, Institutefor Clinical Systems Improvement, 2001
Pharmacologic Treatment of Acute Major Depressionand Dysthymia, American College of Physicians, 2000
GuidingPrinciples
1. Treating essential hypertension greatly reducesrisk for MI, stroke, kidney failure, and prematuremortality. 2. The new Blood Pressure categories are:
3. Treat to goal: BP <140/90 or <130/80 ifdiabetes or chronic kidney disease.
4. The MAJORITY of patients will need TWOmedications to reach goal.
1. Major depression is a potentially life-threateningdisease that, in many cases, can be managed withantidepressant medication in a primary care setting.
2. Treatment of major depression requires that anti-depressants be used for a substantial initial period todetermine effectiveness.
3. Choice of antidepressants should be tailored to theindividual, based on the individual's behavioral andmedical condition and other medications.
4. Treatment of major depression requires follow-upvisits at least every month to check progress.
5. Referral to behavioral health specialists should bemade for atypical or high-risk cases, or cases unresponsive to trials of antidepressants.
CoreElements
1. When clinically indicated, the physician rulesout secondary hypertension.
2. The physician evaluates the patient at leastannually; more often if BP not controlled.
3. Treatment is consistent with JNC VIIrecommendations:
1. A diagnosis is made based on objective criteria, suchas DSM-IV. Clinical evaluation rules-out other medicaland psychiatric conditions that are similar to, or canmimic, major depression.
2. The patient with major depression is considered forantidepressant medication.
3. The choice of antidepressant is individualizedbased on concomitant medical and behavioral conditionsand known drug effects, side-effects, and drug-druginteractions.
4. An initial course of antidepressants is given for asufficient period, often up to twelve (12) weeks, toestablish efficacy.
5. The patient is evaluated at an office visit at leastmonthly during the initial course of therapy.
6. If antidepressant treatment is not successful, or ifthere are atypical or high-risk features, there is consulta-tion or referral to an appropriate mental health provider.
7. If the initial antidepressant therapy is successful,antidepressant treatment is continued for four totwelve months to reduce relapse risk.
To obtainthe fullguidelineand related practicetools
Internet:nhlbi.nih.gov/guidelines/hypertension/express.pdf
Print: JNC VII can be ordered from NHLBI InformationCenter (301) 592-8573 or online:nhlbi.nih.gov/guidelines/hypertension/jncintro.htm
Internet:icsi.org/guide/Anx.pdf acponline.org/sci-policy/depsummary.htm
Print:The ICSI guideline can be ordered at (952) 814-7060 or online: icsi.org/puborder.pdf
The ACP-ASIM guideline is published in Ann InternMed. 2000; 132:738-742
Category SBP mmhg DBP mmhgNormal <120 AND <80
Prehypertension 120-139 OR 80-89
Stage 1 HTN 140-159 OR 90-99
Stage 2 HTN >160 OR >100
ACEI: Angiotension Converting Enzyme Inhibitor
ARB: Angiotensin receptor blocker
BB: Beta blocker
CCB: Calcium channel blocker
BP Treatment
Pre HTN Lifestyle modification should be instituted
Stage 1 For most: Thiazide diuretic
Consider: ACEI, ARB, BB, CCB, or combination
Stage 2 For most: Two drug combinationUsual regimen: Thiazide diuretic PLUS ACEI, ARB,BB, or CCB
If not atgoal
If not <140/90 (or <130/80 if diabetes or kidney disease):
- Optimize doses
- Add additional medications
- If on diuretic + drugs at proper doses, consult with hypertension specialist
Correction: BCBSNM’s 2006-2007 Adult Preventive Health Guidelines did not appear inIssue 2 of Blue Review. They are published on the following page. Our Preventive HealthGuidelines for adults, children, and prenatal care can also be found in the provider area of ourwebsite, at bcbsnm.com.
bluereview3-2006.qxp 5/12/2006 2:56 PM Page 6

The 2006-2007 BCBSNM/HMONM ClinicalPractice Guidelines are highly focused summariesof national recommendations designed for the busypractitioner. These CPGs have been approved bypracticing New Mexico physicians who serve on theBCBSNM Quality Improvement Professional ReviewCommittee. These reflect care that is appropriate formost persons with the disease, however they shouldnot substitute for clinical judgement in individualcases. Variations from the guidelines will be clinical-ly indicated in some patients.
Certain elements within these CPGs, however, areconsidered core elements and BCBSNM/HMONMannually measures how network physicians performin core elements as a basis for ongoing clinical quali-ty improvement and performance-based recognition.
Clinical Practice Guidelines are enclosed here andthe following two pages for the following five conditions:
• Treatment of ADHD in School-Age Children • Asthma• Diabetes• Hypertension• Initial Antidepressant Treatment of Adult Major
Depression
They can also be found in the provider area of bcbsnm.com, under the UM/QI/MedicalManagement heading. Additional information on BCBSNM Blue Care Connection DiseaseManagement is at bcbsnm.com/haw/haw_disease_mgt.htm.
2006-2007 Clinical Practice Guidelines
Treatment of ADHD in School-Age ChildrenEndorsedGuidelines
Clinical Practice Guideline: Treatment of the School-Aged Child with ADHD, AmericanAcademy of Pediatrics as published in: Pediatrics Oct 2001; 108(4):1033-1044
Guiding Principles 1. ADHD in children 6 through 12 years of age requires both a structured approach to diagnosis and the development of a specific treatment plan with concrete goals.
2. The treating clinician should work in collaboration with the child, parents, and school to implement the treatment plan.
3. Based on the available scientific evidence, stimulant medication, behavioral treatment, or both should form the basis of treatment to improve target symptoms.
4. Choice of medications should be tailored to the needs of the child.
5. Once adequate improvement in target symptoms is achieved, the child should be placed in an appropriate monitoring program.
6. Primary care providers should consider referral to behavioral health specialists when target symptoms are not improved despite therapy, or if other risk factors are present.
Core Elements 1. The diagnosis of ADHD is made objectively and is consistent with the American Academyof Pediatrics guideline for ADHD diagnosis. (Pediatrics May 2000; 105 (5):1158-1170)
2. The treating clinician formulates a treatment plan after consulting with the parents and school; and the treatment plan identifies specific target symptoms.
3. Once the diagnosis of ADHD is established, the treating clinician institutes a course of stimulantmedication or recommends formal behavioral therapy or both.
4. The treating clinician monitors children placed on stimulant medication for effectiveness and side-effects with a face-to-face office visit no less often than every six months.
5. If an adequate trial of stimulant therapy (including a second agent if needed) is not effective in improving target symptoms, consideration is given to referring the child to a behavioral healthspecialist.
To obtain the fullguideline and relat-ed practice tools
Internet:aap.org/policy/s0120.html
bluereview3-2006.qxp 5/12/2006 2:56 PM Page 5

PROVIDER REPRESENTATIVESThis team handles general questions for all areas
CENTRAL REGIONNetwork Contract Representative Michelle Quintero, (505) 816-2158
Lead Provider RepresentativeLiz Martinez, (505) 816-2161
SOUTHERN REGIONNetwork ContractRepresentative
Jill Billingsley, (505) 816-2143
Lead Provider RepresentativeJan Montoya, (505) 816-2303
NORTHERN REGIONNetwork Contract Representative
Joann Ireland, (505) 816-2159
Lead Provider RepresentativeGina Gutierrez, (505) 816-2156
PROFESSIONAL CONTRACTINGIncluding Allied Health Practitioners
HOSPITAL CONTRACTINGIncluding Acute Care, Behavioral Health,
and Specialty Hospitals
Network Contract Representative George Salaiz, (505) 816-2139
Lead Provider RepresentativeGina Gutierrez, (505) 816-2156
ANCILLARY CONTRACTINGDivided by Type of Ancillary Service Including
Vendors
Network Contract RepresentativeRick Bogle, (505) 816-2145
Lead Provider RepresentativeJan Montoya, (505) 816-2303
•DME, Home Health, Hospice, Home IV, and supplies (e.g., mastectomy, hearing, prosthetic/orthotic)
•Freestanding and Statewide Labs•Rehab. Hospitals (excluding Albuquerque Rehab.)•Air Ambulance•Radiology Providers•Freestanding Ambulatory Surgical Centers South of I-40•McKesson Specialty Pharmacy
Network Contract Representative Joyce Hamblet, (505) 816-2146
Lead Provider RepresentativeLiz Martinez, (505) 816-2161
•Skilled Nursing Facilities •Birthing Centers•Diabetes/Nutrition Centers •Sleep Study Centers•Cardiac Rehab. Facilities •Bone Density Centers •Dialysis Freestanding Facilities •Freestanding Ambulatory Surgical Centers North of I-40•Mesa Mental Health
Network Services and related service area contacts
Our Provider Representatives are available to assist you Monday - Friday, 8 a.m. to 5 p.m.General department telephone numbers: (505) 837-8800 or toll-free at 800-567-8540Our direct fax numbers: (505) 816-2688 or 866-290-7718
As the health care industry moves toward apaperless environment, payers have designedprograms to complement and/or be used withthe Electronic Remittance Advice (ERA). Thereare two products to assist you:
Electronic Payment Summary (EPS). BCBSNMhas designed an electronic format of the paperProvider Claim Summary, the EPS, which canbe used in coordination with the ERA. The EPSis an easy-to-read electronic print image of thepaper format you currently receive in the mail.You must enroll to receive the ERA and willthen automatically receive the EPS. For anERA enrollment form from BCBSNM, visitthinedi.com/enrollment.htm. The EPS filewill be placed in your electronic mailbox alongwith your ERA file.
Medicare Remit Easy Print. The Centers forMedicare & Medicaid (CMS) has designed aproduct called Medicare Remit Easy Print(MREP). If you are still receiving the StandardPaper Remittance Advice from Medicare (SPR),you can request cancellation of the paper and acopy of your remittance using the MREP soft-ware. For information on MREP, seewpsic.com/edi/pdf/mrep_overview.pdf, orcontact WPS Medicare at 877-567-7261.
Attention ERA users: We’re eliminating paper
Note: Paper remittances will eventually beeliminated. BCBSNM will discontinue thepaper after 30 days, and Medicare hasinformed our THIN Clearinghouse it will notmake the SPR available through the mail.
Altering medical recordsBCBSNM reviewers occasionally receive medical records with clinical information thathas been scribbled over, “whited out,” or other-wise altered. In a recently denied claim,records from a single visit were submittedtwice, with substantive changes made in whatappeared to be an effort to build criteria for aparticular medication, yet no initials, dates, orappropriate documentation accompanied therecord changes.
Altering medical records may have significantlegal implications, including medical fraud.While it is sometimes appropriate to make acorrection or change, such a change should bea made by a single line through the erroneousinformation, dated, and initialed or signed.The Fraud/Special Investigations Division of
BCBSNM and HCSC may become involvedwhen documents have been altered.
In the situation above, the BCBSNM medicaldirector contacted the provider who expressedsurprise and embarrassment about the matter.A support person in his office had made therecords change without his knowledge, and hewas very aware about the potential gravity ofaltering medical records. This was deemed anacceptable explanation and no further actionwas initiated by BCBSNM.
BCBSNM recommends that all medical per-sonnel train their staff on the correct way tochange medical documents and of the potentialimplications of inappropriately altering them.Providers are encouraged to consult their legaladvisors with any questions.
Reimbursement issue — “letters of medical necessity” Clinical documents — medical records thatestablish a relationship between the requestedproduct or service and the member's clinicalsituation — are generally required for determination of medical necessity. “Letters ofmedical necessity” — whether on template furnished by a product’s manufacturer or distributor or an original — are generally considered inadequate.
If you submit a “letter of medical necessity”with your request for approval of a product orservice without supporting clinical documents,
BCBSNM staff will likely request the medicalrecords, delaying processing, and potentiallydelaying your reimbursement. Or if medicalrecords are not furnished, the request may bedenied due to lack of adequate clinical documentation.
Note: The term,“letter of medical necessity,”is a misnomer. Medical necessity is notestablished by a letter, but by documentationin a contemporaneously produced medicalrecord. A “letter of medical necessity” is oftenextraneous.
Claims filing cornerBoniva injectionsBecause the injectable drug Boniva is new anddoes not yet have a published code, submit claimsusing the J3490 unclassified drug code, along withthe written description and NDC (National DrugCode) number. Boniva will be priced per AWP untila code and ASP are established and published.
Oral Boniva (non-injectable) should be submittedaccording to the member’s Pharmacy benefit.
Remember: Injectable Boniva requiresPrior Authorization because strict criteriamust be met in order for this drug to be covered by BCBSNM.
Coming soon!Annual RBRVS updates. All participatingproviders will soon receive a letter announcingupdates to the Maximum Allowable Fee Scheduleof the 2006 Resource Based Relative Value System(RBRVS) Relative Value Units (RVUs). Theseupdates will be effective for dates of service July 1,2006, and forward. Included are Medicare flat feesfor clinical laboratory and durable medical equip-ment, which will be used in our reimbursementmethodology. Please watch your mail.New plan: Blue Transitions. BCBSNM will soonbe offering a new health care plan, Blue Transitions,for New Mexicans who need a short-term policy fortransitional periods, such as between jobs, after gradua-tion, or recently moved to New Mexico. More detailscoming soon!
bluereview3-2006.qxp 5/12/2006 2:56 PM Page 4

Medical policy updatesOnce approved, new or revised medical policies areposted on our website the first day of each month,with their effective dates indicated. You’ll find themost complete and up-to-date information on bothactive and pending medical policies in the provider
area of our websute, bcbsnm.com, under ProviderLibrary. New or revised medical policies developedsince the last Blue Review are summarized below.Please contact Health Services at (505) 816-2093with any questions.
OFFICE StaffIssue 3 - 2006 (May-June)bcbsnm.com
BCBSNM completed the first phase of the transi-tion to Centers for Medicare & Medicaid Services(CMS) consolidated Medicare crossover process lastNovember. The transition of Coordination ofBenefits Contractor (COBC) crossover on supple-mental claims used for calculating secondary payment liability was completed on April 3, 2006.We have appreciated your patience during theCOBC transition period. Here are a few highlightsof the COBC transition:
Enhancements: Under the new COBC process,supplemental claims will continue to cross over formembers in the BCBSNM eligibility files. Butclaims will now cross over to the supplementalinsurer from one party, the COBC contractor,rather than the various individual Medicare contractors.
Full Transition Date: Medicare Parts A and Bclaims processed on or after April 3, 2006, will crossover only after the claims have left Medicare payment floors. Please do not submit your supple-mental claims to BCBSNM prior to release of theMedicare payment floors:
• Electronic claims processed will be released to the supplemental insurer after a 14-day payment floor.
• Paper claims processed will be released after the new 29-day payment floor instituted under the Deficit Reduction Act (DRA).
Mass Adjustments: On February 10, 2006, CMSannounced that the DRA prevents payments forphysicians’ services delivered on or after January 1from being reduced by a negative update of 4.4 per-cent. January claims that have already been paidand have crossed over to the supplemental insurersare being adjusted by Medicare. All mass adjust-ments are expected to be completed by July 1, 2006.Since BCBSNM has elected to receive the massadjustments via the crossover files, please do notsubmit these adjustments on paper.
Medicare Claims with No Liability: Medicareclaims paid at 100% with no additional beneficiaryliability will not cross over. Medicare claims denied
at 100% with no additional beneficiary liability alsowill not crossover. In instances where there is noliability, please do not submit the claim to BCBSNM.
Although most claims will continue to seamlesslycross over, according to CMS, if claims fail to crossover due to claim data errors originating at theMedicare contractor site, the Medicare contractorswill send notification to the providers advisingthem that their claim did not cross over to thepatient's supplemental insurer due to claim dataerrors. If you receive this type of Medicare notifica-tion, please submit the supplemental claim elec-tronically to BCBSNM.
NPI updates now onlineThe Health Insurance Portability andAccountability Act of 1996 (HIPAA) mandated theadoption of standard unique identifiers for healthcare providers — the National Provider Identifier(NPI) — by May 23, 2007. The countdown to NPIimplementation is currently underway at BCBSNMand our goal is to make this transition as seamlessas possible for our providers. To assist you, a newlink, NPI (National Provider Identifier), has beenadded to the provider area of our website, bcbsnm.com. Information now available on our website includes:
• NPI overview• How to apply for your NPI• Links to other helpful websites• Contact information • Frequently Asked Questions• An NPI submission form (for providers who
currently have a BCBSNM provider number)
We will continue to provide updates on our websiteand in Blue Review. You will also receive notifica-tion by mail regarding how to submit your NPI tous. In the meantime, please do not begin usingyour NPI on electronic transactions untilBCBSNM has communicated an effective dateand instructions on how to proceed.
Coordination of Benefits Contractor (COBC) crossover updateEFF. DATE POLICY # POLICY NAME
06/01/2006 DME101.010 Wheelchairs and Accessories
06/01/2006 DME104.012 Lower Limb Prosthetics, Including Microprocessor Knees
06/15/2006 MED201.026 Surface Electrical Stimulation
06/15/2006 SUR712.004 Percutaneous Intervertebral Techniques to Treat Chronic Discogenic Back Pain
06/15/2006 THE801.006 Plasma Exchange (Plasmapheresis)
06/15/2006 DME104.001 Prosthetics, Except Lower Limb Prosthetics
07/15/2006 SUR706.009 Sleep Related Breathing Disorders, Medical and Surgical Management
07/15/2006 SUR702.009 Patient Controlled Analgesia
07/15/2006 MED207.104 Lyme Disease (Borrelia Burgdorferi) Management
07/15/2006 PSY301.014 Autism Spectrum Disorders (ASD)
07/15/2006 SUR716.017 Mastectomy for Gynecomastia
07/15/2006 DME101.001 Hospital Beds and Related Equipment
Special Beginnings® prenatalprogram supports your careBCBSNM provides our Special Beginnings prenatalprogram to members whose health plans includematernity coverage. This program provides additional support during pregnancy and includes educational materials, a 24-hour nurse line, healthrisk assessment, and case management for high-risk pregnancies. Members can receive informationonline via our website or through the mail.
Members are automatically referred to the SpecialBeginnings program when a provider’s office callsfor precertification for delivery or a referral to anOB specialist. Members are then contacted andoffered the option to participate. Members may alsoself-refer.
If you would like more information about SpecialBeginnings, please call the Health Services depart-ment at 800-325-8334.
Blue Care ConnectionSM DiseaseManagement programsBCBSNM continues to provide disease managementprograms for diabetes; asthma; COPD; and cardiacconditions such as CAD, CHF, and hypertension.For more information about our programs and making patient referrals, please call 816-2230 ortoll-free at 866-252-8106. Or, you may email us [email protected].
New! Spanish PHGsThe BCBSNM 2006-2007 Preventive HealthGuidelines for adults and children members arenow available in Spanish. Members and providerscan access ready-to-print versions in the memberand provider areas of our website, bcbsnm.com.
bluereview3-2006.qxp 5/12/2006 2:56 PM Page 3

Brand-Name Medications moving to the Tier 3 Copayment Effective October 1, 2006THIRD-TIER BRAND SECOND-TIER ALTERNATIVES FIRST-TIER GENERIC ALTERNATIVES
Blood glucose test stripsFASTTAKE*ONE TOUCH II/BASIC/PROFILE*ONE TOUCH ULTRA*SURESTEP*
ACCU-CHEK AVIVA, ACCU-CHEK COMPACT, FRESTYLE, FRESTYLE FLASH, PRECISION QID, PRECISION XTRA blood glucose test strips
CAPITAL WITH CODEINECARBATROLCLOZAPINE 12.5mg, 50mg, 200mg tabletsDEXTROSTAT 10mgDILANTIN 100mg
acetaminophen and codeine oral sol 120 12mg/5ml
TEGRETOL XR 100mg, 200mg, 400mg carbamazepine immediate release tabletsclozapine 25mg, 100mg tabletsdextroamphetamine immediate release tabs phenytoin sodium, extended caps, 100mg
ELIXOPHYLLINFLEXERIL 5mgLITHIUM CARBONATE 150mg capsules
marketed by RoxaneLITHIUM CARBONATE 300mg tablets,
600mg capsulesMECLOFENAMATE
NAVANE 20mgORAMORPH SRPARNATEROCALTROLROXICET (oxycodone/acetaminophenoral solution 5-325mg/5 mL)
ZITHROMAX*ZYPREXA
ZYPREXA ZYDIS
theophylline elixircyclobenzapyrine tablets, 5mglithium carbonate 150mg capsules
lithium carbonate 300mg capsules
diclofenac sodium, ibuprofen, naproxen
thiothixene capsules, 2mg, 5mg, 10mg
morphine sulfate extended-release tabsNARDIL
calcitriol caps, oral solutionhydrocodone/acetaminophen elixir
7.5-325mg/15 mL
azithromycin tablets, 250mg, 500mg, 600mgGeodon, RISPERDAL, RISPERDAL
M-TAB, SEROQUELGeodon, RISPERDAL, RISPERDAL
M-TAB, SEROQUEL
ACTOPLUS MET FRESTYLE, FRESTYLE FLASH PARCOPACELONTIN blood glucose test strips PATANOLCHLORAL HYDRATE supp GEODON PRECISION QID, PRECISION XTRACODEINE PHOSPHATE sol tab KALETRA tablets blood glucose test stripsCYPROHEPTADINE syrup MESTINON syrup RENAGELDEXCHLORPHENIRAMINE MESTINON TIMESPAN SUBOXONE
MALEATE syrup METAPROTERENOL tab SUBUTEXDIAZEPAM oral sol, 1mg/mL MYFORTIC tablets TRAVATANEMTRIVA oral sol ORAP
Brand-Name Medications Added to Second-Tier Copay Effective April 1, 2006
* EFFECTIVE APRIL 1, 2006
The BCBSNM and Prime TherapeuticsPharmacy and Therapeutics Committee meton February 28, 2006, and recommended thefollowing changes and additions to the BCBSNM Drug List, effective October 1, 2006except where noted. The brand-name
prescription drugs listed will continue to beavailable to our members but members willpay the higher third-tier copayment effectiveOctober 1, 2006. In the table below, we’veincluded generic alternative medications thatare on our Drug List.
Drug List updates
Our health plan members have rights andresponsibilities that are listed in their BenefitBooklet or Member Handbook. Most members
can also access these documents on our web-site, bcbsnm.com.
Member rights and responsibilities
2006 BlueCard® Program Satisfaction Survey Our BlueCard program allows members of otherBlue Plans to obtain health care services while inanother plan’s service area. That means BCBS members visiting New Mexico can receive the benefits of the BCBS Plan listed on their insurancecard, and access our local BCBSNM provider network and savings.
As a participating BCBSNM provider, your satisfac-tion is a top priority to us. We value the care youprovide to our members. We conduct annual surveysto assess your satisfaction with the BlueCard pro-gram and your feedback allows us to identify waysto serve you more effectively. Last year’s surveynoted continued improvement in provider satisfac-tion with the program, specifically in these areas:
• Claims accuracy and timeliness• Satisfaction with resolving problem claims • Electronic eligibility verification • Customer service• Provider education
In 2005, we implemented the following initiatives tobetter serve you:
• Increased internal employee training resources to maximize quality of service
• Provided internal education to BCBSNM provider relations staff
• Featured ongoing articles in the Blue Review
To continue evaluating our performance, we haveasked The Response Center, an independentresearch company, to conduct telephone interviewson our behalf. They will contact a randomly selectedsample of providers who provided care for BlueCardmembers during 2005 and will ask to speak with the person in your office who is most knowledgeableabout filing BCBS claims and/or someone in thebilling department. The first set of telephone inter-views is currently in progress, and a second set willbe scheduled in the fall.
Thank you in advance for taking the time to provideus with your feedback.
If you have questions about the BlueCard Programor have suggestions for improvement, please emailus at [email protected]. Or, you may callthe BlueCard Provider Service Unit at 800-222-7992.
The 2006-2007 issue of Blue News for Kids has justbeen released. This 4-page newspaper addresseschildren’s health with fun, upbeat stories gearedfor kids and can supplement health care providers’preventive health education efforts. This issueincludes articles on: immunizations, dental care,growth and development, body image, hearing safety, eating disorder prevention, stress, bullies,gun safety, what to do in an emergency, sleep,nutrition, cooking, sun safety, and making physicalactivity fun.
Providers may receive free copies for their officesby contacting Network Services at 837-8800 or800-567-8540.
Blue News for Kids
Have you discovered how much BCBSNM has madeavailable online to provide better service to our net-work providers? Please visit the provider area atbcbsnm.com for the most complete and up-to-datenews and information on topics of concern to you.Among the resources you’ll find valuable: theProvider Library (with the current Blues ProviderReference Manual, medical policy information, and
forms), UM/QI Medical Management (with clini-cal guidelines, Blue Care Connection DiseaseManagement program information, and more),Provider Network, Pharmacy information,Medicaid Utilization Review information, BlueMedicare PPO page, Electronic Commerce andClaims Filing information, and a new NPI(National Provider Identifier) page.
Instant access online just for our network providers
bluereview3-2006.qxp 5/12/2006 2:56 PM Page 2

PRSRTSTDU.S. POSTAGE
PAIDPERMITNO. 581
CHICAGO, IL
INSIDE this issue1 2006 Provider Satisfaction Survey1 BCBSNM/HMONM behavioral health services 2 2006 BlueCard® Program Satisfaction Survey2 Instant access online 2 Blue News for Kids3 Office Staff: COBC crossover update 3 NPI updates now online4 Claims filing corner: Boniva injections4 Network Services contacts and related service areas4 Coming soon! RBRVS updates/Blue Transitions 5-7 2006-2007 Clinical Practice Guidelines8 2006-2007 Adult Preventive Health Guidelines 9 Altering medical records 9 Reimbursement issue “letters of medical necessity” 9 Attention ERA users: We’re eliminating paper 10 Medical policy updates10 Blue Care ConnectionSM Disease Management 10 Special Beginnings® prenatal program10 New! Spanish PHGs11 2006 Drug List updates11 Member rights and responsibilities
P.O. Box 27630Albuquerque, NM 87125-7630
A Division of Health Care Service Corporation, a Mutual LegalReserve Company, an Independent Licensee of the Blue Crossand Blue Shield Association.
BLUEReviewISSUE 3 - 2006
ISSUE 3 - 2006 (May/June) bcbsnm.com
2006 Provider Satisfaction SurveyOur annual provider survey is an importanttool used to develop plans for improving andmaintaining provider satisfaction. This year’sprovider survey will be mailed to you in May.You’ll have the opportunity to rate our performance in a number of areas such astimeliness of claims processing, frequencyand effectiveness of provider visits, variety ofdrug list, the preauthorization process, and
continuity and coordination issues. You willalso be asked for general input on ways wecan serve you better in the future.
Several quality review committees analyzeprovider survey results and utilize providerresponses to formulate improvement plans.We appreciate and encourage your continuedfeedback as a valued member of our providercommunity.
Special InsertThe latest issue of Diabetes Resourcestitled “A1C: An Update on ClinicalRelevance” is a special insert in thisnewsletter. More diabetes informationis available at bcbsnm.com in theprovider area under DiabetesGuidelines and Reference.
BCBSNM’s behavioral health network isgrowing and stronger than ever. Mesa MentalHealth (MMH) administers many of the BCBSNM/HMONM plans and maintains anextensive network of nearly 1,000 behavioralhealth providers throughout the state. Ourbehavioral health network has increased bynearly 150 practitioners in the past year toensure the availability of services to meetmembers’ needs.
A diverse group of independently licensedsocial workers, mental health therapists, substance abuse counselors, psychologists,psychiatrists, and other behavioral healthspecialists contract through MMH.
BCBSNM and MMH partner on several proj-ects of special importance to New Mexicans.
The Alcohol and Other Drug Projectisdesigned to enhance aftercare for membersneeding ongoing chemical dependency services after discharge from a medical facility. It includes an innovative email notification system and new collaborativecommunications so that referrals are initiatedprior to hospital discharge.
Another valuable joint project of BCBSNMand MMH is the Post-Partum DepressionPrevention Project. It identifies women with significant risk factors for serious depressionand refers them for behavioral health
services. To date, more than 500 prenatalwomen have been supplied with the PPD educational brochure. You may preview andprint this brochure at mesamentalhealth.com/pdf/quality/ppd_newsletter.pdf. MMH is now waiving thecopay for initial assessments to the PPD program in orderto remove anyimpediments forparticipants.Providers, how-ever, will bereimbursed 100%for the initialassessment bybilling underCPT code 99420.
For more information anda provider directory, visitbcbsnm.com.Customer Servicestaff are alsoavailable to answer questions about mentalhealth benefits and assist in making appoint-ments with mental health providers by calling 816-6792or toll-free at800-583-6372.
BCBSNM/HMONM behavioral health services
bluereview3-2006.qxp 5/12/2006 2:56 PM Page 1

The Issue:
The A1C remains the best way for clinicians to monitor the long-term blood glucose control oftheir patients with diabetes. It corresponds to the average glucose over a 3-month period.For patients with Type 2, every 1-point fall in A1C is associated with a reduction in relative riskfor microvascular complications by 35%, diabetes-related deaths by 25%, and MI by 14%.For patients with Type 1, every 1-point fall in A1c is associated with a reduction in relative riskfor retinopathy by 38%, nephropathy by 25%, and neuropathy by 14%. Reduction in risk for macrovascular complications is not as clearly correlated with A1C.Many people with DM don't understand A1C. Some providers don't use the term “A1C.” Referring to it as “the test that gives your average sugar over the past three months” may bemore helpful. According to a recent study only 25% of people with diabetes know their A1C.
The Current Clinical Recommendation:
The New Mexico Health Care Takes On Diabetes 2006 Guideline recommends that all people withdiabetes have an A1C test 2- 4 times per year. The goal for patients in general is A1C<7%. Thefollowing are important considerations:
The A1C goal for a typical patient is as close to normal (A1C<6%) as possible withoutsignificant hypoglycemia.Less stringent treatment goals may be appropriate for patients with history of severehypoglycemia, patients with limited life expectancies, very young children or older adults, andindividuals with comorbid conditions.
Table 1. How to Interpret the A1C
P.O. Box 3548Albuquerque, NM 87190
(866) 796-9121(505) 796-9121
A quarterly publication for clinicians caring for people with diabetes - VA quarterly publication for clinicians caring for people with diabetes - Vol. 6 No. 1, 2006ol. 6 No. 1, 2006
In each issue of DiabetesResources we have providedspecific information aboutmanagement for diabetes,including important tests andresources to help reducecomplications associated withthe disease. Information isincluded about the ABCs ofdiabetes: A1C testing 2-4times per year, Bloodpressure screening at everyvisit, and annual Cholesteroltesting. Additional clinicalinformation is also provided.A dilated eye exam, sensoryfoot exam and screening forkidney disease eachrecommended annually.Attention to these risk factorsreduces the chance forcardiac, renal, eye andvascular disease secondary todiabetes.
In support of the New MexicoDiabetes Practice Guideline2006, please see the reverseside of Diabetes Resourcesfor recommendations for careincluding resources and toolsthat can help in your effortsto provide education andsupport among your patientswith diabetes.
Diabetes ResourcesPractical Information for New MexicoHealth Care Professionals
Check www.nmtod.com fororganizations that have graciouslyprovided funding for DiabetesResources.
New Mexico Health Care Takes OnDiabetes is a broad coalition ofNew Mexico's diabetes careprofessionals, New Mexico HealthPlans, the New Mexico Departmentof Health, and the New MexicoMedical Review Association, withtechnical and administrative supportfrom the American DiabetesAssociation.
A1C: An Update on Clinical Relevance
450
400
350
300
250
200
150
100
50
05 6 7 8 9 10 11 12 13 14
Mean PlasmaGlucose(mg/dl)
A1C (%)
135170
415380
345310
275240
205

How to Interpret the A1C—A1C is the most important indicator of glucose control indiabetes, but it can be difficult to interpret the clinical relevance of an A1C value. The goal isan A1C <6.0%, but do you know why? Did you know an A1C level of 9.0% equates to an
average glucose level of 240 mg/dl? Do you know how tointerpret the A1C when patients have repeated episodes ofhypoglycemia or when they are anemic? “How to Interpret theA1C” will help answer those questions and will show you howA1C levels relate to average blood glucose levels and clinicalcomplications. This chart may help clinicians explain theimportance of A1C to their patients by relating A1C to “averagesugar level.” This invaluable “memory jogger” can bedownloaded free from the New Mexico Health Care Takes OnDiabetes website.
A1C Tool for Patients—The New Mexico Department of Health Diabetes Preventionand Control Program has produced an excellent patient education brochure that explains A1C
in simple terms. Written at a fifth grade reading level, itincorporates graphics to enhance patient understanding. Asection called “Steps to Take” assists the patient and provider indocumenting diabetes self-management goals related toimproving the patient's A1C. A color version can be laminatedor put in a plastic sleeve for repeated use in one-on-one trainingwith patients. A black-and-white version can be easily copiedand given to patients to take home. Spanish translations are alsoavailable. There are no copyright restrictions. This form can be
found on the New Mexico Health Care Takes On Diabetes website.
A1C Analyzers for Office or Home Use—It is possible to perform A1C testing inyour office. The advantage in having an A1C Analyzer in the office is that it allows healthcareprofessionals to make immediate diabetes management adjustments during the patient visit.In-home A1C testing is also available, although its role in improving diabetes outcomes isunknown. The American Diabetes Association takes no position on in-home testing. If yourpatients use in-home testing, it may be valuable to encourage them to discuss the results withyou.
To review different manufactures of A1C analyzers for office or home use there is a websitethat compares A1C Analyzers. Go to: Hemoglobin A1C Analyzers - Diagnostics ProductMatrix - Medcompare to review current products on the market for office use.
Per the Medcompare website only Bayer Diagnostic offers a combination analyzer thatgives both A1C and microalbumin/creatinine test results.
NMHCTOD does not endorse any particular manufacturer. Check with individual health plans for information on insurancecoverage.
Resources for CliniciansThe following resources are FREE and can be downloaded from the New Mexico HealthCare Takes On Diabetes website at wwwwww..nnmmttoodd..ccoomm. For further information contactCharm Lindblad, Executive Director, at 550055..779966..99112211 or toll-free 11..886666..779966..99112211.
Advisory Board:Nathaniel G. Clark, MD, MS, RD
National VP, Clinical Affairs American Diabetes Association
Donna Tomky, MSN, RN, C-ANP, CDENurse Practitioner, Dept. of Endocrinology
& Diabetes, Lovelace Sandia Medical Center
Judith Gabriele, MPHProgram Manager, Diabetes Prevention
and Control Program, New MexicoDepartment of Health
Jeremy Gleeson, MD, FACP, CDE Medical Director, Dept. of Endocrinology &Diabetes, Lovelace Sandia Medical Center
JoEllen Habas, MD Endocrinology, Diabetes and Metabolism
Presbyterian Medical Group
Websites—The editorial committee has identified websites that you may find informative:National Diabetes Education Program: wwwwww..nnddeepp..nniihh..ggoovvAmerican Diabetes Association: wwwwww..ddiiaabbeetteess..oorrgg National Institutes of Health: wwwwww..ddiiaabbeetteess..nniiddddkk..nniihh..ggoovvAmerican Heart Association, Heart of Diabetes Program:wwwwww..aammeerriiccaannhheeaarrtt..oorrgg//ddiiaabbeetteess NM Department of Health, Diabetes Prevention and Control Program:wwwwww..ddiiaabbeetteessnnmm..oorrgg
These websites may be accessed directly or through the New Mexico Health Care Takes OnDiabetes website* wwwwww..nnmmttoodd..ccoomm
*Please note that these websites do not necessarily represent the views of NMHCTOD. They are listed for your referenceand convenience. NMHCTOD does not evaluate websites for content accuracy or application to any clinical situation.
Editorial Committee:Patty Anello, RN, BSN
Art Bachechi, RNJeanine Ertel, MPH
Diane Fields, LISW, CCMMary Fluckey, MS, CHES, CPHQ
JoEllen Habas, MDM. L. Johnston, MS, RD, CDE
Charm Lindblad, MHABruce A. Mann, MD, FACP
Erin McDonald BicknellLaura Parker, RN, CDELeslie Shainline, RN, MS
Graphic Layout: Anna Dykeman, MANew Mexico Medical Review Association
Copyright 2006 by New Mexico HealthCare Takes On Diabetes. May bereproduced without restriction in NewMexico and for educational purposes.Permission for other use outside NewMexico may be obtained at505.796.9121. These materials weredeveloped under a contract with the Stateof New Mexico, Department of PublicHealth, Public Health Division.
Printed 2006


















