Blood Pressure and Flow Overview emphasis on SYSTEMIC CIRCUIT Source of pressure Modifies pressure...
48
• Blood Pressure and Flow Overview emphasis on SYSTEMIC CIRCUIT Source of pressur e Modifie s pressur e Perfuses tissues with blood, Maintains flow to cappilari Returns blood to heart
-
Upload
verity-morrison -
Category
Documents
-
view
221 -
download
1
Transcript of Blood Pressure and Flow Overview emphasis on SYSTEMIC CIRCUIT Source of pressure Modifies pressure...

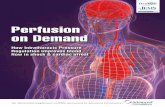
• Blood Pressure and Flow Overview
emphasis on SYSTEMIC CIRCUIT
Source of pressure
Modifies pressure
Perfuses tissues with
blood,Maintains
flow to cappilaries
Returns blood to
heart
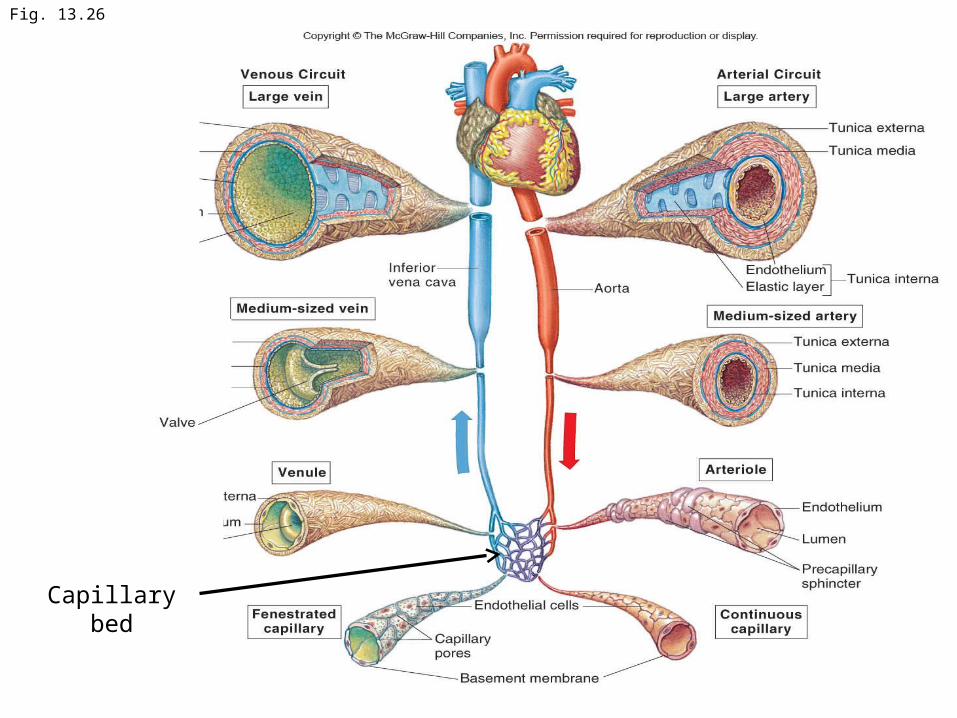
Fig. 13.26
Capillary bed

BLOOD FLOW• Blood flows from high pressure areas to low pressure areas
• Blood flows through vascular system because of these pressure differences
• Arteries arterioles capillaries venules veins
High pressure, no exchange Low pressure,
exchange occurs
low pressure, “no exchange”

Fig. 14.25• As arteries and
arterial branch and vessels become more numerous, pressure decreases and stays low until pumped through heart again.

Total Area ->pressure->velocity
Venous lower then arterial relate to relative fractions in arterial v. venous components
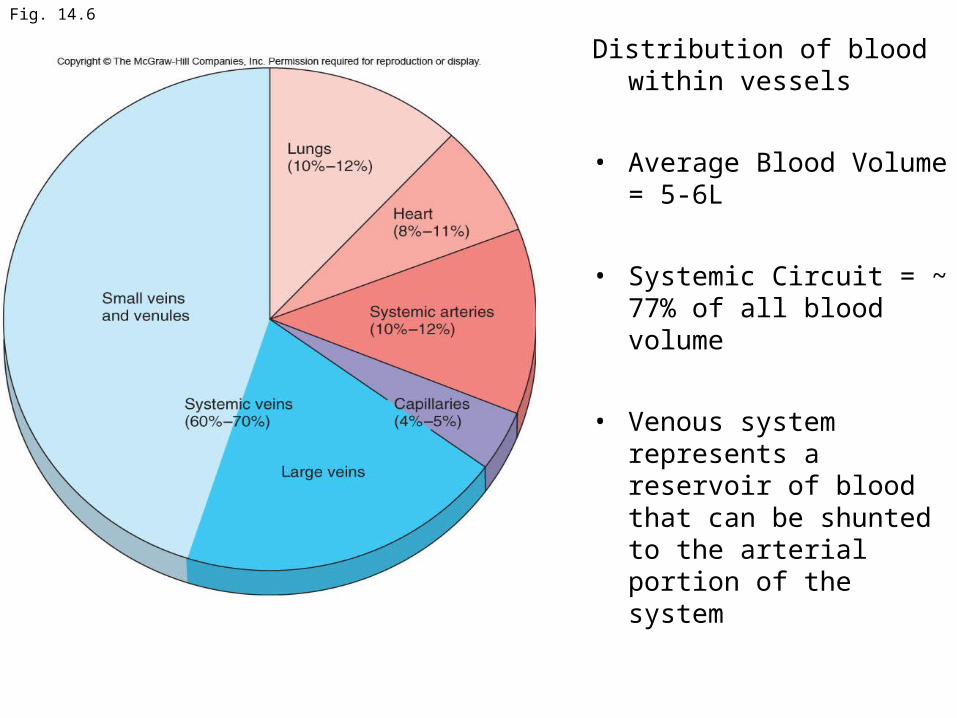
Fig. 14.6
Distribution of blood within vessels
• Average Blood Volume = 5-6L
• Systemic Circuit = ~ 77% of all blood volume
• Venous system represents a reservoir of blood that can be shunted to the arterial portion of the system
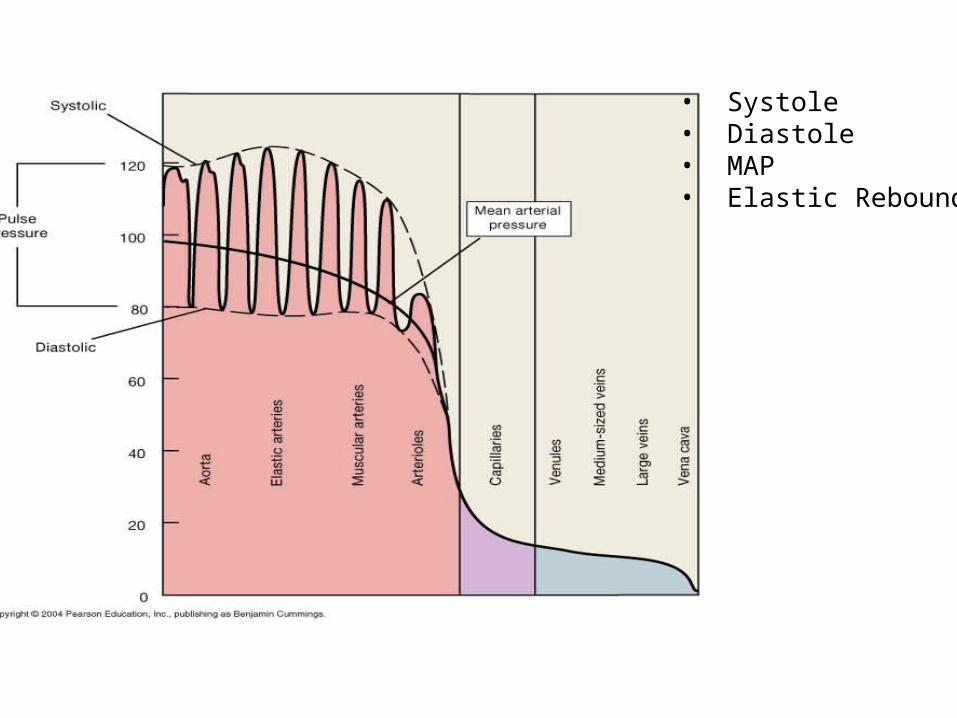
• Systole• Diastole• MAP• Elastic Rebound

Fig. 14.16
Vessel-Pressure Patterns• Pulsation and overall pressure
decrease with distance
• Pulsation due to heart gone by capillaries
• Capillaries and veins are low pressure vessels
key for regulating BP

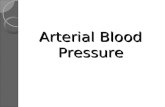
Arterial Flow• Systemic arterial pressure ranges from 120-35 mmHg• This pressure ensures blood flow through capillaries where
exchange happens• Vasoconstriction/Dilation
1. Regulates blood pressure• Constriction/dilation of arterioles is most important
– Constriction increases Resistance increases BP– Dilation decreases resistance decreases PB
2. Shunts blood (re-distributes it) to parrallel “circuits”/other places


Figure 23.5
artery
arteriole
Capillary bed
venule
veins

Capillary flow• Low pressure
– 35mmHg-18mmHg
• Capillary beds– interconnected networks of capillaries
• Local flow/vasomotion– flow through capillaries is not constant, but is regulated by precapillary
sphincters (and terminal arterioles)– Only 25% of capillaries experiences flow at any moment (at rest)
• Vessels are permeable– Capillary exchange

Capillary Exchange• Diffusion/osmosis (due to concentration gradients)
– Between gaps in cells (ions and small organic molecules)– Through transport proteins (ions)– Through membrane lipids (lipid soluble substances)
• Filtration due to: capillary hydrostatic pressure (i.e., blood pressure in capillaries) 35-18mmHg– Primarily at arterial end of capillary drives net filtration out of vessels (~ 35 mmHg)
• Osmotic pressure (colloid osmotic pressure/oncotic pressure)– drives reabsorption of most fluid lost by filtration– Minimized by reabsorption due to colloid osmotic pressure– Primarily at venous end of capillary (~ 18 mmHg)
• Active Transport– Ion pumps– Vessicular transport: endocytosis brings materials into one side of
endothelium and released to opposite site by exocytosis


Fig. 14.9
•If capillary hydrostatic pressure rises increased filtration and accumulation of fluid in interstitial space=edema•If blood volume declines due to bleeding, capillary hydrostatic pressure/filtration declines increased reabsorption (partially compensating volume loss)•During dehydration colloid osmotic pressure increases increased reabsorption (partially compensating volume loss)
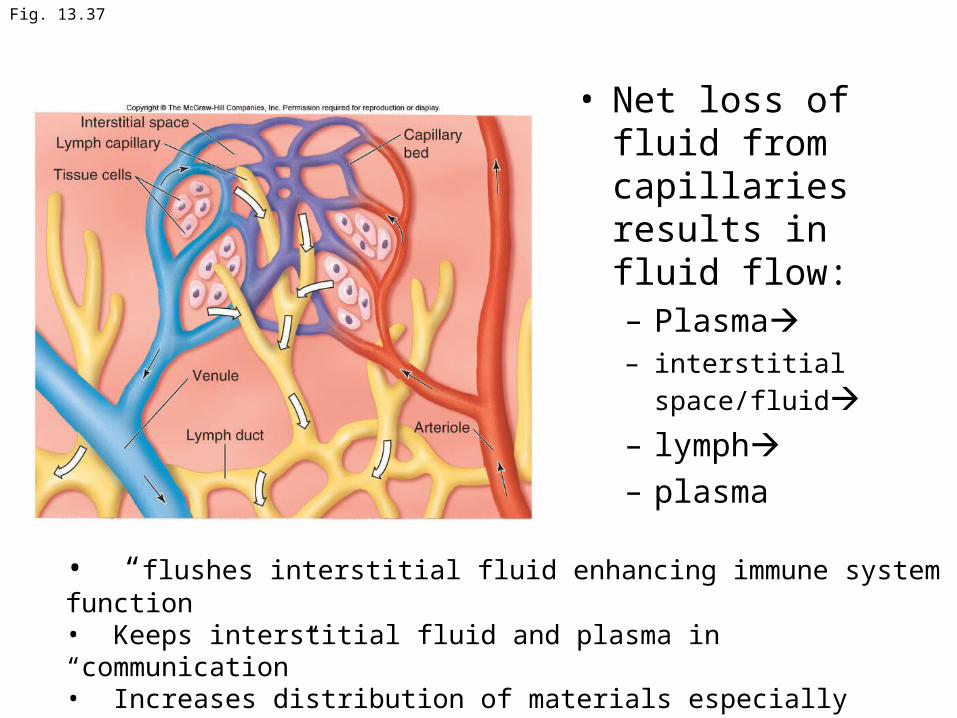
Fig. 13.37
• Net loss of fluid from capillaries results in fluid flow:– Plasma– interstitial space/fluid– lymph– plasma
• “flushes interstitial fluid enhancing immune system function• Keeps interstitial fluid and plasma in “communication”• Increases distribution of materials especially insoluble lipids that have difficulty crossing capillary walls

Fig. 13.38
• Fluid lost from plasma enters lymph and is eventually returned to plasma– No loss of plasma volume
– 3.6L/day transported as lymph
• Lost from capillaries

Fig. 14.10

Venous Flow• Low pressure 18mmHg – 2mmHg
• Non-pulsile
• Venous reservoir
• Flows due to
– Small pressure gradient– Muscle pump (skeletal muscle contraction particularly the lower limbs)
– Respiratory pump • Contraction of diaphragm enhances venous return

Muscle pump:• Constriction muscles
compresses veins and pressurizes blood
• Valves ensure this blood moves towards heart
• Increased muscle use increased venous return

Regulation of Arterial Flow• Extrinsic regulation
– SD-ANS– Hormones
• Intrinsic (autoregulation) Regulation of local flow
• The state of vasoconstriction/dilation and blood flow (and is due to the combined effects of both autoregulation and extrinsic regulation

• Neuroendocrine regulation of BP and Blood Flow
Autoregulation of local flow
Nervous System Regulation• Vasoconstriction/Dilation
• Sympathetic Divison ANS (Vasomotor Centers of Medulla)
– Adrenergic Fibers (neurons)
– Most vessels (including skeletal muscle, see below)
– NE to alpha 1 receptors constriction
– Sympathetic Tone—default state of partial contraction
• due to normal “background” SD activity
– Increased SD– Decreased SD
• Cholinergic Fibers (neurons)
– Primarily Skeletal muscle• Note skeletal muscle vessels have sypathetic tone due to alpha andrenergic innervation
– Ach to cholinergic receptors Dilation
– Skeletal muscle cells also have beta 2 adrenergic receptors that are stimulated by epinephrine released by adrenal medulla that promote dilation.

Sympathetic tone, vasoconstriction and vasodilation
Rate of SD signaling

Autoregulation/Intrinsic Regulation of local blood flow
• local factors (including paracrine regulation) changes in capillary bed flow– Due to constriction/dilation of precapillary sphincters and arterioles
Factors• decrease O2/increase CO2• increase lactic acid/decrease pH• NO increase• K+ increase• histamine release• increase temperature• increased stretch of vascular smooth muscle
• prostoglandins & thromboxanes
promote dilation /
increase flow
promote constriction /
decreased flowreleased during tissue damage and during
clotting
Myogenic mechanisms

Fig. 14.24
• Constriction: reduces flow to “down stream” structures• Increases pressure and flow to “upstream” structures.
Reduced flow
Increased pressure and flow

Regulation of BP
Blood Pressure Influenced by:• CO
– Heart function
• Vascular Resistance– more resistance = increased BP
• Diameter of vessels– dilation reduces resistance/BP
• Length of vessels• Viscosity of blood
• Blood volume– influenced by water balance (water uptake v. water loss)
Changes in minutes
Changes in hours-days

Page 470
• Vasoconstriction• Vasodilation
•Blood Volume
Primary factors influencing BP
Blood Flow and Regulation of Systemic BP
• Blood must flow to tissues that need it
– BP must be sufficient to deliver blood adequately
• Perfussion
– lack of perfusion Ischemia/ischemic infarction
Regulation of BP• Intrinsic/Autoregulation of local flow
• Extrinsic Regulation– Nervous system—sympathetic ANS
• Medulla: vasomotor center– Endocrine System/Hormonal regulation
• Mostly long term regulation of blood volume
• HypothalamuspituitaryKidneys

Fig. 14.7
SV and CO

• Overview of cardiovascular regulation
Baroreceptor reflex• Baroreceptors (pressure) in carotid bodies and aorta
– Glossopharyngeal nerve (carotid bodies)
– Vagus nerve (aorta)
– Detect increases and decreases in pressure
• Send sensory impulses to medulla– Cardiac center sends output to heart—re: CO
• SD (cardioaccelaratory) and PD (cardioinhibitory)
– Vasomotor center send output to vessels—re: constriction/dilation• SD
• BP maintained within normal range

Fig. 14.28

Fig. 14.28
Orthostatic/postural hypotension and
barocrecptor reflex

• Neural responses to changes in BP
SD
PD
SD
PD
SD
SD
↑BP
↓BP
VIS: very important slide

Endocrine/Hormonal Regulation of BP• Mostly through regulation of blood volume
– But also vasoconstriction/dilation effects
Hormones• Antidiuretic Hormone (ADH, vasopressin)• Angiotensin II• Aldosterone• Natriuretic Peptide

Fig. 14.11
ADH
• Decreasing blood/plasma volume increased solute concentration (osmolality)
• ADH release increases
• Increased fluid retention (less urine output)
• Increased water intake
• Blood volume stabilized/increased
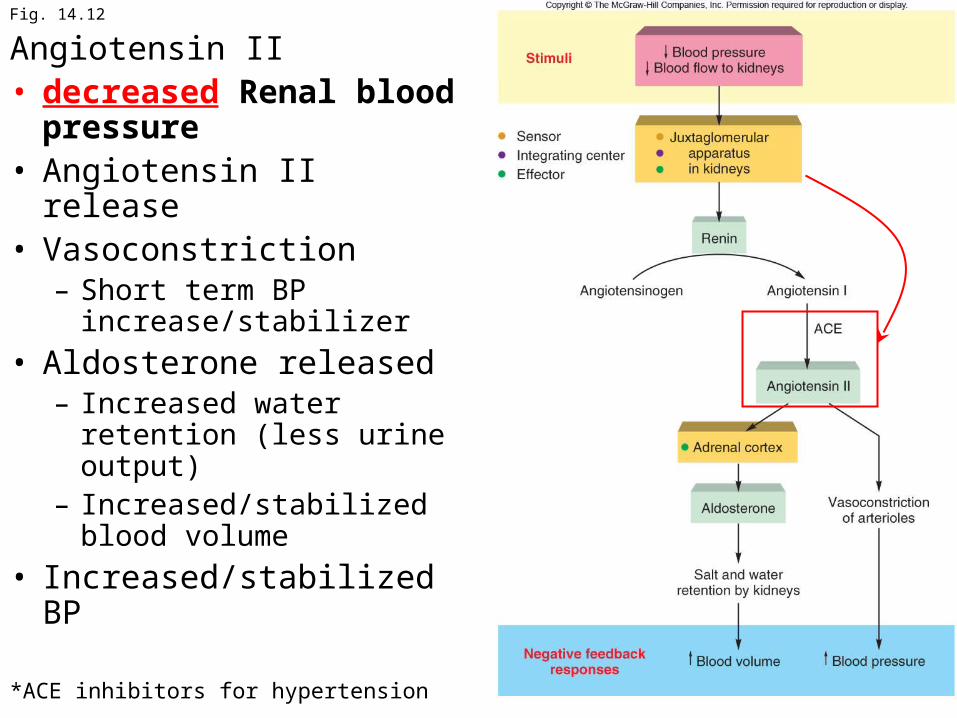
Fig. 14.12
Angiotensin II• decreased Renal blood
pressure• Angiotensin II release• Vasoconstriction
– Short term BP increase/stabilizer
• Aldosterone released– Increased water retention
(less urine output)– Increased/stabilized blood
volume
• Increased/stabilized BP
*ACE inhibitors for hypertension
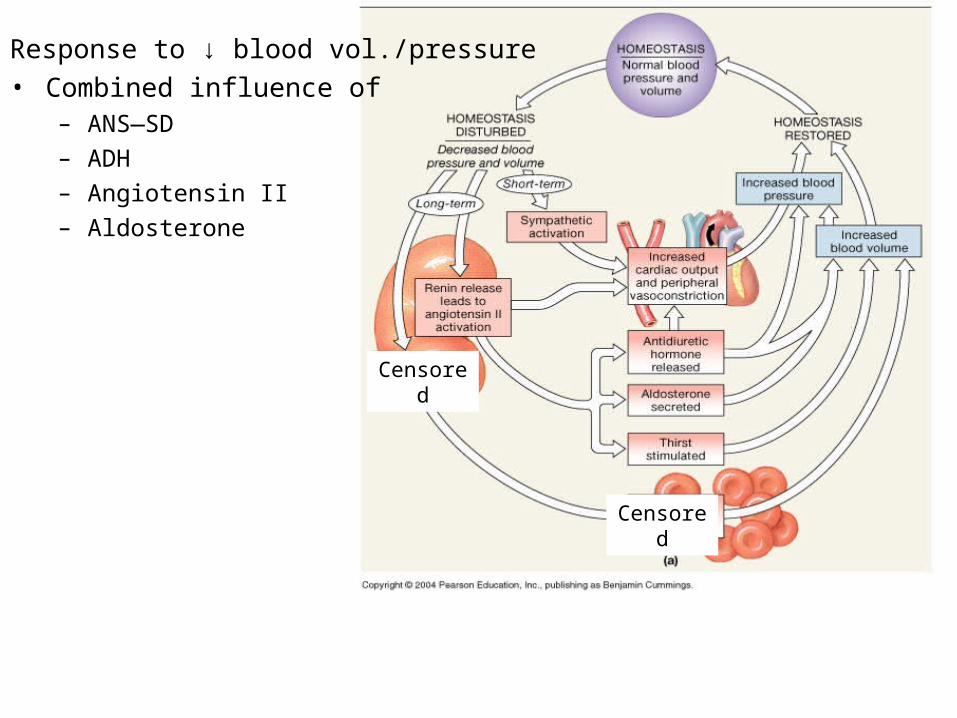
Response to ↓ blood vol./pressure• Combined influence of
– ANS—SD– ADH– Angiotensin II– Aldosterone
Censored
Censored
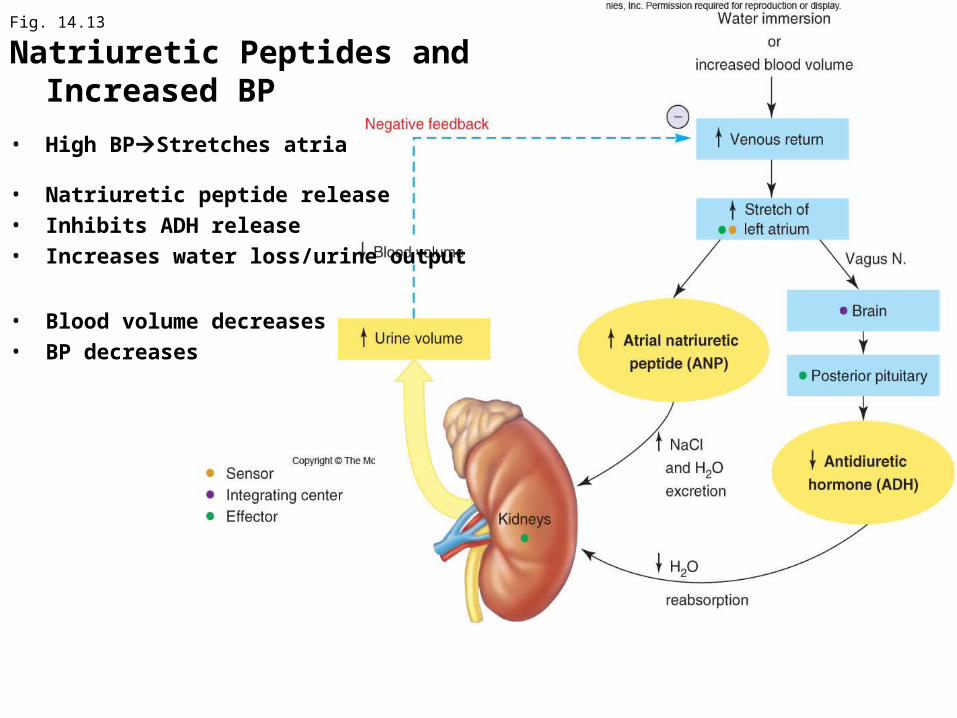
Fig. 14.13
Natriuretic Peptides and Increased BP
• High BPStretches atria
• Natriuretic peptide release• Inhibits ADH release• Increases water loss/urine output
• Blood volume decreases• BP decreases
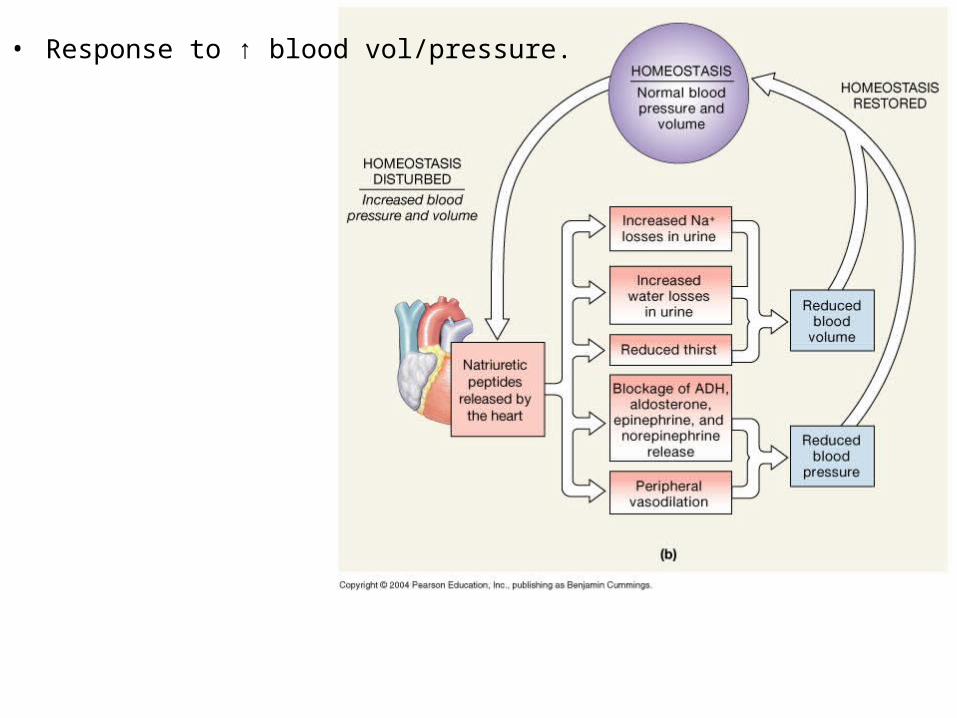
• Response to ↑ blood vol/pressure.

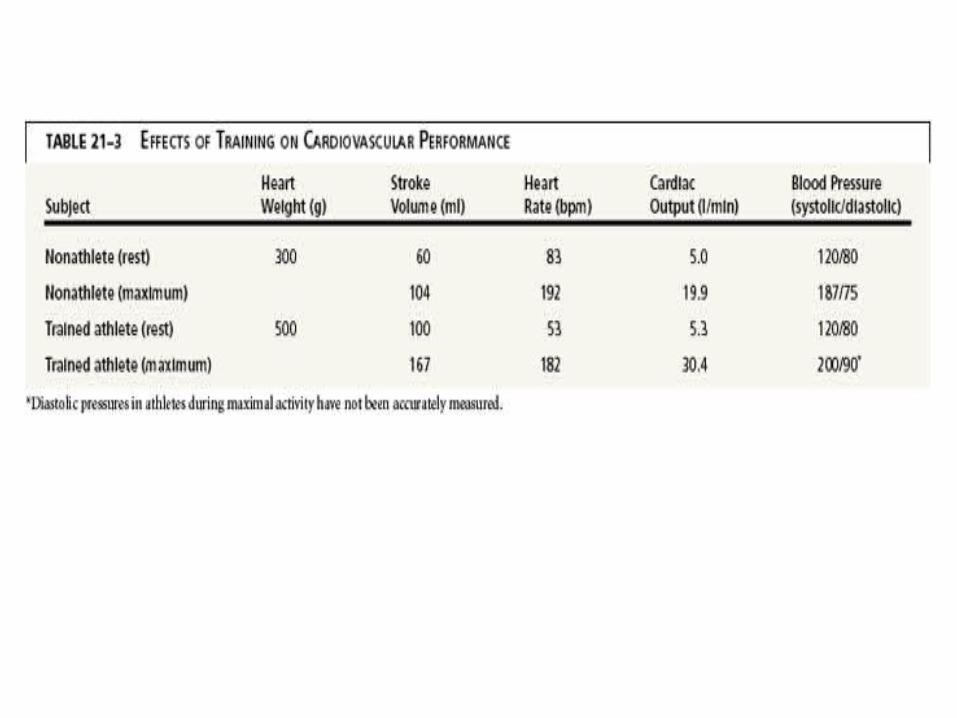
Changes in Systemic Blood Distribution With Exercise

Physiological (circulatory) Shock• Inadequate perfusion (blood flow/BP)
3 fundamental causes• Heart: insufficient CO BP inadequate
– Infarction, severe arrhythmias or valve damage• Vessels: widespread vasodilation BP inadequate
– Brain damage, endotoxins, or histamine (allergic rxn)• Blood Volume: too low BP inadequate
– Bleeding, burns, dehydration

Table 14.4
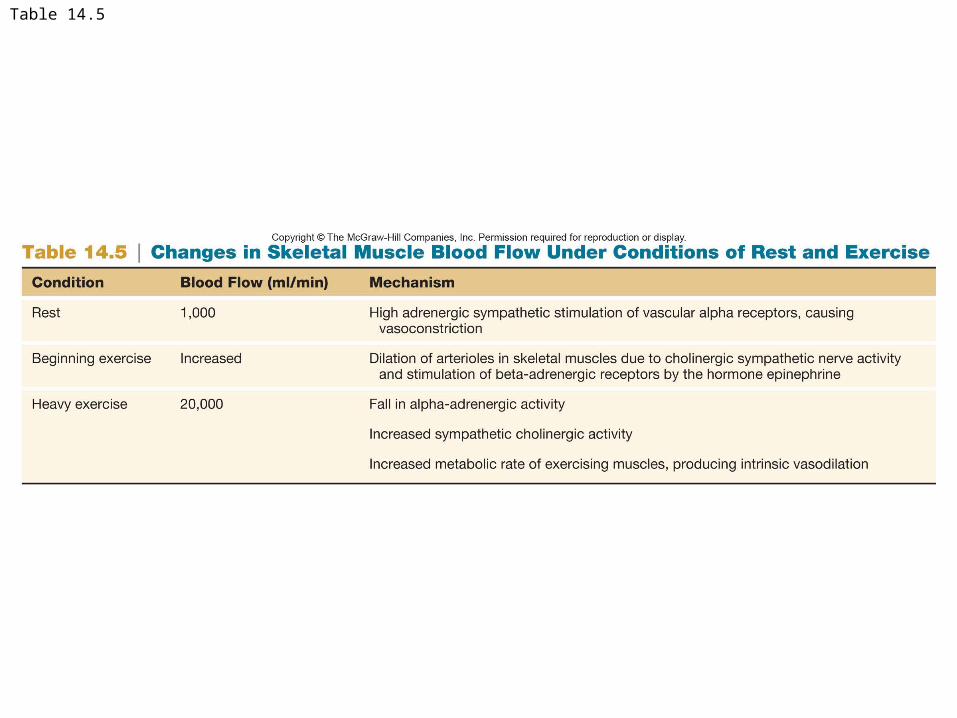
Table 14.5

Fig. 14.21