
Blood Donor Screening 2009 - Current Tests & Risks · HTLV Adult T-Cell Leukaemia, TSP/HAM ......
44
Blood Donor Screening 2009 Blood Donor Screening 2009 - - Current Tests & Risks Current Tests & Risks Dr Patrick Coghlan National Transplantation Services Australian Red Cross Blood Services Melbourne
Transcript of Blood Donor Screening 2009 - Current Tests & Risks · HTLV Adult T-Cell Leukaemia, TSP/HAM ......
Blood Donor Screening 2009 Blood Donor Screening 2009 --Current Tests & RisksCurrent Tests & Risks
Dr Patrick CoghlanNational Transplantation Services
Australian Red Cross Blood ServicesMelbourne
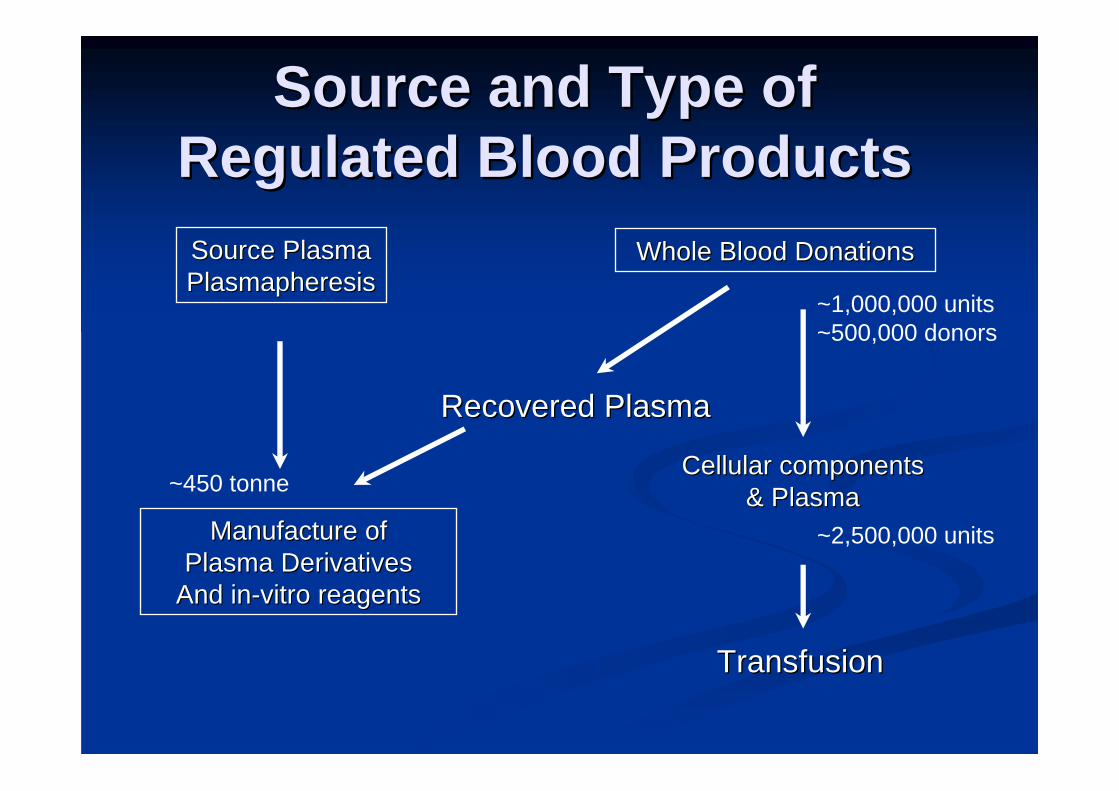
Source and Type of Source and Type of Regulated Blood ProductsRegulated Blood ProductsSource PlasmaSource PlasmaPlasmapheresisPlasmapheresis
Whole Blood DonationsWhole Blood Donations
Cellular componentsCellular components& Plasma& Plasma
TransfusionTransfusion
Recovered PlasmaRecovered Plasma
Manufacture ofManufacture ofPlasma DerivativesPlasma Derivatives
And inAnd in--vitro reagentsvitro reagents
~1,000,000 units~500,000 donors
~2,500,000 units
~450 tonne

Ref: SHOT Annual Report, 2007
SHOT: Cumulative data 1996SHOT: Cumulative data 1996--20072007

(B/O/T) Donor Derived Viral Infections(B/O/T) Donor Derived Viral InfectionsHBV, HCVHBV, HCV hepatitis, cirrhosis, HCChepatitis, cirrhosis, HCCHIVHIV AIDSAIDSHTLVHTLV Adult TAdult T--Cell Cell LeukaemiaLeukaemia, TSP/HAM, TSP/HAMCMVCMV CMV diseaseCMV diseaseEBVEBV Inf. Mononucleosis, Lymphoma PTLPDInf. Mononucleosis, Lymphoma PTLPDHHV8HHV8 Kaposi Sarcoma (Kaposi Sarcoma (immunocompromisedimmunocompromised))ErythrovirusErythrovirus ((ParvoParvo) RBC ) RBC aplasiaaplasiaDengueDengue DengueDengue FeverFeverCHIKVCHIKV ChikungunyaChikungunya FeverFeverWNVWNV WNMEWNMELyssavirusLyssavirus RabiesRabiesArenavirusArenavirus LymphocyticLymphocytic ChorioChorio--MeningitisMeningitis
PlasmodiumPlasmodium MalariaMalariaBabesiaBabesia BabesiosisBabesiosisTrypanosomaTrypanosoma ChagaChaga’’ss diseasediseaseTreponemaTreponema SyphilisSyphilisBorreliaBorrelia LymeLyme DiseaseDiseaseMycobacteriaMycobacteria TBTBTSEsTSEs CJD, CJD, vCJDvCJD,,
All volunteer donorsHBsAg test
AIDS high-risk exclusions
Anti-HIV testALT/HBcAb tests
Anti-HCV test
Improved HCV tests
1965 1970 1975 1980 1985 1990 1995 2000
Year of Transfusion
% R
ecip
ient
s In
fect
ed
25
20
15
10
5
0
NAT Implementation
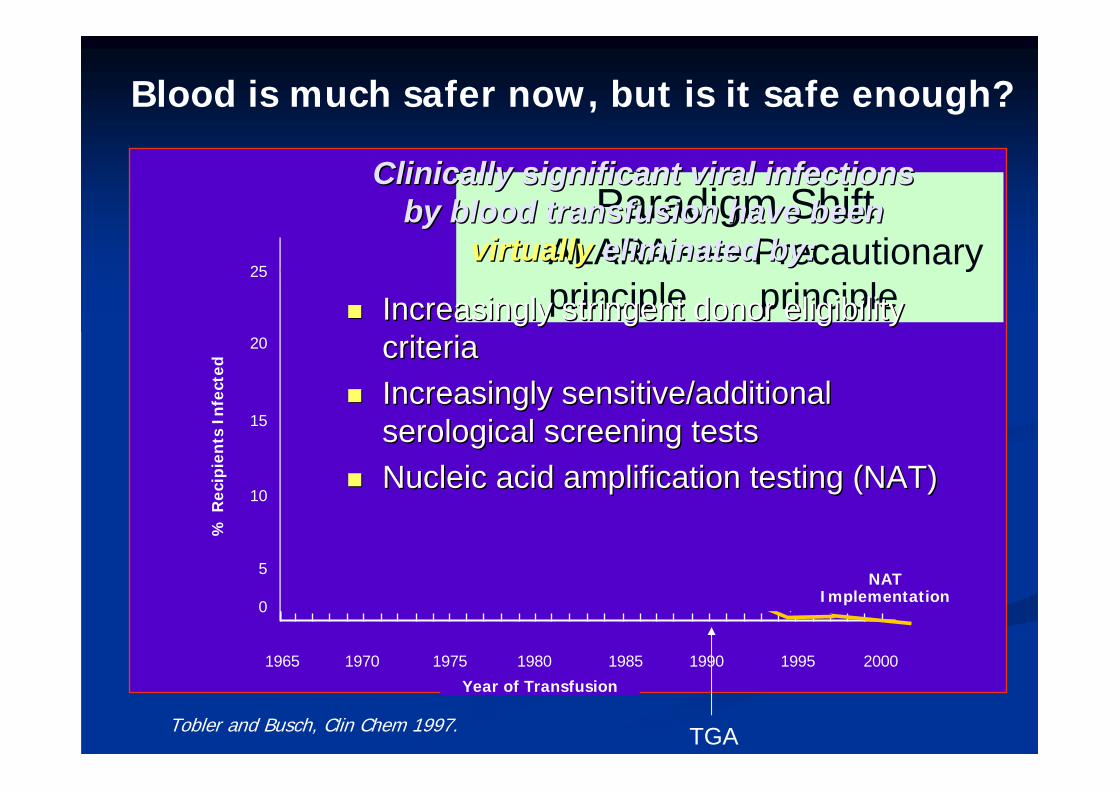
Tobler and Busch, Clin Chem 1997.
Blood is much safer now, but is it safe enough?
TGA
Paradigm ShiftALARA ----- Precautionary principle principle
Clinically significant viral infections Clinically significant viral infections by blood transfusion have been by blood transfusion have been
virtuallyvirtually eliminated by:eliminated by:
Increasingly stringent donor eligibility Increasingly stringent donor eligibility criteriacriteriaIncreasingly sensitive/additional Increasingly sensitive/additional serological screening testsserological screening testsNucleic acid amplification testing (NAT)Nucleic acid amplification testing (NAT)
Sources of Residual RiskSources of Residual Risk
Window period (>90% of risk)Window period (>90% of risk)time between exposure to an agent time between exposure to an agent and detection with screening testsand detection with screening tests
Viral variants (strains, subtypes) not Viral variants (strains, subtypes) not detected by current testsdetected by current testsInfectious chronic antibody neg carriersInfectious chronic antibody neg carriersTesting errorsTesting errors
Busch MP. HIV and Blood Transfusions: Focus on Seroconversion. Vox Sang 67(S3):13-18, 1994.

Source: ANZOD
1 in 11 in 10
1 in 100
1 in 1,000
1 in 10,000
1 in 100,000
1 in 1 million
1 in 10 million
1 in 100 million
1 in 1billion
1 in 1trillion
1 in 10billion
1 in 100billion
-6 -5 -4 -3 -2 -1 0 +1 +2 +3 +4 +5 +6
Pat’s Take Home: Current estimates of risk
The Paling Perspective Scale © John Paling
Blajchman - 2002 Calman 1995
MinusculeRisk
MassiveRisk
Neg Min VL
One in 1 Million = Effective Zero
HCVHIV
HBV
HTLV
? O&T
? O&T
? O&T
General AnaesthesiaMistransfusion
TRALITA-GVHD
Cardiac
Metabolic risk in NeonatesUnder-transfusion
Dzik 2003
CMV
vCJD

‘‘Blood borneBlood borne’’ viral transmissibility viral transmissibility
Three primary criteria that generally need to be Three primary criteria that generally need to be met for a virus to be transmitted by blood met for a virus to be transmitted by blood
It gives rise to asymptomatic infection in the donorIt gives rise to asymptomatic infection in the donor
It is present in the bloodstream It is present in the bloodstream
It is able to survive during subsequent It is able to survive during subsequent storage/processingstorage/processing

Safeguarding the blood supplySafeguarding the blood supply
‘‘Safety tripodSafety tripod’’ **1.1. Donor selectionDonor selection
2.2. TestingTesting
3.3. Pathogen reductionPathogen reduction
4.4. [[HaemovigilanceHaemovigilance]]
** FarrugiaFarrugia A. Vox Sang 2004 86: 1A. Vox Sang 2004 86: 1--77

HIV prevalence in persons aged 15 HIV prevalence in persons aged 15 -- 49 49 years in selected countriesyears in selected countries
0 500 1000 1500 2000
Papua New Guinea
Thailand
Myanmar
Cambodia
Spain
United States
Italy
Malaysia
Vietnam
France
India
United Kingdom
Australia
China
Indonesia
New Zealand
HIV prevalence per 100 000
National Centre in HIV Epidemiology and Clinical Research: 2007

Diagnoses of HIV infectionDiagnoses of HIV infection and AIDSand AIDS11
in Australiain Australia
0
400
800
1200
1600
2000
2400
1981 1983 1985 1987 1989 1991 1993 1995 1997 1999 2001 2003 2005
Year
Num
ber
HIV diagnoses AIDS diagnoses 1. AIDS diagnoses adjusted for reporting delays.
Source: State and Territory health authorities
Donor SelectionDonor SelectionSelect from Select from ‘‘lowlow’’ risk donorsrisk donors
ARCBS ARCBS –– voluntary, non remunerated voluntary, non remunerated Donor education Donor education –– ‘‘riskrisk’’ focusedfocusedComprehensive medical historyComprehensive medical history
Infectious diseases Infectious diseases -- asymptomatic deferral period > asymptomatic deferral period > usually 2x incubation period (e.g. WNV 28 days)usually 2x incubation period (e.g. WNV 28 days)Minimum deferral period after cessation of symptomsMinimum deferral period after cessation of symptomsAdditional deferrals for high risk behaviour, Additional deferrals for high risk behaviour, immunisations, medications, travel, transfusion, immunisations, medications, travel, transfusion, carcinoma etc. carcinoma etc.

How effective is donor selection?How effective is donor selection?
ARCBS studyARCBS studyReducing the risk of transfusion transmissible viral Reducing the risk of transfusion transmissible viral infection through blood donor selection: The Australian infection through blood donor selection: The Australian experience 2000experience 2000--20062006
Mark Polizzotto, Erica Wood, Helen Ingham and Tony Mark Polizzotto, Erica Wood, Helen Ingham and Tony Keller. Transfusion 2008; 48:55Keller. Transfusion 2008; 48:55--6363
6.2 million 6.2 million allogeneicallogeneic blood donations collected by blood donations collected by ARCBS between July 2000 and June 2006ARCBS between July 2000 and June 2006Tested for hepatitis C, hepatitis B, HIV, and HTLV I/IITested for hepatitis C, hepatitis B, HIV, and HTLV I/IIDonors with positive test results contacted for Donors with positive test results contacted for reassessment of risk factors and repeat testingreassessment of risk factors and repeat testing
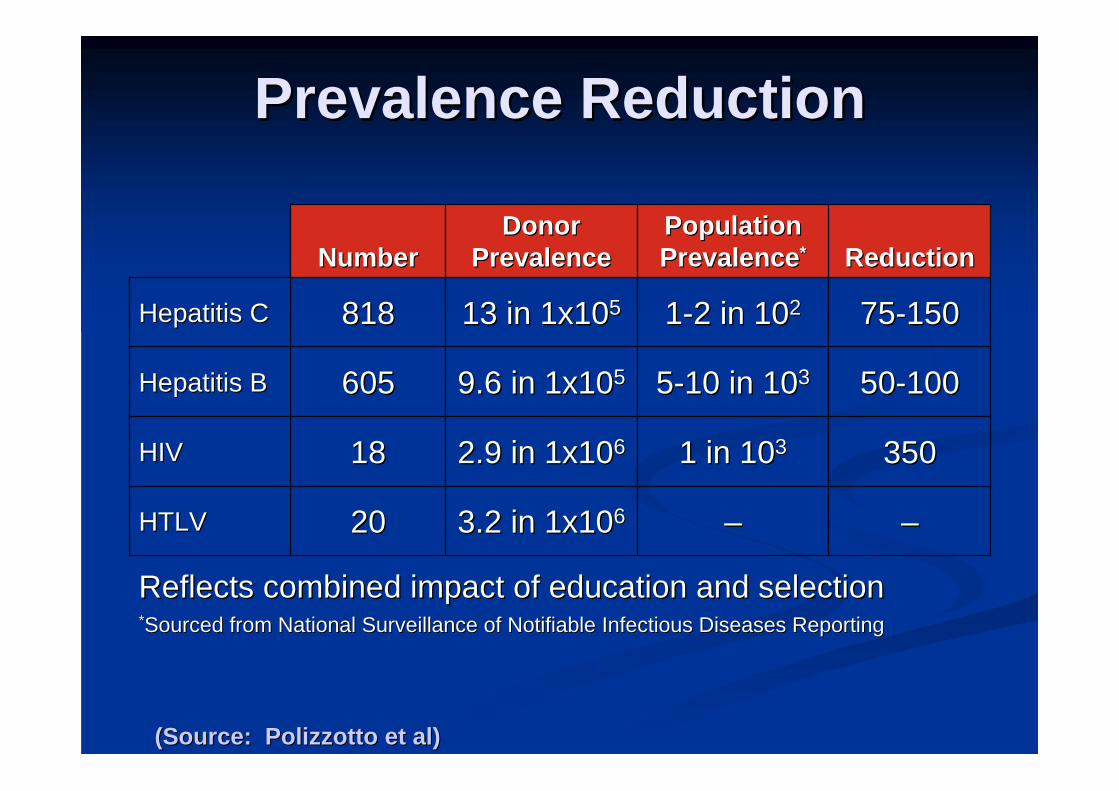
Prevalence ReductionPrevalence Reduction
Reflects combined impact of education and selectionReflects combined impact of education and selection**Sourced from National Surveillance of Sourced from National Surveillance of NotifiableNotifiable Infectious Diseases ReportingInfectious Diseases Reporting
––
1 in 101 in 1033
55--10 in 1010 in 1033
11--2 in 102 in 1022
Population Population PrevalencePrevalence**
––3.2 in 1x103.2 in 1x10662020HTLVHTLV
3503502.9 in 1x102.9 in 1x10661818HIVHIV
5050--1001009.6 in 1x109.6 in 1x1055605605Hepatitis BHepatitis B
7575--15015013 in 1x1013 in 1x1055818818Hepatitis CHepatitis C
ReductionReductionDonor Donor
PrevalencePrevalenceNumberNumber
(Source: (Source: PolizzottoPolizzotto et al)et al)
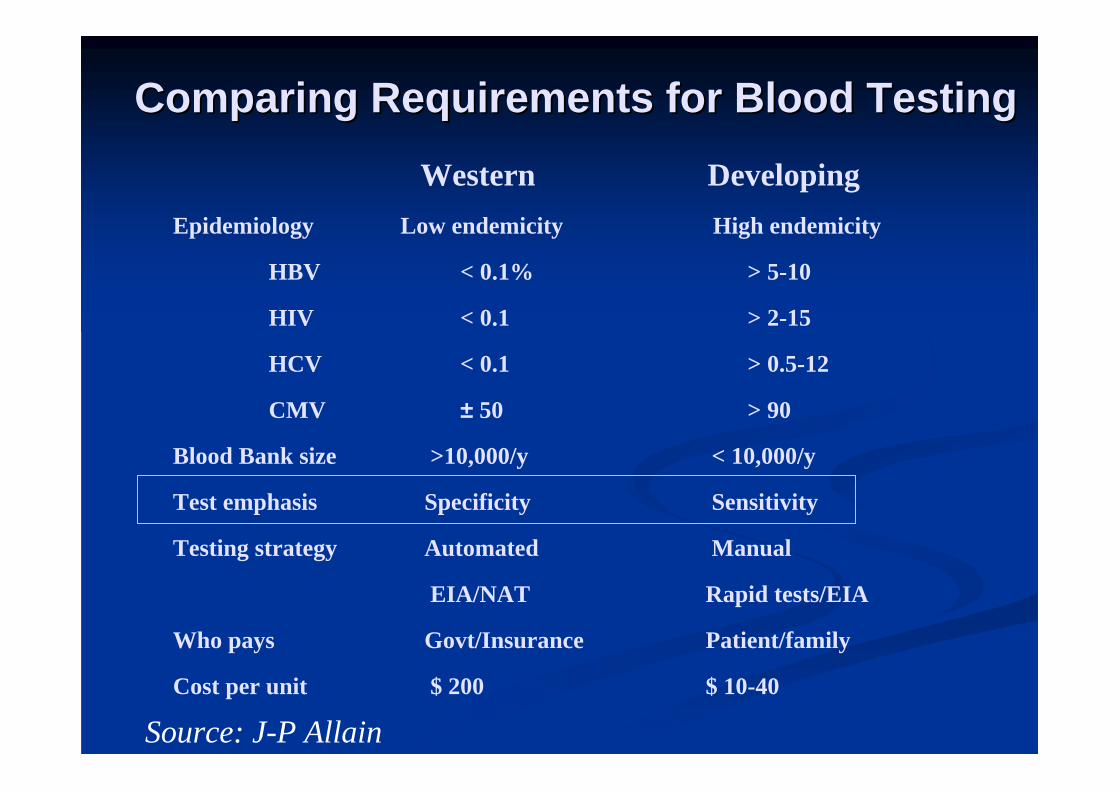
Comparing Requirements for Blood TestingComparing Requirements for Blood TestingWestern Developing
Epidemiology Low endemicity High endemicity
HBV < 0.1% > 5-10
HIV < 0.1 > 2-15
HCV < 0.1 > 0.5-12
CMV ± 50 > 90
Blood Bank size >10,000/y < 10,000/y
Test emphasis Specificity Sensitivity
Testing strategy Automated Manual
EIA/NAT Rapid tests/EIA
Who pays Govt/Insurance Patient/family
Cost per unit $ 200 $ 10-40
Source: J-P Allain

CharacterisingCharacterising AssaysAssays
AssayResult
+
-
Presence of Disease
+ -True Positive
(TP)
False Negative(FN)
False Positive(FP)
True Negative(TN)
+ Predictive valueTP/(TP+FP)
- Predictive valueTN/(TN+FN)
SensitivityTP/(TP+FN)
SpecificityTN/(TN+FP)
Probability that test is negative in the absence
of diseasePJC 2000
Probability of a reactive sample being confirmed as positive.

Universal Viral Screening Universal Viral Screening Markers (ARCBS, 2007)Markers (ARCBS, 2007)
Serological Serological markers:markers:
HBsAgHBsAgAntiAnti--HIVHIV--1/21/2AntiAnti--HCVHCVAntiAnti--HTLVHTLV--I/III/II
(Abbott PRISM (Abbott PRISM ChLIAChLIA))O&T donations:O&T donations:
[Anti[Anti-- HBc/AntiHBc/Anti--HBsHBs]]
NAT:NAT:HIVHIV--1 RNA1 RNA
HCV RNAHCV RNA
(Chiron/(Chiron/GenprobeGenprobeProcleix TMA Procleix TMA multiplex)multiplex)

Repeat Reactive IA-1(anti-HIV, anti-HCV,
anti-HTLV)
Test on IA-2
NEG on IA-2: biological false reactive (BFR)
Reactive on IA-2
Immunoblot
ARCBS Sequential Immunoassay (IA) Strategy
Product discard
(NAT non-reactive)
Initial ReactiveIA-1
Blood Safety StrategiesBlood Safety StrategiesAb & Ag ChLIA
(HIV & HCV Antigen) (US$20m/QALY)NAT (US$~2M/QALY)
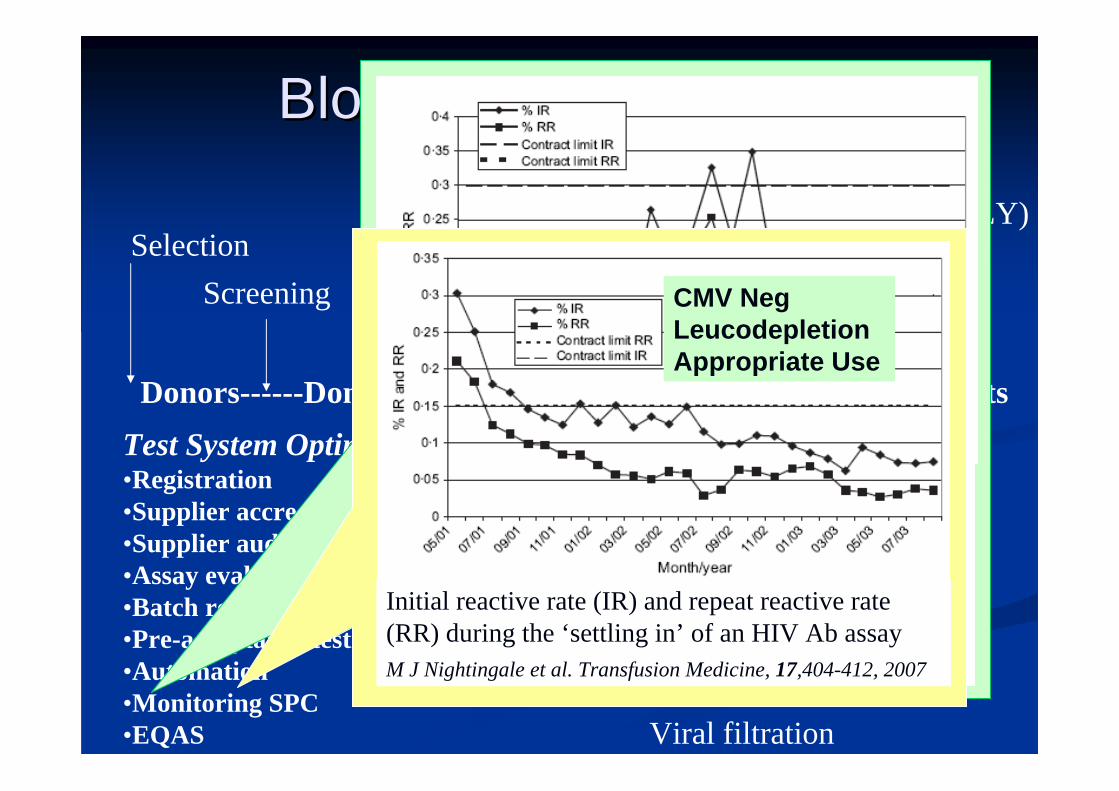
PatientsDonors------Donation
ScreeningSelection
* VI = Solvent Detergent/InactineMethylene BlueUV/PsoralensRiboflavinViral filtration
haemovigilanceTest System Optimisation•Registration•Supplier accreditation•Supplier audit•Assay evaluation/specification•Batch release certification•Pre-acceptance testing•Automation•Monitoring SPC•EQAS
Viral Inactivation*Fractionation
The transient increase in initial reactive rate (IR) and repeat reactive rate (RR) of a problematic HIV antibody assay.
M J Nightingale et al. Transfusion Medicine, 17,404-412, 2007
Initial reactive rate (IR) and repeat reactive rate (RR) during the ‘settling in’ of an HIV Ab assayM J Nightingale et al. Transfusion Medicine, 17,404-412, 2007
CMV NegLeucodepletionAppropriate Use

How good are current tests?How good are current tests?
Current serological tests for HIV, HCV , Current serological tests for HIV, HCV , HBV, HTLV, CMV are capable of HBV, HTLV, CMV are capable of detecting >99.9 % of infectious detecting >99.9 % of infectious donations. donations.
‘‘Window periodWindow period’’ riskrisk



PRISM Assay PerformancePRISM Assay Performance
99.9499.94
99.9399.93
99.8599.85
99.9999.99
Specificity Specificity (%)(%)
0.300.30226746741,153,6431,153,6431,153,6451,153,645AntiAnti--HTLVHTLV
11.611.61071079249241,153,5381,153,5381,153,6451,153,645AntiAnti--HCVHCV
0.170.1733175217521,153,6421,153,6421,153,6451,153,645AntiAnti--HIVHIV
48.848.81011012072071,153,5441,153,5441,153,6451,153,645HBsAgHBsAg
PPV PPV (%)(%)
confirmed confirmed positivepositive
repeatedly repeatedly reactive reactive
(RR)(RR)
negativenegativedonations donations testedtested
AssayAssay
Source: ARCBS 2006
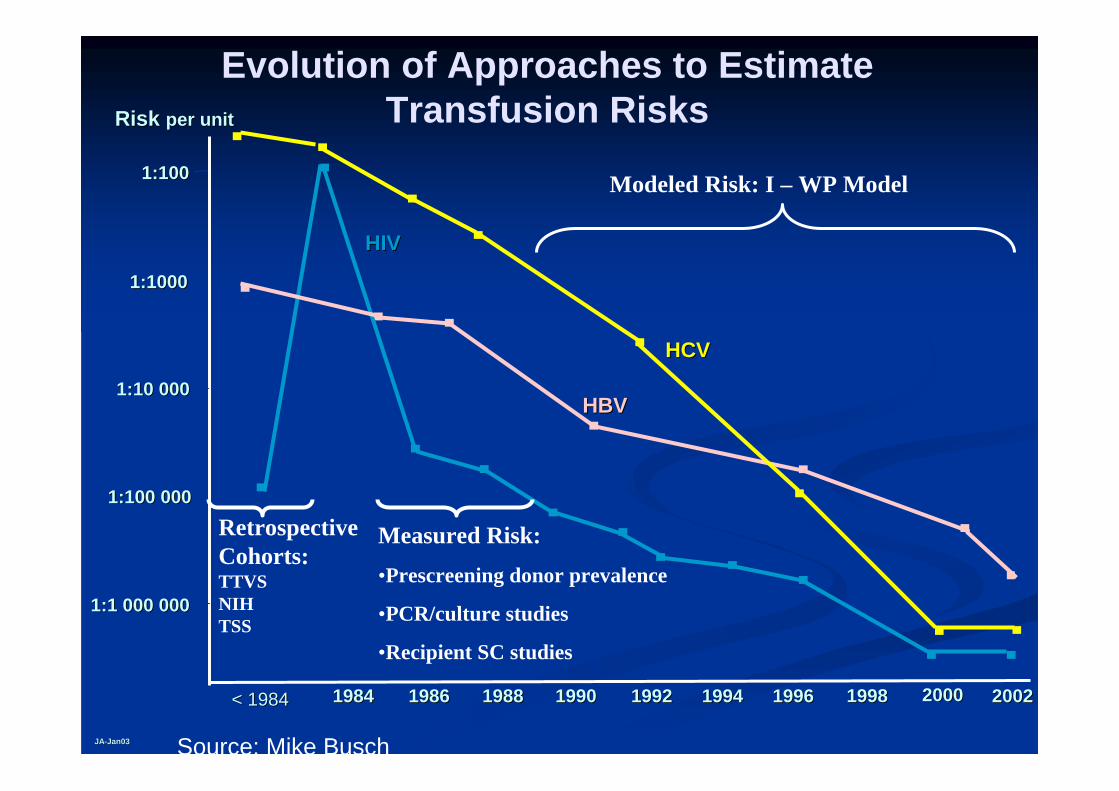
HIVHIV
HBVHBV
HCVHCV
19961996199419941992199219901990198819881986198619841984
1:1001:100
1:10001:1000
1:10 0001:10 000
1:100 0001:100 000
1:1 000 0001:1 000 000
19981998 20002000
Risk Risk per unitper unit
20022002
Evolution of Approaches to Estimate Transfusion Risks
JAJA--Jan03Jan03
Measured Risk:•Prescreening donor prevalence
•PCR/culture studies
•Recipient SC studies
Modeled Risk: I – WP Model
< 1984< 1984
RetrospectiveCohorts:TTVSNIHTSS
Source: Mike Busch

Viral transmission: Measuring riskViral transmission: Measuring risk
Classical approaches to measure risk (i.e. followClassical approaches to measure risk (i.e. follow--up studies/missed infections in screened donors) up studies/missed infections in screened donors) --too few eventstoo few events
Risk estimates now use mathematical modelling Risk estimates now use mathematical modelling yielding theoretical risk levels based on:yielding theoretical risk levels based on:
Frequency of markerFrequency of marker--negative, window period negative, window period donationsdonations
Rare transmission events (variants)Rare transmission events (variants)
Antibody negative carriersAntibody negative carriers
Procedural testing errorsProcedural testing errors

Assumes that Window Period transmissions Assumes that Window Period transmissions represent the major component of the residual represent the major component of the residual riskriskProbably holds true for HIV and HCV, but less Probably holds true for HIV and HCV, but less so for HBV where chronic infection can be so for HBV where chronic infection can be marked by transient HBsAg detectionmarked by transient HBsAg detection
P = P = λλ x WPx WPwhere P = probability donor gave infectious unit where P = probability donor gave infectious unit
during window period,during window period,λλ = = the incidence and the incidence and WP = window periodWP = window period
IncidenceIncidence--Window Period ModelWindow Period Model
Source: Seed et al ARCBS 2005

P = P = λλ x WPx WPwhere P = probability donor gave infectious unit during where P = probability donor gave infectious unit during
window period,window period,λλ = = the incidence and the incidence and WP = window periodWP = window period
For HIV NAT [For HIV NAT [λλ = 6 x 10= 6 x 10--77 ; WP = 9 days (9/365) = ; WP = 9 days (9/365) = 0.02465]0.02465]
P = P = 6 x 106 x 10--77 x 0.02465x 0.02465= 1.479 x 10= 1.479 x 10--77
or 1 in 6,759,259or 1 in 6,759,259
IncidenceIncidence--Window Period ModelWindow Period Model
Source: Seed et al ARCBS 2005
NAT (US$~2M/QALY)

2005-2006 2006-2007Calendar Years Calendar Years
Virus Screening WP Median MedianTechnology (95 CI) (Point estimate) (Point estimate)
HIV Procleix NAT 9 1 in 69,560,000 1 in 35,256,000(8.0-10.3) (8,319,000– 86,473,000) (8,971,000– 41,558,000)
HCV Procleix NAT 5.4 1 in 12,215,000 1 in 3,211,000(4.9- 6.0) (3,565,000– 47,783,000) (2,855,000– 5,023,000)
HBV Prism HBsAg 38.3 1 in 669,000 1 in 1,927,000(33- 43.7) (447,000– 2,657,000) (678,000– 11,002,000)
HTLV Prism HTLV 1/2 51 1 in 10,549,000 1 in 14,728,000(36-72) (2,664,000– 18,578,000) (3,728,000– 25,059,000)
Seed et al: ARCBS 2008
Transfusion Transmitted Infections: Transfusion Transmitted Infections: Residual Risk Estimates for Periods 2005Residual Risk Estimates for Periods 2005--06 and 200606 and 2006--0707
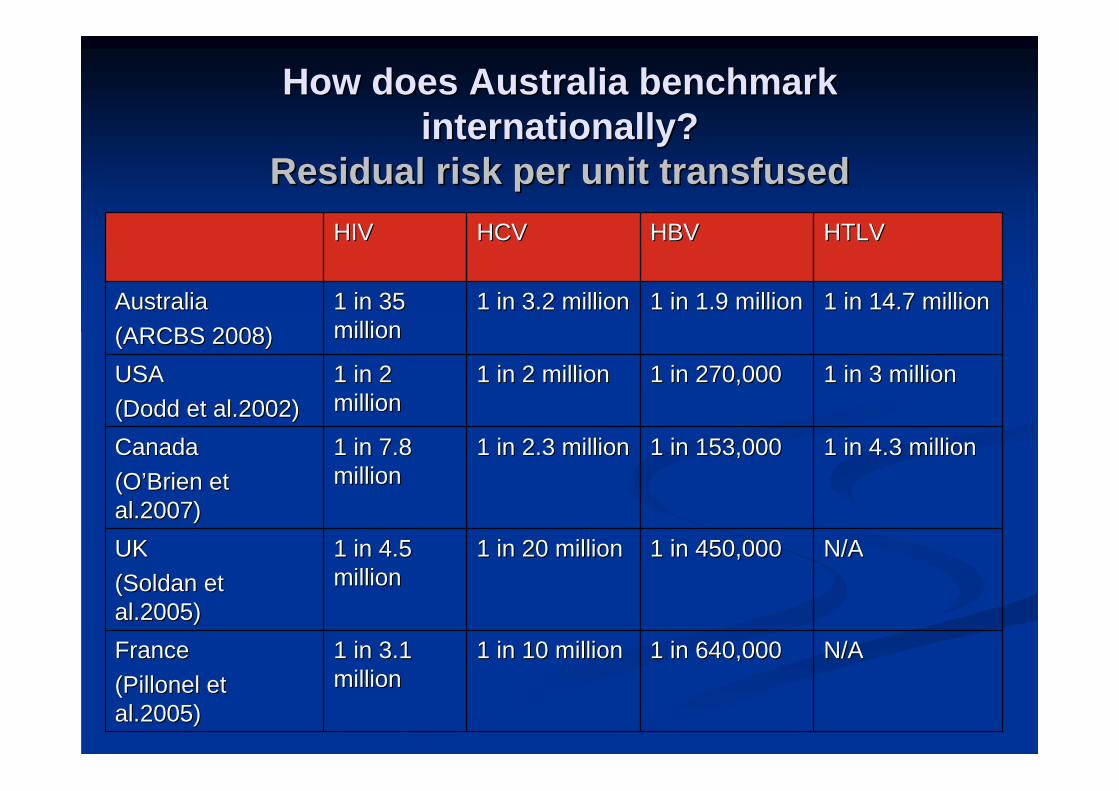
How does Australia benchmark How does Australia benchmark internationally?internationally?
Residual risk per unit transfusedResidual risk per unit transfused
N/AN/A1 in 640,0001 in 640,0001 in 10 million1 in 10 million1 in 3.1 1 in 3.1 millionmillion
FranceFrance((PillonelPillonel et et al.2005)al.2005)
N/AN/A1 in 450,0001 in 450,0001 in 20 million1 in 20 million1 in 4.5 1 in 4.5 millionmillion
UKUK((SoldanSoldan et et al.2005)al.2005)
1 in 4.3 million1 in 4.3 million1 in 153,0001 in 153,0001 in 2.3 million1 in 2.3 million1 in 7.8 1 in 7.8 millionmillion
CanadaCanada(O(O’’Brien et Brien et al.2007)al.2007)
1 in 3 million1 in 3 million1 in 270,0001 in 270,0001 in 2 million1 in 2 million1 in 2 1 in 2 millionmillion
USAUSA(Dodd et al.2002)(Dodd et al.2002)
1 in 14.7 million1 in 14.7 million1 in 1.9 million1 in 1.9 million1 in 3.2 million1 in 3.2 million1 in 35 1 in 35 millionmillion
AustraliaAustralia(ARCBS 2008)(ARCBS 2008)
HTLVHTLVHBVHBVHCVHCVHIVHIV

Documented NAT Breakthrough Infections Documented NAT Breakthrough Infections
1 (since 2002), no NAT1 (since 2002), no NAT0000UK: (England, Scotland, Wales, UK: (England, Scotland, Wales, No Ireland) + EireNo Ireland) + Eire
SpainSpain
70702211JapanJapanN/AN/A0000AustraliaAustralia
000000Rep. So AfricaRep. So Africa
110011FranceFranceEUROPEEUROPE
ASIA ASIA -- PACIFICPACIFIC
AFRICAAFRICA
000000Greece ("covering 75% of the Greece ("covering 75% of the total blood supply")total blood supply")
992222GermanyGermany
000000ItalyItalyPolandPoland
4 (since 2000); no NAT4 (since 2000); no NAT1144USAUSA000000Canada: (Quebec Canada: (Quebec only)only)000000Canada: (Canada: (exclexcl Quebec)Quebec)
NORTH AMERICANORTH AMERICA
HBVHBVHCVHCVHIVHIVRegion / CountryRegion / Country
M. Busch

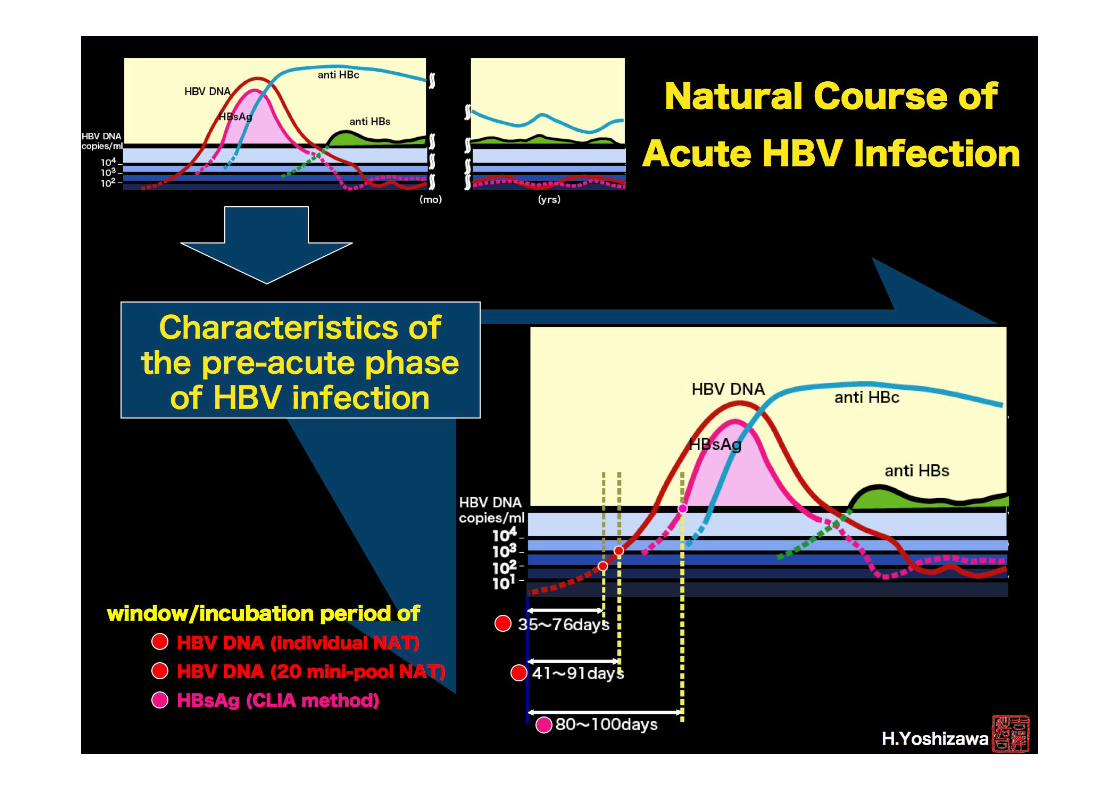
HBV: To NAT or Not?HBV: To NAT or Not?
Current screening test is HBsAgCurrent screening test is HBsAg
Should additional Should additional test(stest(s) be introduced for ) be introduced for detection of Hepatitis B?detection of Hepatitis B?
-- Anti Anti HBcHBc
-- HBV DNAHBV DNA
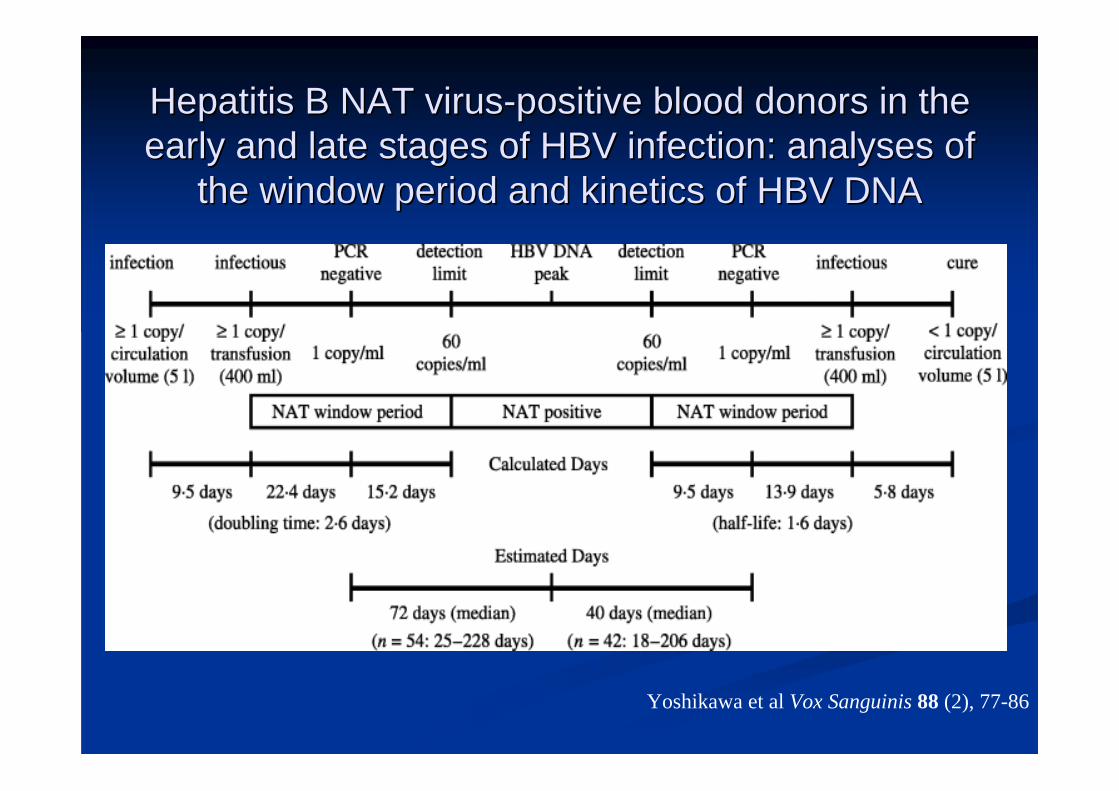
Hepatitis B NAT virusHepatitis B NAT virus--positive blood donors in the positive blood donors in the early and late stages of HBV infection: analyses of early and late stages of HBV infection: analyses of
the window period and kinetics of HBV DNAthe window period and kinetics of HBV DNA
Yoshikawa et al Vox Sanguinis 88 (2), 77-86
HBV NATHBV NATRoche and Chiron have new automated assays Roche and Chiron have new automated assays that include hepatitis B NATthat include hepatitis B NATNeed to be performed in single donor (Chiron Need to be performed in single donor (Chiron UltrioUltrio) or very small pools( Roche S201)) or very small pools( Roche S201)ARCBS participated in a trial to evaluate the ARCBS participated in a trial to evaluate the instrumentationinstrumentationAccurate statistics for hepatitis B transmission Accurate statistics for hepatitis B transmission are unavailable. In the absence of a are unavailable. In the absence of a haemovigilance system transmission rates are haemovigilance system transmission rates are estimated by modelling.estimated by modelling.

Automated NATAnalytical SensitivityAnalytical Sensitivity
-- 95% Limit of Detection of WHO standards (IU/mL)95% Limit of Detection of WHO standards (IU/mL)
NoNo8.48.4(5.0 (5.0 –– 21.7)21.7)
12.212.2(7.3 (7.3 -- 29.2)29.2)
HBV (A) HBV (A) (97/746)(97/746)
YesYes6.06.0(3.9 (3.9 –– 12.5)12.5)
2.02.0(1.4 (1.4 -- 7.4)7.4)
HCV (1) HCV (1) (96/798)(96/798)
NoNo50.550.5(29.6 (29.6 –– 118.2)118.2)
42.242.2(24.8 (24.8 -- 99.3)99.3)
HIVHIV--1 (B)1 (B)(97/650)(97/650)
SignificanceSignificance(P<0.05)(P<0.05)
CobasCobas MPXMPXIDTIDT
Procleix ULTRIO Procleix ULTRIO IDTIDT
95% Detection Limit95% Detection Limit(IU/mL)(IU/mL)WHOWHO
ReferenceReferenceStandardStandard
Margaritis et al. Transfusion 2007; 47:1783-1793
The case of WNV• 2002 first death – blood donation
• FDA challenge – summer 2003
• 2003 WNV NAT
• 2007 – automated NAT

Prevalence & Incidence of HIV, HCV, HBV and HTLV among Musculoskeletal Tissue Donors and First Time Blood Donors
Yao et al . Annals Int Med 148,10; 793-5
22221:345,0001:345,000
44441:172,0001:172,000
WPWPRRRR
HBVHBV
771:500,0001:500,000
66661:55,0001:55,000
WPWPRRRR
HCVHCV
991:400,0001:400,000
22221:161,0001:161,000
WPWPRRRR
HIVHIV
NATNATSero.Sero.NAT: residual risk* NAT: residual risk* reductionreduction
* Estimated probability of viraemia in donor
DDI Risk: Reg BD << FTBD << O&TD

TT TT -- CytomegalovirusCytomegalovirusCMV Abs in 30 CMV Abs in 30 -- 80% blood donors80% blood donors
22--12% 12% AbAb+ capable of transmitting virus+ capable of transmitting virus
WP 42 WP 42 –– 56 days56 days
Residual Risk of seronegative donationResidual Risk of seronegative donation
1:66,000 (1:42,000 1:66,000 (1:42,000 –– 165,000)165,000)
2 2 --3 cases per year3 cases per yearStrategies to eliminate TTStrategies to eliminate TT--CMV:CMV:
CMV CMV AbAb negative bloodnegative blood
LeucocyteLeucocyte depletiondepletion
CMV immune globulin/intravenous immunoglobulinCMV immune globulin/intravenous immunoglobulin
prophylactic acyclovirprophylactic acyclovir
Source: Seed 2008
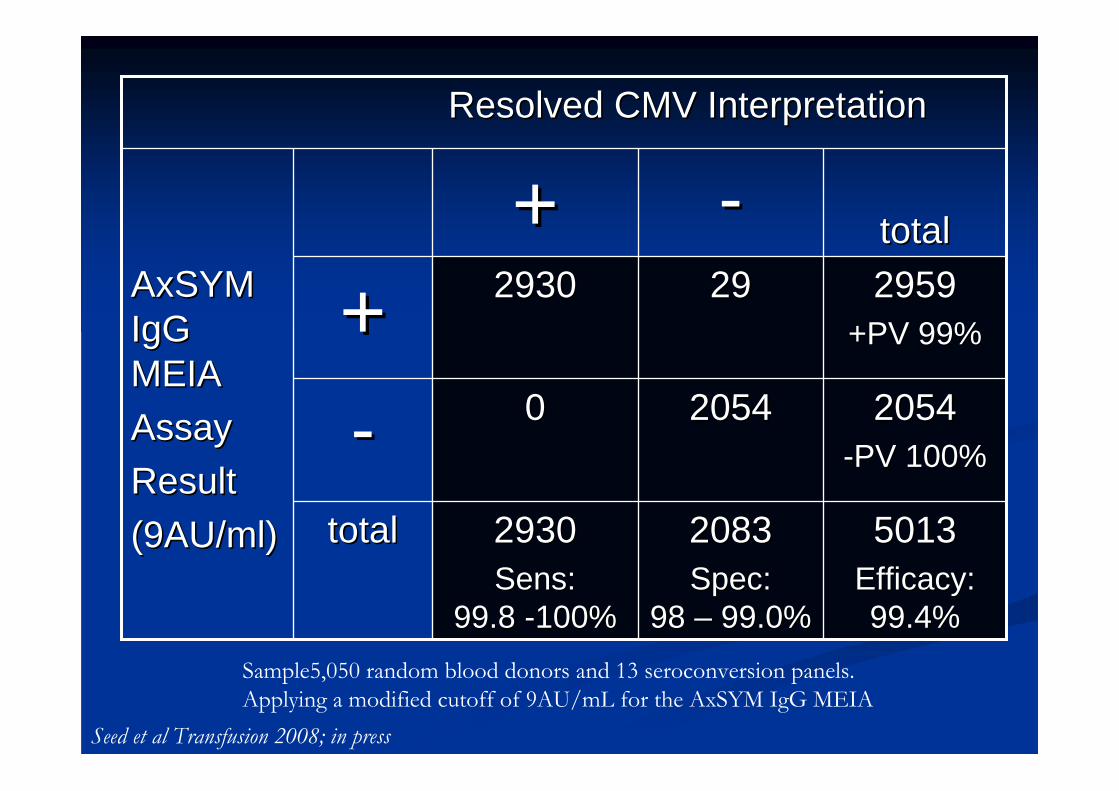
Sample5,050 random blood donors and 13 seroconversion panels. Applying a modified cutoff of 9AU/mL for the AxSYM IgG MEIA
50135013Efficacy: Efficacy: 99.4%99.4%
20832083Spec: Spec:
98 98 –– 99.0%99.0%
29302930Sens: Sens:
99.8 99.8 --100%100%
totaltotal
20542054--PV 100%PV 100%
2054205400--
29592959+PV 99%+PV 99%
292929302930++totaltotal--++
AxSYMAxSYMIgG IgG MEIAMEIAAssayAssayResultResult(9AU/ml)(9AU/ml)
Resolved CMV InterpretationResolved CMV Interpretation
Seed et al Transfusion 2008; in press

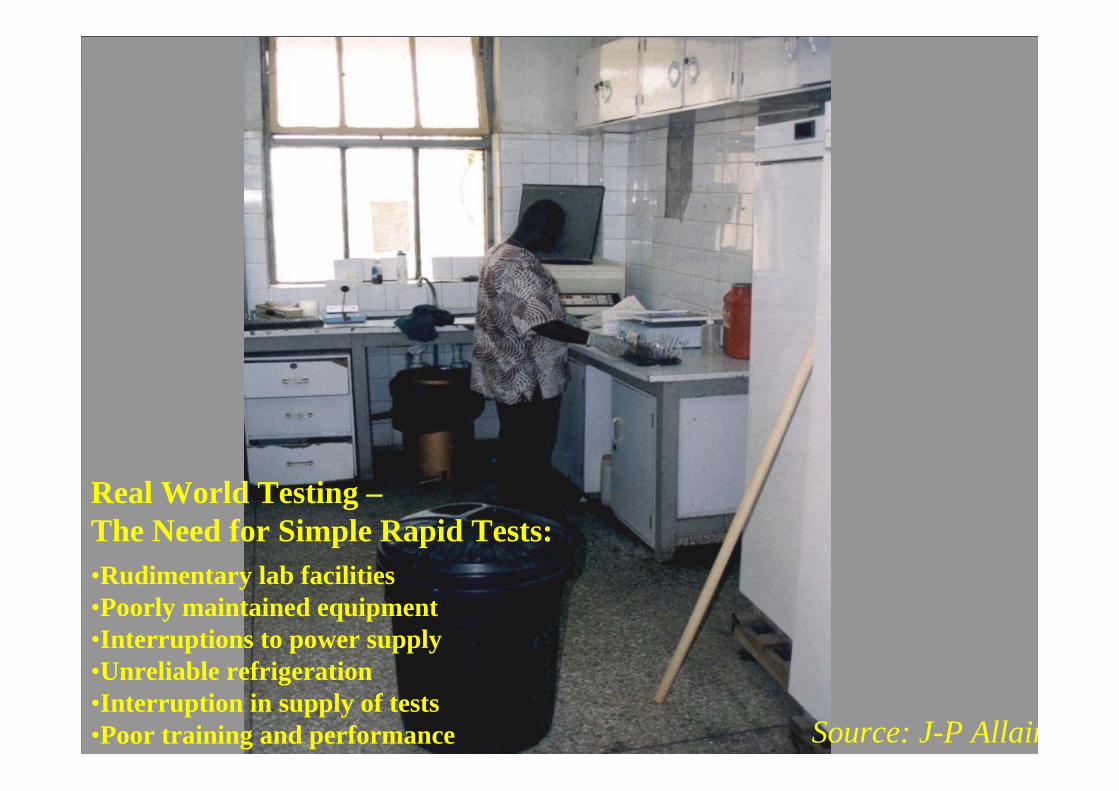
Blood Testing in AfricaBlood Testing in Africa
Most blood centres screen for antiMost blood centres screen for anti--HIV by HIV by ELISA or rapid testsELISA or rapid tests
80% screen for 80% screen for HBsAgHBsAg with rapid testswith rapid tests
< 20% screen for anti< 20% screen for anti--HCVHCV
Few countries have a QA system in placeFew countries have a QA system in place
Kits and equipment are often donated, Kits and equipment are often donated, supply is not sustainedsupply is not sustained
Source: J-P Allain

Simple/Rapid (S/R) TestsSimple/Rapid (S/R) TestsPropertiesProperties
SimpleSimpleInstrumentInstrument--freefreeElectricityElectricity--freefree
TypeTypeAgglutinationAgglutinationMembraneMembrane
ImmunofiltrationImmunofiltration (flow through)(flow through)ImmunochromatographicImmunochromatographic (lateral flow)(lateral flow)
Sensitivity/SpecificitySensitivity/SpecificityHIVHIV 100% / 98.6%100% / 98.6%HBVHBV 99% / 99.6% 99% / 99.6% HCVHCV 100% / 99.4%100% / 99.4%
Source: J-P Allain
Real World Testing –The Need for Simple Rapid Tests:•Rudimentary lab facilities•Poorly maintained equipment•Interruptions to power supply•Unreliable refrigeration•Interruption in supply of tests•Poor training and performance

LACSLEWNDEN2WEE(VEE)CTF
LACSLEPOWWNDEN2EEEHJEVE(VEE)
EEEWEEVEEMAYWNDEN2
EEEWEEVEEMAYSLEWNYFDEN2
SINCHIKWNYFDEN2TAH
SINPOW(TBE)WN(TAH,INK)
CHIKSINPOW(TBE)JEWNSSH
RRBFSINMVEDEN2
Global Distribution of Major Human Flaviviruses

2010
nanobiotechnologies
1990
Ag / Ab
serology
2000
NAT
molecular biology
Microarrays ?
genomics
Emerging technologies

AcknowledgementsAcknowledgements
ARCBSARCBS
Clive SeedClive Seed
Angelo Angelo MargaritisMargaritis
Phil Phil KielyKiely
Dr Tony KellerDr Tony Keller












![Inflammatory manifestations of HTLV-1 and their ... · HTLV-1 and HTLV-2 can usually be discriminated [35]. The immune response to HTLV-1 is strong and the serum antibody titer, which](https://static.fdocuments.in/doc/165x107/5f2ee3b1fcc4502be05de1e8/inflammatory-manifestations-of-htlv-1-and-their-htlv-1-and-htlv-2-can-usually.jpg)




