
Blanca Vazquez, MD
31
Women and Epilepsy Women and Epilepsy Across the Reproductive Across the Reproductive Years Years Blanca Vazquez,MD Director of Clinical Trials Comprehensive Epilepsy program NYU Medical Center
-
Upload
nyu-faces -
Category
Health & Medicine
-
view
1.242 -
download
2
Transcript of Blanca Vazquez, MD

Women and EpilepsyWomen and Epilepsy Across the Reproductive YearsAcross the Reproductive Years
Blanca Vazquez,MD
Director of Clinical Trials
Comprehensive Epilepsy program
NYU Medical Center

Special Considerations in woman Special Considerations in woman
With EpilepsyWith Epilepsy
• Sexuality
• Mood
• Menstrual cycle regularity
• Hormonal contraception
• Fertility
• Bone health
• Pregnancy/breastfeedingMorrell MJ. Epilepsia. 1996;37(suppl 6):S34-S44.
Quality Standards Subcommittee of the American Academy of Neurology. Neurology. 1998;51:944-948.

Epilepsy and SexualityEpilepsy and Sexuality

• Psychosis -- Ictal, Interictal, Post-Ictal
• Anxiety
• Mood Disorders
• Behaviour/Personality
• NES
• AEDs’ Psychotropic Effects

PubertyPuberty
• Several primary generalized seizure syndromes often begin in teens and early 20’s
– Juvenile myoclonic epilepsy– Juvenile absence epilepsy
• Levels of steroid hormones, specifically testosterone, increase during puberty
• Testosterone is converted to:– Estrogen, which is proconvulsant– 3-androstanediol, which is anticonvulsant

Polycystic Ovary Syndrome Polycystic Ovary Syndrome NIH Diagnostic CriteriaNIH Diagnostic Criteria ♀ Presence of ovulatory dysfunction, polymenorrhea, oligomenorrhea, or amenorrhea
♀ Clinical evidence of hyperandrogenism and/or hyperandrogenemia
♀ Exclusion of other endocrinopathies (eg, Cushing syndrome, hypothyroidism, late-onset congenital adrenal hyperplasia)
Duncan S. Epilepsia. 2001;42(suppl 3):60-65.
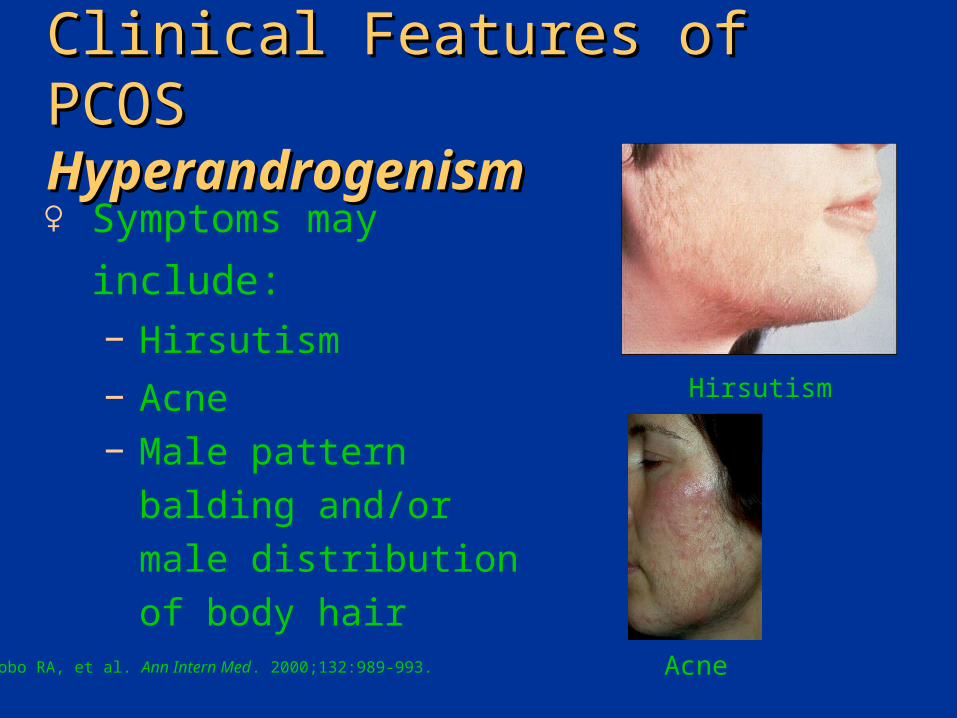
Clinical Features of PCOSClinical Features of PCOS HyperandrogenismHyperandrogenism
♀ Symptoms may
include:− Hirsutism
− Acne− Male pattern balding and/or male distribution of body hair
Lobo RA, et al. Ann Intern Med. 2000;132:989-993.
Hirsutism
Acne

AEDs and ContraceptionAEDs and Contraception• High potential for interaction between some
AEDs and oral contraceptives (OCs) since
both utilize isoenzyme CYP 3A4
• OCs are metabolized by liver, highly protein-
bound and have low and variable
bioavailability
• Inducing effects of some AEDs on estradiol
and progesterone may explain OC failure

Contraception Choices for Contraception Choices for Women with EpilepsyWomen with Epilepsy• Hormonal contraception
– Contraceptive pills– Injectables and depots– Patches
• Rings• Barrier methods• Intrauterine contraceptive devices (IUCDs)• Surgical sterilization• Natural methods

Family Planning for Women on Family Planning for Women on Antiepileptic Drugs (AEDs): Interaction Antiepileptic Drugs (AEDs): Interaction With Hormonal ContraceptionWith Hormonal Contraception
Possible Interaction No Interaction
Carbamazepine GabapentinFelbamate
Oxcarbazepine* Levetiracetam
Phenobarbital Tiagabine
Phenytoin Valproate
Topiramate*
Lamotrigine Zonisamide
*At higher dosage.

Catamenial SeizuresCatamenial Seizures
• Changes in seizure patterns may begin with hormonal fluctuations at menarche and continue during the menstrual cyclea,b
• 30%-50% have epileptic patterns that correspond to their menstrual cycleb,c
– Vulnerability to seizures is highest just before and during flow and at ovulation (relatively high estrogen and low progesterone levels)
aHerzog AG, et al. Epilepsia. 1997;38:1082-1088.bCramer JA, Jones EE. Epilepsia. 1991;32(suppl 6)S19-S26.cMorrell MJ. In: Wyllie E, ed. The Treatment of Epilepsy: Principles and Practice. 2nd ed. Baltimore, Md: Williams & Wilkins; 1997:179-187.

Seizure Frequency in Normal Seizure Frequency in Normal CycleCycle
Average Numberof Seizures Per DayMenstrual0.3
0.4
0.5
0.6
Follicular
Ovulatory Luteal
*P<0.001 vs. ovulatory or luteal and ovulatory and
luteal combined
Number of seizures=1324
Number of cycles=98
*
*
Mean number of
seizures/day
Herzog AG, et al. Epilepsia. 1997;38:1082-1088.
Treatment of Catamenial Treatment of Catamenial EpilepsyEpilepsy
• Difficult to control with AEDs
• Increasing doses of AEDs premenstrually may be beneficial– Important to monitor serum levels to avoid
under- or overdosing
• Acetozolamide of limited benefit
• Natural progesterone for women with regular menses

Effects of AEDs on Body Effects of AEDs on Body WeightWeight
• Weight change important consideration– Leads to health hazards– Impairs body image and self-esteem– Leads to noncompliance
• Most data anecdotal• Actual incidence and magnitude
unknown• Mechanisms unclear
Biton V. CNS Drugs. 2003;17(11):781-791.

Effects of AEDs on Body Effects of AEDs on Body WeightWeight
Gain Neutral Loss
Valproate Lamotrigine Topiramate
Gabapentin Levetiracetam Zonisamide
Carbamazepine
Phenytoin Felbamate
Tiagabine

Retrospective Analysis Retrospective Analysis Of Bone DensityOf Bone Density
• Retrospective analysis of bone density in 153 men and women with epilepsy treated with enzyme-inducing AEDs in an outpatient practice
• Density at femoral neck determined by DXA scan
Pack AM, et al. Epilepsy Behav. 2003;4(2):169-174.
Possible MechanismsPossible Mechanisms
• Induction of cytochrome P450 • enzyme system • Impaired absorption of calcium• Impaired bone resorption and formation• Inhibition of response to parathyroid hormone
(PTH)• Hyperparathyroidism • Vitamin K deficiency • Calcitonin deficiency
Feldcamp J, et al. Exp Clin Endocrinol Diabetes. 2000;108(1):37-43. Koch KH, et al. Epilepsia. 1972;13(6):829-834.Onodera K, et al. Life Sci. 2002;70(13):1533-1542.Valimaki MJ, et al. J Bone Miner Res. 1994;9(5):631-637. Vernillo AT, et al. Matrix. 1990;10(1):27-32. Weinstein RS, et al. J Clin Endocrinol Metab. 1984;58(6):1003-1009.

ConclusionConclusion• PHT, CBZ, and VPA are associated
with low calcium
• PHT is associated with increased bone turnover
• Vitamin D levels are normal suggesting that there are other mechanisms for AED-associated bone disease

Treatment of AED Associated Treatment of AED Associated Bone DiseaseBone Disease
• Multiple therapies available for bone disease
– Calcium – Vitamin D supplementation– Bisphosphonates– Hormone replacement– Calcitonin
• Few studies evaluating the effect of therapies in AED-associated bone disease

Calcium RDACalcium RDA
• Adolescents/Young Adults– 11-24 years 1,200-1,500 mg calcium
• Men– 25-65 years 1,000– Over 65 years 1,500
• Women– 25-50 years 1,000– Over 50 years
(postmenopausal)• On estrogens 1,000• Not on estrogens 1,500
– Over 65 years 1,500– Pregnant and nursing 1,200-1,500

Fetal Anticonvulsant Fetal Anticonvulsant SyndromeSyndrome
• Not drug specific
• Features modify as child grows
• Can be seen with newer as well as older AEDs – Lamotrigine, topiramate
• Clinically indistinguishable from fetal alcohol syndrome

Clinical DilemmaClinical Dilemma
• Drugs generally contraindicated in pregnancy• Women with epilepsy are unable to stop using AEDs
– Increases risk of seizures• Injury• Miscarriage• Developmental delay
– Loss of job or driving privileges– Risk of cognitive decline
• Complications of pregnancy and labor• Risk of congenital malformations may be increased
by AED therapy

PregnancyPregnancyImpact on Maternal SeizuresImpact on Maternal Seizures• Etiology: declining AED concentration
– Decreased protein binding– Increased clearance– Increased plasma volume– Increased renal blood flow
• All AEDs decline
• The more weakly bound, the greater the decline
• 50% of women with epilepsy have seizures when AED levels fall below therapeutic range
Krishnamurthy KB, et al. Epilepsia. 2002;43(suppl 7):232-233.

Folate and Neural Tube Folate and Neural Tube DefectDefect
• Numerous studies of vitamin supplementation
• Pivotal study1
• Supplementation began at least 28 days before conception and continued at least until second missed menses
– Fewer malformations in vitamin supplemented group (13.3 vs. 22.9 per 1000)
– Fewer NT defects in vitamin supplemented group (0 vs. 6)
1. Czeizel AE, Dudas I. N Engl J Med. 1992;327:1832-1835.

Folate SupplementationFolate Supplementation• Centers for Disease Control and Prevention
recommends preconceptional folic acid
– 0.4 mg/d for all women
– 4.0 mg/d for women with a history of previous NT
defect

North American AED and North American AED and Pregnancy RegistryPregnancy Registry
• Toll-free number: 888-233-2334
• Established in 1996
• Higher than expected risk of malformations with phenobarbital and valproate
• Prospective surveillance of AED in pregnancy

What Is the Safest AED What Is the Safest AED in Pregnancy?in Pregnancy?
• No drug without risks
• Maternal seizures hazardous
• Valproate has an additional risk of developing an
NT defect (1%–2%)
• Monotherapy (seizure control)
• Phenobarbital has no advantage
• Choose the best AED for the seizures

1. Zahn CA, et al. Neurology. 1998;51:949-956.2. Quality Standards Subcommittee of the American Academy of Neurology.
Neurology. 1998;51:944-948.
Breastfeeding and AEDsBreastfeeding and AEDs• Assess risks and benefits for individual patients
• AED concentration in breast milk related to protein binding1
• PB and other sedating AEDs may cause sedation or poor feeding1
• American Academy of Neurology encourages breastfeeding with close observation of baby2

Menopausal WomenMenopausal WomenEpilepsy PatternEpilepsy Pattern
0
5
10
15
20
25
30
35
40
45
Increase
Decrease
No change
Catamenial
pattern
Percent of women
*Significantly associated with a decrease in seizures (P=0.013)Harden CL, et al. Epilepsia. 1999;40(10):1402-1407.
*

AEDs and MenopauseAEDs and Menopause• Fluctuation in seizure frequency and
severity may necessitate adjustments to dosing
• No statistically significant association between premature ovulatory failure (early menopause) and AEDs

Women Treated with AEDs Women Treated with AEDs ConclusionConclusion
• Counsel regarding symptoms and signs of reproductive dysfunction
• Monitor bone health• If patient develops reproductive health
dysfunction, bone disease, or excessive weight gain, consider changing to alternate AED
• Provide prophylactic folic acid, calcium, and vitamin D supplementation
• Cooperate with pregnancy registry efforts


















