Bites & Stings
78
2 nd Year
description
types of bites and stings and its management
Transcript of Bites & Stings
2nd Year
OBJECTIVES OF THE CLASS
POISONINGA poison is any agent or substance absorbed
into the system through epithelial surfaces.POISONING AGENTS-Kerosene oilBarbituratesOrganophosphate compoundsCorrosives 90% exposure occurs at home.

1. ORGANOPHOSPHORUS POISONINGMay be acute or chronicChronic exposure may be dietaryAggregate exposureCumulative exposureChildren are at higher risk
SIGNS AND SYMPTOMSBlurring of visionHeadacheGiddinessNauseaChest pain Profuse salivationSweatingConstricted pupilsDeath is usually due to respiratory failure.

EMERGENCY MANAGEMENT1. Assess the victim- ABC, need for CPR2. Watch out for seizures3. Terminate exposure
Empty mouth of poison/agentRemove contaminated clothesFlush eyes continuously with NS or tap water
at home for 15 to 20 mins.Flush skin and wash with soap and a soft clothBring victim into fresh airGive a sip of water to dilute ingested poisonIdentify the poison.

ONGOING MANAGEMENTReduction of dermal contact and gastric emptying
Activated charcoal- 1 g/kgOther cathartics not recommended
Within 60 minutes of poison ingestion
Antidote Atropine sulphate- 0.03-0.04mg/kg IV, repeated after 15 minutes and then every hour until atropinization (maximum 1 mg/kg in 24 hr)
KEROSENE POISONINGChemical pneumonitis
RestlessnessFeverAbdominal distensionConvulsions and coma
Symptomatic treatmentGastric lavage is contraindicated.

LEAD POISONINGLead is present in lead based paints, food cac
soldering, dyes, toys, pottery, ceramic ware, cosmetics and even in water.
Over 51% of the children below the age of 12 living in major urban areas had unacceptably high levels of 10mcg/dl or more.
The George Foundation15-18 million children in developing countries
have permanent brain damage due to lead poisoning
WHO.

Children’s bodies are much more receptive to lead.
A child absorbs approx. 50% of exposed lead whereas an adult absorbs only 10%.
Normal hand to mouth behavior and presence of lead dust in the environment is the usual method of poisoning.
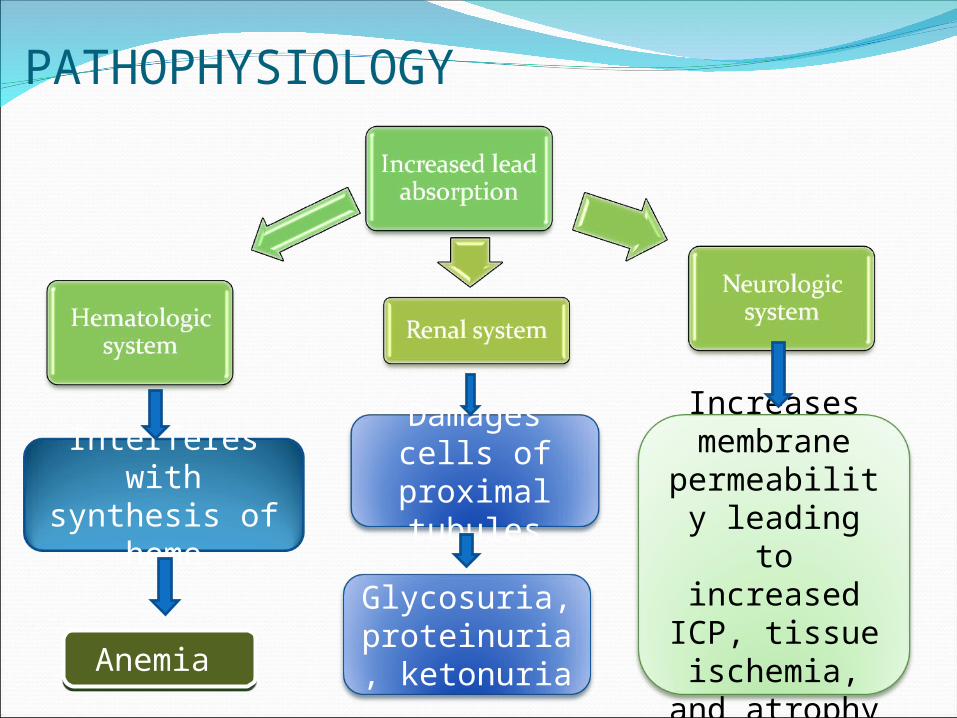
PATHOPHYSIOLOGY
Glycosuria, proteinuria, ketonuria
Damages cells of
proximal tubules
Interferes with synthesis of
heme
Anemia Anemia
Increases membrane
permeability leading to increased ICP, tissue
ischemia, and atrophy
CLINICAL MANIFESTATIONSMild to moderate lead poisoning can cause a
number of cognitive and behavioral problems in young children.
Behavioral effects-AggressionHyperactivityImpulsivenessDelinquencyDisinterestWithdrawal
Neurocognitive effects-Developmental delaysLower IQ scoresSpeech problemsReading skill deficitsVisual-spatial problemsVisual motor problemsLearning disabilitiesLower academic success

Children with extremely high levels of lead manifest with seizures, resulting in coma and death.
DIAGNOSTIC EVALUATIONA fingerstick blood specimen screening testBlood lead level (BLL) testAcceptable serum value- <10mcg/dl.Erythrocyte proto porphyrin (EP) test

Management of lead poisoningA BLL greater than 20mcg/dl requires clinical
management.Environmental investigationFamily education
Harmful efffectsSourcesImportance of wet cleaningGood nutritionFollow up
Chelation therapyBritish antilewisite (BAL) or dimercapolCalcium di sodium edetate (EDTA)Succimer or DMSA
Maintain adequate hydration Periodic monitoring of LFT and KFT
PROGNOSISMost pathophysiologic effects are reversible.Permanent brain damage can lead to
MR, Behavioral changes, Possible paralysis and Seizures.
NURSING CARE Reducing exposure to leadGood nutrition- calcium and ironCare during chelation therapyParent education
BITES: SNAKE BITEMore people in India die of snake bite than
the rest of the world put together.(50,000/year!)
Common poisonous snakes are- cobra, vipers, sea snake, krait
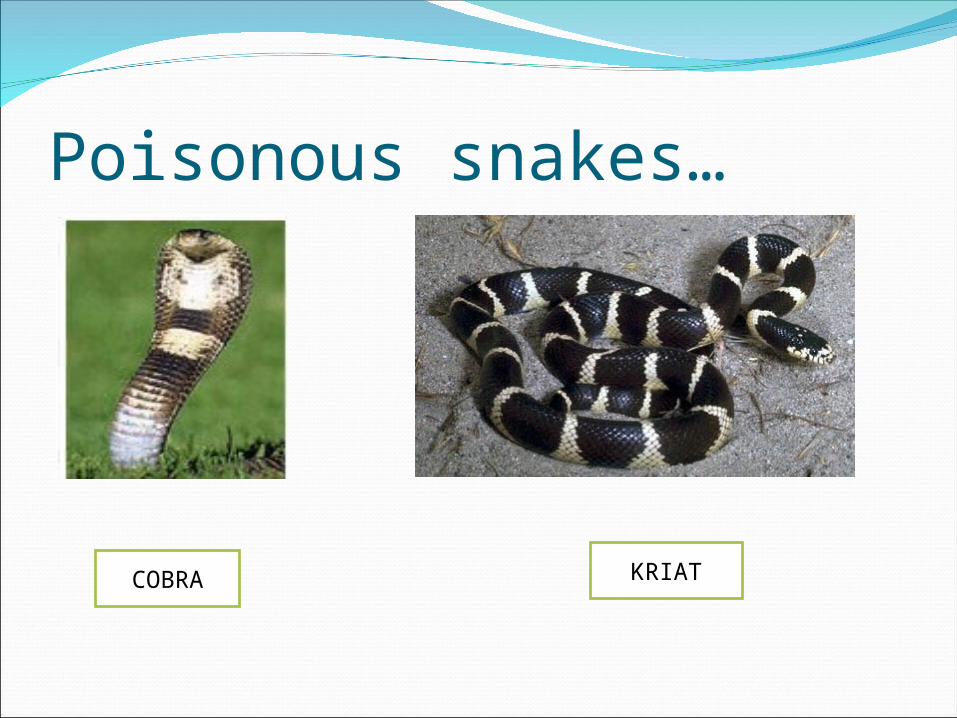
Poisonous snakes…
COBRA KRIAT

VIPER RATTLE SNAKE
Clinical manifestationsLocal tissue destruction
Soft pitting edema that generally develops over 6-12 hours but may start within 5 minutes
Bullae Streaking Erythema or discoloration Contusions

Systemic toxicity Hypotension Petechiae, epistaxis, hemoptysis Paresthesias and dysthesias - Forewarn neuromuscular blockade and respiratory distress (more common with coral snakes)
Investigation Complete blood countUrinalysis PlateletsCreatinineProthrombin timeBlood urea nitrogen
First aid Keep the person calm. Restrict movement Keep the affected area below heart level to
reduce the flow of venom. Remove any rings or constricting items . Create a loose splint to help restrict
movement of the area.
If the area of the bite begins to swell and change color, the snake was probably poisonous.
Monitor the person's vital signs if possible.
Monitor for signs of shock.Get medical help right away.Bring in the dead snake only if this
can be done safely. Do not give antivenom in the field.

In the hospital…ABCs. Monitor vital signs and establish a large-bore
IV line. Administer oxygen therapy. Keep a close watch on the airway at all times in
case intubation becomes necessary. Restrict activity and immobilize the affected
area.Negative-pressure suctioning devices offer
some benefit if used within several minutes of envenomation.
Immediately transfer to definitive care.

DON’TSMake an incision over the bite, Mouth suctioning, Tourniquet use, Ice packs, electric shock.

ANTI VENOMFirst 10-20 minutes…5 vials in 250ml of NS (125ml for infants
weighing <10kgs)Administer slowly (1-2ml/hr)If no adverse reaction…Complete total volume in 2 hoursContinue to administer 5 vial aliquots until
there is no further progression of swelling.
Administer other therapy as necessary-
Pain medicationAntibioticsTetanus toxoidWound debridement

SCORPION BITEScorpions usually hide during the day and
are active at night. Not all scorpion bites are lethal.Most sting in self defenceOnly one considered lethal- Centruroides
sculpturatus

SYMPTOMSA stinging or burning sensation at the
injection site (very little swelling or inflammation)
Positive "tap test" (i.e., extreme pain when the sting site is tapped with a finger)
Restlessness Convulsions Roving eyes Staggering gait

Thick tongue sensation Slurred speech Drooling Muscle twitches Abdominal pain and cramps Respiratory depression

TREATMENTSymptomatic treatmentTetanus prophylaxisScorpion sting antivenin if available.
DOG BITE80-90% of reported animal bitesBoys most often the victimThe dog is known to the victim in 90% of
casesExtremities are the most frequent sitesHead and neck bites are most common in
children

FIRST AIDWash the wound with soap & waterApply a clean dressing over the woundSeek medical help

TREATMENTAntirabies serum to be infiltrated if wound is
<24 hours old (20IU/kg).Give remainder by IMTTActive immunization by rabies vaccine
Cell derivedNerve cell tissue origin- not used now a days as
it is less potent and associated with adverse effects
Pre exposure prophylaxis-3 doses (0.1 ml) on day 0,7, & 28 IM or IDBooster doses every 5 yearsPost exposure treatment-5 doses on day 0,3,7,14, & 28 IM or,2 doses on day 0 followed by 1 dose on day 7
& 21 (4 doses)If immunized-2 doses separated by 3 days (IM or ID)
FRACTURESFracture is a break in the continuity of a
bone. Bone fracture occurs when the resistance of a bone against the stress yields to the stress force.
CAUSATIVE FACTORS-1. Accidents2. Child abuse3. Trauma during delivery
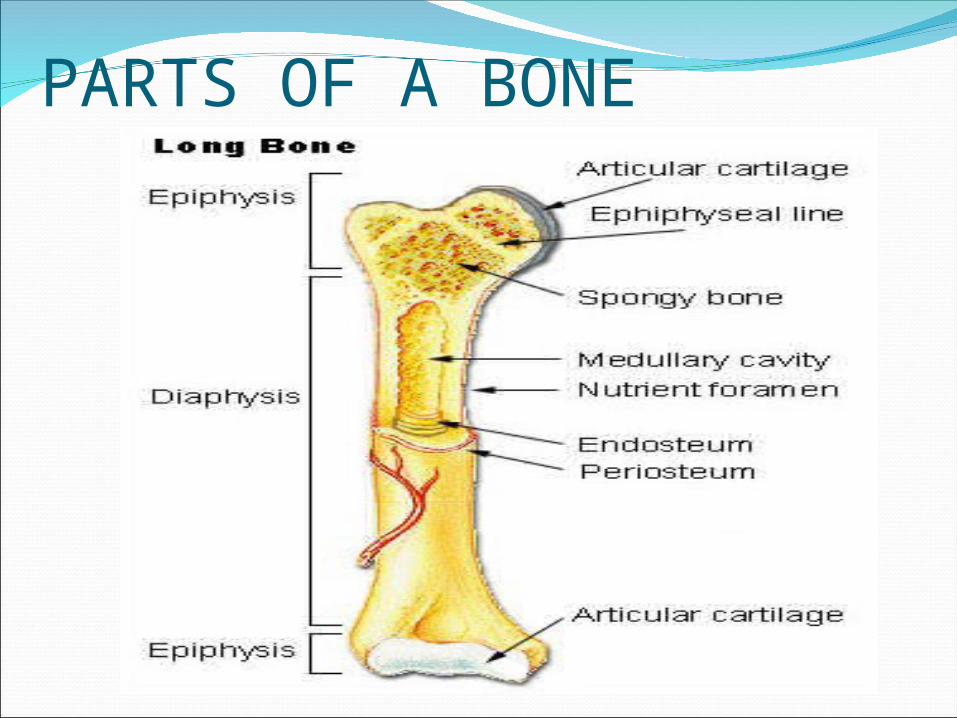
PARTS OF A BONE

GROWTH PLATE
CHARACTERISTICS OF FRACTURES IN CHILDRENAccording to Rang and Willis-1. The growth plates have a rubber like
consistency.2. Thick periosteum3. Plastic bone- porous and flexible.4. Rapid healing5. Stiffness not usual6. Response to injury
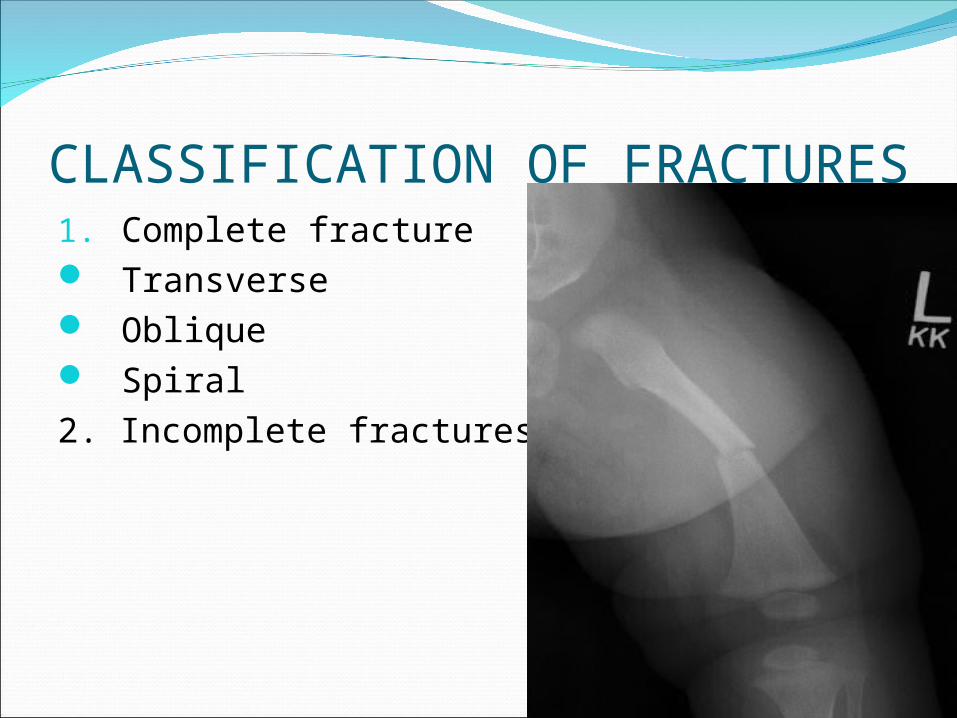
CLASSIFICATION OF FRACTURES1. Complete fracture Transverse Oblique Spiral2. Incomplete fractures
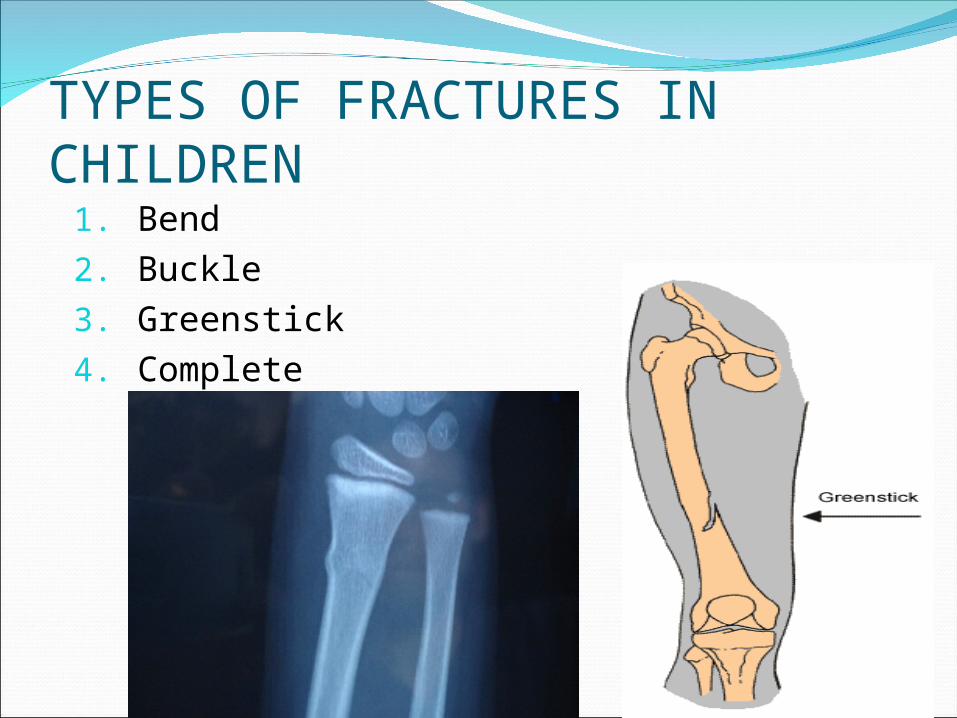
TYPES OF FRACTURES IN CHILDREN1. Bend2. Buckle3. Greenstick4. Complete

CLINICAL MANIFESTATIONSGeneralised swellingPain and/or tendernessDeformityDiminished functional use of affected part

Child may also demonstrate-BruisingSevere muscular rigidityCripitus
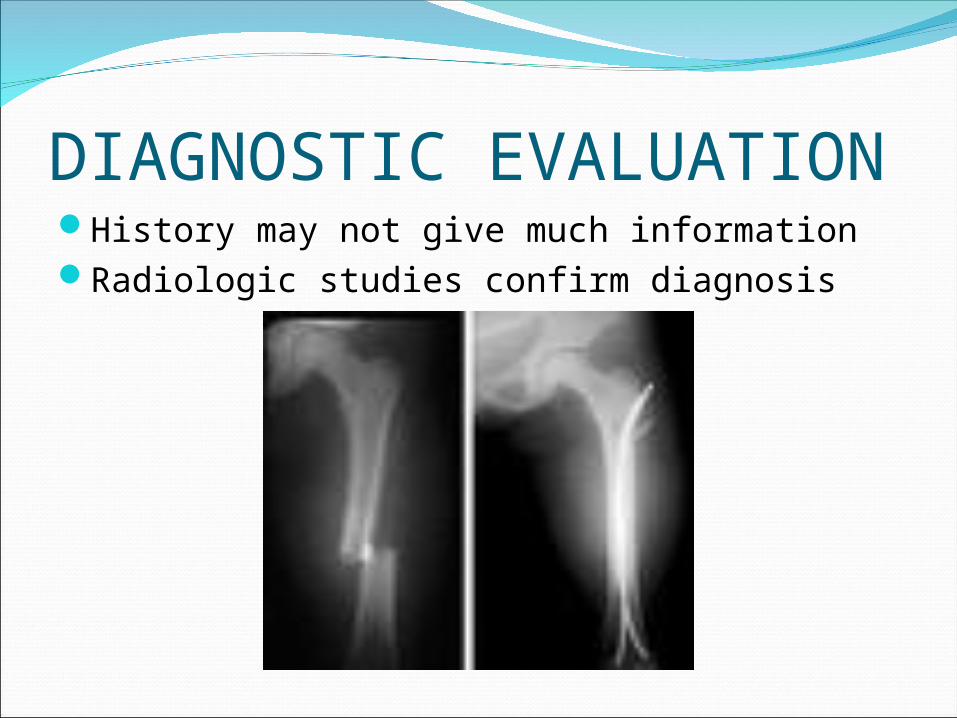
DIAGNOSTIC EVALUATIONHistory may not give much informationRadiologic studies confirm diagnosis
MANAGEMENTGOALS- To regain allignment and length of the bony
fragments (reduction) To retain allignment and length
(immobilization) To prevent further injury

EMERGENCY TREATMENT1. Assess the site of injury : 5Ps Pain and point of tenderness Pallor Pulse* Parasthesia* Paralysis** Distal to the fracture site
EMERGENCY TREATMENT2. Determine the mechanism of injury3. Move the injured part as little as possible4. Cover open wounds with a sterile or clean
dressing5. Immobilise the limb, including the joints
above and below the fracture site
EMERGENCY TREATMENT6. Do not attempt to reduce the fracture or
push protruding bone underneath!7. Use soft but rigid splint8. Reassess neurovascular status9. Apply traction if circulatory compromise is
present10. Elevate the injured limb if possible11. Apply cold to the injured area12. Call emergency or transport to a medical
facility
METHODS OF FRACTURE REDUCTION1. Closed reduction- This is achieved by bringing the bone
fragments into opposition by manipulation and manual traction
2. Traction- Traction is the pulling force
applied in a longitudinal direction to reduce a fracture.
3. Open reduction- Reduction under direct
visualisation by surgery

METHODS OF IMMOBILISATIONCasts- Casts are
constructed from gauze strips or bandages impregnated with plaster of paris or synthetic lighter weight and water resistant materials. Eg. Fibre glass.

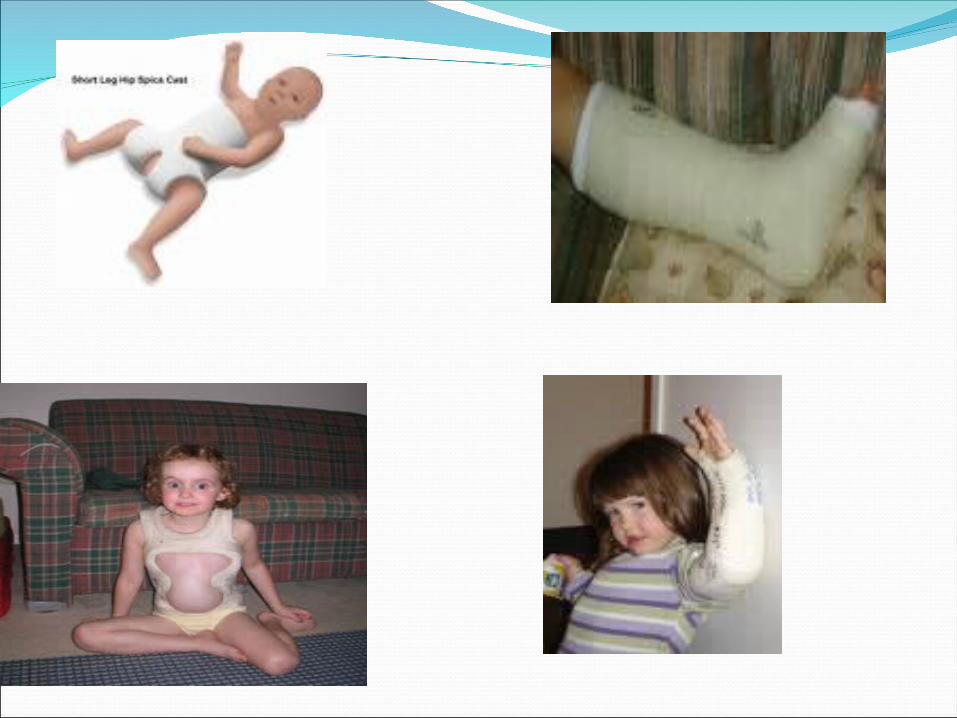
TYPES OF CASTSUpper extremity cast- ankle or kneeLower extremity cast- wrist or elbowSpinal or cervicalSpica cast- hip and knee
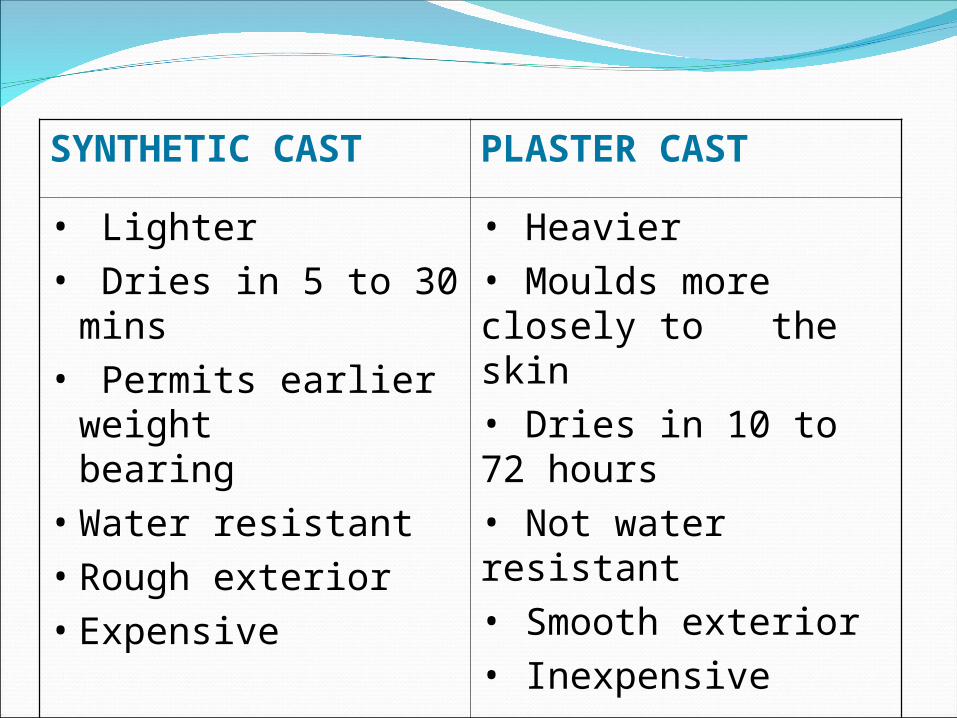
SYNTHETIC CAST PLASTER CAST
• Lighter• Dries in 5 to 30 mins• Permits earlier weight
bearing• Water resistant• Rough exterior• Expensive
• Heavier• Moulds more closely to the skin• Dries in 10 to 72 hours• Not water resistant• Smooth exterior• Inexpensive

Nursing care of a child with a cast-1. Prevention of circulatory, neurologic or
respiratory disturbance. Support wet cast with palms Elevate and support extremity Assess neurovascular status Measure area of bleeding or discolorisation Assess tightness of the cast Assess vital signs
2. Maintenance of body temperature-Check temperature routinely

3. Maintenance of skin integrity and prevention of infection.
Trim, pad and petal rough edges of the castAssess skin for pressure or signs of irritation
or infectionInspect for objects or food particles
underneath the castProvide stout play materialsAssess for presence of “hot spots” on the cast
4. Maintenance of cast integrity and cleanliness
Use plastic sheets to protect the perineumElevate head and upper body higher than the
buttocksTurn the child every 2 hourly
5. Promotion of appropriate muscle activity
6. Provision of comfort measures7. Prevention of urinary stasis and constipation
8. Provision of support during cast removal.
9. Promotion of skin integrity after cast removal

CARE OF A CHILD IN TRACTIONPURPOSES-To provide rest to an extremityTo prevent or improve contracture deformityTo correct deformityTo treat a dislocationTo provide immobilisationTo reduce muscle spasm

COMPONENTS OF TRACTION MANAGEMENTTractionCounteractionFriction
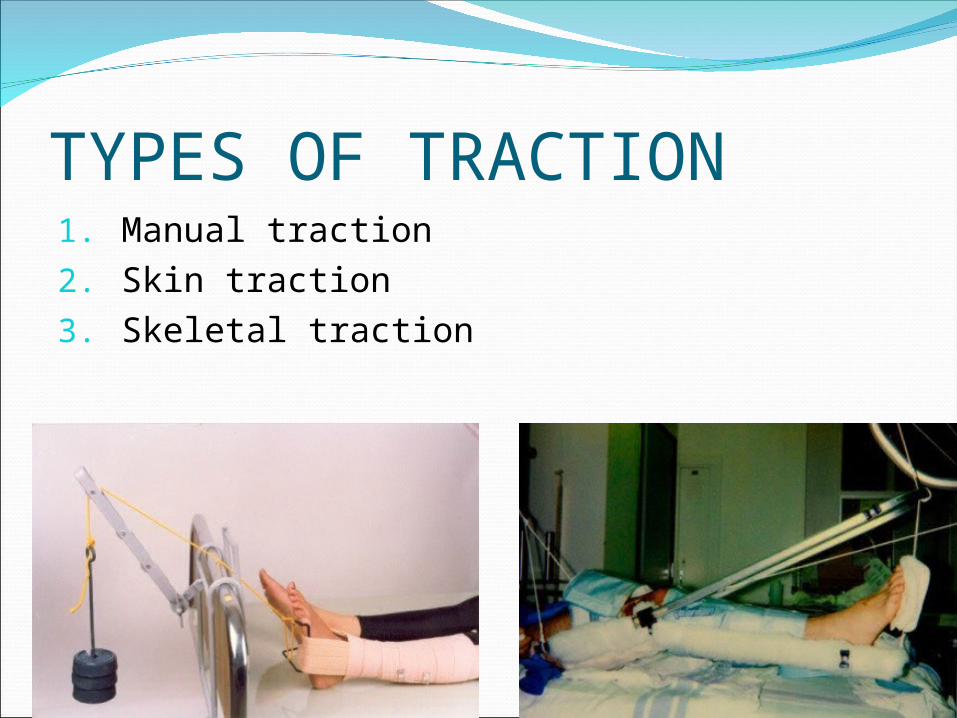
TYPES OF TRACTION1. Manual traction2. Skin traction3. Skeletal traction
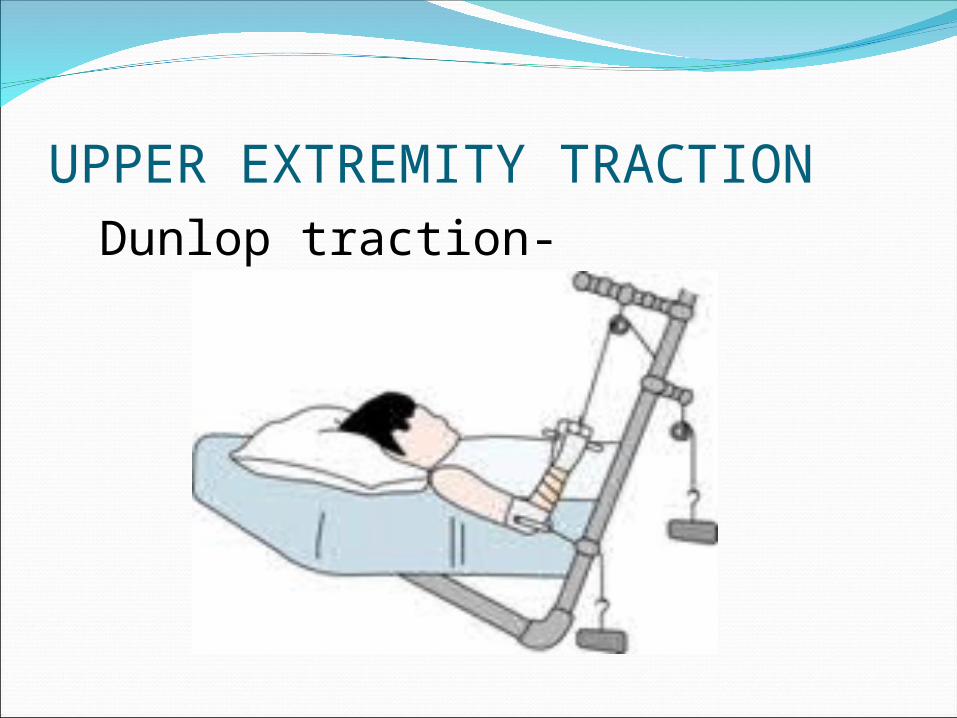
UPPER EXTREMITY TRACTION Dunlop traction-
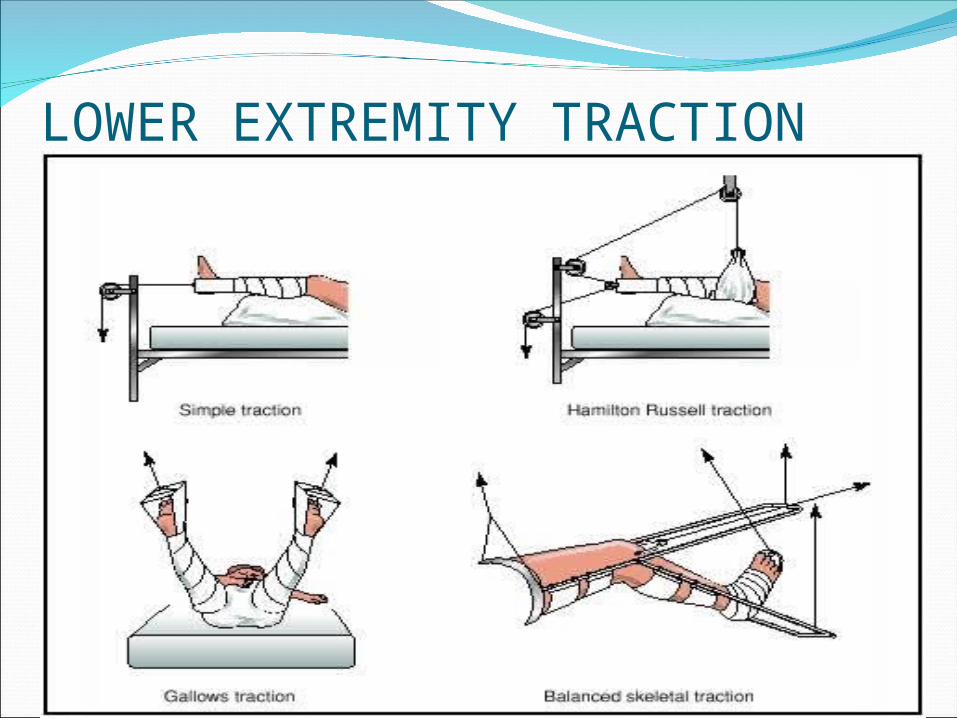
LOWER EXTREMITY TRACTION

Cervical tractionHalo vestCrutchfield tong traction

NURSING MANGEMENTUnderstand therapyMaintain traction- - Check desired line of pull - Function of each component - Position of bandages, frames and splints - Ropes are in the center of pulleys - Wheels are freely movable - Weights are of correct amount

Maintain allignmentSkin traction- - Replace bandages only if absolutely
necessary but maintain traction during procedure
- Bandage should not be too loose nor too tight
Prevent skin breakdownProvide pressure mattressCheck for redness and skin breakdownWash and dry skin dailyInspect pressure points dailyStimulate circulation with gentle massageChange position at least 2 hourly
Care of skeletal tractionCheck pin sites for bleeding, inflammation or
infectionDress and cleanse pin sitesApply antiseptic ointmentCover ends of pins with protective cord or
paddingNote pull of traction on pin
Prevent complicationsCheck pulses in affected areasAssess dressings for excessive tightnessEncourage deep breathingNote any neurovascular changesCarry out active-passive exercisesProvide fibre rich nutritious diet

What did we learn today?
Match the following…Group A Group B
1. Fracture2. OP poisoning3. Scorpion bite4. Dog bite5. Lead poisoning
a) Rabiesb) Greenstickc) Positive tap testd) Low IQe) Atropine

ReferencesThomas D.O., Bernardo, L.M., & Herman, B.
(Eds.) (2003). Core curriculum for pediatric emergency nursing. Emergency Nurses Association. London
WHO (2009). WHO Model formulary.