Birth Defect Prevention: Global Issues - WHO Key Points • 65th World Health Assembly Resolution:...
35
1 Lorenzo D. Botto, MD Division of Medical Genetics University of Utah, USA Pierpaolo Mastroiacovo, MD International Center on Birth Defects Rome, Italy Birth Defect Prevention: Global Issues WHO, Geneva, 16 January 2012: Hosts, Dr. Mario Merialdi, Dr. JP Pena‐Rosas International Clearinghouse for Birth Defects Surveillance and Research ICBDSR WHO Collaborating Center WHO 2012 ‐ Global issues in Birth Defect Prevention Botto ‐ Mastroiacovo |1 42 Members in 38 Countries, and one Centre (ICBD, Rome) 42 Members in 38 Countries, and one Centre (ICBD, Rome) Utah Atlanta Texas California Canada National British Columbia Alberta Cuba Japan (China) Russia Ukraine Western Europe 21 Registries 14 Countries I l India Mexico Costa Rica Chile Maule ECLAMC 10 Countries Western Australia Victoria New Zealand Iran Israel Colombia WHO 2012 ‐ Global issues in Birth Defect Prevention Botto ‐ Mastroiacovo |2
Transcript of Birth Defect Prevention: Global Issues - WHO Key Points • 65th World Health Assembly Resolution:...

1
Lorenzo D. Botto, MDDivision of Medical GeneticsUniversity of Utah, USA
Pierpaolo Mastroiacovo, MDInternational Center on Birth Defects
Rome, Italy
Birth Defect Prevention: Global Issues
WHO, Geneva, 16 January 2012: Hosts, Dr. Mario Merialdi, Dr. JP Pena‐Rosas
International Clearinghouse for Birth Defects Surveillance and Research ICBDSR
WHO Collaborating Center
WHO 2012 ‐ Global issues in Birth Defect Prevention Botto ‐Mastroiacovo | 1
42 Members in 38 Countries, and one Centre (ICBD, Rome)42 Members in 38 Countries, and one Centre (ICBD, Rome)
Utah
Atlanta
Texas California
Canada National
British ColumbiaAlberta
CubaJapan
(China)Russia
Ukraine
Western Europe21 Registries14 Countries
I lIndia
Mexico
Costa Rica
Chile Maule
ECLAMC10 Countries
Western AustraliaVictoria
New Zealand
IranIsrael
Colombia
WHO 2012 ‐ Global issues in Birth Defect Prevention Botto ‐Mastroiacovo | 2
2
Key Points
• 65th World Health Assembly Resolution: call to global action for birth defect surveillance, treatment, prevention
• Modifiable risk factors: what can we do now that works?
• Global opportunities: surveillance, training, prevention
WHO 2012 ‐ Global issues in Birth Defect Prevention Botto ‐Mastroiacovo | 3
Key Points
• 65th World Health Assembly Resolution: call to global action for birth defect surveillance, treatment, prevention
• Modifiable risk factors: what can we do now that works?
• Global opportunities: surveillance, training, prevention
WHO 2012 ‐ Global issues in Birth Defect Prevention Botto ‐Mastroiacovo | 4

3
65th World Health Assembly Resolution
The call to action: urges Member States
• To raise awareness of the importance of birth defects asTo raise awareness of the importance of birth defects as cause of child morbidity and mortality
• To develop and strengthen registration and surveillance of birth defects
• To strengthen research and studies on etiology, diagnosis and prevention of major birth defectsand prevention of major birth defects
WHO 2012 ‐ Global issues in Birth Defect Prevention Botto ‐Mastroiacovo | 5
The call to action: requests the Director‐General
• To promote the collection of data on the global burden
65th World Health Assembly Resolution
of mortality and morbidity due to birth defects
• To continue to collaborate with the ICBDSR to improve collection of data on birth defects
• To support Member States in developing national plans for implementation of effective interventions to prevent and manage birth defects.
WHO 2012 ‐ Global issues in Birth Defect Prevention Botto ‐Mastroiacovo | 6

4
Birth DefectsBirth Defects3% of all births :3% of all births :
burden of disease is high :burden of disease is high :aand increasing everywhere:nd increasing everywhere:
minimum estimateminimum estimatemortality, morbidity, disability, costmortality, morbidity, disability, costalso middle/low income also middle/low income countriescountries
WHO 2012 ‐ Global issues in Birth Defect Prevention Botto ‐Mastroiacovo | 7
Global Issues in Birth Defects = Gaps and Opportunities Global Issues in Birth Defects = Gaps and Opportunities
EvaluationEvaluation ::Prevention :Prevention :
Capacity :Capacity :
llimited/no surveillance programsimited/no surveillance programsknown causes not addressedknown causes not addressedlimited training/expertiselimited training/expertise
WHO 2012 ‐ Global issues in Birth Defect Prevention Botto ‐Mastroiacovo | 8
5
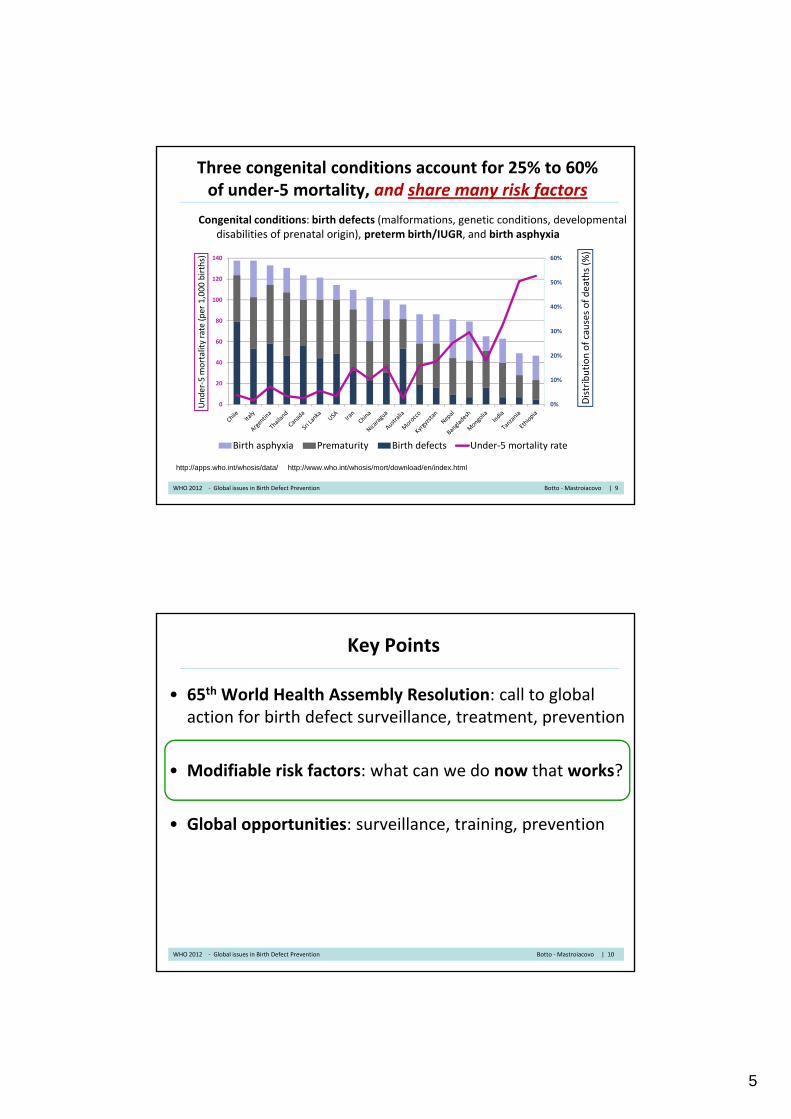
Three congenital conditions account for 25% to 60% of under‐5 mortality, and share many risk factors
Congenital conditions: birth defects (malformations, genetic conditions, developmental disabilities of prenatal origin), preterm birth/IUGR, and birth asphyxia
60%140
(%)
hs)
10%
20%
30%
40%
50%
20
40
60
80
100
120
ribution of causes of deaths
r‐5 mortality rate (per 1,000 birth
0%0 Distr
Under
Birth asphyxia Prematurity Birth defects Under‐5 mortality rate
http://apps.who.int/whosis/data/ http://www.who.int/whosis/mort/download/en/index.html
WHO 2012 ‐ Global issues in Birth Defect Prevention Botto ‐Mastroiacovo | 9
Key Points
• 65th World Health Assembly Resolution: call to global action for birth defect surveillance, treatment, prevention
• Modifiable risk factors: what can we do now that works?
• Global opportunities: surveillance, training, prevention
WHO 2012 ‐ Global issues in Birth Defect Prevention Botto ‐Mastroiacovo | 10

6
Four Pillars of Effective Prevention
LD Botto, Moss and Adams 8th Ed, 2012 in press
SEARO 2011 ‐ Strategies for Birth Defect Prevention Botto | 11
Developmental timing of some birth defects
WHO 2012 ‐ Global issues in Birth Defect Prevention Botto ‐Mastroiacovo | 12

7
Folic acid alone or as a multivitamin prevents over half of neural tube defects
Neural tube defects: from embryology to clinic
N En
glJ Med
341:1509‐1519, 1
999
WHO 2012 ‐ Global issues in Birth Defect Prevention Botto ‐Mastroiacovo | 13
Preventing congenital conditions: mitigating risk factors and promoting protective factors
“Diabesity” Lifestyle Infections Select medications
Physical activity
Folic acid fortification, supplementationHealthy eating
Physical activity
WHO 2012 ‐ Global issues in Birth Defect Prevention Botto ‐Mastroiacovo | 14

8
Crucial challenge worldwide:reduce child mortality, improve maternal‐child health
SEARO 2011 ‐ Strategies for Birth Defect Prevention Botto | 15
Evidence for modifiable risk factors
Folic acid useYes No
Gene variants in folic acid pathway
Biomarkers in folic acid pathway
RCT
CaseControl
Fortification
MTHFR
FolReceptor
etc
Blood folate
B6
Homocysteine
etc
moreclefts
fewerclefts
Different concentration/frequencyin babies with clefts vs. controls
WHO 2012 ‐ Global issues in Birth Defect Prevention Botto ‐Mastroiacovo | 16

9
Risk of Neural‐Tube Defects and the Use of Folic Acid or Multivitamin Supplements, 1981 through 1999
Source: Botto L et al. N Engl J Med 1999;341:1509‐1519
WHO 2012 ‐ Global issues in Birth Defect Prevention Botto ‐Mastroiacovo | 17
Evidence for modifiable risk factors
Folic acid useYes No
Gene variants in folic acid pathway
Biomarkers in folic acid pathway
RCT
CaseControl
Fortification
MTHFR
FolReceptor
etc
Blood folate
B6
Homocysteine
etc
moreNTDs
fewerNTDs
Different concentration/frequencyin babies with NTDs vs. controls
SEARO 2011 ‐ Technical Review Clefts, Limbs, Heart Botto | 18

10
Red Cell Folate Hi h th 906 l/L
Blood folate and neural tube defect risk
Higher than 906 nmol/L
How much Plasma Folate ? How do you get there ?
Daly LE et al.: Jama 1995; 274:1698‐1702
WHO 2012 ‐ Global issues in Birth Defect Prevention Botto ‐Mastroiacovo | 19
Evidence for modifiable risk factors
Folic acid useYes No
Gene variants in folic acid pathway
Biomarkers in folic acid pathway
RCT
CaseControl
Fortification
MTHFR
FolateReceptor
etc
Blood folate
B6
Homocysteine
etc
moreNTDs
fewerNTDs
Different concentration/frequencyin babies with NTDs vs. controls
WHO 2012 ‐ Global issues in Birth Defect Prevention Botto ‐Mastroiacovo | 20

11
Odds ratioCumulative meta-analysis0.1 0.5 1 2 3 5 10
van der Put (1995) ( 55)
677C‐>T variant of MTHFR (folate) gene and neural tube defect risk (patients): cumulative meta‐analysis
( ) ( )Whitehead (1995) ( 137)Papapetrou (1996) ( 178)Ou (1996) ( 219)Mornet (1997) ( 262)BjorkeMonsen (1997) ( 290)van der Put2 (1998) ( 321)Koch (1998) ( 458)Boduroglu (1998) ( 507)Shaw (1998) ( 721)deFranchis (1998) ( 924)Shields (1999) (1195)Christensen (1999) (1251)GarciaFragoso (1999) (1282)Johanning (1999) (1364)Stegmann (1999) (1375)Yu (2000) (1399)Barber (2000) (1423)
C677T MTHFR SNP in NTD-patients and controls (TT vs CC (red) and CT vs CC (green))
Barber (2000) (1423)Volcik (2000) (1657)Richter (2001) (1693)Wenstrom (2001) (1764)Cunha (2002) (1779)Combined TTCT
WHO 2012 ‐ Global issues in Birth Defect Prevention Botto ‐Mastroiacovo | 21
[Source: Vollset and Botto, 2001]
Recommendations for folic acid supplementation had limited or no effect in Europe
BMJ 2005;330:
WHO 2012 ‐ Global issues in Birth Defect Prevention Botto ‐Mastroiacovo | 22

12
Estimated number of pregnancies with neural tube defects preventable by folic acid in study area, 1993‐8. Estimates assume three scenarios of effectiveness (30%, 60%, 90%), which
encompass a reasonable range from low dose fortification to highly effective supplementation
Source: BMJ 2005;330:
WHO 2012 ‐ Global issues in Birth Defect Prevention Botto ‐Mastroiacovo | 23
Fortification with folic acid
No fortification
Planning
Voluntary
Mandatory
WHO 2012 ‐ Global issues in Birth Defect Prevention Botto ‐Mastroiacovo | 24

13
Folic acid reduces the risk of NTD probably down to ~ 0.6 per 1,000 pregnancies
Black vertical line: drop in NTD occurrenceo after FA fortification in 24 areas o after FA supplementation in in 3 RCT and cohort studies
5 0er 1,000
valence of NTD
x 10,000 Dotted blue line: possible threshold of FA‐preventable NTD
5.0
l prevalence of NTD
, p
4.0
3.0
2.0
1 0
Prev
Total 1.0
WHO 2012 ‐ Global issues in Birth Defect Prevention Botto ‐Mastroiacovo | 25
0
Neural tube defect rates per 10,000 population, by race/ethnicity and fortification period status ‐‐‐National Birth Defects Prevention Network,* 1995—2007 (MMWR August 13, 2010 / 59(31);980‐984)
Source: BMJ 2005;330:
WHO 2012 ‐ Global issues in Birth Defect Prevention Botto ‐Mastroiacovo | 26

14
Preventing congenital conditions: NTDsmitigating risk factors and promoting protective factors
“Diabesity” Lifestyle Infections Select medications
Physical activity
Folic acid fortification, supplementationHealthy eating
Physical activity
WHO 2012 ‐ Global issues in Birth Defect Prevention Botto ‐Mastroiacovo | 27
Neural Tube Defects, Oral Clefts, Heart defects
Neural Tube Defects
OrofacialClefts
Heart Defects
Prevalence 6 to 100 15 (CL/P) – 6 (CPO) 80‐90e a e ce(/10,000)
6 to 00(1 in 1,000)
5 (C / ) 6 (C O)(1 in 700)
80 90(1 in 110)
Rate variations +++ ++ +/‐
Key subtypes >3 >2 >12
Coding ICD‐10 Adequate Adequate Challenging for several types
Photographs +++ ++ ‐ (echocardio)
Clinical review ++ ++ +++
Surveillance challenges
+/++‐ External‐ Pregnancy terminations
+‐ External
‐Small cleft palate may be missed at
birth
+++‐Internal
‐ Diagnostic delays, classification
WHO 2012 ‐ Global issues in Birth Defect Prevention Botto ‐Mastroiacovo | 28
15
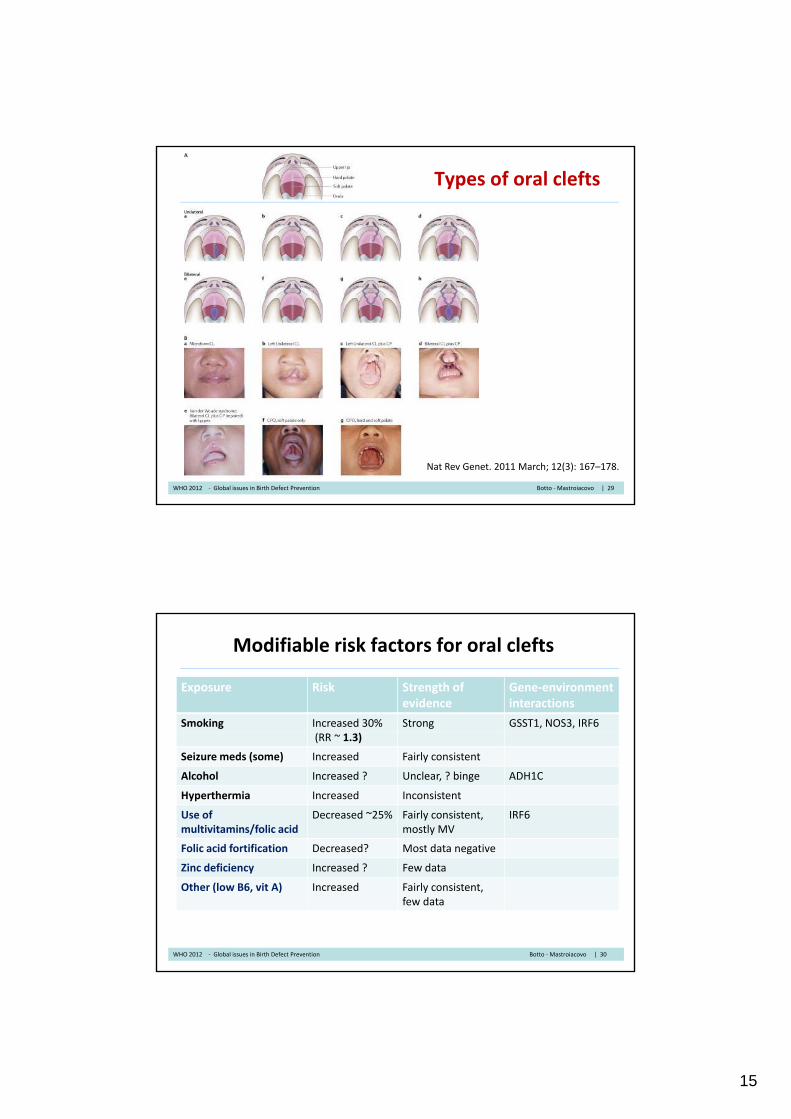
Types of oral clefts
Nat Rev Genet. 2011 March; 12(3): 167–178.
WHO 2012 ‐ Global issues in Birth Defect Prevention Botto ‐Mastroiacovo | 29
Modifiable risk factors for oral clefts
Exposure Risk Strength of evidence
Gene‐environment interactions
Smoking Increased 30% Strong GSST1, NOS3, IRF6(RR ~ 1.3)
Seizure meds (some) Increased Fairly consistent
Alcohol Increased ? Unclear, ? binge ADH1C
Hyperthermia Increased Inconsistent
Use of multivitamins/folic acid
Decreased ~25% Fairly consistent, mostly MV
IRF6
Folic acid fortification Decreased? Most data negativeFolic acid fortification ecreased? Most data negative
Zinc deficiency Increased ? Few data
Other (low B6, vit A) Increased Fairly consistent, few data
WHO 2012 ‐ Global issues in Birth Defect Prevention Botto ‐Mastroiacovo | 30

16
Smoking and cleftsCL/P
CL/P = cleft lit +/‐ cleft palateCPO = cleft palate only
•Consistent relative risk ~1.3 (30% increased risk)
•In some countries, high ratesof smoking in women of childbearing age
• Attributable fraction (fraction ofCPOcases of clefts due to smoking)can be quite high, in the orderof 20%
P Mossey, J Little et al, Lancet 2009
WHO 2012 ‐ Global issues in Birth Defect Prevention Botto ‐Mastroiacovo | 31
Estimated fraction of affected babies due to maternal risk factors, by relative risk and exposure frequency in population
WHO 2012 ‐ Global issues in Birth Defect Prevention Botto ‐Mastroiacovo | 32

17
Modifiable risk factors for oral clefts
Exposure Risk Strength of evidence
Gene‐environment interactions
Smoking Increased 30% Strong GSST1, NOS3, IRF6(RR ~ 1.3)
Seizure meds (some) Increased Fairly consistent
Alcohol Increased ? Unclear, ? binge ADH1C
Hyperthermia Increased Inconsistent
Use of multivitamins/folic acid
Decreased ~25% Fairly consistent, mostly MV
IRF6
Folic acid fortification Decreased? Most data negativeFolic acid fortification ecreased? Most data negative
Zinc deficiency Increased ? Few data
Other (low B6, vit A) Increased Fairly consistent, few data
SEARO 2011 ‐ Technical Review Clefts, Limbs, Heart Botto | 33
Clefts, folic acid, multivitamins: part 1
• Folate deficiency causes clefts in animals
• Folate antagonists (meds) associated with increased risk of OFC
• Hungarian RCT: too small, ‘controls’ took trace elements (incl. Zn)
• Inconsistent findings in case‐control studies of MV with folic acid, maternal dietary folate intake, and red cell and plasma folate
• Fortification: North America, ?small decline in CL/P, not so in Australia (voluntary). For all clefts combined, small decrease in US b i C d Chilbut not in Canada or Chile.
• Open questions: high dose vs. low dose, MV vs. folic acid, recurrence vs. occurrence, population susceptibility
WHO 2012 ‐ Global issues in Birth Defect Prevention Botto ‐Mastroiacovo | 34

18
Clefts, micronutrients: part 2
• Riboflavin and vitamin A: few data
• Homocysteine: increased [hcy] (determined partly by folatestatus) in mothers of infants with CL, CLP, CPO) , ,
• B6: biomarkers of poor vitamin B6 status associated with increased risk of orofacial clefts in the Netherlands and Philippines. Also, B6 deficiency seen in populations with high intakes of polished rice in Asia, and these groups also seem to have high rates of CL, CLP, CPO
• Zinc: deficiency causes CPO in animals In the NetherlandsZinc: deficiency causes CPO in animals. In the Netherlands Children with CL, CLP, CPO and their mothers had lower [Zinc] in erythrocytes. In the Philippines, widespread zinc deficiency ; and high maternal zinc in plasma associated with low risk of orofacialclefts, with a dose‐response relation
WHO 2012 ‐ Global issues in Birth Defect Prevention Botto ‐Mastroiacovo | 35
Congenital heart defects: common, high impact, costly, heterogeneous
Atrial septal defectsVentricular septal defects(several types)
Tetralogy of FallotD-Transposition of the GATruncus arteriosusInterrupted ao arch type B
Hypoplastic left heart s.Aortic stenosisCoarctation of the aortaCoarctation of the aorta
Pulmonary atresia/intact septumPulmonic stenosis
Complex heterotaxy/laterality defects
WHO 2012 ‐ Global issues in Birth Defect Prevention Botto ‐Mastroiacovo | 36

19
Some known risk factors for CHD
Risk CHD types RR Exposure Etiologic factor prevalence
%fraction
%
Diabetes pregest.
most ~4 to 20 3%
6%
8.3
15
Meds various ~4 1 3Meds various 4 1 3
PKU* LVOTO, Conotr.
>6* < 0.01 0.5
* If uncontrolled mat PHE levelsWHO 2012 ‐ Global issues in Birth Defect Prevention Botto ‐Mastroiacovo | 37
Possible risk factors for CHD suggestive but not conclusive (>2 studies, mixed)
Factor CHD types
Relative Risk
Exposure prev., %
Etiologic fract., %
Non use of folic acid, multivitamin
Conotr. Septal
2 30
50
23
33
Fever/flu Septal Tr. Atr.
2 6
8
5.7
7.4
Obesity Various 1.2 20
30
3.8
5.7
Smoking Septal 2 11
15
9.9
13WHO 2012 ‐ Global issues in Birth Defect Prevention Botto ‐Mastroiacovo | 38
20
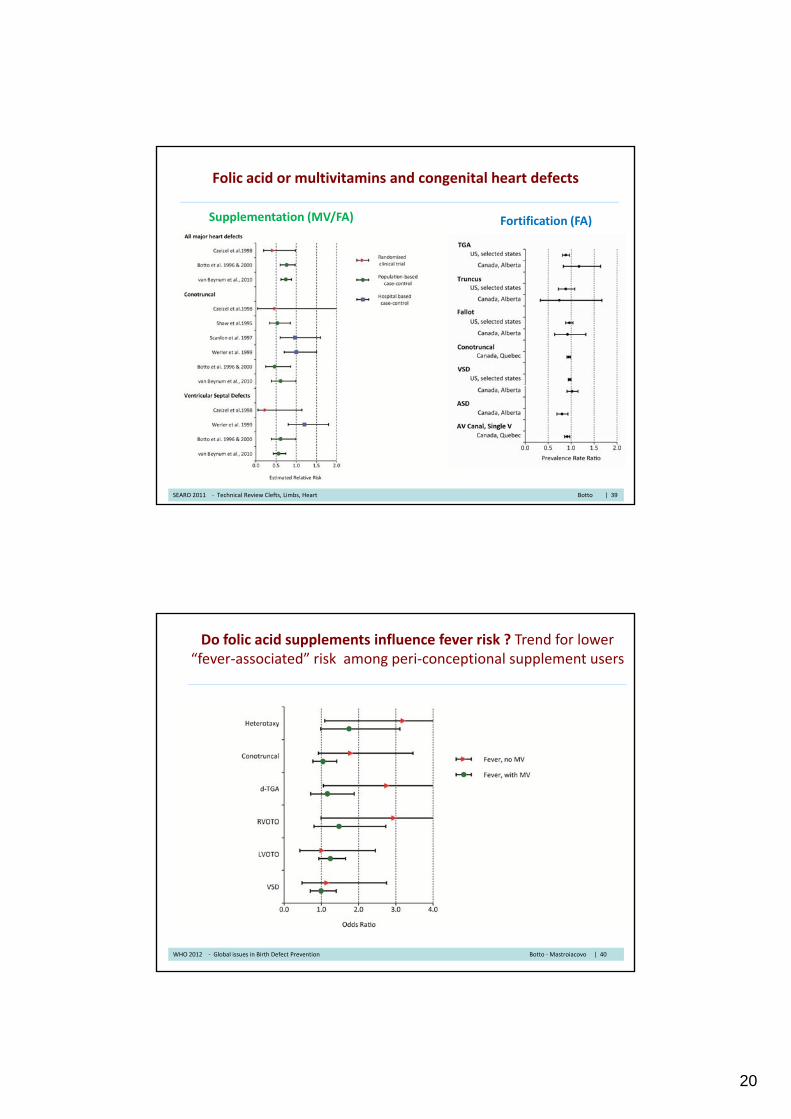
Folic acid or multivitamins and congenital heart defects
Supplementation (MV/FA) Fortification (FA)
SEARO 2011 ‐ Technical Review Clefts, Limbs, Heart Botto | 39
Do folic acid supplements influence fever risk ? Trend for lower “fever‐associated” risk among peri‐conceptional supplement users
WHO 2012 ‐ Global issues in Birth Defect Prevention Botto ‐Mastroiacovo | 40
21
Summary
1. Several known modifiable risk factors:
• folic acid (protective for neural tube defects)
• smoking (oral clefts)• smoking (oral clefts)
• diabetes (many birth defects, including heart defects)
• some medications (valproate‐NTDs; thalidomide ‐limb defects).
2. Evidence for protective effect of folic acid less clear for birth defects other than neural tube defects: clefts > heart defects > limb anomalies
3. Possible reasons ? Study design, classification, genetic factors in different populations, need for higher folic acid dose, need for multivitamin rather than FA alone (‐> implication for fortification)
WHO 2012 ‐ Global issues in Birth Defect Prevention Botto ‐Mastroiacovo | 41
Modifiable risk factors for birth defects: what evidence is helpful?
• Strength of evidence
– Multiple studies, different design, consistent findings
• Magnitude of risk:
– Relative Risk (how many times higher compared to unexposed?), absolute risk (actual chance of birth defect exposed)
– The higher the risk, the higher the number of affected babies
• Frequency of exposure
– How common among women of childbearing age?
– The more common, the more potential cases
• Types of birth defects and associated health outcomes
– The more severe, the more concerning
• Range of outcomes
– Potential for preventing other birth defects, pediatric disorders?
• Effectiveness of interventions
– Potential for high impact (fortification vs. supplementation)
SEARO 2011 ‐ Strategies for Birth Defect Prevention Botto | 42

22
Modifiable risk factors for birth defects: what evidence is helpful?
• Strength of evidence
– Multiple studies, different design, consistent findings
• Magnitude of risk:
– Relative Risk (how many times higher compared to unexposed?), absolute risk (actual chance of birth defect exposed)
– The higher the risk, the higher the number of affected babies
• Frequency of exposure
– How common among women of childbearing age?
– The more common, the more potential cases
• Types of birth defects and associated health outcomes
– The more severe, the more concerning
• Range of outcomes
– Potential for preventing other birth defects, pediatric disorders?
• Effectiveness of interventions
– Potential for high impact (fortification vs. supplementation)
SEARO 2011 ‐ Strategies for Birth Defect Prevention Botto | 43
Folic acid/vitamin supplementation and congenital heart defects
• Relative Risk < 1 = reduced risk• Relative Risk > 1 = increased risk• Confidence interval
• Multiple studies• Different countries• Different study design
SEARO 2011 ‐ Strategies for Birth Defect Prevention Botto | 44

23
Modifiable risk factors for congenital heart defects: multiples studies, consistent findings
Relative Risk (range)Relative Risk (range)
• Maternal conditions
– Diabetes, pregestational 4 to 20
– Phenylketonuria (uncontrolled) > 6
• Medications
– Antiepileptic medications ~4
– Thalidomide very high
– Retinoic acid very high
SEARO 2011 ‐ Strategies for Birth Defect Prevention Botto | 45
Modifiable risk factors for birth defects: what evidence is helpful?
• Strength of evidence
– Multiple studies, different design, consistent findings
• Magnitude of risk:
– Relative Risk (how many times higher compared to unexposed?), absolute risk (actual chance of birth defect exposed)
– The higher the risk, the higher the number of affected babies
• Frequency of exposure
– How common among women of childbearing age?
– The more common, the more potential cases
• Types of birth defects and associated health outcomes
– The more severe, the more concerning
• Range of outcomes
– Potential for preventing other birth defects, pediatric disorders?
• Effectiveness of interventions
– Potential for high impact (fortification vs. supplementation)
SEARO 2011 ‐ Strategies for Birth Defect Prevention Botto | 46
24
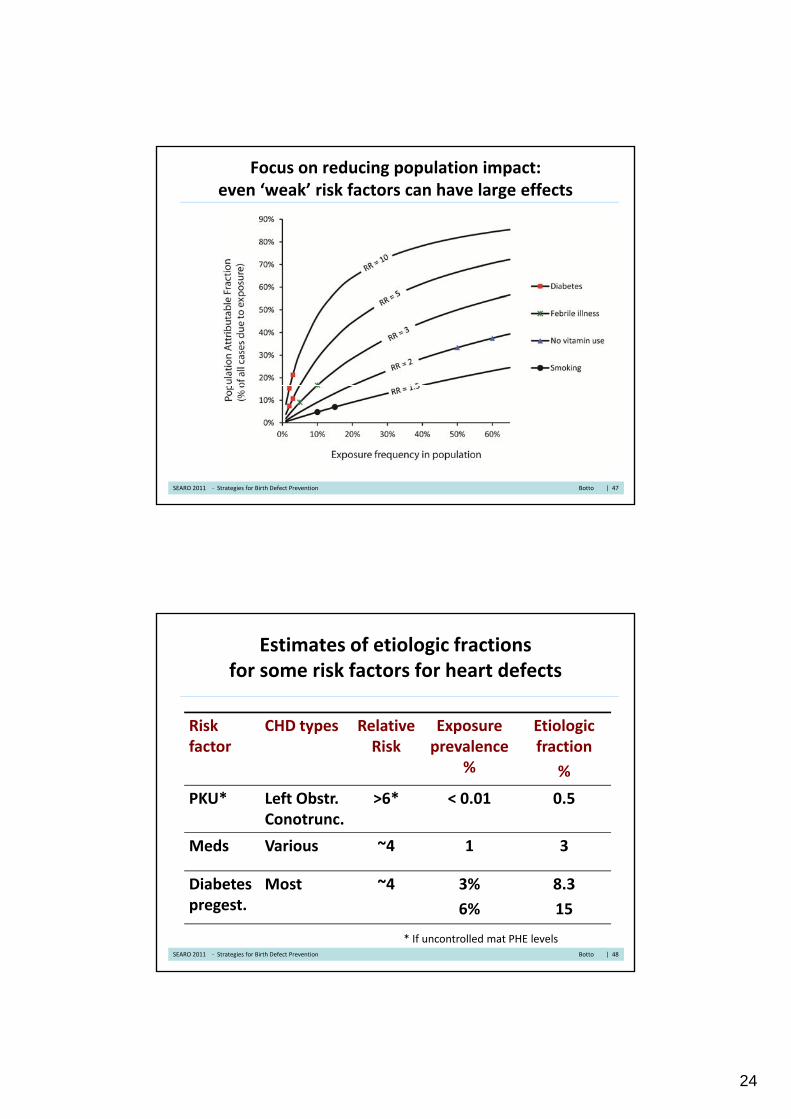
Focus on reducing population impact: even ‘weak’ risk factors can have large effects
SEARO 2011 ‐ Strategies for Birth Defect Prevention Botto | 47
Estimates of etiologic fractions for some risk factors for heart defects
Risk CHD types Relative Exposure Etiologic factor
ypRisk
pprevalence
%
gfraction
%
PKU* Left Obstr. Conotrunc.
>6* < 0.01 0.5
Meds Various ~4 1 3
Diabetes pregest.
Most ~4 3%
6%
8.3
15
* If uncontrolled mat PHE levelsSEARO 2011 ‐ Strategies for Birth Defect Prevention Botto | 48

25
Modifiable risk factors for birth defects: what evidence is helpful?
• Strength of evidence
– Multiple studies, different design, consistent findings
• Magnitude of risk:
– Relative Risk (how many times higher compared to unexposed?), absolute risk (actual chance of birth defect exposed)
– The higher the risk, the higher the number of affected babies
• Frequency of exposure
– How common among women of childbearing age?
– The more common, the more potential cases
• Types of birth defects and associated health outcomes
– The more severe, the more concerning
• Range of outcomes
– Potential for preventing other birth defects, pediatric disorders?
• Effectiveness of interventions
– Potential for high impact (fortification vs. supplementation)
SEARO 2011 ‐ Strategies for Birth Defect Prevention Botto | 49
Multiple risks associated with selected modifiable risk factors
Risk factor Other adverse outcomes Exposure lprevalence %
Diabetes, pregest.
Many birth defects, prematurity, infant deaths
3%
6%
PKU* Mental retardation, microcephaly, heart
< 0.01
defects
Seizure meds
Spina bifida, oral clefts, others
1
SEARO 2011 | 50

26
Risk factor Other adverse outcomes
Exposure prevalence %
Multiple risks associated with selected modifiable risk factors
outcomes prevalence %
Fever Spina bifida, heart def., prematurity
5‐10%
Smoking Clefts, IUGR/low birth weight, etc
10‐15 %
or more
No folic acid use before conception
Spina bifida, anencephaly, probably others (clefts, heart?)
>50% or more
SEARO 2011 ‐ Strategies for Birth Defect Prevention Botto | 51
Approach to primary prevention and health promotion for birth defects
Factor Causes NTDs
Relative
Risk
Common Exposure
Additional Prevention
Non use of folic acid, multivitamin
Definite ++ +++++
(>50%)
Probable
(some clefts, ?CHD)
Diabetes (pregest.) Definite +++ +++
(1‐6%)
Definite
(many birth defects, other)
Select medications Definite ++ + Definite
(NTD, clefts, other)(NTD, clefts, other)
Fever/flu Probable ++ +++
(6‐10%)
Possible
(CHD)
Smoking Possible ++ +++
(10‐20%)
Definite
(clefts, preterm/IUGR)
SEARO 2011 ‐ Strategies for Birth Defect Prevention Botto | 52

27
Modifiers of risk may cluster and interact
• Clustering
– Person: smoking, obesity, diabetes, poor nutrition, SESPerson: smoking, obesity, diabetes, poor nutrition, SES
– Place: occupational exposures, residential proximity to waste sites, contaminated water supply
• Interaction
– Exposures could augment the combined birth defect risk
– Alternatively, one could mitigate the other: fever and multivitamin use?
• Need for a global approach, focused on people
– People (not only exposures), baby (not only heart)
• Effective high‐impact interventions, population‐wide
SEARO 2011 ‐ Strategies for Birth Defect Prevention Botto | 53
Modifiable risk factors for birth defects: what evidence is helpful?
• Strength of evidence
– Multiple studies, different design, consistent findings
• Magnitude of risk:
– Relative Risk (how many times higher compared to unexposed?), absolute risk (actual chance of birth defect exposed)
– The higher the risk, the higher the number of affected babies
• Frequency of exposure
– How common among women of childbearing age?
– The more common, the more potential cases
• Types of birth defects and associated health outcomes
– The more severe, the more concerning
• Range of outcomes
– Potential for preventing other birth defects, pediatric disorders?
• Effectiveness of interventions
– Potential for high impact (fortification vs. supplementation)
SEARO 2011 | 54
28
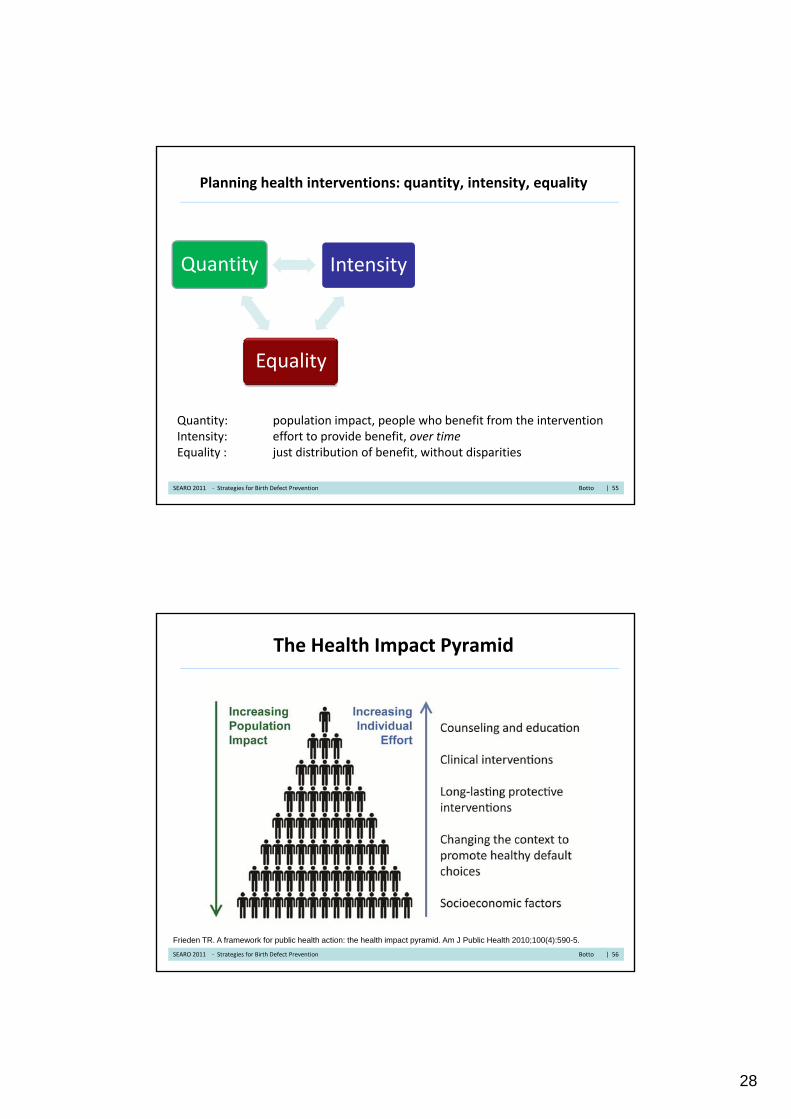
Planning health interventions: quantity, intensity, equality
Quantity IntensityQuantity
Equality
Intensity
Quantity: population impact, people who benefit from the interventionIntensity: effort to provide benefit, over time Equality : just distribution of benefit, without disparities
SEARO 2011 ‐ Strategies for Birth Defect Prevention Botto | 55
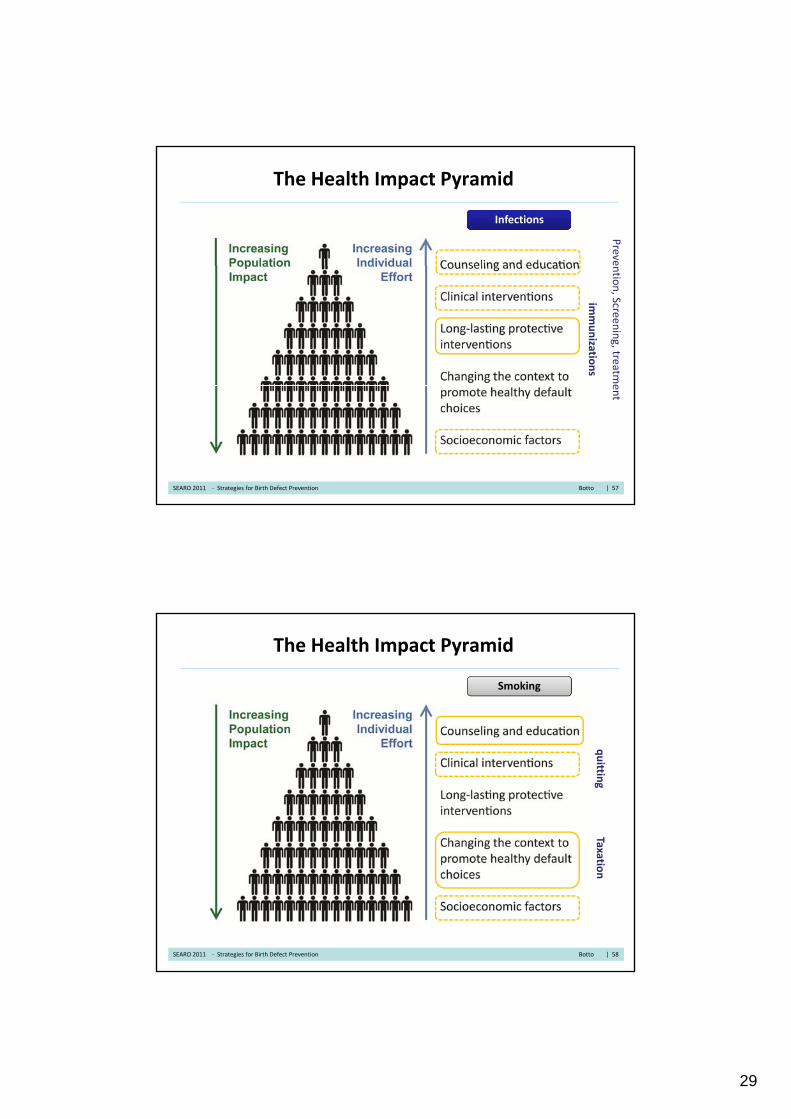
The Health Impact Pyramid
Frieden TR. A framework for public health action: the health impact pyramid. Am J Public Health 2010;100(4):590-5.
SEARO 2011 ‐ Strategies for Birth Defect Prevention Botto | 56
29
The Health Impact Pyramid
InfectionsInfections
Preve
immunizatio
ns
ntio
n, Screen
ing, treatm
eent
SEARO 2011 ‐ Strategies for Birth Defect Prevention Botto | 57
The Health Impact Pyramid
Smoking
Taxquittin
gxatio
n
SEARO 2011 ‐ Strategies for Birth Defect Prevention Botto | 58

30
The Health Impact Pyramid
InfectionsInfections
screen
Immunizatio
ns
ning
School, ccro
wding, h
ygiene
SEARO 2011 ‐ Strategies for Birth Defect Prevention Botto | 59
The Health Impact Pyramid
Diabetes
Food, w
screening
weigh
t, activity
SEARO 2011 ‐ Strategies for Birth Defect Prevention Botto | 60

31
The Health Impact Pyramid
Folic acid
Supple
Fortificatio
ementatio
n
on
SEARO 2011 ‐ Strategies for Birth Defect Prevention Botto | 61
The Health Impact Pyramid: quantity, intensity, equality
Quantity Intensity
Equality
Quantity: people who benefit from the value of the interventionIntensity: effort to provide benefit, over time Equality : just distribution of benefit, without disparities
SEARO 2011 ‐ Strategies for Birth Defect Prevention Botto | 62
32
Key Points
• 65th World Health Assembly Resolution: call to global action for birth defect surveillance, treatment, prevention
• Modifiable risk factors: what can be done now that can work?
• Global opportunities: prevention, training, surveillanceGlobal opportunities: prevention, training, surveillance
WHO 2012 ‐ Global issues in Birth Defect Prevention Botto ‐Mastroiacovo | 63
Global Opportunities: Training Program
• Focuses on prevention and surveillance
– Public health surveillance as a tool for prevention
– Generates baseline, evaluates prevention interventions
– Do interventions work, do they change baselines and trends ?
• Hands‐on, emphasis on small group activities
• 24 trainees, selected from low‐middle income countries
• Collaboration International Clearinghouse, WHO, CDCg , ,
• First course 2011, planning 2012
WHO 2012 ‐ Global issues in Birth Defect Prevention Botto ‐Mastroiacovo | 64

33
Training Program onTraining Program onSurveillance and Prevention
of Birth Defects and Preterm Births
International Clearinghouse for Birth Defects Surveillance and Research (ICBDSR)Centers for Disease Control and Prevention (CDC)
World Health Organization (WHO)
Geneve, Switzerland3 to 6 October 2011
WHO 2012 ‐ Global issues in Birth Defect Prevention Botto ‐Mastroiacovo | 65
Public Health Surveillance: what health events?
S illSurveillance
Risk factors
(folic acid use, folate levels,
etc)
Outcomes
(morbidity, mortality, cost,
disability)
SEARO 2011 | 66
Occurrence
(prevalence of neural tube defects)

34
‐ PoliciesPrevention Surveillance
Enhancing surveillance to include risk factors
‐ Birth defects‐ Preterm births‐ Low birth weight/IUGR‐ Stillbirth‐ Intellectual disability
‐ Folic acid (lack of use)‐ Infections (toxo, rubella, etc)‐Medications (retinoids, VPA)‐ SmokingDiabetes obesity
Policies‐ Interventions
Global burden of risk factors Global burden of disease
1. Three R’s: need for data that are reliable, relevant, recent
2. PAT: Need for Priorities, Approach, Teams optimized to local setting
Intellectual disability‐ …
‐ Diabetes, obesity‐ …
WHO 2012 ‐ Global issues in Birth Defect Prevention Botto ‐Mastroiacovo | 67
Surveillance of Risk Factors: the Awareness ProjectCollaboration of ICBDSR, CDC, WHO, MOD
Risk Factor Status
Diabetes , pregestational Finished
Obesity, high body mass index To be startedy, g y
Folic acid supplement use Updated 2011
Folic acid recommendations, policies Updated 2011
Blood folate status (low) Advanced
Medications (potentially teratogenic) Advanced
Pregnancy unplanned or mis‐timed Started
Smoking StartedSmoking Started
Alcohol To be started
Rubella (seronegativity) Updated 2011
Toxoplasmosis (seronegativity) Updated 2011
Varicella (seronegativity) Finished
WHO 2012 ‐ Global issues in Birth Defect Prevention Botto ‐Mastroiacovo | 68
35
Key Points
• 65th World Health Assembly Resolution: call to global action for birth defect surveillance, treatment, prevention
• Modifiable risk factors: what can be done now that can work?
• Global opportunities: prevention, training, surveillanceGlobal opportunities: prevention, training, surveillance
• DISCUSSION
WHO 2012 ‐ Global issues in Birth Defect Prevention Botto ‐Mastroiacovo | 69