Cohort Study. Objectives To discuss cohort study designs To discuss data from some cohort studies.

Instructions for use
Title Birth Cohort Consortium of Asia : Current and Future Perspectives
Author(s)Kishi, Reiko; Zhang, Jun Jim; Ha, Eun-Hee; Chen, Pau-Chung; Tian, Ying; Xia, Yankai; Tsuchiya, Kenji J.; Nakai,Kunihiko; Kim, Sungkyoon; Hong, Soo-Jong; Hong, Yun-Chul; Lee, Jeong-Rim; Hamid Jan B. Jan Mohamed; Parajuli,Rajendra Prasad; Adair, Linda S.; Chong, Yap Seng; Guo, Yue Leon; Wang, Shu-Li; Nishijo, Muneko; Kido, Teruhiko;Tai, Pham The; Nandasena, Sumal
Citation Epidemiology, 28(Supplement 1), S19-S34https://doi.org/10.1097/EDE.0000000000000698
Issue Date 2017-10
Doc URL http://hdl.handle.net/2115/71564
Rights This is a non-final version of an article published in final form in Epidemiology : Oct-2017, 28(Supplement 1),pp.S19‒S34.
Type article (author version)
Additional Information There are other files related to this item in HUSCAP. Check the above URL.
File Information Epidemiology28_S19.pdf
Hokkaido University Collection of Scholarly and Academic Papers : HUSCAP

Type of manuscript: original article
Birth Cohort Consortium of Asia (BiCCA) - Current and Future Perspectives
Reiko Kishi,a Jun Jim Zhang,b Eun-Hee Ha,c* Pau-Chung Chen,d,e* Ying Tian,b,f Yankai Xia,g
Kenji J Tsuchiya,h Kunihiko Nakai,i Sungkyoon Kim,j Soo-Jong Hong,k Yun-Chul Hong,l
Jeong-Rim Lee,m Hamid Jan B Jan Mohamed,n Rajendra Prasad Parajuli,o Linda S Adair,p
Yap Seng Chong,q Yue Leon Guo,d,e,r Shu-Li Wang,r Muneko Nishijo,s Teruhiko Kido,t Pham
The Tai,u Sumal Nandasena,v
aCenter for Environmental and Health Sciences, Hokkaido University, Sapporo, Japan;
bMOE and Shanghai Key Laboratory of Children's Environmental Health, Xinhua Hospital,
Shanghai Jiao Tong University School of Medicine, Shanghai, China;
cDepartment of Preventive Medicine, Ewha Medical Research Center, Ewha Womans
University, Seoul, South Korea;
dInstitute of Occupational Medicine and Industrial Hygiene, National Taiwan University
College of Public Health, Taipei, Taiwan;
eDepartment of Environmental and Occupational Medicine, National Taiwan University
Hospital and National Taiwan University College of Medicine, Taipei, Taiwan;
fDepartment of Environmental Health, School of Public Health, Shanghai Jiao Tong
University School of Medicine, Shanghai, China;

gState Key Lab of Reproductive Medicine, School of Public Health, Nanjing Medical
University, China;
hHamamatsu University School of Medicine, Research Center for Child Mental Development,
Japan;
iTohoku University Graduate School of Medicine, Japan;
jGraduate School of Public Health, Seoul National University, South Korea;
kDepartment of Pediatrics, Childhood Asthma and Atopy Center, Environmental Health
Center, Asan Medical Center, University of Ulsan College of Medicine, Seoul, South
Korea; lEnvironmental Health Center, Seoul National University, South Korea;
mThe Korean Institute of Child Care and Education (KICCE), South Korea;
nNutrition Program, School of Health Sciences, Universiti Sains Malaysia,
Malaysia; oUniversity of Tokyo, Dept of Human Ecology, Japan;
pCarolina Population Center, University of North Carolina at Chapel Hill, USA;
qDepartment of Obstetrics & Gynaecology, Yong Loo Lin School of Medicine, National
University of Singapore, Singapore;
rNational Institute of Environmental Health Sciences, National Health Research Institutes,
Taiwan;
sDepartment of epidemiology and public health, Kanazawa Medical University, Uchinada,
Ishikawa, Japan;

tInstitute of Medical, Pharmaceutical and Health Sciences, Faculty of Health Sciences,
Kanazawa University, Kanazawa, Japan;
uBiomedical and pharmaceutical research center, Vietnam Military Medical University, Ha
Noi, Vietnam;
vNational Institute of Health Sciences, Kalutara, Sri Lanka;
*Co-corresponding.
Corresponding author:
Eun-Hee Ha MD PhD
Professor
Department of Preventive Medicine
Ewha Womans University College of Medicine
911-1, Mok-6 dong, Yangcheonku, Seoul, 158-056, Korea
Phone: +82-2-2650-5757
Fax: +82-2-2653-1086
E-mail: [email protected]
Pau-Chung Chen MD PhD
Professor and Director
Institute of Occupational Medicine and Industrial Hygiene
National Taiwan University College of Public Health
17 Xuzhou Road, Taipei 10055, Taiwan
Phone: +886-(0)2-3366 8088

Fax: +886-(0)2-3366 8734
Email: [email protected]
Running Title: Birth cohort studies in Asia
Key Words: birth cohort, children’s environmental health, birth cohort consortium of Asia
(BiCCA)
Conflicts of Interest and Source of Funding: The authors have declared that no competing
interests exist. The PI meetings of this consortium were supported financially by grants from
National Science Council (NSC-101-2911-I-002-009) and National Taiwan University
Hospital (NTUH-103-A123, NTUH-104-A123), Taiwan.
Acknowledgments: We thank BiCCA secretariat Dr. Mei Huei Chen to organize the tables
and content of this manuscript. We also thank all cohort researchers and staffs who have
helped with the completion of the inventories.

ABSTRACT
Background: The environmental health of children is one of the great global health
concerns. What a developing child is exposed to in utero and in his/her early years has
major consequences on later health. However, environmental risks or disease burdens
vary from region to region. Birth cohort studies are ideal for investigating different
environmental risks.
Methods: The principal investigators of three birth cohorts in Asia including the
Taiwan Birth Panel Study (TBPS), the Mothers and Children's Environmental Health
Study (MOCEH), and the Hokkaido Study on Environment and Children' Health
(Hokkaido Study) co-established the Birth Cohort Consortium of Asia (BiCCA) in
2011. Through a series of five PI meetings, the enrolment criteria, aim of the
consortium, and a first-phase inventory were confirmed.
Results: To date, 23 birth cohorts have been established in 10 Asian countries,
consisting of approximately 70,000 study subjects in the BiCCA. This article provides
the study framework, environmental exposure and health outcome assessments, as
well as maternal and infant characteristics of the participating cohorts.
Conclusions: The BiCCA provide a unique and reliable source of birth cohort
information in Asian countries. Further scientific cooperation is ongoing to identify
specific regional environmental threats and improve the health of children in Asia.

1
INTRODUCTION
Asia contains half of the world's children, and the countries of Asia are the most
rapidly industrializing nations in the world. Environmental threats to the health of
children are diverse in Asia and include classic infectious disease hazards (i.e.,
pneumonia, dysentery, measles, Acquired Immune Deficiency Syndrome, and tu-
berculosis). Additionally, the prevalence of environmentally related diseases such as
allergic disease, attention deficit hyperactivity disorder (ADHD), and autism is in-
creasing dramatically.1,2 As industrial development proceeds and as nations in the
region pass through the epidemiologic transition, rapid urbanization, unsustainable
consumption, and an increase of industrial disposal such as e-waste, children are
confronted by a rapidly multiplying array of new health threats posed by exposures
to toxic chemicals.1
To address these problems, local and national research efforts must focus on envi-
ronmental risks. In 2002, the International Conference on Environmental Threats to
the Health of Children was held in Bangkok to initiate the very first step towards
awareness about the environmental health hazards affecting children in these regions.
Several actions have been proposed to decrease environmental hazards, including
removal of lead from gasoline, the India clean-water project, the mercury pollution

2
reduction project, international networking and anti-smoking campaigns.3 Neverthe-
less, new challenges continue to emerge. In 2008, hundreds of thousands of infants
and young children suffered from renal dysfunction after exposure to Melamine that
was deliberately added to milk and milk-containing products in China, Hong Kong
and Taiwan.4,5 Later in 2011, plasticizers such as di(2-ethylhexyl) phthalate (DEHP)
and di-iso-nonyl phthalate (DiNP) were found to be illegally added to clouding
agents used in foods and beverages in Taiwan.6 These issues draw new attention to
the importance of food safety. Another trans-boundary threat in the Asia-Pacific re-
gion is outdoor air pollution. Smog and sandstorm in China and Southeast Asia haze
are not regional threats. Even more, we are facing the challenge of climate change
and extreme weather globally. This issue has become the prominent target of policy
reforms and public health efforts.
In response to these new threats, national governments in Asia have taken action
since the 1970s to protect children against environmental threats to health, and in the
past decade, they have developed new approaches to evaluating and managing toxic
chemicals. In 2009, the Ministry of Environment in Korea held the Third Interna-
tional Conference for Children's Health and Environment in Busan, Korea in part-
nership with the World Health Organization.7 In July 2010, in Jeju, Korea, the Gov-

3
ernment of Korea hosted the Second Ministerial Regional Forum on Environment
and Health in South-East and East Asian Countries, which was jointly organized by
the United Nations Environment Program Regional Office for Asia and the Pacific
and the World Health Organization Regional offices for the Western Pacific and
South-East Asia.8 Some associated conferences have further pledged to advocate for
the recognition, assessment and consideration of hazardous environmental influ-
ences on children’s health and development.
Children’s environmental health is an issue of both global and regional importance.
Environmental hazards, lifestyle and genetic susceptibility vary across different re-
gions and races. Thus, a single one cohort or study is unable to explore the whole
picture of this issue. Population size is even the threshold of study investigating
gene- environmental interactions or co-exposure effects. In addition, replication or
validation is crucial for interpretation of results from omic technologies such as
epigenomics and metabolomics. Harmonization of cohort studies has been successes
by ENRIECO (Environmental Health Risks in European Birth Cohorts) 9 and pro-
jects in Europe 10, but not elsewhere. A useful network to exchange information will
facilitate international cooperation for exploring regional and global hazards, under-
standing the health impact of environmental toxicants, and developing effective

4
prevention strategies not only in Asia but also across the world.

5
METHODS
Establishment of the Birth Cohort Consortium of Asia (BiCCA)
The Birth Cohort Consortium of Asia was co-established in 2011 by the principal in-
vestigators (PIs) of the following three birth cohorts in Asia: the Taiwan Birth Panel
Study (TBPS) from Taiwan (PI: Chen), the Mothers and Children's Environmental
Health Study (MOCEH) from Korea (PI: Ha), and the Hokkaido Study on Environ-
ment and Children' Health (Hokkaido Study) from Japan (PI: Kishi). The two main
objectives of BiCCA are 1. to facilitate the exchange of knowledge and collaboration
between cohorts and researchers, and 2. to explore the future need for children’s en-
vironmental health research. The agenda of the BiCCA was first introduced at the
PPTOXIII (Prenatal Programming and Toxicity III) held on May 14-15, 2012 in Paris,
France. Later on, several symposia/seminar, workshop and PI meetings were held to
increase the knowledge about the Asian birth cohorts and to build capacity related to
conducting exposure measurements, and the latest techniques such as genetics and
epigenetics analysis. These activities also determine the criteria to join BiCCA, com-
plete the 1st phase inventory, prepare the introduction paper and plan for future direc-
tion of collaboration. The details are listed as eTable 1.
Definition and identification of Asian birth cohorts

6
Birth cohort studies were included in the project if they 1) were conducted in Asia; 2)
collected information about both prenatal and postnatal exposures; 3) aimed to in-
vestigate environmental and health issues in children; and 4) enrolled more than 200
participants. The last criteria is a guideline but not an absolute exclusion criteria.
Eligible cohorts were identified through a variety of sources, as follows: searchable
websites, publications and personal contacts.
1st phase inventory
An inventory questionnaire was designed to collect detailed information from the
various cohorts about their study design, biological sample collection, measurement
of environmental exposure, and assessment of child health outcomes. The full ques-
tionnaire is listed as Online Supplemental Material. The questionnaire was divided
into the following 3 sections:
1) Basic information: name of the birth cohort, information about the PI and con-
tact person
2) Basic description: main aim, number of children/mother/father recruited, date
and criteria of enrolment, and planned age of children at the end of the fol-
low-up.
3) Questionnaire or registry date and biological samples: birth outcomes of the

7
children, the children’s exposure, the children’s growth and development, social
factors, diet and nutrition, children’s biological samples and outcome assess-
ments; maternal characteristics, maternal exposure and biological samples; en-
vironmental exposure measurement including air pollution, phenol, heavy metals,
pesticide, nutrients, persistent organic pollutants, plasticizers, flame retardants,
tobacco smoke; genetic and epigenetic factors; outcome assessments including
birth outcomes, malformation, allergic diseases, behaviours, neurodevelopment,
sex differentiation and reproductive function.

8
RESULTS
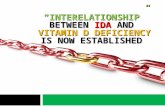
The BiCCA includes 23 birth cohorts, totalling approximately 70,000 study subjects,
that were conducted in 10 Asian countries (Figure 1), including three in China, four
in Japan, five in Korea, one in Malaysia, one in Nepal, one in the Philippines, one in
Singapore, one in Sri Lanka, three in Taiwan and three in Vietnam. Table 1 lists the
full name of birth cohorts as well as the enrolment period and the numbers of par-
ticipants.11-24 The CLHNS is the oldest cohort that began in 1983, while the Nanjing
Medical University Birth Cohort (NJMUBC) and the Kalutara Children’s Health
Study (KCHS) are the newest two, beginning in 2014. The majority of the cohorts
enrolled at least 200 participants, with the current largest cohort (Hokkaido Study)
having 20,818 participants. Two exceptions were the Universiti Sains Malaysia
Pregnancy Cohort Study (USM Pregnancy Cohort), which had enrolled 159 children
and 188 mothers, and the Nepali Birth Cohort Study in Chitwan Valley (Nepali)
from Nepal with 100 participants.
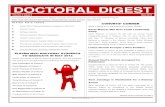
Figure 2 shows the different time points of enrolment and follow-up in the birth co-
horts collaborating in the BiCCA. The predefined periods included pre-pregnancy,
three trimesters of pregnancy, and newborn to the adolescent stage of participating
children. Most of the cohorts recruited mothers during pregnancy (n=15) or before

9
pregnancy (n=2), and the remaining began at birth. Participating children were fol-
lowed or were planned to be followed at least two points before the age of 2 years
and then once every 2 to 5 years until puberty. The time points already performed
and those planned are marked with different symbols. At our reference date (March
2015), children in the 10 cohorts were between 5 to 10 years of age, children in 6
cohorts were older than 10 years, and in seven cohorts, they were younger than 5
years of age (Figure 2).
Biological samples were collected in all cohorts with two exception [Panel Study on
Korean Children (PSKC) and KCHS] from mothers and children, covering the pre-
natal and postnatal periods with various types of tissues including amniotic fluid,
blood, breast milk, cord blood, deoxyribonucleic acid (DNA), hair, meconium, pla-
centa, stool, nail, urine and umbilical cord collected (Table 2). The NJMUBC, SBC
and The COhort for Childhood Origin of Asthma and allergic diseases (COCOA)
collected blood and DNA from biological fathers. Urine and semen were collected
additionally by the former two cohorts.
Heavy metals were the most commonly measured environmental exposure, but some
cohorts (especially those conducted in Japan and Korea) only focused on mercury,

10
cadmium or lead. About half of the participating cohorts collected information about
tobacco smoking by measuring biomarkers. COCOA, MOCEH and KCHS meas-
ured information about both indoor and outdoor air pollution. The Hokkaido Study
from Japan collected indoor dust to measure mite allergens and phthalate, among
others. The KCHS focused mainly on exposure to PM2.5 and Black carbon. Around
half of the cohorts measured emerging environmental pollutants, such as persistent
organic pollutants (dioxin and related compounds, polyfluoroalkyl substances or
brominated flame retardants), bisphenol A and phthalate. The cohorts in Vietnam
focused mainly on dioxin exposure (Table 3).
All of the studies had information about birth outcomes, including birth weight and
gestational age, and most of them collected the body weight and height of children
at a later follow-up visit. The GUSTO from Singapore performed comprehensive
measurements of body composition of children including skinfolds and magnetic
resonance imaging (MRI). Congenital malformations were recorded in about half of
participating cohorts. Twelve studies assessed allergic diseases using The Interna-
tional Study of Asthma and Allergies in Childhood questionnaires (ISAAC). Neuro-
development and behaviour problems were the most important outcomes for most of
the studies, but the studies used a diverse set of measurement tools. Most studies

11
measured endocrine function and puberty status (or plan to do so in the future) (Ta-
ble 4).
Maternal characteristics are shown in Table 5-1 and 5-2. The average maternal age
and standard deviation among the cohorts ranged from 22.9 ± 3.7 (Nepali) to 33.5 ±
4.1 years (Children’s Health and Environmental Chemicals in Korea, CHECK). The
maternal pre-pregnancy BMI did not demonstrate large variations, ranging from
20.7 ± 2.6 (COCOA) to 23.7 ± 4.8 kg/m2 (GUSTO). Comparisons of maternal edu-
cational levels among participants of the different cohorts are a little complex, as
shown in Table 5-1 based on the education system of each country. The CLHNS had
the highest percentages of multipara (76.9%), and the Laizhou Wan Birth Cohort
(LWBC) in China had the highest percentage of primipara (67.3%) among cohorts
(Table 5-2). The mothers in the Sapporo birth cohort (Japan) had the highest per-
centage of smokers (20.3%) and alcohol drinkers (30.9%) during pregnancy (Table
5-2).
The infants’ gender ratio was diverse among the cohorts (Table 6); the percentage of
males ranged between 45.1% (USM Pregnancy Cohort) and 57.4% (DaNang Dioxin
Cohort Study, DaNang study). Although the average gestational ages were almost

12
the same, but the range of birth weights among the infants was wide; the infants’
birth weight in the KCHS (2940 ± 567 g) was the lowest, and LWBC (3419 ± 500 g)
had the highest infant birth weights among the cohorts. This variation may be due to
differences in the recruitment and source of populations among the cohorts. The
CLHNS study had the highest percentage of infants with preterm birth (15.6%), and
low birth weight (14.1%).
DISCUSSION
The BiCCA enrolled cohorts established in Asia that were diverse in terms of indus-
trialization and urbanization. The regional and/or global differences need to be dis-
covered through an integrated platform; for example, we are able to explore the dif-
ferences in cohort findings not only between developed versus developing Asian
countries but also with European or North America cohorts. Information including
standardized or state-of-art analytic methods, cohort design, assessments of health
outcome can be smoothly exchanged. In addition, the experiences shared between
studies or countries will help to promote environmental child health through health
policy-making or strategy implementation. Furthermore, the knowledge derived
from the BiCCA should note the future need for research of new emerging environ-
mental threats or public health priorities that contribute towards organizing the next

13
generation of birth cohorts.
The theory “Developmental Origins of Health and Disease, DOHaD” illustrated that
exogenous maternal malnutrition or environmental factors during pregnancy cause a
lifelong, persisting adaptation of the foetus resulting in low birth weight, in-
creased cardiovascular risk, and non-insulin dependent diabetes as adults.25 However,
the science underlying the impact of environmental factors on children’s health
(from the stage of the foetus to the age of 18) is more complex. While most of the
cohort studies in the BiCCA focused on environmental pollutants, CLHNS, GUSTO,
USM Pregnancy Cohort and Nepali were designed to investigate the role of nutrients.
Integration of participating cohorts in BiCCA with different study focus such as nu-
trition, social economic factors and environmental toxicants are promising to testify
the DOHaD hypothesis and related mechanism.
From the aspect of the exposure assessment, many East Asian countries have some
unique features compared with European countries and the USA. For example, the
Perfluoroalkyl substances (PFASs) are persistent organic pollutants that are detected
in humans worldwide. Their concentrations in plasma in Japan and Korea are quite a
lot lower than in western countries, and the temporal trends of PFAS levels indicate

14
that PFOS (perfluorooctyl sulfonate) and PFOA (perfluorooctanoic acid) concentra-
tions are decreasing every year due to the restriction of PFOS by the Stockholm
convention on POPs in 2009. However, the levels of long-chain PFASs (i.e., PFNA,
PFUnDA, and PFTrDA) seem to be increasing in Japan and Korea because they are
manufactured primarily in Japan via oxidating a mixture of linear fluorotelomer ole-
fins, and prenatal exposure to these compounds may have adverse health out-
comes.26, 27 In Taiwan, the concentrations of PFOS and PFOA in rivers near semi-
conductor and electronics industries are higher than in other countries, and industrial
wastewater treatment plants are a source of contamination.28 Therefore, the related
environmental hazards of PFASs could be an issue among countries with flourishing
high-tech or electronics industries. In contrast, the use of polybrominated diphenyl
ethers (PBDEs) in Japan diminished in the early 1990s following the recommenda-
tions of the Japanese Flame Retardants Conference for voluntary controls, and
phosphate esters (PFRs) have been the most frequently used organic flame retardants.
In 2003, the EU banned the use of PBDEs, and only a few epidemiological studies
on the alternatives to PBDEs have been reported. Therefore, Asian cohort studies
provide information about PFRs in indoor environments and their relationship to
asthma and allergies in children.29 The use of other alternative flame retardants, e.g.,
non-brominated flame retardants, is increasing and warrants further studies as well.

15
Different eating habit or culture may result in diverse chemical exposures or health
impact. For example, the benefits of essential fatty acid and toxicity of chemical
pollutants, such as mercury and dioxin related compounds, are always the scientific
basis of fish consumption advisories. Maternal plasma fatty acid concentrations
were significantly correlated with PFOS concentrations and may affected birth
weight of female offsprings.30 Associations between prenatal methylmercury expo-
sure and cognitive deficits were reported in a Faroe Islands cohort, but few were
found by the Seychelles Islands’ study. Evidence of negative confounding by prena-
tal docosahexaenoic acid (DHA) which partially obscured the association of prenatal
mercury with lower Intelligence quotient had reported. 31 Meanwhile, the adverse
health impacts of mercury were only observed among those children carrying the
susceptible APOE (Apolipoprotein E) genotype in TBPS.32 Genetic variation be-
tween races or ethnicities could further impose a diverse susceptibility to environ-
mental pollutants. In addition, canned food is common in Western countries whereas
hot food in plastic containers is common in Asia. Whether these habits increase the
exposure risk to certain endocrine disrupters such as bisphenol A or phthalate or not
is another question to be solved. The complex interaction between diet or nutrients,
co-exposure to environmental pollutants and genetic polymorphisms are crucial is-

16
sues in children’s health.
Climate change and extreme weather are potential environmental threats. Season
and weather especially cold ambient temperature have been identified as potential
risk factors for lower birth weight and preterm birth.33, 34 Nevertheless, null associa-
tion had been reported.35 Meanwhile, evidence is growing that climate change has
affect human health including mortality from extreme weather events, changes in
quality of air and water and changes in the ecology of infectious disease. Humidity
and temperature may change the composition of ambient air pollution and further
cause diverse toxic effects. The survival and spread of infectious pathogens are
highly correlated with weather. For example, the Aedes species mosquito carrying
Zika virus is distributed in tropical and subtropical regions that Taiwan and the
southern Chinese island province of Hainan could be at greater risk of locally trans-
mitted cases. However, the effect of global warming is unclear. Climate change is a
global issue and its related knowledge should be uncovered through international
cooperation.
The BiCCA consortium intends to expand beyond Asia and provide collaborations
among cohorts. One of the major challenges is the comparison of existing data

17
among the studies and harmonization of the exposure assessment and children’s
health outcome. Definition of basic demographic variables and questionnaires
should be harmonized. The potential bias of environmental exposure measurements
derived from various analytic methods or specimen could be verified by inter- and
intra- laboratory tests. Homogeneity of country or language specific assessment
tools needs to be identified. In addition, two different approach including pooled
analysis and meta-analysis will be applied. 36 Reviewing existing data will provide a
potential or direction for future collaborative analyses. Furthermore, evaluating new
methods and technologies for future studies will be enhanced by aggregation of data
from each cohort. After overcoming these challenges, combining and harmonizing
cohort data in this consortium will help to improve statistical power, reduce publica-
tion bias, and assess the exposure-outcome relationship in emerging concerns of
child health, even for relatively rare health outcomes. Further contribution will be
made for researches of co-exposure effects, gene-environmental interaction and rep-
lication and validation in omic studies through transnational and interracial coopera-
tion.
The BiCCA especially welcomes birth cohorts in Asia to collect epidemiological
data across different Asian countries. The BiCCA provides detailed information

18
about the Asian birth cohorts and facilitates access to information regarding existing
Asian cohort studies. Any group can contact us for further information or consider
potential collaboration from all around the world. Enquiries and initial approaches
regarding membership or detailed information are welcome. Please contact us
at [email protected]; decisions will be made by the Executive Committee Profes-
sors Reiko Kish, Jun Jim Zhang, Eun-Hee Ha and Pau-Chung Chen. More infor-
mation is available in our website (http://www.bicca.org/).

19
REFERENCES
1. Philip j Landrigan and Ruth A Etzel. Text book of children’s environmental health.
Oxford University Press, 2014.
2. Grandjean P and Landrigan PJ. Neurobehaviorual effects of developmental tox-
icity. Lancet Neurol. 2014;13:330-338.
3. Suk WA, Ruchirawat KM, Balakrishnan K, et al. Environmental threats to chil-
dren’s health in southeast Asia and the western pacific. Environ Health Perspect.
2003;111:1340-1347.
4. Gossner CM, Schlundt J, Ben Embarek P, et al. The melamine incident: implica-
tions for international food and feed safety. Environ Health Perspect.
2009;117:1803-1808.
5. Wang IJ, Chen PC, Hwang KC. Melamine and nephrolithiasis in children in Tai-
wan. N Engl J Med. 2009; 360:1157-1158.
6. Yang J, Hauser R, Goldman RH. Taiwan food scandal: the illegal use of
phthalates as a clouding agent and their contribution to maternal exposure. Food
Chem Toxicol. 2013;58:362-368.
7. World Health Organization. The Busan Pledge for Action on Children's Environ-
mental Health. Database: http://www.who.int/ifcs/meetings/3ceh_pledge.pdf
Accessed July 27, 2013.

20
8. Jeju Declaration on Environment and Health, Second Ministerial Regional Ferum
on Environment and Health in South-East and East Asian Countries, Jeju, Korea,
2010. Database:
http://www.environment-health.asia/rfeh/policy_documents/4_jeju_declaration.pd
f Accessed Feb 08, 2014.
9. Gehring U, Casas M, Brunekreef B, et al. Environmental exposure assessment in
European birth cohorts: results from the ENRIECO project. Environ Health.
2013;23:8.
10. Bousquet J, Anto J, Sunyer J, et al. Pooling birth cohorts in allergy and asthma:
European Union-funded initiatives- a MeDALL, CHICOS, ENRIECO and
GA2LEN joint paper. Int Arch Allergy Immunol. 2013;16:1-10.
11. Tsuchiya KJ, Matsumoto K, Suda S, et al. Searching for very early precursors
of autism spectrum disorders: the Hamamatsu Birth Cohort for Mother and Chil-
dren (HBC). J Dev Orig Health Dis. 2010;1:158-173.
12. Kishi R, Sasaki S, Yoshioka E, et al. Cohort profile: the Hokkaido Study on en-
vironment and children’s health in Japan. Int J Epidemiol. 2011;40:611-618.
13. Kishi R, Kobayashi S, Ikeno T, et al. Ten years of progress in the Hokkaido
birth cohort study on environment and children’s health: cohort profile—updated
2013. Environ Health Prev Med. 2013:18:429-450.

21
14. Nakai K, Suzuki K, Oka T, et al. The Tohoku study of perinatal exposures to
methylmercury and environmentally persistent organic pollutants on neurobehav-
ioral development in Japanese children. Tohoku J Exp Med. 2004;202:227-237.
15. Yang HJ, Lee SY, Suh DI, et al. The Cohort for Childhood Origin of Asthma
and allergic diseases (COCOA) study: design, rationale and methods. BMC Pulm
Med. 2014;14:109.
16. Kim BM, Ha M, Park HS, et al. The Mothers and Children’s Environmental
Health (MOCEH) study. Eur J Epidemiol. 2009;24:573-583.
17. Loy SL and Hamid Jan JM. The Universiti Sains Malaysia Pregnancy Cohort
Study: maternal-infant adiposity development until the first year of life. Health
and the Environment Journal. 2014;5:50-64.
18. Parajuli RP, Fujiwara T, Umezaki M, Furusawa H, Ser PH, Watanabe C. Cord
blood levels of toxic and essential trace elements and their determinants in the
Terai region of Nepal: a birth cohort study. Biol Trace Elem Res. 2012;147:75-83.
19. Adair LS, Popkin BM, Akin JS, Guilkey DK, Gultiano S, Borja J. Cohort pro-
file: the Cebu longitudinal health and nutrition survey. Int J Epidemiol.
2011;40:619-625.
20. Soh SE, Tint MT, Gluckman PD, et al. Cohort profile: Growing Up in Singa-
pore Towards health Outcomes (GUSTO) birth cohort study. Int J Epidemiol.

22
2014;43:1401-1409.
21. Hsieh CJ, Hsieh WS, Su YN, et al. The Taiwan Birth Panel Study: a prospective
cohort study for environmentally-related child health. BMC Res Notes.
2011;4:291.
22. Wen HJ, Wang YJ, Lin YC, et al. Prediction of atopic dermatitis in 2-yr-old
children by cord blood IgE, genetic polymorphisms in cytokine genes and mater-
nal mentality during pregnancy. Pediatr Allergy Immunol. 2011;22:695-703.
23. Wang Y, Rogan WJ, Chen PC, et al. Association between maternal serum per-
fluoroalkyl substances during pregnancy and maternal and cord thyroid hormone:
Taiwan maternal and infant cohort study. Environ Health Perspect.
2014;133:529-534.
24. Nishijo M, Tai PT, Nakagwa H, et al. Impact of perinatal dioxin exposure on
infant growth: a cross-sectional and longitudinal studies in dioxin-contaminated
area in Vietnam. PLoS One. 2012;7:e40273.
25. Schug TT, Barouki R, Gluckman PD, Grandjean P, Hanson M, Heindel JJ.
PPTOX III: environmental stressors in the developmental origins of disease- evi-
dence and mechanisms. Toxicol Sci. 2013;131:343-350.
26. Harada KH, Hitomi T, Niisoe T, et al. Odd-numbered perfluorocarboxylates
predominate over perfluorooctanoic acid in serum samples from Japan, Korea and

23
Vietnam. Environ Int. 2011;37:1183-1189.
27. Okada E, Kashino I, Matsuura H, et al. Temproral trends of perfluoroalkyl ac-
ids in plasa samples of pregnant women in Hokkaido, Japan, 2003-2011. Environ
Int. 2013;60:89-96.
28. Lin AY, Panchangam SC, Ciou PS. High levels of perfluorochemicals in Tai-
wan’s wastewater treatment plants and downstream rivers pose great risk to local
aquatic ecosystems. Chemosphere. 2010;80:1167-1174.
29. Araki A, Saito I, Kanazawa A, et al. Phosphorus flame retardants in indoor dust
and their relation to asthma and allergies of inhabitants. Indoor Air. 2014;24:3-15.
30. Kishi R, Nakajima T, Goudarzi H, et al. The Association of Prenatal Exposure
to Perfluorinated Chemicals with Maternal Essential and Long-Chain Polyun-
saturated Fatty Acids during Pregnancy and the Birth Weight of their Offspring:
The Hokkaido Study. Environ Health Perspect. 2015;123:1038-1045.
31. Jacobson JL, Muckle G, Ayotte P, Dewailly E, Jacobson SW. Relation of pre-
natal methylmercury exposure from environmental sources to childhood IQ. En-
viron Health Perspect. 2015;123:827-833.
32. Ng S, Lin CC, Jeng SF, Hwang YH, Hsieh WS, Chen PC. Mercury, APOE, and
children’s neurodevelopment. Neurotoxicology. 2013;37:85-92.
33. Strand LB, Barnett AG, Tong S. The influence of season and ambient tempera-

24
ture on birth outcomes: a review of the epidemiological literature. Environ Res
2011;113:451-462.
34. Bruckner TA, Modin B, Vagero D. Cold ambient temperature in utero and birth
outcomes in Uppsala, Sweden, 1915-1929. Ann Epidemiol 2014;24:116-121.
35. Wolf J, Armstrong B. The association of season and temperature with adverse
pregnancy outcome in two German states, a time-series analysis. PLoS One
2012;7:e40228.
36. Hohmann C, Govarts E, Bergstrom A, Cordier S, Eggesbo M, Guxens M. Joint
data analyses of European birth cohorts: two different approaches. WebmedCen-
tral Epidemiology. 2012;3:WMC00386.

25
FIGURE LEGENDS
Figure 1. Asian birth cohort studies collaborating in BiCCA.

26
Figure 2. Start of enrollment and time points of follow up participating studies in
BiCCA. See Table 1 for full names and locations of cohorts.

Fig. 1

Fig. 2

Table 1. General description of participating studies in Birth Cohort Consortium of Asia
Country Birth cohort Full name and key reference Regions covered Source Enrollment period
No. of children at birth
No. of mother enrolled
CHINA LWBC Laizhou Wan Birth Cohort
South coast area of Laizhou Wan of Bohai Sea, Shandong province, China
Hospital based 2010-2013 773 773
NJMUBC
Nanjing Medical University Birth Cohort
Nanjing, Suzhou, Wuxi, Huai'an, Changzhou
Hospital & Community based
2014-2016 26,000* 30,000*
SBC Shanghai Birth Cohort Shanghai Hospital based 2013-2015 3,000 4,000
JAPAN HBC Study Hamamatsu Birth Cohort for Mothers and Children11
Hamamatsu Hospital & Community based
2007-2011 1,258 1,138
Hokkaido
Hokkaido cohort: Hokkaido Study on Environment and Children's Health12,13
Hokkaido Hospital & Community based
2003-2013 20,818 20,929
Sapporo
Sapporo cohort: Hokkaido Study on Environment and Children's Health12,13
Sapporo Hospital based 2002-2005 504 514
TSCD
The Tohoku Study of Child Development14
Sendai Hospital based 2001-2006 1,348 1,323

Country Birth cohort Full name and key reference Regions covered Source Enrollment period
No. of children at birth
No. of mother enrolled
KOREA CHECK Children’s Health and Environmental Chemicals in Korea
South Korea University hospital based
2011-2013 352 352
COCOA
COhort for Childhood Origin of Asthma and allergic diseases15
Korea Hospital & Community based
2007-2016 2,400 2,400
EDC study
Environment and Development of Children Study
Seoul Community based 2008-2014 698 698
MOCEH
The Mothers and Children’s Environmental Health study16
Seoul, Ulsan and Cheonan
Hospital & Community based
2006-2010 1,751 1,751
PSKC Panel Study on Korean Children Korea Hospital based 2008 2,150 2,150
MALAYSIA USM Pregnancy Cohort
Universiti Sains Malaysia Pregnancy Cohort Study17
Kubang Kerian Hospital based 2010-2011 159 188
NEPAL Nepali Nepali Birth Cohort Study in Chitwan Valley18
Chitwan Hospital & Community based
2008Sep-Oct 100 100
PHILIPPINES CLHNS Cebu Longitudinal Health and Nutrition Survey19
Metro Cebu, Philippines
Community based 1983-1984 3,080 3,327
SINGAPORE GUSTO Growing Up in Singapore Towards healthy Outcomes20
Singapore Hospital based 2009-2010 1,190 1,247

Country Birth cohort Full name and key reference Regions covered Source Enrollment period
No. of children at birth
No. of mother enrolled
SRI LANKA KCHS Kalutara Children’s Health Study Kalutara, Sri Lanka Community based 2014-2015 450 450
TAIWAN TBPS Taiwan Birth Panel Study21 Taipei and New Taipei Hospital based & Community based
2004-2005 486 486
TEC Taiwan Early-Life Cohort22
Hsinjuang, Jiayi, Yulin, Tainan, Kaohsiung, Taitung
Hospital based 2001-2005 1,589 1,589
TMICS
Taiwan Maternal and Infant Cohort Study23
Taipei, Hsinchu, Taichung, Changjua, Kaohsiung, Hualien
Hospital based 2000-2014 1,616 2,577
VIETNAM BienHoa study
BienHoa Dioxin Cohort study24 Bien Hoa Hospital based 2012Sep -Nov
200 200
DaDoCiV
Dioxin and Development of Children in Vietnam
Hanoi, Phu, Cat, Bien Hoa
Community based 2008-2013 200 200
DaNang study
DaNang Dioxin Cohort study DaNang Hospital based 2008-2010 241 241
*Targeted recruitment numbers.

Table 2. Collected biological samples of participating studies in Birth Cohort Consortium of Asia Child
Father Mother
1~6 6~24 2~5 5~10 ≧10
Cohort T1 T2 T3 at deliverya postpartum Birth mo mo year year year
LWBC
U B, P BM CB,M
U U U
NJMUBC B, Db, U, Se
B, Db, U B, Db,
U B, Db, U
A, B, Db, P, U, UC
BM CB, M BM U B, Db, U B, Db, U B, Db,
U
SBC B, Db,
Ds, U, Se B, Db, U
B, Db, U
B, Db, U P H CB
N, U B, U, N B, U, N B, U,
N HBC Study
B P
CB
Ds
Hokkaido B
B Db
CB, Db
U
Sapporob
B, Db P BM, H CB, Db
TSCD
B P, H BM CB
CHECK
B B, P BM CB, M, UC, U U U, H U, H
COCOA B, Db
B, Db U,
S B, Db, P
CB, Db S B
U, B, Db, S
U, B, Db,S U,B
EDC study
B,U
B,U
MOCEH
B, Db, H, U
B, Db, U P BM CB, Db U B, Db, U B, Db, U B, Db, U
PSKC

Child
Father Mother
1~6 6~24 2~5 5~10 ≧10
Cohort T1 T2 T3 at deliverya postpartum Birth mo mo year year year
USM Pregnancy Cohort
B B H BM
H
Nepali
UC, H
CB, M
B, H
CLHNS
B
GUSTO Ds
B, H, Db, Ds
B, P, Db BM, H, Ds UC, CB, Ds,
M Ds, S Ds, S Ds, H, S
KCHS
TBPS
B, Db, P, U
CB, Db
B, H, S, U U
B, Db, Ds, U
TEC
B, Db, P, U
CB, Db
B, Db, Ds, U
TMICS
B, Db, U U B, Db, U P BM CB, M
B, Db, U B, Db, U B, Db, H, U B, Db, H, U
BienHoa
BM CB, UC
U U
DaDoCiV
B BM
Ds Ds
DaNang
BM
U
Abbreviations: A, amniotic fluid; B, blood; BM, breast milk; CB, cord blood; Db, DNA from blood; Ds, DNA from buccal swab ; H, hair; M, meconium; P, placenta; T1, T2, T3, first, second and third trimesters; S, stool; Se, semen; N, nail; U, urine; UC, umbilical cord;

a biosample collected during the hospital stay for delivery b Sapporo cohort did its first enrollment during T2-T3

Table 3. Measurements of selected environmental exposure/biomarkera of participating studies in Birth Cohort Consortium of Asia
Cohort Indoor air pollutions
Outdoor air pollutions
Tobacco smoking
Metals and Metalloids
Pesticides Persistent organic
pollutants other chemical exposures
LWBC
18 metalse Organophosphate,
pyrethrin PBDEs
BPA, trclosan, nonylphenol
NJMUBCb PM2.5, PM10 Cotinine, Nicotine,
Myosmine 25 metalsf
Organophosphate pesticides, Carbamate
pesticides, Organochlorine insecticides, Pyrethroid pesticides, Herbicides,
Fungicides
PCBs, PFASs, PBDEs
Pheonls, VOCs, Phthalates,
Phytoestrogens, Polycyclic aromatic
hydrocarbons
SBC dust
18 metalse Organophosphate,
pyrethrin PCBs, PFASs, PBDEs
BPA, trclosan, nonylphenol
HBC Study
Cu, Se, Zn
Hokkaido dust mite, phthalate
Cotininec
Dioxin, PCBs, PFASs BPA, phthalates
Sapporo
Cotinine Hg DDT, Drins, Chlordane, Heptaclor, HCH, Mirex,
Toxaphene, HCB Dioxin, PCBs, PFASs BPA, phthalates
TSCD
MeHg, Pb, Cd
Organochlorine Dioxin, PCBs

Cohort Indoor air pollutions
Outdoor air pollutions
Tobacco smoking
Metals and Metalloids
Pesticides Persistent organic
pollutants other chemical exposures
CHECK
Pb, Cd DDTs, chlordanes, HCB, HCHs, heptachlor, heptachlor epoxide, mirex
PBDEs, PCBs BPA, phthalates,
parabens
COCOA PM, Dust,
mite, Endotoxin
PM, NO2, O3 Cotinine
Phthalates
EDC study PM10, NO2, CO, O3, SO2
Cotinine Pb, Cd,
Hg PFASs
BPA, phthalates, Pyrethrids (3-PBA),
PAHs, VOCs
MOCEH
PM2.5, PM10, NO2,
HCHO, VOCs, dust
mite, endotoxin
PM2.5, PM10, NO2, HCHO,
VOCs Cotinineb
Pb, Cd, Hg, Mn
BPA, phthalates, PAHs
PSKC Humidity/
Mold Nicotine

Cohort Indoor air pollutions
Outdoor air pollutions
Tobacco smoking
Metals and Metalloids
Pesticides Persistent organic
pollutants other chemical exposures
USM Pregnancy Cohort
Nicotinec
Nepali
Pb, As, Cd, Zn, Se, Cu
CLHNS
GUSTO
PM2.5 Cotinine
KCHS PM2.5, Black
carbon PM2.5, Black
carbon
TBPS
Cotinine 18 metalse chlorpyrifos, cypermethrin, Flucythrinate
PFASs BPA, phenols, phthalates
TEC
PM2.5, PM10, NO2, HCHO,
VOCs
18 metalse
PFASs
TMICS
Cotinined 18 metalse DDT, Chlordane,
Heptaclor, HCH, HCB PFASs, PCBs, Dioxin BPA, phthalates, phenols
BienHoa
Dioxin

Cohort Indoor air pollutions
Outdoor air pollutions
Tobacco smoking
Metals and Metalloids
Pesticides Persistent organic
pollutants other chemical exposures
DaDoCiV
Dioxin
DaNang Dioxin Abbreviations: BPA, bisphenol A; DDTs, dichlorodiphenyl trichloroethanes; HCB, hexachlorobenzene; HCHs, hexachlorocyclohexanes; PAHs, Polycyclic aromatic hydrocarbons; PBDEs, polybrominated diphenyl ester; PCB, polychlorinated biphenyl; PFASs, polyfluoroalkyl substances; VOCs,Volatile Organic Compounds; a prenatal exposure, unless specified b planned to measure in the future c measurement include prenatal and postal exposure d postnatal exposure e 18 metals: lead, arsenic, mercury, cadmium, beryllium, antimony, barium, cerium, platinum, thorium, manganese, zinc, copper, selenium, cobalt, molybdenum, gallium, uranium f 25 metals: Aluminum, Antimony, Arsenic, Barium, Beryllium, Cadmium, Calcium, Cesium, Chromium, Cobalt, Copper, Gallium, Iron, Lead, Manganese, Mercury, Molybdenum, Nickel, Platinum, Selenium, Thallium, Thorium, Tungsten, Uranium, Zinc

Table 4. Health outcomes/surrogate marker recorded by participating studies in Birth Cohort Consortium of Asia
Cohort Fetal growth Pregnancy outcome
Growth and obesity
Allergic disease and immune function
Neurodevelopment and behavior problems
Endocrine function and puberty
Others
LWBC BW, BL preterm birth,
congenital malformation
weight, height
GESELL, CBCL, IQ (WPPSI/ WISC), ADHD-RS
thyroid function, sex
hormone
NJMUBC fetal sonography,
BW, BL
preterm birth, congenital
malformation, miscarriage,
stillbirth, FGR, LBW, SGA, macrosomia
weight, height, head, fat
ISAAC
CBCL, DDST, GESELL,PSQ, Japan S-M social adaptability scale,
SPM, C-WISC
thyroid function, sex
hormone
SBC fetal sonography,
BW, BL
preterm birth, congenital
malformation, stillbirth
weight, height, fat
ISAAC ASQ, ASQ-SE, Bayley III,
CBCL, M-CHAT, IQ (WPPSI/ WISC)
thyroid function, sex
hormone

Cohort Fetal growth Pregnancy outcome
Growth and obesity
Allergic disease and immune function
Neurodevelopment and behavior problems
Endocrine function and puberty
Others
HBC Study
fetal sonography, BW, BL
preterm birth, stillbirth, LBW,
SGA
weight, height, head
circumference ISAAC
ADHD-RS, ADI-R, ADOS, BISQ, Early Child
Behavioural Questionnaire, Edinburgh Handedness
Inventory, MacArthur CDI, M-CHAT, MSEL, SDQ,
WPPSI, VABS II
Eye gaze patterns for measuring
sociability and attention using Gazefinder®
Hokkaido BW, BL
preterm birth, congenital
malformation, miscarriage,
stillbirth, FGR, LBW, SGA
weight, height ISAAC
SCQ, SDQ, DCDQ,
M-CHAT, KIDS, CBCL, ADHD-Rating scale, Conners3P, WISC-IV
thyroid function,
reproductive hormones
Sapporo BW, BL
preterm birth, congenital
malformation, stillbirth, FGR,
LBW, SGA
weight, height IgE, ISAAC Bayley II, CBCL, WISC-III,
K-ABC, FT-II, DDST, WCST-KFS
thyroid function,
reproductive hormones

Cohort Fetal growth Pregnancy outcome
Growth and obesity
Allergic disease and immune function
Neurodevelopment and behavior problems
Endocrine function and puberty
Others
TSCD BW, BL preterm birth,
congenital malformation
weight, height
ADHD-Rating scale, Bayley II, Boston Naming Test, CBCL, CPT, Fagan Test, K-ABC, KSPD, NABS,
WISC-III, WISC_IV
thyroid function
CHECK BW, BL preterm birth weight, height
Bayley II, SMS tests
thyroid function
COCOA BW, BL preterm birth weight, height IgE,
IL-13, IFNγ, SPT, ISAAC
Mullen, ASQ, CBCL, IQ (WPPSI/ WISC), MSEL
EDC study fetal sonography,
BW
preterm birth, congenital
malformation weight, height
thyroid function,
sexual maturation, bone age
liver and kidney function
MOCEH fetal sonography,
BW, BL
preterm birth, congenital
malformation FGR, LBW, SGA
weight, height, head
ISAAC Bayley II, ASQ, WPPSI, CAT, CBCL, SRS,
SDQ, ARS

Cohort Fetal growth Pregnancy outcome
Growth and obesity
Allergic disease and immune function
Neurodevelopment and behavior problems
Endocrine function and puberty
Others
PSKC BW, BL preterm birth weight, height,
head, waist ISAAC
ASQ(Korea), Bayley II, CBCL 1.5-5(Korea), DDST II(Korea), WPPSI(Korea),
REVT
USM Pregnancy Cohort
BW, BL
weight, height, head, fat
(skinfold)
ASQ
Nepali BW, BL preterm birth
Brazelton III, Bayley II
CLHNS BW, BL preterm birth weight, height
GUSTO fetal sonography,
BW, BL
preterm birth, congenital
malformation FGR, LBW, SGA
weight, height, head, mid-arm,
abdominal circumference,
body composition
ISAAC, SPT ASQ, ASQ-SE, Bayley III,
CBCL, CTS, ITSEA, PEDS, PEDS:DM, Q-CHAT
KCHS BW, BL preterm birth,
congenital malformation
weight, height
Respiratory Conditions
(Symptom diaries,
Pneumonia, etc.)

Cohort Fetal growth Pregnancy outcome
Growth and obesity
Allergic disease and immune function
Neurodevelopment and behavior problems
Endocrine function and puberty
Others
TBPS fetal sonography,
BW, BL preterm birth, LBW, SGA
weight, height IgE, ISAAC CBCL, CDIIT, WPPSI
thyroid function,
sexual maturation, bone age
TEC BW, BL preterm birth weight, height IgE, ISAAC CBCL sexual
maturation, bone age
TMICS BW, BL, fetal sonography
preterm birth, congenital
malformation weight, height IgE, ISAAC Bayley II, CBCL, WPPSI
thyroid function,
sexual maturation, bone age
BienHoa BW, BL
weight, height, head and
abdominal circumference
Bayley III
thyroid function, sex
hormone, gender
difference of behavior

Cohort Fetal growth Pregnancy outcome
Growth and obesity
Allergic disease and immune function
Neurodevelopment and behavior problems
Endocrine function and puberty
Others
DaDoCiV BW, BL preterm birth
sex hormone
DaNang BW, BL
weight, height, head and
abdominal circumference
Bayley III, Kauffman-ABC II, M-ABC2, Eating
behavior, Autism Spectrum rating Scale (ASRS), ADHD
gender difference of
behavior
Abbreviations: ADHD rating scales, attention deficit hyperactivity disorder rating scales; ADI-R, Autism Diagnositc Interview Revised; ADOS, autism diagnositic observation scale; Bayley, Bayley Scales of Infant and Toddler Development; ASQ, Ages and Stages Questionnaire; ASQ-SE, ASQ- social Emotional; BIA, bioelectrical Impedance Analysis; BISQ, Brief Infant Sleep Questionnaire; BL, birth length; BW, birth weight; CBCL, Child Behavior Checklist; CPT, The Conners' Continuous Performance Test; Conners3P, The Conners Third edition Parent; CTS, Carey temperament Scales; DCDQ, developmental coordination disorder questionnaire; DDST, the Denver Developmental Screening Test; FGR, fetal growth restriction; FTII, The Fagan Test of Infant Intelligence; GA, gestational age; GESELL, the Gesell developmental schedules; IFNγ, Interferon gamma; IgE, immunoglobulin E; IL-13, Interleukin 13; ISAAC, The International Study of Asthma and Allergies in Childhood questionnaires; ITSEA, Infant Toddler Social Emotional Assessment; K-ABC, The Kaufman-Assessment Battery for Children; KIDS, Kinder Infant Development Scale; KSPD, Kyoto Scale of Psychological Development; LBW, low birth weight; MacArthur CDI, MacArthur Communicative Developmental Inventory; M-CHAT, modified checklist for autism in Toddlers; MSEL, Mullen Scales of Early learning; NABS, the Neonatal Behaviroal Assessment Scale; PEDS, Parent's Evaluation of Developmental Status; PEDS:DM, PEDS: Developmental Milestones; PST, Parent Symptom Questionnaire; Q-CHAT, Quantitative Checklist for Autism in Toddlers; REVT, Receptive and Expressive Vocabulary Test; SCID, structured clinical interview for DSM-IV Axis-I disorders; SCQ, social communication questionnaire; SDQ, the strength and difficulties questionnaire; SGA, small for gestational age; SPT, skin prick test; SMS, Social Maturity Scale; VABS II, Vineland Adaptive

Behavior Scales, second edition; WCST-KFS, Wisconsin Card Sorting Test-Keio-F–S version; WISC-III The Wechsler Intelligence Scale for Children-Third edition; WISC-IV The Wechsler Intelligence Scale for Children-Forth edition; WPPSI, Wechsler Preschool and Primary Scale of Intelligence.

Table 5-1 Maternal characteristics
Birth cohort
Age (years), N (mean±SD)
Pre-pregnancy BMI (kg/m2), N (mean±SD)
Educational level (years) N (%)
LWBC 756 (28.3±4.5) 741 (21.7±3.0) no education
5 (0.6) elementary
46 (6.0)
junior high school
303 (39.6)
senior high school
216 (28.2)
university 189 (24.7)
graduate school 7 (0.9)
NJMUBC * * * * * * * * * Shanghai * * * * * * * * *
HBC Study
1138 (31.4 ± 5.1)a
1138 (21.0 ± 3.4)
<12y (junior high
school) 68 (6.0)
12y (high
school) 317 (27.9)
13-15y (vocational &
college) 469 (41.2)
16y (university) 235 (20.7)
>16y (graduate school)
49 (4.3)
Hokkaido 18598
(29.8 ± 4.8) 19307
(21.2 ± 3.3)
≤9y (junior high
school) 1084 (5.5)
10-15y (high school or junior
college) 16553 (83.3)
university 2229 (11.2)
Sapporo 510 (30.4 ± 4.9) 506 (21.2 ± 3.2)
≤12y 225 (44.3)
13-16y 274 (53.9)
≥17y 9 (1.8)

Birth cohort
Age (years), N (mean±SD)
Pre-pregnancy BMI (kg/m2), N (mean±SD)
Educational level (years) N (%)
TSCD 1348 (30.3 ± 4.8) 1348 (21.2 ± 3.1)
≤12y 756 (56.1)
>12y 591 (43.9)
CHECK 352 (33.5 ± 4.1) 352 (21.4 ± 3.3) N.A.
COCOA 2224 (32.6 ± 3.6) 2041 (20.7 ± 2.6) no education
1 (0.1) elementary
1 (0.1)
middle school
1 (0.1)
high school 110 (5.5)
vocational college 61 (3.0)
university 1415 (70.1)
graduate school
430 (21.3)
EDC study 663 (31.4 ± 3.6) 662 (21.9 ± 3.0)
Junior high school 1 (0.15)
Senior high school 124 (18.7)
university 461 (69.5)
Graduate school
77 (11.6)
MOCEH 1604
(30.30 ± 3.74) 1432 (22.9 ± 3.0)
<12y (high school)
397 (26.5)
>12y (university or graduated
school) 1103 (73.5)
PSKC 2077
(31.3 ± 3.7) 2067 (21.2±2.9)
below high school
14 (0.6)
high school 629 (30.5)
college 590 (28.6)
university 714 (34.6)
postgraduate degree
115 (5.6) USM Pregnancy Cohort
153 (28.9 ± 4.5) 153 (22.6 ± 4.1) no education
0 primary 1(0.7)
secondary 51(33.3)
diploma 64 (41.8)
university degree
26 (17.0)
postgraduate degree
11 (7.2)

Birth cohort
Age (years), N (mean±SD)
Pre-pregnancy BMI (kg/m2), N (mean±SD)
Educational level (years) N (%)
Nepali 100 (22.9 ± 3.7) 100 (23.2 ± 2.9) Mean year (SD)
9.2 (3.8) and Range 0 to 17
CLHNS 3327 (26.0 ± 6.0) N.A. no education
61 (1.8) elementary 1984 (59.6)
high school 860 (25.8)
college 422 (12.7)
GUSTO 1247 (30.6 ± 5.2) 1141 (23.7 ± 4.8) no education
2 (0.2) primary 55
(4.5) secondary 451 (36.7)
GCE A Level/Diploma
311 (25.3)
university 409 (33.3)
KCHS 375 (29.6 ± 5.2) 326 (22.6 ± 4.2) Never gone to school 2 (0.5)
Primary education
3 (0.8)
Secondary education 96 (25.5)
G.C.E O/L 108 (28.6)
G.C.E O/L & Vocational education
2 (0.5)
G.C.E A/L 134 (35.5)
Degree 28 (7.4)
TBPS 486 (30.9 ± 4.6) 486 (20.9 ± 3.0) no education
3 (0.6) elementary
10 (2.1)
junior high school
32 (6.6)
senior high school
113 (23.3)
specialized training school
112 (23.1)
university 149 (30.7)
graduate school
66 (13.6)

Birth cohort
Age (years), N (mean±SD)
Pre-pregnancy BMI (kg/m2), N (mean±SD)
Educational level (years) N (%)
TEC 1521 (27.6 ± 8.9) 1265 (20.9 ± 3.3) no education
15 (1) elementary
50 (3.2)
junior high school
215 (13.8)
senior high school
823 (52.8)
specialized training school
303 (19.4)
university 132 (8.4)
graduate school
22 (1.4)
TMICS 1987 (31.1 ± 4.8) 1611 (21.9 ± 3.8) no education
5 (0.2) elementary
28 (1.4)
junior high school
203 (10.1)
senior high school
404 (20.1)
specialized training school/university
1141 (56.8)
graduate school
229 (11.4)
BienHoa 210 (28.6 ± 4.6) N.A. no education
1 (0.5) elementary
13(6.2)
junior high school
57 (27.1)
senior high school
70 (33.3)
specialized training school
39 (18.6)
university 30 (14.3)
DaDoCiV 236 (24.8 ± 3.6) N.A. elementary 34 (14.8)
junior high school
99 (43.2)
high school
67 (29.3)
university 29 (12.7)
DaNang 217 (27.8 ± 6.0) N.A. no education
9 (4.1) elementary 44 (20.3)
junior high school
94 (43.3)
senior high school
48 (22.1)
specialized training school
19 (8.8)
university 3 (1.4)
Abbreviations: N.A., not available.

a number of participating parturient [1138)] is not equal to participating infants [1258] because of multiple births and multiple entry of some of the parturient *: still recruiting subjects

Table 5-2 Maternal characteristics
Birth cohort Parity Smoking status during pregnancy,
N (%)
Environmental tobacco smoke Exposure during
pregnancy, N(%)
Alcohol drinking during pregnancy,
N(%) primipara multipara non-smoker Quitter smoker yes yes LWBC 489 (67.3) 238 (32.7) 766 (99.0) 4 (0.5) 4 (0.5) 339 (43.8) 0 NJMUBC * * * * * * * Shanghai * * * * * * * HBC Study 615 (54.0) 523 (46.0) 884 (77.6) 192 (16.8)a 62 (5.5)b N.A. 145 (12.8)c Hokkaido 8183 (43.8) 10498 (56.1) 9113 (54.5) 5284 (31.6) 2298 (13.7) 8662 (43.9)d 2438 (18.3) Sapporo 240 (47.7) 263 (52.3) 228 (44.9) 177 (34.8) 103 (20.3) 372 (73.2)e 157 (30.9) TSCD 725 (53.8) 623 (46.2) 1046(77.8) 222(16.5) 76(5.7) N.A. 140 (10.4) CHECK 136 (38.6) 216 (61.4) 252 (96.6)
9 (3.4) 131 (45.3) 37 (13.7)
COCOA 1099 (58.4) 782 (41.6) 164 (95.9)
7 (4.1) 1050 (60.6) 164 (9.4) EDC study 374 (56.6) 287 (43.4) 531 (92.7) 42 (7.3) 163 (24.6) 173 (30.6) MOCEH 681 (50.9) 657 (49.1) 1327 (88.2) 164 (10.9) 13 (0.9) 921 (65.1)d 75 (5.4) PSKC 984 (47.5) 1088 (52.5) 1813 (97.3) 33 (1.8) 17 (0.9) 556 (60.3) 502 (26.9) USM Pregnancy Cohort
43 (28.1) 110 (71.9) 153 (100.0) 0 0 65 (44.2) 0
Nepali 66 (66.0) 34 (34.0)
5 (5.0)
4 (4.0) CLHNS 768 (23.1) 2559 (76.9) 2875 (86.4)
452 (13.6)
813 (24.4)
GUSTO 545 (45.9) 643 (54.1) 1149 (97.5)
29 (2.5) 432 (38.0) 21 (1.8)

Birth cohort Parity Smoking status during pregnancy,
N (%)
Environmental tobacco smoke Exposure during
pregnancy, N(%)
Alcohol drinking during pregnancy,
N(%) primipara multipara non-smoker Quitter smoker yes yes KCHS 105 (29.6) 227 (63.9) 377 (100)
0 5 (1.3) 0
TBPS 230 (47.3) 256 (52.7) 460 (94.7)
26 (5.30) 139 (28.6) 21 (4.3) TEC 647 (47.2) 723 (52.8) 1452 (95.8) 16 (1.1) 48 (3.2) 618 (44.0) 32 (2.1) TMICS 682 (43.5) 887 (56.5) 1974 (98.4) 12 (0.6) 20 (1.0) N.A. 95 (4.7) BienHoa 77 (36.7) 133 (63.3) 207 (98.6) 0 3 (1.4) 136 (64.8) 10 (4.8) DaDoCiV 152 (64.7) 83 (35.3) 233 (99.2) 0 2 (0.8) 114 (48.5) 7 (3.0) DaNang 73 (30.5) 163 (69.5) 241 (100) 0 0 198 (82.8) 17 (8.7) a quitted before 12wks of gestational age b any smoking at/after 12wks of gestational age (including those quitted after 12 wks) c any drinking at/after 12wks of gestational age d assessed based on exposure of pregnant women at home or workplace e pregnant women who lived with smoker(s) during pregnancy *: still recruiting subjects

Table 6. Infant Characteristics
Birth cohort Male, N (%) Gestational age (weeks), N (mean±SD)
Birth weight (gm), N (mean±SD)
Preterm, N (%) Low birth weight, N (%)
LWBC 391 (51.2) 756 (39.3 ± 2.0) 763 (3419 ± 501) 30 (4.0) 17 (2.2) NJMUBC * * * * * SBC * * * * * HBC Study 648 (51.5) 1258 (38.9 ± 1.6) 1258 (2943 ± 435) 82 (6.5) 160 (12.7) Hokkaidoa 9204 (50.4) 18004 (38.7 ± 1.5) 18004 (3029 ± 420) 980 (5.4) 1592 (8.8) Sapporo 242 (48.0) 504 (38.9 ± 1.5) 504 (3039 ± 521) 35 (6.9) 34 (6.7) TSCD 696 (51.6) 1349 (39.6 ± 1.2) 1349 (3111 ± 355) N.A. N.A. CHECK 177 (50.4) 352 (39.3 ± 1.2) 352 (3256 ± 388) 4 (1.1) 13 (3.7) COCOA 1029 (52.0) 1915 (39.1 ± 1.3) 1690 (3184 ± 438) 80 (4.2) 94 (5.6) EDC study 356 (53.7) 660 (38.7 ± 1.5) 608 (3240 ± 447) 8 (1.2) 26 (4.3) MOCEH 774 (52.2) 1502 (39.0 ± 1.7) 1475 (3261 ± 444) 80 (5.3) 41 (2.8) PSKC 1059 (51.0) 2066 (39.2 ± 1.2) 2073 (3258 ± 408) 63(3.0) 62(3.0) USM Pregnancy Cohort
69 (45.1) 153 (38.8 ± 1.2) 153 (3110 ± 420) 0 11 (7.2)
Nepali 47 (47.0) 100 (38.9 ± 1.4) 100 (3029 ± 438)
CLHNS 1632 (53.0) 3052 (38.9 ± 2.6) 3040 (2987 ± 442) 478 (15.6) 372 (14.1) GUSTO 627 (52.7) 1190 (38.6 ± 1.7) 1190 (3065 ± 484) 103 (8.7) 117 (9.8) KCHS 170 (48.0) 327 (38.3 ± 2.1) 354 (2940 ± 567) 38 (10.7) 43 (12.1) TBPS 247 (50.8) 486 (38.5 ± 1.7) 486 (3158 ± 476) 42 (8.6) 28 (5.8)

Birth cohort Male, N (%) Gestational age (weeks), N (mean±SD)
Birth weight (gm), N (mean±SD)
Preterm, N (%) Low birth weight, N (%)
TEC 809 (51.9) 1510 (38.9 ± 1.2) 1480 (3094 ± 429) 76 (5.0) 80 (5.4) TMICS 712 (53.5) 1332 (38.4 ± 2.0) 1308 (3087 ± 465) 90 (6.8) 90 (6.9) BienHoa 111 (52.9) 210 (38.9 ± 2.6) 210 (3297 ± 411) 6 (2.9) 2 (1.0) DaDoCiV 125 (53.2) N.A. 120 (3211 ± 433) N.A. 6 (5.0) DaNang 125 (57.4) 217 (39.5 ± 0.8) 217 (3228 ± 375) 0 4 (1.8) Abbreviations: N.A., not available. a In Hokkaido cohort, gestational age, birth weight, preterm birth and low birth weight were calculated among subjects with live birth *: still recruiting subjects