Bioprosthetic Valve Thrombosis Versus Structural Failure · Bioprosthetic Valve Thrombosis Versus...
10
Bioprosthetic Valve Thrombosis Versus Structural Failure Clinical and Echocardiographic Predictors Alexander C. Egbe, MD, MPH,* Sorin V. Pislaru, MD, PHD,* Patricia A. Pellikka, MD,* Joseph T. Poterucha, DO,* Hartzell V. Schaff, MD,y Joseph J. Maleszewski, MD,z Heidi M. Connolly, MD* ABSTRACT BACKGROUND Bioprosthetic valve thrombosis (BPVT) is considered uncommon; this may be related to the fact that it is often unrecognized. Recent data suggest that BPVT responds to vitamin K antagonists, emphasizing the need for reliable diagnosis. OBJECTIVES This study sought to determine the diagnostic features of BPVT and to formulate a diagnostic model for BPVT. METHODS Cases of BPVT occurring between 1997 and 2013 were identified from the Mayo Clinic pathology database. Patients with BPVT were matched 1:2 for age, sex, and prosthesis position with patients whose valves were explanted for structural failure. We formulated a diagnostic model for BPVT using multivariate linear logistic regression and receiver operating characteristic. RESULTS Among 397 consecutive cases of explanted bioprostheses, there were 46 cases of BPVT (11.6%; aortic 29, mitral 9, tricuspid 7, pulmonary 1), mean age was 63 years, and 68% were male. Thirty (65%) cases occurred >12 months post-implantation; median bioprosthetic valve longevity was 24 months (cases) versus 108 months (controls) (p < 0.001). Independent predictors of BPVT were >50% increase in mean echo-Doppler gradient from baseline within 5 years (odds ratio [OR]: 12.7), paroxysmal atrial fibrillation (OR: 5.19), subtherapeutic international normalized ratio (OR: 7.37), increased cusp thickness (OR: 12.2), and abnormal cusp mobility (OR: 6.94). Presence of all 5 diagnostic features was predictive of BPVT with 76% sensitivity, 93% specificity, 85% positive predictive value, and 89% negative predictive value (p < 0.001). CONCLUSIONS BPVT is not uncommon and can occur several years after surgery. A combination of clinical and echocardiographic features can reliably diagnose BPVT. (J Am Coll Cardiol 2015;66:2285–94) © 2015 by the American College of Cardiology Foundation. T he predominant mechanism of bioprosthetic valve (BPV) dysfunction is structural deterio- ration (1,2), and the risk of bioprosthetic valve thrombosis (BPVT) is considered very low. As a result, the American College of Cardiology/American Heart Association (ACC/AHA) and European Society of Cardiology (ESC) guidelines (3,4) do not recommend oral anticoagulation with vitamin K antagonists (VKAs) beyond 3 months for mitral, tricuspid, and pulmonary valve implantation. Furthermore, the guidelines are discordant for aortic BPVs, with aspirin preferred over VKA in the European guidelines and VKA recommended for 3 to 6 months in the ACC/AHA guidelines. The diagnosis of BPVT remains very chal- lenging due to a general lack of awareness of its existence. Several case series have shown that BPVT can be effectively treated with VKA, avoiding the need for thrombolytic therapy and surgery (5–8). We previously suggested that presence of an increased gradient >50% over baseline should raise From the *Division of Cardiovascular Diseases, Mayo Clinic, Rochester, Minnesota; yDivision of Cardiovascular Surgery, Mayo Clinic, Rochester, Minnesota; and zAnatomic Pathology, Mayo Clinic, Rochester, Minnesota. The authors have reported that they have no relationships relevant to the contents of this paper to disclose. Manuscript received August 7, 2015; revised manuscript received September 10, 2015, accepted September 14, 2015. Listen to this manuscript’s audio summary by JACC Editor-in-Chief Dr. Valentin Fuster. JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY VOL. 66, NO. 21, 2015 ª 2015 BY THE AMERICAN COLLEGE OF CARDIOLOGY FOUNDATION ISSN 0735-1097/$36.00 PUBLISHED BY ELSEVIER INC. http://dx.doi.org/10.1016/j.jacc.2015.09.022
Transcript of Bioprosthetic Valve Thrombosis Versus Structural Failure · Bioprosthetic Valve Thrombosis Versus...

Listen to this manuscript’s
audio summary by
JACC Editor-in-Chief
Dr. Valentin Fuster.
J O U R N A L O F T H E AM E R I C A N C O L L E G E O F C A R D I O L O G Y V O L . 6 6 , N O . 2 1 , 2 0 1 5
ª 2 0 1 5 B Y T H E AM E R I C A N C O L L E G E O F C A R D I O L O G Y F O U N DA T I O N I S S N 0 7 3 5 - 1 0 9 7 / $ 3 6 . 0 0
P U B L I S H E D B Y E L S E V I E R I N C . h t t p : / / d x . d o i . o r g / 1 0 . 1 0 1 6 / j . j a c c . 2 0 1 5 . 0 9 . 0 2 2
Bioprosthetic Valve Thrombosis VersusStructural Failure
Clinical and Echocardiographic PredictorsAlexander C. Egbe, MD, MPH,* Sorin V. Pislaru, MD, PHD,* Patricia A. Pellikka, MD,* Joseph T. Poterucha, DO,*Hartzell V. Schaff, MD,y Joseph J. Maleszewski, MD,z Heidi M. Connolly, MD*
ABSTRACT
Fro
Cli
ha
Ma
BACKGROUND Bioprosthetic valve thrombosis (BPVT) is considered uncommon; this may be related to the fact that it
is often unrecognized. Recent data suggest that BPVT responds to vitamin K antagonists, emphasizing the need for
reliable diagnosis.
OBJECTIVES This study sought to determine the diagnostic features of BPVT and to formulate a diagnostic
model for BPVT.
METHODS Cases of BPVT occurring between 1997 and 2013 were identified from the Mayo Clinic pathology database.
Patients with BPVT were matched 1:2 for age, sex, and prosthesis position with patients whose valves were explanted for
structural failure. We formulated a diagnostic model for BPVT using multivariate linear logistic regression and receiver
operating characteristic.
RESULTS Among 397 consecutive cases of explanted bioprostheses, there were 46 cases of BPVT (11.6%; aortic 29,
mitral 9, tricuspid 7, pulmonary 1), mean age was 63 years, and 68% were male. Thirty (65%) cases occurred >12 months
post-implantation; median bioprosthetic valve longevity was 24 months (cases) versus 108 months (controls)
(p < 0.001). Independent predictors of BPVT were >50% increase in mean echo-Doppler gradient from baseline within
5 years (odds ratio [OR]: 12.7), paroxysmal atrial fibrillation (OR: 5.19), subtherapeutic international normalized ratio
(OR: 7.37), increased cusp thickness (OR: 12.2), and abnormal cusp mobility (OR: 6.94). Presence of all 5 diagnostic
features was predictive of BPVT with 76% sensitivity, 93% specificity, 85% positive predictive value, and 89% negative
predictive value (p < 0.001).
CONCLUSIONS BPVT is not uncommon and can occur several years after surgery. A combination of clinical and
echocardiographic features can reliably diagnose BPVT. (J Am Coll Cardiol 2015;66:2285–94)
© 2015 by the American College of Cardiology Foundation.
T he predominant mechanism of bioprostheticvalve (BPV) dysfunction is structural deterio-ration (1,2), and the risk of bioprosthetic valve
thrombosis (BPVT) is considered very low. As a result,the American College of Cardiology/American HeartAssociation (ACC/AHA) and European Society ofCardiology (ESC) guidelines (3,4) do not recommendoral anticoagulation with vitamin K antagonists(VKAs) beyond 3 months for mitral, tricuspid, andpulmonary valve implantation. Furthermore, the
m the *Division of Cardiovascular Diseases, Mayo Clinic, Rochester, Mi
nic, Rochester, Minnesota; and zAnatomic Pathology, Mayo Clinic, Roches
ve no relationships relevant to the contents of this paper to disclose.
nuscript received August 7, 2015; revised manuscript received Septembe
guidelines are discordant for aortic BPVs, with aspirinpreferred over VKA in the European guidelines andVKA recommended for 3 to 6 months in the ACC/AHAguidelines. The diagnosis of BPVT remains very chal-lenging due to a general lack of awareness of itsexistence. Several case series have shown that BPVTcan be effectively treated with VKA, avoiding theneed for thrombolytic therapy and surgery (5–8).
We previously suggested that presence of anincreased gradient >50% over baseline should raise
nnesota; yDivision of Cardiovascular Surgery, Mayo
ter, Minnesota. The authors have reported that they
r 10, 2015, accepted September 14, 2015.

ABBR EV I A T I ON S
AND ACRONYMS
AF = atrial fibrillation
BPV = bioprosthetic valve
BPVT = bioprosthetic valve
thrombosis
INR = international normalized
ratio
TEE = transesophageal
echocardiogram
TTE = transthoracic
echocardiogram
VKA = vitamin K antagonist
Egbe et al. J A C C V O L . 6 6 , N O . 2 1 , 2 0 1 5
Predictors of Bioprosthetic Valve Thrombosis D E C E M B E R 1 , 2 0 1 5 : 2 2 8 5 – 9 4
2286
suspicion of BPVT (9), but direct comparisonof echocardiographic characteristics of BPVTand degenerated BPV has not been per-formed. Thus, we set forth to delineate theclinical and echocardiographic characteristicsof pathologically proven BPVT to help clini-cians recognize BPVT and, with effective VKAtherapy, potentially help patients avoid sur-gical intervention.
METHODS
PATIENT SELECTION AND CHARACTERISTICS.
The Mayo Clinic Institutional Review Board
approved the study protocol. The pathology and sur-gical databases were used to identify all BPVsexplanted from adults (age $18 years). We reviewedthe pathology reports of 397 patients whose prosthe-ses were explanted within the study period, and BPVTwas considered to be present whenever valve throm-bosis was the main mechanism of BPV dysfunction(n ¼ 46). We then matched BPVs that were explantedfor structural valve failure to cases of BPVT (1 BPVT: 2structural valve failures). The structural valve failuregroup was matched by age (�5 years), sex, and pros-thesis position. To estimate the overall incidence ofBPVT in our surgical practice, we also recorded thetotal numbers of BPV implantations performed at theMayo Clinic during the same time interval. Our studyobjectives were to estimate the prevalence of BPVT asa reason for BPV explantation, identify clinical andechocardiographic characteristics of BPVT, andformulate a diagnostic model for BPVT.SEE PAGE 2295
Clinical, echocardiographic, and surgical data atthe time of initial BPV implantation, during follow-up, and at the time of BPV dysfunction and explan-tation were retrieved from the medical record. Weclassified atrial fibrillation (AF) into: paroxysmal AF(defined as history of AF lasting <7 days documentedin clinical notes, electrocardiogram, or Holter moni-toring), perioperative AF (defined as AF occurringwithin 1 month of valve surgery), and persistent AF(defined as AF >7 days duration that is being treatedwith VKA � rate control therapy). We reviewed allinternational normalized ratio (INR) results obtainedwithin the last 3 months prior to diagnosis of BPVT orexplantation; patients were classified as having sub-therapeutic INR if they had any INR <2.0.
ECHOCARDIOGRAPHY. Reports and digitally storedimages of transthoracic echocardiogram (TTE) andtransesophageal echocardiograms (TEE) were sys-tematically reviewed. Baseline prosthetic gradients
were obtained from the “fingerprint” echocardiogramperformed early after surgical BPV implantation; whenbaseline data were unavailable because these pros-theses were implanted elsewhere (n ¼ 17), meannormal values from the published literature were usedas surrogates for baseline post-implantation gradients(10,11). The images from the index echocardiogram(TTE ¼ 94 and TEE ¼ 108) at the time of diagnosis ofBPV dysfunction were systematically reviewed(A.C.E). Two-dimensional (2D) morphology of the BPVwas assessed using the following pre-defined param-eters: cusp thickness, presence of abnormal cusp mo-tion, possible intracardiac thrombus or spontaneousechocardiographic contrast, and presence of calcifi-cation. These 2D parameters were collected both forBPVT and structural valve failure. Increased cuspthickness was defined as thickness >2 mm or signifi-cantly thicker compared to “fingerprint” echocardio-gram. An echocardiographer with experience invalvular disease and BPVT (S.V.P.) reviewed randomlyselected studies in one-half of the entire cohort.Discordant interpretations were adjudicated after athird review by a senior echocardiographer (H.M.C).All reviewers were blinded to the interpretation ofothers and the etiology of BPV dysfunction.
STATISTICAL ANALYSIS. All statistical calculationswere performed with the JMP version 10.0 software(SAS Institute Inc., Cary, North Carolina). Categoricalvariables were expressed as percentages whereascontinuous variables were expressed as mean � SD ormedian and interquartile range (IQR) for skewed data.Comparison of categorical variables was performedusing the chi-square test or Fisher exact test, whereascomparison of continuous variables was performedwith Student t test or Wilcoxon rank sum test, asappropriate. To identify clinical and echocardio-graphic predictors of BPVT, data from BPVT andmatched structural valve failure were analyzed withmultivariable logistic regression model. Receiveroperating characteristic (ROC) curves were plottedand the corresponding areas under the curve (AUC)were compared by the method of DeLong et al. (12) todetermine the best combination of these clinical andechocardiographic predictors that identified BPVT,providing optimal balance between sensitivity andspecificity.
RESULTS
Baseline clinical characteristics of BPVT and struc-tural valve failure groups are shown in Table 1.Between January 1997 and December 2013, a totalof 397 adult patients underwent surgical explantationof a BPV at the Mayo Clinic. Excluded from analysis

TABLE 1 Baseline Clinical Characteristics
All (N ¼ 138) BPVT (n ¼ 46) SVF (n ¼ 92) p Value
Age, yrs 62 � 13 63 � 15 61 � 15 0.88
Males 96 (70) 31 (68) 65 (70) 0.73
Hemoglobin, g/dl 13.2 � 1.4 13.4 � 1.6 12.9 � 1.1 0.39
BSA, m2 2.0 � 0.2 2.0 � 0.1 2.0 � 0.3 0.95
Paroxysmal AF 57 (42) 21 (64) 28 (30) 0.002
Perioperative AF 44 (32) 20 (46) 24 (26) 0.03
Persistent AF 26 (19) 9 (20) 17 (18) 0.35
Atrial flutter 12 (9) 6 (13) 6 (7) 0.21
Hypertension 77 (57) 41 (45) 36 (80) 0.001
Diabetes 41 (30) 20 (44) 21 (23) 0.016
CAD 56 (41) 18 (40) 38 (41) 0.91
Hyperlipidemia 68 (50) 33 (76) 35 (37) 0.02
Patients on VKA 40 15 25 0.19
Subtherapeutic INR 19 12 6 0.02
Indication for VKA
Persistent AF 26 9 17
Prior thromboembolism* 14 6 8
Post-operative use of APA† 37 (59) 23 (95) 14 (36) 0.001
Post-operative use of VKA‡ 24 (38) 9 (37) 15 (38) 0.89
Values are mean � SD, n (%), or n. *Defined as venous thromboembolism, pulmonary embolism, stroke/transient ischemic attack. †Within the first 3 post-operative months(number of patients with available data ¼ 63). ‡Within the first 3 post-operative months (number of patients with available data ¼ 63).
AF ¼ atrial fibrillation; APA ¼ antiplatelet agent; BPVT ¼ bioprosthetic valve thrombosis; BSA ¼ body surface area; CAD ¼ coronary artery disease; INR ¼ internationalnormalized ratio; SVF ¼ structural valve failure; VKA ¼ vitamin K antagonist.
TABLE 2 Prevalence and Estimated Incidence of BPVT
BPV Explanted (n) BPVT (n) BPVT Prevalence (%)
Aortic 265 29 10.9
Mitral 71 9 12.7
Tricuspid 58 7 12.1
Pulmonary 3 1
Total 397 46 11.6
EstimatedBPVT Incidence* (%)
Aortic 3,843 29 0.57
Mitral 1,395 9 0.64
Tricuspid 722 7 1.0
Pulmonary 218 1 0.5
Total 6,178 3 0.74
*Incidence based on total number of valves implanted during the study interval;see text for details.
BPV ¼ bioprosthetic valve; BPVT ¼ bioprosthetic valve thrombosis.
J A C C V O L . 6 6 , N O . 2 1 , 2 0 1 5 Egbe et al.D E C E M B E R 1 , 2 0 1 5 : 2 2 8 5 – 9 4 Predictors of Bioprosthetic Valve Thrombosis
2287
were patients with mixed disease (thrombosis anddegeneration) in whom the main mechanism couldnot be established (n ¼ 4), those with active endo-carditis (n ¼ 2), and those with history of thrombo-philia (n ¼ 1). A diagnosis of BPVT was identified inthe pathology report of 46 patients, of which 29 (63%)were aortic, 9 (20%) mitral, 7 (15%) tricuspid, and1 (2%) pulmonary. Porcine valves were the mostcommon type in the BPVT group (n ¼ 36; 78%), fol-lowed by pericardial valves (n ¼ 8; 18%) and homo-grafts (n ¼ 2; 4%). Isolated stenosis without evidenceof BPV regurgitation was seen in 25 (54%) patients;isolated prosthetic regurgitation was noted in only 5(11%); and a mixed mechanism of prostheticdysfunction was present in 15 (33%) patients.
A total of 92 patients with pathology-demonstratedstructural failure and no thrombus were selected asmatched controls. Porcine valves were explantedfrom 50 (54%), pericardial valves from 41 (45%), andhomografts from 1 (1%). Isolated stenosis or regurgi-tation was seen each in 30 (33%) patients, while amixed mechanism was noted in 32 (35%) patients.BPVT patients and structural valve failure patientswere well matched for main demographic character-istics (Table 1).
The overall prevalence of BPVT was 11.6% (46 of 397explanted BPVs), with no significant differencesamong various valve positions (Table 2). There were
6,178 BPV implantations; 3,161 (51%) had a follow-upechocardiogram at the Mayo Clinic up to 24 monthspost-surgery. The incidence of BPVT based on the totalnumber of BPV implantations performed in the similarinterval is thus estimated at 0.74%, or 1.46% if onlythose with a follow-up echocardiogram are included.
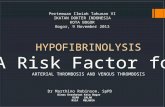
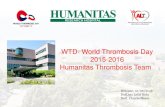
TIMING OF BPV EXPLANTATION. The time intervalto surgical explantation is presented in Figure 1. Only16 (35%) instances of BPVT occurred within the first

FIGURE 1 Timing of BPVT
100
80
60
40
20
00 5 10 15 20
Time (Years)
Free
Fro
m E
xpla
ntat
ion
(%)
BPVT
Structural Failure
Log–rank p <0.0001
Freedom From Explantation Time to Explantation by Position
Aortic Mitral Tricuspid PulmonaryBPV Position
BPVT Structural Failure
**
*
15
10
5
0
Tim
e (Y
ears
)
At risk 4692
1373
535
113
03
A B
(A) Kaplan-Meier curves show freedom from BPV explantation in BPVT (orange) versus structural valve failure (blue). BPVT occurred
significantly earlier than structural deterioration, after a median of 24 months; this was true regardless of BPV position (B). *p < 0.05 compared
to structural valve failure. Pulmonary BPVT was seen in only 1 patient; hence statistical analysis was not performed for this position.
BPV ¼ bioprosthetic valve; BPVT ¼ bioprosthetic valve thrombosis.
Egbe et al. J A C C V O L . 6 6 , N O . 2 1 , 2 0 1 5
Predictors of Bioprosthetic Valve Thrombosis D E C E M B E R 1 , 2 0 1 5 : 2 2 8 5 – 9 4
2288
12 months of initial implantation, with a median time-to-explantation of 24 months (IQR: 12 to 60 months).Late BPVT (more than 5 years post-implantation) wasseen in 7 (15%) patients. The timing of BPVT did notvary significantly by prosthesis position (p ¼ 0.77).Analysis of matched cases of structural valve failureshowed that the time to explantation for structuralvalve failure occurred significantly later (median: 108months; IQR: 72 to 132 months; p < 0.001), regardlessof BPV position (Figure 1B). Freedom from explanta-tion was significantly lower for BPVT (39% and 15% at3 and 6 years, respectively) compared to structuralvalve failure (81% and 66% at 3 and 6 years, respec-tively) (p < 0.001) (Figure 1A, Central Illustration).
ECHOCARDIOGRAPHY. The index TTE and TEE re-ports described abnormal BPV in each case; possibleBPVT was mentioned in only 2 of 42 TTEs (5%) and in6 of 45 TEEs (13%). Description of the 2D morphologyof the BPV by review of all available digital images forBPVT and structural valve failures is shown in Table 3.
BPVT usually presented with increased cuspthickness (commonly on the downstream aspect ofthe valve), and associated reduced cusp mobility withincreased gradients; moderate or more regurgitationwas less common in BPVT compared to structuralvalve failure patients for aortic (p < 0.001) and mitral(p ¼ 0.056) positions (Table 3). On the otherhand, structural valve failure was more commonlyassociated with calcified cusps, reduced leafletmobility, and significant regurgitation. The typical
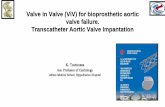
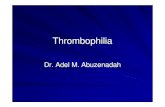
echocardiographic features of BPVT and structuralvalve failure are illustrated in Figure 2 and in OnlineVideos 1 and 2.
RISK FACTORS AND INDEPENDENT PREDICTORS
FOR BPVT. Forty patients (10%) in the entire cohortwere on VKA at the time of diagnosis of BPVdysfunction; 19 (48%) of these patients had subther-apeutic INRs within the last 3 months before diag-nosis of BPV dysfunction. One additional patient wasstarted on unfractionated heparin at the time of BPVTdiagnosis and underwent surgery 2 days later. Nopatient received novel anticoagulant or thrombolytictherapy and none of the patients had high cardiacoutput state.
In considering univariate and multivariate analysisof BPVT predictors (Table 4), multivariate logisticregression analysis showed that paroxysmal AF,subtherapeutic INR for patients on VKA therapy, anincrease in mean transvalvular gradient of >50%above baseline within 5 years in the absence of a highcardiac output state, increased cusp thickness, andabnormal cusp mobility all were strongly associatedwith BPVT. Multiple ROC curves were generated todetermine the diagnostic accuracy of each of the 5independent predictors of BPVT. The comparison ofthe discriminatory ability of the different ROCmodels showed that the combination of all 3 echo-cardiographic predictors (50% increase in gradientwithin 5 years, increased cusp thickness, andabnormal cusp mobility) had the highest AUC

CENTRAL ILLUSTRATION Predictors of Bioprosthetic Valve Thrombosis: BPVT Versus Structural Valve Failure
Egbe, A.C. et al. J Am Coll Cardiol. 2015; 66(21):2285–94.
BPVT (left) and structural deterioration (right) are distinct diseases, with different pathological substrate, timingof presentation (Kaplan-Meier curves
show freedom from BPV explantation), and echocardiographic characteristics. BPV ¼ bioprosthetic valve; BPVT ¼ bioprosthetic valve thrombosis.
J A C C V O L . 6 6 , N O . 2 1 , 2 0 1 5 Egbe et al.D E C E M B E R 1 , 2 0 1 5 : 2 2 8 5 – 9 4 Predictors of Bioprosthetic Valve Thrombosis
2289
(AUC ¼ 0.852; 95% confidence interval [CI]: 0.763to 0.940) compared to the other models. The pres-ence of all 3 echocardiographic predictors reliablydiagnosed BPVT with sensitivity of 72% and speci-ficity of 90% when we applied it to the 138 patientsincluded in our cohort (Table 5).
DISCUSSION
To the best of our knowledge, this is the first studyto directly compare the clinical and echocardio-graphic characteristics of thrombosed and degen-erated bioprostheses. Our major findings are: 1)BPVT referred for surgical intervention occurssignificantly earlier than BPV degeneration, after amedian of 24 months post-implantation; 2) BPVT ismore common than previously reported; and 3)concomitant presence of 3 echocardiographic char-acteristics (an increased gradient >50% over baselinewithin first 5 years after implantation, increased cuspthickness, and abnormal cusp mobility) appears tocharacterize BPVT with acceptable sensitivity and
high specificity in the setting of concordant clinicalfeatures.
PROSTHETIC DYSFUNCTION DUE TO BPVT. Thepredominant mechanism of BPV dysfunction isstructural deterioration (1,2), and in the past, the riskof thrombosis was considered to be very low. Incontrast, our experience and that of others suggestthat BPVT is not uncommon (6,7,13,14). Butnaru et al.(6) retrospectively reviewed TEEs of 149 patients whounderwent mitral BPV implantation at a single centerand identified BPVT in 9 patients (6%). The indicationfor TEE was prosthesis dysfunction suspected onTTE, and the mean time interval from implantation toTEE diagnosis was 12 months. The diagnosis of BPVTwas confirmed by pathology in 3 patients who un-derwent reoperation and by resolution of prosthesisdysfunction in the other 6 patients treated with VKA.Similarly, Oliver et al. (7) reviewed TEEs of 161 pa-tients with mitral BPV dysfunction and identified10 cases of BPVT (6.2%). The time interval fromimplantation to TEE diagnosis was 83 months in

TABLE 3 Echocardiographic Characteristics*
BPVT(n ¼ 41)
SVF(n ¼ 83) p Value
Mean gradient, mm Hg
Aortic 52 � 18 38 � 16 <0.001
Mitral 14 � 9 11 � 3 0.37
Tricuspid 9 � 4 11 � 4 0.34
Pulmonic — 34 � 6 —
LVEF, %
Aortic 60 � 11 55 � 10 0.06
Mitral 52 � 12 55 � 7 0.48
Tricuspid 53 � 7 53 � 14 0.94
Pulmonic — 66 � 1 —
Regurgitation > moderate
Aortic 7 (24) 37 (64) <0.001
Mitral 2 (22) 11 (61) 0.056
Tricuspid 7 (100) 14 (100) —
Pulmonic 1 (100) 2 (100)
Leaflet thickness <0.001
Normal 5 (12) 57 (69)
Thickened† 36 (88) 26 (31)
Leaflet motion <0.001
Normal 6 (15) 42 (51)
Restricted/immobile 35 (85) 41 (49)
Possible thrombus <0.001
No 29 (71) 83 (100)
SEC/possible ICT 12 (29) 0 (0)
Calcification/pannus <0.001
Yes 10 (24) 64 (77)
No 31 (76) 19 (23)
Values are mean� SD or n (%). *Digital images available included 94 transthoracicechocardiogram and 108 transesophageal echocardiogram studies from 41 (89%)BPVT patients and 83 (90%) SVF patients. †Defined as leaflet thickness >2 mm orsignificantly thicker compared to baseline echocardiogram.
ICT ¼ intracardiac thrombus; LVEF ¼ left ventricular ejection fraction;SEC ¼ spontaneous echo contrast; other abbreviations as in Table 1.
Egbe et al. J A C C V O L . 6 6 , N O . 2 1 , 2 0 1 5
Predictors of Bioprosthetic Valve Thrombosis D E C E M B E R 1 , 2 0 1 5 : 2 2 8 5 – 9 4
2290
their series. The diagnosis of BPVT was confirmed bypathology in 3 of their patients who underwentreoperation and by resolution of clinical and echo-cardiographic features of thrombosis after VKA anti-coagulation in the other 7 patients (7). Our studyshowed that BPVT was present in 11.6% of allexplanted BPV and in 12.7% of BPV in the mitralposition. The median duration from the time ofimplantation to explantation was 24 months for ourentire BPVT cohort and 31 months for mitral BPVT.We defined BPVT based on pathological diagnosiswhile Butnaru et al. (6) and Oliver et al. (7) definedBPVT based on echocardiographic diagnosis, whichmight have resulted in underestimation of the trueincidence of BPVT in their cohorts because of misseddiagnosis. Our result is consistent with BPVT preva-lence of 10% to 11% reported in other pathology seriesof BPV explanted at surgery or autopsy (15,16).
A surgical study from our institution reported 8cases of BPVT in the aortic position among 4,568 aortic
BPV implantations (incidence of 0.18%), with signifi-cantly higher incidence in porcine valves compared topericardial valves (13). In that study, Brown et al. (13)identified cases of BPVT by chart review of all pa-tients who underwent reoperation for aortic BPV fail-ure within 2 years of implantation. Our study did notshow any significant difference in BPVT occurrence byprosthesis position or prosthesis type. The mediantime to explantation in our cohort was 24 months with50% of prostheses explanted more than 2 years fromthe time of initial implantation. The lower incidencerate reported by Brown et al. (13) may be because theirstudy design did not capture cases of BPVT thatoccurred more than 2 years after implantation.
RISK FACTORS AND PREDICTIVE MODEL FOR BPVT. Inour series, clinical and echocardiographic character-istics associated with increased risk of BPVT wereparoxysmal atrial fibrillation (AF), subtherapeuticINR for patients on VKA therapy, an increase in meantransvalvular gradient >50% above baseline valueswithin 5 years, increased cusp thickness, andabnormal/restricted cusp mobility. The 3 echocar-diographic features of BPVT were similar to thosedescribed in prior studies (5–7). Interestingly, persis-tent AF was not an independent risk factor for BPVT.Our data suggest that inadequate anticoagulation issignificant in both persistent and paroxysmal AF.Most patients with paroxysmal AF in our cohort werenot anticoagulated and that might be the reason fortheir increased risk of BPVT, as shown in our multi-variate analysis.
Among our thrombosis cohort, the diagnosis ofBPVT was correctly made on the initial echocardio-gram in only a minority of patients (5% using TTE and13% using TEE). This highlights not only the difficultyin identifying BPVT using echocardiography, but alsosuggests a low level of awareness that BPVT mayoccur late after implantation. Based on our proposedrisk model, diagnosis of BPVT can be made with >70%sensitivity and >90% specificity in patients with 3 of 5independent risk factors listed above. By applyingthis risk model retrospectively among the 138 pa-tients included in our study, the diagnosis of BPVTwould have been considered in the majority of pa-tients in the case group, and the confirmatory crite-rion would be resolution of echocardiographicfindings and associated clinical improvement afterVKA therapy. Most likely some of these patients couldhave avoided reoperation.
Accurate diagnosis of BPVT is critical because thesepatients have been shown to respond very well toVKA (5–7,14). In a prior series from our institution, wecompared efficacy and safety of VKA (target INR of

FIGURE 2 Echocardiographic and Pathological Characteristics of BPVT and Structural Failure
The classical features of BPVT (top) are demonstrated in this TEE diastolic frame of a mitral BPVT (A), and confirmed on the explanted
specimen (B). Note the soft echodense material located in the BPV cusps, with restricted opening (arrow). While thrombus is more commonly
seen on the downstream aspect of the valve (ventricular side for mitral/tricuspid BPV, and arterial side for aortic/pulmonary BPV), in this
patient, thrombus was also present on the atrial side. Corresponding TEE diastolic frame (C) and pathology specimen (D) were taken from
a patient with structural bioprosthetic deterioration (bottom). Restricted leaflet opening is also present (arrow), but usually cusp thickening
is less prominent and more echodense. Note extensive pannus formation on the explanted valve. See accompanying Online Videos 1 and 2.
TEE ¼ transesophageal echocardiographic; other abbreviations as in Figure 1.
J A C C V O L . 6 6 , N O . 2 1 , 2 0 1 5 Egbe et al.D E C E M B E R 1 , 2 0 1 5 : 2 2 8 5 – 9 4 Predictors of Bioprosthetic Valve Thrombosis
2291
2.0 to 3.0) to surgery/thrombolysis in 31 patients withBPVT diagnosis (5). The endpoint for efficacy wasimprovement in prosthetic gradient and New YorkHeart Association functional class, while the safetyendpoint was freedom from death and thromboem-bolic complications. VKA was similar to surgery/thrombolysis and there were no deaths or thrombo-embolic complications in either cohort. Similarly,other series have also demonstrated resolution in88% to 100% of patients with BPVT in the mitralposition after anticoagulation with VKA for 4 to 14weeks (6,7). Data from a Danish registry showed thatprophylactic anticoagulation with VKA beyond6 months post-implantation of BPV in the aorticposition is associated with decreased thromboem-bolic events and cardiovascular death without a sig-nificant increase in bleeding; this may be relatedto BPVT prevention (17). This observation led to achange in the 2014 ACC/AHA guidelines, which now
recommend 3 to 6 months of VKA anticoagulationafter aortic BPV implantation.
ESTIMATING INCIDENCE OF BPVT. Given the retro-spective nature of our study, the true incidence ofBPVT cannot accurately be determined. Whencomparing reoperation due to bioprosthetic throm-bosis to the total number of bioprosthetic valve im-plantations during the study period, BPVT incidenceappears relatively low: 0.74% to 1.46% (46 BPVT casescompared to a total 6,178 implantations, or to 3,161patients who had at least 1 follow-up at the MayoClinic after initial implantation, respectively). How-ever, this clearly underestimates the true incidence,as BPVT patients successfully treated with anti-coagulation avoided surgery and, thus, are notcaptured in this study.
In a previous report we identified another 15 BPVTpatients treated with anticoagulation alone in a

TABLE 4 Predictors of BPVT
Univariate Multivariate
Odds Ratio (95% CI) p Value Odds Ratio (95% CI) p Value
Clinical factors
Paroxysmal AF 3.74 (2.43-3.81) 0.001 5.19 (1.42-21.77) 0.01
Perioperative AF 1.04 (0.22-2.19) 0.54
Persistent AF 2.34 (0.43-6.22) 0.12
Persistent AF with subtherapeutic INR 1.66 (1.26-2.17) 0.001 3.44 (0.78-11.13) 0.72
Prior thromboembolic events 1.01 (0.31-5.14) 0.09
Hypertension 1.62 (0.66-3.89) 0.42
Diabetes 1.83 (0.26-2.21) 0.13
CAD 1.52 (0.66-3.89) 0.42
Post-operative use of APA 0.81 (0.62-3.03) 0.36
Post-operative use of VKA 0.62 (0.25-1.84) 0.29
On VKA with subtherapeutic INR 3.91 (2.61-4.21) 0.001 7.37 (1.60-42.13) 0.001
Porcine prosthesis 1.62 (1.25-1.84) 0.06
Pericardial prosthesis 0.88 (0.61-1.021) 0.12
Echocardiographic indexes
50% increase in gradient within 5 yrs 2.04 (1.22-2.19) 0.007 12.7 (2.83-75.91) 0.001
Increased cusp thickness 6.37 (2.94-14.95) <0.001 12.2 (2.71-75.08) 0.001
Abnormal cusp mobility 3.89 (1.87-8.36) <0.001 6.94 (1.74-33.45) 0.005
Presence of calcification/pannus 0.81 (0.68-1.08) 0.05 0.66 (0.23-2.09) 0.42
ICT/SEC 4.47 (1.11-21.92) 0.03 2.78 (0.33-31.87) 0.35
CI ¼ confidence interval; other abbreviations as in Tables 1 and 3.
TABLE 5
Variables
A. 50%incre
B. Incre
C. Abno
D. Parox
E. Subth
Combinati
A and B
A, B, an
A, B, C,
A, B, C,
NPV ¼ negTable 1.
Egbe et al. J A C C V O L . 6 6 , N O . 2 1 , 2 0 1 5
Predictors of Bioprosthetic Valve Thrombosis D E C E M B E R 1 , 2 0 1 5 : 2 2 8 5 – 9 4
2292
similar time interval (5). Furthermore, both a lack ofclinical awareness and of set echocardiographicdiagnostic criteria for BPVT impacted our ability todetect this disease. Indeed, considering that theoriginal TTE and TEE reports reviewed for this seriesmentioned BPVT diagnosis in <15% of confirmedcases, a significant number of BPVT cases were clini-cally missed. Of note, recent data on computed to-mography evaluation post-transcatheter aortic valvereplacement suggests BPVT may be present in 4% ofpatients (18). Whether the true incidence of BPVT in
Test Performance Characteristics for the Diagnosis of BPVT
TotalScore
Sensitivity(%)
Specificity(%)
PPV(%)
NPV(%)
mean gradientase
1 45 89 68 77
ase cusp thickness 1 74 69 55 84
rmal cusp mobility 1 63 70 51 81
ysmal AF 1 63 73 54 80
erapeutic INR 1 30 92 67 73
on of variables
2 86 57 50 89
d C 3 72 90 78 87
and D 4 70 94 87 86
D, and E 5 66 93 85 89
ative predictive value; PPV ¼ positive predictive value; other abbreviations as in
the community will be as high as the 11.6% prevalenceamong patients requiring reoperation (46 BPVT for397 reoperations) remains to be determined in large,prospective trials.
CLINICAL IMPLICATIONS. The current ESC guide-lines for the management of valvular heart disease donot recommend VKA for BPV in the aortic positionbeyond the first 3 months, and both ESC and currentACC/AHA guidelines do not recommend VKA for BPVbeyond 3 months for mitral, tricuspid, and pulmonaryvalves (3,4). Additionally, routine TTE surveillance inthe absence of change in clinical status is not rec-ommended in patients with BPV until 10 years post-implantation (3,4).
Based on our results and experience we havechanged our practice and recommend the following:
1. Patients with BPV in any position who require VKAfor any indication such as AF or prior thrombo-embolic event should have their INR meticulouslymaintained between 2.0 and 3.0.
2. All patients with paroxysmal AF who receive BPVshould be on VKA for anticoagulation unlesscontraindicated.
3. Patients who present with BPV dysfunction, espe-cially when this is identified <5 years after im-plantation, should be meticulously evaluated forevidence of BPVT using the above-proposed riskmodel.

J A C C V O L . 6 6 , N O . 2 1 , 2 0 1 5 Egbe et al.D E C E M B E R 1 , 2 0 1 5 : 2 2 8 5 – 9 4 Predictors of Bioprosthetic Valve Thrombosis
2293
4. Patients who present with clinical and/or echo-cardiographic features of BPVT (and have no con-traindications to anticoagulant therapy) should beconsidered for a trial of VKA as initial therapyrather than being referred directly for valvereplacement.
5. Echocardiographic surveillance of BPV should beperformed within 12 months of cessation of VKA inhigh-risk patients.
PERSPECTIVES
COMPETENCY IN MEDICAL KNOWLEDGE: Thrombosis of
bioprosthetic heart valves can occur several years after implan-
tation. Likely predictors of this complication include a >50%
increase in mean echo-Doppler transvalvular gradient within
5 years, paroxysmal atrial fibrillation, subtherapeutic INR in
patients anticoagulated with vitamin K antagonists, increased
cusp thickness, and abnormal cusp mobility.
TRANSLATIONAL OUTLOOK: Additional studies are needed
to validate these predictors of thrombosis in broad populations
of patients with bioprosthetic valve dysfunction.
STUDY LIMITATIONS. First, this is a retrospectivestudy based on a cohort from a single tertiary center,which lends itself to potential bias. The cross-sectional study design makes it difficult to infercausality between associated risk factors and BPVT.There were 17 patients without baseline assessmentof transvalvular gradient at the time of BPV implan-tation. We determined the performance of our diag-nostic model in a highly selected population of 138explanted BPV; thus, it may not be representativeof the general population of patients with BPVdysfunction. Consequently, we anticipate that ourmodel may be less predictive in other populationsand a larger study is needed to prospectively validatethis model in the general population of patients withBPV dysfunction. Finally, the exact onset of BPVTis unknown, as prosthetic thrombosis certainlypreceded the time of explantation.
CONCLUSIONS
BPVT is not uncommon and can occur several yearsafter surgery. A combination of clinical and echocar-diographic features can reliably diagnose BPVT. It iscrucial to consider the diagnosis of BPVT beforereferring for reoperation because VKA therapy mayreverse the BPV dysfunction.
REPRINT REQUESTS AND CORRESPONDENCE: Dr.Sorin V. Pislaru, Division of Cardiovascular Diseases,Mayo Clinic, 200 First Street SW, Rochester, Minnesota55905. E-mail: [email protected].
RE F E RENCE S
1. Marchand M, Aupart M, Norton R, et al. Twelve-year experience with Carpentier-Edwards PERI-MOUNT pericardial valve in the mitral position: amulticenter study. J Heart Valve Dis 1998;7:292–8.
2. Valfre C, Ius P, Minniti G, et al. The fate ofHancock II porcine valve recipients 25 yearsafter implant. Eur J Cardiothorac Surg 2010;38:141–6.
3. Nishimura RA, Otto CM, Bonow RO, et al. 2014AHA/ACC guideline for the management ofpatients with valvular heart disease: executivesummary: a report of the American College ofCardiology/American Heart Association Task Forceon Practice Guidelines. J Am Coll Cardiol 2014;63:2438–88.
4. Vahanian A, Alfieri O, Andreotti F, et al.Guidelines on the management of valvular heartdisease (version 2012): the Joint Task Force onthe Management of Valvular Heart Diseaseof the European Society of Cardiology (ESC) andthe European Association for Cardio-ThoracicSurgery (EACTS). Eur J Cardiothorac Surg 2012;42:S1–44.
5. Pislaru SV, Hussain I, Pellikka PA, et al. Mis-conceptions, diagnostic challenges and treatmentopportunities in bioprosthetic valve thrombosis:
lessons from a case series. Eur J Cardiothorac Surg2015;47:725–32.
6. Butnaru A, Shaheen J, Tzivoni D, Tauber R,Bitran D, Silberman S. Diagnosis and treatment ofearly bioprosthetic malfunction in the mitral valveposition due to thrombus formation. Am J Cardiol2013;112:1439–44.
7. Oliver JM, Gallego P, Gonzalez A, et al. Bio-prosthetic mitral valve thrombosis: clinical profile,transesophageal echocardiographic features, andfollow-up after anticoagulant therapy. J Am SocEchocardiogr 1996;9:691–9.
8. Jander N, Kienzle RP, Kayser G, Neumann FJ,Gohlke-Baerwolf C, Minners J. Usefulness ofphenprocoumon for the treatment ofobstructing thrombus in bioprostheses in theaortic valve position. Am J Cardiol 2012;109:257–62.
9. Pislaru SV, Pellikka PA, Schaff HV, Connolly HM.Bioprosthetic valve thrombosis: the eyes will notsee what the mind does not know. J Thorac Car-diovasc Surg 2015;149:e86–7.
10. Zoghbi WA, Chambers JB, Dumesnil JG, et al.Recommendations for evaluation of prostheticvalves with echocardiography and doppler ultra-sound: a report From the American Society ofEchocardiography’s Guidelines and Standards
Committee and the Task Force on ProstheticValves. Am Soc Echocardiogr 2009;22:975–1014;quiz 1082�4.
11. Blauwet LA, Danielson GK, Burkhart HM, et al.Comprehensive echocardiographic assessment ofthe hemodynamic parameters of 285 tricuspidvalve bioprostheses early after implantation.J Am Soc Echocardiogr 2010;23:1045–59, 1059e1�2.
12. DeLong ER, DeLong DM, Clarke-Pearson DL.Comparing the areas under two or more correlatedreceiver operating characteristic curves: anonparametric approach. Biometrics 1988;44:837–45.
13. Brown ML, Park SJ, Sundt TM, Schaff HV. Earlythrombosis risk in patients with biologic valves inthe aortic position. J Thorac Cardiovasc Surg 2012;144:108–11.
14. Jander N, Sommer H, Pingpoh C, et al. Theporcine valve type predicts obstructive thrombosisbeyond the first three postoperative months inbioprostheses in the aortic position. Int J Cardiol2015;199:90–5.
15. Thiene G, Bortolotti U, Panizzon G, Milano A,Gallucci V. Pathological substrates of thrombusformation after heart valve replacement with the

Egbe et al. J A C C V O L . 6 6 , N O . 2 1 , 2 0 1 5
Predictors of Bioprosthetic Valve Thrombosis D E C E M B E R 1 , 2 0 1 5 : 2 2 8 5 – 9 4
2294
Hancock bioprosthesis. J Thorac Cardiovasc Surg1980;80:414–23.
16. Zeien LB, Klatt EC. Cardiac valve prosthesesat autopsy. Arch Pathol Lab Med 1990;114:933–7.
17. Merie C, Kober L, Skov Olsen P, et al.Association of warfarin therapy duration afterbioprosthetic aortic valve replacement with
risk of mortality, thromboembolic com-plications, and bleeding. JAMA 2012;308:2118–25.
18. Leetmaa T, Hansson NC, Leipsic J, et al. Earlyaortic transcatheter heart valve thrombosis:diagnostic value of contrast-enhanced multi-detector computed tomography. Circ CardiovascInterv 2015;8:e001596.
KEY WORDS atrial fibrillation, cusp,Doppler gradient, valvular heart disease,vitamin K antagonist
APPENDIX For the accompanying videos,please see the online version of this article.