
Biomechanical comparison of two different locking plates ... · Available online xxx abstract...
7
Original Article Biomechanical comparison of two different locking plates for open wedge high tibial osteotomy Nienke van Egmond a, * , Dennis Janssen b , Gerjon Hannink b , Nico Verdonschot b, c , Albert van Kampen a a Department of Orthopaedics, Radboud University Medical Centre, P.O. Box 9101, 6500 HB Nijmegen, The Netherlands b Orthopaedic Research Laboratory, Radboud University Medical Center, P.O. Box 9101, 6500 HB Nijmegen, The Netherlands c Laboratory of Biomechanical Engineering, University of Twente, P.O. Box 217, 7500 AE Enschede, The Netherlands article info Article history: Received 9 December 2016 Received in revised form 11 August 2017 Accepted 17 September 2017 Available online xxx abstract Background: The purpose of this study was to compare the mechanical stability of a relatively thin locking plate (FlexitSystem implant) with a relatively firm locking plate (TomoFix implant), both used for opening wedge high tibial osteotomy. Methods: Seven fresh frozen paired human cadaveric tibiae were used. The opening wedge high tibial osteotomies in the left tibiae were fixated with the FlexitSystem implant and in the right tibiae with the TomoFix implant. The tibiae were CT-scanned to determine the bone mineral density. Axial loading was applied in a cyclic fashion for 50,000 cycles. We compared throughout the loading history the relative motions between the proximal and distal tibia using roentgen stereophotogrammetry analysis at set intervals. Also the strength of the reconstructions was compared using a displacement-controlled compressive test until failure. Results: One pair (with the lowest bone mineral density) failed during the preparation of the osteotomy. The FlexitSystem implant displayed a similar stability compared to the TomoFix implant, with low translations (mean 2.16 ± 1.02 mm vs. 4.29 ± 5.66 mm) and rotations (mean 3.17 ± 2.04 vs. 4.30 ± 6.78 ), which was not significant different. Although on average the FlexitSystem reconstructions were slightly stronger than the Tomofix reconstructions (mean 4867 ± 944 N vs. 4628 ± 1987 N), no significant (p ¼ 0.71) differences between the two implants were found. Conclusion: From a biomechanical point of view, the FlexitSystem implant is a suitable alternative to the TomoFix implant for a high tibial open wedge osteotomy. © 2017 The Japanese Orthopaedic Association. Published by Elsevier B.V. All rights reserved. 1. Introduction Patients with knee osteoarthritis (OA) of the medial compart- ment often have a varus leg alignment which causes an overload of the medial compartment. Malalignment increases the risk for progression of knee OA and is associated with a decline in physical function and progression of pain [1e3]. In order to unload the medial compartment, a valgus high tibial osteotomy is the treat- ment of choice for the young and active patient [4]. The most commonly used techniques include closed-wedge osteotomy (CWO) and open-wedge osteotomy (OWO) [5,6]. The disadvantages of a lateral closed wedge osteotomy are the need for a fibular osteotomy, the high rate of tibial neuropathies, peroneal neuropathies, bone stock loss, and a more demanding subsequent total knee arthroplasty [6]. On the other hand, OWO has been associated with high non-union rates and loss of correction due to unstable fixation [6,7]. Therefore, fixation strength and mainte- nance of stability until osseous consolidation are a prerequisite of the implants used in OWO [8]. Several implants have been designed for OWO [8e11]. The TomoFix implant (Fig. 1) is widely used because of its well-reported clinical [5,12,13] and biomechanical [9,11,14] track record. The TomoFix implant is a long and rigid ti- tanium plate with locking screws, which functions as an internal fixator [8]. Due to its size, the disadvantages of this implant have been reported to be local irritation and wound healing problems [15e18]. Therefore, implant removal after surgery is often needed [18]. The FlexitSystem implant (Fig. 1) is a novel implant to be used for OWO. The FlexitSystem implant is shorter and thinner * Corresponding author. Fax: þ31 24 3540230. E-mail address: [email protected] (N. van Egmond). Contents lists available at ScienceDirect Journal of Orthopaedic Science journal homepage: http://www.elsevier.com/locate/jos https://doi.org/10.1016/j.jos.2017.09.014 0949-2658/© 2017 The Japanese Orthopaedic Association. Published by Elsevier B.V. All rights reserved. Journal of Orthopaedic Science xxx (2017) 1e7 Please cite this article in press as: van Egmond N, et al., Biomechanical comparison of two different locking plates for open wedge high tibial osteotomy, Journal of Orthopaedic Science (2017), https://doi.org/10.1016/j.jos.2017.09.014
Transcript of Biomechanical comparison of two different locking plates ... · Available online xxx abstract...

Original Article
Biomechanical comparison of two different locking plates for openwedge high tibial osteotomy
Nienke van Egmond a, *, Dennis Janssen b, Gerjon Hannink b, Nico Verdonschot b, c,Albert van Kampen a
a Department of Orthopaedics, Radboud University Medical Centre, P.O. Box 9101, 6500 HB Nijmegen, The Netherlandsb Orthopaedic Research Laboratory, Radboud University Medical Center, P.O. Box 9101, 6500 HB Nijmegen, The Netherlandsc Laboratory of Biomechanical Engineering, University of Twente, P.O. Box 217, 7500 AE Enschede, The Netherlands
a r t i c l e i n f o
Article history:Received 9 December 2016Received in revised form11 August 2017Accepted 17 September 2017Available online xxx
a b s t r a c t
Background: The purpose of this study was to compare the mechanical stability of a relatively thinlocking plate (FlexitSystem implant) with a relatively firm locking plate (TomoFix implant), both used foropening wedge high tibial osteotomy.Methods: Seven fresh frozen paired human cadaveric tibiae were used. The opening wedge high tibialosteotomies in the left tibiae were fixated with the FlexitSystem implant and in the right tibiae with theTomoFix implant. The tibiae were CT-scanned to determine the bone mineral density. Axial loading wasapplied in a cyclic fashion for 50,000 cycles. We compared throughout the loading history the relativemotions between the proximal and distal tibia using roentgen stereophotogrammetry analysis at setintervals. Also the strength of the reconstructions was compared using a displacement-controlledcompressive test until failure.Results: One pair (with the lowest bone mineral density) failed during the preparation of the osteotomy.The FlexitSystem implant displayed a similar stability compared to the TomoFix implant, with lowtranslations (mean 2.16 ± 1.02 mm vs. 4.29 ± 5.66 mm) and rotations (mean 3.17 ± 2.04! vs. 4.30 ± 6.78!),which was not significant different. Although on average the FlexitSystem reconstructions were slightlystronger than the Tomofix reconstructions (mean 4867 ± 944 N vs. 4628 ± 1987 N), no significant(p ¼ 0.71) differences between the two implants were found.Conclusion: From a biomechanical point of view, the FlexitSystem implant is a suitable alternative to theTomoFix implant for a high tibial open wedge osteotomy.
© 2017 The Japanese Orthopaedic Association. Published by Elsevier B.V. All rights reserved.
1. Introduction
Patients with knee osteoarthritis (OA) of the medial compart-ment often have a varus leg alignment which causes an overload ofthe medial compartment. Malalignment increases the risk forprogression of knee OA and is associated with a decline in physicalfunction and progression of pain [1e3]. In order to unload themedial compartment, a valgus high tibial osteotomy is the treat-ment of choice for the young and active patient [4].
The most commonly used techniques include closed-wedgeosteotomy (CWO) and open-wedge osteotomy (OWO) [5,6]. Thedisadvantages of a lateral closed wedge osteotomy are the need for
a fibular osteotomy, the high rate of tibial neuropathies, peronealneuropathies, bone stock loss, and a more demanding subsequenttotal knee arthroplasty [6]. On the other hand, OWO has beenassociated with high non-union rates and loss of correction due tounstable fixation [6,7]. Therefore, fixation strength and mainte-nance of stability until osseous consolidation are a prerequisite ofthe implants used in OWO [8]. Several implants have been designedfor OWO [8e11]. The TomoFix implant (Fig. 1) is widely usedbecause of its well-reported clinical [5,12,13] and biomechanical[9,11,14] track record. The TomoFix implant is a long and rigid ti-tanium plate with locking screws, which functions as an internalfixator [8]. Due to its size, the disadvantages of this implant havebeen reported to be local irritation and wound healing problems[15e18]. Therefore, implant removal after surgery is often needed[18]. The FlexitSystem implant (Fig. 1) is a novel implant to be usedfor OWO. The FlexitSystem implant is shorter and thinner
* Corresponding author. Fax: þ31 24 3540230.E-mail address: [email protected] (N. van Egmond).
Contents lists available at ScienceDirect
Journal of Orthopaedic Science
journal homepage: http: / /www.elsevier .com/locate / jos
https://doi.org/10.1016/j.jos.2017.09.0140949-2658/© 2017 The Japanese Orthopaedic Association. Published by Elsevier B.V. All rights reserved.
Journal of Orthopaedic Science xxx (2017) 1e7
Please cite this article in press as: van Egmond N, et al., Biomechanical comparison of two different locking plates for open wedge high tibialosteotomy, Journal of Orthopaedic Science (2017), https://doi.org/10.1016/j.jos.2017.09.014
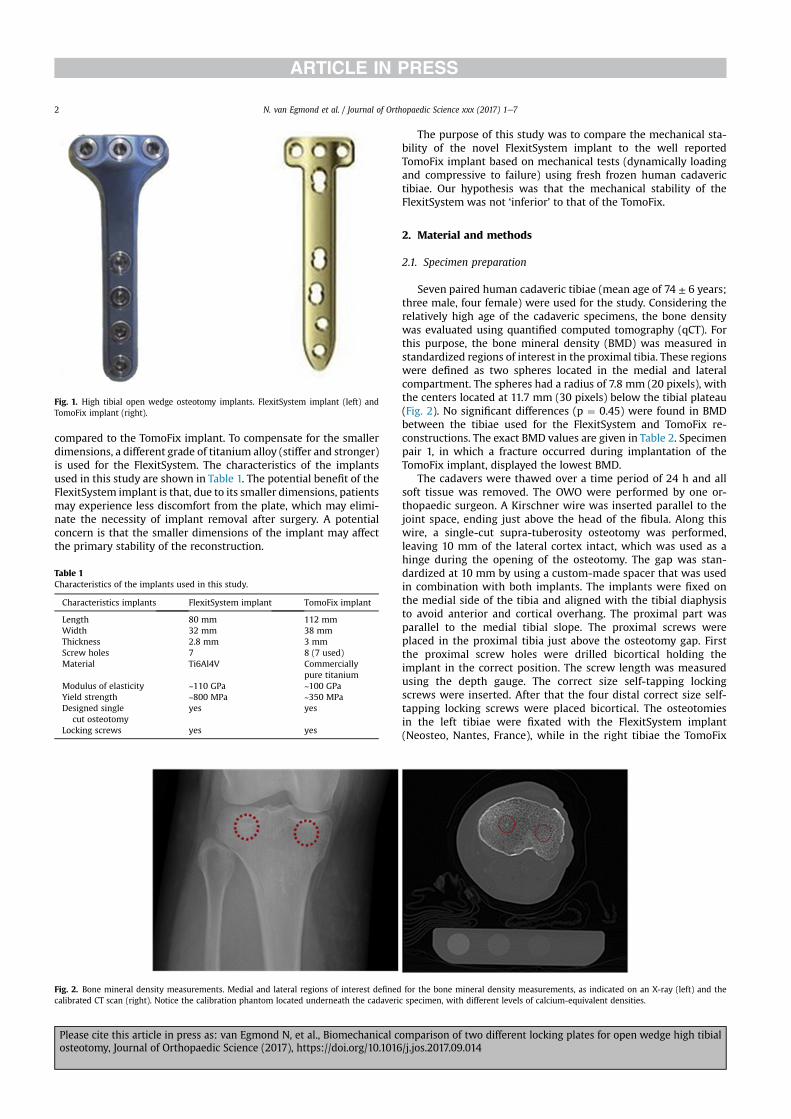
compared to the TomoFix implant. To compensate for the smallerdimensions, a different grade of titanium alloy (stiffer and stronger)is used for the FlexitSystem. The characteristics of the implantsused in this study are shown in Table 1. The potential benefit of theFlexitSystem implant is that, due to its smaller dimensions, patientsmay experience less discomfort from the plate, which may elimi-nate the necessity of implant removal after surgery. A potentialconcern is that the smaller dimensions of the implant may affectthe primary stability of the reconstruction.
The purpose of this study was to compare the mechanical sta-bility of the novel FlexitSystem implant to the well reportedTomoFix implant based on mechanical tests (dynamically loadingand compressive to failure) using fresh frozen human cadaverictibiae. Our hypothesis was that the mechanical stability of theFlexitSystem was not ‘inferior’ to that of the TomoFix.
2. Material and methods
2.1. Specimen preparation
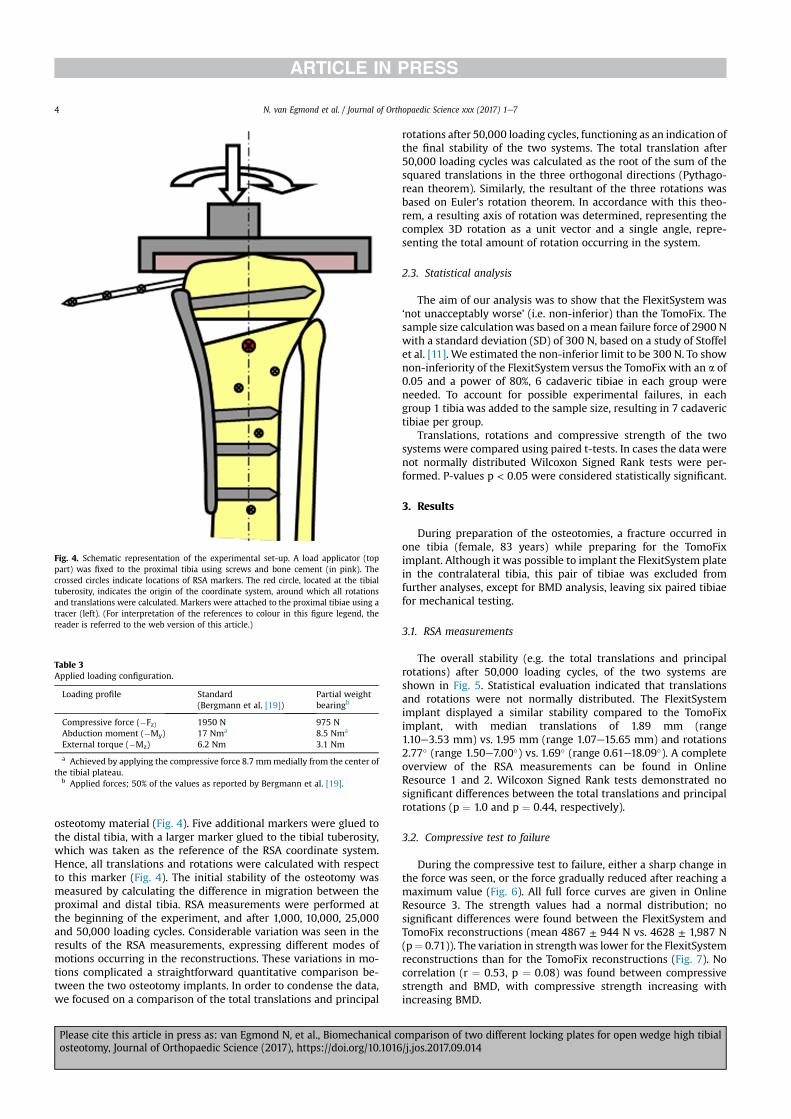
Seven paired human cadaveric tibiae (mean age of 74 ± 6 years;three male, four female) were used for the study. Considering therelatively high age of the cadaveric specimens, the bone densitywas evaluated using quantified computed tomography (qCT). Forthis purpose, the bone mineral density (BMD) was measured instandardized regions of interest in the proximal tibia. These regionswere defined as two spheres located in the medial and lateralcompartment. The spheres had a radius of 7.8 mm (20 pixels), withthe centers located at 11.7 mm (30 pixels) below the tibial plateau(Fig. 2). No significant differences (p ¼ 0.45) were found in BMDbetween the tibiae used for the FlexitSystem and TomoFix re-constructions. The exact BMD values are given in Table 2. Specimenpair 1, in which a fracture occurred during implantation of theTomoFix implant, displayed the lowest BMD.
The cadavers were thawed over a time period of 24 h and allsoft tissue was removed. The OWO were performed by one or-thopaedic surgeon. A Kirschner wire was inserted parallel to thejoint space, ending just above the head of the fibula. Along thiswire, a single-cut supra-tuberosity osteotomy was performed,leaving 10 mm of the lateral cortex intact, which was used as ahinge during the opening of the osteotomy. The gap was stan-dardized at 10 mm by using a custom-made spacer that was usedin combination with both implants. The implants were fixed onthe medial side of the tibia and aligned with the tibial diaphysisto avoid anterior and cortical overhang. The proximal part wasparallel to the medial tibial slope. The proximal screws wereplaced in the proximal tibia just above the osteotomy gap. Firstthe proximal screw holes were drilled bicortical holding theimplant in the correct position. The screw length was measuredusing the depth gauge. The correct size self-tapping lockingscrews were inserted. After that the four distal correct size self-tapping locking screws were placed bicortical. The osteotomiesin the left tibiae were fixated with the FlexitSystem implant(Neosteo, Nantes, France), while in the right tibiae the TomoFix
Fig. 1. High tibial open wedge osteotomy implants. FlexitSystem implant (left) andTomoFix implant (right).
Table 1Characteristics of the implants used in this study.
Characteristics implants FlexitSystem implant TomoFix implant
Length 80 mm 112 mmWidth 32 mm 38 mmThickness 2.8 mm 3 mmScrew holes 7 8 (7 used)Material Ti6Al4V Commercially
pure titaniumModulus of elasticity ~110 GPa ~100 GPaYield strength ~800 MPa ~350 MPaDesigned single
cut osteotomyyes yes
Locking screws yes yes
Fig. 2. Bone mineral density measurements. Medial and lateral regions of interest defined for the bone mineral density measurements, as indicated on an X-ray (left) and thecalibrated CT scan (right). Notice the calibration phantom located underneath the cadaveric specimen, with different levels of calcium-equivalent densities.
N. van Egmond et al. / Journal of Orthopaedic Science xxx (2017) 1e72
Please cite this article in press as: van Egmond N, et al., Biomechanical comparison of two different locking plates for open wedge high tibialosteotomy, Journal of Orthopaedic Science (2017), https://doi.org/10.1016/j.jos.2017.09.014

implant (TomoFix Osteotomy system, DePuy Synthesis, WestChester, PA, USA) was used (Fig. 3).
After preparation of the osteotomy, the distal tibia was resectedand potted using polymethylmethacrylate (PMMA), at a level of30 mm distally to the lowest position of the TomoFix implant (thelongest plate of the two systems). The contralateral tibiae with theFlexitSystem implants were resected at the same level (Fig. 3). Next,a custom load applicator was attached to the proximal tibia, whichwas aligned perpendicular to the long axis of the tibia using agoniometer. The load applicator was fixed using four screws, afterwhich additional fixation was provided by potting the proximaltibiae using PMMA (Fig. 4). Care was taken that the osteotomyplates were not embedded in the cement. The custom load appli-cator was fixed perpendicularly to the tibial shaft.
2.2. Mechanical testing
The reconstructions were subjected to a loading regime repre-senting the forces occurring during the toe-off phase of normalwalking [19] (Table 3), which is the most frequent activity of daily
living, and is therefore representative of one of the most frequentloading configurations that were applied to the reconstruction.During this phase, the axial force acting on the tibia is at its peak,but also substantial moments of force are acting, forcing abductionand external rotation of the tibia. The load applicator attached tothe proximal tibia was specifically designed to apply this complexloading condition. It allowed loading at an offset of 8.7 mm. For thispurpose, the proximal tibia was placed in the applicator with theintercondylar eminence aligned with the center of the load appli-cator. The compressive force was applied through the linear actu-ator of the mechanical testing system (MTS Systems, Eden Prairie,MN, USA). An abduction moment was accounted for by applyingthe force medially from the center of the tibia. External torque wasapplied through a separate air power driven actuator, attached to alever arm of the load applicator (Fig. 3). This actuator was syn-chronized with the linear actuator of the mechanical testing sys-tem, and cyclically activated in an alternating fashion. To simulatepartial weight bearing of a patient immediately after surgery, theapplied forces were scaled down to 50% [9] of the values as reportedby Bergmann et al. [19]. The resulting loading configuration appliedto the constructs is given in Table 3.
The loading regimewas applied for 50,000 cycles, at a frequencyof 2 Hz (ca. 7 h of testing), representing approximately 2e3 weeksof normal functioning after surgery [20]. A frequency of 2 Hz waschosen to prevent the formation of fatigue damage in the bonetissue [9].
After completion of this loading history, a displacement-controlled crush test was performed, at a speed of 5.0 mm/min[21]. The maximum load measured during this test served as ameasure for the strength of the reconstruction.
The stability of the reconstructionwas evaluated using roentgenstereophotogrammetry analysis (RSA). Six tantalum markers wereattached to the proximal part of the osteotomy using plastic tracers,to ensure they were not obscured by the load applicator and
Table 2Averaged bone mineral density in the tested specimens.
Specimen Sex Age BMD (mg/cm3)FlexitSystem
BMD (mg/cm3)TomoFix
1a Female 83 51.07 18.252 Female 67 72.74 84.453 Female 78 85.52 115.044 Male 77 99.19 145.095 Male 70 152.83 129.046 Female 68 101.87 119.107 Male 70 126.59 139.28
BMD Bone mineral density.a Fracture occurred during implantation, not included in experimental testing.
Fig. 3. Tibial osteotomies with the implants. Tibial osteotomies with the TomoFix (left) and FlexitSystem (right) implants. Notice the plastic tracers attached to the proximal tibia,containing tantalum roentgen stereophotogrammetry analysis (RSA) markers.
N. van Egmond et al. / Journal of Orthopaedic Science xxx (2017) 1e7 3
Please cite this article in press as: van Egmond N, et al., Biomechanical comparison of two different locking plates for open wedge high tibialosteotomy, Journal of Orthopaedic Science (2017), https://doi.org/10.1016/j.jos.2017.09.014
osteotomy material (Fig. 4). Five additional markers were glued tothe distal tibia, with a larger marker glued to the tibial tuberosity,which was taken as the reference of the RSA coordinate system.Hence, all translations and rotations were calculated with respectto this marker (Fig. 4). The initial stability of the osteotomy wasmeasured by calculating the difference in migration between theproximal and distal tibia. RSA measurements were performed atthe beginning of the experiment, and after 1,000, 10,000, 25,000and 50,000 loading cycles. Considerable variation was seen in theresults of the RSA measurements, expressing different modes ofmotions occurring in the reconstructions. These variations in mo-tions complicated a straightforward quantitative comparison be-tween the two osteotomy implants. In order to condense the data,we focused on a comparison of the total translations and principal
rotations after 50,000 loading cycles, functioning as an indication ofthe final stability of the two systems. The total translation after50,000 loading cycles was calculated as the root of the sum of thesquared translations in the three orthogonal directions (Pythago-rean theorem). Similarly, the resultant of the three rotations wasbased on Euler's rotation theorem. In accordance with this theo-rem, a resulting axis of rotation was determined, representing thecomplex 3D rotation as a unit vector and a single angle, repre-senting the total amount of rotation occurring in the system.
2.3. Statistical analysis
The aim of our analysis was to show that the FlexitSystem was‘not unacceptably worse’ (i.e. non-inferior) than the TomoFix. Thesample size calculationwas based on a mean failure force of 2900 Nwith a standard deviation (SD) of 300 N, based on a study of Stoffelet al. [11]. We estimated the non-inferior limit to be 300 N. To shownon-inferiority of the FlexitSystem versus the TomoFix with an a of0.05 and a power of 80%, 6 cadaveric tibiae in each group wereneeded. To account for possible experimental failures, in eachgroup 1 tibia was added to the sample size, resulting in 7 cadaverictibiae per group.
Translations, rotations and compressive strength of the twosystems were compared using paired t-tests. In cases the data werenot normally distributed Wilcoxon Signed Rank tests were per-formed. P-values p < 0.05 were considered statistically significant.
3. Results
During preparation of the osteotomies, a fracture occurred inone tibia (female, 83 years) while preparing for the TomoFiximplant. Although it was possible to implant the FlexitSystem platein the contralateral tibia, this pair of tibiae was excluded fromfurther analyses, except for BMD analysis, leaving six paired tibiaefor mechanical testing.
3.1. RSA measurements
The overall stability (e.g. the total translations and principalrotations) after 50,000 loading cycles, of the two systems areshown in Fig. 5. Statistical evaluation indicated that translationsand rotations were not normally distributed. The FlexitSystemimplant displayed a similar stability compared to the TomoFiximplant, with median translations of 1.89 mm (range1.10e3.53 mm) vs. 1.95 mm (range 1.07e15.65 mm) and rotations2.77! (range 1.50e7.00!) vs. 1.69! (range 0.61e18.09!). A completeoverview of the RSA measurements can be found in OnlineResource 1 and 2. Wilcoxon Signed Rank tests demonstrated nosignificant differences between the total translations and principalrotations (p ¼ 1.0 and p ¼ 0.44, respectively).
3.2. Compressive test to failure
During the compressive test to failure, either a sharp change inthe force was seen, or the force gradually reduced after reaching amaximum value (Fig. 6). All full force curves are given in OnlineResource 3. The strength values had a normal distribution; nosignificant differences were found between the FlexitSystem andTomoFix reconstructions (mean 4867 ± 944 N vs. 4628 ± 1,987 N(p¼ 0.71)). The variation in strength was lower for the FlexitSystemreconstructions than for the TomoFix reconstructions (Fig. 7). Nocorrelation (r ¼ 0.53, p ¼ 0.08) was found between compressivestrength and BMD, with compressive strength increasing withincreasing BMD.
Table 3Applied loading configuration.
Loading profile Standard(Bergmann et al. [19])
Partial weightbearingb
Compressive force ($Fz) 1950 N 975 NAbduction moment ($My) 17 Nma 8.5 Nma
External torque ($Mz) 6.2 Nm 3.1 Nm
a Achieved by applying the compressive force 8.7 mmmedially from the center ofthe tibial plateau.
b Applied forces; 50% of the values as reported by Bergmann et al. [19].
Fig. 4. Schematic representation of the experimental set-up. A load applicator (toppart) was fixed to the proximal tibia using screws and bone cement (in pink). Thecrossed circles indicate locations of RSA markers. The red circle, located at the tibialtuberosity, indicates the origin of the coordinate system, around which all rotationsand translations were calculated. Markers were attached to the proximal tibiae using atracer (left). (For interpretation of the references to colour in this figure legend, thereader is referred to the web version of this article.)
N. van Egmond et al. / Journal of Orthopaedic Science xxx (2017) 1e74
Please cite this article in press as: van Egmond N, et al., Biomechanical comparison of two different locking plates for open wedge high tibialosteotomy, Journal of Orthopaedic Science (2017), https://doi.org/10.1016/j.jos.2017.09.014
3.3. Post-failure analyses
Radiographs of the reconstructions after the destructive testindicated that for both systems no damage occurred to the implantsor screws. After removal of the plates, the screw holes in theproximal tibia appeared to be oval-shaped, suggesting a collapse of
the proximal tibial bone, possibly due to fracturing of the lateralcortex, as the origin of failure of the reconstructions (Fig. 8).
4. Discussion
The results of the experiments showed that the FlexitSystemimplanthasa stability comparable to theTomoFix implant,whichhasawell-reported clinical and biomechanical track record. Openwedgehigh tibial osteotomy has been associatedwith high non-union ratesand loss of correction due to unstable fixation [6,7]. Therefore suffi-cient strength of the implants is very important. The FlexitSystemimplant displayed translations lower than 5mmand rotations lowerthan5!. The strengthof the FlexitSystemreconstructionswas slightlyhigher compared to the TomoFix reconstructions, although this dif-ference was not statistically significant.
As this is a novel implant, no previous studies comparing theFlexitSystem to other implants have beenperformed. The strength ofthe reconstructions as found in the current study in general is slightlyhigher than published in the literature. Agneskirchner et al. [9] re-ported a strength of 3069 N for a reconstruction with a TomoFiximplant in Sawbones. Stoffel et al. [11] compared the Puddu plate(modified Arthrex Osteotomy Plate) to the TomoFix plate, also insynthetic tibiae. Failure occurred after axial compression loading at amean load of 2537 N (Puddu plate) and 2904 N (TomoFix plate). TheTomoFix plate was also compared to the Aescular Plate and PudduPlate by Kim et al. [10]. The maximal loads at failure were6793.8 ± 499.8 N, 6055.1 ± 1184.7 N and 6798.2 ± 988.7 N, respec-tively. They used porcine bone and considered only axial loading,both could explain the higher maximal loads compared to our study.Evidently, there are differences between all these studies in terms ofthe type of bone used (synthetic or cadaveric, human or porcine),surgical approach (single- or bi-planar cuts), loading history andbrand and type of implants.
We found no differences in themagnitude of the failure load andfailure mechanism between the two implants. Post-failure analysisshowed oval-shaped screw holes, due to a collapse of the proximaltibial bone. This suggests compressive failure of the lateral tibia andfracturing of the trabecular bone surrounding the screws as theorigin of failure of the reconstructions. Fracturing of the lateralcortex as construct's failure is also seen in the literature [9,11,22].An intact lateral cortex is important for the stability of the osteot-omy [23]. Our results suggest that with an intact lateral cortex,partial axial loading postoperative in both implants, could betolerated.
0
5
10
15
20
TomoFix FlexitSystem
Tota
l tra
nsla
tion
[mm
]
0
5
10
15
20
TomoFix FlexitSystem
Prin
cipa
l rot
atio
n [°]
Fig. 5. Median total translation (left) and principal rotation (right) after 50,000 loading cycles. Boxes represent the 25th and 75th percentile, whiskers represent the minimal andmaximal values.
Fig. 7. Compressive strength of the reconstructions with the TomoFix and FlexitSystemimplants. The FlexitSystem implants had a slightly higher compressive strength, whichwas not significant.
Fig. 6. Example results of a compressive failure test (specimen 5). Both systems hadreconstructions that caused a reaction force displaying a sharp peak (TomoFix in thisparticular case), and specimens that displayed a gradual decrease in reaction forceafter reaching a maximum (FlexitSystem in this particular case).
N. van Egmond et al. / Journal of Orthopaedic Science xxx (2017) 1e7 5
Please cite this article in press as: van Egmond N, et al., Biomechanical comparison of two different locking plates for open wedge high tibialosteotomy, Journal of Orthopaedic Science (2017), https://doi.org/10.1016/j.jos.2017.09.014

When evaluating the biomechanical functionality of implantsfor OWO, obviously, the choice of the base material affects theoutcome of the investigation. The main advantage of using syn-thetic tibiae is that it minimizes the inter-specimen variability,making the results more reproducible [24,25]. Synthetic bones aredesigned such that they reproduce the structural biomechanicalresponse of the bone, such as the global stiffness of the bone. Adrawback of using such a material is that, although the globalbiomechanics are well-represented, the local interaction betweenthe screw and the bone is not. Hence, testing with actual humancadaveric tissue therefore may provide additional insights into theactual failure mechanisms that otherwise would have been missed.Moreover it provides more information about the relation betweenstrength of the reconstruction and bone quality. In the currentexperiments, the strength of the reconstructions with both im-plants decreased with BMD, suggesting that patient selection isimportant for the procedure, with a preference for younger, activepatients with an adequate bone stock, in line with previousreports [4].
Some limitations of our study should be discussed. First, the useof cadaveric tissue over synthetic tibiae could reduce the repro-ducibility [24,25]. To minimize the effect of inter-specimen varia-tion on the comparison between the implants, a paired study wasperformed comparing the left and right tibiae. Nonetheless, a sig-nificant amount of variation in translations and rotations was seen,of which the patterns could not be explained easily based on thelocal CT-based BMD measurements. Second, in the current studythe fourth proximal screw for the TomoFix systemwas not used, asit lines up with the osteotomy gap. In the current study, supra-tuberosity osteotomies with a single cut were created using bothsystems. The biplanar cut technique allows for the use of the fourthscrew. The biplanar cut and the additional screw for the TomoFixsystemmay increase the initial stability of the osteotomy. From thatpoint of view, one can consider the current experiments to repre-sent aworst case scenario for the Tomofix implant. One could arguethat, as the FlexitSystem implant does not facilitate a fourth prox-imal screw, the approach adopted in the current study provided afairer comparison of the two systems. Moreover, as the post-failureanalyses of the failure mechanisms indicated that the trabecularbone was crushed through the screws, rather than damage occur-ring to the screws or the connection between screws and implants,it is debatable whether the addition of the fourth screwwould haveprovided a significant increase to the strength of the reconstruc-tion. Third, the loading condition reported by Bergmann et al. [19],which evaluated the simulated loads during daily activities in pa-tients with TKA, were used. Obviously, there still are substantial
differences between an intact and a TKA reconstructed knee joint,but we tried to incorporate out-of-plane loads to apply a morerigorous loading regime, which may be more demanding on theosteotomy reconstruction compared with other experimentsdescribed in the literature [9e11]. Due to the pre-operative con-dition of the osteotomy patients the medial compartment will beoff-loaded after the osteotomy, restoring a more natural alignment.We aimed at representing loads occurring during such an align-ment by adopting loads of reconstructed patients. Moreover, byincreasing the wedge in an OWO the loads may indeed be shiftedfurther to the lateral compartment, which may be different fromthe loading configuration adopted here.
In conclusion, from a biomechanical point of view, the Flex-itSystem implant behaves similarly to the TomoFix implant. Bothsystems can be used to fixate a high tibial open wedge osteotomy.
Conflict of interest
The authors declare that they have no competing interests.
Funding
The authors declare that they have received research supportfrom Neosteo (Nantes, France) and DePuy Synthes Netherlands(Amersfoort, the Netherlands) for this study. The study sponsorsdid not have any involvement in the study design, collection, ana-lysing and interpretation of data; in the writing of the manuscript;and in the decision to submit the manuscript for publication.
Appendix A. Supplementary data
Supplementary data related to this article can be found athttps://doi.org/10.1016/j.jos.2017.09.014.
References
[1] Amis A. Biomechanics of High tibial osteotomy. Knee Surg Sports TraumatolArthrosc 2013 Jan;21(1):197e205.
[2] Andriacchi TP. Dynamics of knee malalignment. Orthop Clin North Am 1994Jul;25(3):395e403.
[3] Sharma L, Song J, Felson DT, September C, Shamiyeh E, Dunlop DD. The role ofknee alignment in disease progression and functional decline in knee osteo-arthritis. JAMA 2001 Jul 11;286(2):188e95.
[4] Iorio R, Healy WL. Unicompartmental arthritis of the knee. J Bone Jt Surg Am2003 Jul;85-A(7):1351e64.
[5] Bode G, von Heyden J, Pestka J, Schmal H, Salzmann G, Südkamp N,Niemeyer P. Prospective 5-year survival rate data following open-wedgevalgus high tibial osteotomy. Knee Surg Sports Traumatol Arthrosc 2015Jul;23(7):1949e55.
Fig. 8. Post-failure analysis, after removal of the proximal screws. Removal of the proximal screws revealed oval-shaped screw holes in the proximal tibiae, both for the TomoFix(left) and FlexitSystem (right) reconstructions, suggesting collapse of the proximal tibiae as a mode of failure during the destructive tests.
N. van Egmond et al. / Journal of Orthopaedic Science xxx (2017) 1e76
Please cite this article in press as: van Egmond N, et al., Biomechanical comparison of two different locking plates for open wedge high tibialosteotomy, Journal of Orthopaedic Science (2017), https://doi.org/10.1016/j.jos.2017.09.014

[6] Lee DC, Byun SJ. High tibial osteotomy. Knee Surg Relat Res 2002 Jun;24(2):61e9.[7] Lustig S, Scholes CJ, Costa AJ, Coolican MJ, Parker DA. Different changes in
slope between the medial and lateral tibial plateau after open-wedge hightibial osteotomy. Knee Surg Sports Traumatol Arthrosc 2013 Jan;21(1):32e8.
[8] Lobenhoffer P, Agneskirchner J, Zoch W. Die €offnende valgisierende Osteoto-mie der proximalen Tibia mit Fixation durch einen medialen Plattenfixateur.Orthop€ade 2004 Feb;33(2):153e60.
[9] Agneskirchner JD, Freiling D, Hurschler C, Lobenhoffer P. Primary stability offour different implants for opening wedge high tibial osteotomy. Knee SurgSports Traumatol Arthrosc 2006 Mar;14(3):291e300.
[10] Kim KJ, Song EK, Seon JK, Seol JH. Biomechanical study of the fixation platesfor opening wedge high tibial osteotomy. Knee Surg Relat Res 2015 Sep;27(3):181e6.
[11] Stoffel K, Stachowiak G, Kuster M. Open wedge high tibial osteotomy:biomechanical investigation of the modified Arthrex Osteotomy Plate (PudduPlate) and theTomoFix Plate. Clin Biomech 2004 Nov;19(9):944e50.
[12] Floerkemeier S, Staubli AE, Schroeter S, Goldhahn S, Lobenhoffer P. Outcomeafter high tibial open-wedge osteotomy: a retrospective evaluation of 533patients. Knee Surg Sports Traumatol Arthrosc 2013 Jan;21(1):170e80.
[13] Jung WH, Chun CW, Lee JH, Ha JH, Kim JH, Jeong JH. Comparative study ofmedial opening-wedge high tibial osteotomy using 2 different implants.Arthroscopy 2013 Jun;29(6):1063e71.
[14] Raja Izaham RM, Abdul Kadir MR, Abdul Rashid AH, Hossain MG, Kamarul T.Finite element analysis of Puddu and Tomofix plate fixation for open wedgehigh tibial osteotomy. Injury 2012 Jun;43(6):898e902.
[15] Miller BS, Downie B, McDonough EB, Wojtys EM. Complications after medialopening wedge high tibial osteotomy. Arthroscopy 2009 Jun;25(6):639e46.
[16] Niemeyer P, Schmal H, Hauschild O, von Heyden J, Südkamp NP, K€ostler W.Open-wedge osteotomy using an internal plate fixator in patients with
medial-compartment gonarthritis and varus malalignment: 3-year resultswith regard to preoperative arthroscopic and radiographic findings.Arthroscopy 2010 Dec;26(12):1607e16.
[17] Valkering KP, van den Bekerom MP, Kappelhoff FM, Albers GH. Complicationsafter Tomofix medial opening wedge high tibial osteotomy. J Knee Surg 2009Jul;22(3):218e25.
[18] Woodacre T, Ricketts M, Evans JT, Pavlou G, Schranz P, Hockings M, Toms A.Complications associated with opening wedge high tibial osteotomy e a re-view of the literature and of 15 years of experience. Knee 2016 Mar;23(2):276e82.
[19] Bergmann G, Bender A, Graichen F, Dymke J, Rohlmann A, Trepczynski A,Heller MO, Kutzner I. Standardized loads acting on knee implants. PLoS One2014 Jan 23;9(1):e86035.
[20] Morlock M, Schneider E, Bluhm A, Vollmer M, Bergmann G, Müller V, Honl M.Duration and frequency of everyday activities in total hip patients. J Biomech2011 Jul;34(7):873e81.
[21] Martinez de Albornoz P, Leyes M, Forriol F, Del Buono A, Maffulli N. Openingwedge high tibial osteotomy: plate position and biomechanics of the medialtibial plateau. Knee Surg Sports Traumatol Arthrosc 2014 Nov;22(11):2641e7.
[22] Spahn G, Wittig R. Primary stability of various implants in tibial openingwedge osteotomy: a biomechanical study. J Orthop Sci 2002;7(6):683e7.
[23] Flamme CH, Kohn D, Kirsch L, Hurschler C. Primary stability of different im-plants used in conjunction with high tibial osteotomy. Arch Orthop TraumaSurg 1999;119(7e8):450e5.
[24] Cristofolini L, Viceconti M. Mechanical validation of whole bone compositetibia models. J Biomech 2000 Mar;33(3):279e88.
[25] Heiner AD. Structural properties of fourth-generation composite femurs andtibias. J Biomech 2008 Nov 14;41(15):3282e4.
N. van Egmond et al. / Journal of Orthopaedic Science xxx (2017) 1e7 7
Please cite this article in press as: van Egmond N, et al., Biomechanical comparison of two different locking plates for open wedge high tibialosteotomy, Journal of Orthopaedic Science (2017), https://doi.org/10.1016/j.jos.2017.09.014






![Sport Utility Vehicle...Rated output1 (kW [HP] at rpm) XXX XXX XXX XXX XXX Acceleration from 0 to 100 km/h (s) XXX XXX XXX XXX XXX Top speed (km/h) XXX 3XXX XXX 3XXX XXX3 Fuel consumption4](https://static.fdocuments.in/doc/165x107/5e9ad03bae36bf4b5c045c78/sport-utility-vehicle-rated-output1-kw-hp-at-rpm-xxx-xxx-xxx-xxx-xxx-acceleration.jpg)











