BIOL 2402 Fluid/Electrolyte Regulation - Collin...
25
1 1 BIOL 2402 Fluid/Electrolyte Regulation Collin County Community College Dr. Chris Doumen 2 On average, we are 50 - 60 % water For a 70 kg male = 40 liters water This water is divided into • intracellular water ( 28 L) • extracellular water • plasma ( 3 L) • interstitial fluid ( 11 L) Body Water Content
Transcript of BIOL 2402 Fluid/Electrolyte Regulation - Collin...
1
1
BIOL 2402Fluid/Electrolyte Regulation
Collin County Community College
Dr. Chris Doumen
2
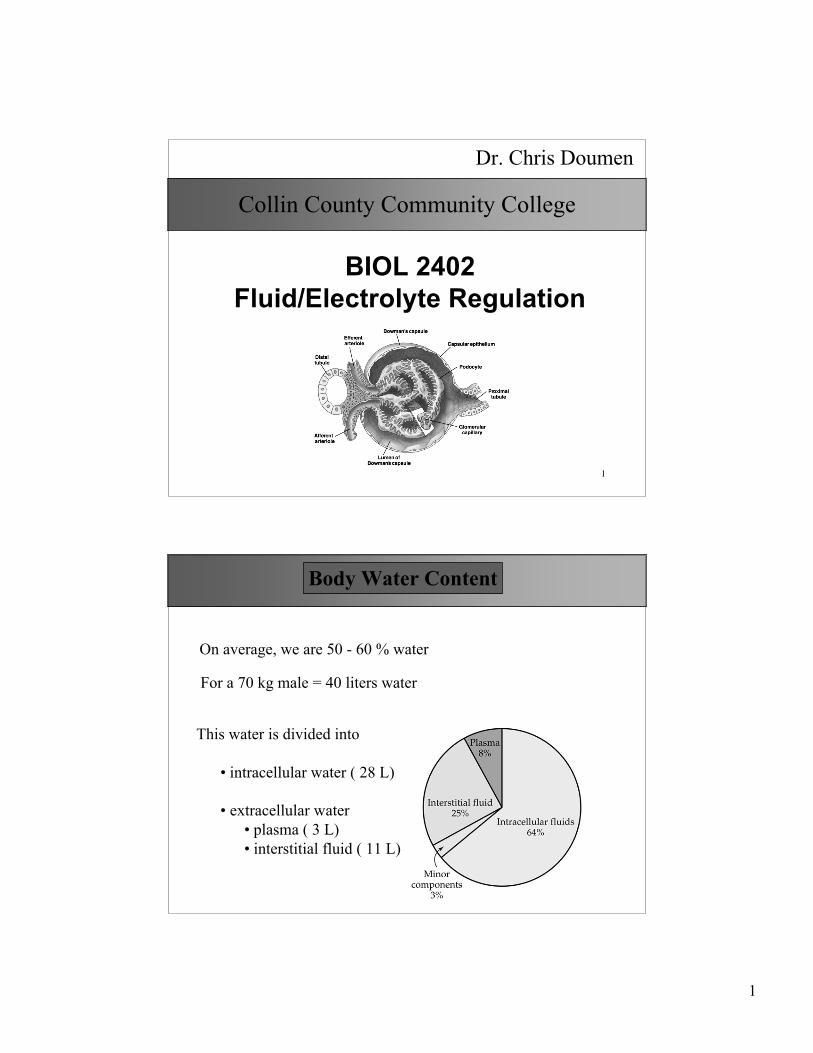
On average, we are 50 - 60 % water
For a 70 kg male = 40 liters water
This water is divided into
• intracellular water ( 28 L)
• extracellular water• plasma ( 3 L)• interstitial fluid ( 11 L)
Body Water Content
2
3
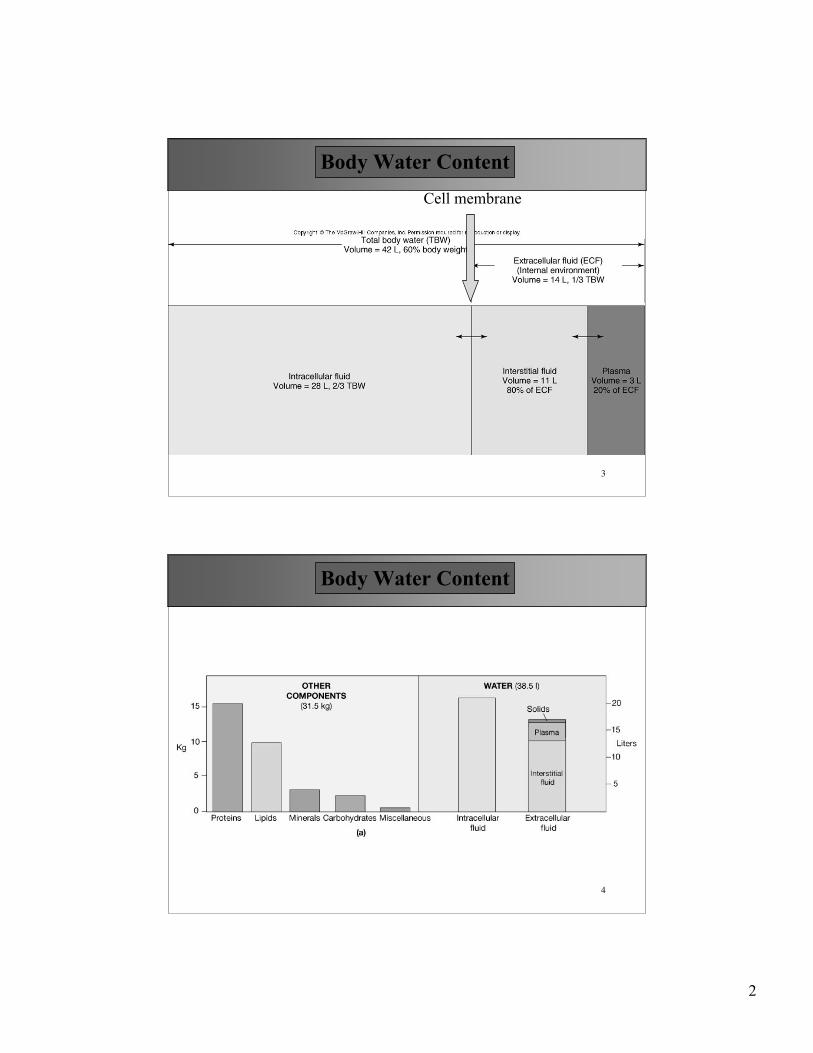
Cell membrane
Body Water Content
4
Body Water Content
3
5
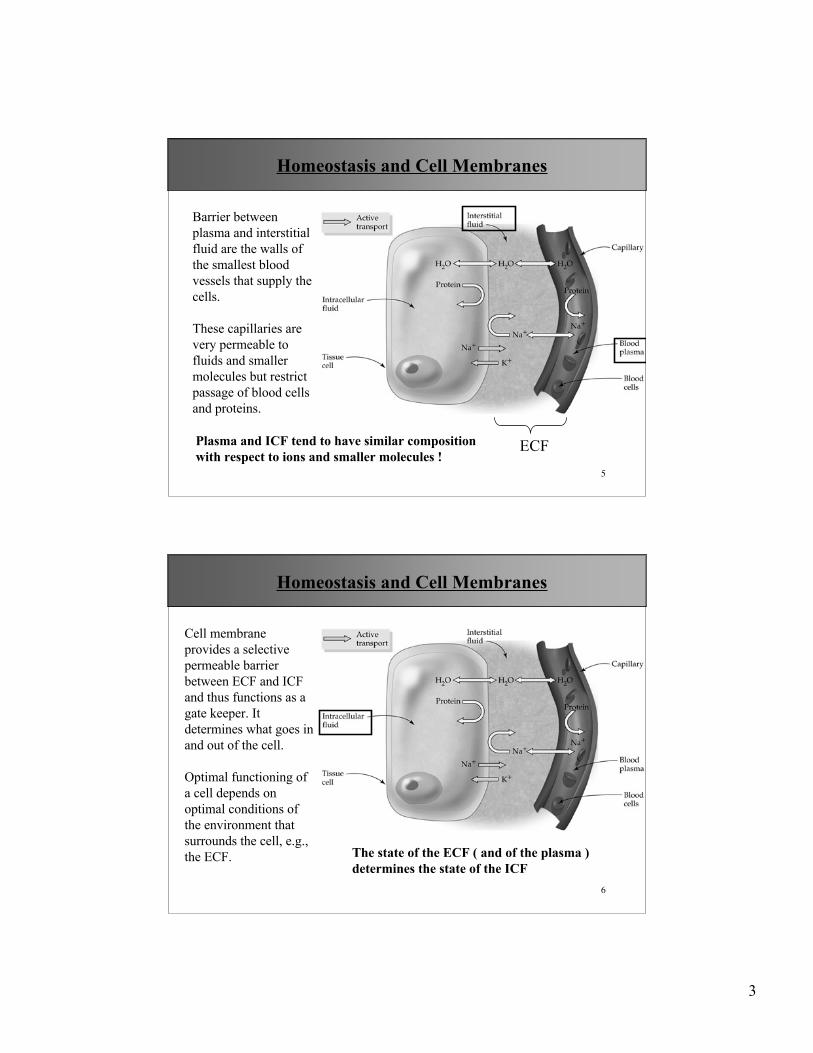
Barrier betweenplasma and interstitialfluid are the walls ofthe smallest bloodvessels that supply thecells.
These capillaries arevery permeable tofluids and smallermolecules but restrictpassage of blood cellsand proteins.
ECFPlasma and ICF tend to have similar compositionwith respect to ions and smaller molecules !
Homeostasis and Cell Membranes
6
Cell membraneprovides a selectivepermeable barrierbetween ECF and ICFand thus functions as agate keeper. Itdetermines what goes inand out of the cell.
Optimal functioning ofa cell depends onoptimal conditions ofthe environment thatsurrounds the cell, e.g.,the ECF. The state of the ECF ( and of the plasma )
determines the state of the ICF
Homeostasis and Cell Membranes
4
7
Electrolyte Distribution
8
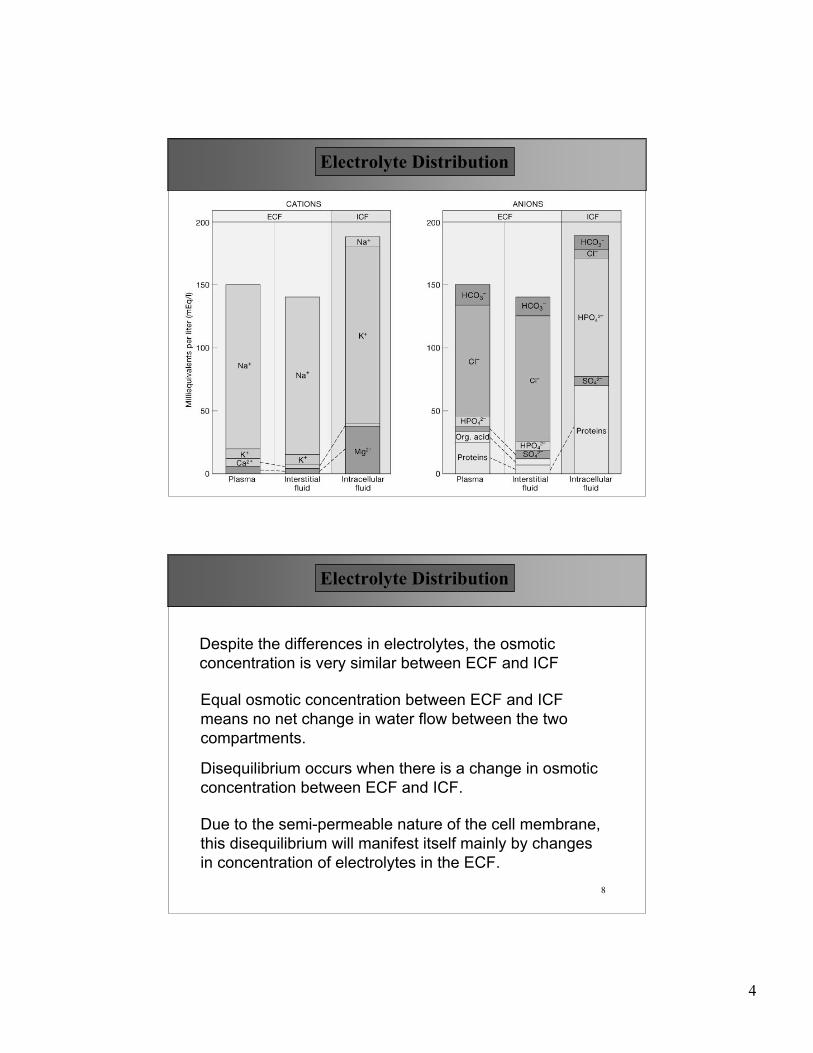
Despite the differences in electrolytes, the osmoticconcentration is very similar between ECF and ICF
Equal osmotic concentration between ECF and ICFmeans no net change in water flow between the twocompartments.
Disequilibrium occurs when there is a change in osmoticconcentration between ECF and ICF.
Due to the semi-permeable nature of the cell membrane,this disequilibrium will manifest itself mainly by changesin concentration of electrolytes in the ECF.
Electrolyte Distribution
5
9
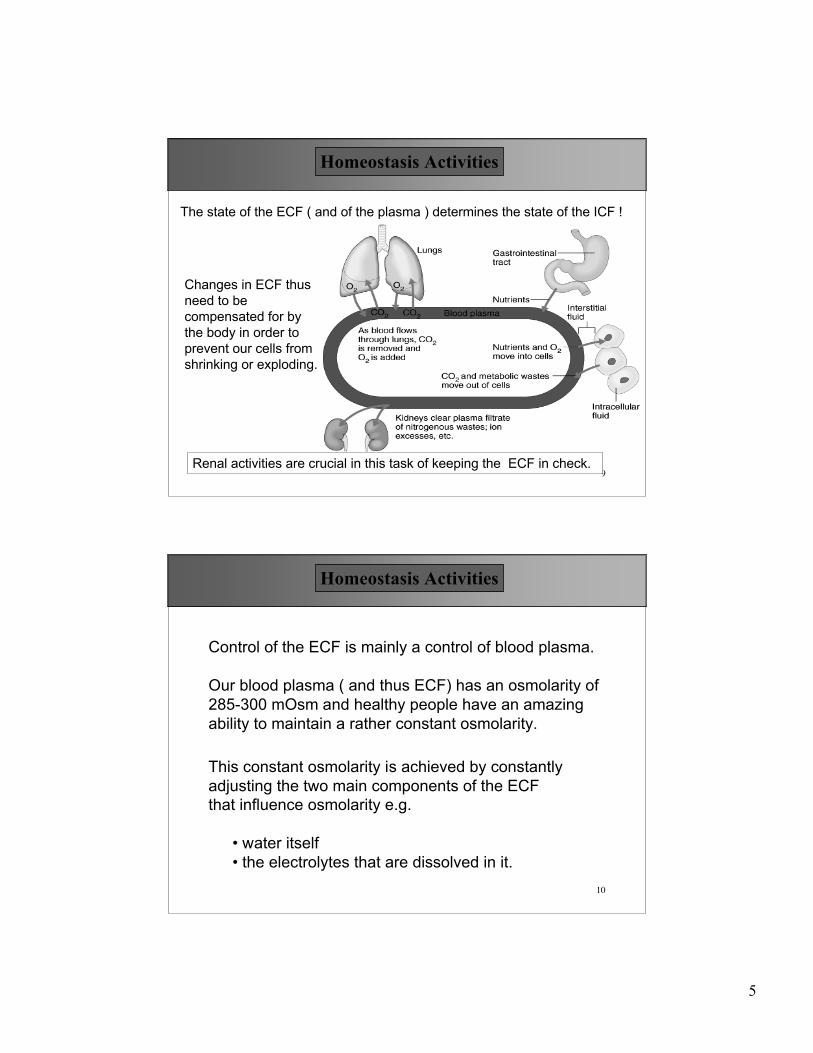
The state of the ECF ( and of the plasma ) determines the state of the ICF !
Changes in ECF thusneed to becompensated for bythe body in order toprevent our cells fromshrinking or exploding.
Renal activities are crucial in this task of keeping the ECF in check.
Homeostasis Activities
10
Control of the ECF is mainly a control of blood plasma.
Our blood plasma ( and thus ECF) has an osmolarity of285-300 mOsm and healthy people have an amazingability to maintain a rather constant osmolarity.
This constant osmolarity is achieved by constantlyadjusting the two main components of the ECFthat influence osmolarity e.g.
• water itself• the electrolytes that are dissolved in it.
Homeostasis Activities

6
11
Stabilizing water volume, electrolyte balance and pH valueof the ECF involves three inter-related processes. Controlof the ECF is mainly a control of blood plasma.
Fluid Balance• is present when amount of water gain per day equals
water loss• fluid balance is mostly a digestive and urinary system
process
Homeostasis Activities
Electrolyte Balance• because cells can’t transport water, the ICF water content is
regulated by regulation of electrolytes in and out of the cells.• once again, electrolyte balance is mostly a function of
digestive and urinary system.
12
The last process is not a direct water and osmolaritystabilizing process, but protons have drastic effects onpH values and are regulated very tightly.
Acid-Base Balance• The body is in acid-base balance when the
production of hydrogen ions is offset by their loss• The primary problem for the body is a reduction in pH
values since many daily metabolic processesgenerate protons
• The kidneys are responsible for proton eliminationand bicarbonate retention.
• The lungs play an essential role in elimination ofcarbon dioxide.
Homeostasis Activities
7
13
BASIC CONCEPTS OF REGULATION
• All homeostatic mechanisms respond to changes inECF, not ICF
• Receptors don’t monitor total fluid or total electrolytebalance, but do monitor plasma volume andosmolarity changes.
• Cells cannot transport water molecules by activetransport; water moves by means of osmotic forces.
• Body content of water or electrolytes rises if intakeexceeds outflow
Homeostasis Activities
14
PRIMARY HORMONES INVOLVED IN REGULATION
Homeostasis Regulation
• Antidiuretic hormone (ADH)– Stimulates water conservation and the thirst
center• Aldosterone
– Controls Na+ absorption and K+ loss along theDCT
• Natriuretic peptides (ANP and BNP)– Reduce thirst and block the release of ADH and
aldosterone
8
15
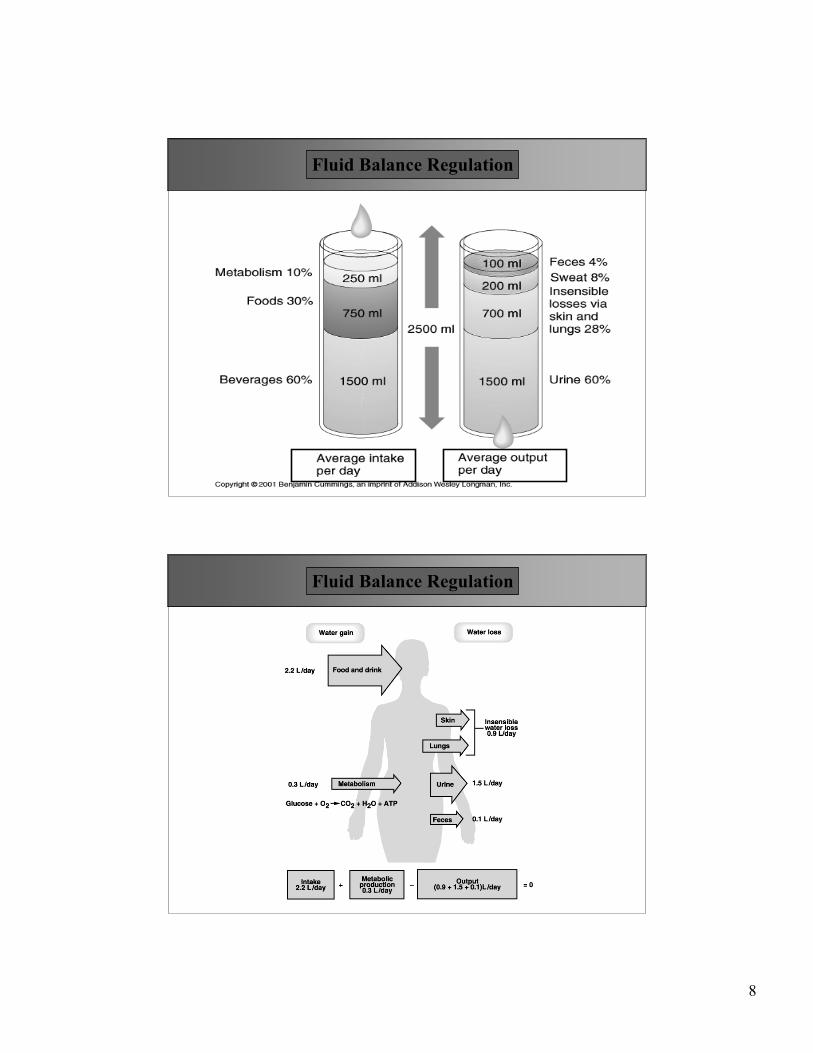
Fluid Balance Regulation
16
Fluid Balance Regulation
9
17
The loss we experience daily is a combination of waterAND electrolytes such as
• K+ , Na+ , Cl- ,• HPO4
- , HCO3- .
Kidneys can only regulate the loss of water andelectrolytes.
The function of the kidneys is to regulate the water andelectrolyte balance.
However, the kidneys cannot replenish the water lost or theelectrolytes excreted by the body. This replenishmentneeds to come from the intake sources.
Fluid Balance Regulation
18
Since the kidneys can only regulate the amount of waterthat is lost via the urinary system, the water loss via non-kidneys avenues makes fluid intake a necessary event inorder to balance blood homeostasis
Water Balance is achieved by 2 mechanisms
1. Thirst center
Fluid Balance Regulation
• When water is lost from our system, the Osmolarity of our bloodtends to rise (makes things more concentrated)
• Osmoreceptor cells in hypothalamus ‘dehydrate’ and depolarize• Together with a dry mouth (less saliva production, it triggers the
thirst sensation• Conditions that result in an increase in osmolarity (Loss of lots of
blood or eating salty food) make you thirsty.

10
19
Fluid Balance Regulation
20
2. ADH
• When Osmolarity rises , the hypothalamus isstimulated as well to release ADH
• ADH specifically works on the collecting ducts andinserts more “water-channels”
• This allows water to escape into the medulla area ofthe kidney as the collecting ducts move deeperalong the osmotic gradient in the medulla.
• Release of ADH results in the kidneys excreting lessurine, and more water redirected to blood
Fluid Balance Regulation

11
21
22
Plasma ADH in function of Plasma Osmolarity
Fluid Balance Regulation

12
23
(no ADH) +ADH
Fluid Balance Regulation
24
ADH works via a cAMP mechanism and results in the insertion ofwater channels (aquaporins) in collecting ducts cells
Fluid Balance Regulation
13
25
Fluid Balance Regulation
Result of water imbalances are overhydration or dehydration.Both conditions will cause changes in osmolarity of thebody water compartments, and hence, osmosis. Theresulting water movement between ECF and ICF is calledfluid shifts !
– If ECF becomes hypertonic relative to ICF, water movesfrom ICF to ECF
– If ECF becomes hypotonic relative to ICF, mater movesfrom ECF into cells
26
Fluid Balance Regulation
Because the ICF is twice as large as the ECF, it acts as abuffer zone for water and physiological changes in ECF watercontent will quickly be exchanged with ICF, resulting in minorchanges in both compartments.
ICF ECF
Prolonged fluid shifts without corrections ( fluid or electrolyte intake forexample) will result in pathological problems.
14
27
The balance of all the salts in our body is crucial for a widearray of activities
• Na+, K+ for electrical activities of neurons, muscle• Ca++ for contractile activity, bone deposit• Mg++ for DNA replication, liberation of energy from ATP
The kidneys are the organs that try to maintain thatelectrolyte balance. The food we take in is mostly adequatein salt content although some diets may be lacking in severalsalts.
Electrolyte Balance Regulation
Electrolytes are ions released through the dissociation ofinorganic compounds. They are usually associated with salts !
28
Because sodium is most abundant in the ECF, sodium is themajor player in electrolyte imbalances.
Potassium imbalances are less common, but if they do occur ,are significantly more dangerous !
• Sodium• Potassium
Electrolyte Balance Regulation
Two major ions are important that exert significantosmotic contribution and directly affect normalcellular function . They are
15
29
Central Role of Sodium
Wherever sodium moves, water will follow by osmosis(water follows salts)
Thus regulation of sodium is linked to BP, Blood volumeand many other processes such as acid -base control
• Sodium salts make up 90% of all solutes in ECF• Single most abundant cation in ECF (~142 mEq/L)• Exerts significant osmotic pressure
How is sodium content regulated ?
Electrolyte Balance Regulation
30
1. Aldosterone
Normally, 65 % of Na+ is reabsorbed in PCT andanother 25 % in loop of Henle
• The final 10 % of sodium re-absorption isdetermined by the presence of Aldosterone
• Action of aldosterone is to insert more Na-Kpumps into the basolateral side of the Distaltubules.
Sodium Regulation

16
31
If Aldosterone is high• most all remaining Na+ is reabsorbed as NaCl in
DCT and Collecting tubules• Water will follow when possible (depending on
location)• Urine volume decreases
If Aldosterone is low• No Na+ is reclaimed and thus excreted• Water will follow and excreted urine volume
increases
Sodium Regulation
32
How does Aldosterone work ?
Sodium Regulation
17
33
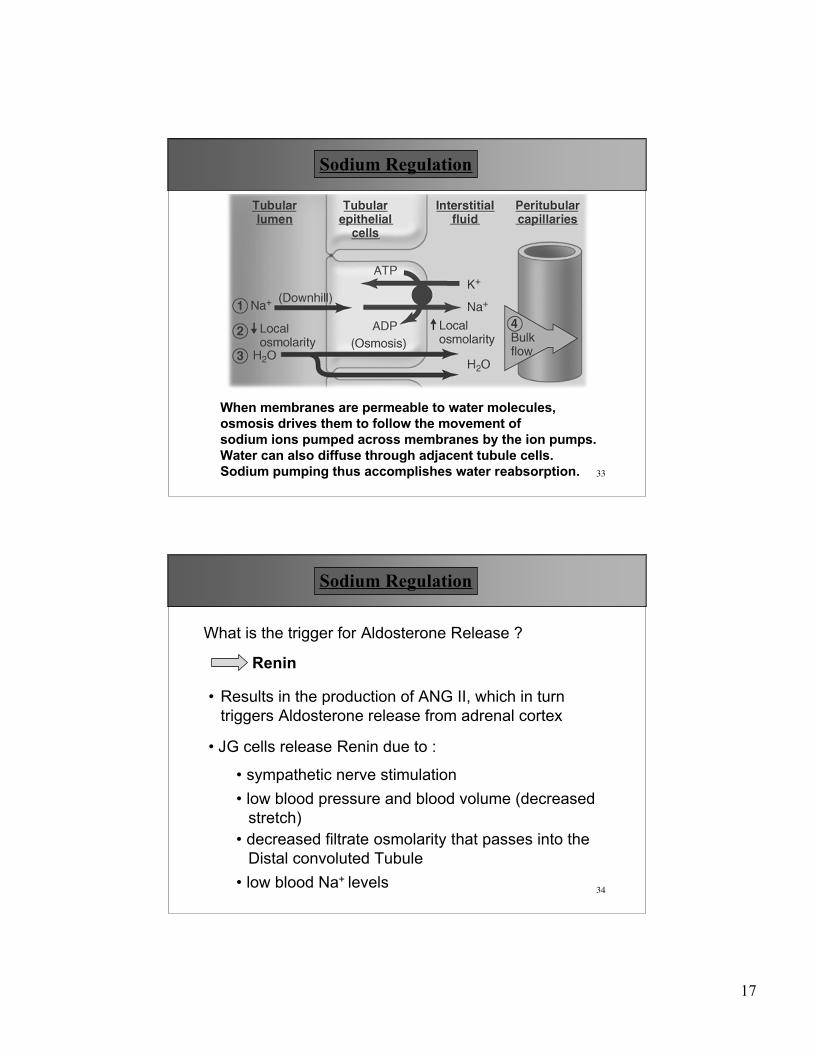
When membranes are permeable to water molecules, osmosis drives them to follow the movement of sodium ions pumped across membranes by the ion pumps.Water can also diffuse through adjacent tubule cells.Sodium pumping thus accomplishes water reabsorption.
Sodium Regulation
34
Renin
What is the trigger for Aldosterone Release ?
• JG cells release Renin due to :
• Results in the production of ANG II, which in turntriggers Aldosterone release from adrenal cortex
• low blood pressure and blood volume (decreasedstretch)
• decreased filtrate osmolarity that passes into theDistal convoluted Tubule
• low blood Na+ levels
• sympathetic nerve stimulation
Sodium Regulation
18
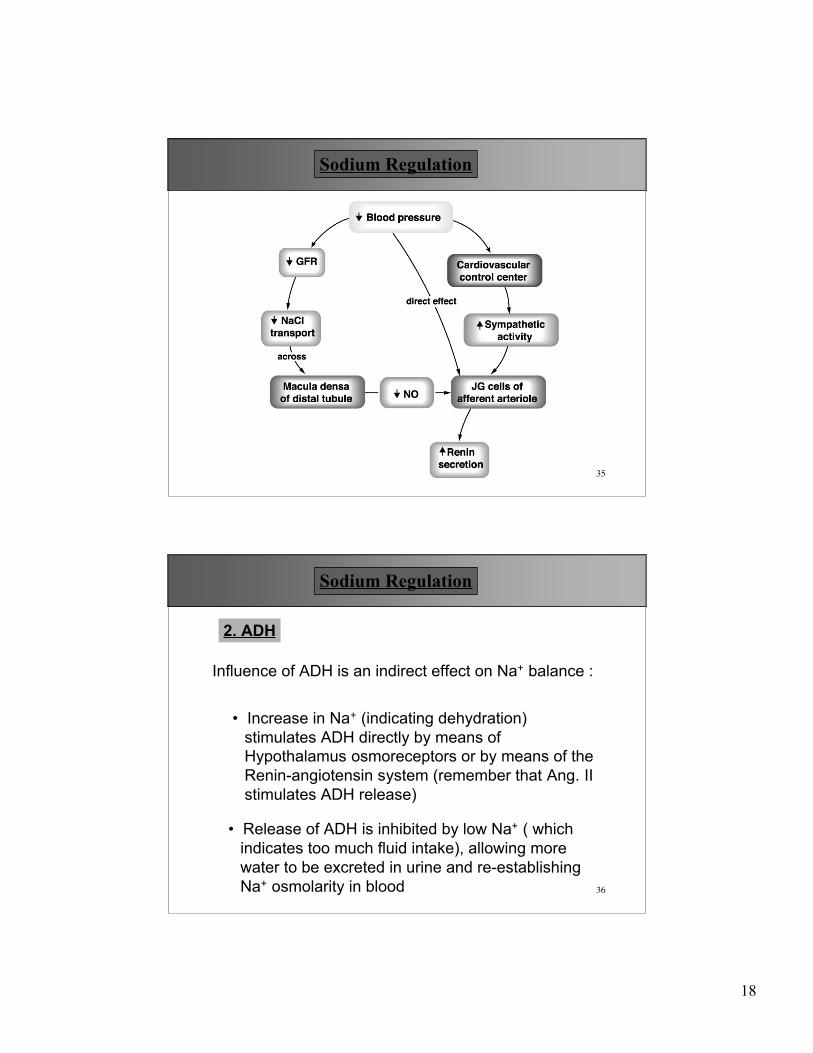
35
Sodium Regulation
36
2. ADH
Influence of ADH is an indirect effect on Na+ balance :
• Increase in Na+ (indicating dehydration)stimulates ADH directly by means ofHypothalamus osmoreceptors or by means of theRenin-angiotensin system (remember that Ang. IIstimulates ADH release)
• Release of ADH is inhibited by low Na+ ( whichindicates too much fluid intake), allowing morewater to be excreted in urine and re-establishingNa+ osmolarity in blood
Sodium Regulation
19
37
Sodium Regulation
38
Atrial Natriuretic peptide (ANP):
3. Other Factors
• produced by atria when blood pressure is high
• opposes ANG II effects by downregulating Reninproduction
• also inhibits ADH and aldosterone production
• promotes vasodilation and Na+ and water loss bythe kidneys (reduce BP)
Sodium Regulation
20
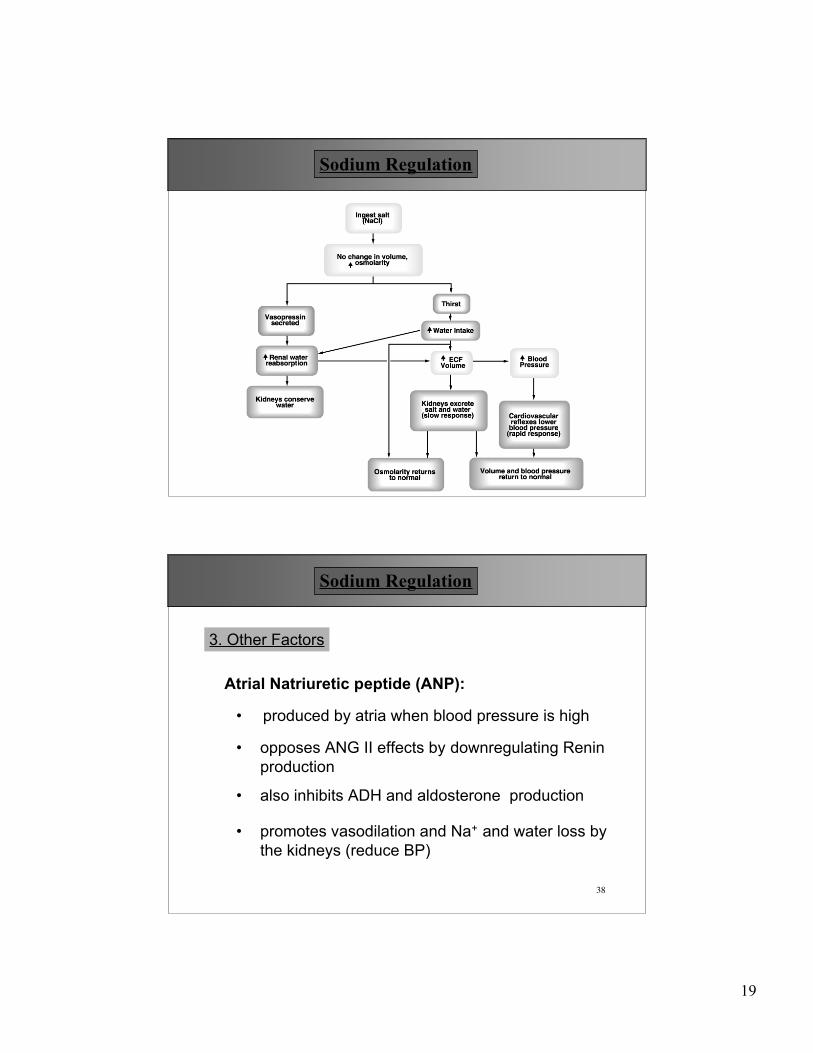
39
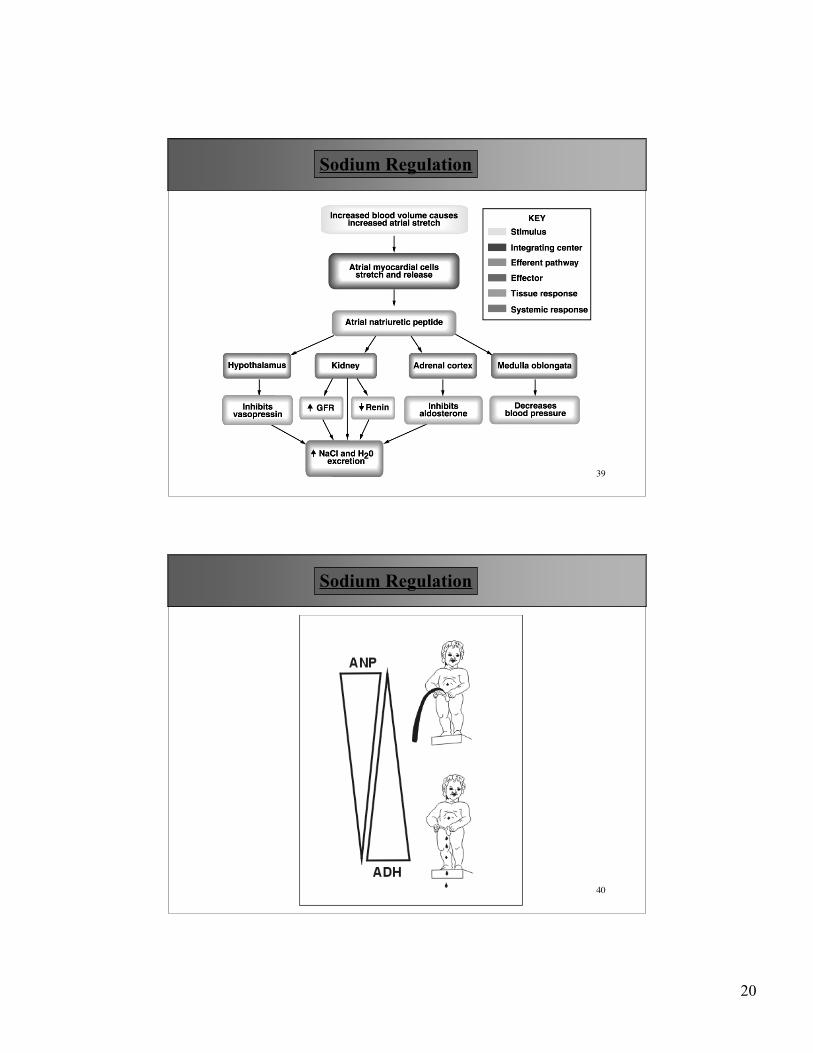
Sodium Regulation
40
Sodium Regulation
21
41
Estrogens
• are similar to Aldosterone and thus enhanceNaCl retention ( and thus water)
• explains water retention by woman duringmenstrual cycle when estrogens are high
Sodium Regulation
42
Regulation of Potassium
K+ is important in that too much or not enough potassiumcan lead to electrical malfunctioning with specific cardiacconsequences and possibilities for sudden death.
Similar to Na+, over 90 % of K+ is reabsorbed innephron tubules leaving some 10% to be excreted inthe urine.
Electrolyte Balance Regulation
22
43
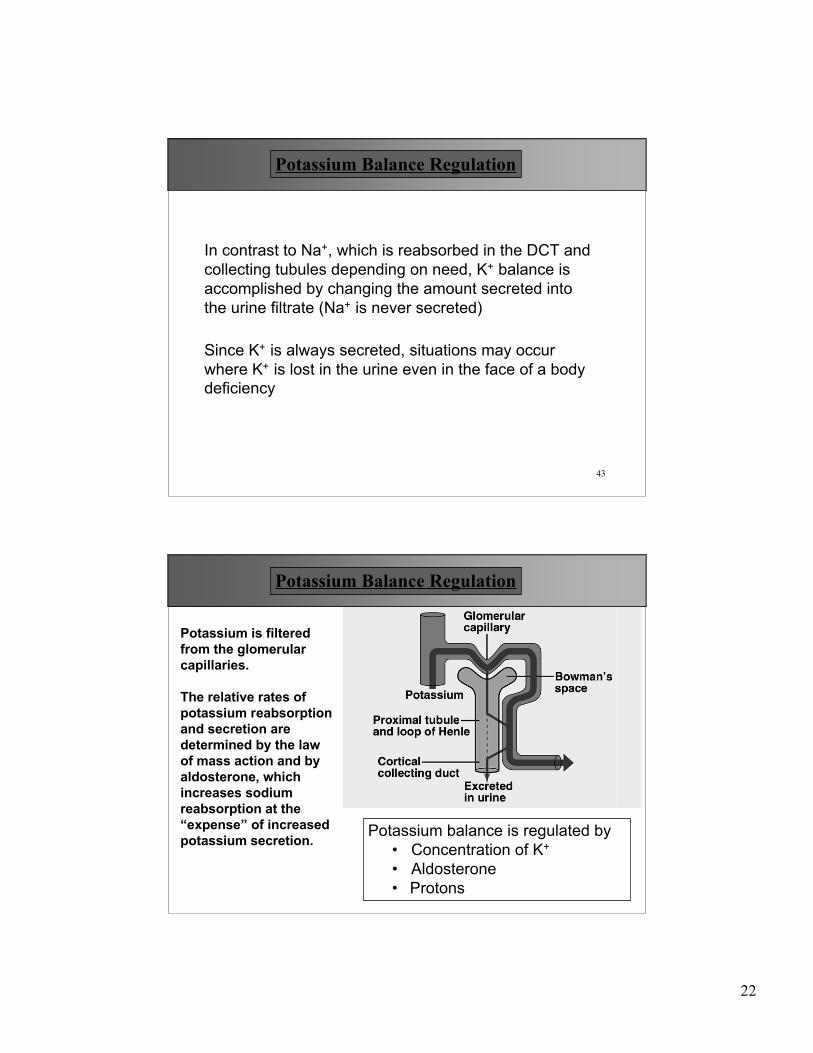
In contrast to Na+, which is reabsorbed in the DCT andcollecting tubules depending on need, K+ balance isaccomplished by changing the amount secreted intothe urine filtrate (Na+ is never secreted)
Since K+ is always secreted, situations may occurwhere K+ is lost in the urine even in the face of a bodydeficiency
Potassium Balance Regulation
44
Potassium is filteredfrom the glomerularcapillaries.
The relative rates ofpotassium reabsorptionand secretion aredetermined by the lawof mass action and byaldosterone, whichincreases sodiumreabsorption at the“expense” of increasedpotassium secretion. Potassium balance is regulated by
• Concentration of K+
• Aldosterone• Protons
Potassium Balance Regulation

23
45
If levels of K+ increase in blood stream• More K+ diffuses into Interstitial fluid• More K+ transported into DCT via Na/K Pump
Mass action regulation of K
Cells of the distal nephrons have a higher resting membranepotential at the lumen side ( -50 mV)• The driving force for K+ to leak out the cell is greater• In addition, there is now a higher K+ inside the DCT cells• Lumen side has an abundance of K+ leakage channels.• Final result, more K+ leaves (secreted) the cells into the
lumen of the nephron via these leakage channels
Potassium Balance Regulation
46
Perit
ubul
ar c
apilla
ry
K+
Why does K+ secretion not happen in PCT but mostly in distalparts of the nephron ?
-50 mV
Mass action regulation of K
Potassium Balance Regulation
24
47
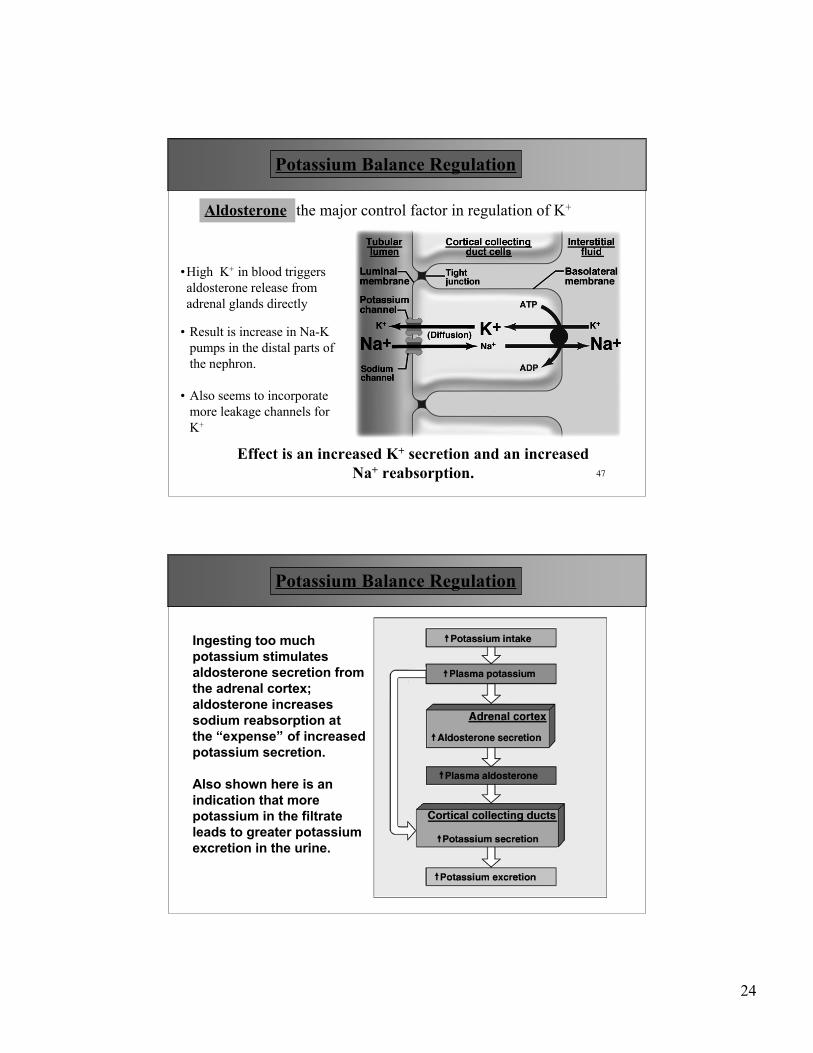
Aldosterone the major control factor in regulation of K+
•High K+ in blood triggersaldosterone release fromadrenal glands directly
• Result is increase in Na-Kpumps in the distal parts ofthe nephron.
• Also seems to incorporatemore leakage channels forK+
Effect is an increased K+ secretion and an increasedNa+ reabsorption.
Potassium Balance Regulation
48
Ingesting too muchpotassium stimulatesaldosterone secretion fromthe adrenal cortex;aldosterone increasessodium reabsorption atthe “expense” of increasedpotassium secretion.
Also shown here is anindication that morepotassium in the filtrateleads to greater potassiumexcretion in the urine.
Potassium Balance Regulation

25
49
• Whenever the pH of blood declines, the rate of potassiumsecretion declines
• This is due to the fact that hydrogen will compete withpotassium , and thus hydrogen will be secreted inexchange for sodium instead of potassium in exchangefor sodium
• Typical result is that people with acidosis may end upwith hyperkalemia !
Potassium Balance Regulation
Regulation by Protons
50
Any factor that triggers aldosteronerelease can thus result in increased K+
secretion
• Na+ depletion
• ECF depletion
• drop in BP
may result in K+
depletion
The Na-K pump in the distal parts of thenephron can also use H+ instead of K+.
Thus if there is an increased amount ofblood H+ ( acidosis) , the excess H+ willcompete with K+ and less K+ gets to besecreted.
Potassium Balance Regulation