Biography of Camran Nezhat, MD, FACOG, FACSnezhat.org/.../2015/09/James_Carter_about_Camran.pdf ·...
6
Biography of Camran Nezhat, MD, FACOG, FACS James E. Carter, MD, PhD Camran Nezhat has influ- enced almost every as- pect of our laparoscopic lives. His vision, perse- verance, and humanistic focus have propelled our field away from the estab- lished yet awkward “sin- gle eye” and mostly diag- nostic laparoscopy to his method of operative laparoscopy, which has revolutionized modern day surgery. Also, his prediction and claim that almost all open surgeries could be and should be avoided is increas- ingly becoming a reality. 1–6 Indeed, he has paved the way through the years by his pioneering work of successful management of many complex surgical pathologies lapa- roscopically for the first time and proving that it is possible and probably preferable. 4–6 Of equal importance, Camran on a personal level has positively affected many of us as well. His sincerity, clarity of thought, and faith that the future can be made better than the present—if only we apply ourselves to the un- solved problems of medicine—remain a source of contin- ual inspiration. I recall vividly the experience of Camran inspiring me to strive for broader frontiers, when, at the 2nd European Congress in Gynecological Endoscopy in Heidelberg, Germany, a packed audience sat transfixed on uncomfort- ably hard folding chairs as he unveiled his uncannily prescient vision for the field of laparoscopy, foretelling of a time years into the future when large incisions would eventually become obsolete. This was in 1993, ten years ahead of the curve, when operative laparoscopy was still considered quite limited and dangerous, especially since the technology did not exist to match this futuristic view. Despite this technological lag, Camran demonstrated via video footage of his collaborative work with colleagues from other disciplines that laparoscopic techniques could be integrated into therapy for the abdominal and pelvic cavity, heart, brain, lungs, vessels, endocrine system, and to every aspect of surgery where a cavity existed or a cavity could be created. For, in these situations, he found that the anatomy could be magnified and therefore better visualized. 4–5 As with so many pioneers in our profession, Camran indeed attracted numerous negative reviews, in the cate- gory of “medical heresy.” 7 Yet today, we see that his early commitment to advancing medicine has helped pave the way for laparoscopic specialists the world over to provide patients with the option of speedier recoveries and im- proved outcomes. That day in Heidelberg, I was en- thralled and felt challenged by him to participate more fully in expanding the frontiers to help with his vision. Camran introduced the technique of operating in an up- right position off the television monitor and on the images rather than on the tissue! By doing so, he changed the “single eye” world of endoscopy forever. 1,6 Second, he is the forerunner of successful laparoscopic reparative man- agement of many diseases of the pelvic and abdominal organs including laparoscopic bladder, ureter, bowel and diaphragm resection, laparoscopic paraaortic lymph node dissection, radical hysterectomy, vesicovaginal fistulas, rectovaginal fistulas; and laparoscopic treatment of ovar- ian remnant. Sacral colpopexy and laparoscopy during advanced pregnancy and repair of major vessels were also first reported by Camran and his team. 1– 6,8 –34 Thus, Cam- ran opened the road for those in other surgical disciplines to approach almost all surgical pathologies laparoscopi- cally. Third, his claims are becoming increasingly evident that advantages of laparoscopic surgery are not only shorter hospital stays, smaller incisions, and faster recov- ery, but also that laparoscopic surgery when performed by an experienced surgeon is associated with fewer compli- cations and better results than laparotomy is. 30 –38 So where did such a man come from? Camran was born in Iran (Persia). His interest in medicine started very early and became his desire when his mother I would like to thank Farr and Ceana Nezhat for sharing family memories and especially to Camran Nezhat for opening his heart for this article. Address reprint requests to: James E. Carter, MD, PhD, 26732 Crown Valley Parkway, Ste 541, Mission Viejo, CA 92691, USA. Telephone: 949 364 5802, Fax: 949 364 2871 © 2006 by JSLS, Journal of the Society of Laparoendoscopic Surgeons. Published by the Society of Laparoendoscopic Surgeons, Inc. Camran Nezhat, MD JSLS (2006)10:275–280 275 PROFILE IN LAPAROSCOPY
Transcript of Biography of Camran Nezhat, MD, FACOG, FACSnezhat.org/.../2015/09/James_Carter_about_Camran.pdf ·...

Biography of Camran Nezhat MD FACOG FACS
James E Carter MD PhD
Camran Nezhat has influ-enced almost every as-pect of our laparoscopiclives His vision perse-verance and humanisticfocus have propelled ourfield away from the estab-lished yet awkward ldquosin-gle eyerdquo and mostly diag-nostic laparoscopy to hismethod of operativelaparoscopy which hasrevolutionized modern
day surgery Also his prediction and claim that almost allopen surgeries could be and should be avoided is increas-ingly becoming a reality1ndash6 Indeed he has paved the waythrough the years by his pioneering work of successfulmanagement of many complex surgical pathologies lapa-roscopically for the first time and proving that it is possibleand probably preferable4ndash6
Of equal importance Camran on a personal level haspositively affected many of us as well His sincerity clarityof thought and faith that the future can be made betterthan the presentmdashif only we apply ourselves to the un-solved problems of medicinemdashremain a source of contin-ual inspiration
I recall vividly the experience of Camran inspiring me tostrive for broader frontiers when at the 2nd EuropeanCongress in Gynecological Endoscopy in HeidelbergGermany a packed audience sat transfixed on uncomfort-ably hard folding chairs as he unveiled his uncannilyprescient vision for the field of laparoscopy foretelling ofa time years into the future when large incisions wouldeventually become obsolete This was in 1993 ten yearsahead of the curve when operative laparoscopy was stillconsidered quite limited and dangerous especially sincethe technology did not exist to match this futuristic view
Despite this technological lag Camran demonstrated viavideo footage of his collaborative work with colleaguesfrom other disciplines that laparoscopic techniques couldbe integrated into therapy for the abdominal and pelviccavity heart brain lungs vessels endocrine system andto every aspect of surgery where a cavity existed or acavity could be created For in these situations he foundthat the anatomy could be magnified and therefore bettervisualized4ndash5
As with so many pioneers in our profession Camranindeed attracted numerous negative reviews in the cate-gory of ldquomedical heresyrdquo7 Yet today we see that his earlycommitment to advancing medicine has helped pave theway for laparoscopic specialists the world over to providepatients with the option of speedier recoveries and im-proved outcomes That day in Heidelberg I was en-thralled and felt challenged by him to participate morefully in expanding the frontiers to help with his vision
Camran introduced the technique of operating in an up-right position off the television monitor and on the imagesrather than on the tissue By doing so he changed theldquosingle eyerdquo world of endoscopy forever16 Second he isthe forerunner of successful laparoscopic reparative man-agement of many diseases of the pelvic and abdominalorgans including laparoscopic bladder ureter bowel anddiaphragm resection laparoscopic paraaortic lymph nodedissection radical hysterectomy vesicovaginal fistulasrectovaginal fistulas and laparoscopic treatment of ovar-ian remnant Sacral colpopexy and laparoscopy duringadvanced pregnancy and repair of major vessels were alsofirst reported by Camran and his team1ndash68ndash34 Thus Cam-ran opened the road for those in other surgical disciplinesto approach almost all surgical pathologies laparoscopi-cally Third his claims are becoming increasingly evidentthat advantages of laparoscopic surgery are not onlyshorter hospital stays smaller incisions and faster recov-ery but also that laparoscopic surgery when performed byan experienced surgeon is associated with fewer compli-cations and better results than laparotomy is30ndash38
So where did such a man come from
Camran was born in Iran (Persia) His interest in medicinestarted very early and became his desire when his mother
I would like to thank Farr and Ceana Nezhat for sharing family memories andespecially to Camran Nezhat for opening his heart for this article
Address reprint requests to James E Carter MD PhD 26732 Crown ValleyParkway Ste 541 Mission Viejo CA 92691 USA Telephone 949 364 5802 Fax 949364 2871
copy 2006 by JSLS Journal of the Society of Laparoendoscopic Surgeons Published bythe Society of Laparoendoscopic Surgeons Inc
Camran Nezhat MD
JSLS (2006)10275ndash280 275
PROFILE IN LAPAROSCOPY
became ill and required a great deal of medical care Thedoctors involved in her care saved her life
After this incident Camranrsquos father praised the doctors assaviors of their mother The Nezhat brothers thereforegrew up with the knowledge that doctors were highlyvalued in their family and in the world for their life-savingservices This fueled the desire in the Nezhat brothers toenter medicine On reflection because of the significantrole that Mrs Nezhat had in the life of her children andbecause of her steadfast devotion 3 of the Nezhat broth-ers did in fact became gynecological surgeons
During internship and residency at the State University ofNew York under the tutelage of Dr Ronald Batt Camranwas exposed to laparoscopy as a diagnostic tool for infer-tility patients and for those suffering from pelvic painDuring those days laparotomies were performed even formild endometriosis After observing so much postopera-tive distress suffered by laparotomy patients comparedwith patients who had diagnostic laparoscopy Camranthought to himself ldquoWhy shouldnrsquot we treat more surgicalpathologies laparoscopicallyrdquo The hindrance to expand-ing from diagnostic to operative laparoscopy it seemed tohim was not a question of anatomical or physical con-straints but rather was a question of conceptualizing newtechnologies and methodologies He learned that otherinvestigators around the world aware of this potentialwere trying to expand the application of laparoscopyVisualization difficulties from peering crouched overthrough the endoscope with only one eye seemed themost crucial impediment to overcome Thus in recogniz-ing this need and inspired by the earlier pioneersrsquo workthis crucial moment of realization led to a turning point foroperative laparoscopy as Camran embarked on refininglaparoscopic procedures to assist both patients and theoperating team to achieve greater results
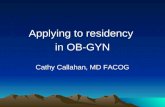
At the forefront and important juncture of the discovery ofthe advantages of operating on the images (videolaparos-copy) Camran performed endoscopic surgery off themonitor starting in the late 1970s using very heavy andawkward video camera equipment that had been pro-duced for other uses and which instead he customizedmdashrigged actuallymdashfor use with the laparoscope1ndash6 (Figure 1)
Due to the poor intensity of light sources at times he usedan extra laparoscope connected to the light source only tobring ldquomore light to the subjectrdquo
Operating directly from the visual field utilizing only themonitor transformed the operating room from a ldquoone manbandrdquo into an ldquoorchestrardquo so that assisting surgeons
nurses anesthesiologists students and others could fullyview and therefore more readily assist in and learn thesurgery
After residency Dr Harold Feldman one of Camranrsquosprofessors at that time recommended him for a fellowshipin reproductive endocrinology and infertility under thementorship of Drs Robert Greenblatt Don Gambrell andVirenda Mahesh PhD in Augusta Georgia who werethemselves leaders in reproductive endocrinology andimmunology During this time especially he confirmedhis interest in helping couples suffering from infertility ashe saw their overwhelming joy in experiencing parent-hood after successful treatment He was also motivated toassist those women suffering from other debilitating re-productive disorders
Following this fellowship in 1980 he started his owninfertility practice in Atlanta It was at this time that Cam-ran was able to concentrate more fully on improving andexpanding the use of the videolaparoscopy technique anddesigning new instrumentation Soon he became one ofthe most skilled surgeons Word of mouth began to spreadof this approach and soon his practice began to thrivePatients started arriving from all over the country andabroad
The videolaparoscopy technique was working extraordi-narily well for his infertility patients many of whom hadendometriosis With these excellent clinical results con-firmed Camran set out to share this technique with othercolleagues Along with Dr Scott Crowgey a pediatricianteaching physics at the Georgia Institute of Technologyhe started teaching postgraduate courses in operativelaparoscopy in 1983 It was not until 1986 that he was
Figure 1 Camran Nezhat MD performs endoscopic surgery offthe monitor
Biography of Camran Nezhat MD FACOG FACS Carter JE
JSLS (2006)10275ndash280276
finally able for the first time to publish about successfullaparoscopic treatment of extensive endometriosis2
Camran has always shared his experiences with his col-leagues around the world and has continued to presenthis methods results and his experiences at different med-ical societies and congresses to explain the benefits of thistechnique
He demonstrated that even the most advanced pelvic andabdominal pathologies including advanced stages of en-dometriosis involving bowel bladder ureter diaphragmand liver can be successfully treated by videolaparos-copy2458ndash34 Camran his brothers and others also en-gaged in research to better understand the origin of en-dometriomas39
After achieving clinical success numerous times withvideolaparoscopy Camran stated early on that ldquoif ad-vanced stages of endometriosis can be successfully treatedby videolaparoscopy with the results at least as good as[those of] laparotomy we can perform practically all thesurgical procedures by videolaparoscopyrdquo In his opinionvideolaparoscopy was the method of choice for an oper-ation whenever a cavity exists in the body or when acavity can be created439
Camran is fortunate to have the support of his family Allof his brothers including a psychologist an industrialengineer and 2 physicians have encouraged and inspiredhim His mother who passed on 5 years ago also joinedthem in Atlanta and was an especially significant source ofinspiration Their father had passed on earlier Farr andCeana later joined Camran in his practice
In collaboration with their colleagues such as urologistscolorectal surgeons oncologists cardiothoracic vascularand neurosurgeons the 3 brothers were the forerunnersto perform some of the most advanced procedures lapa-roscopically58ndash34
As they were being recruited by different universities indifferent parts of the country to teach their techniquesStanford University Medical Center was the winner
Ms Linda Meier chairman of the board at Stanford MedicalCenter and Kenneth Bloom CEO of the Stanford MedicalCenter at that time and Claire Mailhot traveled to Atlantato convince Camran and his brothers to move to Palo Altoand start teaching and sharing their experience with per-sons in other surgical disciplines for the purpose of pro-liferation of endoscopic surgery and teaching future gen-erations of surgeons
Upon arriving at Stanford they did collaborate with phy-
sicians in different surgical disciplines and propelled Stan-ford University to the forefront of endoscopic surgery Infact in September 1993 Stanford was one of the fewuniversities to embrace endoscopic surgery The chairmanof surgery at that time was Dr John Niederhauber anopen-minded surgeon specializing in oncological sur-gery After seeing Camran demonstrate the new tech-niques in the operating room Dr Niederhauber became atrue convert and subsequently collaborated with Camranand other colleagues to perform many general surgicalprocedures laparoscopically
Shortly thereafter Dr Niederhauber honored Camran witha clinical professorship in the Department of Surgery atStanford Thus as a result of these initial leaps of faith andin collaboration with those in different disciplines of sur-gery endoscopic surgery at Stanford bound forward
In 1995 Dr Mary Lake Pollan OBGYN DepartmentChairman at Stanford said
Nezhatrsquos contribution was and is unique He has devel-oped such facility with the technique in the operatingroom that he serves as a mentor for other physicianschallenging us to learn the new technique by showing usnot only the art of the possible but the tremendousadvantage minimal access surgery offers When you watchhim operate you have to cast off the excuse lsquothis proce-dure canrsquot be done using video laparoscopyrsquo37 The intro-duction of videolaparoscopy and videolaseroscopy byNezhat allowed the involvement of the entire operatingteam in the surgery Camran along with his brothers notonly performed these procedures elegantly but he wasalso willing to teach any- and everyone who expressed aninterest They are very freely and unselfishly willing toshare their experience and knowledge with the world37
In 2000 the late Kurt Semm35 said
With his genius he widened the operative field creatingnew techniques employing new instruments and appa-ratuses In my opinion with the cooperation of his 2brothers Camran enriched the entire field of surgical lapa-roscopy On June 30 1980 I performed a laparoscopicappendectomy which ultimately opened the door forsurgeons to perform endoscopic surgery especially sincethe appendix was a holy grail of surgery Today DrNezhatrsquos book opens a new door to a whole new era ofendoscopic surgery35
JSLS (2006)10275ndash280 277
In 1995 Alan DeCherney MD Professor Department ofObstetrics and Gynecology UCLA said
In the past decade gynecologic surgery because of en-doscopic surgery has undergone a tremendous revolu-tion There are few cases in the gynecologistrsquos surgicalarmamentarium that cannot be carried out through anendoscopic approach Many of these changes are due tothe courage innovativeness and technical skill of DrCamran Nezhat Just as in Star Trek he dared to go whereno man had gone before and by doing this he opened upunimagined vistas to endoscopic surgeons all over theworld For his courage Camran over the years has suf-fered but persevered3435
Like Bozzini Semm and others Camran too was sub-jected to undue ridicule7 For centuries there has beenresistance to accepting novel ideas even for concepts assimple as washing hands before an operation It costSemmelweis his life while Louis Pasteur was challengedto a duel by a general surgeon Camran too had to sufferyears of struggle and hardship7
For example when in the mid 1980rsquos Camran presented atthe annual meeting of the American Society of Reproduc-tive Medicine (then American Fertility Society) laparo-scopic management of extensive endometriosis and en-dometriomas he was faced with disbelief and accordingto one observer the audience was ready to ldquothrow toma-toesrdquo at him In another instance when Camran and hiscolleagues first performed and stated that bowel surgerycould be accomplished with the laparoscope in the late1980rsquos many were ready to crucify them for making suchclaims It was not until 2004 that New England Journal ofMedicine recommended and encouraged laparoscopicbowel resection40
Camran is testament to the fact that being a pioneer isoften a very lonely place until our beliefs are tested andproven It took 20 years but we are grateful that Camranpreserved and held steadfast to his dreams
We take operating directly off the video monitor or man-aging advanced surgical pathology laparoscopically forgranted but Camran paid dearly for it His declaration thatldquoalmost all laparotomies can be avoidedrdquo was not popu-larly received at the time but created such a shift in thethinking that it sparked a whole new generation of surgi-cal specialists to become inspired opening the door for alldisciplines35ndash37
Camran has been sharing his experiences by teachingpostgraduate courses in advanced laparoscopy and hys-
teroscopy since September 1983 and thousands of phy-sicians have been exposed to his teachings
He especially enjoys being a mentor to young physiciansand scientists who inspire him immensely with their op-timism and enthusiasm
Today Camran continues to contribute to the Art andScience of Surgery He is the immediate past president andsits on the Board of Trustees of the Society of Laparoen-doscopic Surgeons is the Director of the Center for Spe-cial Minimally Invasive Surgery and is Clinical Professorof Surgery and OBGYN at Stanford University School ofMedicine He has published more than 500 articles bookchapters abstracts letters to the editor and video presen-tations He is coauthor of 2 textbooks and has won nu-merous awards and honors from prestigious societies likeACOG ACS ASRM and the Excel Award from the Societyof Laparoendoscopic Surgeons More recent awards in-clude the ACOG 2004 ASRM 2004 and ACOG 2005 He ison the editorial board of the Journal of Fertility andSterility and is an associate editor for the Journal of Societyof Laparoendoscopic Surgeons
To Camran Nezhat we give our thanks for his hard workin sharing with all of us his vision and helping all of us tohelp our patients and improve our skills He has ex-panded our reach and allowed us to provide better carefor our patients He has unselfishly shared his knowledgewith us so we could integrate what he knows and doesinto our work No wonder he has been called the ldquoFatherof Modern Laparoscopyrdquo41
And yet one of the fondest memories is my image of himwalking with his brothers on a crowded New York Citystreet so much just the older brother providing love andsupport to his family He has expanded that familial bondto many who have become part of his laparoscopic familythrough our work with him especially in that extendedfamily known as the Society of Laparoendoscopic Sur-geons
I have to this day on my desk a picture of Paul WetterCamran Nezhat Farr Nezhat and Ceana Nezhat standingwith me in front of the JSLS display to remind me of thecollegiality the honor and the challenge of being a caringphysician in the spirit of our SLS family He has challengedall of us to do better for our patients and we gratefullyaccept that challenge
References
1 Nezhat C Laser laparoscopy for the treatment of endome-triosis Paper presented at Conjoint Meeting of the American
Biography of Camran Nezhat MD FACOG FACS Carter JE
JSLS (2006)10275ndash280278
Society for Reproductive Medicine and the Canadian Fertility andAndrology Society 1985 Toronto Canada
2 Nezhat C Crowgey SR Garrison CP Surgical treatment ofendometriosis via laser laparoscopy Fertil Steril 198645778ndash783
3 Nezhat C Nezhat FR Safe laser endoscopic excision orvaporization of peritoneal endometriosis Fertil Steril 198952149ndash151
4 Nezhat C Nezhat F Nezhat C Operative laparoscopy (min-imally invasive surgery) State of the art J Gynecol Surg 19928111ndash141
5 Nezhat C Nezhat F Silfen SL Videolaseroscopy the CO2laser for advanced operative laparoscopy Obstet Gynecol ClinNorth Am 199118585ndash604
6 Cowley G Hanging up the knife A novel surgical techniquepromises to save patients time money and blood NewsweekFebruary 12 199058ndash59
7 Nezhat F Triumphs and controversies in laparoscopy thepast the present and the future JSLS 200371ndash5
8 Nezhat F Nezhat C Silfen S Fehnel S Laparoscopic treat-ment of ovarian cyst during pregnancy J Laparoendosc Surg19911161ndash164
9 Nezhat C Pennington E Nezhat F Silfen S Laparoscopicallyassisted anterior rectal wall resection and reanastomosis fordeeply infiltrating endometriosis Surg Laparosc Endosc 19911(2)106ndash108
10 Nezhat C Winder WK Nezhat F Laparoscopic removal ofdermoid cysts Obst Gynecol 198973(2)278ndash281
11 Nezhat F Nezhat C Pennington E Laparoscopic proctec-tomy for infiltrating endometriosis of the rectum Fertil Steril1992571129ndash1132
12 Nezhat C Nezhat F Green B Laparoscopic treatment ofobstructed ureter due to endometriosis by resection and ureter-oureterostomy A case report J Urol 1992148865ndash868
13 Nezhat C Burrell M Nezhat F Benigno B Welander CELaparoscopic radical hysterectomy with paraaortic and pelvicnode dissection Am J Obstet Gynecol 1992166864ndash865
14 Nezhat F Nezhat C Levy JS Laparoscopic treatment ofsymptomatic diaphragmatic endometriosis A case report FertilSteril 199258614ndash616
15 Nezhat F Nezhat C Nezhat CH Laparoscopic sacral col-popexy for vaginal wall prolapse Obstet Gynecol 199484885ndash888
16 Nezhat CR Nezhat FR Ramirez CE et al Laparoscopicradical hysterectomy and laparoscopic assisted vaginal radicalhysterectomy with pelvic and para aortic node dissection JGynecol Surg 19939105ndash120
17 Nezhat C Nezhat F Burrell M Laparoscopically assistedhysterectomy for the management of borderline ovarian tumorA case report J Laparoendosc Surg 19922167ndash169
18 Nezhat C Nezhat F Laparoscopic segmental bladder resec-tion for endometriosis a report of two cases Obstet Gynecol199381882ndash884
19 Nezhat C Nezhat F Pennington E et al Laparoscopic diskexcision and primary repair of the anterior rectal wall for thetreatment of full thickness bowel endometriosis Surg Endosc19948682ndash685
20 Nezhat CH Nezhat F Nezhat C Rottenberg H Laparoscopicrepair of a vesicovaginal fistula a case report Obstet Gynecol199483899ndash901
21 Nezhat CH Bastidas A Pennington E Nezhat F Raga FNezhat C Treatment of type IV rectovaginal fistula treatmentJ Am Assoc Gyn Lap 19985297ndash299
22 Jacobson M Oesterling S Milki A Nezhat CR Laparoscopiccontrol of a leaking inferior mesenteric vessel secondary totrocar injury JSLS 20026389ndash391
23 Jacobson M Osias J Velasco A Charles R Nezhat C Lapa-roscopic repair of a uteroperitoneal fistula JSLS 20037367ndash369
24 Nezhat C Kazerooni T Berker B LaShay N Susan Fernan-dez S Marziali M Laparoscopic management of hepatic endo-metriosis report of Two Cases and review of literature J MinInvas Gynecol 200512196ndash200
25 Nezhat F Nezhat C Pennington E Ambroze W Jr Laparo-scopic segmental resection for infiltrating endometriosis of therecto sigmoid colon a preliminary report Surg Laparosc Endosc19922212ndash216
26 Nezhat C Nezhat F Pennington E Laparoscopic treatmentof lower colorectal and infiltrating rectovaginal septum endome-triosis by the technique of videolaseroscopy Br J Obstet Gynae-col 199299664ndash667
27 Nezhat CH Malik S Nezhat F Nezhat C Laparoscopic ure-teroneocystostomy and vesicopsoas hitch for infiltrative endo-metriosis JSLS 200483ndash7
28 Nezhat CH Nezhat F Freiha F Nezhat C Laparoscopicvesicopsoas hitch for infiltrative ureteral endometriosis FertilSteril 199971376ndash379
29 Nezhat C Nezhat F Incidental appendectomy during video-laseroscopy Am J Obstet Gynecol 1991165559ndash564
30 Nezhat C Childers J Nezhat F et al Major retroperitonealvascular injury during laparoscopic surgery Hum Reprod 199712480ndash483
31 Nezhat C Nezhat F Nezhat CH Laparoscopic Burch proce-dure Operative laparoscopy (minimally invasive surgery) stateof the art J Gynecol Surg 19928111ndash141
JSLS (2006)10275ndash280 279
32 Nezhat F Nezhat C Bess O Nezhat CH Laparoscopic am-putation of a non-communicating rudimentary horn after a hys-teroscopic diagnosis a case study Surg Laparosc Endosc 19944155ndash156
33 Nezhat C Nezhat F Silfen SL et al Laparoscopic myomec-tomy Int J Fertil 199136275ndash280
34 Nezhat C Siegler A Nezhat F Nezhat C Metzger D LucianoA Complications In Operative Gynecologic Laparoscopy Prin-ciples and Techniques New York NY McGraw-Hill 1995287ndash310
35 Nezhat C Siegler A Nezhat F Nezhat C Seidman D LucianoA Complications In Operative Gynecologic Laparoscopy Prin-ciples and Techniques 2nd ed New York NY McGraw-Hill2000365ndash390
36 Nezhat C Nezhat FR Nezhat CH Admon D Endometriosisof the intestine and genitourinary tract In Nezhat CR ed En-dometriosis Advanced Management and Surgical TechniquesSpringer-Verlag 1995
37 Nezhat C Berger GS Nezhat FR Buttram VC Nezhat C edsOperative laparoscopy preventing and managing complica-tions In Nezhat CR ed Endometriosis Advanced Managementand Surgical Techniques Springer-Verlag 1995
38 Nezhat F Nezhat C Allan CJ Metzger DA Sears DL Clinicaland histologic classification of endometriomas implications for amechanism of pathogenesis J Repro Med 199237771ndash776
39 Nezhat C Operative endoscopy will replace almost all openprocedures JSLS 20048101ndash102
40 Pappas TN Jacobs DO Laparoscopic resection for coloncancermdashthe end of the beginning N Engl J Med 2004350(20)2091ndash2092
41 Stanford News Services Media Monitor Stanford ReportFebruary 9 20059
Biography of Camran Nezhat MD FACOG FACS Carter JE
JSLS (2006)10275ndash280280

became ill and required a great deal of medical care Thedoctors involved in her care saved her life
After this incident Camranrsquos father praised the doctors assaviors of their mother The Nezhat brothers thereforegrew up with the knowledge that doctors were highlyvalued in their family and in the world for their life-savingservices This fueled the desire in the Nezhat brothers toenter medicine On reflection because of the significantrole that Mrs Nezhat had in the life of her children andbecause of her steadfast devotion 3 of the Nezhat broth-ers did in fact became gynecological surgeons
During internship and residency at the State University ofNew York under the tutelage of Dr Ronald Batt Camranwas exposed to laparoscopy as a diagnostic tool for infer-tility patients and for those suffering from pelvic painDuring those days laparotomies were performed even formild endometriosis After observing so much postopera-tive distress suffered by laparotomy patients comparedwith patients who had diagnostic laparoscopy Camranthought to himself ldquoWhy shouldnrsquot we treat more surgicalpathologies laparoscopicallyrdquo The hindrance to expand-ing from diagnostic to operative laparoscopy it seemed tohim was not a question of anatomical or physical con-straints but rather was a question of conceptualizing newtechnologies and methodologies He learned that otherinvestigators around the world aware of this potentialwere trying to expand the application of laparoscopyVisualization difficulties from peering crouched overthrough the endoscope with only one eye seemed themost crucial impediment to overcome Thus in recogniz-ing this need and inspired by the earlier pioneersrsquo workthis crucial moment of realization led to a turning point foroperative laparoscopy as Camran embarked on refininglaparoscopic procedures to assist both patients and theoperating team to achieve greater results
At the forefront and important juncture of the discovery ofthe advantages of operating on the images (videolaparos-copy) Camran performed endoscopic surgery off themonitor starting in the late 1970s using very heavy andawkward video camera equipment that had been pro-duced for other uses and which instead he customizedmdashrigged actuallymdashfor use with the laparoscope1ndash6 (Figure 1)
Due to the poor intensity of light sources at times he usedan extra laparoscope connected to the light source only tobring ldquomore light to the subjectrdquo
Operating directly from the visual field utilizing only themonitor transformed the operating room from a ldquoone manbandrdquo into an ldquoorchestrardquo so that assisting surgeons
nurses anesthesiologists students and others could fullyview and therefore more readily assist in and learn thesurgery
After residency Dr Harold Feldman one of Camranrsquosprofessors at that time recommended him for a fellowshipin reproductive endocrinology and infertility under thementorship of Drs Robert Greenblatt Don Gambrell andVirenda Mahesh PhD in Augusta Georgia who werethemselves leaders in reproductive endocrinology andimmunology During this time especially he confirmedhis interest in helping couples suffering from infertility ashe saw their overwhelming joy in experiencing parent-hood after successful treatment He was also motivated toassist those women suffering from other debilitating re-productive disorders
Following this fellowship in 1980 he started his owninfertility practice in Atlanta It was at this time that Cam-ran was able to concentrate more fully on improving andexpanding the use of the videolaparoscopy technique anddesigning new instrumentation Soon he became one ofthe most skilled surgeons Word of mouth began to spreadof this approach and soon his practice began to thrivePatients started arriving from all over the country andabroad
The videolaparoscopy technique was working extraordi-narily well for his infertility patients many of whom hadendometriosis With these excellent clinical results con-firmed Camran set out to share this technique with othercolleagues Along with Dr Scott Crowgey a pediatricianteaching physics at the Georgia Institute of Technologyhe started teaching postgraduate courses in operativelaparoscopy in 1983 It was not until 1986 that he was
Figure 1 Camran Nezhat MD performs endoscopic surgery offthe monitor
Biography of Camran Nezhat MD FACOG FACS Carter JE
JSLS (2006)10275ndash280276
finally able for the first time to publish about successfullaparoscopic treatment of extensive endometriosis2
Camran has always shared his experiences with his col-leagues around the world and has continued to presenthis methods results and his experiences at different med-ical societies and congresses to explain the benefits of thistechnique
He demonstrated that even the most advanced pelvic andabdominal pathologies including advanced stages of en-dometriosis involving bowel bladder ureter diaphragmand liver can be successfully treated by videolaparos-copy2458ndash34 Camran his brothers and others also en-gaged in research to better understand the origin of en-dometriomas39
After achieving clinical success numerous times withvideolaparoscopy Camran stated early on that ldquoif ad-vanced stages of endometriosis can be successfully treatedby videolaparoscopy with the results at least as good as[those of] laparotomy we can perform practically all thesurgical procedures by videolaparoscopyrdquo In his opinionvideolaparoscopy was the method of choice for an oper-ation whenever a cavity exists in the body or when acavity can be created439
Camran is fortunate to have the support of his family Allof his brothers including a psychologist an industrialengineer and 2 physicians have encouraged and inspiredhim His mother who passed on 5 years ago also joinedthem in Atlanta and was an especially significant source ofinspiration Their father had passed on earlier Farr andCeana later joined Camran in his practice
In collaboration with their colleagues such as urologistscolorectal surgeons oncologists cardiothoracic vascularand neurosurgeons the 3 brothers were the forerunnersto perform some of the most advanced procedures lapa-roscopically58ndash34
As they were being recruited by different universities indifferent parts of the country to teach their techniquesStanford University Medical Center was the winner
Ms Linda Meier chairman of the board at Stanford MedicalCenter and Kenneth Bloom CEO of the Stanford MedicalCenter at that time and Claire Mailhot traveled to Atlantato convince Camran and his brothers to move to Palo Altoand start teaching and sharing their experience with per-sons in other surgical disciplines for the purpose of pro-liferation of endoscopic surgery and teaching future gen-erations of surgeons
Upon arriving at Stanford they did collaborate with phy-
sicians in different surgical disciplines and propelled Stan-ford University to the forefront of endoscopic surgery Infact in September 1993 Stanford was one of the fewuniversities to embrace endoscopic surgery The chairmanof surgery at that time was Dr John Niederhauber anopen-minded surgeon specializing in oncological sur-gery After seeing Camran demonstrate the new tech-niques in the operating room Dr Niederhauber became atrue convert and subsequently collaborated with Camranand other colleagues to perform many general surgicalprocedures laparoscopically
Shortly thereafter Dr Niederhauber honored Camran witha clinical professorship in the Department of Surgery atStanford Thus as a result of these initial leaps of faith andin collaboration with those in different disciplines of sur-gery endoscopic surgery at Stanford bound forward
In 1995 Dr Mary Lake Pollan OBGYN DepartmentChairman at Stanford said
Nezhatrsquos contribution was and is unique He has devel-oped such facility with the technique in the operatingroom that he serves as a mentor for other physicianschallenging us to learn the new technique by showing usnot only the art of the possible but the tremendousadvantage minimal access surgery offers When you watchhim operate you have to cast off the excuse lsquothis proce-dure canrsquot be done using video laparoscopyrsquo37 The intro-duction of videolaparoscopy and videolaseroscopy byNezhat allowed the involvement of the entire operatingteam in the surgery Camran along with his brothers notonly performed these procedures elegantly but he wasalso willing to teach any- and everyone who expressed aninterest They are very freely and unselfishly willing toshare their experience and knowledge with the world37
In 2000 the late Kurt Semm35 said
With his genius he widened the operative field creatingnew techniques employing new instruments and appa-ratuses In my opinion with the cooperation of his 2brothers Camran enriched the entire field of surgical lapa-roscopy On June 30 1980 I performed a laparoscopicappendectomy which ultimately opened the door forsurgeons to perform endoscopic surgery especially sincethe appendix was a holy grail of surgery Today DrNezhatrsquos book opens a new door to a whole new era ofendoscopic surgery35
JSLS (2006)10275ndash280 277
In 1995 Alan DeCherney MD Professor Department ofObstetrics and Gynecology UCLA said
In the past decade gynecologic surgery because of en-doscopic surgery has undergone a tremendous revolu-tion There are few cases in the gynecologistrsquos surgicalarmamentarium that cannot be carried out through anendoscopic approach Many of these changes are due tothe courage innovativeness and technical skill of DrCamran Nezhat Just as in Star Trek he dared to go whereno man had gone before and by doing this he opened upunimagined vistas to endoscopic surgeons all over theworld For his courage Camran over the years has suf-fered but persevered3435
Like Bozzini Semm and others Camran too was sub-jected to undue ridicule7 For centuries there has beenresistance to accepting novel ideas even for concepts assimple as washing hands before an operation It costSemmelweis his life while Louis Pasteur was challengedto a duel by a general surgeon Camran too had to sufferyears of struggle and hardship7
For example when in the mid 1980rsquos Camran presented atthe annual meeting of the American Society of Reproduc-tive Medicine (then American Fertility Society) laparo-scopic management of extensive endometriosis and en-dometriomas he was faced with disbelief and accordingto one observer the audience was ready to ldquothrow toma-toesrdquo at him In another instance when Camran and hiscolleagues first performed and stated that bowel surgerycould be accomplished with the laparoscope in the late1980rsquos many were ready to crucify them for making suchclaims It was not until 2004 that New England Journal ofMedicine recommended and encouraged laparoscopicbowel resection40
Camran is testament to the fact that being a pioneer isoften a very lonely place until our beliefs are tested andproven It took 20 years but we are grateful that Camranpreserved and held steadfast to his dreams
We take operating directly off the video monitor or man-aging advanced surgical pathology laparoscopically forgranted but Camran paid dearly for it His declaration thatldquoalmost all laparotomies can be avoidedrdquo was not popu-larly received at the time but created such a shift in thethinking that it sparked a whole new generation of surgi-cal specialists to become inspired opening the door for alldisciplines35ndash37
Camran has been sharing his experiences by teachingpostgraduate courses in advanced laparoscopy and hys-
teroscopy since September 1983 and thousands of phy-sicians have been exposed to his teachings
He especially enjoys being a mentor to young physiciansand scientists who inspire him immensely with their op-timism and enthusiasm
Today Camran continues to contribute to the Art andScience of Surgery He is the immediate past president andsits on the Board of Trustees of the Society of Laparoen-doscopic Surgeons is the Director of the Center for Spe-cial Minimally Invasive Surgery and is Clinical Professorof Surgery and OBGYN at Stanford University School ofMedicine He has published more than 500 articles bookchapters abstracts letters to the editor and video presen-tations He is coauthor of 2 textbooks and has won nu-merous awards and honors from prestigious societies likeACOG ACS ASRM and the Excel Award from the Societyof Laparoendoscopic Surgeons More recent awards in-clude the ACOG 2004 ASRM 2004 and ACOG 2005 He ison the editorial board of the Journal of Fertility andSterility and is an associate editor for the Journal of Societyof Laparoendoscopic Surgeons
To Camran Nezhat we give our thanks for his hard workin sharing with all of us his vision and helping all of us tohelp our patients and improve our skills He has ex-panded our reach and allowed us to provide better carefor our patients He has unselfishly shared his knowledgewith us so we could integrate what he knows and doesinto our work No wonder he has been called the ldquoFatherof Modern Laparoscopyrdquo41
And yet one of the fondest memories is my image of himwalking with his brothers on a crowded New York Citystreet so much just the older brother providing love andsupport to his family He has expanded that familial bondto many who have become part of his laparoscopic familythrough our work with him especially in that extendedfamily known as the Society of Laparoendoscopic Sur-geons
I have to this day on my desk a picture of Paul WetterCamran Nezhat Farr Nezhat and Ceana Nezhat standingwith me in front of the JSLS display to remind me of thecollegiality the honor and the challenge of being a caringphysician in the spirit of our SLS family He has challengedall of us to do better for our patients and we gratefullyaccept that challenge
References
1 Nezhat C Laser laparoscopy for the treatment of endome-triosis Paper presented at Conjoint Meeting of the American
Biography of Camran Nezhat MD FACOG FACS Carter JE
JSLS (2006)10275ndash280278
Society for Reproductive Medicine and the Canadian Fertility andAndrology Society 1985 Toronto Canada
2 Nezhat C Crowgey SR Garrison CP Surgical treatment ofendometriosis via laser laparoscopy Fertil Steril 198645778ndash783
3 Nezhat C Nezhat FR Safe laser endoscopic excision orvaporization of peritoneal endometriosis Fertil Steril 198952149ndash151
4 Nezhat C Nezhat F Nezhat C Operative laparoscopy (min-imally invasive surgery) State of the art J Gynecol Surg 19928111ndash141
5 Nezhat C Nezhat F Silfen SL Videolaseroscopy the CO2laser for advanced operative laparoscopy Obstet Gynecol ClinNorth Am 199118585ndash604
6 Cowley G Hanging up the knife A novel surgical techniquepromises to save patients time money and blood NewsweekFebruary 12 199058ndash59
7 Nezhat F Triumphs and controversies in laparoscopy thepast the present and the future JSLS 200371ndash5
8 Nezhat F Nezhat C Silfen S Fehnel S Laparoscopic treat-ment of ovarian cyst during pregnancy J Laparoendosc Surg19911161ndash164
9 Nezhat C Pennington E Nezhat F Silfen S Laparoscopicallyassisted anterior rectal wall resection and reanastomosis fordeeply infiltrating endometriosis Surg Laparosc Endosc 19911(2)106ndash108
10 Nezhat C Winder WK Nezhat F Laparoscopic removal ofdermoid cysts Obst Gynecol 198973(2)278ndash281
11 Nezhat F Nezhat C Pennington E Laparoscopic proctec-tomy for infiltrating endometriosis of the rectum Fertil Steril1992571129ndash1132
12 Nezhat C Nezhat F Green B Laparoscopic treatment ofobstructed ureter due to endometriosis by resection and ureter-oureterostomy A case report J Urol 1992148865ndash868
13 Nezhat C Burrell M Nezhat F Benigno B Welander CELaparoscopic radical hysterectomy with paraaortic and pelvicnode dissection Am J Obstet Gynecol 1992166864ndash865
14 Nezhat F Nezhat C Levy JS Laparoscopic treatment ofsymptomatic diaphragmatic endometriosis A case report FertilSteril 199258614ndash616
15 Nezhat F Nezhat C Nezhat CH Laparoscopic sacral col-popexy for vaginal wall prolapse Obstet Gynecol 199484885ndash888
16 Nezhat CR Nezhat FR Ramirez CE et al Laparoscopicradical hysterectomy and laparoscopic assisted vaginal radicalhysterectomy with pelvic and para aortic node dissection JGynecol Surg 19939105ndash120
17 Nezhat C Nezhat F Burrell M Laparoscopically assistedhysterectomy for the management of borderline ovarian tumorA case report J Laparoendosc Surg 19922167ndash169
18 Nezhat C Nezhat F Laparoscopic segmental bladder resec-tion for endometriosis a report of two cases Obstet Gynecol199381882ndash884
19 Nezhat C Nezhat F Pennington E et al Laparoscopic diskexcision and primary repair of the anterior rectal wall for thetreatment of full thickness bowel endometriosis Surg Endosc19948682ndash685
20 Nezhat CH Nezhat F Nezhat C Rottenberg H Laparoscopicrepair of a vesicovaginal fistula a case report Obstet Gynecol199483899ndash901
21 Nezhat CH Bastidas A Pennington E Nezhat F Raga FNezhat C Treatment of type IV rectovaginal fistula treatmentJ Am Assoc Gyn Lap 19985297ndash299
22 Jacobson M Oesterling S Milki A Nezhat CR Laparoscopiccontrol of a leaking inferior mesenteric vessel secondary totrocar injury JSLS 20026389ndash391
23 Jacobson M Osias J Velasco A Charles R Nezhat C Lapa-roscopic repair of a uteroperitoneal fistula JSLS 20037367ndash369
24 Nezhat C Kazerooni T Berker B LaShay N Susan Fernan-dez S Marziali M Laparoscopic management of hepatic endo-metriosis report of Two Cases and review of literature J MinInvas Gynecol 200512196ndash200
25 Nezhat F Nezhat C Pennington E Ambroze W Jr Laparo-scopic segmental resection for infiltrating endometriosis of therecto sigmoid colon a preliminary report Surg Laparosc Endosc19922212ndash216
26 Nezhat C Nezhat F Pennington E Laparoscopic treatmentof lower colorectal and infiltrating rectovaginal septum endome-triosis by the technique of videolaseroscopy Br J Obstet Gynae-col 199299664ndash667
27 Nezhat CH Malik S Nezhat F Nezhat C Laparoscopic ure-teroneocystostomy and vesicopsoas hitch for infiltrative endo-metriosis JSLS 200483ndash7
28 Nezhat CH Nezhat F Freiha F Nezhat C Laparoscopicvesicopsoas hitch for infiltrative ureteral endometriosis FertilSteril 199971376ndash379
29 Nezhat C Nezhat F Incidental appendectomy during video-laseroscopy Am J Obstet Gynecol 1991165559ndash564
30 Nezhat C Childers J Nezhat F et al Major retroperitonealvascular injury during laparoscopic surgery Hum Reprod 199712480ndash483
31 Nezhat C Nezhat F Nezhat CH Laparoscopic Burch proce-dure Operative laparoscopy (minimally invasive surgery) stateof the art J Gynecol Surg 19928111ndash141
JSLS (2006)10275ndash280 279
32 Nezhat F Nezhat C Bess O Nezhat CH Laparoscopic am-putation of a non-communicating rudimentary horn after a hys-teroscopic diagnosis a case study Surg Laparosc Endosc 19944155ndash156
33 Nezhat C Nezhat F Silfen SL et al Laparoscopic myomec-tomy Int J Fertil 199136275ndash280
34 Nezhat C Siegler A Nezhat F Nezhat C Metzger D LucianoA Complications In Operative Gynecologic Laparoscopy Prin-ciples and Techniques New York NY McGraw-Hill 1995287ndash310
35 Nezhat C Siegler A Nezhat F Nezhat C Seidman D LucianoA Complications In Operative Gynecologic Laparoscopy Prin-ciples and Techniques 2nd ed New York NY McGraw-Hill2000365ndash390
36 Nezhat C Nezhat FR Nezhat CH Admon D Endometriosisof the intestine and genitourinary tract In Nezhat CR ed En-dometriosis Advanced Management and Surgical TechniquesSpringer-Verlag 1995
37 Nezhat C Berger GS Nezhat FR Buttram VC Nezhat C edsOperative laparoscopy preventing and managing complica-tions In Nezhat CR ed Endometriosis Advanced Managementand Surgical Techniques Springer-Verlag 1995
38 Nezhat F Nezhat C Allan CJ Metzger DA Sears DL Clinicaland histologic classification of endometriomas implications for amechanism of pathogenesis J Repro Med 199237771ndash776
39 Nezhat C Operative endoscopy will replace almost all openprocedures JSLS 20048101ndash102
40 Pappas TN Jacobs DO Laparoscopic resection for coloncancermdashthe end of the beginning N Engl J Med 2004350(20)2091ndash2092
41 Stanford News Services Media Monitor Stanford ReportFebruary 9 20059
Biography of Camran Nezhat MD FACOG FACS Carter JE
JSLS (2006)10275ndash280280

finally able for the first time to publish about successfullaparoscopic treatment of extensive endometriosis2
Camran has always shared his experiences with his col-leagues around the world and has continued to presenthis methods results and his experiences at different med-ical societies and congresses to explain the benefits of thistechnique
He demonstrated that even the most advanced pelvic andabdominal pathologies including advanced stages of en-dometriosis involving bowel bladder ureter diaphragmand liver can be successfully treated by videolaparos-copy2458ndash34 Camran his brothers and others also en-gaged in research to better understand the origin of en-dometriomas39
After achieving clinical success numerous times withvideolaparoscopy Camran stated early on that ldquoif ad-vanced stages of endometriosis can be successfully treatedby videolaparoscopy with the results at least as good as[those of] laparotomy we can perform practically all thesurgical procedures by videolaparoscopyrdquo In his opinionvideolaparoscopy was the method of choice for an oper-ation whenever a cavity exists in the body or when acavity can be created439
Camran is fortunate to have the support of his family Allof his brothers including a psychologist an industrialengineer and 2 physicians have encouraged and inspiredhim His mother who passed on 5 years ago also joinedthem in Atlanta and was an especially significant source ofinspiration Their father had passed on earlier Farr andCeana later joined Camran in his practice
In collaboration with their colleagues such as urologistscolorectal surgeons oncologists cardiothoracic vascularand neurosurgeons the 3 brothers were the forerunnersto perform some of the most advanced procedures lapa-roscopically58ndash34
As they were being recruited by different universities indifferent parts of the country to teach their techniquesStanford University Medical Center was the winner
Ms Linda Meier chairman of the board at Stanford MedicalCenter and Kenneth Bloom CEO of the Stanford MedicalCenter at that time and Claire Mailhot traveled to Atlantato convince Camran and his brothers to move to Palo Altoand start teaching and sharing their experience with per-sons in other surgical disciplines for the purpose of pro-liferation of endoscopic surgery and teaching future gen-erations of surgeons
Upon arriving at Stanford they did collaborate with phy-
sicians in different surgical disciplines and propelled Stan-ford University to the forefront of endoscopic surgery Infact in September 1993 Stanford was one of the fewuniversities to embrace endoscopic surgery The chairmanof surgery at that time was Dr John Niederhauber anopen-minded surgeon specializing in oncological sur-gery After seeing Camran demonstrate the new tech-niques in the operating room Dr Niederhauber became atrue convert and subsequently collaborated with Camranand other colleagues to perform many general surgicalprocedures laparoscopically
Shortly thereafter Dr Niederhauber honored Camran witha clinical professorship in the Department of Surgery atStanford Thus as a result of these initial leaps of faith andin collaboration with those in different disciplines of sur-gery endoscopic surgery at Stanford bound forward
In 1995 Dr Mary Lake Pollan OBGYN DepartmentChairman at Stanford said
Nezhatrsquos contribution was and is unique He has devel-oped such facility with the technique in the operatingroom that he serves as a mentor for other physicianschallenging us to learn the new technique by showing usnot only the art of the possible but the tremendousadvantage minimal access surgery offers When you watchhim operate you have to cast off the excuse lsquothis proce-dure canrsquot be done using video laparoscopyrsquo37 The intro-duction of videolaparoscopy and videolaseroscopy byNezhat allowed the involvement of the entire operatingteam in the surgery Camran along with his brothers notonly performed these procedures elegantly but he wasalso willing to teach any- and everyone who expressed aninterest They are very freely and unselfishly willing toshare their experience and knowledge with the world37
In 2000 the late Kurt Semm35 said
With his genius he widened the operative field creatingnew techniques employing new instruments and appa-ratuses In my opinion with the cooperation of his 2brothers Camran enriched the entire field of surgical lapa-roscopy On June 30 1980 I performed a laparoscopicappendectomy which ultimately opened the door forsurgeons to perform endoscopic surgery especially sincethe appendix was a holy grail of surgery Today DrNezhatrsquos book opens a new door to a whole new era ofendoscopic surgery35
JSLS (2006)10275ndash280 277
In 1995 Alan DeCherney MD Professor Department ofObstetrics and Gynecology UCLA said
In the past decade gynecologic surgery because of en-doscopic surgery has undergone a tremendous revolu-tion There are few cases in the gynecologistrsquos surgicalarmamentarium that cannot be carried out through anendoscopic approach Many of these changes are due tothe courage innovativeness and technical skill of DrCamran Nezhat Just as in Star Trek he dared to go whereno man had gone before and by doing this he opened upunimagined vistas to endoscopic surgeons all over theworld For his courage Camran over the years has suf-fered but persevered3435
Like Bozzini Semm and others Camran too was sub-jected to undue ridicule7 For centuries there has beenresistance to accepting novel ideas even for concepts assimple as washing hands before an operation It costSemmelweis his life while Louis Pasteur was challengedto a duel by a general surgeon Camran too had to sufferyears of struggle and hardship7
For example when in the mid 1980rsquos Camran presented atthe annual meeting of the American Society of Reproduc-tive Medicine (then American Fertility Society) laparo-scopic management of extensive endometriosis and en-dometriomas he was faced with disbelief and accordingto one observer the audience was ready to ldquothrow toma-toesrdquo at him In another instance when Camran and hiscolleagues first performed and stated that bowel surgerycould be accomplished with the laparoscope in the late1980rsquos many were ready to crucify them for making suchclaims It was not until 2004 that New England Journal ofMedicine recommended and encouraged laparoscopicbowel resection40
Camran is testament to the fact that being a pioneer isoften a very lonely place until our beliefs are tested andproven It took 20 years but we are grateful that Camranpreserved and held steadfast to his dreams
We take operating directly off the video monitor or man-aging advanced surgical pathology laparoscopically forgranted but Camran paid dearly for it His declaration thatldquoalmost all laparotomies can be avoidedrdquo was not popu-larly received at the time but created such a shift in thethinking that it sparked a whole new generation of surgi-cal specialists to become inspired opening the door for alldisciplines35ndash37
Camran has been sharing his experiences by teachingpostgraduate courses in advanced laparoscopy and hys-
teroscopy since September 1983 and thousands of phy-sicians have been exposed to his teachings
He especially enjoys being a mentor to young physiciansand scientists who inspire him immensely with their op-timism and enthusiasm
Today Camran continues to contribute to the Art andScience of Surgery He is the immediate past president andsits on the Board of Trustees of the Society of Laparoen-doscopic Surgeons is the Director of the Center for Spe-cial Minimally Invasive Surgery and is Clinical Professorof Surgery and OBGYN at Stanford University School ofMedicine He has published more than 500 articles bookchapters abstracts letters to the editor and video presen-tations He is coauthor of 2 textbooks and has won nu-merous awards and honors from prestigious societies likeACOG ACS ASRM and the Excel Award from the Societyof Laparoendoscopic Surgeons More recent awards in-clude the ACOG 2004 ASRM 2004 and ACOG 2005 He ison the editorial board of the Journal of Fertility andSterility and is an associate editor for the Journal of Societyof Laparoendoscopic Surgeons
To Camran Nezhat we give our thanks for his hard workin sharing with all of us his vision and helping all of us tohelp our patients and improve our skills He has ex-panded our reach and allowed us to provide better carefor our patients He has unselfishly shared his knowledgewith us so we could integrate what he knows and doesinto our work No wonder he has been called the ldquoFatherof Modern Laparoscopyrdquo41
And yet one of the fondest memories is my image of himwalking with his brothers on a crowded New York Citystreet so much just the older brother providing love andsupport to his family He has expanded that familial bondto many who have become part of his laparoscopic familythrough our work with him especially in that extendedfamily known as the Society of Laparoendoscopic Sur-geons
I have to this day on my desk a picture of Paul WetterCamran Nezhat Farr Nezhat and Ceana Nezhat standingwith me in front of the JSLS display to remind me of thecollegiality the honor and the challenge of being a caringphysician in the spirit of our SLS family He has challengedall of us to do better for our patients and we gratefullyaccept that challenge
References
1 Nezhat C Laser laparoscopy for the treatment of endome-triosis Paper presented at Conjoint Meeting of the American
Biography of Camran Nezhat MD FACOG FACS Carter JE
JSLS (2006)10275ndash280278
Society for Reproductive Medicine and the Canadian Fertility andAndrology Society 1985 Toronto Canada
2 Nezhat C Crowgey SR Garrison CP Surgical treatment ofendometriosis via laser laparoscopy Fertil Steril 198645778ndash783
3 Nezhat C Nezhat FR Safe laser endoscopic excision orvaporization of peritoneal endometriosis Fertil Steril 198952149ndash151
4 Nezhat C Nezhat F Nezhat C Operative laparoscopy (min-imally invasive surgery) State of the art J Gynecol Surg 19928111ndash141
5 Nezhat C Nezhat F Silfen SL Videolaseroscopy the CO2laser for advanced operative laparoscopy Obstet Gynecol ClinNorth Am 199118585ndash604
6 Cowley G Hanging up the knife A novel surgical techniquepromises to save patients time money and blood NewsweekFebruary 12 199058ndash59
7 Nezhat F Triumphs and controversies in laparoscopy thepast the present and the future JSLS 200371ndash5
8 Nezhat F Nezhat C Silfen S Fehnel S Laparoscopic treat-ment of ovarian cyst during pregnancy J Laparoendosc Surg19911161ndash164
9 Nezhat C Pennington E Nezhat F Silfen S Laparoscopicallyassisted anterior rectal wall resection and reanastomosis fordeeply infiltrating endometriosis Surg Laparosc Endosc 19911(2)106ndash108
10 Nezhat C Winder WK Nezhat F Laparoscopic removal ofdermoid cysts Obst Gynecol 198973(2)278ndash281
11 Nezhat F Nezhat C Pennington E Laparoscopic proctec-tomy for infiltrating endometriosis of the rectum Fertil Steril1992571129ndash1132
12 Nezhat C Nezhat F Green B Laparoscopic treatment ofobstructed ureter due to endometriosis by resection and ureter-oureterostomy A case report J Urol 1992148865ndash868
13 Nezhat C Burrell M Nezhat F Benigno B Welander CELaparoscopic radical hysterectomy with paraaortic and pelvicnode dissection Am J Obstet Gynecol 1992166864ndash865
14 Nezhat F Nezhat C Levy JS Laparoscopic treatment ofsymptomatic diaphragmatic endometriosis A case report FertilSteril 199258614ndash616
15 Nezhat F Nezhat C Nezhat CH Laparoscopic sacral col-popexy for vaginal wall prolapse Obstet Gynecol 199484885ndash888
16 Nezhat CR Nezhat FR Ramirez CE et al Laparoscopicradical hysterectomy and laparoscopic assisted vaginal radicalhysterectomy with pelvic and para aortic node dissection JGynecol Surg 19939105ndash120
17 Nezhat C Nezhat F Burrell M Laparoscopically assistedhysterectomy for the management of borderline ovarian tumorA case report J Laparoendosc Surg 19922167ndash169
18 Nezhat C Nezhat F Laparoscopic segmental bladder resec-tion for endometriosis a report of two cases Obstet Gynecol199381882ndash884
19 Nezhat C Nezhat F Pennington E et al Laparoscopic diskexcision and primary repair of the anterior rectal wall for thetreatment of full thickness bowel endometriosis Surg Endosc19948682ndash685
20 Nezhat CH Nezhat F Nezhat C Rottenberg H Laparoscopicrepair of a vesicovaginal fistula a case report Obstet Gynecol199483899ndash901
21 Nezhat CH Bastidas A Pennington E Nezhat F Raga FNezhat C Treatment of type IV rectovaginal fistula treatmentJ Am Assoc Gyn Lap 19985297ndash299
22 Jacobson M Oesterling S Milki A Nezhat CR Laparoscopiccontrol of a leaking inferior mesenteric vessel secondary totrocar injury JSLS 20026389ndash391
23 Jacobson M Osias J Velasco A Charles R Nezhat C Lapa-roscopic repair of a uteroperitoneal fistula JSLS 20037367ndash369
24 Nezhat C Kazerooni T Berker B LaShay N Susan Fernan-dez S Marziali M Laparoscopic management of hepatic endo-metriosis report of Two Cases and review of literature J MinInvas Gynecol 200512196ndash200
25 Nezhat F Nezhat C Pennington E Ambroze W Jr Laparo-scopic segmental resection for infiltrating endometriosis of therecto sigmoid colon a preliminary report Surg Laparosc Endosc19922212ndash216
26 Nezhat C Nezhat F Pennington E Laparoscopic treatmentof lower colorectal and infiltrating rectovaginal septum endome-triosis by the technique of videolaseroscopy Br J Obstet Gynae-col 199299664ndash667
27 Nezhat CH Malik S Nezhat F Nezhat C Laparoscopic ure-teroneocystostomy and vesicopsoas hitch for infiltrative endo-metriosis JSLS 200483ndash7
28 Nezhat CH Nezhat F Freiha F Nezhat C Laparoscopicvesicopsoas hitch for infiltrative ureteral endometriosis FertilSteril 199971376ndash379
29 Nezhat C Nezhat F Incidental appendectomy during video-laseroscopy Am J Obstet Gynecol 1991165559ndash564
30 Nezhat C Childers J Nezhat F et al Major retroperitonealvascular injury during laparoscopic surgery Hum Reprod 199712480ndash483
31 Nezhat C Nezhat F Nezhat CH Laparoscopic Burch proce-dure Operative laparoscopy (minimally invasive surgery) stateof the art J Gynecol Surg 19928111ndash141
JSLS (2006)10275ndash280 279
32 Nezhat F Nezhat C Bess O Nezhat CH Laparoscopic am-putation of a non-communicating rudimentary horn after a hys-teroscopic diagnosis a case study Surg Laparosc Endosc 19944155ndash156
33 Nezhat C Nezhat F Silfen SL et al Laparoscopic myomec-tomy Int J Fertil 199136275ndash280
34 Nezhat C Siegler A Nezhat F Nezhat C Metzger D LucianoA Complications In Operative Gynecologic Laparoscopy Prin-ciples and Techniques New York NY McGraw-Hill 1995287ndash310
35 Nezhat C Siegler A Nezhat F Nezhat C Seidman D LucianoA Complications In Operative Gynecologic Laparoscopy Prin-ciples and Techniques 2nd ed New York NY McGraw-Hill2000365ndash390
36 Nezhat C Nezhat FR Nezhat CH Admon D Endometriosisof the intestine and genitourinary tract In Nezhat CR ed En-dometriosis Advanced Management and Surgical TechniquesSpringer-Verlag 1995
37 Nezhat C Berger GS Nezhat FR Buttram VC Nezhat C edsOperative laparoscopy preventing and managing complica-tions In Nezhat CR ed Endometriosis Advanced Managementand Surgical Techniques Springer-Verlag 1995
38 Nezhat F Nezhat C Allan CJ Metzger DA Sears DL Clinicaland histologic classification of endometriomas implications for amechanism of pathogenesis J Repro Med 199237771ndash776
39 Nezhat C Operative endoscopy will replace almost all openprocedures JSLS 20048101ndash102
40 Pappas TN Jacobs DO Laparoscopic resection for coloncancermdashthe end of the beginning N Engl J Med 2004350(20)2091ndash2092
41 Stanford News Services Media Monitor Stanford ReportFebruary 9 20059
Biography of Camran Nezhat MD FACOG FACS Carter JE
JSLS (2006)10275ndash280280

In 1995 Alan DeCherney MD Professor Department ofObstetrics and Gynecology UCLA said
In the past decade gynecologic surgery because of en-doscopic surgery has undergone a tremendous revolu-tion There are few cases in the gynecologistrsquos surgicalarmamentarium that cannot be carried out through anendoscopic approach Many of these changes are due tothe courage innovativeness and technical skill of DrCamran Nezhat Just as in Star Trek he dared to go whereno man had gone before and by doing this he opened upunimagined vistas to endoscopic surgeons all over theworld For his courage Camran over the years has suf-fered but persevered3435
Like Bozzini Semm and others Camran too was sub-jected to undue ridicule7 For centuries there has beenresistance to accepting novel ideas even for concepts assimple as washing hands before an operation It costSemmelweis his life while Louis Pasteur was challengedto a duel by a general surgeon Camran too had to sufferyears of struggle and hardship7
For example when in the mid 1980rsquos Camran presented atthe annual meeting of the American Society of Reproduc-tive Medicine (then American Fertility Society) laparo-scopic management of extensive endometriosis and en-dometriomas he was faced with disbelief and accordingto one observer the audience was ready to ldquothrow toma-toesrdquo at him In another instance when Camran and hiscolleagues first performed and stated that bowel surgerycould be accomplished with the laparoscope in the late1980rsquos many were ready to crucify them for making suchclaims It was not until 2004 that New England Journal ofMedicine recommended and encouraged laparoscopicbowel resection40
Camran is testament to the fact that being a pioneer isoften a very lonely place until our beliefs are tested andproven It took 20 years but we are grateful that Camranpreserved and held steadfast to his dreams
We take operating directly off the video monitor or man-aging advanced surgical pathology laparoscopically forgranted but Camran paid dearly for it His declaration thatldquoalmost all laparotomies can be avoidedrdquo was not popu-larly received at the time but created such a shift in thethinking that it sparked a whole new generation of surgi-cal specialists to become inspired opening the door for alldisciplines35ndash37
Camran has been sharing his experiences by teachingpostgraduate courses in advanced laparoscopy and hys-
teroscopy since September 1983 and thousands of phy-sicians have been exposed to his teachings
He especially enjoys being a mentor to young physiciansand scientists who inspire him immensely with their op-timism and enthusiasm
Today Camran continues to contribute to the Art andScience of Surgery He is the immediate past president andsits on the Board of Trustees of the Society of Laparoen-doscopic Surgeons is the Director of the Center for Spe-cial Minimally Invasive Surgery and is Clinical Professorof Surgery and OBGYN at Stanford University School ofMedicine He has published more than 500 articles bookchapters abstracts letters to the editor and video presen-tations He is coauthor of 2 textbooks and has won nu-merous awards and honors from prestigious societies likeACOG ACS ASRM and the Excel Award from the Societyof Laparoendoscopic Surgeons More recent awards in-clude the ACOG 2004 ASRM 2004 and ACOG 2005 He ison the editorial board of the Journal of Fertility andSterility and is an associate editor for the Journal of Societyof Laparoendoscopic Surgeons
To Camran Nezhat we give our thanks for his hard workin sharing with all of us his vision and helping all of us tohelp our patients and improve our skills He has ex-panded our reach and allowed us to provide better carefor our patients He has unselfishly shared his knowledgewith us so we could integrate what he knows and doesinto our work No wonder he has been called the ldquoFatherof Modern Laparoscopyrdquo41
And yet one of the fondest memories is my image of himwalking with his brothers on a crowded New York Citystreet so much just the older brother providing love andsupport to his family He has expanded that familial bondto many who have become part of his laparoscopic familythrough our work with him especially in that extendedfamily known as the Society of Laparoendoscopic Sur-geons
I have to this day on my desk a picture of Paul WetterCamran Nezhat Farr Nezhat and Ceana Nezhat standingwith me in front of the JSLS display to remind me of thecollegiality the honor and the challenge of being a caringphysician in the spirit of our SLS family He has challengedall of us to do better for our patients and we gratefullyaccept that challenge
References
1 Nezhat C Laser laparoscopy for the treatment of endome-triosis Paper presented at Conjoint Meeting of the American
Biography of Camran Nezhat MD FACOG FACS Carter JE
JSLS (2006)10275ndash280278
Society for Reproductive Medicine and the Canadian Fertility andAndrology Society 1985 Toronto Canada
2 Nezhat C Crowgey SR Garrison CP Surgical treatment ofendometriosis via laser laparoscopy Fertil Steril 198645778ndash783
3 Nezhat C Nezhat FR Safe laser endoscopic excision orvaporization of peritoneal endometriosis Fertil Steril 198952149ndash151
4 Nezhat C Nezhat F Nezhat C Operative laparoscopy (min-imally invasive surgery) State of the art J Gynecol Surg 19928111ndash141
5 Nezhat C Nezhat F Silfen SL Videolaseroscopy the CO2laser for advanced operative laparoscopy Obstet Gynecol ClinNorth Am 199118585ndash604
6 Cowley G Hanging up the knife A novel surgical techniquepromises to save patients time money and blood NewsweekFebruary 12 199058ndash59
7 Nezhat F Triumphs and controversies in laparoscopy thepast the present and the future JSLS 200371ndash5
8 Nezhat F Nezhat C Silfen S Fehnel S Laparoscopic treat-ment of ovarian cyst during pregnancy J Laparoendosc Surg19911161ndash164
9 Nezhat C Pennington E Nezhat F Silfen S Laparoscopicallyassisted anterior rectal wall resection and reanastomosis fordeeply infiltrating endometriosis Surg Laparosc Endosc 19911(2)106ndash108
10 Nezhat C Winder WK Nezhat F Laparoscopic removal ofdermoid cysts Obst Gynecol 198973(2)278ndash281
11 Nezhat F Nezhat C Pennington E Laparoscopic proctec-tomy for infiltrating endometriosis of the rectum Fertil Steril1992571129ndash1132
12 Nezhat C Nezhat F Green B Laparoscopic treatment ofobstructed ureter due to endometriosis by resection and ureter-oureterostomy A case report J Urol 1992148865ndash868
13 Nezhat C Burrell M Nezhat F Benigno B Welander CELaparoscopic radical hysterectomy with paraaortic and pelvicnode dissection Am J Obstet Gynecol 1992166864ndash865
14 Nezhat F Nezhat C Levy JS Laparoscopic treatment ofsymptomatic diaphragmatic endometriosis A case report FertilSteril 199258614ndash616
15 Nezhat F Nezhat C Nezhat CH Laparoscopic sacral col-popexy for vaginal wall prolapse Obstet Gynecol 199484885ndash888
16 Nezhat CR Nezhat FR Ramirez CE et al Laparoscopicradical hysterectomy and laparoscopic assisted vaginal radicalhysterectomy with pelvic and para aortic node dissection JGynecol Surg 19939105ndash120
17 Nezhat C Nezhat F Burrell M Laparoscopically assistedhysterectomy for the management of borderline ovarian tumorA case report J Laparoendosc Surg 19922167ndash169
18 Nezhat C Nezhat F Laparoscopic segmental bladder resec-tion for endometriosis a report of two cases Obstet Gynecol199381882ndash884
19 Nezhat C Nezhat F Pennington E et al Laparoscopic diskexcision and primary repair of the anterior rectal wall for thetreatment of full thickness bowel endometriosis Surg Endosc19948682ndash685
20 Nezhat CH Nezhat F Nezhat C Rottenberg H Laparoscopicrepair of a vesicovaginal fistula a case report Obstet Gynecol199483899ndash901
21 Nezhat CH Bastidas A Pennington E Nezhat F Raga FNezhat C Treatment of type IV rectovaginal fistula treatmentJ Am Assoc Gyn Lap 19985297ndash299
22 Jacobson M Oesterling S Milki A Nezhat CR Laparoscopiccontrol of a leaking inferior mesenteric vessel secondary totrocar injury JSLS 20026389ndash391
23 Jacobson M Osias J Velasco A Charles R Nezhat C Lapa-roscopic repair of a uteroperitoneal fistula JSLS 20037367ndash369
24 Nezhat C Kazerooni T Berker B LaShay N Susan Fernan-dez S Marziali M Laparoscopic management of hepatic endo-metriosis report of Two Cases and review of literature J MinInvas Gynecol 200512196ndash200
25 Nezhat F Nezhat C Pennington E Ambroze W Jr Laparo-scopic segmental resection for infiltrating endometriosis of therecto sigmoid colon a preliminary report Surg Laparosc Endosc19922212ndash216
26 Nezhat C Nezhat F Pennington E Laparoscopic treatmentof lower colorectal and infiltrating rectovaginal septum endome-triosis by the technique of videolaseroscopy Br J Obstet Gynae-col 199299664ndash667
27 Nezhat CH Malik S Nezhat F Nezhat C Laparoscopic ure-teroneocystostomy and vesicopsoas hitch for infiltrative endo-metriosis JSLS 200483ndash7
28 Nezhat CH Nezhat F Freiha F Nezhat C Laparoscopicvesicopsoas hitch for infiltrative ureteral endometriosis FertilSteril 199971376ndash379
29 Nezhat C Nezhat F Incidental appendectomy during video-laseroscopy Am J Obstet Gynecol 1991165559ndash564
30 Nezhat C Childers J Nezhat F et al Major retroperitonealvascular injury during laparoscopic surgery Hum Reprod 199712480ndash483
31 Nezhat C Nezhat F Nezhat CH Laparoscopic Burch proce-dure Operative laparoscopy (minimally invasive surgery) stateof the art J Gynecol Surg 19928111ndash141
JSLS (2006)10275ndash280 279
32 Nezhat F Nezhat C Bess O Nezhat CH Laparoscopic am-putation of a non-communicating rudimentary horn after a hys-teroscopic diagnosis a case study Surg Laparosc Endosc 19944155ndash156
33 Nezhat C Nezhat F Silfen SL et al Laparoscopic myomec-tomy Int J Fertil 199136275ndash280
34 Nezhat C Siegler A Nezhat F Nezhat C Metzger D LucianoA Complications In Operative Gynecologic Laparoscopy Prin-ciples and Techniques New York NY McGraw-Hill 1995287ndash310
35 Nezhat C Siegler A Nezhat F Nezhat C Seidman D LucianoA Complications In Operative Gynecologic Laparoscopy Prin-ciples and Techniques 2nd ed New York NY McGraw-Hill2000365ndash390
36 Nezhat C Nezhat FR Nezhat CH Admon D Endometriosisof the intestine and genitourinary tract In Nezhat CR ed En-dometriosis Advanced Management and Surgical TechniquesSpringer-Verlag 1995
37 Nezhat C Berger GS Nezhat FR Buttram VC Nezhat C edsOperative laparoscopy preventing and managing complica-tions In Nezhat CR ed Endometriosis Advanced Managementand Surgical Techniques Springer-Verlag 1995
38 Nezhat F Nezhat C Allan CJ Metzger DA Sears DL Clinicaland histologic classification of endometriomas implications for amechanism of pathogenesis J Repro Med 199237771ndash776
39 Nezhat C Operative endoscopy will replace almost all openprocedures JSLS 20048101ndash102
40 Pappas TN Jacobs DO Laparoscopic resection for coloncancermdashthe end of the beginning N Engl J Med 2004350(20)2091ndash2092
41 Stanford News Services Media Monitor Stanford ReportFebruary 9 20059
Biography of Camran Nezhat MD FACOG FACS Carter JE
JSLS (2006)10275ndash280280

Society for Reproductive Medicine and the Canadian Fertility andAndrology Society 1985 Toronto Canada
2 Nezhat C Crowgey SR Garrison CP Surgical treatment ofendometriosis via laser laparoscopy Fertil Steril 198645778ndash783
3 Nezhat C Nezhat FR Safe laser endoscopic excision orvaporization of peritoneal endometriosis Fertil Steril 198952149ndash151
4 Nezhat C Nezhat F Nezhat C Operative laparoscopy (min-imally invasive surgery) State of the art J Gynecol Surg 19928111ndash141
5 Nezhat C Nezhat F Silfen SL Videolaseroscopy the CO2laser for advanced operative laparoscopy Obstet Gynecol ClinNorth Am 199118585ndash604
6 Cowley G Hanging up the knife A novel surgical techniquepromises to save patients time money and blood NewsweekFebruary 12 199058ndash59
7 Nezhat F Triumphs and controversies in laparoscopy thepast the present and the future JSLS 200371ndash5
8 Nezhat F Nezhat C Silfen S Fehnel S Laparoscopic treat-ment of ovarian cyst during pregnancy J Laparoendosc Surg19911161ndash164
9 Nezhat C Pennington E Nezhat F Silfen S Laparoscopicallyassisted anterior rectal wall resection and reanastomosis fordeeply infiltrating endometriosis Surg Laparosc Endosc 19911(2)106ndash108
10 Nezhat C Winder WK Nezhat F Laparoscopic removal ofdermoid cysts Obst Gynecol 198973(2)278ndash281
11 Nezhat F Nezhat C Pennington E Laparoscopic proctec-tomy for infiltrating endometriosis of the rectum Fertil Steril1992571129ndash1132
12 Nezhat C Nezhat F Green B Laparoscopic treatment ofobstructed ureter due to endometriosis by resection and ureter-oureterostomy A case report J Urol 1992148865ndash868
13 Nezhat C Burrell M Nezhat F Benigno B Welander CELaparoscopic radical hysterectomy with paraaortic and pelvicnode dissection Am J Obstet Gynecol 1992166864ndash865
14 Nezhat F Nezhat C Levy JS Laparoscopic treatment ofsymptomatic diaphragmatic endometriosis A case report FertilSteril 199258614ndash616
15 Nezhat F Nezhat C Nezhat CH Laparoscopic sacral col-popexy for vaginal wall prolapse Obstet Gynecol 199484885ndash888
16 Nezhat CR Nezhat FR Ramirez CE et al Laparoscopicradical hysterectomy and laparoscopic assisted vaginal radicalhysterectomy with pelvic and para aortic node dissection JGynecol Surg 19939105ndash120
17 Nezhat C Nezhat F Burrell M Laparoscopically assistedhysterectomy for the management of borderline ovarian tumorA case report J Laparoendosc Surg 19922167ndash169
18 Nezhat C Nezhat F Laparoscopic segmental bladder resec-tion for endometriosis a report of two cases Obstet Gynecol199381882ndash884
19 Nezhat C Nezhat F Pennington E et al Laparoscopic diskexcision and primary repair of the anterior rectal wall for thetreatment of full thickness bowel endometriosis Surg Endosc19948682ndash685
20 Nezhat CH Nezhat F Nezhat C Rottenberg H Laparoscopicrepair of a vesicovaginal fistula a case report Obstet Gynecol199483899ndash901
21 Nezhat CH Bastidas A Pennington E Nezhat F Raga FNezhat C Treatment of type IV rectovaginal fistula treatmentJ Am Assoc Gyn Lap 19985297ndash299
22 Jacobson M Oesterling S Milki A Nezhat CR Laparoscopiccontrol of a leaking inferior mesenteric vessel secondary totrocar injury JSLS 20026389ndash391
23 Jacobson M Osias J Velasco A Charles R Nezhat C Lapa-roscopic repair of a uteroperitoneal fistula JSLS 20037367ndash369
24 Nezhat C Kazerooni T Berker B LaShay N Susan Fernan-dez S Marziali M Laparoscopic management of hepatic endo-metriosis report of Two Cases and review of literature J MinInvas Gynecol 200512196ndash200
25 Nezhat F Nezhat C Pennington E Ambroze W Jr Laparo-scopic segmental resection for infiltrating endometriosis of therecto sigmoid colon a preliminary report Surg Laparosc Endosc19922212ndash216
26 Nezhat C Nezhat F Pennington E Laparoscopic treatmentof lower colorectal and infiltrating rectovaginal septum endome-triosis by the technique of videolaseroscopy Br J Obstet Gynae-col 199299664ndash667
27 Nezhat CH Malik S Nezhat F Nezhat C Laparoscopic ure-teroneocystostomy and vesicopsoas hitch for infiltrative endo-metriosis JSLS 200483ndash7
28 Nezhat CH Nezhat F Freiha F Nezhat C Laparoscopicvesicopsoas hitch for infiltrative ureteral endometriosis FertilSteril 199971376ndash379
29 Nezhat C Nezhat F Incidental appendectomy during video-laseroscopy Am J Obstet Gynecol 1991165559ndash564
30 Nezhat C Childers J Nezhat F et al Major retroperitonealvascular injury during laparoscopic surgery Hum Reprod 199712480ndash483
31 Nezhat C Nezhat F Nezhat CH Laparoscopic Burch proce-dure Operative laparoscopy (minimally invasive surgery) stateof the art J Gynecol Surg 19928111ndash141
JSLS (2006)10275ndash280 279
32 Nezhat F Nezhat C Bess O Nezhat CH Laparoscopic am-putation of a non-communicating rudimentary horn after a hys-teroscopic diagnosis a case study Surg Laparosc Endosc 19944155ndash156
33 Nezhat C Nezhat F Silfen SL et al Laparoscopic myomec-tomy Int J Fertil 199136275ndash280
34 Nezhat C Siegler A Nezhat F Nezhat C Metzger D LucianoA Complications In Operative Gynecologic Laparoscopy Prin-ciples and Techniques New York NY McGraw-Hill 1995287ndash310
35 Nezhat C Siegler A Nezhat F Nezhat C Seidman D LucianoA Complications In Operative Gynecologic Laparoscopy Prin-ciples and Techniques 2nd ed New York NY McGraw-Hill2000365ndash390
36 Nezhat C Nezhat FR Nezhat CH Admon D Endometriosisof the intestine and genitourinary tract In Nezhat CR ed En-dometriosis Advanced Management and Surgical TechniquesSpringer-Verlag 1995
37 Nezhat C Berger GS Nezhat FR Buttram VC Nezhat C edsOperative laparoscopy preventing and managing complica-tions In Nezhat CR ed Endometriosis Advanced Managementand Surgical Techniques Springer-Verlag 1995
38 Nezhat F Nezhat C Allan CJ Metzger DA Sears DL Clinicaland histologic classification of endometriomas implications for amechanism of pathogenesis J Repro Med 199237771ndash776
39 Nezhat C Operative endoscopy will replace almost all openprocedures JSLS 20048101ndash102
40 Pappas TN Jacobs DO Laparoscopic resection for coloncancermdashthe end of the beginning N Engl J Med 2004350(20)2091ndash2092
41 Stanford News Services Media Monitor Stanford ReportFebruary 9 20059
Biography of Camran Nezhat MD FACOG FACS Carter JE
JSLS (2006)10275ndash280280

32 Nezhat F Nezhat C Bess O Nezhat CH Laparoscopic am-putation of a non-communicating rudimentary horn after a hys-teroscopic diagnosis a case study Surg Laparosc Endosc 19944155ndash156
33 Nezhat C Nezhat F Silfen SL et al Laparoscopic myomec-tomy Int J Fertil 199136275ndash280
34 Nezhat C Siegler A Nezhat F Nezhat C Metzger D LucianoA Complications In Operative Gynecologic Laparoscopy Prin-ciples and Techniques New York NY McGraw-Hill 1995287ndash310
35 Nezhat C Siegler A Nezhat F Nezhat C Seidman D LucianoA Complications In Operative Gynecologic Laparoscopy Prin-ciples and Techniques 2nd ed New York NY McGraw-Hill2000365ndash390
36 Nezhat C Nezhat FR Nezhat CH Admon D Endometriosisof the intestine and genitourinary tract In Nezhat CR ed En-dometriosis Advanced Management and Surgical TechniquesSpringer-Verlag 1995
37 Nezhat C Berger GS Nezhat FR Buttram VC Nezhat C edsOperative laparoscopy preventing and managing complica-tions In Nezhat CR ed Endometriosis Advanced Managementand Surgical Techniques Springer-Verlag 1995
38 Nezhat F Nezhat C Allan CJ Metzger DA Sears DL Clinicaland histologic classification of endometriomas implications for amechanism of pathogenesis J Repro Med 199237771ndash776
39 Nezhat C Operative endoscopy will replace almost all openprocedures JSLS 20048101ndash102
40 Pappas TN Jacobs DO Laparoscopic resection for coloncancermdashthe end of the beginning N Engl J Med 2004350(20)2091ndash2092
41 Stanford News Services Media Monitor Stanford ReportFebruary 9 20059
Biography of Camran Nezhat MD FACOG FACS Carter JE
JSLS (2006)10275ndash280280