Bioelectrical impedance analysis-part I review of principle and methods

of 18
-
Upload
layzarleska -
Category
Documents
-
view
224 -
download
0
Transcript of Bioelectrical impedance analysis-part I review of principle and methods
-
8/7/2019 Bioelectrical impedance analysis-part I review of principle and methods
1/18
www.elsevier.com/locate/clnu
ESPEN GUIDELINES
Bioelectrical impedance analysisFpart I: review ofprinciples and methods
Ursula G. Kylea, Ingvar Bosaeusb, Antonio D. De Lorenzoc,Paul Deurenbergd, Marinos Eliae, Jos !e Manuel G !omezf,Berit Lilienthal Heitmanng, Luisa Kent-Smithh, Jean-Claude Melchiori,
Matthias Pirlichj
, Hermann Scharfetterk
, Annemie M.W.J. Scholsl
,Claude Pichardm,*, Composition of the ESPEN Working Group
aGeneva University Hospital, Geneva, SwitzerlandbSahlgrenska University Hospital, Gothenbury, SwedencUniversity Rome Tor Vergata, Rome, ItalydNutrition Consultant, SingaporeeSouthampton General Hospital, Southampton, UKfHospital Universitario de Bellvitge, Barcelona, SpaingCopenhagen University Hospital, Copenhagen, DenmarkhUniversity of Porto, Porto, Portugali
Hospital Raymond Poincar!e, Garches, FrancejUniversitatsklinikum Charit!e, Berlin, Germany
kGraz University of Technology, Graz, AustrialUniversity Hospital Maastricht, Maastricht, The NetherlandsmClinical Nutrition Unit, Geneva University Hospital, Micheli-du-Crest, 24, 1211 Geneva 14, Switzerland
Received 3 June 2004; accepted 4 June 2004
Summary The use of bioelectrical impedance analysis (BIA) is widespread both inhealthy subjects and patients, but suffers from a lack of standardized method andquality control procedures. BIA allows the determination of the fat-free mass (FFM)
and total body water (TBW) in subjects without significant fluid and electrolyteabnormalities, when using appropriate population, age or pathology-specific BIAequations and established procedures. Published BIA equations validated against areference method in a sufficiently large number of subjects are presented andranked according to the standard error of the estimate.
ARTICLE IN PRESS
KEYWORDS
Bioelectrical impedance
analysis;Segmental bioelectrical
impedance analysis;
Multi-frequency bioelectri-
cal impedance analysis;
Abbreviations: BCM, body cell mass; BF, body fat; BIA, bioelectrical impedance analysis; BIS, bioelectrical impedance spectroscopy(BIS); BMI, body mass index; BIVA, bioelectrical impedance vector analysis; DXA, dual-energy X-ray absorptiometry; ECW, extracellularwater; FFM, fat-free mass; ICW, intracellular water; MF-BIA, multi-frequency bioelectrical impedance analysis; PhA, phase angle; R,resistance; SF-BIA, single frequency bioelectrical impedance analysis; TBK, total body potassium; TBW, total body water; Xc,reactance; Z, impedance.
*Corresponding author. Tel.: 41-22-372-93-45; fax: 41-22-372-93-63.E-mail address: [email protected] (C. Pichard).
0261-5614/$ - see front matter & 2004 Elsevier Ltd. All rights reserved.doi:10.1016/j.clnu.2004.06.004
Clinical Nutrition (2004) 23, 12261243
-
8/7/2019 Bioelectrical impedance analysis-part I review of principle and methods
2/18
The determination of changes in body cell mass (BCM), extra cellular (ECW) andintra cellular water (ICW) requires further research using a valid model thatguarantees that ECW changes do not corrupt the ICW. The use of segmental-BIA,multifrequency BIA, or bioelectrical spectroscopy in altered hydration states alsorequires further research.
ESPEN guidelines for the clinical use of BIA measurements are described in a paperto appear soon in Clinical Nutrition.
& 2004 Elsevier Ltd. All rights reserved.
Introduction
This review discusses the application of bioelec-trical impedance analysis (BIA). BIA is widely usedin many clinical situations. Part 1 is a review of the principles and methodsof BIA, the body compart-ments evaluated with BIA, selection criteria, and
selected BIA equations reported in the literature.Part II will provide guidelines for BIA use in clinicalpractice.
Historical background
Electrical properties of tissues have been de-scribed since 1871.1 These properties were furtherdescribed for a wider range of frequencies onlarger range of tissues, including those that were
damaged or undergoing change after death.Thomasset2,3 conducted the original studies usingelectrical impedance measurements as an index oftotal body water (TBW), using two subcutaneouslyinserted needles. Hoffer et al.4 and Nyboer5 firstintroduced the four-surface electrode BIA techni-que. A disadvantage of surface electrodes isthat a high current (800mA) and high voltagemust be utilized to decrease the instability ofinjected current related to cutaneous impedance(10 000O/cm2).6 By the 1970s the foundationsof BIA were established, including those thatunderpinned the relationships between the im-
pedance and the body water content of the body.A variety of single frequency BIA analyzers thenbecame commercially available, and by the 1990s,the market included several multi-frequencyanalyzers. The use of BIA as a bedside methodhas increased because the equipment is portableand safe, the procedure is simple and non-invasive, and the results are reproducible andrapidly obtained. More recently, segmental BIAhas been developed to overcome inconsisten-cies between resistance (R) and body mass ofthe trunk.
Principles of bioelectrical impedance
The resistance (R) of a length of homogeneousconductive material of uniform cross-sectional areais proportional to its length (L) and inverselyproportional to its cross sectional area (A)(Fig. 1). Although the body is not a uniform cylinder
and its conductivity is not constant, an empiricalrelationship can be established between the im-pedance quotient (Length2/R) and the volume ofwater, which contains electrolytes that conduct theelectrical current through the body. In practice, itis easier to measure height than the conductivelength, which is usually from wrist to ankle.Therefore, the empirical relationship is betweenlean body mass (typically 73% water) and height2/R. Due to the inherent field inhomogeneity inthe body, the term height2/R describes an equiva-lent cylinder, which must be matched to the
real geometry by an appropriate coefficient. Thiscoefficient depends on various factors, among themalso the anatomy of the segments under investiga-tion. Therefore, errors occur when there arealterations in resistivity of the conductive material,
ARTICLE IN PRESS
Length (L)
Current
Cylinder
Cross-sectionalarea (A)
Figure 1 Principles of BIA from physical characteristicsto body composition. Cylinder model for the relationshipbetween impedance and geometry. The resistance of alength of homogeneous conductive material of uniformcross-sectional area is proportional to its length (L) andinversely proportional to its cross sectional area (A).Hence resistance R rL=A rL2=V; and volume V rL2=R; where r is the resistivity of the conductingmaterial and Vequals AL.
Bioelectrical spectroscopy;
ESPEN guidelines;
Fat-free mass;
Total body water;
Extracellular water;
Intracellular water;
Body cell mass
Bioelectrical impedance analysis 1227
-
8/7/2019 Bioelectrical impedance analysis-part I review of principle and methods
3/18
variations in the ratio height to conductive length,and variations in the shape of the body andbody segments (body segments behave as ifthey are in series with each other, with shorterand thicker segments contributing less to thetotal R).
Another complexity is that the body offers twotypes of R to an electrical current: capacitative R(reactance), and resistive R (simply called resis-tance). The capacitance arises from cell mem-branes, and the R from extra- and intracellularfluid. Impedance is the term used to describe thecombination of the two. Several electrical circuitshave been used to describe the behavior ofbiological tissues in vivo.7 One of them involvesarranging R and capacitance in series, another inparallel (Fig. 2), whilst others are more complex. Acircuit that is commonly used to represent biologi-cal tissues in vivo is one in which the R of
extracellular fluid is arranged in parallel to thesecond arm of the circuit, which consists ofcapacitance and R of intracellular fluid in series.R and capacitance can all be measured over a rangeof frequencies (most single-frequency BIA analyzersoperate at 50-kHz).
At zero (or low) frequency, the current does notpenetrate the cell membrane, which acts as aninsulator, and therefore the current passes throughthe extracellular fluid, which is responsible for themeasured R of the body R0.
At infinite frequency (or very high frequency) the
capacitor behaves as a perfect (or near perfect)capacitor, and therefore the total body R (RN
)reflects the combined of both intracellular andextracellular fluid.
Since practical constraints and the occurrenceof multiple dispersions prevent the use of adirect current (zero frequency) or very highfrequency AC currents, the R values at the ideal
measurement frequencies are predicted using aColeCole plot8 (negative reactance versus R plot),with R0 theoretically representing the R of theextracellular fluid (intracellular water) and R
N
representing the R of intra- and extracellular fluid(TBW) (Fig. 3).
At 50 kHz, the current passes through both intra-and extracellular fluid, although the proportionvaries from tissue to tissue. Another parallel modelattempts to take into account the effect ofmixing. Mixing theory predicts that the Rof conductive fluids increases as the amount of
suspended non-conducting material increases(explained simplistically by the increased conduc-tive path taken by the current as it curves aroundnon-conducting particles, which in vivo maybe represented by cells). The formula devised byHanai for in vitro models has been extrapolatedfor use in vivo, but this requires a number offurther assumptions.9,10 Different conceptual par-allel models have been devised for assessingcomposition of limbs, for example limb musclemass.11
The relationship between capacitance and R isinteresting because it reflects different electrical
properties of tissues that are affected in variousways by disease and nutritional status and hydra-tion status. The phase angle, which is one measureof this relationship, and other interrelated indices,including R0/RN, have been used to predict clinicaloutcome.1214 Furthermore, when the R and capa-citance are plotted graphically after standardisingfor height, different disease/conditions appear toform distinct clusters (bioelectric impedance vec-tor analysis (BIVA)) as proposed by Piccoli et al.1517
(Fig. 4). These may have potential value withrespect to diagnosis and prognosis.
ARTICLE IN PRESS
R(ECW)
R(ICW)XC
Fricke's circuit
Two parallel electrical conductors:
R(ECW): H2O-Na
R(ICW): H2O-K
isolated by a cell membrane (Xc)
Figure 2 The human body consists of resistance andcapacitance connected in parallel or in series. In theparallel model, two or more resistors and capacitors areconnected in parallel, with the current passing at highfrequencies through the intracellular space and at lowfrequencies passing through the extracellular space.
Frequency
increases
Resistance R ()R
Impedance Z ()
Ro
Phase angle
-ReactanceXc
()
Figure 3 Diagram of the graphical derivation of thephase angle; its relationship with resistance (R), reac-tance (Xc), impedance (Z) and the frequency of theapplied current.
1228 U.G. Kyle et al.
-
8/7/2019 Bioelectrical impedance analysis-part I review of principle and methods
4/18
Methods of bioelectrical impedanceanalysis
Single frequency BIA (SF-BIA)
SF-BIA, generally at 50kHz, is passed betweensurface electrodes placed on hand and foot (Fig. 5).Some BIA instruments use other locations such asfoot-to-foot18,19 or hand-to-hand electrodes. At50 kHz BIA is strictly speaking not measuring TBWbut a weighted sum of extra-cellular water (ECW)and intra-cellular water (ICW) resistivities (B25%).SF-BIA permits to estimate fat-free mass (FFM) andTBW, but cannot determine differences in ICW. BIAresults are based on a mixture theories and
empirical equations. The latter have been derived
in healthy subjects with tight biological home-ostasis. Although SF-BIA is not valid under condi-tions of significantly altered hydration, this doesnot negate its use to predict absolute FFM or TBW innormally hydrated subjects.7 The relative merits ofthe various equations have to be discussed, whenthe normal relationships are not met.
Multi-frequency BIA (MF-BIA)
As with SF-BIA, MF-BIA uses empirical linearregression models but includes impedances at
multiple frequencies. MF-BIA uses different fre-quencies (0, 1, 5, 50, 100, 200 to 500 kHz) toevaluate FFM, TBW, ICW and ECW. At frequenciesbelow 5 kHz, and above 200 kHz, poor reproduci-bility have been noted, especially for the reactanceat low frequencies.20 According to Patel et al.21 MF-BIA was more accurate and less biased than SF-BIAfor the prediction of ECW, whereas SF-BIA, com-pared to MF-BIA, was more accurate and less biasedfor TBW in critically ill subjects. Hannan et al.22
noted that MF-BIA, compared to bioelectricalspectroscopy (BIS), resulted in better prediction
of TBW and equal prediction for ECW in surgicalpatients. Olde-Rikkert et al.23 determined that MF-BIA was unable to detect changes in the distributionor movement of fluid between extracellular andintracellular spaces in elderly patients.
Bioelectrical spectroscopy (BIS)
In contrast to MF-BIA, BIS uses mathematicalmodeling and mixture equations (e.g. ColeCole plot (Fig. 3) and Hanai formula)8,24 togenerate relationships between R and body fluid
ARTICLE IN PRESS
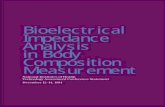
Figure 4 Bioelectrical impedance vector analysis (BIVA)with the RXc path graph of one patient following lungtransplantation. The gender-specific, bivariate toleranceintervals for the impedance vector are depicted as 50%,75%, and 95% tolerance ellipses calculated in our healthy
Swiss reference population (age 18
59 yr, 2643 women, Ris the resistance, Xc the negative reactance, and H theheight). Repeated impedance measurements were ob-tained after lung transplantation: (a) 1 month, (b) 6months, (c) 12 months, (d) 18 months, (e) 24 months. Theinitial vector position (a in woman) indicates soft tissuemass decrease (bioelectrical impedance vector analysis(BIVA) pattern of cachexia). The subsequent vectormigration parallel to the minor axis of ellipses towardthe target ellipse (bd in woman) indicates an improve-ment of nutritional status with increasing hydrated softtissue mass (i.e. decreasing R with increasing Xc). Thefinal vector migration from the lower pole (BIVA pattern
of tissue hyperhydration) to the center of the 50%tolerance ellipse, following a trajectory parallel to themajor axis (i.e. proportional increase in both R and Xc),indicates loss of excess fluid leading to the completerestoration of tissue impedance, which was reached after24 months in woman (e). Body weight increased from54.2 to 68.8kg in woman (156cm, 47 yr). Unpublisheddata, adapted from Piccoli et al.16
Figure 5 Standard placement of electrodes on hand andwrist and foot and ankle for tetrapolar single (SF-BIA) andmultiple-frequency (MF-BIA) BIA.
Bioelectrical impedance analysis 1229
-
8/7/2019 Bioelectrical impedance analysis-part I review of principle and methods
5/18
compartments or to predict R0 and RN and thendevelop empirically derived prediction equationsrather than go to mixture modeling.25 BIS models,constants and equations generated in healthypopulations have shown to be accurate, withminimal bias in non-physiologically perturbed sub-
jects.
26
However, modeling techniques need furtherrefinement in disease. As pointed out by Schoeller,27
body cell mass (BCM), especially muscle mass,constitutes the major current path. These cellsare non-spherical, but rather cylindrical, arrangedalong the currents path. He speculated that thedifferences in geometry account for the reductionin the mixture effect. Furthermore, the determina-tion of accurate values of resistivity (rICW andrECW) presented the most difficulty. Publishedvalues are widely discrepant. Ward et al.10 sug-gested wide biological variations even in the normalpopulation, may explain the apparent lack of
improvement of mixture theory analysis overempirical prediction seen by some.22,28 Severalstudies have suggested that resistivity constantsused should be adjusted for population mea-sured.9,2931 Since the absolute magnitude andbiological constancy of resistivity are at presentunknown, application of mixture theory for theprediction of both the absolute magnitude of bodyfluid volume or changes in magnitude of bodycompartments requires further investigation.10
Mixture equations in some studies show improve-ment in accuracy,3234 no improvement35,36 or
worse accuracy7
than regression approach. Thepotential of BIS can only be exhausted if the dataare interpreted with adequate algorithm thatinclude reliable data fitting and a valid fluiddistribution model.37
Segmental-BIA
Segmental-BIA is performed by either placing twoadditional electrode on wrist and foot on theopposite side,38 or by placing sensor electrodes onwrist, shoulder (acromion), upper iliac spine and
ankle,39 or by placing electrodes on proximalportion of the forearm and the lower leg and tr unkelectrode on the shoulder and the upper thigh.7,40
For a detailed review, we refer the reader to DeLorenzo and Andreoli.41 The trunk of the body withits large cross sectional area contributes as little as10% to whole body impedance whereas it repre-sents as much as 50% of whole body mass.42 Thisimplies three aspects for body composition analysisby the whole body BIA approach: (1) changes of theimpedance are closely related to changes of theFFM (or muscle mass or body cell mass (BCM)) of the
limbs; (2) changes of the FFM (or muscle mass orBCM) of the trunk are probably not adequatelydescribed by whole body impedance measure-ments, and (3) even large changes in the fluidvolume within the abdominal cavity have onlyminor influence on the measurement of FFM or
BCM as could demonstrated in patients with livercirrhosis and ascites undergoing paracentesis.43
Segmental-BIA requires prior standardization, par-ticularly when different approaches and different BIAdevices are employed. Standardization of the type ofelectrodes used and their placement is a majorconcern. Segmental-BIA has been used to determinefluid shifts and fluid distribution in some diseases(ascites, renal failure, surgery), and may be helpful inproviding information on fluid accumulation in thepulmonary or abdominal region of the trunk.
Bracco et al.44 and Tagliabue et al.45 found highrelative errors with segmental-BIA for arms and
legs: 13
17% for arm FFM and 10
13% for leg FFM.Tagliabue et al.45 noted that frequencies higherthan 50kHz did not improve the segmental BIAresults. Additional research is needed to examinethe accuracy of the segmental BIA.
Localized bioelectrical impedance analysis
Whole body BIA measures various body segmentsand is influenced by a number of effects (hydration,fat fraction, geometrical boundary conditions,etc.). Hence the validity of simple empirical
regression models is population-specific. For thesereasons, localized BIA, which focuses on well-defined body segments and thus minimizes theinterference effects, has been proposed. Scharfet-ter et al.46 determined local abdominal fat mass bylocalized BIA. Rutkove et al.47 determined inpatients with neuromuscular disease that phaseangle and resistivity of limbs decreased withdisease progression and normalized with diseaseremission and may be useful in the therapeuticevaluation of such diseases.
Bioelectrical impedance vector analysis(BIVA or vector BIA)
The ultimate attractiveness of BIA lies in itspotential as a stand-alone procedure that permitspatient evaluation from the direct measurement ofthe impedance vector and does not depend onequations or models. The BIVA approach developedby Piccoli et al. 16,48,49 is only affected by theimpedance measurement error and the biologicalvariability of subjects. In BIVA, R and reactance(Xc), standardized for height, are plotted as point
ARTICLE IN PRESS
1230 U.G. Kyle et al.
-
8/7/2019 Bioelectrical impedance analysis-part I review of principle and methods
6/18
vectors in the RXc plane. An individual vector canthen be compared with the reference 50%, 75%,and 95% tolerance ellipses calculated in the healthypopulation of the same gender and race (RXcgraph method) (Fig. 4). The ellipse varies with ageand body size.50
Clinical validation studies (renal patients, criticalcare patients and obese subjects)1719 showed thatvectors falling outside the 75% tolerance ellipseindicate an abnormal tissue impedance, which canbe interpreted as follows: (1) vector displacementsparallel to the major axis of tolerance ellipsesindicate progressive changes in tissue hydration(dehydration with long vectors, out of the upperpole, and hyperhydration with short vectors, out ofthe lower pole); and (2) vectors falling above (left)or below (right) the major axis of tolerance ellipsesindicate more or less BCM, respectively, containedin lean body tissues. Long-term monitoring of
patients has shown combined changes in hydrationand soft tissue mass. Fig. 4 shows an example ofBIVA follow-up with the RXc path graph in a femalepatient following lung transplantation, using the50th, 75th and 95th tolerance percentiles of ahealthy Swiss reference population (data unpub-lished). However, Cox-Reijven et al.51 found a lowsensitivity (but high specificity) of BIVA in detectingdepletion in gastrointestinal patients. Furthervalidation seems necessary.
Body compartments
Fat-free mass
FFM is everything that is not body fat (Fig. 6). Alarge number of BIA equations in the literaturepredict FFM. These equations vary in the para-meters included in the multiple regression equa-tions and their applicability in various subjects.Early BIA equations (before 1987) only includedheight2/resistance. Later equations include otherparameters, such as weight, age, gender, reac-
tance, and anthropometric measurements of thetrunk and/or extremities to improve the predictionaccuracy. FFM can be determined by SF-BIAprovided that hydration is normal and BIA equationsused are applicable to the study population, withregard to gender, age, and ethnic group.
Total body water (TBW), extracellular (ECW)and intracellular water (ICW)
OBrien et al.52 found that current BIA methods (SF-and MF-BIA) are not sufficiently accurate to assess
TBW under conditions of hydration change. Equa-
tions that were developed in euhydrated popula-tions have not been shown to be valid forindividuals with altered hydration. Data from bothhypo- and hyper-hydration studies suggest thatelectrolyte balance influences BIA measurementsindependently of fluid changes. Such effects maybe difficult to predict, as fluid and electrolytechanges will also affect the ratio of intra- to extra-cellular water which, in turn, influences resistivity.The ECW:ICW ratio is a factor known to limit theapplicability of predictive equations generated byBIA to external populations.53 Furthermore, BIA
does not allow to accurately assess TBW and ECWwhen body water compartments are undergoingacute changes.54,55 In addition, the average bodyhydration of the FFM varies with age (newborns80%; 10-yr old children 75%,56 healthy adults 73%).
According to Ellis et al.57 50 kHz SF-BIA primarilyreflects the ECW space, which represents aconstant proportion of TBW in normal condition.An increase in ECW or in the ECW/TBW ratio mayindicate edema and/or malnutrition. MF-BIA ap-pears to be sensitive to such changes, even if thereare no significant changes in body weight. On theother hand, the parallel-transformed, SF-BIA mod-
el58 appears to be sensitive to changes in ICW (orBCM),7 but not to changes in ECW. Therefore thismodel may have limited use for estimating FFM orbody fat when there is an abnormal hydrationstate.57
Among the MF-BIA and BIS models, the 0/Nparallel (ColeCole) model is considered moreprecise and accurate for the measurement of ECWand ICW than variables obtained by SF-BIA. Gudi-vaka et al.7 found the 0/N parallel (ColeCole)model accurately predicted changes in TBW, ECWand ICW in subjects receiving Ringers solution or
ARTICLE IN PRESS
Figure 6 Schematic diagram of fat-free mass (FFM),total body water (TBW), intracellular water (ICW),extracellular water (ECW) and body cell mass (BCM).
Bioelectrical impedance analysis 1231
-
8/7/2019 Bioelectrical impedance analysis-part I review of principle and methods
7/18
diuretic therapy with proximally placed detectorelectrodes (elbow and knee). Scharfetter et al.59
estimated that, due to electrolyte changes, at theend of dialysis, the error with respect to thevolume change was large (p15% for the ECW and420% for ICW). They concluded that a correction of
the fluid distribution model for resistivity changesis necessary to obtain more reliable ICW data. Thepotential of BIS can only be exhausted if the dataare interpreted with adequate algorithm thatinclude reliable data fitting and a valid fluiddistribution model which considers tissue non-homogeneities.37 A valid model must guaranteethat ECW changes do not corrupt the ICW and viceversa.37 Standardization of BIS method remains aconcern.
The meta-analysis by Martinoli et al.60 concludedthat SF-BIA and BIS significantly overestimated TBWin healthy individuals, whereas there was no
overestimation by MF-BIA. MF-BIA seems to be amore accurate method for determining the TBWcompartment for healthy and obese adults and forpersons with chronic renal failure.
Body cell mass (BCM)
Whereas FFM is everything that is not body fat,there is no consensus on the physiological meaningof measures of cellular mass, BCM or meta-bolically active tissue and ICW. The BCM is the
protein rich compartment which is affected incatabolic states, and loss ofBCM is associated withpoor clinical outcome.61,62 In overhydrated pa-tients, even precise determination of FFM mightfail to detect relevant protein malnutrition becauseof expansion of the ECW. Estimating the size isdifficult because it is a complex compartment,comprising all nonadipose cells as well as theaqueous compartment of adipocytes. Future re-search is needed to define BCM and the role of BIAin its clinical evaluation.
In patients with severe fluid overload, such aspatients with ascites, inter-individual differences
of lean tissue hydration are probably too high todevelop uniform equations to assess BCM. Pirlichet al.63 concluded that in patients with largealterations of body geometry or hydration statusthe application of standard BIA is not appropriateto assess BCM.
Ward and Heitmann64 evaluated assessment ofBCM and ECW by BIA without the need formeasurement of height and found that the sig-nificant differences in the mean values and widelimits of agreement compared to reference data forBCM and ECW do not permit to predict these body
compartments without inclusion of height in spiteof obvious advantages of not requiring an accuratemeasurement of height.
BIA measurements and equations
BIA measurements must be standardized in order toobtain reproducible results (see BIAFpart 2).Reported mean coefficients of variation for with-in-day R measurements areE12%; daily or weeklyintra-individual variability is slightly larger rangingfrom E2% to 3.5%.6568 Day-to-day coefficients ofvariation increases for frequencies lower than50kHz.69 Overall reproducibility/precision is 2.74.0%.67 Prediction errors were estimated to be 38%for TBW and 3.56% for FFM, respectively.70,71
Early BIA equations were validated in inadequatepopulations, as demonstrated in respiratory insuf-ficiency patients.72 Large variations in results werenoted with many formulas published in the litera-ture that precluded clinical interpretation. The useof general prediction equations across differentage and ethnic groups without prior testing of theirvalidity should be avoided. Choosing a BIA equationthat is adapted to the populations studied con-tinues to be a limiting factor of BIA.
Standardization of future studies with regard tomethodological considerations (such as inclusionand exclusion criteria, standardization of BIAmethods etc.) as discussed by Gonzalez et al.73
should help to improve BIA results in the future.
Table of validated equations
Selected BIA equations published since l990 foradults for FFM (Table 1);6,58,70,7488 body fat (Table2),38,82,86,88,89 TBW (Table 3),20,25,32,58,65,70,78,88,9094
ECW (Table 4),20,25,32,90,92,93,95 ICW (Table 5)96,97 andBCM (Table 6)58,98 are shown in order of increasingstandard error of the estimate (SEE). They arelimited to studies in healthy subjects that include atleast 40 subjects and are validated against acriterion measure. For discussion of BIA equations
in specific diseases, we refer the reader toBioelectrical impedance analysisFpart II: utiliza-tion in clinical practice. The equation for TBW byKushner and Schoeller65 is included because it isfrequently cited in the literature. For BIA equationsfor FFM, TBW and body fat published prior to l990,we refer the reader to Houtkooper et al.99
How to choose a BIA equation
Houtkouper et al.99 suggested that prediction error(SEE) of 2.02.5 kg in men and 1.51.8 kg in women
ARTICLE IN PRESS
1232 U.G. Kyle et al.
-
8/7/2019 Bioelectrical impedance analysis-part I review of principle and methods
8/18
Table 1 Bioelectrical impedance analysis equation reported in the literature since 1990 for fat-free mass (FFM) classified ac
elderly, overweight) and standard error of the estimate (SEE).Population Source n Criterion
measureEquation
Adults
Healthy subjects,1894yr
Kyle et al.74 343 DXA 4:104 0:518 Ht2=R500:231 weight0:130 Xc 4:229 sex
Healthy adults,1829yr
Lohman75 153 Densitometry85 , w Women 5:49 0:476 Ht2=R500:295 weight
Healthy adults,3049yr
Lohman75 122 Densitometry85 , w Women 11:59 0:493 Ht2=R500:141 weight
Healthy, ethnic divers Kotler et al.SF parallel58
126 DXA Women 0:07 0:88 Ht1:97=Z0:4950 1:0=22:22 0:081 weight
Healthy subjects,416yr
Deurenberg et al.76 661 Multi-C,87
densitometry86 , z12:44 0:34Ht2=R500:1534 height0:273 weight 0:127 age 4:56 sex
Healthy subjects,1271yr
Boulier et al.6 202 Densitometry 6:37 0:64 weight 0:40Ht2=Z1 MHz0:16 age2:71 sex men 1; women 2
Women 1860 yr Stolarczyk et al.77 95 Multi-Cy 20:05 0:04904 R500:001254 Ht2
0:1555 weight 0:1417 Xc 0:0833 ageHealthy adults,5070yr
Lohman75 72 Densitometry85 , w Women 6:34 0:474 Ht2=R500:180 weight
Healthy adults,1829yr
Lohman75 153 Densitometry85 , w Men 5:32 0:485 Ht2=R500:338 weight
Healthy subjects,1294yr
Sun et al.70 1095 Multi-C Women: 9:529 0:696 Ht2=R500:168 weight 0:016 R50
Healthy, ethnic divers Kotler et al.SF parallel58
206 DXA Men 0:49 0:50 Ht1:48=Z0:5550 1:0=1:21 0:42 weight
Healthy adults,3049yr
Lohman75
111 Densitometry85 , w
Men 4:51 0:549 Ht2
=R500:163 weight 0:092 Xc
Healthy subjects,3565yr
Heitmann78 139 Multi-C,88 3H2O,TBK
14:94 0:279 Ht2=R500:181 weight0:231 height 0:064 sex weight 0:077 ag
Healthy adults,5070yr
Lohman75 74 Densitometry85 , w Men 11:41 0:600 Ht2=R500:186 weight 0:226 Xc
Healthy subjects,1294yr
Sun et al.70 734 4 compart Men : 10:678 0:652 Ht2=R500:262 weight 0:015 R
-
8/7/2019 Bioelectrical impedance analysis-part I review of principle and methods
9/18
Overweight
Overweight women2545yr
Jakicic et al.79 123 DXA 2:68 0:20 Ht2=R500:19 weight2:55 ethnicityCaucasian 0;AfricanAmerican 1 0:1157 height
Overweight women2545yr
Jakicic et al.79 DXA 2:04 0:02 R500:19 weight2:63 ethnicityCaucasian 0;
AfricanAmerican 10:2583 height
Elderly
Elderly women6272yr
Haapala et al.80 93 DXA 128:06 1:85 BMI 0:63 weight1:07 height 0:03 R5010:0 waisthip ratio
Elderly Roubenoff et al.81 294 DXA Women : 7:7435 0:4542 Ht2=R500:1190 weight 0:0455 Xc
Elderly, 6594 y r Baumgartner et al.82 98 Multi-C82 , z 1:732 0:28Ht2=R500:27 weight4:5 sex 0:31 thigh circ
Elderly Dey et al.83 106 4 compart 11:78 0:499 Ht2=R500:134 weight3:449 sex
Elderly, 6083 yr Deurenberg et al.84 72 Densitometry86 , z 7:0 0:360 Ht2=R504:5 sex0:359 weight 0:20 thigh circ
Elderly, 60
83 yr Deurenberg et al.84 72 Densitometry86 , z 3:9 0:672 Ht2=R503:1 Sex Elderly, 6594 y r Baumgartner et al.82 98 Densitometry86 , z 15:44 0:34Ht2=R500:36 weight
4:3 sex 0:57 ankle circElderly Roubenoff et al.81 161 DXA Men: 9:1536 0:4273 Ht2=R50
0:1926 weight 0:0667 XcElderly Roubenoff et al.81 445 DXA 5:741 0:4551 Ht2=R500:1405 weight
0:0573 Xc 6:2467 sex
BIA equations are shown in order of increasing standard error of the estimate (SEE). They are limited to studies in healthy subjects that includagainst a criterion measure.nRSME, root mean square error; R, resistance; Ht2/R, height2/resistance, Xc, reactance; V, body volume; Z, impedance; Z5, impedance at 5 kHz0 for women, unless otherwise stated, NR, not reported, height in cm, weight in kg, thigh circumference in cm, resistance in ohm, reactance in Xitron Technologies, San Diego, CA; Valhalla Scientific, San Diego, CA; BIA-2000-M, Data Input, Hofheim, Germany; IMP BO-1, (2 subcutaneous elsubjects are Caucasian, except Jakicic (Caucasian and African-American), Stolarczyk et al. (Native American), and Sun (Caucasian and Africaw%BF ((4.570/body density) 4.142) 100.z%BF (4.95/body density) 4.5)100.y%BF (6.38/body density) 3.961 bone mineral mass 6.090)100.z%BF ((1.34/body density) 0.35age0.56 mineral content 1) 205.
-
8/7/2019 Bioelectrical impedance analysis-part I review of principle and methods
10/18
Table 2 Bioelectrical impedance analysis equation reported in the literature since 1990 for body fat (BF) classified accordin(SEE).
Comments Source n Criterion measure Equation
Body fat (%)Elderly, 6594yr Baumgartner et al.82 98 Multi-C82 , n 23:58 20:03 R50 weight=Ht
2
0:29 thigh circ4:99 sex 0:52 arm circ
Elderly, 6594yr Baumgartner et al.82 98 Densitometry86 , w 18:89 22:12 R50 weight=Ht2
0:64 calf circ4:13 sex
Body fat (kg)
Healthy subjects,2164 yr,segmental BIA
Organ et al.
38
104 Underwaterweighing, 2H2O Women :5:9150 0:7395 weight0:3327 height 0:0846 age
0:048 upperlimb R500:2705 trunk R500:0384 lowerlimb R500:1219lowerlimb Xc
Healthy subjects,2164 yr,segmental BIA
Organ et al.38 96 Underwaterweighing, 2H2O
Men : 4:2422 0:7368 weight 0:0482 height
0:1170 age 0:0393 upperlimb R500:5110trunk R500:0654 lowerlimb R500:2560lowerlimb Xc
Healthy subjects,3565yr
Heitmann89 139 FM multi-C88 14:94 0:079Ht2=R500:818 weight 0:231 height
0:064 sex weight 0:077 age
BIA equations are shown in order of increasing standard error of the estimate (SEE). They are limited to studies in healthy subjects that includagainst a criterion measure.
R, resistance; Ht2/R, height2/resistance; Xc, reactance; V, body volume; Z, impedance; Z5, impedance at 5 kHz; Z100, impedance at 100 kHz; 1stated; circ, circumference.RJL Systems, Inc, Clinton Twp, MI; Xitron Technologies, San Diego, CA; Valhalla Scientific, San Diego, CA; BIA-2000-M, Data Input, Hofheim, Gn%BF ((1.34/body density) 0.35age0.56 mineral content 1) 205.w%BF (4.95/body density) 4.5)100.
-
8/7/2019 Bioelectrical impedance analysis-part I review of principle and methods
11/18
-
8/7/2019 Bioelectrical impedance analysis-part I review of principle and methods
12/18
Table 4 Bioelectrical impedance analysis equation reported in the literature since 1990 for extracellular water (ECW), classifieestimate (SEE).
Population Source n Criterionmeasure
Equation r2
Healthy subjects Deurenberg et al.90 139 KBr 2:30 0:19528 Ht2=Z10:06987 weight
0:02 age
0.87
Healthy subjects Deurenberg et al.90 139 KBr 2:53 0:18903 Ht2=Z50:06753 weight
0:02 age0.86
Healthy subjects,1965yr
Van Loan andMayclin92
60 NaBr 5:17753 0:09989 Ht2=R2240:09322 weight 1:3962
sexmen 0; women 1
0.92
Healthy22 andill subjects18
Sergi et al.95 40 NaBr 7:24 0:34Ht2=R10:06 weight2:63healthy 1; ill 2 2:57sexmen 0; women 1
0.89
Healthy22 andill subjects18
Sergi et al.95 40 NaBr F5:22 0:20Ht2=R500:005Ht2=Xc50
0:08 weight 1:9healthy 1; ill 2
1:86 sexmen 0; women 1
0.89
Healthy non-obeseand obese subjects
Cox-Reijven andSoeters32
90 NaBr 3:511 0:351Ht2=Recw0:05 weight 0.77
Healthy subjects Cornish et al.25 60 NaBr 6:3 0:352Ht2=R00:099 weight 3:09sex0 male; 1 female
0.7
Healthy subjects Cornish et al.25 60 NaBr 1:2 0:194 Ht2=R00:115 weight 0.65 Healthy subjects Cornish et al.25 60 NaBr 5:3 0:480Ht2=R03:5sex0 male;
1 female
0.66
Elderly, 6387 yr Visser et al.93 117 KBr Men 4:8 0:2249 Ht2=Z5 0.39 Women 1:7 0:1998 Ht2=Z50:0571 weight 0.65
Surgical patients Hannan et al.20 43 NaBr 5:75 0:01Ht2=Xc500:165Ht2=R5 0.87
Surgical patients Hannan et al.20 43 NaBr 6:15 0:0119 Ht2=Xc500:123 Ht2=R50 0.87
BIA equations are shown in order of increasing standard error of the estimate (SEE). They are limited to studies in healthy subjects that includagainst a criterion measure.
R, resistance; Ht2
/R, height2
/resistance; Recw, Resistance by Cole
Cole plot; Xc, reactance; V, body volume; Z, impedance; Z5, impedance at men, 0 for women, unless otherwise stated.NaBr sodium bromide, KBrPotassium bromide.Human-IM Scanner, Dietosystem, Milan, Italy; Xitron Technologies, San Diego, CA; RJL Systems, Inc, Clinton Twp, MI; SEAC, Brisbane, Australi
-
8/7/2019 Bioelectrical impedance analysis-part I review of principle and methods
13/18
Table 5 Bioelectrical impedance analysis equation reported in the literature since 1990 for intracellular water (ICW), classifieestimate (SEE).
Comments Source n Criterionmeasure Equation
Elderly, 6080 yr Dittmar and Reber, SFBIA96 159 TBK 9:182 0:285 Ht2=Z57:114 PA52:113 sex
Healthy men, 2353 yr De Lorenzo et al.97 57 TBK 12:2 0:37065 Ht2=Ricw0:132 age 0:105 weigh
BIA equations are shown in order of increasing standard error of the estimate (SEE). They are limited to studies in healthy subjects that includagainst a criterion measure.TBK, total body potassium; Ricw, intracellular resistance; Ht
2/Z5, height2/impedance at 5 kHz; PA5, phase angle at 5 kHz; 1 for men, 0 for wo
Xitron Technologies, San Diego, CA; BIA-2000-M, Data Input, Hofheim, Germany.
Table 6 Bioelectrical impedance analysis equation reported in the literature since 1990 for body cell mass (BCM), classifiedestimate (SEE)n.
Comments Source n Criterionmeasure
Equation
Elderly, 6090yr Dittmar and Reber, SFBIA98 160 TBK 1:898 Ht2=Xcp500:051 weight 4:180 sex 15:496
Elderly, 6090 yr MFBIA1 160 TBK 1:118 Ht2=Ric5=504:250 sex 14:457
Elderly, 6090 yr MFBIA2 160 TBK 0:822 Ht2=Ric5=1004:158 sex 14:096
Healthy, ethnic diverse Kotler et al. SF parallel58 206 TBK Men 1=120 0:76 59:06Ht1:6=X0:5cp50 18:52 weight 38
Healthy, ethnic diverse Kotler et al. SF parallel58
126 TBK Women 1=120 0:96 1:3 Ht2:07
=X0:36cp50 5:79 weight 23
BIA equations are shown in order of increasing standard error of the estimate (SEE). They are limited to studies in healthy subjects that includagainst a criterion measure.BIA-2000-M, Data Input, Hofheim, Germany; RJL Systems, Inc, Clinton Twp, MI.nRMSE, root mean square error; TBK, total body potassium; R, resistance; Ht2/Xcp50, height
2/parallel reactance at 50 kHz; Ric5=50; R5R50/(R5men, 0 for women.
-
8/7/2019 Bioelectrical impedance analysis-part I review of principle and methods
14/18
and actual error of 0.01.8 kg is considered ideal.Prediction error of less than 3.0 kg for men and2.3 kg for women would be considered very good.BIA equations chosen should not be used withoutprior verification against reference methods in thesubject population studied.
Limitations of BIA equations
BIA integrates various body segments with variablephysical effects of hydration, fat fraction, geome-trical boundary conditions etc. on tissue conductiv-ity (see Part II). This explains, in part, whyempirical regression models are population-speci-fic. Furthermore, the trunk contributes only a smallproportion to whole body impedance because it isrelatively short and has a large cross-sectionalarea. Limitations of BIA measurements in case of
body water alterations or body geometry abnorm-alities are described in Part II. ECW:ICW ratio is afactor known to limit the applicability of predictiveequations generated by BIA to populations withvarying hydration.53
The difficulties of validating BIA in different ageand ethnic groups, and clinical conditions withabnormal hydration states has resulted in aplethora of BIA equations that confuse, rather thanaid in the interpretation of BIA results. Tables 16try to facilitate this selection by presentingequations according to the respective value ofstandard error of the estimate. Specific BIA
measurement errors associated with clinical condi-tions are discussed in Part II.
Reference methods
Validation of BIA equations must be done againstreference methods, including multi-compartmentmodel,100,101 densitometry (underwater weigh-ing),102 dual-energy X-ray absorptiometry(DXA),102 isotope dilution102,103 and total bodypotassium (TBK). Each of these reference methodshas limitations and makes assumptions (such as
total body potassium (TBK)/FFM is constant withage, constant hydration of FFM of 73%, constantdensity for FFM with densitometry) that are notvalid in all situations.104 Although DXA is not yetconsidered a gold standard method, it is in-cluded as reference method because of its wideavailability and it can be used in patients. Alimitations of DXA is that results by differentmanufacturers do not agree.105,106 Although TBK isa reference method for body cell mass (BCM),107 itis limited in the determination of FFM because TBKcontent varies with sex and age.108,109 The two-
compartment model makes assumptions regardingthe constancy of composition of FFM, which is nottrue in all ethnic groups and across the life. Theselimitations can be overcome with a multi-compart-ment model.104
Thus, some of the discrepancies reported in the
literature are due to different reference methodsand different software versions of the referencemethods used in the validation process. This leavesus with the dilemma of choosing a BIA equation fora specific population that was considered validbased on a reference method that may or may nothave been accurate and may or may not becomparable to other reference methods.
Study population
Most studies were done on Caucasian subjects.Kotler et al.58 and Sun et al.70 include African-American and Hispanic subjects. Stolarczyk et al.77
includes native American Indians. Ethnic-specificimpedance-based equations for body compositionare justified because of differences in body buildamong ethnic groups.110 Relative leg lengths,111
frame size112 and body build113 are factors respon-sible for ethnic differences in the body mass index(BMI) to % body fat relationship. Failing to adjustfor differences in FFM density in ethnic groups mayresult in systematic biases of up to 3%.111 Futurebody composition research should include non-Caucasian subjects.
Conclusion
Whole-body BIA allows the determination of the FFMand TBW in subjects without significant fluid andelectrolyte abnormalities, when using appropriatepopulation, age or pathology-specific BIA equationsand established procedures. The determination ofchanges in BCM, ECW and ICW requires furtherresearch using a valid model that guarantees thatECW changes do not corrupt the ICW and vice versa.
The use of segmental, MF-BIA or BIS in alteredhydration states also requires further research.
ESPEN guidelines for the use of BIA measure-ments (see Bioelectrical impedance analysisFPartII) are described in another paper to be publishedsoon in Clinical Nutrition.
Acknowledgements
We acknowledge the financial support by PublicFoundation Nutrition 2000Plus.
ARTICLE IN PRESS
Bioelectrical impedance analysis 1239
-
8/7/2019 Bioelectrical impedance analysis-part I review of principle and methods
15/18
References
1. Hermann L. Ueber eine Wirking galvanischer Strome aufMuskeln und Nerven. Pflugers Arch gesamte Physiol1871;5:22375.
2. Thomasset A. Bio-electrical properties of tissues. Lyon Med1963;209:132552.
3. Thomasset A. Bio-electrical properties of tissue impedancemeasurements. Lyon Med 1962;207:10718.
4. Hoffer EC, Clifton KM, Simpson DC. Correlation of whole-body impedance with total body volume. J Appl Physiol1969;27:5314.
5. Nyboer J. Electrical impedance plethysmograph, 2nd ed.Springfield, IL: CC Thomas; 1970.
6. Boulier A, Fricker J, Thomasset A-L, Apfelbaum M. Fat-freemass estimation by the two-electrode impedance method.
Am J Clin Nutr 1990;52:5815.
7. Gudivaka R, Schoeller DA, Kushner RF, Bolt MJ. Single- andmultifrequency models for bioelectrical impedance analy-sis of body water compartments. J Appl Physiol 1999;87:108796.
8. Cole KS. Dispersion and absorption in dielectrics. I.
Alternating current characteristics. J Chem Phys 1941;9:341951.
9. De Lorenzo A, Andreoli A, Matthie J, Withers P. Predictingbody cell mass with bioimpedance by using theoreticalmethods: a technological review. J Appl Physiol 1997;85:154258.
10. Ward LC, Elia M, Cornish BH. Potential errors in the
application of mixture theory to multifrequency bio-electrical impedance analysis. Physiol Meas 1998;19:5360.
11. Fuller NJ, Hardingham CR, Graves M, et al. Predictingcomposition of leg sections with anthropometry and
bioelectrical impedance analysis, using magnetic reso-nance imaging as reference. Clin Sci 1999;96:64757.
12. Schwenk A, Beisenherz A, R.omer K, Kremer G, Salzberger
B, Elia M. Phase angle from bioelectrical impedanceanalysis remains an independent predictive marker inHIV-infected patients in the era of highly active antire-troviral treatment. Am J Clin Nutr 2000;72:496501.
13. Schwenk A, Ward LC, Elia M, Scott GM. Bioelectrical
impedance analysis predicts outcome in patients withsuspected bacteremia. Infection 1998;26:27782.
14. Toso S, Piccoli A, Gusella M, et al. Altered tissue electricproperties in lung cancer patients as detected by bio-electric impedance vector analysis. Nutrition 2000;16:
1204.15. Piccoli A, Rossi B, Pillon L, Bucciante G. A new method for
monitoring body fluid variation by bioimpedance analysis:the RXc graph. Kidney Int 1994;46:5349.
16. Piccoli A, Pillon L, Dumler F. Impedance vector distribution
by sex, race, body mass index, and age in the UnitedStates: standard reference intervals as bivariate Z scores.
Nutrition 2002;18:15367.17. Piccoli A, Pillon L, Favaro E. Asymmetry of the total body
water prediction bias using the impedance index. Nutrition1997;13:43841.
18. Jebb SA, Cole TJ, Doman D, Murgatroyd PR, Prentice AM.
Evaluation of the novel Tanita body-fat analyser to measurebody composition by comparison with a four-compartmentmodel. Brit J Nutr 2000;83:11522.
19. Utter AC, Nieman DC, Ward AN, Butterworth DE. Use of theleg-to-leg bioelectrical impedance method in assessing
body-composition change in obese women. Am J Clin Nutr1999;69:6037.
20. Hannan WJ, Cowen SJ, Fearson KCH, Plester CE, Falconer
JS, Richardson RA. Evaluation of multi-frequency bio-impedance analysis for the assessment of extracellular
and total body water in surgical patients. Clin Sci1994;86:47985.
21. Patel RV, Peterson EL, Silverman N, Zarowitz BJ. Estimation
of total body and extracellular water in post-coronary
artery bypass surgical patients using single and multiple
frequency bioimpedance. Crit Care Med 1996;24:18248.22. Hannan WJ, Cowen SJ, Plester CE, Fearon KCH, de Beau A.
Comparison of bio-impedance spectroscopy and multi-frequency bio-impedance analysis for the assessment of
extracellular and total body water in surgical patients. Clin
Sci 1995;89:6518.23. Olde Rikkert MGM, Deurenberg P, Jansen RWMM, vant Hof
MA, Hoefnagels WHL. Validation of multifrequency bioelec-
trical impedance analysis in detecting changes in geriatricpatients. J Am Geriatr Soc 1997;45:134551.
24. Hanai T. Electrical properties of emulsions. In: Sherman PH,
editor. Emulsion science. UK: Academic; 1968. p. 354477.
25. Cornish BH, Ward LC, Thomas BJ, S.A. J, Elia M. Evaluationof multiple frequency bioelectrical impedance and Cole
Cole analysis for the assessment of body water volumes inhealthy humans. Eur J Clin Nutr 1996;50:15964.26. Patel RV, Peterson EL, Silverman N, Zarowitz BJ. Estimation
of total body and extracellular water using single- andmultiple-frequency bioimpedance. Ann Pharmacother1994;28:5659.
27. Schoeller DA. Bioelectrical impedance analysis. What does
it measure? Ann N Y Acad Sci 2000;904:15962.28. Deurenberg P, Andreoli A, de Lorenzo A. Multi-frequency
bioelectrical impedance: a comparison between the ColeCole modelling and Hanai equations with the classicalimpedance index approach. Ann Hum Biol 1996;23:3140.
29. Van Loan MD, Kopp LE, King JC, Wong WW, Mayclin PL. Fluid
changes during pregnancy: use of bioimpedance spectro-scopy. J Appl Physiol 1995;78:103742.
30. Van Marken Lichtenbelt WD, Snel YE, Brummer R-J,Koppeschaar HP. Deuterium and bromide dilution, and
bioimpedance spectrometry independently show that
growth hormone-deficient adults have an enlarged extra-
cellular water compartment related to intracellular water.
J Clin Endocr Metab 1997;82:90711.
31. Ellis KJ, Wong WW. Human hydrometry: comparison of
multifrequency bioelectrical impedance with 2H2O andbromine dilution. J Appl Physiol 1998;85:105662.
32. Cox-Reijven PL, Soeters PB. Validation of bio-impedance
spectroscopy: effects of degree of obesity and ways of
calculating volumes from measured resistance values. Int JObesity Rel Metab Disord 2000;24:27180.
33. Hannan WJ, Cowen SJ, Plester C, Fearson KCH. Proximal
and distal measurements of extracellular and total bodywater by multi-frequency bio-impedance analysis in surgi-
cal patients. Appl Radiat Isot 1998;49:6212.34. Earthman CP, Matthie JR, Reid PM, Harper IT, Ravussin E,
Howell WH. A comparison of bioimpedance methods for
detection of body cell mass change in HIV infection. J Appl
Physiol 2000;88:94456.35. Ho LT, Kushner RF, Schoeller DA, Gudivaka R, Spiegel DM.
Bioimpedance analysis of total body water in hemodialysis
patients. Kidney Int 1994;46:143842.36. Baarends EM, Van Marken Lichtenbelt WD, Wouters
EFM, Schols AMWJ. Body-water compartments measured
by bio-electrical impedance spectroscopy in patients with
chronic obstructive pulmonary disease. Clin Nutr 1998;17:1522.
ARTICLE IN PRESS
1240 U.G. Kyle et al.
-
8/7/2019 Bioelectrical impedance analysis-part I review of principle and methods
16/18
37. Scharfetter H, Monif M, Laszlo Z, Lambauer T, Hutten H,
Hinghofer-Szalkay H. Effect of postural changes on thereliability of volume estimations from bioimpedance
spectroscopy data. Kidney Int 1997;51:107887.
38. Organ LW, Bradham GB, Gore DT, Lozier SL. Segmentalbioelectrical impedance analysis: theory and application of
a new technique. J Appl Physiol 1994;77:98112.
39. Zhu F, Schneditz D, Levin NW. Sum of segmental bioimpe-
dance analysis during ultrafiltration and hemodialysisreduces sensitivity to changes in body position. Kidney Int1999;56:6929.
40. Scheltinga MR, Jacobs DO, Kimbrough TD, Wilmore DW.Identifying body fluid distribution by measuring electrical
impedance. J Trauma 1992;33:66570.
41. De Lorenzo AD, Andreoli A. Segmental bioelectricalimpedance analysis. Curr Opin Clin Nutr Metab Care2003;6:5515.
42. Foster KR, Lukaski HC. Whole-body impedanceFwhat does
it measure? Am J Clin Nutr 1996;64:388S96S.
43. Pirlich M, Schutz T, Spachos T, et al. Bioelectrical
impedance analysis is a useful bedside technique to assessmalnutrition in cirrhotic patients with and without ascites.
Hepatology 2000;32:1208
15.44. Bracco D, Thiebaud D, Chiolero R, Landry M, Burckhardt P,Schutz Y. Segmental body composition assessed by bioelec-
trical impedance analysis and DEXA in humans. J ApplPhysiol 1996;81:25807.
45. Tagliabue A, Andreoli A, Comelli M, et al. Prediction of lean
body mass from multifrequency segmental impedance:
influence of adiposity. Acta Diabetol 2001;38:937.46. Scharfetter H, Schlager T, Stollberger R, Felsberger R,
Hutten H, Hinghofer-Szalkay H. Assessing abdominal
fatness with local bioimpedance analysis: basics andexperimental findings. Int J Obesity Rel Metab Disord2001;25:50211.
47. Rutkove SB, Aaron R, Shiffman CA. Localized bioimpedance
analysis in the evaluation of neuromuscular disease. Muscle
Nerve 2002;25:390
7.48. Piccoli A, Piazza P, Noventa D, Pillon L, Zaccaria M. A new
method for monitoring hydration at high altitude by
bioimpedance analysis. Med Sci Sports Exerc1996;28:151722.
49. Piccoli A, Pittoni G, Facco E, Favaro E, Pillon L. Relationship
between central venous pressure and bioimpedance vector
analysis in critically ill patients. Crit Care Med 2000;28:1327.
50. Ward L, Heitmann BL. Comments on Electrical matura-
tion trajectory of human tissues identified by bioelec-
trical impedance vector analysis. Nutrition 2000;16:31920.
51. Cox-Reijven PL, van Kreel B, Soeters PB. Bioelectrical
impedance measurements in patients with gastrointestinaldisease: validation of the spectrum approach and a
comparison of different methods for screening for nutri-tional depletion. Am J Clin Nutr 2003;78:11119.
52. OBrien C, Young AJ, Sawka MN. Bioelectrical impedance to
estimate changes in hydration status. Int J Sports Med2002;23:3616.
53. Heitmann B. Impedance: a valid method in assessment of
body composition. Eur J Clin Nutr 1994;48:22840.
54. Battistini N, Virgili F, Bedogni G, Gambella GR, Bini A. Invivo total body water assessment by total body electrical
conductivity in rats suffering perturbations of water
compartment equilibrium. Brit J Nutr 1993;70:4338.55. De Lorenzo A, Deurenberg P, Andreoli A, Sasso GF, Palestini
M, Docimo R. Multifrequency impedance in the assessment
of body water losses during dialysis. Ren Physiol Biochem1994;17:32632.
56. Fomon SJ, Haschke F, Ziegler EE, Nelson SE. Body
composition of reference children from birth to age 10
years. Am J Clin Nutr 1982;35:116975.57. Ellis KJ, Bell SJ, Chertow GM, et al. Bioelectrical
impedance methods in clinical research: a follow-up to
the NIH Technology Assessment Conference. Nutrition1999;15:87480.
58. Kotler DP, Burastero S, Wang J, Pierson Jr RN. Prediction of
body cell mass, fat-free mass, and total body water with
bioelectrical impedance analysis: effects of race, sex, anddisease. Am J Clin Nutr 1996;64:489S97S.
59. Scharfetter H, Wirnsberger GH, Holzer H, Hutten H.Influence of ionic shifts during dialysis on volume estima-
tions with multifrequency impedance analysis. Med Biol
Eng Comput 1997;35:96102.60. Martinoli R, Mohamed EI, Maiolo C, et al. Total body water
estimation using bioelectrical impedance: a meta-analysis
of the data available in the literature. Acta Diabetol
2003;40(Suppl 1):S203S206.61. Selberg O, B .ottcher J, Tusch G, Pichlmayr R, Henkel E,
M.
uller MJ. Identification of high- and low-risk patientsbefore liver transplantation: a prospective cohort study ofnutritional and metabolic parameters in 150 patients.
Hepatology 1997;25:6527.62. Kotler D, Tierney A, Wang J, Pierson RJ. Magnitude of body-
cell-mass depletion and the timing of death from wasting in
AIDS. Am J Clin Nutr 1989;50:4447.
63. Pirlich M, Schutz T, Ockenga J, et al. Improved assessmentof body cell mass by segmental bioimpedance analysis in
malnourished subjects and acromegaly. Clin Nutr2003;22:16774.
64. Ward LC, Heitmann BL. Assessment of body composition by
bioelectrical impedance analysis without the need for
measurement of height. Clin Nutr 2001;20:216.
65. Kushner RF, Schoeller DA. Estimation of total body water by
bioelectrical impedance analysis. Am J Clin Nutr 1986;44:41724.
66. Segal KR, Gutin B, Presta E, Wang J, Van Itallie TB.
Estimation of human body composition by electrical
impedance methods: a comparative study. J Appl Physiol1985;58:156571.
67. Lukaski HC, Johnson PE, Bolonchuk WW, Lykken GL.
Assessment of fat-free mass using bioelectrical impedancemeasurements of the human body. Am J Clin Nutr1985;41:8107.
68. Ward LC, Byrne NM, Rutter K, et al. Reliability of mul-
tiple frequency bioelectrical impedance analysis: anintermachine comparison. Am J Human Biol 1997;9:
6372.69. Jansen DF, Korbijn CM, Deurenberg P. Variability of body
density and body impedance at different frequencies. Eur J
Clin Nutr 1992;46:86571.70. Sun SS, Chumlea WC, Heymsfield SB, et al. Development of
bioelectrical impedance analysis prediction equations for
body composition with the use of a multicomponent model
for use in epidemiologic surveys. Am J Clin Nutr 2003;77:33140.
71. Kushner RF. Bioelectrical impedance analysis a review of
principles and applications. J Am Coll Nutr 1992;11:199209.
72. Pichard C, Kyle UG, Janssens JP, et al. Body composition by
X-ray absorptiometry and bioelectrical impedance inchronic respiratory insufficiency patients. Nutrition1997;13:9528.
ARTICLE IN PRESS
Bioelectrical impedance analysis 1241
-
8/7/2019 Bioelectrical impedance analysis-part I review of principle and methods
17/18
73. Gonzalez CH, Evans JA, Smye SW, Holland P. Total body
water measurement using bioelectrical impedance analy-sis, isotope dilution and total body potassium: a scoring
system to facilitate intercomparison. Eur J Clin Nutr2002;56:32637.
74. Kyle UG, Genton L, Karsegard L, Slosman DO, Pichard C.
Single prediction equation for bioelectrical impedance
analysis in adults aged 2094 years. Nutrition2001;17:24853.
75. Lohman TG. Advances in body composition assessment.
Champaign, IL: Human Kinetics Publishers; 1992.
76. Deurenberg P, van der Kooy K, Leenen R, Westrate JA,Seidell JC. Sex and age specific prediction formulas for
estimating body composition from bioelectrical impe-
dance: a cross-validation study. Int J Obesity 1991;15:1725.
77. Stolarczyk LM, Heyward VH, Hicks VL, Baumgartner RN.Predictive accuracy of bioelectrical impedance in estimat-
ing body composition of Native American women. Am J Clin
Nutr 1994;59:96470.
78. Heitmann BL. Prediction of body water and fat in adultDanes from measurement of electrical impedance. A
validation study. Int J Obesity 1990;14:417
24.79. Jakicic JM, Wing RR, Lang W. Bioelectrical impedanceanalysis to assess body composition in obese adult women:
the effect of ethnicity. Int J Obesity 1998;22:2439.
80. Haapala I, Hirvonen A, Niskanen L, et al. Anthropometry,bioelectrical impedance and dual-energy X-ray absorptio-
metry in the assessment of body composition in elderly
Finnish women. Clin Phys Physiol Meas 2002;22:38391.81. Roubenoff R, Baumgartner RN, Harris TB, et al. Application
of bioelectrical impedance analysis to elderly population.
J Gerontol 1997;52A:M12936.82. Baumgartner RN, Heymsfield SB, Lichtman S, Wang J,
Pierson RNJ. Body composition in elderly people: effect of
criterion estimates on predictive equations. Am J Clin Nutr1991;53:134553.
83. Dey DK, Bosaeus I, Lissner L, Steen B. Body compositionestimated by bioelectrical impedance in the Swedishelderly. Development of population-based prediction equa-
tion and reference values of fat-free mass and body fat for
70- and 75-y olds. Eur J Clin Nutr 2003;57:90916.84. Deurenberg P, van der Kooij K, Evers P, Hulshof T.
Assessment of body composition by bioelectrical impe-
dance in a population aged greater than 60 y. Am J ClinNutr 1990;51:36.
85. Siri WE. Body volume measurement by gas dilution. In:
Brozek J, editor. Techniques of measuring body composi-tion. Washington, DC: National Academy of Sciences,National Research Council; 1961. p. 10817.
86. Siri WE. Body composition from fluid spaces and density:
analysis of methods. In: Brozek J, editor. Techniques of
measuring body composition. Washington, DC: National
Academy of Sciences, National Research Council; 1961.p. 22344.
87. Deurenberg P, Smit HE, Kusters CS. Is the bioelectrical
impedance method suitable for epidemiological field
studies? Eur J Clin Nutr 1989;43:64754.88. Bruce A, Andersson M, Arvidsson B, Isaksson B. Body
composition. Prediction of normal body potassium, body
water and body fat in adults on the basis of body height,body weight and age. Scand J Clin Lab Invest 1980;40:
46173.
89. Heitmann BL. Evaluation of body fat estimated from bodymass index, skinfolds and impedance. A comparative study.
Eur J Clin Nutr 1990;44:8317.
90. Deurenberg P, Tagliabue A, Schouten FJM. Multi-frequency
impedance for the prediction of extracellular water andtotal body water. Brit J Nutr 1995;73:34958.
91. Vach!e C, Rousset P, Gachon P, et al. Bioelectrical
impedance analysis measurements of total body waterand extracellular water in healthy elderly subjects. Int J
Obesity 1998;22:53743.
92. Van Loan MD, Mayclin PL. Use of multi-frequency bioelec-
trical impedance analysis for the estimation of extracel-lular fluid. Eur J Clin Nutr 1992;46:11724.
93. Visser M, Deurenberg P, van Staveren WA. Multi-frequency
bioelectrical impedance for assessing total body water andextracellular water in elderly subjects. Eur J Clin Nutr1995;49:25666.
94. De Lorenzo A, Sorge RP, Candeloro C, Di Campli C, Sesti G,
Lauro R. New insights into body composition assess-
ment in obese women. Can J Physiol Pharmacol 1999;77:1721.
95. Sergi G, Bussolotto M, Perini P, et al. Accuracy of
bioelectrical impedance analysis in estimation of extra-
cellular spaces in healthy subjects and in fluid retention.
Ann Nutr Metab 1992;38:15865.
96. Dittmar M, Reber H. Evaluation of different methodsfor assessing intracellular fluid in healthy older people:a cross-validation study. J Am Geriatr Soc 2002;50:
10410.97. De Lorenzo A, Candeloro N, Andreoli A, Deurenberg P.
Determination of intracellular water by multifre-
quency bioelectrical impedance. Ann Nutr Metab 1995;39:
17784.98. Dittmar M, Reber H. New equations for estimating body cell
mass from bioimpedance parallel models in healthy older
Germans. Am J Physiol Endocrinol Metab 2001;281:E1005E1014.
99. Houtkooper LB, Lohman TG, Going SB, Howell WH. Why
bioelectrical impedance analysis should be used for
estimating adiposity. Am J Clin Nutr 1996;64:436S48S.
100. Heymsfield SB, Nunez C, Testolin C, Gallagher D. Anthro-pometry and methods of body composition measurementfor research and field application in the elderly. Eur J Clin
Nutr 2000;54:S2632.
101. Pietrobelli A, Heymsfield SB, Wang ZM, Gallagher D. Multi-component body composition models: recent advances and
future directions. Eur J Clin Nutr 2001;55:6975.
102. Pietrobelli A, Wang ZM, Heymsfield SB. Techniques used inmeasuring human body composition. Curr Opin Clin Nutr
Metab Care 1998;1:43948.
103. Wagner DR, Heyward VH. Techniques of body composition
assessment: a review of laboratory and field methods. Res
Q Exerc Sport 1999;70:13549.
104. Heymsfield SB, Waki M. Body composition in humans:advances in the development of multicompartment che-
mical models. Nutr Rev 1991;49:97
108.
105. Genton L, Hans D, Kyle UG, Pichard C. Dual-energy X-rayabsorptiometry and body composition: differences be-
tween devices and comparison with reference methods.
Nutrition 2002;18:6670.
106. Tylavsky FA, Lohman TG, Dockrell M, et al. Comparisonof the effectiveness of 2 dual-energy X-ray absorptio-
meters with that of total body water and computed
tomography in assessing changes in body composi-tion during weight change. Am J Clin Nutr 2003;77:
35663.
107. Moore FD, Boyden CM. Body cell mass and limits ofhydration of the fat-free body: their relation to estimated
skeletal weight. Ann N Y Acad Sci 1963;110:6271.
ARTICLE IN PRESS
1242 U.G. Kyle et al.
-
8/7/2019 Bioelectrical impedance analysis-part I review of principle and methods
18/18
108. Kehayias JJ, Fiatarone MA, Zhuang H, Roubenoff R. Totalbody potassium and body fat: relevance to aging. Am J ClinNutr 1997;66:90410.
109. Kyle UG, Genton L, Hans D, Karsegard L, Slosman D, PichardC. Age-related differences in fat-free, skeletal muscle,body cell mass and fat mass between 18 and 94 years ofage. Eur J Clin Nutr 2001;55:66372.
110. Deurenberg P, Deurenberg-Yap M, Schouten FJ. Validity of
total and segmental impedance measurements for predic-tion of body composition across ethnic population groups.Eur J Clin Nutr 2002;56:21420.
111. Deurenberg P, Deurenberg-Yap M. Validity of body composi-tion methods across ethnic population groups. ActaDiabetol 2003;40(Suppl 1):S246S249.
112. Deurenberg P, Weststrate JA, Seidell JC. Body mass indexas a measure of body fatness: age- and sex-specificprediction formula. Brit J Nutr 1991;65:10514.
113. Deurenberg P, Wolde-Gebriel Z, Schouten FJ. Validityof predicted total body water and extracellular water
using multifrequency bioelectrical impedance in anEthiopian population. A nn N ut r M eta b 1995;39:23441.
ARTICLE IN PRESS
Bioelectrical impedance analysis 1243


















