
Binary therapies in the treatment of cancer - stfc.ukri.org · graphite reflector FLUENTAL...
32
Binary therapies in the treatment of cancer translational research from the physics laboratory to the clinic Stuart Green University Hospital Birmingham and British Institute of Radiology STFC Innovations Birmingham, January 2010
Transcript of Binary therapies in the treatment of cancer - stfc.ukri.org · graphite reflector FLUENTAL...
Binary therapies
in the treatment of cancer
translational research
from the physics
laboratory to the clinic
Stuart Green
University Hospital Birmingham and British Institute of Radiology
STFC Innovations
Birmingham, January 2010

Overview of techniques and projects
• External beam treatments
– X-ray therapy
– Proton and ion beam therapy
• Binary therapies
– Boron Neutron Capture Therapy
– High Z enhanced radiotherapy
• Systemic treatment
– Targeted radionuclide therapy
– chemotherapy
localised
disease
locally spread
disease
Systemic disease
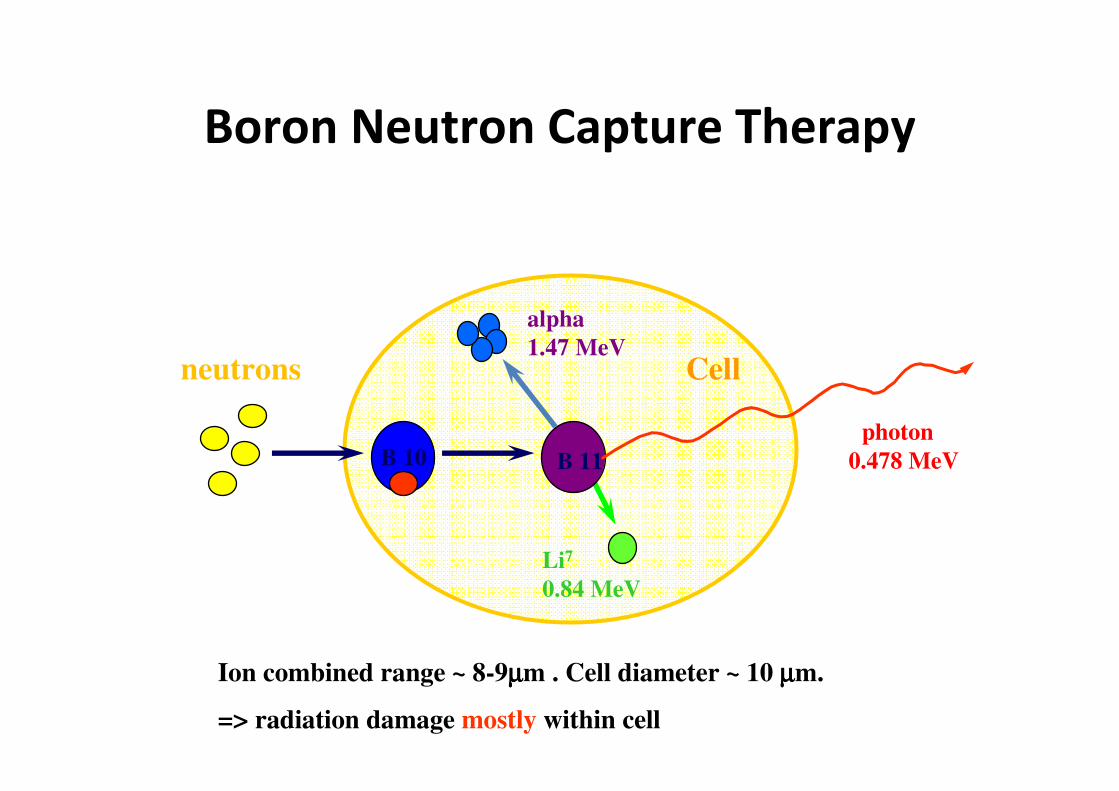
Boron Neutron Capture Therapy
Cell
B 10
neutrons
B 11
Li7
0.84 MeV
alpha
1.47 MeV
photon
0.478 MeV
Ion combined range ~ 8-9µµµµm . Cell diameter ~ 10 µµµµm.
=> radiation damage mostly within cell

Plot is from Kiger et al, Journal of Neuro-Oncology 62:171-186 (2003)
Typical 10B concentrations, 15 µg/g in Blood and Brain, 52.5 µg/g in Tumour
BPA administered is approx 20g for an average person.
BPA pharmacokinetics

Photon Capture Therapy (PCT) - Physics
• Physics of the photo-electric effect is well known
• Energy not used to overcome binding is liberated as
electron kinetic energy (so range is tuneable?)
• Cross section increases roughly as Z4, and decreases
as 1/E3
• Introduction of a high Z material preferentially into a
tumour can significantly increase the local dose for
the same irradiating x-ray fluence

Photon Capture Therapy (PCT)
0.01 0.1
0.01
0.1
1
10
100
m ass absorption coeffic ient
(µ/ρ
) en
E (M eV)
I
G d
P t
A u
H20
Energies released per reaction are in the keV range (for BNCT, they
are in the MeV range) and both are cross-section driven
For similar dose enhancements, PCT requires local contrast agent
concentrations which are approx 1000 x those required for BNCT
Key requirements for binary therapies
• Efficient contrast agents with large interaction
difference from normal body materials
• Contrast agent with very low toxicity (to allow
administration at very high levels)
• Contrast agent must preferentially
accumulate in tumour cells
• Tumour must be accessible to the beam
(epithermal neutrons or low energy photons)
• But do they work?
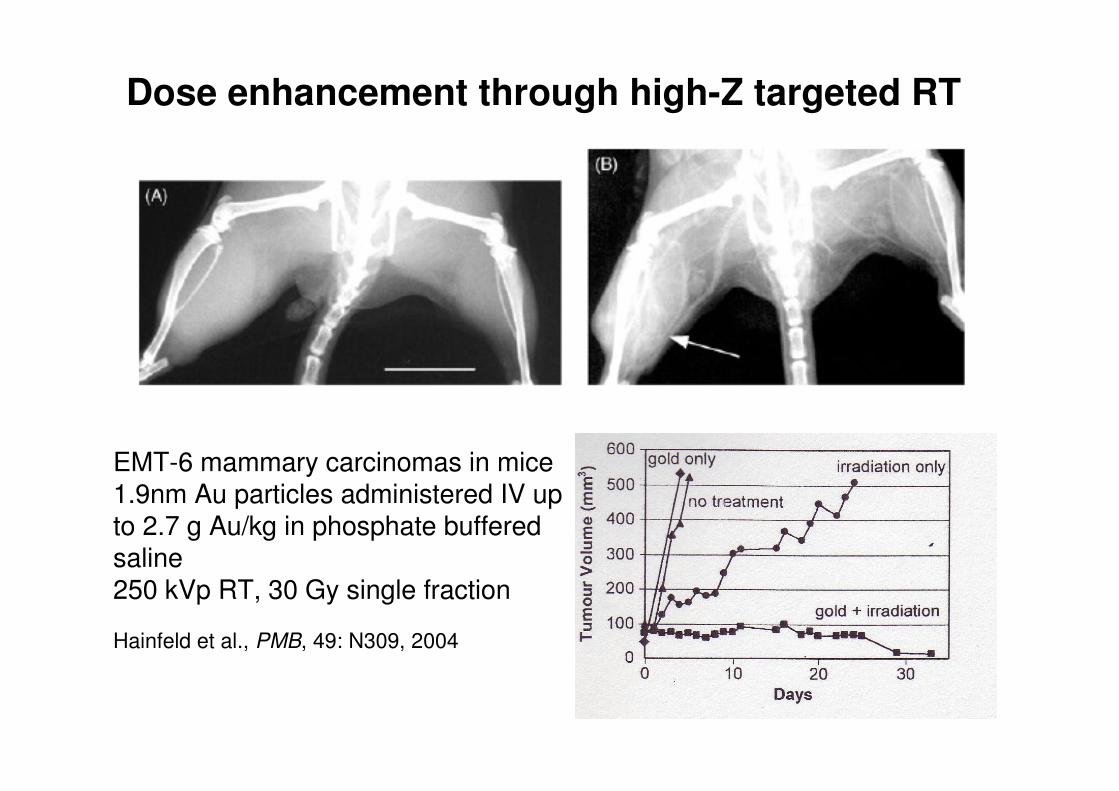
Dose enhancement through high-Z targeted RT
EMT-6 mammary carcinomas in mice1.9nm Au particles administered IV up to 2.7 g Au/kg in phosphate buffered saline250 kVp RT, 30 Gy single fraction
Hainfeld et al., PMB, 49: N309, 2004

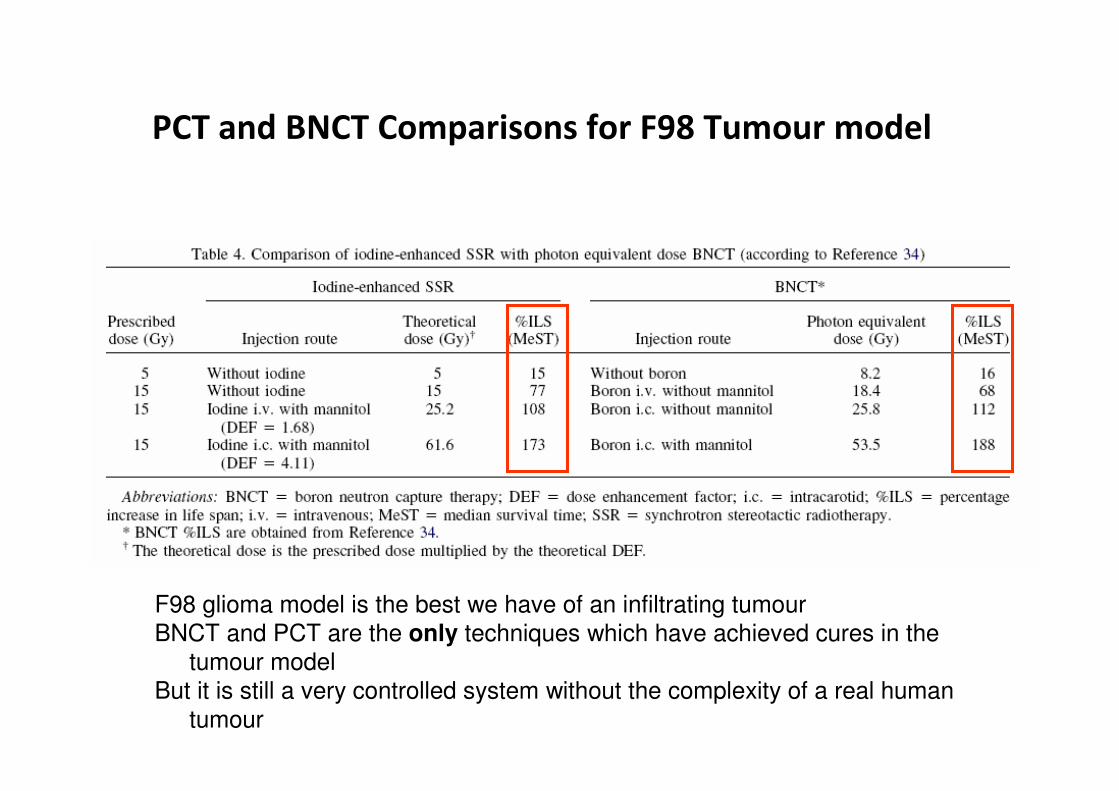
PCT and BNCT Comparisons for F98 Tumour model
F98 glioma model is the best we have of an infiltrating tumour
BNCT and PCT are the only techniques which have achieved cures in the
tumour model
But it is still a very controlled system without the complexity of a real human
tumour

Glioblastoma - clinical course
post-surgery
Head trauma
9M before
9M
Mild headache
Post-chemo-
radiotherapy
Courtesy of Tetsuya Yamamoto, Tsukuba, Japan
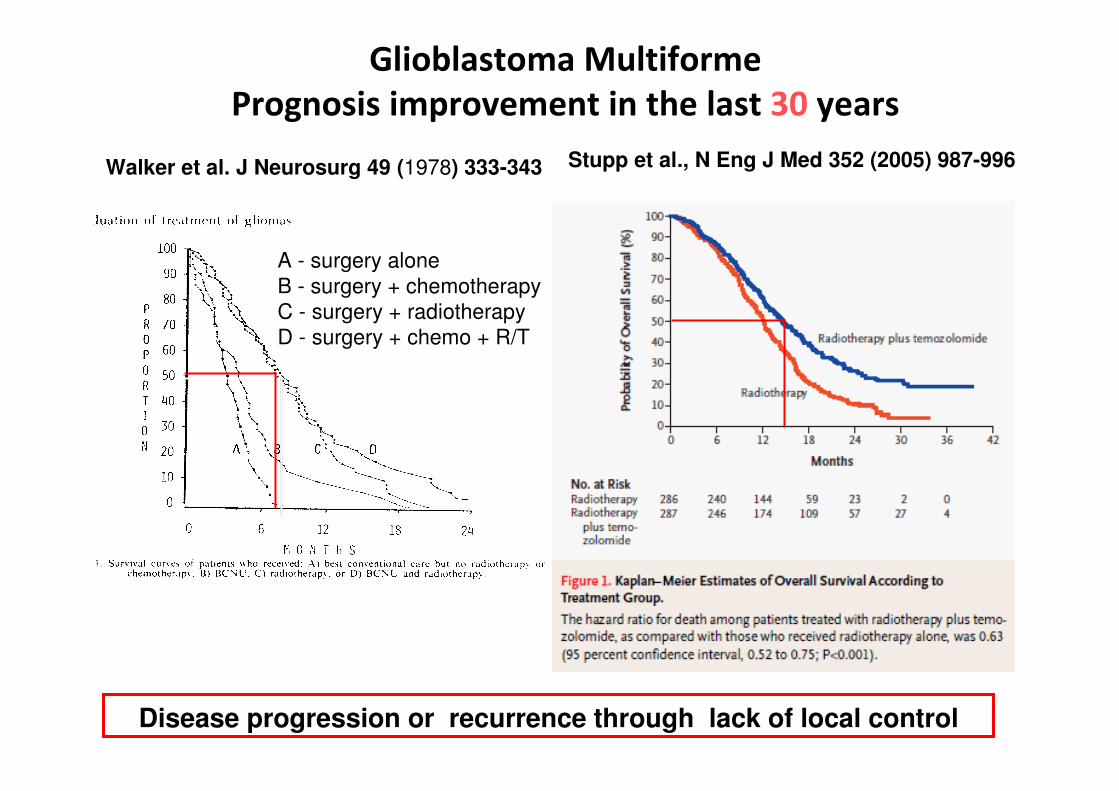
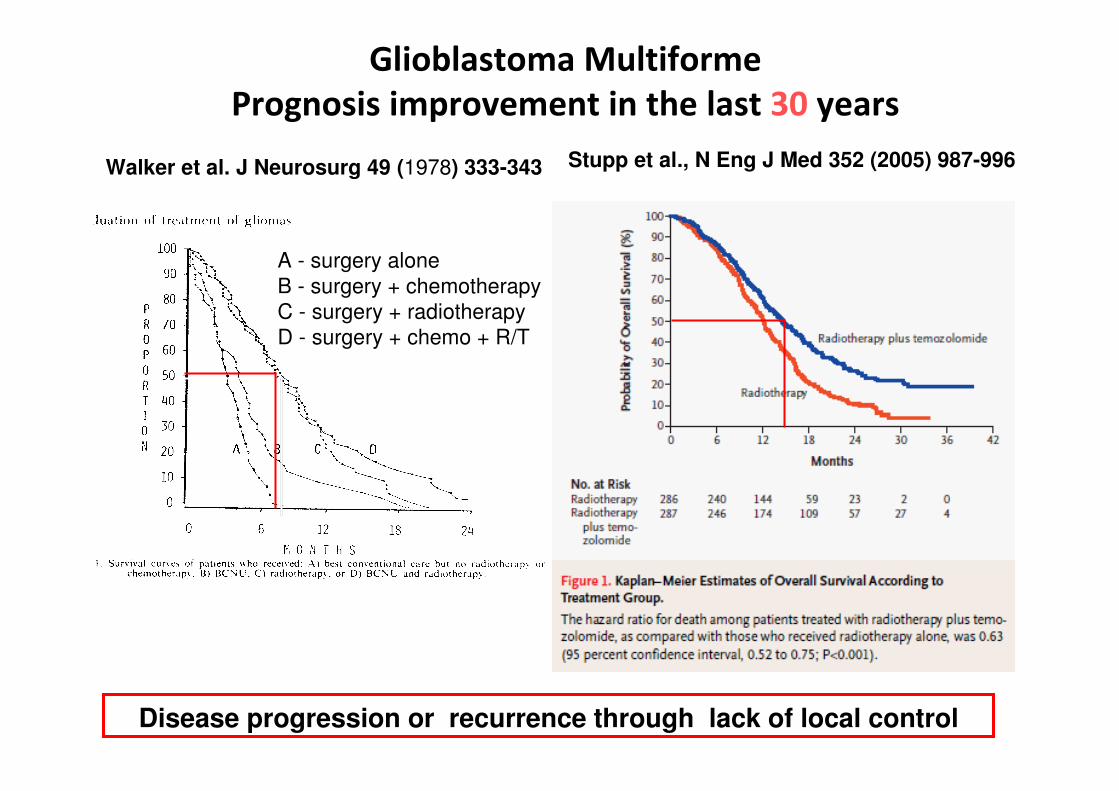
Walker et al. J Neurosurg 49 (1978) 333-343
A - surgery alone
B - surgery + chemotherapy
C - surgery + radiotherapy
D - surgery + chemo + R/T
Su
rviv
al
(%)
Glioblastoma Multiforme
Prognosis improvement in the last 30 years
Stupp et al., N Eng J Med 352 (2005) 987-996
Disease progression or recurrence through lack of local control
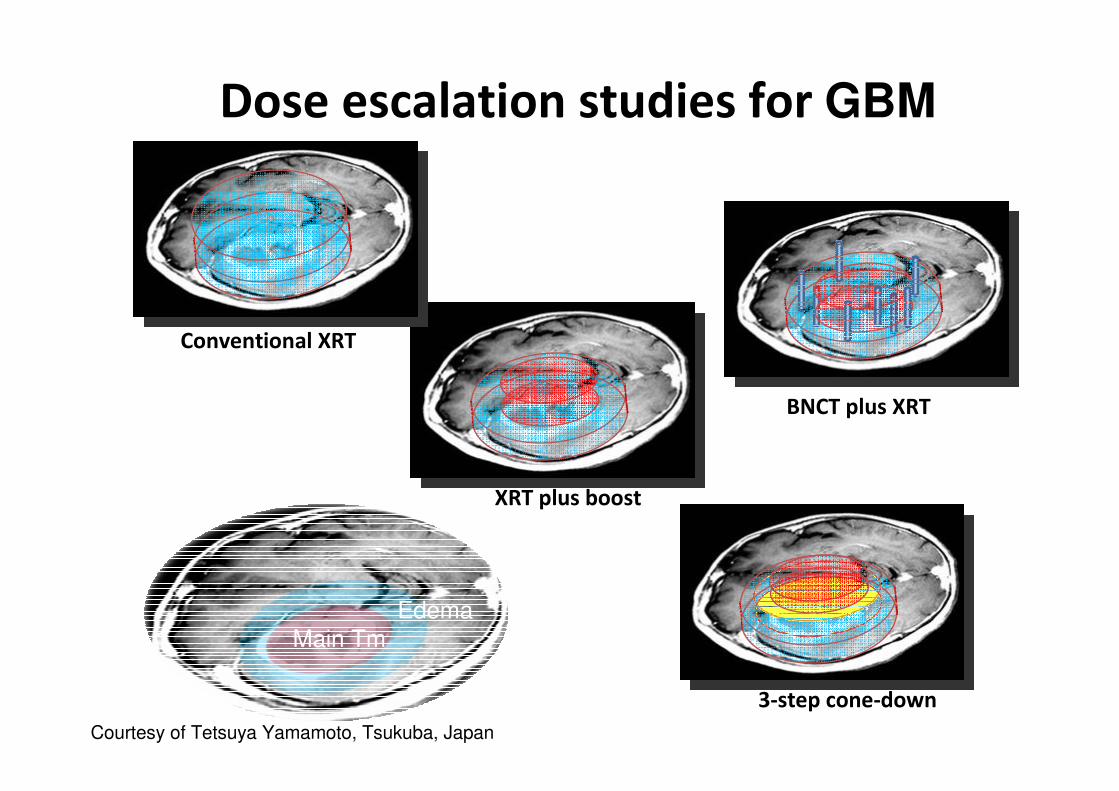
BNCT plus XRT
3-step cone-down
XRT plus boost
Conventional XRT
Dose escalation studies for GBM
EdemaMain Tm
11Courtesy of Tetsuya Yamamoto, Tsukuba, Japan
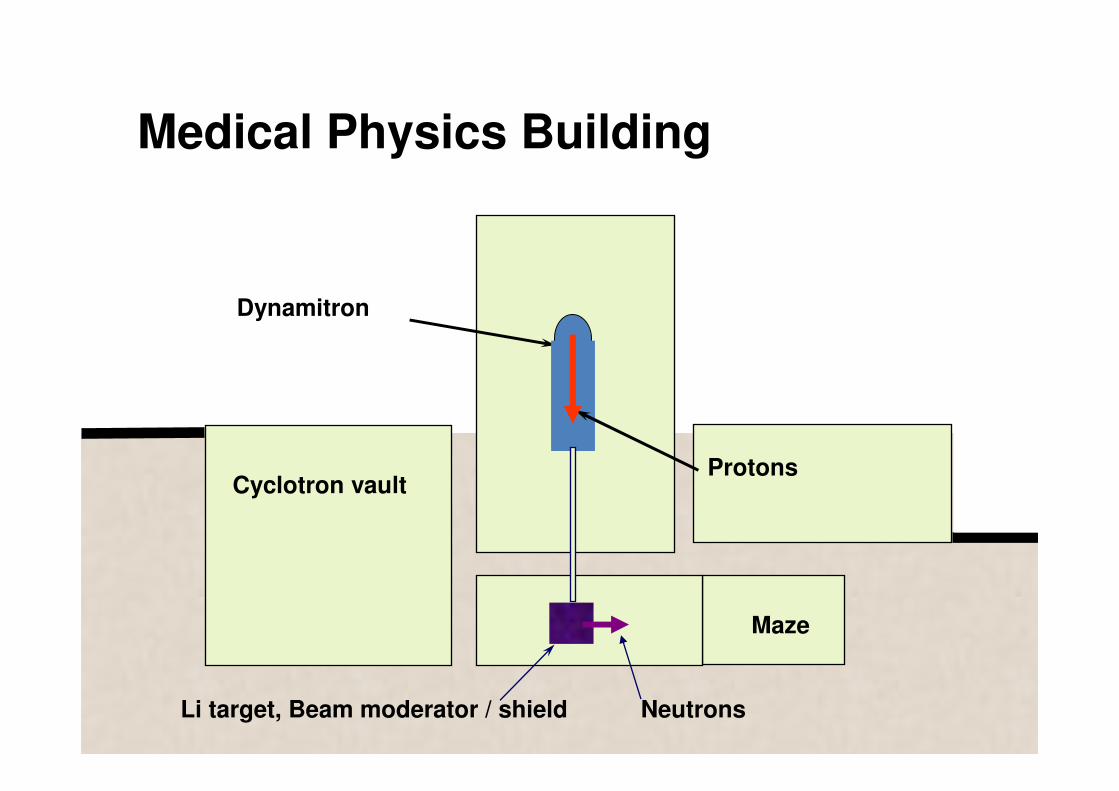
Medical Physics Building
Cyclotron vault
Dynamitron
Protons
NeutronsLi target, Beam moderator / shield
Maze

Neutron generation and moderation
scanned proton beam
shield
graphite reflector
FLUENTAL moderator / shifter
Li target
lead filter
heavy water cooling circuit
Neutron source is > 1 x 1012 s-1
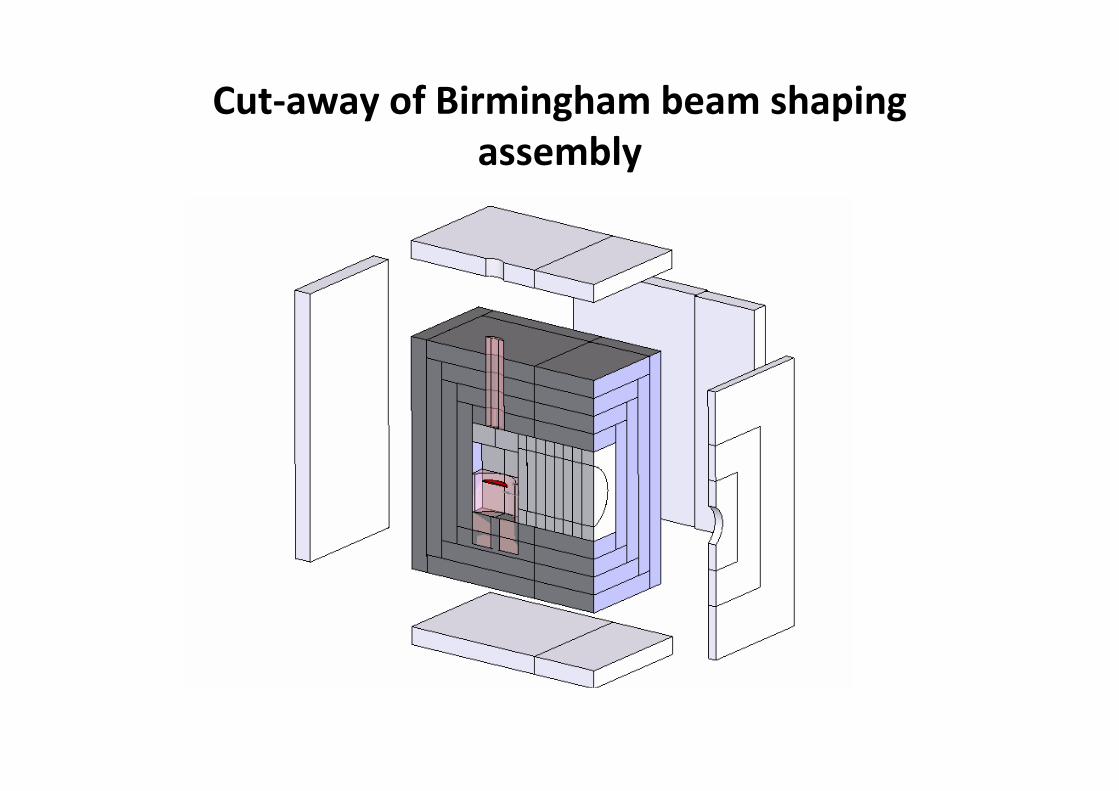
Cut-away of Birmingham beam shaping
assembly

Li target during fabrication

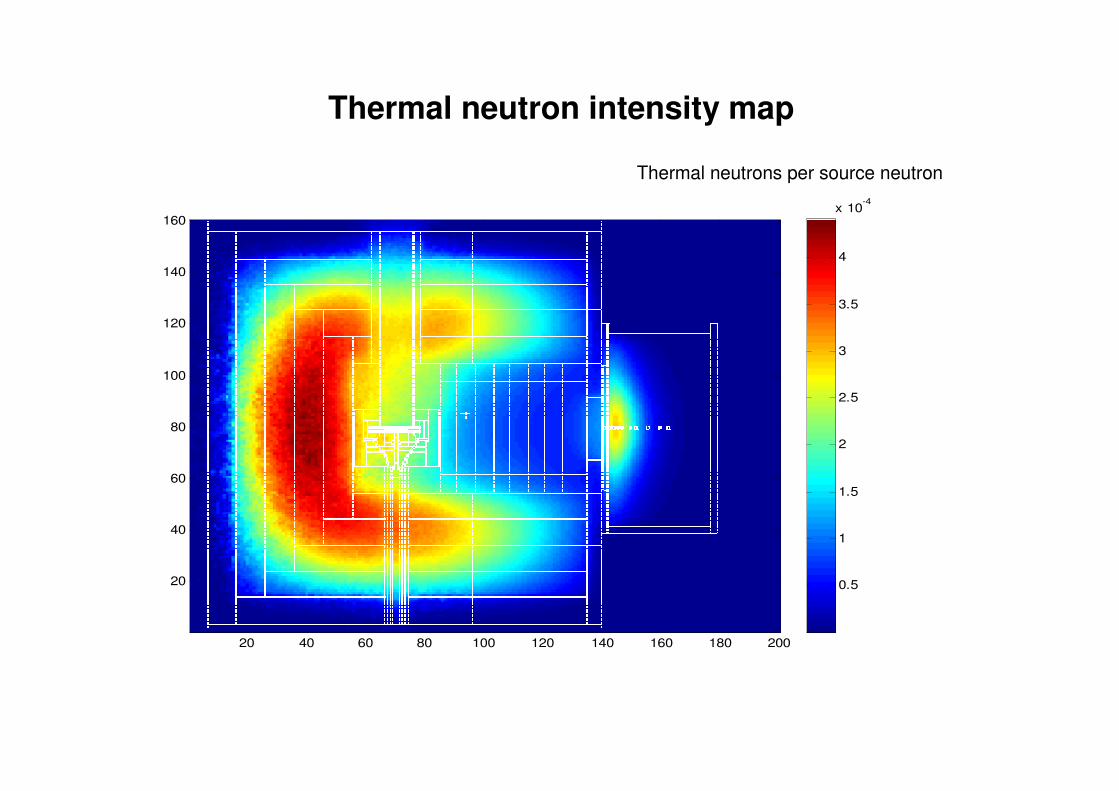
Thermal neutron intensity map
20 40 60 80 100 120 140 160 180 200
20
40
60
80
100
120
140
160
0.5
1
1.5
2
2.5
3
3.5
4
x 10-4
Thermal neutrons per source neutron
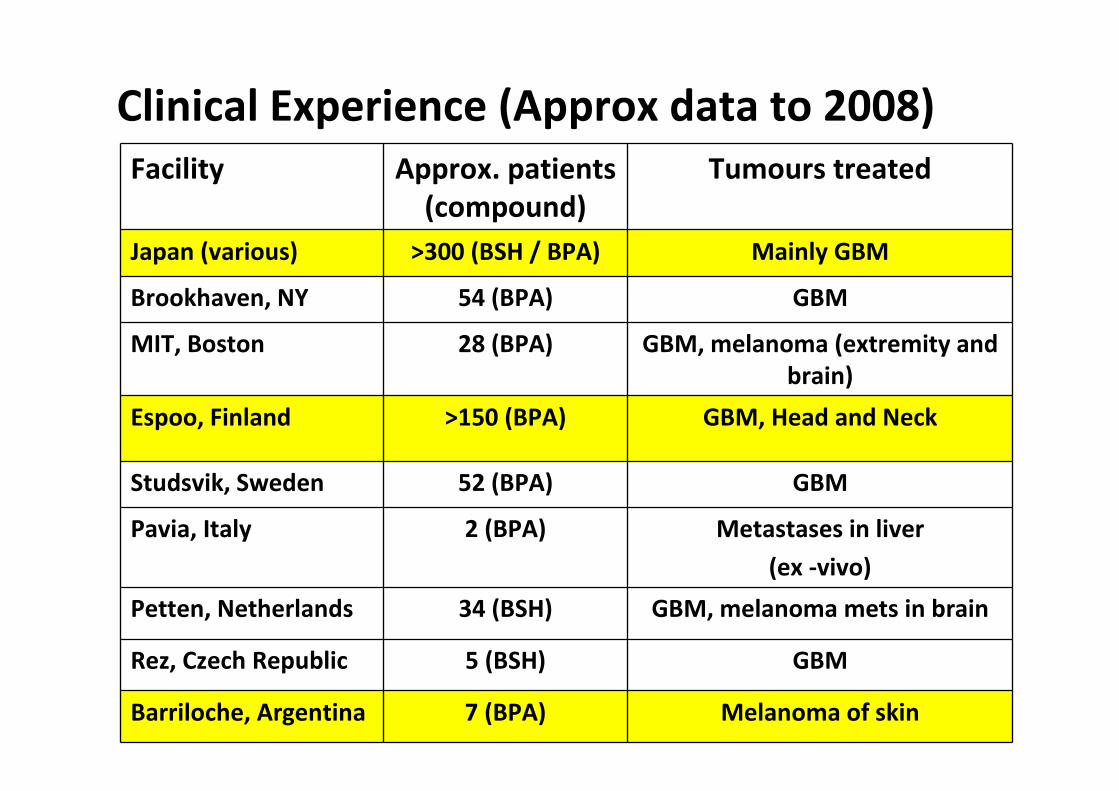
Clinical Experience (Approx data to 2008)
Facility Approx. patients
(compound)
Tumours treated
Japan (various) >300 (BSH / BPA) Mainly GBM
Brookhaven, NY 54 (BPA) GBM
MIT, Boston 28 (BPA) GBM, melanoma (extremity and
brain)
Espoo, Finland >150 (BPA) GBM, Head and Neck
Studsvik, Sweden 52 (BPA) GBM
Pavia, Italy 2 (BPA) Metastases in liver
(ex -vivo)
Petten, Netherlands 34 (BSH) GBM, melanoma mets in brain
Rez, Czech Republic 5 (BSH) GBM
Barriloche, Argentina 7 (BPA) Melanoma of skin

BPA accumulation via the Phenylalanine transport mechanism
• Uptake of amino-acids into cells is surprisingly poorly understood
• Thought to be selectively transported across the blood brain barrier, endothelial cells and astrocytic cells by a common LAT-1 transporter system.
• LAT-1 is up-regulated in tumour cells and might be expected to enhance the concentration of L amino acids particularly in tumour cells.
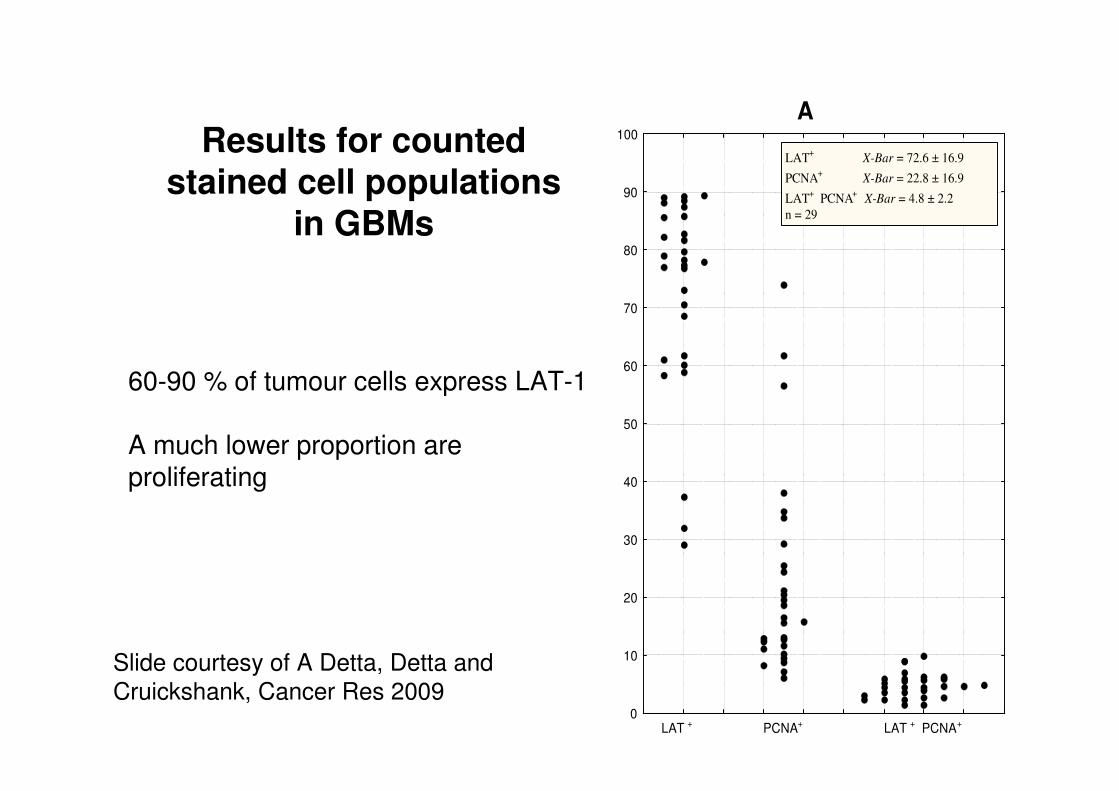
Results for counted stained cell populations
in GBMs
A
0
10
20
30
40
50
60
70
80
90
100
LAT + PCNA+ LAT + PCNA+
LAT+ X-Bar = 72.6 ± 16.9
PCNA+ X-Bar = 22.8 ± 16.9
LAT+ PCNA
+ X-Bar = 4.8 ± 2.2
n = 29
60-90 % of tumour cells express LAT-1
A much lower proportion are proliferating
Slide courtesy of A Detta, Detta and
Cruickshank, Cancer Res 2009
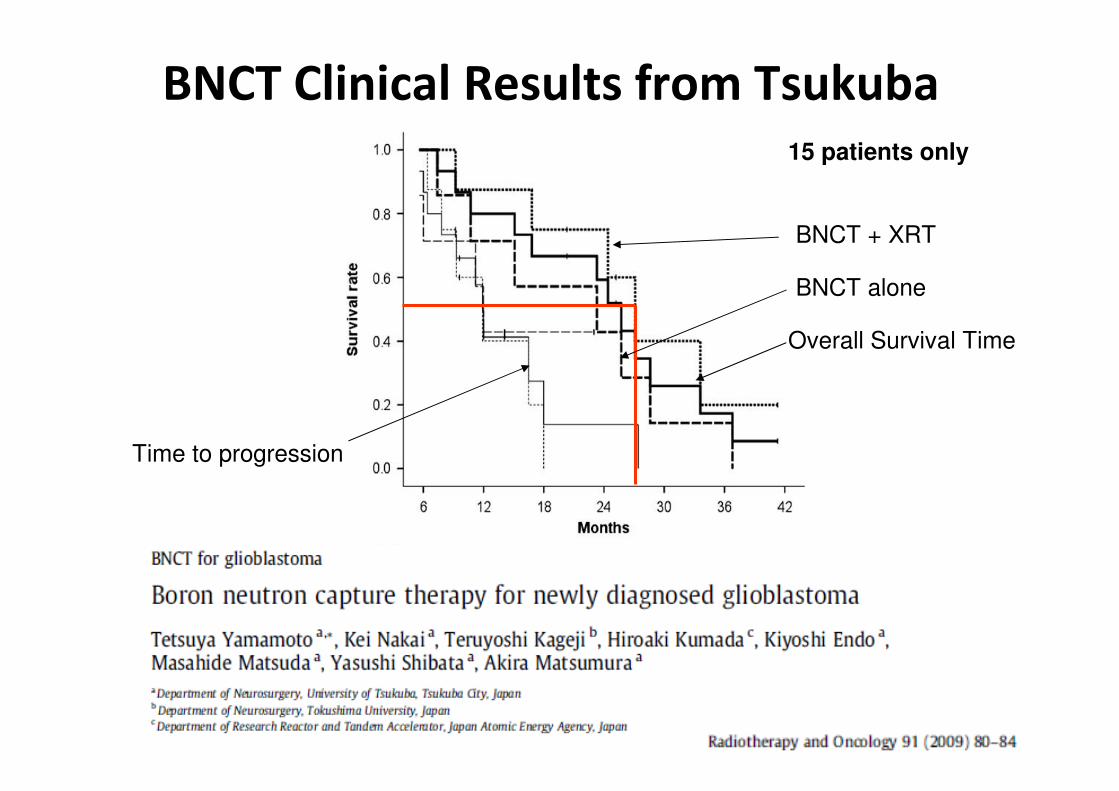
BNCT Clinical Results from Tsukuba15 patients only
Overall Survival Time
Time to progression
BNCT alone
BNCT + XRT
Walker et al. J Neurosurg 49 (1978) 333-343
A - surgery alone
B - surgery + chemotherapy
C - surgery + radiotherapy
D - surgery + chemo + R/T
Su
rviv
al
(%)
Glioblastoma Multiforme
Prognosis improvement in the last 30 years
Stupp et al., N Eng J Med 352 (2005) 987-996
Disease progression or recurrence through lack of local control
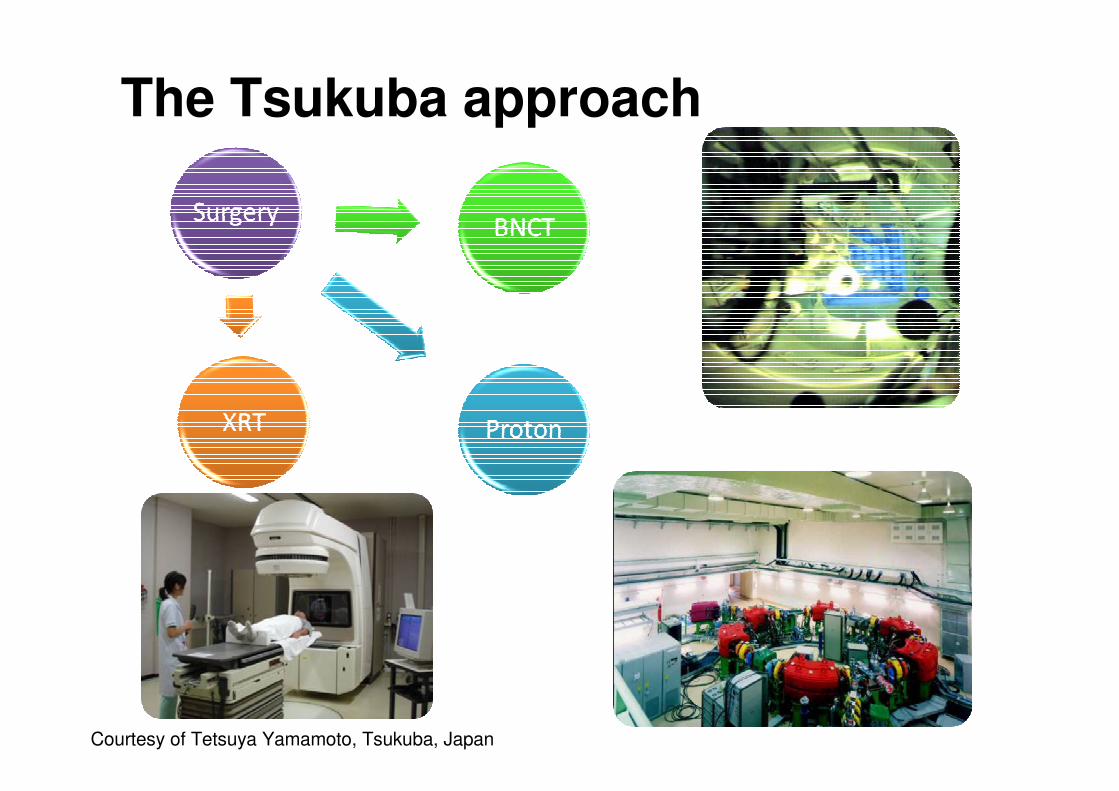
The Tsukuba approach
Courtesy of Tetsuya Yamamoto, Tsukuba, Japan

Final thoughts
• Different treatment strategies are required depending on the type, stage and degree of spread of the cancer to be treated
• Binary therapies are aimed specifically at tumours which exhibit a high degree of infiltration into the surrounding healthy tissues
• Binary therapies are still at a very early stage of development (patient numbers for BNCT still < 1000)
• They require input from a wide range of scientific disciplines
• They are ripe for investment and provide a great opportunity for the UK to take a lead
• Can we afford to miss this opportunity ? (as we did with particle therapy)
• What can UK Research Councils do to help ?

Collaborations and Acknowledgements
UHB Trust: Profs Alun Beddoe and Bleddyn Jones (now Oxford), Drs Cecile
Wojnecki and Richard Hugtenburg (now Swansea Uni), Dr Spyros
Manolopoulos (ex STFC)
University of Birmingham: Profs David Parker and Garth Cruickshank, Drs
Monty Charles and Andy Mill
University of Oxford: Dr Mark Hill
PhD students: Zamir Ghani, Ben Phoenix, Shane O’Hehir, Adam Baker and
Mohammed Sidek
Funding bodies, EPSRC, CR-UK, UHB Charities

Work of Biston et al, Cures of rats bearing radioresistant F98 Glioma
tumours
• F98 glioma model is the best we have of an infiltrating tumour
• Pt-based chemotherapy drug (CDDP) administered via intra-tumoral injection (3 mg in 5 ml saline)
• Synchrotron irradiation at various energies above / below Pt K-edge
• Best median survival times at 78.8 keV (above Pt K-edge) = 206 days
• Best previous results for this tumour model are with BNCT where median survival time = 72 days (Barth et al, IJROBP 2000, 47, 209-1218)
CANCER RESEARCH 64, 2317–2323, April 1, 2004
This success has lead to further work to plan human clinical trials, although big questions remain on the nature of the observed effect

high Z
SR
1. Administration of a high Z element
therapy either via physical dose enhancementalone or from combination with chemotherapy (administration of a platinum chemotherapy drug)
beam fitted to the tumour size tumour = center of rotation monochromatic beam
2. Irradiation in tomography mode
Synchrotron Stereotactic Radiotherapy (SSR)
S
R
From the work of Boudou et al based around ESRF, Grenoble
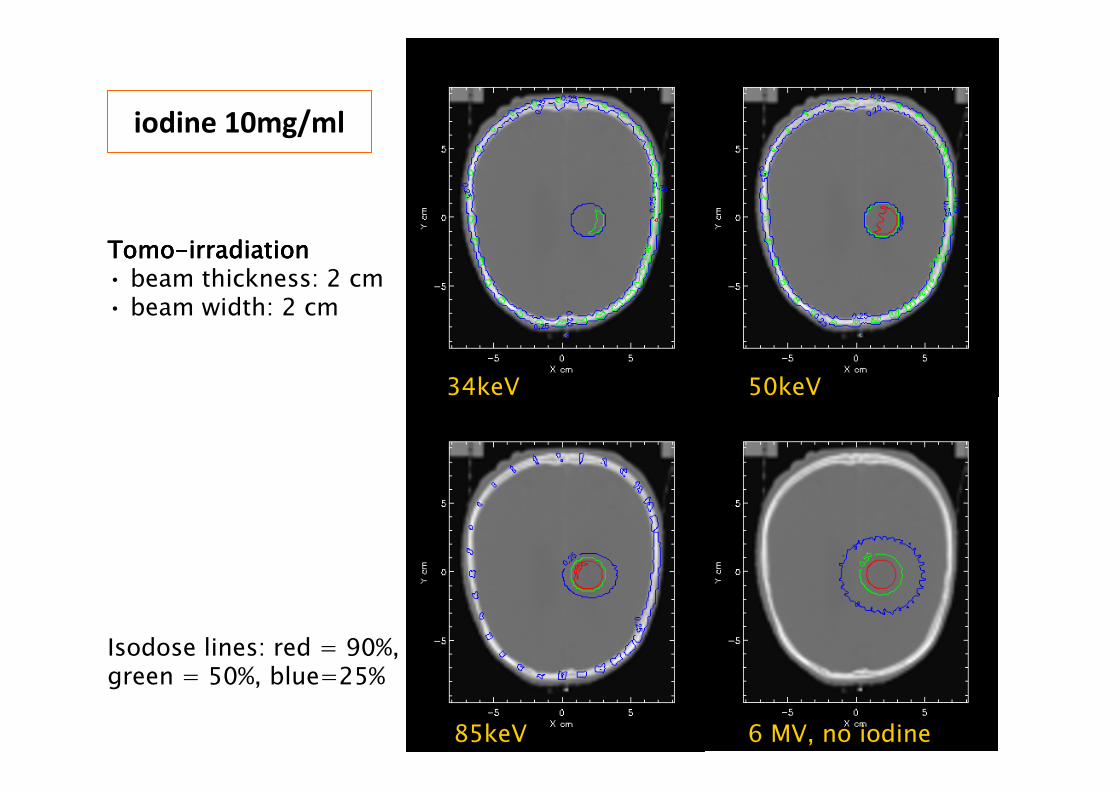
34keV 50keV
85keV
iodine 10mg/ml
TomoTomoTomoTomo----irradiationirradiationirradiationirradiation• beam thickness: 2 cm• beam width: 2 cm
Isodose lines: red = 90%, green = 50%, blue=25%
6 MV, no iodine
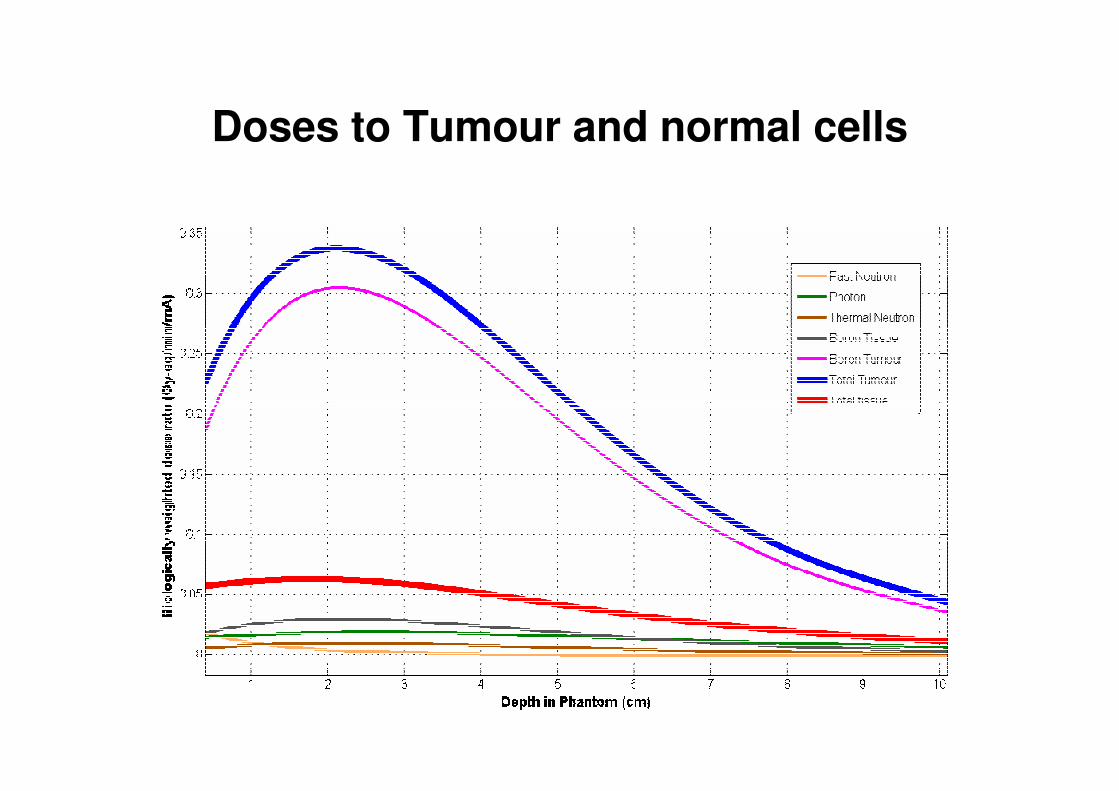
Doses to Tumour and normal cells
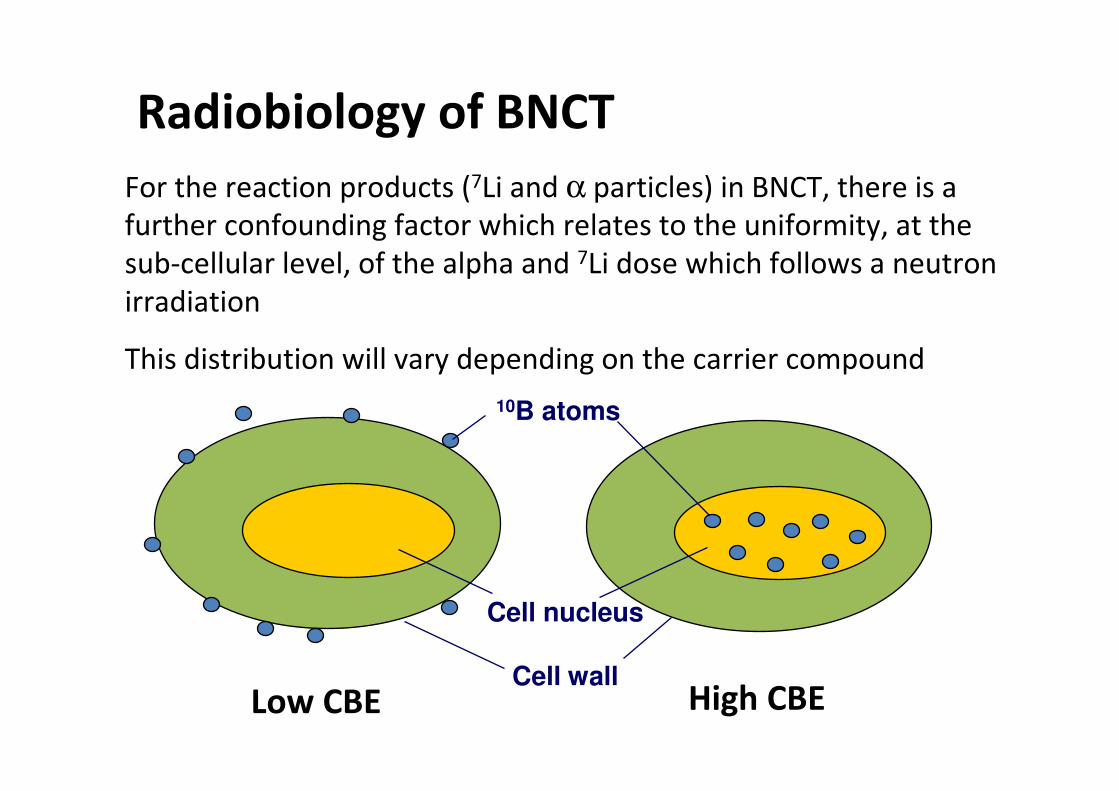
Radiobiology of BNCT
For the reaction products (7Li and α particles) in BNCT, there is a
further confounding factor which relates to the uniformity, at the
sub-cellular level, of the alpha and 7Li dose which follows a neutron
irradiation
This distribution will vary depending on the carrier compound
Low CBE High CBE
Cell nucleus
Cell wall
10B atoms



![Welcome [stfc.ukri.org] · 2015-10-01 · Induction training . Dementia Friends — The 750/0 of people of people with in the UK dementia don't think feel anxious society is or depressed](https://static.fdocuments.in/doc/165x107/5f4ab81ae335df6d300693c6/welcome-stfcukriorg-2015-10-01-induction-training-dementia-friends-a-the.jpg)













