
BILLING GUIDE - Horizon NJ Health - Medicaid Health ... NJ Health Billing Guide: ... Therefore, all...
32
This guide is intended to offer hospitals, physicians and health care professionals the information required for Horizon NJ Health to accurately and efficiently process claims prepared by or for hospitals, physicians and health care professionals for medical services provided to members of our health plan. This section contains notes of interest highlighting billing information relevant to the topic detailed above them. The notes may be titled as follows: IMPORTANT – Reminds the reader of claim submission problems that can be avoided. These errors can result in rejection, inaccurate claim payments or denials, usually because required information is missing, invalid, incomplete or inconsistent with standard billing practices. NOTE – Reviews an associated piece of information, which clarifies or explains specific details about the service, but may not directly impact reimbursement. For example, place of service is required to determine eligibility for payment, but does not necessarily affect payment amount. REFER TO – Directs the reader to another more complete source of explanation or additional resource information within this document. In the event of additional questions about Horizon NJ Health programs or policies, please review the entire Manual or contact the Physician & Health Care Hotline at 1-800-682-9091. In order to comply with contractual obligations, regulatory requirements or state and federal law, Horizon NJ Health reserves the right, at any time, to modify or update information contained in this document. Notifications will be posted at least 30 days prior to the effective date unless the effective date of a law or regulation does not permit this timeframe. Hospitals, physicians and health care professionals may access the For Providers section of the Horizon NJ Health website at www.horizonNJhealth.com to check for updates on billing requirements and other policies and procedures relevant to reimbursements for services. IMPORTANT – Horizon NJ Health, its subcontracted vendors or the State of New Jersey are responsible for payment for all services included in the member’s benefit package. Services not included in the benefit package are reimbursable by the member only if the hospital, physician or health care professional notifies the member in writing and in advance of providing the service(s) of this obligation. Members should not be billed for any service covered under their benefit package. Should Horizon NJ Health require a copayment for any service or population group, an itemization of these items will be included in the benefit listing and will be available on the website. The practice of balance billing Medicaid/NJFC beneficiaries, whether eligible for FFS benefits or enrolled in managed care, is prohibited under both federal and State law. These prohibitions apply to both Medicaid/NJFC-only beneficiaries, as well as those eligible for Medicare coverage or other insurance. A provider enrolled in the Medicaid/NJFC FFS program or in managed care is required to accept as payment in full the reimbursement rate established by the FFS program or managed care plan. All costs related to the delivery of health care benefits to a Medicaid/NJFC eligible beneficiary, other than authorized cost-sharing, are the responsibility of the FFS program, the managed care plan, Medicare (if applicable) and/or a third-party payer (if applicable). If a provider receives a Medicaid/NJFC FFS or managed care payment, the provider shall accept this payment as payment in full and shall not bill the beneficiary or anyone on the beneficiary's behalf for any additional charges. 1.0 Requirements for Filing Claims 1.1 General Requirements Horizon NJ Health will pay claims based only on eligible charges. Unless the provider contract states otherwise, claims will be paid on the lesser of billed charges or the contracted rate (Horizon NJ Health fee schedule). Horizon NJ Health is a Medicaid managed care plan that is under contract with the New Jersey Department of Human Services. Horizon NJ Health will pay claims based only on eligible charges. Claims submitted by nonparticipating Horizon NJ Health providers will be paid on the lesser of billed charges or the Horizon NJ Health nonparticipating provider fee schedule. Consistent with CFR 42 Part § 447.45: the following definition shall apply to clean claims as used within the Horizon NJ Health Billing Guide: “Clean claim means one that can be processed without obtaining additional information from the provider of the service or from a third party. It does not include a claim from a provider who is under investigation for fraud or abuse or a claim under review for medical necessity.” Horizon NJ Health Billing Guide, February 2014 1 Horizon NJ Health BILLING GUIDE
Transcript of BILLING GUIDE - Horizon NJ Health - Medicaid Health ... NJ Health Billing Guide: ... Therefore, all...

This guide is intended to offer hospitals, physicians andhealth care professionals the information required forHorizon NJ Health to accurately and efficiently processclaims prepared by or for hospitals, physicians and healthcare professionals for medical services provided tomembers of our health plan.
This section contains notes of interest highlighting billinginformation relevant to the topic detailed above them.The notes may be titled as follows:
IMPORTANT – Reminds the reader of claim submissionproblems that can be avoided. These errors can result inrejection, inaccurate claim payments or denials, usuallybecause required information is missing, invalid, incomplete orinconsistent with standard billing practices.
NOTE – Reviews an associated piece of information, whichclarifies or explains specific details about the service, but maynot directly impact reimbursement. For example, place ofservice is required to determine eligibility for payment, but doesnot necessarily affect payment amount.
REFER TO – Directs the reader to another more completesource of explanation or additional resource information withinthis document.
In the event of additional questions about Horizon NJ Health programs or policies, please review the entireManual or contact the Physician & Health Care Hotlineat 1-800-682-9091.
In order to comply with contractual obligations,regulatory requirements or state and federal law, HorizonNJ Health reserves the right, at any time, to modify orupdate information contained in this document.Notifications will be posted at least 30 days prior to theeffective date unless the effective date of a law orregulation does not permit this timeframe. Hospitals,physicians and health care professionals may access theFor Providers section of the Horizon NJ Health websiteat www.horizonNJhealth.com to check for updates onbilling requirements and other policies and proceduresrelevant to reimbursements for services.
IMPORTANT – Horizon NJ Health, its subcontracted vendorsor the State of New Jersey are responsible for payment for allservices included in the member’s benefit package. Servicesnot included in the benefit package are reimbursable by themember only if the hospital, physician or health careprofessional notifies the member in writing and in advance ofproviding the service(s) of this obligation. Members should notbe billed for any service covered under their benefit package.
Should Horizon NJ Health require a copayment for any service orpopulation group, an itemization of these items will be includedin the benefit listing and will be available on the website.The practice of balance billing Medicaid/NJFC beneficiaries,whether eligible for FFS benefits or enrolled in managed care, isprohibited under both federal and State law. These prohibitionsapply to both Medicaid/NJFC-only beneficiaries, as well asthose eligible for Medicare coverage or other insurance.A provider enrolled in the Medicaid/NJFC FFS program or inmanaged care is required to accept as payment in full thereimbursement rate established by the FFS program or managedcare plan.All costs related to the delivery of health care benefits to aMedicaid/NJFC eligible beneficiary, other than authorizedcost-sharing, are the responsibility of the FFS program, themanaged care plan, Medicare (if applicable) and/or a third-partypayer (if applicable).If a provider receives a Medicaid/NJFC FFS or managed carepayment, the provider shall accept this payment as payment in full and shall not bill the beneficiary or anyone on thebeneficiary's behalf for any additional charges.
1.0 Requirements for Filing Claims
1.1 General Requirements
Horizon NJ Health will pay claims based only on eligible charges.
Unless the provider contract states otherwise, claims willbe paid on the lesser of billed charges or the contractedrate (Horizon NJ Health fee schedule).
Horizon NJ Health is a Medicaid managed care plan thatis under contract with the New Jersey Department ofHuman Services. Horizon NJ Health will pay claimsbased only on eligible charges. Claims submitted bynonparticipating Horizon NJ Health providers will bepaid on the lesser of billed charges or the Horizon NJ Health nonparticipating provider fee schedule.
Consistent with CFR 42 Part § 447.45: the followingdefinition shall apply to clean claims as used within theHorizon NJ Health Billing Guide:
“Clean claim means one that can be processed withoutobtaining additional information from the provider of theservice or from a third party. It does not include a claimfrom a provider who is under investigation for fraud orabuse or a claim under review for medical necessity.”
Horizon NJ Health Billing Guide, February 2014 1
Horizon NJ HealthBILLING GUIDE

Under the New Jersey Health Claims Authorization,Processing and Payment Act, claims must also meet the following criteria:
(a) the health care provider is eligible at the date of service
(b) the person who received the health care service was covered on the date of service
(c) the claim is for a service or supply covered underthe health benefits plan
(d) the claim is submitted with all the informationrequested by the payor on the claim form or inother instructions that were distributed in advanceto the health care provider or covered person inaccordance with the provisions of section 4 ofP.L.2005, c.352 (C.17B:30-51)
(e) the payor has no reason to believe that the claimhas been submitted fraudulently
Other requirements, including timeliness of claimsprocessing, shall mean:
Horizon NJ Health must receive all claims within 180calendar days from the initial date when services wererendered. If claims are not received within 180 calendardays from the initial date of service, claims will bedenied for untimely filing.
Horizon NJ Health shall pay all clean claims fromhospitals, physicians and other health care professionalswithin 30 days of the date of receipt of EDI claims andwithin 40 days for paper claims.
The time limitation does not apply to claims fromproviders under investigation for fraud or abuse.
The date of receipt is the date Horizon NJ Healthreceives the claim, as indicated by its date stamp on the claim.
The date of payment is the date of the check or otherform of payment.
Practitioners and facilities may not use a P.O. Box as anacceptable billing address. A physical street address mustbe used. In addition, when submitting ZIP codesanywhere on a claim, practitioners and facilities must usethe full nine-digit format. Horizon NJ Health is requiredto report all claims to the State of New Jersey forservices provided to members through electronic media.Therefore, all billing addresses, whether submitted onpaper or electronically, must contain a physical billingaddress. To have payments sent to a different address orP.O. Box, the pay-to provider name and address field onthe 837-I and 837-P transaction must be used.
1.2 National Practitioner Identifier (NPI)
Horizon NJ Health requires all practitioners use their NPInumbers for all claim submissions. To ensure our systemsproperly identify you as an individual, group or facility,Horizon NJ Health requires you register the NPI withyour taxonomy and tax identification numbers.
Another requirement that will affect both timeliness andpayment is the use of name differential on your W-9.Horizon NJ Health continues to accept the use of yourprovider identification numbers (legacy ID).
The continued use of the legacy ID is recommended, as the claims processing system uses this number foradjudication and payment activities. Please make sureyour name matches the name used on your W-9.
Below are some helpful hints, which will facilitateaccurate and consistent management of your claims.
• Physicians, facilities, and health care professionals arerequired to have an NPI. Please register for one if youhave not already secured your NPI.
• Groups are not technically required to have an NPI,but are encouraged to have one as long as there is alegal entity associated with the business name and taxidentification number. To register the group NPI withHorizon NJ Health, we will need the W-9 for thebusiness and all associated individual NPIs paid to thattax ID number.
• Facilities, including hospitals and groups chosen tosubpart their type 2 NPI, will need to choose a masterNPI if all of the registered numbers are under the sametax identification number. Designating a master NPInumber will help Horizon NJ Health assign claims tothe right location for payment purposes. A valid W-9for the business and all associated individual NPIs thatare paid to that tax ID number should be registeredwith Horizon NJ Health.
• Where an NPI number is shared among differentlocations using the same tax ID number, the HorizonNJ Health legacy ID is needed to distinguish wherethe claim payment should be sent.
• Nonparticipating practitioners and facilities are alsorequired to adhere to the NPI requirements. Tofacilitate payment for claims, Horizon NJ Healthencourages you to register your NPI with us in thesame manner described above. To complete this task,please visit the “For Providers” section ofwww.horizonNJhealth.com and download our NPICollection Form. Once completed, fax your forms and CMS documentation to Horizon NJ Health at 1-609-583-3004.
2 Horizon NJ Health Billing Guide, February 2014
BILLING GUIDE

1.3 Procedures for Claim Submission
Horizon NJ Health is required by state and federalregulations to capture and report specific data regardingservices rendered to its members. All services rendered,including capitated encounters and Fee-for-Serviceclaims, must be submitted on the CMS 1500 (HCFA1500) or UB-04 claims form, or via electronic submissionin a HIPAA-compliant 837 or NCPDP format. Theseclaims forms and electronic submissions must beconsistent with the instructions provided by the CMSrequirements, as stated in the Claims Manual, which canbe accessed at www.cms.gov/Manuals/IOM/list.asp.
The hospital, physician and health care professional, to appropriately account for services rendered and toensure timely processing of claims, must adhere to all billing requirements.
When data elements are missing, incomplete, invalid or coded incorrectly, Horizon NJ Health cannot processthe claims.
• Claims for billable services provided to Horizon NJ Health members must be submitted by the hospital,physician or health care professional that performedthe services.
• Professional services are not reimbursable to a hospitalunless the hospital is specifically contracted forprofessional services. Horizon NJ Health policy is to reimburse these services only when billed on a CMS 1500.
• Claims filed with Horizon NJ Health are subject to thefollowing procedures:
– Verification that all required fields are completedon the claim
– Verification that all diagnosis codes, modifiers andprocedure codes are valid for the date of service
– When appropriate, verification of the referral forspecialist or non-primary care physician claims(excluding “self-referral” types of care)
– Verification of member’s eligibility for servicesunder Horizon NJ Health during the time period in which services were provided
– Verification that the services were provided by a participating or nonparticipating hospital, physician or health care professional that hasreceived authorization to provide services to theeligible member
– Verification that the hospital, physician or healthcare professional has been given approval forservices that require prior authorization by HorizonNJ Health
• Horizon NJ Health is the “payor of last resort” on allclaims submitted for members of its health plan.Hospitals, physicians and health care professionalsmust verify whether the member has Medicarecoverage or any other third party resources and, if so,provide documentation that the claim was firstprocessed by this other insurer as appropriate
IMPORTANT – Rejected claims are defined as claims withinvalid or missing data elements, such as the tax ID number, thatare returned to the submitter or EDI source without registration inthe claim processing system. Since rejected claims are notregistered in the claim processing system, the hospital, physicianor health care professional must re-submit corrected claimswithin 180 calendar days from the date of service. This guidelineapplies to claims submitted on paper or electronically. Rejectedclaims are different than denied claims, which are registered inthe claim processing system, but do not meet requirements forpayment under Horizon NJ Health guidelines.
Submit claims for all medical services to Horizon NJ Health at the following address:
Horizon NJ HealthClaim Processing Department
P.O. Box 7117London, KY 40742
NOTE – Out-of-state, non-Horizon NJ Health providers should sendclaims to their local Blue Cross Blue Shield Plan.
IMPORTANT – Requests for adjustments may be submitted by telephone to:
Physician Claim Services1-800-682-9091
NOTE – Be sure to include the member’s Social SecurityNumber and Horizon NJ Health or Medicaid ID number on allfamily planning claims.
IMPORTANT – Requests for reimbursement for retailpharmacy and all outpatient drugs for persons designated asaged, blind or disabled should be submitted directly to the Stateof New Jersey.
IMPORTANT – Requests for reimbursement for mental healthservices for all enrollees, except the developmentally disabled,should be submitted directly to the State of New Jersey.
NOTE – Be sure to include the member’s Medicaid ID number on all claims submitted to the State of New Jersey.
NOTE – Horizon NJ Health subcontracts with Davis Vision toprovide and/or coordinate vision services for eligible members.All services, except ophthalmologic procedures, are coordinatedand paid by Davis Vision. Please call 1-877-226-3729 forinformation about submitting invoices.
Horizon NJ Health Billing Guide, February 2014 3
BILLING GUIDE
NOTE – Horizon NJ Health subcontracts with Scion Dental toprovide and/or coordinate dental services for eligible members.Please call the Provider Call Center at 1-855-878-5368 for routineprovider questions related to eligibility, claims, authorizations,credentialing, contracting, adding/changing providerdata/locations, and fee schedules.
NOTE – Horizon NJ Health subcontracts with LaboratoryCorporation of America, Inc. (LabCorp) for most routine andspecialized laboratory services. Generally, Horizon NJ Health isresponsible for payment of claims for PAT/STAT laboratoryservice provided in hospitals and ambulatory surgical centers.Horizon NJ Health will also provide reimbursements for claimsfor laboratory services included on LabCorp’s excluded testlisting. An authorization is required for any test included on thislisting; please submit claims to Horizon NJ Health as specifiedabove. Unless otherwise specified within specific contractualarrangements, laboratory services should be referred to LabCorp.
Horizon NJ Health encourages all hospitals, physiciansand health care professionals to submit claimselectronically. For those interested in electronic claim filing, call the EDI Technical Support Hotline at 1-877-234-4273 or send an e-mail [email protected] to obtain moreinformation.
Benefits to sending claims electronically include:• Cleaner claim submission• Confirmation of submitted claims within 24 hours• Faster processing and payment• Administrative efficiencies• No postage or handling of paper claims
NOTE – EDI Technical Support Team is available during regularbusiness hours, 8 a.m. through 5 p.m., Monday through Friday.
For more information on EDI, review Section 9.3Procedures for Electronic Submission- ElectronicData Interchange.
1.4 Claim Filing Deadlines
Horizon NJ Health must receive all claims within 180calendar days from the initial date when services wererendered. If claims are not received within 180 calendardays from the initial date of service, claims will bedenied for untimely filing.
• Horizon NJ Health’s Appeals department utilizesspecific criteria when reviewing valid proof of timelyfiling. The information submitted should consist of acomputer-generated ledger that cannot be altered andincludes the following information:• Member’s name• Horizon NJ Health or Medicaid ID number• Billed amount• Date of service• Billed/mailed date• Address where the claim form was sent (HorizonNJ Health or insurance code)
• For EDI submissions, a 999 report indicatingsubmission to the correct insurance code is requiredfor consideration of timely submission.
REFER TO – Section 10.0 Complaint and Appeals Process forcomplete instructions of the submission timeframes andprocedures for administrative or medical appeals.
NOTE – If the physician/facility’s ledger uses internal insurancecodes, they must submit a copy of the code descriptions.
NOTE – Horizon NJ Health’s Appeals area will also acceptcertified mail receipts as valid proof of timely filing.
NOTE – If a physician/facility receives a claim rejection formfrom the Claims department, a copy of the form will also serveas valid proof of timely filing.
Corrected claims* must be submitted within 365calendar days from the initial date of service to thefollowing address:
Horizon NJ HealthClaim Processing Department
P.O. Box 7117London, KY 40742
*When submitting corrected claims, please add“CORRECTED CLAIM” to the form.
ExceptionsClaims with an explanation of benefits (EOB) fromprimary insurers that fall beyond the timely filingrequirements must be submitted within 60 days from the date of the primary insurer’s EOB.
4 Horizon NJ Health Billing Guide, February 2014
BILLING GUIDE

2.0 Claim Forms (Paper)
Horizon NJ Health requires that all hospitals, physiciansand health care professionals use the standard CMS 1500(HCFA 1500) or UB-04 claim forms to report services,which are reimbursable or capitated. The CMS 1500(HCFA 1500) claim form must be completed for allprofessional medical services. The UB-04 claim formmust be completed for all facility claims.
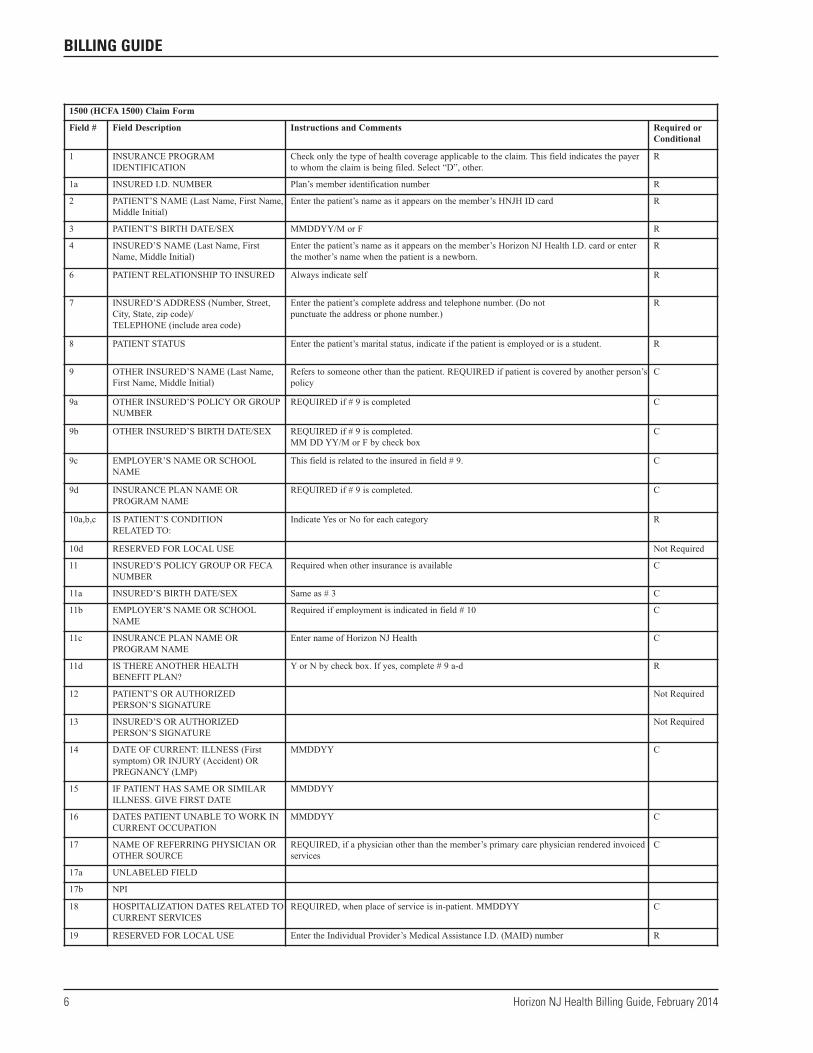
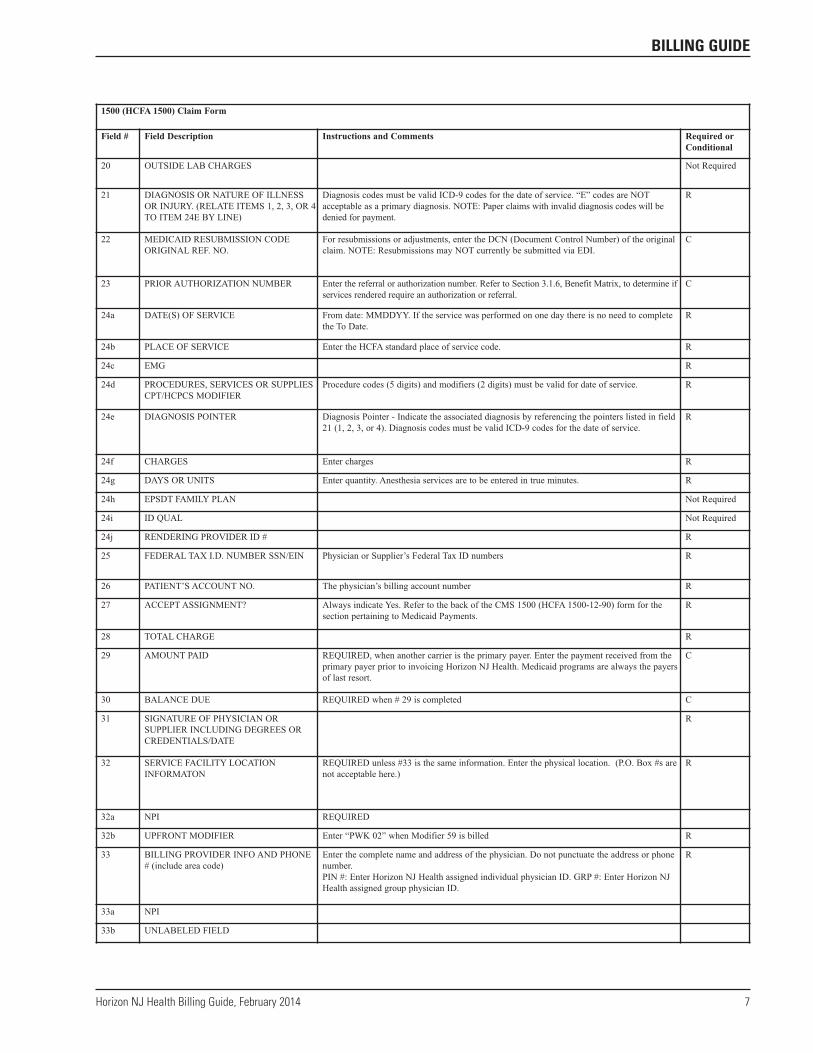
2.1 CMS 1500 (HCFA 1500) Claim Form(Paper Submissions)
The CMS 1500 (HCFA 1500) claim form must be used to bill all professional services to Horizon NJ Health. This section will provide the list of required fields forHorizon NJ Health; however, you must refer to the mostcurrent CMS coding instructions for a complete list ofcodes and requirements.
Place of Service CodesCode Description
11 Office12 Home21 Inpatient Hospital22 Outpatient Hospital23 Emergency Room – Hospital24 Ambulatory Surgical Center25 Birthing Center26 Military Treatment Facility31 Skilled Nursing Facility32 Nursing Facility33 Custodial Care Facility34 Hospice41 Ambulance – Land42 Ambulance – Air or Water50 Federally Qualified Health Center51 Inpatient Psychiatric Facility52 Psychiatric Residential Treatment Center
Code Description
53 Community Mental Health Center54 Intermediate Care Facility/Mentally Retarded55 Residential Substance Abuse Treatment Center56 Psychiatric Residential Treatment Center60 Mass Immunization Center61 Comprehensive Inpatient Rehabilitation Facility62 Comprehensive Outpatient Rehabilitation Facility65 End Stage Renal Disease Treatment Facility71 State or Local Public Health Clinic72 Rural Health Clinic81 Independent Laboratory99 Other Unlisted Facility
Type of Service CodesCode Description
1 Medical Services2 Surgery3 Consultations4 Radiology (total component)5 Laboratory (total component)6 Radiation Therapy (total component)7 Anesthesia8 Assistant Surgery9 Other (e.g., prosthetic eyewear, contacts,
ambulance)D DMEF ASC
Required and Conditional Field Indicator IMPORTANT – An authorization number and/or referralnumber must be included in box #23 on a CMS 1500 (HCFA1500) claim form or box #63 on a UB-04 form.
The required fields that must be completed for the standardCMS 1500 (HCFA 1500) or UB-04 claim forms are in therespective claim form areas. If the field is required withoutexception, an “R” (required) is noted in the “Required orConditional” box. If completing the field is dependentupon certain circumstances, the requirement is listed as“C” (conditional) and the relevant conditions are explainedin the “Instructions and Comments” box.
Horizon NJ Health Billing Guide, February 2014 5
BILLING GUIDE
6 Horizon NJ Health Billing Guide, February 2014
BILLING GUIDE
1500 (HCFA 1500) Claim Form
Field # Field Description Instructions and Comments Required orConditional
1 INSURANCE PROGRAM IDENTIFICATION
Check only the type of health coverage applicable to the claim. This field indicates the payerto whom the claim is being filed. Select “D”, other.
R
1a INSURED I.D. NUMBER Plan’s member identification number R
2 PATIENT’S NAME (Last Name, First Name,Middle Initial)
Enter the patient’s name as it appears on the member’s HNJH ID card R
3 PATIENT’S BIRTH DATE/SEX MMDDYY/M or F R
4 INSURED’S NAME (Last Name, FirstName, Middle Initial)
Enter the patient’s name as it appears on the member’s Horizon NJ Health I.D. card or enterthe mother’s name when the patient is a newborn.
R
6 PATIENT RELATIONSHIP TO INSURED Always indicate self R
7 INSURED’S ADDRESS (Number, Street,City, State, zip code)/ TELEPHONE (include area code)
Enter the patient’s complete address and telephone number. (Do not punctuate the address or phone number.)
R
8 PATIENT STATUS Enter the patient’s marital status, indicate if the patient is employed or is a student. R
9 OTHER INSURED’S NAME (Last Name,First Name, Middle Initial)
Refers to someone other than the patient. REQUIRED if patient is covered by another person’spolicy
C
9a OTHER INSURED’S POLICY OR GROUPNUMBER
REQUIRED if # 9 is completed C
9b OTHER INSURED’S BIRTH DATE/SEX REQUIRED if # 9 is completed. MM DD YY/M or F by check box
C
9c EMPLOYER’S NAME OR SCHOOLNAME
This field is related to the insured in field # 9. C
9d INSURANCE PLAN NAME OR PROGRAM NAME
REQUIRED if # 9 is completed. C
10a,b,c IS PATIENT’S CONDITION RELATED TO:
Indicate Yes or No for each category R
10d RESERVED FOR LOCAL USE Not Required
11 INSURED’S POLICY GROUP OR FECANUMBER
Required when other insurance is available C
11a INSURED’S BIRTH DATE/SEX Same as # 3 C
11b EMPLOYER’S NAME OR SCHOOLNAME
Required if employment is indicated in field # 10 C
11c INSURANCE PLAN NAME OR PROGRAM NAME
Enter name of Horizon NJ Health C
11d IS THERE ANOTHER HEALTH BENEFIT PLAN?
Y or N by check box. If yes, complete # 9 a-d R
12 PATIENT’S OR AUTHORIZED PERSON’S SIGNATURE
Not Required
13 INSURED’S OR AUTHORIZED PERSON’S SIGNATURE
Not Required
14 DATE OF CURRENT: ILLNESS (Firstsymptom) OR INJURY (Accident) ORPREGNANCY (LMP)
MMDDYY C
15 IF PATIENT HAS SAME OR SIMILARILLNESS. GIVE FIRST DATE
MMDDYY
16 DATES PATIENT UNABLE TO WORK INCURRENT OCCUPATION
MMDDYY C
17 NAME OF REFERRING PHYSICIAN OROTHER SOURCE
REQUIRED, if a physician other than the member’s primary care physician rendered invoicedservices
C
17a UNLABELED FIELD
17b NPI
18 HOSPITALIZATION DATES RELATED TOCURRENT SERVICES
REQUIRED, when place of service is in-patient. MMDDYY C
19 RESERVED FOR LOCAL USE Enter the Individual Provider’s Medical Assistance I.D. (MAID) number R
Horizon NJ Health Billing Guide, February 2014 7
BILLING GUIDE
1500 (HCFA 1500) Claim Form
Field # Field Description Instructions and Comments Required orConditional
20 OUTSIDE LAB CHARGES Not Required
21 DIAGNOSIS OR NATURE OF ILLNESSOR INJURY. (RELATE ITEMS 1, 2, 3, OR 4TO ITEM 24E BY LINE)
Diagnosis codes must be valid ICD-9 codes for the date of service. “E” codes are NOTacceptable as a primary diagnosis. NOTE: Paper claims with invalid diagnosis codes will bedenied for payment.
R
22 MEDICAID RESUBMISSION CODEORIGINAL REF. NO.
For resubmissions or adjustments, enter the DCN (Document Control Number) of the originalclaim. NOTE: Resubmissions may NOT currently be submitted via EDI.
C
23 PRIOR AUTHORIZATION NUMBER Enter the referral or authorization number. Refer to Section 3.1.6, Benefit Matrix, to determine ifservices rendered require an authorization or referral.
C
24a DATE(S) OF SERVICE From date: MMDDYY. If the service was performed on one day there is no need to completethe To Date.
R
24b PLACE OF SERVICE Enter the HCFA standard place of service code. R
24c EMG R
24d PROCEDURES, SERVICES OR SUPPLIESCPT/HCPCS MODIFIER
Procedure codes (5 digits) and modifiers (2 digits) must be valid for date of service. R
24e DIAGNOSIS POINTER Diagnosis Pointer - Indicate the associated diagnosis by referencing the pointers listed in field21 (1, 2, 3, or 4). Diagnosis codes must be valid ICD-9 codes for the date of service.
R
24f CHARGES Enter charges R
24g DAYS OR UNITS Enter quantity. Anesthesia services are to be entered in true minutes. R
24h EPSDT FAMILY PLAN Not Required
24i ID QUAL Not Required
24j RENDERING PROVIDER ID # R
25 FEDERAL TAX I.D. NUMBER SSN/EIN Physician or Supplier’s Federal Tax ID numbers R
26 PATIENT’S ACCOUNT NO. The physician’s billing account number R
27 ACCEPT ASSIGNMENT? Always indicate Yes. Refer to the back of the CMS 1500 (HCFA 1500-12-90) form for thesection pertaining to Medicaid Payments.
R
28 TOTAL CHARGE R
29 AMOUNT PAID REQUIRED, when another carrier is the primary payer. Enter the payment received from theprimary payer prior to invoicing Horizon NJ Health. Medicaid programs are always the payersof last resort.
C
30 BALANCE DUE REQUIRED when # 29 is completed C
31 SIGNATURE OF PHYSICIAN ORSUPPLIER INCLUDING DEGREES ORCREDENTIALS/DATE
R
32 SERVICE FACILITY LOCATIONINFORMATON
REQUIRED unless #33 is the same information. Enter the physical location. (P.O. Box #s arenot acceptable here.)
R
32a NPI REQUIRED
32b UPFRONT MODIFIER Enter “PWK 02” when Modifier 59 is billed R
33 BILLING PROVIDER INFO AND PHONE# (include area code)
Enter the complete name and address of the physician. Do not punctuate the address or phonenumber. PIN #: Enter Horizon NJ Health assigned individual physician ID. GRP #: Enter Horizon NJHealth assigned group physician ID.
R
33a NPI
33b UNLABELED FIELD

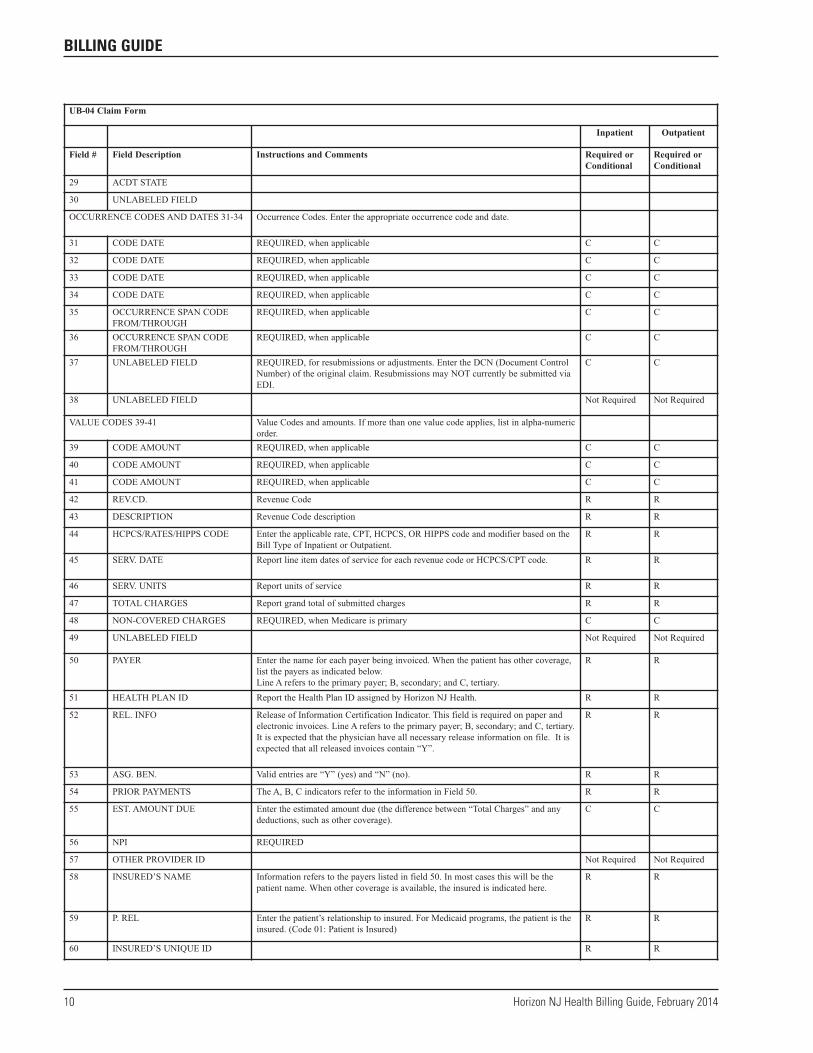
2.2 The UB-04 (CMS 1450) Claim Form (Paper)
The UB-04 (CMS 1450) claim form must be used to billall facility services to Horizon NJ Health. This sectionwill provide the list of required fields for Horizon NJ Health. However, you must refer to the most currentCMS coding instructions for a complete list of codes and requirements.
Type of Bill CodesCode Description
111 Hospital/Inpatient (Part A)/Admit throughDischarge
Code Description112 Hospital/Inpatient (Part A)/Interim – First Claim113 Hospital/Inpatient (Part A)/Interim – Continuing
Claims114 Hospital/Inpatient (Part A)/Interim – Last Claim115 Hospital/Inpatient (Part A)/Late Charge Only117 Hospital/Inpatient (Part A)/Replacement of Prior
Claim121 Hospital/Hospital Based or Inpatient
(Part B)/Admit Through Discharge
Code Description
131 Hospital/Outpatient/Admit Through Discharge211 Skilled Nursing/Inpatient (Part A)/Admit
Through Discharge212 Skilled Nursing/Inpatient (Part A)/Interim –
First Claim213 Skilled Nursing/Inpatient (Part A)/Interim –
Continuing Claims214 Skilled Nursing/Inpatient (Part A)/Interim –
Last Claim321 Home Health/Hospital Based or Inpatient
(Part B)/Admit Through Discharge331 Home Health/Hospital Based or Inpatient
(Part B)/Admit Through Discharge711 Clinic/Rural Health Clinic (RHC)/Admit
Through Discharge721 Clinic/Independent Renal Dialysis
Facility/Admit through Discharge731 Clinic/FQHC/Admit Through Discharge831 Special Facility or Hospital ASC/ASC for
Outpatients/Admit Through Discharge
Type of Admission CodesCode Description
1 Emergency2 Urgent3 Elective
Patient Status CodesCode Description
01 Discharged to Home or Self Care (routinedischarge)
02 Discharged/Transferred to Another Short-TermGeneral Hospital
03 Discharged/Transferred to SNF04 Discharged/Transferred to ICF05 Discharged/Transferred to Another Type of
Institution (including distinct parts) or Referredfor Outpatient Services to Another Institution
06 Discharged/Transferred to Home Under Care of Organized Home Health Service Organization
07 Left Against Medical Advice08 Discharged/Transferred to Home Under Care
of an IV Drug Therapy Provider09 Admitted as an Inpatient to this Hospital20 Expired (or did not recover – Christian Science
Patient)30 Still Patient or Expected to Return for
Outpatient Services40 Expired at Home (hospice claims only)41 Expired in a Medical Facility, such as Hospital,
SNF, ICF or Freestanding Hospice (hospiceclaims only)
42 Expired – Place Unknown (hospice claims only)50 Hospice – Home51 Hospice – Medical Facility
Commonly Used Revenue CodesCode Description
100 – 129 Room and Board Charges130 – 249 Semi-private; Private; Ward, Nursery,
Subacute, ICU, CCU250 – 259 Pharmacy260 – 269 IV Therapy270 – 279 Medical/Surgical Supplies & Devices280 – 289 Oncology
8 Horizon NJ Health Billing Guide, February 2014
BILLING GUIDE

Horizon NJ Health Billing Guide, February 2014 9
BILLING GUIDE
UB-04 Claim Form
Inpatient Outpatient
Field # Field Description Instructions and Comments Required orConditional
Required orConditional
1 UNLABELED FIELD Line a: Enter the complete physician name. Line b: Enter the complete address orpost office number. Line c: City, state, and ZIP code Line d: Enter the area code,telephone number.
R R
2 UNLABELED FIELD Enter the Facility Medical Assistance ID (MAID) number. R R
3a PATIENT CONTROL NO. Physician’s patient account/control number R R
3b MED REC NO.
4 TYPE OF BILL Enter the appropriate three-digit code. 1st position indicates type of facility. 2ndposition indicates type of care. 3rd position indicates billing sequence.
R R
5 FED. TAX NO. Enter the number assigned by the federal government for tax reporting purposes. R R
6 STATEMENT COVERS PERIODFROM/THROUGH
Enter dates for the full ranges of services being invoiced. MMDDYY R R
7 UNLABELED FIELD
8a PATIENT NAME Last name, first name, and middle initial. Enter the patient name as it appears onHorizon NJ Health ID card. Use a comma or space to separate the last and firstnames. Titles (Mr., Mrs., etc.) should not be reported in this field. Prefix: No spaceshould be left after the prefix of a name, e.g. McKendrick. Hyphenated names: Bothnames should be capitalized and separated by a hyphen (no space). Suffix: A spaceshould separate a last name and suffix.
R R
8b UNLABELED FIELD
9a PATIENT ADDRESS Enter the complete mailing address of the patient. R R
9b UNLABELED FIELD
9c UNLABELED FIELD
9d UNLABELED FIELD
9e UNLABELED FIELD
10 BIRTHDATE MMDDYY R R
11 SEX Enter the patient’s sex, as recorded at the time of registration. Only M, F, and U areacceptable.
R R
ADMISSION INFOR 12-17
12 DATE MMDDYY R R
13 HR Admission Hour R R
14 TYPE Admission Type R Not Required
15 SRC Source of Admission R Not Required
16 DHR Discharge Hour R R
17 STAT Patient Status ( disposition ) R Not Required
CONDITION CODES 18-28
18 CONDITION CODE REQUIRED, when applicable C C
19 CONDITION CODE REQUIRED, when applicable C C
20 CONDITION CODE REQUIRED, when applicable C C
21 CONDITION CODE REQUIRED, when applicable C C
22 CONDITION CODE REQUIRED, when applicable C C
23 CONDITION CODE REQUIRED, when applicable C C
24 CONDITION CODE REQUIRED, when applicable C C
25 CONDITION CODE REQUIRED, when applicable C C
26 CONDITION CODE REQUIRED, when applicable C C
27 CONDITION CODE REQUIRED, when applicable C C
28 CONDITION CODE REQUIRED, when applicable C C
10 Horizon NJ Health Billing Guide, February 2014
BILLING GUIDE
UB-04 Claim Form
Inpatient Outpatient
Field # Field Description Instructions and Comments Required orConditional
Required orConditional
29 ACDT STATE
30 UNLABELED FIELD
OCCURRENCE CODES AND DATES 31-34 Occurrence Codes. Enter the appropriate occurrence code and date.
31 CODE DATE REQUIRED, when applicable C C
32 CODE DATE REQUIRED, when applicable C C
33 CODE DATE REQUIRED, when applicable C C
34 CODE DATE REQUIRED, when applicable C C
35 OCCURRENCE SPAN CODEFROM/THROUGH
REQUIRED, when applicable C C
36 OCCURRENCE SPAN CODEFROM/THROUGH
REQUIRED, when applicable C C
37 UNLABELED FIELD REQUIRED, for resubmissions or adjustments. Enter the DCN (Document ControlNumber) of the original claim. Resubmissions may NOT currently be submitted viaEDI.
C C
38 UNLABELED FIELD Not Required Not Required
VALUE CODES 39-41 Value Codes and amounts. If more than one value code applies, list in alpha-numericorder.
39 CODE AMOUNT REQUIRED, when applicable C C
40 CODE AMOUNT REQUIRED, when applicable C C
41 CODE AMOUNT REQUIRED, when applicable C C
42 REV.CD. Revenue Code R R
43 DESCRIPTION Revenue Code description R R
44 HCPCS/RATES/HIPPS CODE Enter the applicable rate, CPT, HCPCS, OR HIPPS code and modifier based on theBill Type of Inpatient or Outpatient.
R R
45 SERV. DATE Report line item dates of service for each revenue code or HCPCS/CPT code. R R
46 SERV. UNITS Report units of service R R
47 TOTAL CHARGES Report grand total of submitted charges R R
48 NON-COVERED CHARGES REQUIRED, when Medicare is primary C C
49 UNLABELED FIELD Not Required Not Required
50 PAYER Enter the name for each payer being invoiced. When the patient has other coverage,list the payers as indicated below.Line A refers to the primary payer; B, secondary; and C, tertiary.
R R
51 HEALTH PLAN ID Report the Health Plan ID assigned by Horizon NJ Health. R R
52 REL. INFO Release of Information Certification Indicator. This field is required on paper andelectronic invoices. Line A refers to the primary payer; B, secondary; and C, tertiary.It is expected that the physician have all necessary release information on file. It isexpected that all released invoices contain “Y”.
R R
53 ASG. BEN. Valid entries are “Y” (yes) and “N” (no). R R
54 PRIOR PAYMENTS The A, B, C indicators refer to the information in Field 50. R R
55 EST. AMOUNT DUE Enter the estimated amount due (the difference between “Total Charges” and anydeductions, such as other coverage).
C C
56 NPI REQUIRED
57 OTHER PROVIDER ID Not Required Not Required
58 INSURED’S NAME Information refers to the payers listed in field 50. In most cases this will be thepatient name. When other coverage is available, the insured is indicated here.
R R
59 P. REL Enter the patient’s relationship to insured. For Medicaid programs, the patient is theinsured. (Code 01: Patient is Insured)
R R
60 INSURED’S UNIQUE ID R R

Code Description
290 – 299 Durable Medical Equipment (DME)300 – 319 Laboratory/Laboratory Pathological320 – 339 Radiology Diagnostic/Therapeutic340 – 349 Nuclear Medicine350 – 359 CT Scan360 – 369 Operating Room Services370 – 379 Anesthesia410 – 449 Therapy Services
Code Description
450 – 459 Emergency Codes 540 – 548 Ambulance Services720 – 729 Labor and Delivery730 – 750 Outpatient Surgery800 – 880 Radiology900 – 919 Psychiatric/Psychological920 – 999 Nuclear Medicine
Horizon NJ Health Billing Guide, February 2014 11
BILLING GUIDE
UB-04 Claim Form
Inpatient Outpatient
Field # Field Description Instructions and Comments Required orConditional
Required orConditional
61 GROUP NAME Use this field only when a patient has other insurance and group coverage applies. Donot use this field for individual coverage. Line A refers to the primary payer; B,secondary; and C, tertiary.
C C
62 INSURANCE GROUP NO. Use this field only when a patient has other insurance and group coverage applies. Donot use this field for individual coverage. Line A refers to the primary payer; B,secondary; and C, tertiary.
C C
63 TREATMENT AUTHORIZATIONCODES
Enter Horizon NJ Health referral or authorization number. Line A refers to theprimary payer; B, secondary; and C, tertiary.
R R
64 DOCUMENT CONTROLNUMBER
R R
65 EMPLOYER NAME REQUIRED if field 64 contains 1, 2, or 4. Line A refers to the primary payer; B,secondary; and C, tertiary.
C C
66 DX C C
67 A-Q Enter the complete ICD-9-CM diagnosis code. Include the 4th and 5th digits ifapplicable. Each diagnosis code must be valid for the date of service.
R R
OTHER DIAG. CODES 68-75
68 UNLABELED FIELD R R
69 ADMIT DX R R
70 PATIENT REASON DX (a-c) R R
71 PPS CODE Enter the complete ICD-9-CM diagnosis code. Include the 4th and 5th digits ifapplicable. Each diagnosis code must be valid for the date of service.
R R
72 ECI R R
73 UNLABELED FIELD
74 PRINCIPAL PROCEDURE CODEDATE
Enter the procedure code for the principal procedure performed during the periodcovered by the invoice. Inpatient claims and all surgical procedures requireICD-9-CM codes. Outpatient claims require CPT/HCPCS codes.
R R
74 a-e OTHER PROCEDURE CODEDATE
Enter the procedure code for the other procedure performed during the period coveredby the invoice. Inpatient claims and all surgical procedures require ICD-9-CM codes.Outpatient claims require CPT/HCPCS codes.
R R
75 UNLABELED FIELD
76 ATTENDING PHYS. ID Enter the name of the physician who has primary responsibility for the patient’smedical care or treatment, in the lower line and the medical license # or UPIN # inthe upper line.
R R
77 OPERATING REQUIRED for reporting external cause of injury. Enter the complete ICD-9-CMdiagnosis code. Include the 4th and 5th digits if applicable
C C
78 OTHER Not Required Not Required
79 UPFRONT MODIFIER Enter “PWK 02” when Modifier 59 is billed R R
80 REMARKS C C
81 a-d CC

Required and Conditional Field IndicatorRequired (R) fields must be completed on all claims.Conditional (C) fields must be completed if theinformation applies to the services rendered to Horizon NJ Health members.
IMPORTANT –When a referral form is required by Horizon NJHealth, please attach the original to the CMS 1500 (HCFA 1500)or the UB-04 claim form submitted for payment.
3.0 Procedures for Electronic Submission –Electronic Data Interchange
IMPORTANT – All claims submitted electronically must be in a HIPAA compliant 837 or NCPDP format.
Electronic data interchange (EDI) allows faster, moreefficient and cost-effective claim submission forhospitals, physicians and health care professionals. EDI,performed in accordance with nationally recognizedstandards, supports the industry’s efforts to reduceoverhead administrative costs.
The benefits of billing electronically include:
• Reduction of overhead and administrative costs. EDIeliminates the need for paper claim submission. It hasalso been proven to reduce claim rework (adjustments).
• Receipt of reports as proof of claim receipt. This makes it easier to track the status of claims.
• Faster transaction time for claims submittedelectronically. An EDI claim averages about 24 to 48hours from the time it is sent to the time it is received.This enables providers to easily track their claims.
• Validation of data elements on the claim. By the timea claim is successfully received electronically,information needed for processing is present. Thisreduces the chance of data entry errors that occurwhen completing paper claim forms.
• Quicker claim completion. Claims that do not needadditional investigation are generally processedquicker. Reports have shown that a large percentage of EDI claims are processed within 10 to 15 days of their receipt.
IMPORTANT – Referrals are valid for up to 180 days from thedate indicated in box 3 (Date of Service) of the Horizon NJHealth referral form. The referral number on the claim does notgenerate a payment. The actual referral must be submitted witheach claim to avoid claim processing delays or denials.
NOTE – Hospitals, physicians and health care professionalssubmitting claims electronically should make sure the referralnumber is present on the claim. Referral forms must besubmitted separately, by mail to:
Horizon NJ HealthClaim Processing Department
P. O. Box 7117London, KY 40742
NOTE – EDI Technical Support Team is available during regularbusiness hours, 8 a.m. through 5 p.m., Monday through Friday.
IMPORTANT – Requests for adjustments may be submitted by telephone to:
Physician & Health Care Hotline1-800-682-9091
3.1 Hardware/Software Requirements
There are many different products that can be used tobill electronically. Hospitals, physicians and health careprofessionals should send EDI claims to Emdeon,whether through direct submission or through anotherclearinghouse/vendor using payor number 22326. Only Emdeon can submit claims electronically toHorizon NJ Health.
Emdeon is the largest clearinghouse for EDI health caretransactions in the world. It has the capability to acceptelectronic data from numerous physicians in severalstandardized EDI formats and forwards acceptedinformation to carriers in an agreed-upon format.
Contracting with Emdeon and Other Electronic VendorsIf you are a hospital, physician or health careprofessional interested in submitting claimselectronically to Horizon NJ Health but do not haveEmdeon EDI services, contact Emdeon’s Salesdepartment at 1-800-845-6592. You may also choose to contract with another EDI clearinghouse or vendorwho already has access to Emdeon EDI services.
Contacting the EDI Technical Support GroupHospitals, physicians and health care professionalsinterested in sending claims to Horizon NJ Healthelectronically may contact the EDI Technical SupportGroup for information and assistance.
Once Horizon NJ Health is notified of the intent tosubmit claims through EDI, the organization’s contactwill receive a complete list of ID numbers for HorizonNJ Health hospitals, physicians and health careprofessionals, the electronic payor number,Emdeon-specific edits, and any other information neededto initiate electronic billing with Horizon NJ Health.
NOTE – Physicians can contact the EDI Technical Support Groupto obtain names of other EDI clearinghouses and vendors.
12 Horizon NJ Health Billing Guide, February 2014
BILLING GUIDE

Transmission RequirementsOnce the material is received, proceed as follows:
• Read over the materials carefully• Transmission can begin upon receipt of ID numbersfor Horizon NJ Health individual hospitals, physiciansand health care professionals.
Contact the EDI Technical Support Group to answer anyquestions you may have. If you wish to receiveconfirmation to begin electronic submission, the EDITechnical Support Group will contact you via fax, mail oremail on the effective day for EDI claim submission. No approval is necessary.
Contact your system vendor and/or Emdeon to informthem that you are now going to submit production claimselectronically to Horizon NJ Health. You will be askedfor the electronic payor address and the Emdeon specificedits included in your Horizon NJ Health documentation.
NOTE – Contact EDI Technical Support at 1-877-234-4273 tonotify them of your intention to begin EDI transmissions.
3.2 Specific Data Record Requirements
EDI claims should be submitted according to HIPAAstandards. These standards can be found in theImplementation Guides written by the DesignatedStandard Maintenance Organizations (DSMOs)responsible for each transaction. Additional informationcan be obtained through the Center for Medicare andMedicaid Services website at www.cms.hhs.gov.
3.3 Electronic Claim Flow Description
In order to send claims electronically to Horizon NJ Health, all EDI claims must first be forwarded toEmdeon using payor number 22326. This can becompleted via a direct submission or through anotherEDI clearinghouse or vendor.
Once Emdeon receives the transmitted claims, they arevalidated against Emdeon’s proprietary specifications andHorizon NJ Health specific requirements. Claims notmeeting the requirements are immediately rejected andsent back to the sender via an Emdeon error report. Thename of this report can vary, based on the physician’scontract with their intermediate EDI vendor or Emdeon.
Claims are then passed to Horizon NJ Health, andEmdeon returns a conditional acceptance report to thesender immediately.
Claims forwarded to Horizon NJ Health by Emdeon areimmediately validated against physician and membereligibility records. Claims that do not meet thisrequirement are rejected and sent back to Emdeon, which also forwards this rejection to its trading partner –the intermediate EDI vendor or directly to the hospital,physician or health care professional. Claims passingeligibility requirements are then passed to the claimprocessing queues. Claims are not considered receivedunder timely filing guidelines if rejected for missing orinvalid provider or member data.
Hospitals, physicians and health care professionals areresponsible for verification of EDI claims receipts.Acknowledgements for accepted or rejected claimsreceived from Emdeon or other contracted vendors mustbe reviewed and validated against transmittal records daily.
NOTE – For a detailed list of Emdeon data requirements,contact EDI Technical Support at 1-877-234-4273 or [email protected].
3.4 Invalid Electronic Claim Record
Rejections/DenialsAll claim records sent to Horizon NJ Health must firstpass Emdeon’s proprietary edits and Horizon NJ Healthspecific edits, prior to acceptance. Claim records that donot pass these edits are invalid and will be rejectedwithout being recognized as received at Horizon NJ Health. In these cases, the claim must be correctedand resubmitted within the required filing deadline of 180 calendar days from the date of service. It is important that you review the rejection notices (the functionalacknowledgements to each transaction set and theunprocessed claim report) received from Emdeon or your vendor in order to identify and resubmit theseclaims accurately.
IMPORTANT – Missing/invalid member ID will result in claim rejection.
Common Rejections• Invalid electronic claim records – common rejectionsfrom Emdeon
• Claims with missing or invalid batch level records• Claim records with missing or invalid required fields• Claim records with invalid (unlisted, discontinued,etc.) codes (CPT-4, HCPCS, ICD-9, etc.)
• Claims without or that have invalid hospital, physicianor health care professional National Provider Identifier(NPI) numbers whenever applicable. Per federalrequirements, atypical providers are excluded.
Horizon NJ Health Billing Guide, February 2014 13
BILLING GUIDE
• Invalid electronic claim records – common rejectionsfrom Horizon NJ Health (EDI edits within the claim system)
• No physical billing address on file
NOTE – Hospital, physician or health care professionalidentification number validation is not performed at Emdeon.Emdeon will reject claims for hospital, physician or health careprofessional information only if the hospital, physician or healthcare professional number fields are empty.
3.5 Submitting Corrected Claims with EDI
Providers using electronic data interchange (EDI) cansubmit “professional” corrected claims electronicallyrather than via paper to Horizon NJ Health.
NOTE – A corrected claim is defined as a resubmission of a claim with a specific change that you have made, such aschanges to CPT codes, diagnosis codes or billed amounts. It is not a request to review the processing of a claim.
The electronic corrected claim submission capabilityallows for faster processing, increased claims accuracyand a streamlined submission process. For your EDIclearinghouse or vendor to start using this new featurethey need to:
• Use “6” for adjustment of prior claims or “7” forreplacement of a prior claim utilizing bill type in loop2300, CLM05-03 (837P).
• Include the original claim number in segmentREF01=F8 and REF02=the original claim number; no dashes or spaces.
• Include the Horizon NJ Health claim number in orderto submit your claim with the 6 or 7.
• Do use this indicator for claims that were previouslyprocessed (approved or denied).
• Do not use this indicator for claims that containederrors and were not processed (such as claims that did not appear on a remittance advice; i.e., rejected up front).
• Do not submit corrected claims electronically and viapaper at the same time.
3.6 Electronic Billing Inquiries
Please direct inquiries as follows:
Action• If you would like to be authorized to transmitelectronic claims
• If you have specific EDI technical questions• If you have general EDI questions or questions onwhere to enter required data
Contact • EDI Technical Support at 1-877-234-4273
Action • If you have questions about your claims transmissionsor status reports
Contact • Contact your System Vendor or call the EmdeonCorporation Help Desk at 1-800-845-6592
Action • If you have questions about your claim status (receipt or completion dates)
• If you have questions about claims that are reported on the Remittance Advice
• If you need to know a provider ID number
Contact • Physician & Health Care Hotline at 1-800-682-9091
Action• If you would like to update provider, payee, UPIN, tax ID number, physical billing address or paymentaddress information
• For questions about changing or verifying provider information
Contact• Physician & Health Care Hotline in writing at:
Physician Services, Horizon NJ Health200 Stevens Drive, 1st FloorPhiladelphia, PA 19113-1570
fax: 1-215-937-5300 phone: 1-800-682-9091
4.0 Common Coding Requirements
4.1 Diagnosis Codes
All claims must include the proper ICD-9-CM diagnostic code.
The Centers for Medicare and Medicaid Services (CMS)provides specific guidelines to aid in standardizing U.S.coding practices. The guidelines for outpatient facilities,physician offices and ancillary care are summarized below:
• Identify each service, procedure or supply with anICD-9-CM code to describe the diagnosis, symptom,complaint, condition or problem.
• Identify services or visits for circumstances other thandisease or injury, such as follow-up care afterchemotherapy, with V codes provided for this purpose.
• Code the primary diagnosis first, followed by thesecondary, tertiary and so on. Code any coexisting
14 Horizon NJ Health Billing Guide, February 2014
BILLING GUIDE

conditions that affect the treatment of the patient. Do not code a diagnosis that is no longer applicable.
• Code to the highest degree of specificity. Carry thenumerical code to the fourth or fifth digit whenavailable. Remember, there are only approximately100 valid three-digit codes; all other ICD-9-CM codesrequire additional digits.
• Code a chronic diagnosis, when it is applicable to thepatient’s treatment.
• When only ancillary services are provided, list theappropriate V code first and the problem second. Forexample, if a patient is receiving only ancillarytherapeutic services, such as physical therapy, use theV code first, followed by the code for the condition.
• For surgical procedures, code the diagnosis applicableto the procedure. If, after the procedure has been done,the condition necessitating the surgery is morespecifically identified, or even determined to bedifferent than the preoperative diagnosis, code themost specific diagnosis determined to be the reasonfor the surgery.
Horizon NJ Health has adopted these diagnosisguidelines for its health plan and recommends thathospitals, physicians and health care professionals remaininformed about these requirements through updatedICD-9-CM coding manuals pending the transition toICD-10 in 2014.
Both the State of New Jersey and the HIPAA transactioncode sets require the use of a diagnosis code on all claims.To ensure that diagnosis codes are accurate, use theappropriate codes from the most recent ICD-9-CM codingmanuals. Using deleted or incorrect codes will result ininability to process your claim or payment delays.
NOTE – Horizon NJ Health does not have the ability to returninvalid diagnosis codes to submitters. Invalid diagnosis codesare returned to the hospitals, physicians and health careprofessionals with zeros (00000) and an explanation that thecodes are not valid.
4.2 Procedure Codes
Common Procedure TerminologyCPT is a standardized system of five-digit codes anddescriptive terms used to report the medical services andprocedures performed by physicians or health careprofessionals. It was developed and is updated andpublished annually by the American Medical Association(AMA). CPT codes communicate to physicians, healthcare professionals, patients and payors the proceduresperformed during a medical encounter. Accurate coding
is crucial for proper reimbursement from payors andcompliance with government regulations.
The AMA revises and publishes the CPT Book on anannual basis. Appendix B of CPT always consists of asummary of additions, deletions and revisions to thecurrent edition. Of these three types of changes, only the descriptions of revised codes appear in Appendix B, so you must refer to the manual itself to look at thedescriptors of the new codes.
All physicians and health care professionals must use theappropriate procedure codes from the most recentHCPCS and CPT coding manuals or quarterly updates.Claim processing cannot be completed without accurateprocedure codes, which reflect the services provided toenrollees.
IMPORTANT – Procedure coding must meet the current criteriaset by the American Medical Association (AMA) for medicalpractice norms. Horizon NJ Health does not have the ability toreturn invalid procedure codes to submitters. Invalid procedurecodes are returned to the hospitals, physicians and health careprofessionals with zeros (00000) and an explanation that thecodes are not valid.
4.3 Modifiers
Modifiers are used to report that the procedure has beenaltered by a specific circumstance. Modifiers providevaluable information about the actual services rendered,reimbursement and payment data. Modifiers also providefor coding consistency and editing for Level I (CommonProcedure Terminology Codes) and Level II (HealthcareCommon Procedure Coding System).
Sometimes, CPT codes require the addition of two-digitmodifiers. CPT modifiers allow you to show that a servicewas altered in some way from the stated CPT Bookdescription. Because the use of modifiers is frequently theonly way to alter the meaning of a CPT code, it is veryimportant to know how to use modifiers correctly.
Modifiers can indicate:
• A service or procedure has both a professional and a technical component
• A service or procedure was performed by more thanone physician
• Only part of a service was performed• An adjunctive service was performed• A bilateral procedure was performed• A service or procedure was provided more than once• Unusual events occurred
Horizon NJ Health Billing Guide, February 2014 15
BILLING GUIDE

Use the appropriate modifier from the most recentHCPCS and CPT coding manuals. Using deleted orincorrect codes and failing to use a modifier can result indenials, incorrect payments or claim payment delays.
IMPORTANT – The correct modifier must be used whenrequired by the current CPT or HCPCS publications. A validmodifier must be used to indicate the circumstance under whichthe service or item is being billed. Using appropriate modifiersprovides valuable information when evaluating claims forpayment. Missing or inaccurate modifiers, as well as missingrequired medical documentation, may result in inaccuratereimbursements or inaccurate denials for duplicate services.
IMPORTANT – All family planning procedures must be reportedusing the “FP” modifier. Claims submitted without the modifierwill be denied and returned to the submitter to be re-coded andresubmitted.
IMPORTANT – Modifiers should not be used to for multipleevaluation and management events unless the activity occurs atseparate times on the same day. The Evaluation andManagement Services Guide from CMS will be used by HorizonNJ Health to determine the appropriateness of codingsubmitted by physicians and health care professions, includingthe use of modifiers. For more information on the Evaluationand Management Services Guide please visit the MedicareLearning Network (MLN) at www.cms.gov/MLNGenInfo
NOTE – These modifiers are subject to change. Consult thecurrent CPT or HCPCS publications for the most up-to-datemodifier list.
4.4 Units
The number of units or times a particular service isperformed must be accurately indicated on all claims.When spanning dates of services, the number of unitsmust match the count of the actual days within thespanned dates. If services were performed intermittentlythroughout the spanned dates of services, each date mustbe listed separately on the bill or an itemized statementmust be submitted along with the claim.
When billing for loaded mileage, exact mileage must beidentified on the claim.
When billing for observation, units are equivalent to hours.
All anesthesia providers are required to indicate the trueamount of minutes in the days/units field of the claimform when billing for services.
IMPORTANT – The number of units and the service dates mustbe coordinated in order to obtain the most accurate reimbursementfor the services billed. Services performed once (one date of service)must be indicated with a “1” in the unit’s field.
4.5 Other Coding
Use the appropriate coding as indicated in the officialguides for the CMS 1500 and UB-04 claim forms orHIPAA compliant electronic transaction sets whencompleting additional fields such as bill type, place ofservice and type of service. Incorrect coding can causeunder- or over-payments or claim payment delays.
4.6 Pharmacy (HCPC Codes)
When billing for all “J” and “Q” codes via revenue codes634, 635, 636 and 637, the appropriate National DrugCodes (NDC) number, metric units, unit of measure, andrevenue code must be submitted as well. Failure to submitthe NDC number, metric units, unit of measure, andrevenue code along with the “J” or “Q” code will result inthe claim being rejected. This guideline applies only tofacility claims.
5.0 Common Causes of Claim ProcessingDelays, Rejections or Denials
• Authorization or referral number invalid or missing • Billed charges missing or incomplete• Claim information does not match authorization • Coordination of benefits (COB) information missingor incomplete
• Diagnosis code missing 4th or 5th digit• Diagnosis, procedure or modifier codes invalid or missing
• DRG codes missing or invalid• Early and Periodic Screening, Diagnostic andTreatment (EPSDT) information missing orincomplete
• Eligibility/enrollment is not valid on DOS• Explanation of benefits (EOB) missing or incomplete• Illegible claim information• Incomplete forms• Payor or other insurer information missing or incomplete
• Place of service code missing or invalid• Procedure/service code does not match authorization• Physician name missing or invalid• Hospital, physician or health care professionalidentification number missing or invalid
• Revenue codes missing or invalid• Spanning dates of service do not match the listeddays/units
• Signature missing• Employer identification number (EIN) missing or invalid
16 Horizon NJ Health Billing Guide, February 2014
BILLING GUIDE

• Third party liability (TPL) information missing or incomplete
• Type of service code missing or invalid
5.1 Newborn Claim Information Missing or Invalid
All newborns receive an individual member number.Always include the first and last name of the mother andbaby on the claim. If the baby has not been named, insert“Girl” or “Boy” in front of the mother’s last name as thebaby’s first name. Verify that the appropriate last name isrecorded for the mother and baby.
IMPORTANT – The claim for baby must include the baby’s dateof birth.
IMPORTANT – On claims for twins or other multiple births,indicate the birth order in the patient name field, e.g., Baby GirlSmith A, Baby Girl Smith B, etc.
5.2 Attachments Missing From Original Claim
Hospitals, physicians and health care professionals arerequired to submit an invoice for implantable items,referrals and other insurance EOBs. If these items are notsubmitted with the claim or are submitted separately(EDI and paper), incorrect payment or denials may occur.Adjustments to these payments or denials should besubmitted as corrected claims not as a resubmission ofthe original claim. Please submit to the correspondenceaddress below:
Horizon NJ HealthPhysician Claim Services
200 Stevens DrivePhiladelphia, PA 19113
Signed consent forms for sterilization are required forpayment under federal requirements. (See Section 3.3 Family Planning.) These forms should be submitted to the address below:
Horizon NJ HealthP.O. Box 7117
London, KY 40472
Signed receipt of information form, FD-189 must be submitted during the request for pre-certification for hysterectomies.
5.3 Claims and Clinical Editing
The Centers for Medicare and Medicaid Services (CMS)and the American Medical Association (AMA) havespearheaded a correct coding initiative that intends to
establish norms for coding medical services. Medicaidprograms are required to apply National Correct CodingInstitute (NCCI) edits to physician and outpatient hospitalclaims. Services deemed to be a part of a more complexservice as defined by the NCCI will be re-bundled ordenied as established by current criteria set by CMS in its claims processing manual. Horizon HJ Health alsouses the CMS Claims Processing Manual as a guide tomanaging payments for services provided to its members,including the medically unlikely edits (MUE) subset and redundant edits. CMS publishes the majority of existing MUEs on the CMS website atwww.cms.gov/nationalCorrectCodInitEd/.
Horizon NJ Health continues to enhance its software usedto adjudicate medical, professional and hospitaloutpatient claims. Horizon NJ Health uses McKessonClaimCheck software for our claim system. This softwareensures that the claim editing system is transparent to allparticipating providers and claim payments are accurateand consistent with standard business practices andmedical policies.
ClaimCheck edits are applied to all claims submitted to Horizon NJ Health by physicians, health careprofessionals and hospitals.
Horizon NJ Health also offers a claim modeling tool,Clear Claim Connection, which allows users to view howa claim will process based on the entered diagnosis andprocedure codes. Use of the system will benefitproviders, resulting in fewer claim denials due to codingerrors. Participating providers will be able to access ClearClaim Connection through the NaviNet portal. Oncesigned on to NaviNet, providers will see the link in theleft column of the Horizon NJ Health Plan Central.
6.0 Coordination of Benefits
Any services provided to a Horizon NJ Health memberare reviewed against benefits provided for that sameindividual under other insurance carriers with whom themember has coverage. Horizon NJ Health, as a managedcare program for Medicaid and NJ FamilyCare membersin New Jersey, is the “payor of last resort” on claims forservices provided to members also covered by Medicare,employee health plans or other third party medicalinsurance. Payors, which are primary to Horizon NJHealth, include (but are not limited to):
• Private health insurance, including assignableindemnity contracts
• Health maintenance organizations (HMOs)• Public health programs, such as Medicare• Profit and nonprofit health plans
Horizon NJ Health Billing Guide, February 2014 17
BILLING GUIDE

18 Horizon NJ Health Billing Guide, February 2014
BILLING GUIDE
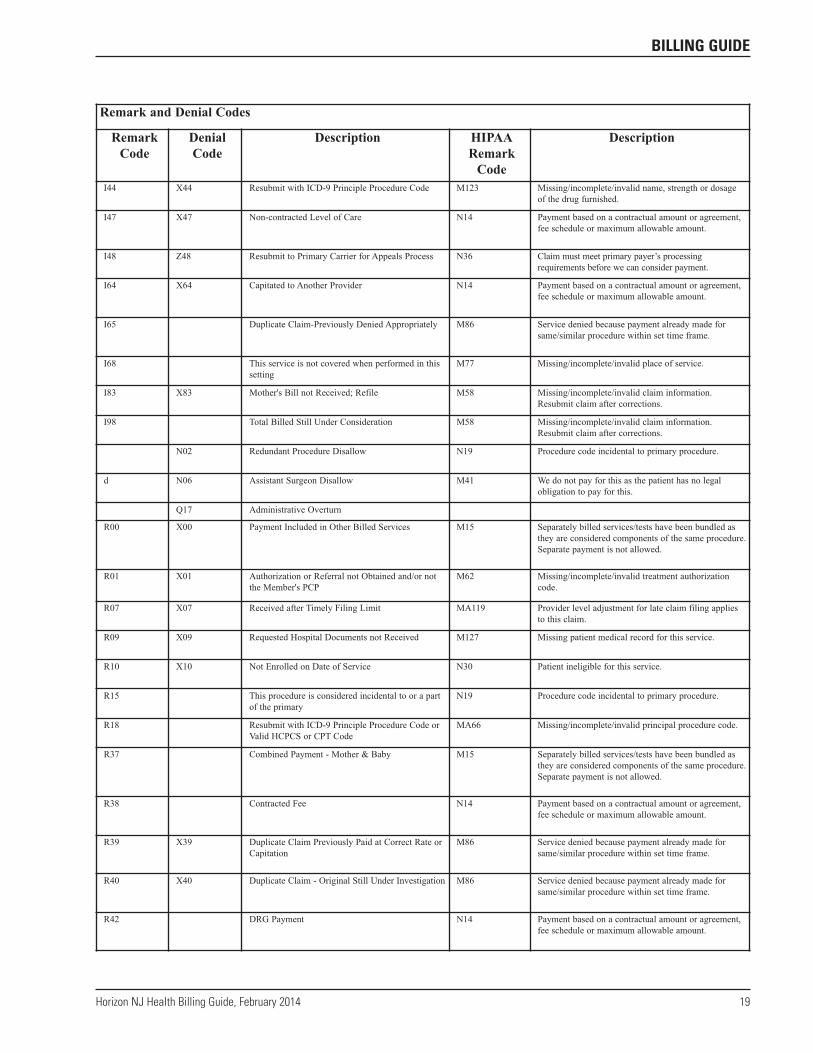
Remark and Denial Codes
RemarkCode
DenialCode
Description HIPAARemarkCode
Description
CDD Definite Duplicate Claim M86 Service denied because payment already made forsame/similar procedure within set time frame.
CRS Code Superceded - AMA CPT Guidelines N56 Procedure code billed is not correct/valid for theservices billed or the date of service billed.
CRT Code Superceded - AMA CPT Guidelines - Denied N56 Procedure code billed is not correct/valid for theservices billed or the date of service billed.
F47 F47 N9 Adjustment represents the estimated amount a previouspayer may pay.
F50 Claim Adjustment-Third Party Denied or BenefitsExhausted
N14 Payment based on a contractual amount or agreement,fee schedule or maximum allowable amount.
I02 X02 Illegible Records Submitted; Please Refile M127 Missing patient medical record for this service.
I04 X04 Correct NDC Code and/or Drug Name Required forConsideration.
M58 Missing/incomplete/invalid claim information.Resubmit claim after corrections.
I05 X05 Invalid/Inappropriate/Deleted Code, Modifier orDescription
N56 Procedure code billed is not correct/valid for theservices billed or the date of service billed.
I06 X06 Itemized Bill, Dates of Service, Charges or InvoiceRequired
M58 Missing/incomplete/invalid claim information.Resubmit claim after corrections.
I08 X08 Diagnosis Invalid/Missing/Deleted/ Requires 4th or5th digit
M81 You are required to code to the highest level ofspecificity.
I10 E-Code Cannot Be Used As Primary Diagnosis M76 Missing/incomplete/invalid diagnosis or condition.
I11 X11 EOB from Primary Carrier Required MA04 Secondary payment cannot be considered without theidentity of or payment information from the primarypayer. The information was either not reported or wasillegible.
I18 Paid Billed Charges N14 Payment based on a contractual amount or agreement,fee schedule, or maximum allowable amount.
I19 X19 Carrier of Service Scion Dental N193 Specific federal/state/local program may cover thisservice through another payer.
I22 X22 Resubmit with Visit codes & Charges M58 Missing/incomplete/invalid claim information.Resubmit claim after corrections.
I24 X24 Carrier of Service-Davis Vision N193 Specific federal/state/local program may cover thisservice through another payer.
I26 X26 Exhaustion of Benefits N130 Alert: Consult plan benefit documents/guidelines forinformation about restrictions for this service.
I27 X27 Submit Medical Records to Horizon NJ HealthAppeals Unit
N193 Specific federal/state/local program may cover thisservice through another payer.
I28 Reprocessed-Claim Subject to Interest MA67 Correction to a prior claim.
I30 X30 Service Exceeds Lifetime Limitation N117 This service is paid only once in a patient’s lifetime.
I37 X37 Resubmit with Appropriate Modifier and/or Units M53 Missing/incomplete/invalid days or units of service.
I42 X42 Illegible/Incomplete/Inappropriate ReferralReceived
M62 Missing/incomplete/invalid treatment authorizationcode.
I43 X43 Bi-Lateral Procedure Previously Paid with Modifier"50"
M86 Service denied because payment already made forsame/similar procedure within set time frame.
I44 X44 Resubmit with ICD-9 Principle Procedure Code M123 Missing/incomplete/invalid name, strength or dosageof the drug furnished.
Horizon NJ Health Billing Guide, February 2014 19
BILLING GUIDE
Remark and Denial Codes
RemarkCode
DenialCode
Description HIPAARemarkCode
Description
I44 X44 Resubmit with ICD-9 Principle Procedure Code M123 Missing/incomplete/invalid name, strength or dosageof the drug furnished.
I47 X47 Non-contracted Level of Care N14 Payment based on a contractual amount or agreement,fee schedule or maximum allowable amount.
I48 Z48 Resubmit to Primary Carrier for Appeals Process N36 Claim must meet primary payer’s processingrequirements before we can consider payment.
I64 X64 Capitated to Another Provider N14 Payment based on a contractual amount or agreement,fee schedule or maximum allowable amount.
I65 Duplicate Claim-Previously Denied Appropriately M86 Service denied because payment already made forsame/similar procedure within set time frame.
I68 This service is not covered when performed in thissetting
M77 Missing/incomplete/invalid place of service.
I83 X83 Mother's Bill not Received; Refile M58 Missing/incomplete/invalid claim information.Resubmit claim after corrections.
I98 Total Billed Still Under Consideration M58 Missing/incomplete/invalid claim information.Resubmit claim after corrections.
N02 Redundant Procedure Disallow N19 Procedure code incidental to primary procedure.
d N06 Assistant Surgeon Disallow M41 We do not pay for this as the patient has no legalobligation to pay for this.
Q17 Administrative Overturn
R00 X00 Payment Included in Other Billed Services M15 Separately billed services/tests have been bundled asthey are considered components of the same procedure.Separate payment is not allowed.
R01 X01 Authorization or Referral not Obtained and/or notthe Member's PCP
M62 Missing/incomplete/invalid treatment authorizationcode.
R07 X07 Received after Timely Filing Limit MA119 Provider level adjustment for late claim filing appliesto this claim.
R09 X09 Requested Hospital Documents not Received M127 Missing patient medical record for this service.
R10 X10 Not Enrolled on Date of Service N30 Patient ineligible for this service.
R15 This procedure is considered incidental to or a partof the primary
N19 Procedure code incidental to primary procedure.
R18 Resubmit with ICD-9 Principle Procedure Code orValid HCPCS or CPT Code
MA66 Missing/incomplete/invalid principal procedure code.
R37 Combined Payment - Mother & Baby M15 Separately billed services/tests have been bundled asthey are considered components of the same procedure.Separate payment is not allowed.
R38 Contracted Fee N14 Payment based on a contractual amount or agreement,fee schedule or maximum allowable amount.
R39 X39 Duplicate Claim Previously Paid at Correct Rate orCapitation
M86 Service denied because payment already made forsame/similar procedure within set time frame.
R40 X40 Duplicate Claim - Original Still Under Investigation M86 Service denied because payment already made forsame/similar procedure within set time frame.
R42 DRG Payment N14 Payment based on a contractual amount or agreement,fee schedule or maximum allowable amount.

20 Horizon NJ Health Billing Guide, February 2014
BILLING GUIDE
RemarkCode
DenialCode
Description HIPAARemarkCode
Description
R43 Interim Bill Payment N14 Payment based on a contractual amount or agreement,fee schedule or maximum allowable amount.
R44 Multiple Surgical Reduction N14 Payment based on a contractual amount or agreement,fee schedule or maximum allowable amount.
R45 X45 Complete Medical Records Required forConsideration; Refile
N101 Additional information is needed in order to processthis claim. Please resubmit the claim with theidentification number of the provider where thisservice took place. The Medicare number of the site ofservice provider should be preceded with the letter
R46 X46 Over Maximum Procedure/Benefit Limit N130 Alert: Consult plan benefit documents/guidelines forinformation about restrictions for this service.
R47 Payment Reflects Coordination of Benefits, if $0,Max Liability Met
N9 Adjustment represents the estimated amount a previouspayer may pay.
R49 X49 Previous Payments Equal to Purchase Price M15 Separately billed services/tests have been bundled asthey are considered components of the same procedure.Separate payment is not allowed.
R50 X50 Same Procedure Paid to a Different Provider MA29 Missing/incomplete/invalid provider name, city, stateor ZIP code.
R51 X51 Service Not Covered N30 Patient ineligible for this service.
R53 X53 Services Were not Provided N29 Missing documentation/orders/notes/summary/report/chart.
R55 Billed Info Reflects Lower DegreeAcuity/Treatment
M25 The information furnished does not substantiate theneed for this level of service. If you believe theservice should have been fully covered as billed, or ifyou did not know and could not reasonably have beenexpected to know that we would not pay for theservice.
R56 Administrative Approval N10 Payment based on the findings of a revieworganization/professional consult/manualadjudication/medical or dental advisor.
R59 X59 Authorization/Referral Expired M62 Missing/incomplete/invalid treatment authorizationcode.
R60 X60 Dates and/or Services OutsideReferral/Authorization
M62 Missing/incomplete/invalid treatment authorizationcode.
R61 X61 No PCP Referral N54 Claim information is inconsistent withprecertified/authorized services.
R65 Interim Bill 2nd Cycle Payment N14 Payment based on a contractual amount or agreement,fee schedule, or maximum allowable amount.
R66 Z34 Interim Bill Final Cycle Payment N14 Payment based on a contractual amount or agreement,fee schedule, or maximum allowable amount.
R67 X67 Discrepancy with Level of Care - Appeal Required M25 The information furnished does not substantiate theneed for this level of service. If you believe theservice should have been fully covered as billed, or ifyou did not know and could not reasonably have beenexpected to know that we would not pay for theservice.
R70 X70 EPSDT Screening Didn't Comply with PeriodicitySchedule
N78 The necessary components of the child and teencheckup (EPSDT) were not completed.
R71 X71 Duplicate of Previously Submitted EPSDTScreening
M86 Service denied because payment already made forsame/similar procedure within set time frame.
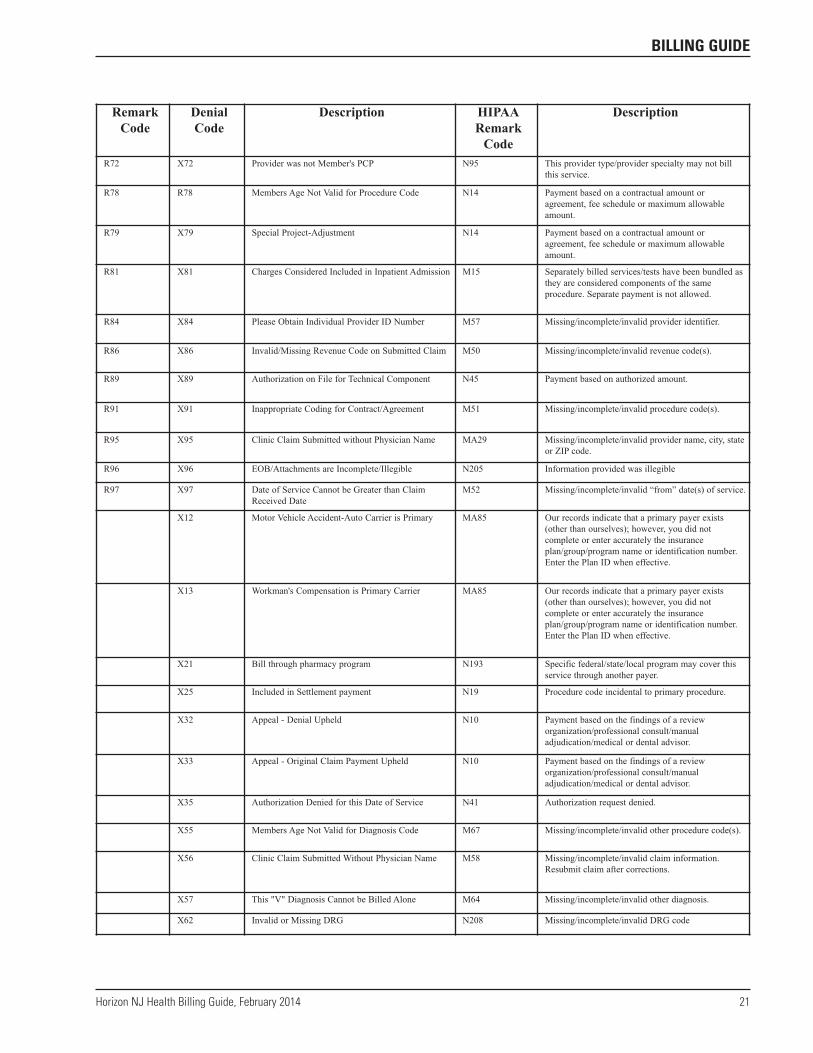
Horizon NJ Health Billing Guide, February 2014 21
BILLING GUIDE
RemarkCode
DenialCode
Description HIPAARemarkCode
Description
R72 X72 Provider was not Member's PCP N95 This provider type/provider specialty may not billthis service.
R78 R78 Members Age Not Valid for Procedure Code N14 Payment based on a contractual amount oragreement, fee schedule or maximum allowableamount.
R79 X79 Special Project-Adjustment N14 Payment based on a contractual amount oragreement, fee schedule or maximum allowableamount.
R81 X81 Charges Considered Included in Inpatient Admission M15 Separately billed services/tests have been bundled asthey are considered components of the sameprocedure. Separate payment is not allowed.
R84 X84 Please Obtain Individual Provider ID Number M57 Missing/incomplete/invalid provider identifier.
R86 X86 Invalid/Missing Revenue Code on Submitted Claim M50 Missing/incomplete/invalid revenue code(s).
R89 X89 Authorization on File for Technical Component N45 Payment based on authorized amount.
R91 X91 Inappropriate Coding for Contract/Agreement M51 Missing/incomplete/invalid procedure code(s).
R95 X95 Clinic Claim Submitted without Physician Name MA29 Missing/incomplete/invalid provider name, city, stateor ZIP code.
R96 X96 EOB/Attachments are Incomplete/Illegible N205 Information provided was illegible
R97 X97 Date of Service Cannot be Greater than ClaimReceived Date
M52 Missing/incomplete/invalid “from” date(s) of service.
X12 Motor Vehicle Accident-Auto Carrier is Primary MA85 Our records indicate that a primary payer exists(other than ourselves); however, you did notcomplete or enter accurately the insuranceplan/group/program name or identification number.Enter the Plan ID when effective.
X13 Workman's Compensation is Primary Carrier MA85 Our records indicate that a primary payer exists(other than ourselves); however, you did notcomplete or enter accurately the insuranceplan/group/program name or identification number.Enter the Plan ID when effective.
X21 Bill through pharmacy program N193 Specific federal/state/local program may cover thisservice through another payer.
X25 Included in Settlement payment N19 Procedure code incidental to primary procedure.
X32 Appeal - Denial Upheld N10 Payment based on the findings of a revieworganization/professional consult/manualadjudication/medical or dental advisor.
X33 Appeal - Original Claim Payment Upheld N10 Payment based on the findings of a revieworganization/professional consult/manualadjudication/medical or dental advisor.
X35 Authorization Denied for this Date of Service N41 Authorization request denied.
X55 Members Age Not Valid for Diagnosis Code M67 Missing/incomplete/invalid other procedure code(s).
X56 Clinic Claim Submitted Without Physician Name M58 Missing/incomplete/invalid claim information.Resubmit claim after corrections.
X57 This "V" Diagnosis Cannot be Billed Alone M64 Missing/incomplete/invalid other diagnosis.
X62 Invalid or Missing DRG N208 Missing/incomplete/invalid DRG code
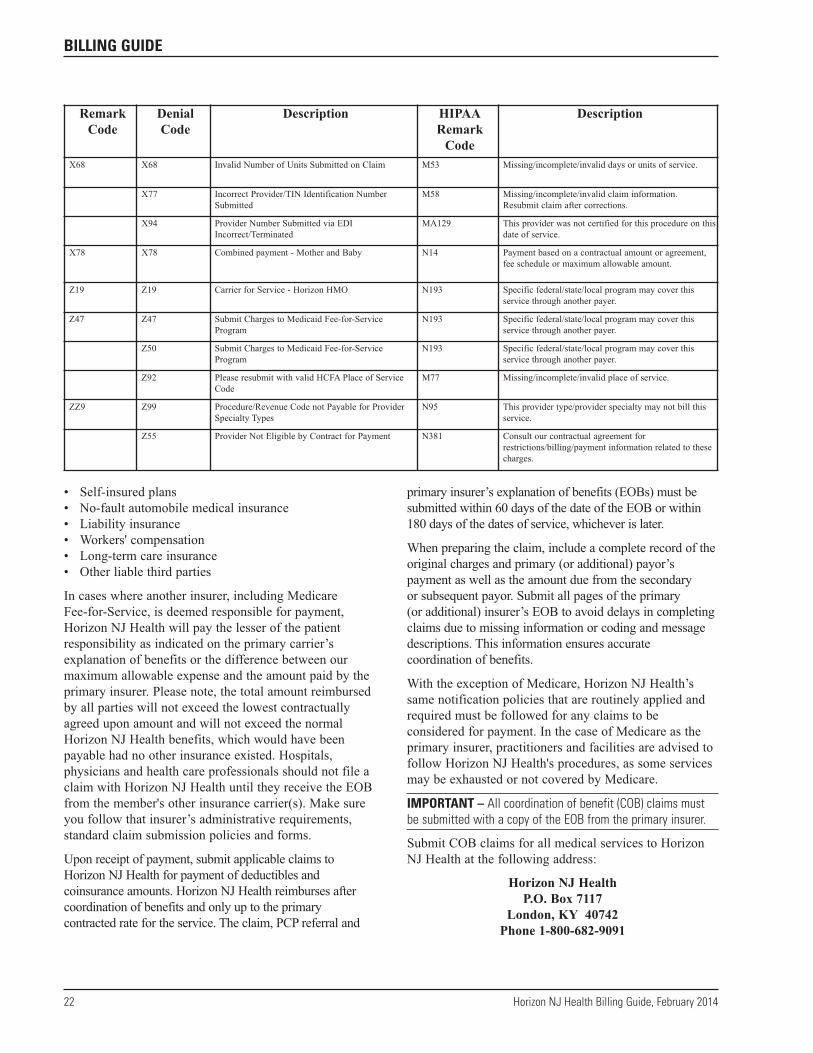
• Self-insured plans• No-fault automobile medical insurance• Liability insurance• Workers' compensation• Long-term care insurance• Other liable third parties
In cases where another insurer, including MedicareFee-for-Service, is deemed responsible for payment,Horizon NJ Health will pay the lesser of the patientresponsibility as indicated on the primary carrier’sexplanation of benefits or the difference between ourmaximum allowable expense and the amount paid by theprimary insurer. Please note, the total amount reimbursedby all parties will not exceed the lowest contractuallyagreed upon amount and will not exceed the normalHorizon NJ Health benefits, which would have beenpayable had no other insurance existed. Hospitals,physicians and health care professionals should not file aclaim with Horizon NJ Health until they receive the EOBfrom the member's other insurance carrier(s). Make sureyou follow that insurer’s administrative requirements,standard claim submission policies and forms.
Upon receipt of payment, submit applicable claims toHorizon NJ Health for payment of deductibles andcoinsurance amounts. Horizon NJ Health reimburses aftercoordination of benefits and only up to the primarycontracted rate for the service. The claim, PCP referral and
primary insurer’s explanation of benefits (EOBs) must besubmitted within 60 days of the date of the EOB or within180 days of the dates of service, whichever is later.
When preparing the claim, include a complete record of theoriginal charges and primary (or additional) payor’spayment as well as the amount due from the secondary or subsequent payor. Submit all pages of the primary (or additional) insurer’s EOB to avoid delays in completingclaims due to missing information or coding and messagedescriptions. This information ensures accuratecoordination of benefits.
With the exception of Medicare, Horizon NJ Health’ssame notification policies that are routinely applied andrequired must be followed for any claims to beconsidered for payment. In the case of Medicare as theprimary insurer, practitioners and facilities are advised tofollow Horizon NJ Health's procedures, as some servicesmay be exhausted or not covered by Medicare.
IMPORTANT – All coordination of benefit (COB) claims mustbe submitted with a copy of the EOB from the primary insurer.
Submit COB claims for all medical services to HorizonNJ Health at the following address:
Horizon NJ HealthP.O. Box 7117
London, KY 40742Phone 1-800-682-9091
22 Horizon NJ Health Billing Guide, February 2014
BILLING GUIDE
RemarkCode
DenialCode
Description HIPAARemarkCode
Description
X68 X68 Invalid Number of Units Submitted on Claim M53 Missing/incomplete/invalid days or units of service.
X77 Incorrect Provider/TIN Identification NumberSubmitted
M58 Missing/incomplete/invalid claim information.Resubmit claim after corrections.
X94 Provider Number Submitted via EDIIncorrect/Terminated
MA129 This provider was not certified for this procedure on thisdate of service.
X78 X78 Combined payment - Mother and Baby N14 Payment based on a contractual amount or agreement,fee schedule or maximum allowable amount.
Z19 Z19 Carrier for Service - Horizon HMO N193 Specific federal/state/local program may cover thisservice through another payer.
Z47 Z47 Submit Charges to Medicaid Fee-for-ServiceProgram
N193 Specific federal/state/local program may cover thisservice through another payer.
Z50 Submit Charges to Medicaid Fee-for-ServiceProgram
N193 Specific federal/state/local program may cover thisservice through another payer.
Z92 Please resubmit with valid HCFA Place of ServiceCode
M77 Missing/incomplete/invalid place of service.
ZZ9 Z99 Procedure/Revenue Code not Payable for ProviderSpecialty Types
N95 This provider type/provider specialty may not bill thisservice.
Z55 Provider Not Eligible by Contract for Payment N381 Consult our contractual agreement forrestrictions/billing/payment information related to thesecharges.

NOTE – Although a primary insurer may have unique codingspecific to their business, providers must bill with validICD-9-CM, CPT-4 and HCPCS codes. Unique or invalid codesspecific to other insurers will cause claim processing delays ordenials.
IMPORTANT – The hospital, physician or health careprofessional may not submit billed charges to Horizon NJ Health that are different than charges submitted to otherinsurers for the same services. The submitted bill must containthe exact billed amounts by procedure line as is reflected on theprimary or additional insurer’s EOB.
IMPORTANT – The primary or additional insurer’s EOB mustinclude member name, billed amounts, paid amounts,adjustments, coinsurance amounts, deductibles, copaymentsand all associated messages and notes. Incomplete informationmay result in a claim processing delay or denial.
6.1 Medicare
When both Medicare and Medicaid cover a member andthe service is a benefit of both programs, the claim mustfirst be filed with Medicare. Hospitals, physicians andhealth care professionals should not file a claim withHorizon NJ Health until they receive the Medicare EOB.Upon receipt of payment, submit the claim along with acopy of the Medicare EOB to Horizon NJ Health within60 days of the date of the Medicare EOB or 180 daysfrom the date of service, whichever is later.
Medicare primary members have no prior authorizationrequirements and are not required to be seen by aparticipating Horizon NJ Health hospital, physician orhealth care professional, unless Medicare does not coverthe service. When Horizon NJ Health, by default,becomes the primary payor, the hospital, physician orhealth care professional must comply with all coveragerequirements indicated by Horizon NJ Health to beconsidered for payment. Horizon NJ Health advises thatservices to members covered by Medicare and Medicaidbe reported despite the fact that authorization is notrequired. This will avoid delays in claims payment forservices that Horizon NJ Health must cover.
Medicare-eligible services denied by Medicare due tofailure to comply with medical, administrative or filingrequirements will not be covered by Horizon NJ Health.
NOTE – When Medicare is primary…
• and the procedure is covered by Medicare, an authorizationor referral is not required by Horizon NJ Health, even if oneis normally required by Horizon NJ Health. Reporting theseservices to Horizon NJ Health is advised.
• and the procedure is not covered by Medicare, anauthorization or referral is required by Horizon NJ Health ifone is normally required by Horizon NJ Health.
IMPORTANT – The hospital, physician or health careprofessional may re-bill for services originally denied byMedicare when Medicare overturns the denial. The hospital,physician or health care professional must submit the re-billwithin 60 days of the date of Medicare’s EOB.
6.2 Other Third Party Medical Insurance
Members covered by a primary insurer including Medicareshould be instructed to notify Horizon NJ Health of theirprimary coverage.
Claims submitted to Horizon NJ Health as the secondaryor tertiary insurer are subject to eligibility and benefitcoverage. To receive payment for a claim submitted toHorizon NJ Health as the secondary or tertiary insurer,the hospital, physician or health care professional mustsubmit a copy of the primary insurer’s EOB or denialletter along with the claim to Horizon NJ Health.
NOTE – Submit claims to Horizon NJ Health within 60 days ofthe date of the primary insurer’s remittance and/or EOB or 180days from the date of service, whichever is later.
Participating hospitals, physicians or health careprofessionals may not bill Horizon NJ Health membersfor deductibles and coinsurance or balances above ourallowable fees. Medicaid is the “payor of last resort;”therefore, the payments received from the primary insurerand/or Horizon NJ Health must be considered payment infull. Members are not to be billed for any Horizon NJHealth covered service. If the service is not covered bythe other insurer or Horizon NJ Health, there must beprior written agreement to bill the member for thesenon-covered services.
REFER TO – Section 10.0 Complaint and Appeals Process, forcomplete instructions of the submission timeframes andprocedures for administrative or medical appeals.
IMPORTANT – If there is any possibility that the servicesprovided will not be covered by the primary insurer, thehospitals, physicians or health care professionals should obtainthe appropriate referrals or prior authorizations needed toobtain coverage under Horizon NJ Health. Failure to do so mayresult in denial for payment.
IMPORTANT – If you provide services to a member who is illor injured as the result of a third party action, you must notifyHorizon NJ Health of this information. In the event that thisinformation is determined after the claim is submitted and/or
Horizon NJ Health Billing Guide, February 2014 23
BILLING GUIDE
resolved, you are still required to inform Horizon NJ Health.This includes recording the information about the injury orcondition on the claim and notifying Horizon NJ Health of anylawsuits or legal action in relation to the injury or condition.
IMPORTANT –When completing the CMS 1500 (HCFA 1500)claim form, be sure to complete item #7 on the form.
Motor Vehicle AccidentsMotor vehicle accident-related claims should besubmitted to the primary carrier prior to being submittedto Horizon NJ Health. If benefits exhaust or areunavailable, the claim may be submitted to Horizon NJ Health along with an explanation of benefits or adenial letter in order to be considered for payment.
In all cases, Horizon NJ Health’s referral, priorauthorization and notification policies that are routinelyapplied and required must be followed for any claims tobe considered for payment.
Upon receipt of a letter of exhaustion or denial letterfrom the primary carrier, the hospital, physician or healthcare professional will have 60 days from the date of theletter to submit the claim. Upon receipt of an EOB fromthe primary carrier, Horizon NJ Health will pay the lesserof the patient responsibility as indicated on the primarycarrier’s EOB or the difference between our maximumallowable expense and the amount paid by the primaryinsurer. Please note, the total amount reimbursed by allparties will not exceed the lowest contractually agreedupon amount and normal Horizon NJ Health benefits,which would have been payable had no other insuranceexisted. In all cases, Horizon NJ Health’s referral, priorauthorization and notification policies that are routinelyapplied and required must be followed for any claims tobe considered for payment.
IMPORTANT – When preparing the claim, all informationrelating to the accident must be included on the claim. Thisincludes diagnosis codes, accident indicators and occurrencecodes (UB-04 claim forms) where appropriate. Additionally, if aprimary insurer has made payment for services, the insurer’sEOB must be included when submitting the claim for payment.
Worker’s CompensationWorkers’ compensation covers any injury that is the resultof a work-related accident. If Horizon NJ Health is awareof a workers’ compensation carrier, Horizon NJ Health willreject the hospital, physician or health care professional’sclaim and direct that the claim be submitted first to theprimary workers' compensation carrier. If insurancecoverage is not available at the time the claim is submitted
or the workers' compensation carrier ceases to providecoverage, the claim will be considered for payment.
Upon receipt of a letter of exhaustion or denial letterfrom the primary carrier, the hospital, physician or healthcare professional will have 60 days from the date of theletter to submit the claim.
IMPORTANT –When completing the CMS 1500 (HCFA 1500)claim form, be sure to complete #7 on the form. For moreinformation on the referral form, refer to Section 6.0 Referralsto Specialty Care Providers.
6.3 Reimbursement
MedicareIf a member has Medicaid and Medicare coverage, thehospital, physician or health care professional may billfor charges Medicare applied to the deductible orcoinsurance, or both. Horizon NJ Health will pay thelesser of the patient responsibility as indicated on theprimary carrier’s EOB or the difference between ourmaximum allowable expense and the amount paid by theprimary insurer. Please note, the total amount reimbursedby all parties will not exceed the lowest contractuallyagreed upon amount and normal Horizon NJ Healthbenefits, which would have been payable had no otherinsurance existed.
NOTE – Horizon NJ Health considers the deductible, coinsuranceand copayments a component of the total primary care capitationfor primary care reimbursement for services, which are capitated.If your primary care contact is for Fee-for-Service reimbursement,please first bill the primary carrier and then bill Horizon NJ Healthwith the carrier(s) EOB.
IMPORTANT – Bills submitted to the secondary insurer mustexactly match the services and amount billed to the primaryinsurer. This information, along with the primary insurer’s EOB,is necessary to complete an accurate COB. Incompleteinformation could result in processing delays or denials.
Other Third Party Medical InsuranceHorizon NJ Health will pay the lesser of the patientresponsibility as indicated on the primary carrier’sexplanation of benefits or the difference between ourmaximum allowable expense and the amount paid by theprimary insurer. Please note, the total amount reimbursedby all parties will not exceed the lowest contractuallyagreed upon amount and normal Horizon NJ Healthbenefits, which would have been payable had no otherinsurance existed.
24 Horizon NJ Health Billing Guide, February 2014
BILLING GUIDE

Guidelines on Billing Mileage for MemberTransportation Services Horizon NJ Health members shall be transported to andfrom medical appointments in a manner that results in theaccrual of the least number of miles. Mileage is measuredby odometer from the place of departure or the point atwhich the member enters the vehicle to the destination orpoint at which the member exits the vehicle. At no timeshall the transportation provider’s base location be usedwhen calculating mileage.
6.4 Services That Do Not Require a Primary Insurer EOB
Services Not Covered by Traditional Medicare• Hearing aids• Diapers/Under-pads/Incontinence items• EPSDT• Personal care assistants (Medicare FFS only)• Medical day care (Medicare FFS only)
Physician and health care professionals may bill HorizonNJ Health for these services without submission of aprimary insurer’s EOB.
NOTE – If a service is covered by Medicare Advantage, pleasesupply the resulting EOB.
IMPORTANT – If billing for room and board only at a skillednursing facility, reimbursement will be considered withoutsubmission of Medicare EOB.
Other Third Party Medical InsuranceAn EOB or notice of refusal must be submitted with allcommercial and Medicare Advantage insurers’ claims.
6.5 Denials from Primary Insurers
If the primary insurer denies payment to the hospital,physician or health care professional based on coverageexclusion, non-coverage, benefit exhaustion ornon-compliance with administrative guidelines, thephysician must submit a copy of the EOB or notice ofrefusal. The EOB or notice of refusal must include anexplanation of the reason for the denial.
Services denied by the primary insurer and billed toHorizon NJ Health without an explanation of the denialfrom the primary insurer will be denied payment. Servicesdenied by the primary insurer for noncompliance withmedical or administrative guidelines may be submitted tothe secondary with a copy of the EOB or notice of refusal
and a copy of the final appeal denial letter or notice ofrefusal. Medical and/or administrative denials will not beconsidered without receipt of the final appeal denial letter.
IMPORTANT – Horizon NJ Health will document receipt ofnotices that the member's primary carrier does not cover aservice or that the service is exhausted. No additional noticeswill be required until the anniversary date of the member'spolicy with that other insurer. Annually, on or after theanniversary date, the hospital, physician or health careprofessional must provide notice again that the service isexhausted or not covered by the primary carrier.
NOTE – The hospital, physician or health care professional mustfile a claim with the primary insurer within the appropriate timelyfiling deadlines and according to appropriate filing requirements.Failure to submit medical and administrative denial informationfrom a primary insurer could result in processing delays or denials.
IMPORTANT – Upon receipt of a letter of exhaustion or denialletter from the primary carrier, the hospital, physician or healthcare professional will have 60 days from the date of the letterto submit the claim.
7.0 Early and Periodic Screening, Diagnosisand Treatment (EPSDT)
EPSDT claims are paid based on the periodicity schedule.The biological component of immunizations is only paidwhere the Vaccine for Children (VFC) program does notoffer the biological or the supply is not available.Administration of VFC-sponsored immunizations is paidon a per-visit basis; therefore, multiple shots given in asingle visit will result in a per-vaccine administrationpayment. Physicians and health care professionals areencouraged to use combination immunizations when available.
To allow for efficiencies in monitoring, tracking andreporting encounter data to the Department of HumanServices, Division of Medical Assistance and HealthServices (DMAHS), an “EP” modifier should be usedwhen reporting EPSDT services, including venipunctureCPT codes 36406, 36415 and 36416 when used for lead testing.
Horizon NJ Health sends quarterly EPSDTunderutilization reports to physicians, identifyingmembers whose EPSDT services are overdue.Compliance with using the EP modifier will increase the accuracy of these reports.
Horizon NJ Health Billing Guide, February 2014 25
BILLING GUIDE
8.0 Risk Assessment Program/Encounters
Horizon NJ Health is required by the State of New Jerseyto report encounter data for all services rendered to ourmembers, including capitated and fee-for-serviceactivities. All physicians, hospitals and health careprofessionals are required to submit timely, accurate andcomplete encounter data. This is required even when themember is covered by another insurer.
Health care resource consumption in chronic disease canbe very high. The State of New Jersey is using a riskadjustment payment model in an attempt to fairlydistribute Medicaid funds in proportion to the severity of illness. Horizon NJ Health is required to submitencounter data to the State of New Jersey as an estimateof the prevalence of disease in the population we serve.
It is paramount that accurate data be gathered on theprevalence of illness of Horizon NJ Health members.This leads to accurate, severity-adjusted payment fromthe State to the health plan and, ultimately, the provider.
For example: Not only should members seek medicalcare for acute conditions, they should also visit theirprovider for chronic conditions, such as diabetes orhypertension. Moreover, if a member visits for an acuteissue and a chronic issue is relevant or discussed, we askthat this is documented in both the records and theencounter claim form.
For further information, please call Horizon NJ Health’sRisk Adjustment nurse at 1-800-682-9094, ext. 89625.
All services must be submitted on the CMS 1500 (HCFA1500) or the UB-04 claim form, or via electronicsubmission in a HIPAA-compliant 837I, 837P or NCPDPformat. Horizon NJ Health is required to submit this datain a HIPAA standard file format to the State. Any codedfield or data element contained in a HIPAA transactionmust adhere to the national set of codes, includingmedical services and diagnosis. Due to the requirement tosubmit all services to the State, all requirements for EDItransactions are also applied to paper claims.
The State of New Jersey will reject encounter data if itdoes not meet their processing criteria. In some instances,Horizon NJ Health will be required to reverse paymentalready made to the provider if the encounter does notmeet the State’s criteria. A complete list of all possibleencounter rejections can be obtained by going towww.njmmis.com. Under the Information section, selectEdit Codes, then Encounter Edits. The following aresome causes for rejections:
Facility Services• NPI – Any practitioner who is required to have an NPI must report that number in the Billing Provider,Rendering Provider, Attending Provider, OperatingProvider and Other Provider fields, if applicable. TheNPI is required by the State of New Jersey’s Divisionof Medical Assistance and Health Services for bothelectronic and paper claims submissions. Horizon NJ Health and all practitioners of facilities servingmembers are required to comply with this requirement.
• Type of Bill – The bill type must be consistent withthe type of service rendered with applicable revenuecodes and corresponding HCPCS. Common bill typesare listed in Section 9.2.2 of this manual.
• Statement Covers Period – Any practitioner billing forservices must ensure that the dates of service arewithin the time period indicated in the StatementCovers Period stated on the claim. If a date of serviceis outside the dates placed in the From/Through field,the encounter will be rejected.
• Principle Procedure Date – Any practitioner billing forsurgical services must ensure that the dates of serviceare within the time period indicated in the StatementCovers Period indicated on the claim. If the PrincipleProcedure date or Other Procedure date field is outsidethe dates reported in the Statement Covers Period, theencounter will be rejected.
• Revenue Codes – All revenue codes billed must bevalid for the type of claim being billed.
• Laboratory Services – When billing revenue codes300-319, the corresponding HCPCS or CPT codesmust be billed.
• Physician Administered Drug – Outpatient services arerequired to report units of measure for all drugs,including their corresponding NDC code when billingwith “J” or “Q” codes, with the exception of Q0091and Q0092. The corresponding 11 digit NDC codemust be reported along with the correct unit ofmeasure:• F2 - International measure• GR- Gram• ME - Milligram• ML- Milliliter• UN- Unit (for example, tablet, capsule)
Claims cannot be paid by Horizon NJ Health withoutthis information.
• Claims received with member coverage secondary toMedicare or commercial insurance are excluded fromthis requirement.
26 Horizon NJ Health Billing Guide, February 2014
BILLING GUIDE

• Diagnosis Codes – All diagnosis codes must bereported and coded to the 4th and 5th digit
Professional Services• NPI – Any practitioner who is required to have an NPImust report that number in the Billing Provider,Rendering Provider and Service Facility Location ifapplicable. The NPI is required by the State of NewJersey’s Division of Medical Assistance and HealthServices for both electronic and paper claimssubmissions. Horizon NJ Health and all practitionersof facilities serving members are required to complywith this requirement.
• Physician Administered Drugs – All claims submittedfor physician-administered prescription drugs,regardless of setting, must include the 11-digit NDCnumber, the quantity of the drug administered ordispensed and the two-digit qualifier identifying theunit of measure (UOM). This requirement is a resultof the Federal Deficit Reduction Act of 2005. Outpatient-administered drugs are identified by theHCPCS procedure codes J0120 - J9999; Q0035,Q0081, Q0091, Q0111 - Q0115, Q0138 - Q0139,Q0144, Q0162 - Q0181, Q0481 - Q4130, Q3001,Q3014 - Q3031, Q9955 - Q9968.Acceptable UOM for these codes are:• F2 – International measure• GR – Gram• ME - Milligram• ML – Milliliter• UN – Unit (for example, tablet, capsule)
• Claims received with member coverage secondary toMedicare or commercial insurance are excluded fromthis requirement.
• The Division of Medical Assistance and HealthServices has created a website with key billinginformation. Visit www.njmmis.com and click onPhysician Administered Drugs (UOM). By enteringthe NDC for the drug being administered, informationregarding the drug name and the correct UOM will be displayed.
• Transportation Services – When billing fortransportation services, a valid origin and destinationmodifier are required. Horizon NJ Health membersshall be transported to and from medical appointmentsin a manner that results in the accrual of the leastnumber of miles. Mileage is measured by odometerfrom the place of departure or the point at which themember enters the vehicle to the destination or pointat which the member exits the vehicle. At no time
shall the transportation provider’s base location beused when calculating mileage. The CMS-1500 claimform should be completed by choosing modifiers thatappropriately support the member’s place of departureand destination locations.
• Procedure Codes – All codes are to be inHIPAA-compliant format. The use of CPT Level IIIcodes (local codes) is no longer valid
• Diagnosis Codes – All diagnosis codes must bereported and coded to the 4th and 5th digit asappropriate
• Retroactive Terminations – Horizon NJ Healthparticipates in the Medicaid and NJ FamilyCareprograms. Our members must maintain eligibility inorder to receive services. There may be times when a member’s eligibility is retroactively terminated, asdetermined by the Medicaid/NJ FamilyCare program.This retroactivity will result in an encounter rejection.Horizon NJ Health is required to reverse paymentalready made to the physician, hospital and health care professional
• Medical Claims for Fluoride Varnish – providersshould use the following procedure and diagnosiscodes when submitting medical claims for fluoridevarnish applications: • 99420-DA• V07.31 (ICD 9)
9.0 Remittance Advice Documentation
Overview of Payment Summary PageHorizon NJ Health provides a comprehensive summaryof financial information and activity on the RemittanceAdvice (RA).
The body of the RA contains claim detail and thePayment Summary page indicates whether thephysician/payee has a positive (+) or negative (-) balance.
Many hospitals, physicians or health care professionalshave requested ongoing notification of overpayments andnegative payee balances in relation to claim adjudicationactivities, capitation payments, or accounts payableadjustments. The Payment Summary page displays thisinformation as “rolling balances” of overpaid amountsthat are owed to Horizon NJ Health. The “rollingbalance” is updated on each RA after current claimpayments and other adjustments have been applied.
If, after reviewing the RA, you have questions or want torequest a reconsideration, contact the Physician & HealthCare Hotline at 1-800-682-9091 for assistance.
Horizon NJ Health Billing Guide, February 2014 27
BILLING GUIDE
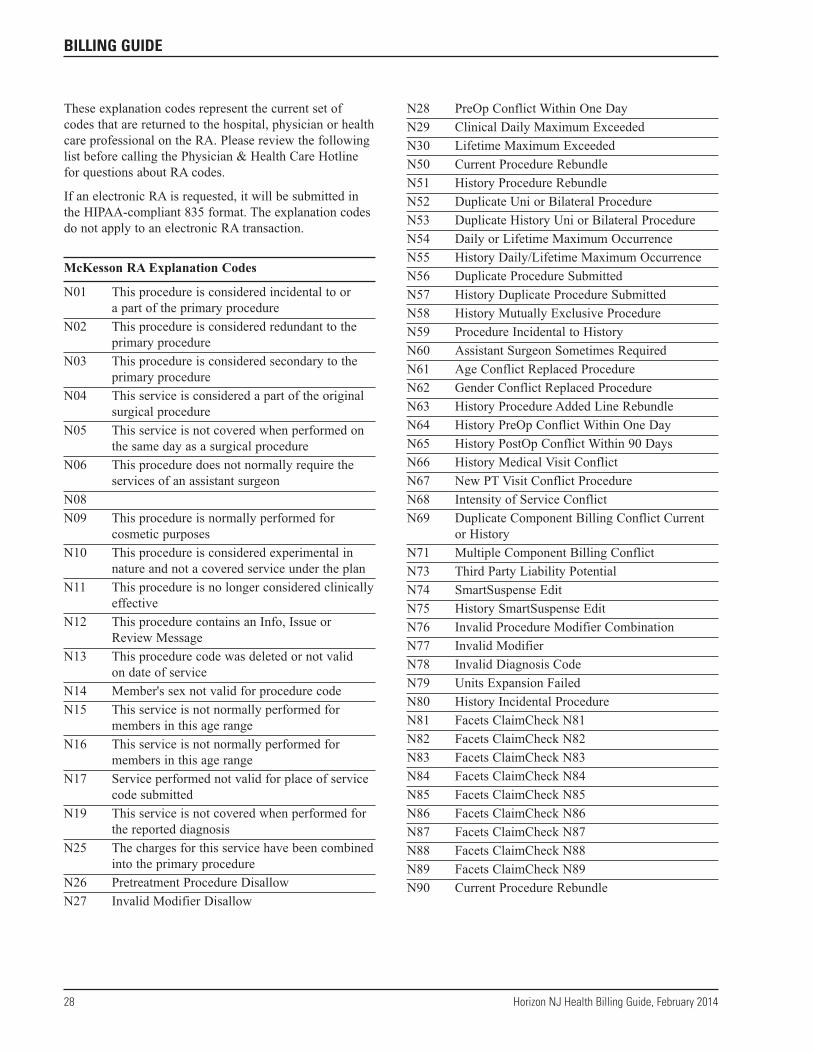
These explanation codes represent the current set ofcodes that are returned to the hospital, physician or healthcare professional on the RA. Please review the followinglist before calling the Physician & Health Care Hotlinefor questions about RA codes.
If an electronic RA is requested, it will be submitted inthe HIPAA-compliant 835 format. The explanation codesdo not apply to an electronic RA transaction.
McKesson RA Explanation Codes
N01 This procedure is considered incidental to or a part of the primary procedure
N02 This procedure is considered redundant to theprimary procedure
N03 This procedure is considered secondary to theprimary procedure
N04 This service is considered a part of the originalsurgical procedure
N05 This service is not covered when performed onthe same day as a surgical procedure
N06 This procedure does not normally require theservices of an assistant surgeon
N08N09 This procedure is normally performed for
cosmetic purposesN10 This procedure is considered experimental in
nature and not a covered service under the planN11 This procedure is no longer considered clinically
effectiveN12 This procedure contains an Info, Issue or
Review MessageN13 This procedure code was deleted or not valid
on date of serviceN14 Member's sex not valid for procedure codeN15 This service is not normally performed for
members in this age rangeN16 This service is not normally performed for
members in this age rangeN17 Service performed not valid for place of service
code submittedN19 This service is not covered when performed for
the reported diagnosisN25 The charges for this service have been combined
into the primary procedureN26 Pretreatment Procedure DisallowN27 Invalid Modifier Disallow
N28 PreOp Conflict Within One DayN29 Clinical Daily Maximum ExceededN30 Lifetime Maximum ExceededN50 Current Procedure RebundleN51 History Procedure RebundleN52 Duplicate Uni or Bilateral ProcedureN53 Duplicate History Uni or Bilateral ProcedureN54 Daily or Lifetime Maximum OccurrenceN55 History Daily/Lifetime Maximum OccurrenceN56 Duplicate Procedure SubmittedN57 History Duplicate Procedure SubmittedN58 History Mutually Exclusive ProcedureN59 Procedure Incidental to HistoryN60 Assistant Surgeon Sometimes RequiredN61 Age Conflict Replaced ProcedureN62 Gender Conflict Replaced ProcedureN63 History Procedure Added Line RebundleN64 History PreOp Conflict Within One DayN65 History PostOp Conflict Within 90 DaysN66 History Medical Visit ConflictN67 New PT Visit Conflict ProcedureN68 Intensity of Service ConflictN69 Duplicate Component Billing Conflict Current
or HistoryN71 Multiple Component Billing ConflictN73 Third Party Liability PotentialN74 SmartSuspense EditN75 History SmartSuspense EditN76 Invalid Procedure Modifier CombinationN77 Invalid ModifierN78 Invalid Diagnosis CodeN79 Units Expansion FailedN80 History Incidental ProcedureN81 Facets ClaimCheck N81N82 Facets ClaimCheck N82N83 Facets ClaimCheck N83N84 Facets ClaimCheck N84N85 Facets ClaimCheck N85N86 Facets ClaimCheck N86N87 Facets ClaimCheck N87N88 Facets ClaimCheck N88N89 Facets ClaimCheck N89N90 Current Procedure Rebundle
28 Horizon NJ Health Billing Guide, February 2014
BILLING GUIDE

N91 CCI Incidental ProcedureN92 History CCI Incidental ProcedureN93 CCI Mutually Exclusive ProcedureN94 History CCI Mutually Exclusive ProcedureN95 Assistant at Surgery ProcedureN96 McKesson User Defined DisallowNPPa01 Invalid number of units for site-specific
modifiersa02 Incorrect billing days/units mismatchedb01 Modifier/procedure code combination exceptionc01 Add-on procedure code billed without basec02 Billed procedure was billed with a more
comprehensive servicec03 Billed procedure does not match the member's agec04 This procedure has a limit of once per lifetime
and was previously paid for this memberc05 Procedure not valid for gender and/or diagnosis
10.0 LabCorp Billing
The following CPTs are not available through LabCorp.These procedures are to be completed at a hospital or clinicalsetting and billed accordingly. (Tests marked with an asterisk(*) are not performed in hospitals and require priorauthorization.) More information on LabCorp services may be received from LabCorp Customer Service.
LabCorp Customer Service1-800-631-5250
CPTs Not Performed by LabCorp
CPT 12 LCA Short Name
80103 Drug Prep, Tissue81007 UA; bacteriuria screen81020 UA; two or three glass test81099 Unlisted urinalysis procedure*81208 BCR/ABL 1 (t(9;22)) (eg, chronic myelogenous
leukemia) translocation analysis; otherbreakpoint, qualitative or quantitative
*81211 BRCA1, BRCA2 (breast cancer 1 and 2) (eg, hereditary breast and ovarian cancer) geneanalysis; full sequence analysis and commonduplication/deletion variants in BRCA1 (ie, exon13 del 3.835kb, exon 13 dup 6kb, exon 14-20 del26kb, exon 22 del 510bp, exon 8-9 del 7.1kb)
*81212 BRCA1, BRCA2 (breast cancer 1 and 2) (eg, hereditary breast and ovarian cancer) gene analysis; 185delAG, 5385 insC, 6174 delTvariants
*81213 BRCA1, BRCA2 (breast cancer 1 and 2) (eg, hereditary breast and ovarian cancer) gene analysis; uncommon duplication/deletionvariants
*81214 BRCA1, (breast cancer 1 ) (eg, hereditary breastand ovarian cancer) gene analysis; full sequenceanalysis and common duplication/deletionvariants (ie, exon 13 del 3.835kb, exon 13 dup6kb, exon 14-20 del 26kb, exon 22 del 510bp,exon 8-9 del 7.1kb)
*81215 BRCA1, (breast cancer 1) (eg, hereditary breastand ovarian cancer) gene analysis; knownfamilial variant
*81216 BRCA2 (breast cancer 2) (eg, hereditary breastand ovarian cancer) gene analysis; full sequenceanalysis
*81217 BRCA2 (breast cancer 2) (eg, hereditary breastand ovarian cancer) gene analysis; knownfamilial variant
*81228 Cytogenomic constitutional (genome-wide)microarray analysis; interrogation of genomicregions for copy number variants (eg, BacterialArtificial Chromosome [BAC] or oligo-basedcomparative genomic hybridization [CGH]microarray analysis)
*81268 Chimerism (engraftment) analysis, posttransplantation specimen (eg, hematopoieticstem cell), includes comparison to previouslyperformed baseline analyses; with cell selection(eg, CD3, CD33), each cell type
*81280 Long QT syndrome gene analysis (eg, KCNQ1,KCNH2, SCN5A, KCNE1, KCNE2, KCNJ2,CACNA1C, CAV3, SCN4B, AKAP, SNTA1,AND ANK2); full sequence analysis
*81281 Long QT syndrome gene analysis (eg, KCNQ1,KCNH2, SCN5A, KCNE1, KCNE2, KCNJ2,CACNA1C, CAV3, SCN4B, AKAP, SNTA1,AND ANK2); known familial sequence variant
*81282 Long QT syndrome gene analysis (eg, KCNQ1,KCNH2, SCN5A, KCNE1, KCNE2, KCNJ2,CACNA1C, CAV3, SCN4B, AKAP, SNTA1,AND ANK2); duplication/deletion variants
*81294 MLH1 (mutS homolog 1, colon cancer,nonpolyposis type 2) (eg, hereditary nonpolyposiscolorectal cancer, Lynch syndrome) gene analysis;duplication/deletion variants
Horizon NJ Health Billing Guide, February 2014 29
BILLING GUIDE

*81297 MLH2 (mutS homolog 1, colon cancer,nonpolyposis type 1) (eg, hereditarynonpolyposis colorectal cancer, Lynchsyndrome) gene analysis; duplication/deletionvariants
*81300 MSH6 (mutS homolog 6 [E. coli]) (eg, hereditary nonpolyposis colorectal cancer, Lynch syndrome) gene analysis;duplication/deletion variants
*81303 MECP2 (methyl CpG binding protein 2) (eg, Rett syndrome) gene analysis; knownfamilial variant
*81316 PML/RARalpha, (t(15;17)), promyelocyticleukemia/ retinoic acid receptor alpha) (eg, promyelocytic leukemia translocationanalysis; single breakpoint (eg, intron 3, intron 6or exon 6), qualitative or quantitative
*81319 PMS2 (postmeiotic segregation increased 2 [S. cerevisiae]) (eg, hereditary nonpolyposiscolorectal cancer, Lynch syndrome) geneanalysis; duplication/deletion variants
81370 HLA Class I and II typing, low resolution (eg, antigen equivalents); HLA-A, -B, -C,-DRB1/3/4/5, and -DQB1
81371 HLA Class I and II typing, low resolution (eg, antigen equivalents); HLA-A, -B, and-DRB1/3/4/5, (eg, verification typing)
81375 HLA Class II typing, low resolution (eg, antigenequivalents); HLA-DRB1/3/4/5 and -DQB1
81378 HLA Class I and II typing, high resolution (ie, alleles or allelle groups), HLA-A, -B, -C and-DRB1
81379 HLA Class I typing, high resolution (ie, allelesor allele groups); complete (ie, HLA-A, -B and -C)
82075 Alcohol, Breath82286 Bradykinin82307 Calciferon (Vitamin D)82376 Carbon dioxide, (carboxyhemoglobin);
qualitative*82485 Chondroitin B sulfate, quantitative82646 Dihydrocodeinone82666 Epiandrosterone82805 Blood Gas+Anal+O2 sat82810 Blood Gas,O2 sat82820 Hemoglobin Sat82930 Gastric acid analysis, includes pH if performed,
each specimen
83987 pH; exhaled breath condensate82953 Glucose; tolbutamide tolerance test82979 Glutathione reductase, RBC83008 Guanosine monophosphate (GMP), cyclic83055 Hemoglobin; sulfhemoglobin, qualitative83065 Hemoglobin; thermolabile83570 Isocitric dehydrogenase (IDH)83775 Malate dehydrogenase83861 Microfluidic analysis utilizing an integrated
collection and analysis device, tear osmolarity84061 Phosphatase, acid; forensic examination84704 Gonadotropin, chorionic (hCG); free beta chain84830 Ovulation tests85348 Coagulation time; Lee and White, other methods85530 Heparin-protamine tolerance test85547 Mechanical fragility, RBC85675 Thrombin time; titer86077 Path Review, Crossmatch86078 Path Review, Transfuse Rx 86079 Path Review, BldBank Authorization w/written
report86155 Chemotaxis assay, specify method86185 Counterimmunoelectrophoresis, each antigen86310 Heterophile antibodies; titers after absorption
with beef cells and guinea pig kidney86327 Immunoelectrophoresis; crossed (2-dimensional
assay)86386 Nuclear Matrix Protein 22 (NMP22) qualitative86378 Migration inhibitory factor test (MIF)86481 Tuberculosis test, cell mediated immunity
antigen response measurement; enumeration of gamma interferon-producing T-cells in cellsuspension
86485 Candida Test, Skin86486 Skin test; unlisted antigen, each86490 Cocci Test, Skin86510 Histo Test, Skin86580 Skin test; TB Test, Intradermal86732 Antibody; mucomycosis86744 Antibody; Nocardia86759 Antibody; rotavirus86805 Lymphocytox + Titration86806 Lymphocytox without Titration86825 HLA crossmatch; first serum sample or dilution86826 HLA crossmatch; additional
30 Horizon NJ Health Billing Guide, February 2014
BILLING GUIDE
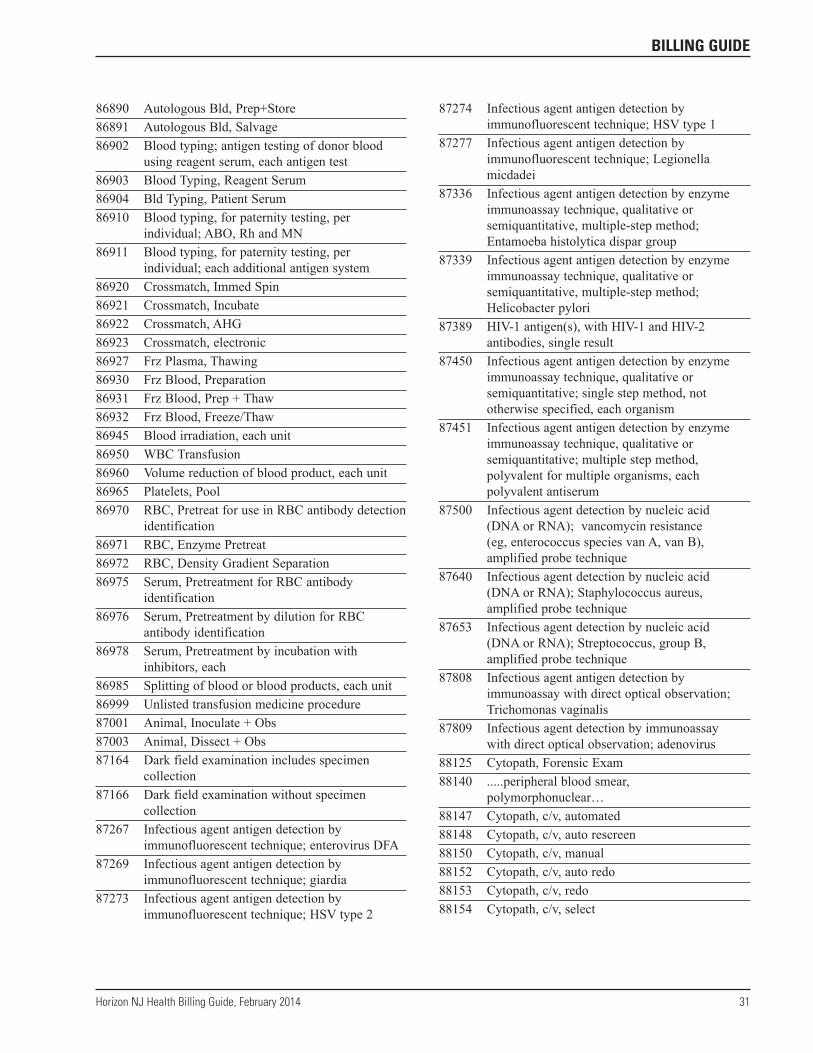
86890 Autologous Bld, Prep+Store86891 Autologous Bld, Salvage86902 Blood typing; antigen testing of donor blood
using reagent serum, each antigen test86903 Blood Typing, Reagent Serum86904 Bld Typing, Patient Serum86910 Blood typing, for paternity testing, per
individual; ABO, Rh and MN86911 Blood typing, for paternity testing, per
individual; each additional antigen system86920 Crossmatch, Immed Spin86921 Crossmatch, Incubate86922 Crossmatch, AHG86923 Crossmatch, electronic86927 Frz Plasma, Thawing86930 Frz Blood, Preparation86931 Frz Blood, Prep + Thaw86932 Frz Blood, Freeze/Thaw86945 Blood irradiation, each unit86950 WBC Transfusion86960 Volume reduction of blood product, each unit86965 Platelets, Pool86970 RBC, Pretreat for use in RBC antibody detection
identification86971 RBC, Enzyme Pretreat86972 RBC, Density Gradient Separation86975 Serum, Pretreatment for RBC antibody
identification86976 Serum, Pretreatment by dilution for RBC
antibody identification86978 Serum, Pretreatment by incubation with
inhibitors, each86985 Splitting of blood or blood products, each unit86999 Unlisted transfusion medicine procedure87001 Animal, Inoculate + Obs87003 Animal, Dissect + Obs87164 Dark field examination includes specimen
collection87166 Dark field examination without specimen
collection87267 Infectious agent antigen detection by
immunofluorescent technique; enterovirus DFA87269 Infectious agent antigen detection by
immunofluorescent technique; giardia87273 Infectious agent antigen detection by
immunofluorescent technique; HSV type 2
87274 Infectious agent antigen detection byimmunofluorescent technique; HSV type 1
87277 Infectious agent antigen detection byimmunofluorescent technique; Legionellamicdadei
87336 Infectious agent antigen detection by enzymeimmunoassay technique, qualitative orsemiquantitative, multiple-step method;Entamoeba histolytica dispar group
87339 Infectious agent antigen detection by enzymeimmunoassay technique, qualitative orsemiquantitative, multiple-step method;Helicobacter pylori
87389 HIV-1 antigen(s), with HIV-1 and HIV-2antibodies, single result
87450 Infectious agent antigen detection by enzymeimmunoassay technique, qualitative orsemiquantitative; single step method, nototherwise specified, each organism
87451 Infectious agent antigen detection by enzymeimmunoassay technique, qualitative orsemiquantitative; multiple step method,polyvalent for multiple organisms, eachpolyvalent antiserum
87500 Infectious agent detection by nucleic acid (DNA or RNA); vancomycin resistance (eg, enterococcus species van A, van B),amplified probe technique
87640 Infectious agent detection by nucleic acid (DNA or RNA); Staphylococcus aureus,amplified probe technique
87653 Infectious agent detection by nucleic acid (DNA or RNA); Streptococcus, group B,amplified probe technique
87808 Infectious agent antigen detection byimmunoassay with direct optical observation;Trichomonas vaginalis
87809 Infectious agent detection by immunoassay with direct optical observation; adenovirus
88125 Cytopath, Forensic Exam88140 .....peripheral blood smear,
polymorphonuclear…88147 Cytopath, c/v, automated88148 Cytopath, c/v, auto rescreen88150 Cytopath, c/v, manual88152 Cytopath, c/v, auto redo88153 Cytopath, c/v, redo88154 Cytopath, c/v, select
Horizon NJ Health Billing Guide, February 2014 31
BILLING GUIDE
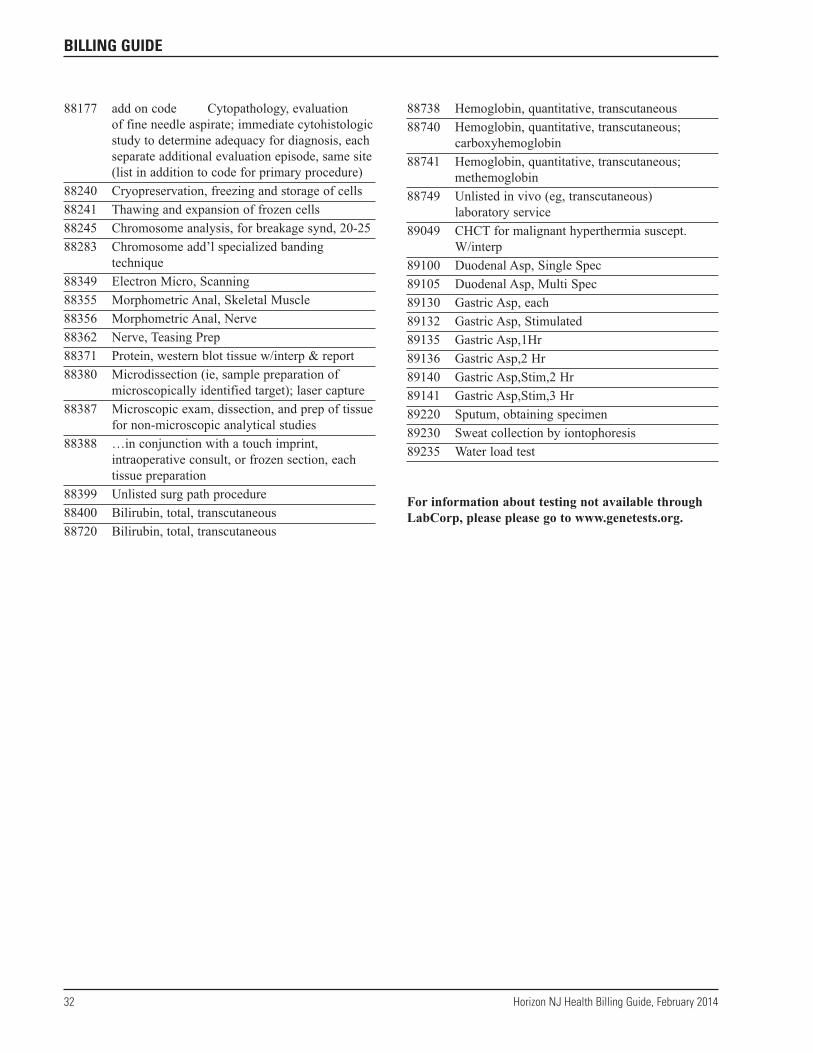
88177 add on code Cytopathology, evaluation of fine needle aspirate; immediate cytohistologicstudy to determine adequacy for diagnosis, eachseparate additional evaluation episode, same site(list in addition to code for primary procedure)
88240 Cryopreservation, freezing and storage of cells88241 Thawing and expansion of frozen cells88245 Chromosome analysis, for breakage synd, 20-2588283 Chromosome add’l specialized banding
technique88349 Electron Micro, Scanning88355 Morphometric Anal, Skeletal Muscle88356 Morphometric Anal, Nerve88362 Nerve, Teasing Prep88371 Protein, western blot tissue w/interp & report88380 Microdissection (ie, sample preparation of
microscopically identified target); laser capture88387 Microscopic exam, dissection, and prep of tissue
for non-microscopic analytical studies88388 …in conjunction with a touch imprint,
intraoperative consult, or frozen section, eachtissue preparation
88399 Unlisted surg path procedure88400 Bilirubin, total, transcutaneous88720 Bilirubin, total, transcutaneous
88738 Hemoglobin, quantitative, transcutaneous88740 Hemoglobin, quantitative, transcutaneous;
carboxyhemoglobin88741 Hemoglobin, quantitative, transcutaneous;
methemoglobin88749 Unlisted in vivo (eg, transcutaneous)
laboratory service89049 CHCT for malignant hyperthermia suscept.
W/interp89100 Duodenal Asp, Single Spec89105 Duodenal Asp, Multi Spec89130 Gastric Asp, each89132 Gastric Asp, Stimulated89135 Gastric Asp,1Hr89136 Gastric Asp,2 Hr89140 Gastric Asp,Stim,2 Hr89141 Gastric Asp,Stim,3 Hr89220 Sputum, obtaining specimen89230 Sweat collection by iontophoresis89235 Water load test
For information about testing not available throughLabCorp, please please go to www.genetests.org.
32 Horizon NJ Health Billing Guide, February 2014
BILLING GUIDE


















