BIC Presentation by Laura Coco
37
Binaural Interaction Component of the ABR in Veterans with Type 2 Diabetes Laura Coco, B.A. 1,2 , Marilyn Dille, Ph.D. 2 , Garnett P. McMillan, Ph.D. 2 , Dawn Konrad-Martin, Ph.D. 2 (1) University of Texas at Austin, Austin TX (2) National Center for Rehabilitative Auditory Research, Portland VA Medical Center, Portland OR
description
The Binaural Interaction Component of the ABR in Veterans with Type II Diabetes
Transcript of BIC Presentation by Laura Coco
PowerPoint Presentation
Binaural Interaction Component of the ABR in Veterans with Type 2 DiabetesLaura Coco, B.A.1,2, Marilyn Dille, Ph.D.2, Garnett P. McMillan, Ph.D.2, Dawn Konrad-Martin, Ph.D. 2(1) University of Texas at Austin, Austin TX (2) National Center for Rehabilitative Auditory Research, Portland VA Medical Center, Portland OR
1Type 2 Diabetes Mellitus (DM) affects >8% of population
Complications retinopathynephropathynumbnessataxia
IntroductionWHO, 2010; Austin et al 2009; Vaughn et al 2006; Miller et al 2004Its estimated that 25.8 million Americans have diabetes, thats more than 8% of the population, its been reported that the among VA population, diabetes is up to 3x more prevalent than the national averageestimating about 30% of all veterans have the disease.Its also estimated that total health care and related costs run about 170 billion dollars a year. this includes hospitalization, medical care, time off from work, and premature death.
Diabetes is a metabolic disease, which means it has to do with the way our body processes the food we eat.
Most of what we eat is broken down into glucose, which is a form of sugar in the blood, and is the primary source of fuel for our bodies.
The glucose enters our bloodstream, and our cells use it for energy and growth. Before our cells can use the glucose, a hormone called Insulin must be present for our cells to take in the glucose.
Diabetics have an inability to regulate the exact amount of insulin, or have developed a resistance to the insulin needed to move the glucose thats in our blood, to our cells so they can be used as fuel.
Type II DM results from an overabundance of glucose in the bloodstream that swamps the ability of the insulin-producing pancreas to regulate a steady stream to the cells.
Common diabetic microvascular complications affect the eyes (retinopathy) and the kidneys (nephropathy).
Neural complications include peripheral sensorimotor injury leading to numbness, neuropathic pain, ataxia and neuropathic ulcers.
2Type 2 Diabetes Mellitus (DM) affects >8% of population
Complications
Hearing Loss and DMPeripheral (Diaz de Leon-Morales et al., 2005; Frisina et al., 2006; Vaughn et al., 2006; Bainbridge et al., 2008; Austin et al., 2009; Cheng et al., 2009; Mitchell et al., 2009; Bainbridge et al., 2011; Bamanie and Al-Noury, 2011; Lerman-Garber et al., 2012)
Introduction
Bainbridge 20083. individ w DM have an increased risk of impaired hearing. numerous studies have demonstrated DMs effect on the peripheral hearing system, or at a cochlear level.
The cochlea relies on a consistent healthy blood supply to function. Disruptions in blood supply cause thickening of membranes and cell walls and loss of hair cells that lead to impaired peripheral auditory function 3This slide has too many words now...use bullets.Type 2 Diabetes Mellitus (DM) affects >8% of population
Complications
Hearing Loss and DMPeripheral (Bainbridge et al. 2008; Dalton et al. 1998; Agrawal et al. 2009; Cullen & Cinnamond 1993; Lisowska et al. 2001, Frisina et al. 2006; Vaughan et al. 2007; Austin et al. 2009)
Central (Parving et al., 1990; Bayazit et al., 2000; Durmus et al., 2004; Diaz de Leon-Morales et al., 2005; Vaughn et al., 2007; Konrad-Martin et al., 2010) Introduction
In addition to peripheral complications, diabetics have also shown to have an central component: central hearing loss refers to dysfunction in the auditory pathway that is post inner ear, its in the brain.
The brain is vulnerable to both metabolic and circulatory problems. The oxidative stress of prolonged hyperglycemia induces neuroinflammation, neuro-de-generation and changes in neurochemistry that could each contribute to abnormal central auditory processing.
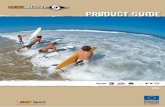
This graph shows the central impairment at each of the main areas we measure along the central auditory pathway. Its showing only diabetic patients, and the larger bar on the graph represents the biggest difference between DM and controls without DM. Here they are separated by severity but what I want us to focus on is that there is a difference, or an impairment, among diabetics a nearly every level of the central auditory pathway. This translates to reduced efficiency of neural conduction in diabetics.
At least one study has shown the central loss to be independent of peripheral loss. We wanted to investigate that further because a central hearing loss has to do with what we do with what we hear, or how we process auditory information. Its no use to hear the sound peripherally if we cant process it centrally.
4This slide has too many words now...use bullets.Type 2 Diabetes Mellitus (DM) affects >8% of population
Complications
Hearing Loss and DMPeripheral (Bainbridge et al. 2008; Dalton et al. 1998; Agrawal et al. 2009; Cullen & Cinnamond 1993; Lisowska et al. 2001, Frisina et al. 2006; Vaughan et al. 2007; Austin et al. 2009)
Central (Diaz de Leon-Morales et al 2005; Vaughan et al 2007; Bayazit et al 2000; Konrad-Martin et al 2010) Introduction
Konrad-Martin et al 2010
This graph shows the central impairment at each of the main areas we measure along the central auditory pathway. Its showing only diabetic patients, and the larger bar on the graph represents the biggest difference between DM and controls without DM. Here they are separated by severity but what I want us to focus on is that there is a difference, or an impairment, among diabetics a nearly every level of the central auditory pathway. This translates to reduced efficiency of neural conduction in diabetics.
At least one study has shown the central loss is present even in the absence of peripheral loss. We wanted to investigate that further because a central hearing loss has to do with what we do with what we hear, or how we process auditory information. Its no use to hear the sound peripherally if we cant process it centrally.
5This slide has too many words now...use bullets.Poor performance on speech in noise tasks
Diabetes and Hearing Frisina et al 2006
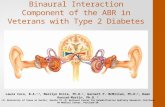
To expand on the diabetic central auditory impairment, theres also evidence to believe diabetics have a more difficult time understanding speech in noise. In one study, older diabetics were age matched with controls and a test was administered that evaluated their ability to process speech in the presence of noise. They were given a series of sentences measured in quiet and when the challenge of background noise from different spatial locations is added.
Their performance in these conditions is evaluated as a S/N threshold. The more negative, the better their ability to understand speech in background noise.
Normally subjects are able to perform better (more negative SNR) when the noise and speech come from different spatial locations. (best when noise is at left ear)
Diabetics threshold was poorer than controls in quiet, but the task became significantly more difficult for diabetics than controls when speech and noise were separated.
Noise added to speech challenges not only the peripheral system, but also the binaural neural networks of the auditory brainstem used to distinguish sounds at different spatial locations.
Extra stuff:Speech was presented at 0 azimuth in quiet (Q) and in each of the following three noise conditions (1) in 65 dBA of noise located at 0 azimuth 90 azimuth and at 270 azimuth The DM groups average threshold of speech understanding under noisy conditionsincreased by 1.6 at 0, 1.9 at 90 degrees, and 2.5 dB at 270). Although these threshold differences appear small, each decibel improvement in S/N threshold represents a critical increase in speech recognition of up to 20% (Frisina and Frisina, 1997).
They hypothesized that as one develops presbycusis, the right ear advantage is lost, and this decline is accelerated by diabetes. They attribute the acceleration to consequences of elevated blood sugar levels that cause, among other things, oxidative stress.6
Sound localizationSeparating noise from speechLoudness summationRedundancy/ComparisonSquelchBinaural HearingIf diabetics have more difficulty hearing in noise, that leads us to think there might be some binaural hearing deficit so a little background about why we care so much about binaural hearing, or, why do we have 2 ears?
Hearing equally from both ears gives us many perceptual benefits including Sound localization: we make comparisons based on when the sound arrives at each ear to help us localize the sound, can help you focus your attention to the targetSeparating noise from speech: When sound and noise are separated in space, theres an SNR advantage at one ear relative to the other. The head acts as an acoustical barrier producing a level and time difference between the ears. this is known as a head shadow effectLoudness summation: listening with two ears gives us an increased perception of loudness. Up to 10dB. Binaural redundancy and comparison: the advantage given to listners when they receive identical information about the signal. If the input signal is less than ideal, having two references aids in teasing out the desired auditory signal from the noise, and reduces the effort needed to do so. Binaural squelch: (focusing on one talker in an environment w many talkers) or the cocktail party effect. its considered an activity of nuclei of the brainstem processing timing, amplitude, and spectral differences between the two ears to allow us to attend to a talker while the brain suppresses the other signals.
Impaired populationsElderlyMultiple SclerosisCAPDhearing impaired
people with impaired binaural hearing have difficulty hearing in noise, localizing sounds, so as you can imagine this impacts quality of life
7How do we evaluate binaural hearing?Behavioral tests: SSI, HINT, SPIN, WIN, DDT, MLD, SCAN
Electrophysiological tests: N1P2 speech in noise
Binaural HearingFirst, evaluation of binaural hearing is not part of the main audiological battery of testing. its performed in cases of suspected auditory processing disorder, typically.
Most tests of central function and specifically binaural hearing are behavioral, which means they require some degree of cooperation, motivation and cognitive function. some, like the SCAN, are not normed for very old or very young populations, and cannot be used in hearing impaired populations.
A benefit to electrophysiological testing is that they dont depend on cognitive load.
EXTRA STUFF: behavioral: words in noise, dichotic digits, masking level difference. some of these are influenced by memory, cognitive skill, attentionWIN: word recognition in multitalker babble across a range of SNRsNU6 words presented at 7SNRs. babble level is fixed. and word level varies. words presented to LE, RE and binaurally.
DDT: objective: electrophysiological is the bic**MLD: tone bursts varying SNR
AEPs reflect the synchronized neural activity from neurons activated by the evoking stimuli. t occurs within a 10 ms time window after stimulus onset and is typically characterized by a series of five to seven vertex positive peaks that are labeled with I through VII. 8
Binaural HearingInputs from each ear travel up ipsilateral and contralateral brainstem pathways where the 2 inputs are compared and processed at various nuclei before reaching the auditory cortex.Binaural processing is introduced at the level of the superior olivary. SOC processes and integrates binaural information in the form of ITD (LSO) and ILD (MSO) ITDs and ILDs are then combined in the IC
Outputs go to the dorsal nucleus of the lateral lemniscus and the IC
9
Binaural Hearing
The auditory brainstem response is an auditory evoked potential extracted from electrical activity in the brain. Its recorded by surface electrodes on the scalp and in the ear canal.
The recording is a series of waves that occur in the first 10ms after a stimulus is presented.
When interpreting the abr we are interested in these waves that are numbered here, from which we measure amplitude and latency.
10
Binaural HearingWave I/II Wave III Wave V
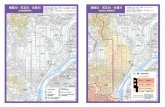
Each wave represents activity happening at a general location in the central auditory pathway. This image is showing you a simplified version of the location in the brainstem that is the main contribution to each of the waves.
If we want to study binaural interaction, wave V is a good place to look since its the most reliable largest wave in this sequence of waves, occurring after binaural integration takes place.
EXTRA STUFF: The first point at which binaural crossover happens is wave III, there are bics further up, mlr and llr. 11Normal: (L+R) > BINBinaural Interaction ComponentThe difference between the sum of the two Monaural ABRs and the Binaural ABR
Fowler & Broadard 1988LeftRightBinaural (BIN)Left + RightWhen we collect the ABR, we typically do three traces, a left ear a right ear and then both ears at the same time, or binaural
From these 3 waveforms we can measure a binaural interaction component, which is considered the difference between the sum of the 2 monaurals (L+R) and the binaural ABR.
In a normal system, youll see that the L+R, what we will now call monaural aggregate, is consistently larger than the binaural response. If the left and right ear were just additive, wed see that they would equal binaural. But the auditory system isnt that simple. The binaural response is consistently smaller in amplitude at the wave V latency window. 12
Binaural Interaction ComponentThe difference between the sum of the two Monaural ABRs and the Binaural ABRAbnormal: (L+R) = BIN
Neural disorders
CAPD
animal model with intentional lesion
1. Fowler 20022. Delb 2003; Gopal & Pierel 19993. Wada & Starr 1989; Gardi & Berlin 1981abnormalnormalL + RBINI II III IV VI II III IV VAn abnormal BIC means the binaural and the monaural aggregates are closer to identical.
We might think some neural disorders that effect binaural hearing would demonstrate an abnormal bic and in fact Folwer has demonstrated this in animal model.
More than one study has linked a gold standard CAPD test to reduced BIC in children (scan)
Intentional lesion: Animal model shows us the BIC is occurring at the same level as ABR wave IV-V implicating SOC and lateral lemniscus auditory pathwaysGuinea pig: Section of fibers of trapezoid body Complete unilateral lesion of SOC Transection of LL bilaterally
13Binaural Interaction ComponentDisappears at ILD >16dB and ITD> 1.6msecBehavioral tests show that Binaural Interaction disappears when signal is no longer intracranially fused Furst 1985, McPherson & Starr 1995The BIC correlates well with psychophysical measures of binaural processes
The BIC correlates well with gross psychophysical measures of binaural processes
BIC is only present if the two stimuli are intracranially fused14Binaural Interaction ComponentHow to measureDifference Waveform
BIC Amplitude
BIC RatioThree standard estimators of Binaural Interaction:
15Difference WaveformControlAbnormal
Binaural Interaction ComponentHow to measureFowler 19886.17-7.5msecAmplitude ratio 16%Amplitude: .43mV (.15)
The bottom right has Multiple SclerosisNo B-wave
16Binaural Interaction ComponentHow to measureBIC Amplitude = Monaural Aggregate Binaural response Values closer to zero indicate smaller Binaural Interaction.
Gopal et al 1998
Two standard estimators of Binaural Interaction: bic amplitude estimates BI as a constant difference between BIN and Monagg
By subtracting .91 from 1.32, we get .41, the difference between binaural and monaural aggregate.17Binaural Interaction ComponentBIC Ratio = Binaural response Monaural AggregateValues closer to one indicate smaller Binaural Interaction.
How to measureGopal et al 1998
Two standard estimators of Binaural Interaction: Binaural response is proportional to the monaural aggregate.
BIC ratio estimates BI as a slope of that relationship between BIN and Monagg.
18Research QuestionDo Veterans with DM have a decreased BIC of the ABR when compared to Veterans without the disease?
We hypothesized that perhaps they do have a decreased binaural interaction due to the nature of DMs effects on central auditory system and evidence that binaural hearing is impaired in diabetics.19 MethodsABR obtained and scored from 81 subjects As part of a larger Longitundal study on Diabetes and Hearing Loss
Subset of 47 subjects met inclusion criteria
Average age of controls was 44, average age of diabetics was 49, they were mostly male. we can also see that our exclusion criteria was stricta lot of people were kicked out. We did this
Inclusion Criteria:No more than .25ms difference in wave V latency between earsNo more than 10dB difference between ears at 2kHz, 3kHz or 4kHzDM Group: Type II DM onlyControl Group: not diagnosed with DM and HbA1c