
Bevacizumab Has Differential and Dose-Dependent Effects on … · zine). Craniectomy was done and...
15
Cancer Therapy: Preclinical See commentary by de Groot, p. 6109 Bevacizumab Has Differential and Dose-Dependent Effects on Glioma Blood Vessels and Tumor Cells Louisa von Baumgarten 1 , David Brucker 2 , Anca Tirniceru 3 , Yvonne Kienast 1,2 , Stefan Grau 4 , Steffen Burgold 2 , Jochen Herms 2 , and Frank Winkler 5 Abstract Purpose: Bevacizumab targets VEGF-A and has proved beneficial in glioma patients, improving clinical symptoms by the reduction of tumor edema. However, it remains controversial whether or not bevaci- zumab exerts antitumor effects in addition to (and potentially independent of) its effects on tumor vessels, and it is unknown what doses are needed to achieve this. Experimental Design: We established a novel orthotopic glioma mouse model that allowed us to simultaneously study the kinetics of the morphologic and functional vascular changes, tumor growth, and the viability of individual tumor cells during the course of anti-VEGF therapy in the same microscopic tumor region in real-time. Three doses of bevacizumab were compared, a subclinical dose and two clinical doses (medium and high). Results: Low (subclinical) doses of bevacizumab led to a significant reduction of the total vascular volume without affecting tumor cell viability or the overall tumor growth rates. Medium and high doses triggered a similar degree of vascular regression but significantly decreased tumor growth and prolonged survival. Remaining vessels revealed morphologic features of vascular normalization, reduced perme- ability, and an increase in blood flow velocity; the latter was dose dependent. We observed an uncoupling of the antitumoral and the antivascular effects of bevacizumab with the high dose only, which showed the potential to cause microregional glioma cell regression. In some tumor regions, pronounced glioma cell regression occurred even without vascular regression. In vitro, there was no effect of bevacizumab on glioma cell proliferation. Conclusions: Regression of glioma cells can occur independently from vascular regression, suggesting that high doses of bevacizumab have indirect anticancer cell properties in vivo. Clin Cancer Res; 17(19); 6192–205. Ó2011 AACR. Introduction Glioblastoma multiforme is an invariably fatal brain tumor accounting for approximately 40% of all primary malignant brain tumors. At present, the standard therapy is a multimodal regimen consisting of surgical resection combined with daily temozolomide and radiation, fol- lowed by 6 monthly cycles of temozolomide alone. Despite this treatment, the mean overall survival from time of diagnosis has been only moderately increased from 12.1 to 14.6 months in the selected study population (1). The development of novel, more effective strategies to treat malignant gliomas, therefore, remains an unmet medical need. Gliomas are highly vascularized tumors, and preclinical data have suggested that glioma growth critically depends on the generation of tumor-associated blood vessels (2). Among multiple factors controlling the complex process of angiogenesis, VEGF and its associated signaling cascade are considered of central importance (3). Glioma cells are a major source of VEGF, and high levels of VEGF generation have been reported to correlate with high-grade malig- nancy and poor prognosis (4, 5). Consequently, novel therapeutic strategies targeting VEGF or its downstream signaling pathways have yielded promising results as an addendum to standard therapy (6). Currently, the most prominent drug targeting VEGF is bevacizumab, a recombinant humanized monoclonal anti- body (mAb) that binds to human VEGF-A. Encouraging Authors' Affiliations: Departments of 1 Neurology and 2 Neuropathology, University Hospital, Ludwig-Maximilians University; 3 Deutsches Herzzen- trum, Technische Universit€ at, Munich; 4 Department of Neurosurgery, University Hospital, Cologne; and 5 Department of Neurooncology, Neu- rology Clinic and National Center for Tumor Disease, University Hospital Heidelberg, Heidelberg, Germany Note: Supplementary data for this article are available at Clinical Cancer Research Online (http://clincancerres.aacrjournals.org/). Corresponding Author: Frank Winkler, Department of Neurooncology, Neurology Clinic and National Center for Tumor Disease, University Hospital Heidelberg, Im Neuenheimer Feld 400, Heidelberg D-69120, Germany. Phone: 49-6221-56-7107; Fax: 49-6221-56-7554; E-mail: [email protected] doi: 10.1158/1078-0432.CCR-10-1868 Ó2011 American Association for Cancer Research. Clinical Cancer Research Clin Cancer Res; 17(19) October 1, 2011 6192 on August 28, 2021. © 2011 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from Published OnlineFirst July 25, 2011; DOI: 10.1158/1078-0432.CCR-10-1868
Transcript of Bevacizumab Has Differential and Dose-Dependent Effects on … · zine). Craniectomy was done and...

Cancer Therapy: PreclinicalSee commentary by de Groot, p. 6109
Bevacizumab Has Differential and Dose-Dependent Effectson Glioma Blood Vessels and Tumor Cells
Louisa von Baumgarten1, David Brucker2, Anca Tirniceru3, Yvonne Kienast1,2, Stefan Grau4,Steffen Burgold2, Jochen Herms2, and Frank Winkler5
AbstractPurpose: Bevacizumab targets VEGF-A and has proved beneficial in glioma patients, improving clinical
symptoms by the reduction of tumor edema. However, it remains controversial whether or not bevaci-
zumab exerts antitumor effects in addition to (and potentially independent of) its effects on tumor vessels,
and it is unknown what doses are needed to achieve this.
Experimental Design: We established a novel orthotopic glioma mouse model that allowed us to
simultaneously study the kinetics of the morphologic and functional vascular changes, tumor growth, and
the viability of individual tumor cells during the course of anti-VEGF therapy in the same microscopic
tumor region in real-time. Three doses of bevacizumab were compared, a subclinical dose and two clinical
doses (medium and high).
Results: Low (subclinical) doses of bevacizumab led to a significant reduction of the total vascular
volume without affecting tumor cell viability or the overall tumor growth rates. Medium and high doses
triggered a similar degree of vascular regression but significantly decreased tumor growth and prolonged
survival. Remaining vessels revealed morphologic features of vascular normalization, reduced perme-
ability, and an increase in blood flow velocity; the latter was dose dependent. We observed an uncoupling
of the antitumoral and the antivascular effects of bevacizumab with the high dose only, which showed the
potential to cause microregional glioma cell regression. In some tumor regions, pronounced glioma cell
regression occurred evenwithout vascular regression. In vitro, there was no effect of bevacizumab on glioma
cell proliferation.
Conclusions: Regression of glioma cells can occur independently from vascular regression, suggesting
that high doses of bevacizumab have indirect anticancer cell properties in vivo. Clin Cancer Res; 17(19);
6192–205. �2011 AACR.
Introduction
Glioblastoma multiforme is an invariably fatal braintumor accounting for approximately 40% of all primarymalignant brain tumors. At present, the standard therapy isa multimodal regimen consisting of surgical resectioncombined with daily temozolomide and radiation, fol-
lowed by 6monthly cycles of temozolomide alone. Despitethis treatment, the mean overall survival from time ofdiagnosis has been only moderately increased from 12.1to 14.6 months in the selected study population (1). Thedevelopment of novel, more effective strategies to treatmalignant gliomas, therefore, remains an unmet medicalneed.
Gliomas are highly vascularized tumors, and preclinicaldata have suggested that glioma growth critically dependson the generation of tumor-associated blood vessels (2).Among multiple factors controlling the complex process ofangiogenesis, VEGF and its associated signaling cascade areconsidered of central importance (3). Glioma cells are amajor source of VEGF, and high levels of VEGF generationhave been reported to correlate with high-grade malig-nancy and poor prognosis (4, 5). Consequently, noveltherapeutic strategies targeting VEGF or its downstreamsignaling pathways have yielded promising results as anaddendum to standard therapy (6).
Currently, the most prominent drug targeting VEGF isbevacizumab, a recombinant humanizedmonoclonal anti-body (mAb) that binds to human VEGF-A. Encouraging
Authors' Affiliations: Departments of 1Neurology and 2Neuropathology,University Hospital, Ludwig-Maximilians University; 3Deutsches Herzzen-trum, Technische Universit€at, Munich; 4Department of Neurosurgery,University Hospital, Cologne; and 5Department of Neurooncology, Neu-rology Clinic and National Center for Tumor Disease, University HospitalHeidelberg, Heidelberg, Germany
Note: Supplementary data for this article are available at Clinical CancerResearch Online (http://clincancerres.aacrjournals.org/).
Corresponding Author: Frank Winkler, Department of Neurooncology,Neurology Clinic and National Center for Tumor Disease, UniversityHospital Heidelberg, Im Neuenheimer Feld 400, Heidelberg D-69120,Germany. Phone: 49-6221-56-7107; Fax: 49-6221-56-7554; E-mail:[email protected]
doi: 10.1158/1078-0432.CCR-10-1868
�2011 American Association for Cancer Research.
ClinicalCancer
Research
Clin Cancer Res; 17(19) October 1, 20116192
on August 28, 2021. © 2011 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst July 25, 2011; DOI: 10.1158/1078-0432.CCR-10-1868

results have been obtained in patients with malignantgliomas treated with bevacizumab, when used in combina-tion with irinotecan (7) and as monotherapy (8). Becausethe progression-free and overall survival data from thephase II trials on recurrent glioblastomas, in which bev-acizumab was tested as a single agent (8–11), do not seemto differ much from the survival data obtained with com-binations of bevacizumab with chemotherapy (8, 12),bevacizumab monotherapy may gain further clinicalimportance in the future. Because the vast majority ofclinical studies showed high radiographic response rates,promising progression-free survival rates and a low overalltoxicity, bevacizumab was approved for therapy of recur-rent glioma by the U.S. Food and Drug Administration inMay 2009 (13).Although bevacizumab is most often used at a dose of
10 mg/kg every 2 weeks in glioblastoma, its optimal dosehas not been established yet (14). No sound data onbevacizumab dosing exists: bevacizumab has been givento glioblastoma patients with a dose of 15 mg/kg every3 weeks (7, 10), at 10 mg every 2 weeks (6, 9, 12), and at 5mg/kg every 2 weeks (15). A recent meta-analysis of phaseII studies for recurrent glioblastoma could not detect asignificant difference between the 5 and the 10 mg/kggroups (16). Still, the inherent limitation of this kind ofanalysis calls for a formal and prospective comparison ofthe doses. Outside the brain, there is at least one recentphase III study showing that bevacizumab 15 mg/kgevery 3 weeks is more efficient than 7.5 mg/kg in breastcancer (17), and one phase II study showing the same fornon–small cell lung carcinoma (18). However, thesedose–response relationships could not be recapitulatedfor other tumor types and, sometimes, seem to beeven reversed (19). Moreover, the question has been
raised whether targeted therapies might have a differentdose–response relationship (20, 21) than conventionalcytotoxic therapies, which show increasing efficacy athigher doses (22).
The mode of action of bevacizumab that accounts for itsclinical benefits is still not fully understood and might notbe attributed to one mechanism alone; even off-tumortargets have been suggested recently (23). Initially, preven-tion of tumor angiogenesis and subsequent starvation ofthe tumor from oxygen and nutrients was considered themajor mechanism of action of antiangiogenic therapy (24).However, preclinical studies suggested that antiangiogenictherapies induce vascular normalization, thereby improv-ing glioma oxygenation and subsequent response to radia-tion therapy (25). This could explain the positivesynergistic effects of VEGF-targeted therapies when usedin a multimodal approach (26). Normalization of tumor-associated vessels and reduction of peritumoral edemacould be shown for glioma patients receiving an anti-VEGFtyrosine kinase inhibitor (27). Finally, the results of arecent preclinical study suggest that the antiedema effectof anti-VEGF monotherapy is the major reason for itsclinical efficiency (28). Likewise, the clinical impressionthat malignant gliomas continue to grow diffusely in thebrain under bevacizumab therapy (29, 30) rose the ques-tion whether bevacizumab has any antitumor cell activitywhatsoever. Contrast-enhanced MRI imaging is used toassess the therapeutic response to anti–VEGF-A treatment,but its antiedema and antipermeability effects make itdifficult to assess its effects on tumor burden (31). Takentogether, the exact role of vascular normalization versusvascular regression, the existence of direct or indirect anti-tumor actions, and the optimum dose for each of theseeffects during anti-VEGF therapy are still unresolved butimportant questions (32).
In this study, we established a mouse glioma model thatmade it possible to assesshowvascular changesdynamicallyinteract with tumor cell proliferation or regression duringbevacizumab therapy. This allowed novel insights into therelevant modes of action and their dose dependencies.
Materials and Methods
Cell culture and gene transfection of cancer cellsThe human glioblastoma cell line U87MG was obtained
from the American type culture collection in 2006. Todetermine the influence of therapy on tumor cells in realtime, the red fluorescent protein (RFP) DsRed was stablytransfected into U87MG cells. Briefly, the plasmid pEGFP-C3 (Clontech Laboratories, Inc.) was cut by using enzymesEco47III and ScaI. For generation of DsRed under thecontrol of the CMV promoter, the HindIII/ApaI fragmentfrom pDsRed2 (Clontech Laboratories, Inc.), containingthe full-length DsRed2 cDNA, was inserted into the Hin-dIII/NotI site of pC3-cloning. The resulting construct wastransfected into cancer cells by using Lipofectamine. Clonesof cancer cells expressing DsRed were isolated, cultured inselective medium for 3 weeks, and subsequently sorted by
Translational Relevance
Controversy exists whether the clinical benefit ofpatients treated with bevacizumab results exclusivelyfrom its effect on tumor vessels or whether any addi-tional antitumor cell activity might contribute to itsclinical efficacy, and what doses are needed to achievethis. In glioblastoma, bevacizumab is most often used ata dose of 10mg/kg every 2 weeks, either as addendum tochemotherapy or as monotherapy; however, its optimaldose has not been established yet.This study shows that VEGF inhibition by bevacizu-
mab as a monotherapy induces normalization andregression of tumor vasculature in vivo, even at low(subclinical) doses, but has no antitumor effect by itself.Yet, higher doses (e.g., doses equivalent to 15 mg/kgevery 2 weeks in patients) lead to a relevant tumor cellregression in addition to the vascular actions of thedrug. Hence, despite increased costs and potential toxi-city, higher doses might be most efficient in monother-apeutic approaches.
Bevacizumab Effects on Gliomas In Vivo
www.aacrjournals.org Clin Cancer Res; 17(19) October 1, 2011 6193
on August 28, 2021. © 2011 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst July 25, 2011; DOI: 10.1158/1078-0432.CCR-10-1868

using fluorescence-activated cell sorting (FACS) Vantage(Becton Dickinson).
Animal modelCranial window preparation and stereotactic cortical
tumor cell injection was carried out as previously described(Winkler and colleagues, 2009). Briefly, 8- to 10-week-oldmale NMRI nu/nu nude mice (Charles River Laboratories)were anesthetized with an intraperitoneal (i.p.) injection ofketamine/xylazine (100 mg/kg ketamine/10 mg/kg xyla-zine). Craniectomy was done and the dura mater wasremoved. The brain surface was covered with physiologicsodium chloride solution and a custom-made round coverglass (6 mm diameter) was glued to the skull with dentalacrylic glue. Three weeks after cranial window preparation,the cover glass was removed, and 3 mL of a viscous suspen-sion containing 1 � 105 U87-RFP cells was injected stereo-tactically into the mouse brain by using a 10 mL Hamiltonmicrosyringe and a 2-pt style needle (Hamilton). Cells wereinjected 1 mm lateral to the sagittal sinus into a depth of1mm. All animal experiments were conducted according tothe Bavarian state regulations for animal experimentationand approved by the state authorities.
Application of bevacizumabBevacizumab (Avastin; Roche) was used to inhibit
tumor cell–derived human VEGF-A and was administeredi.p. at doses of 25, 5, and 0.5 mg/kg bodyweight (n ¼ 5per group) every second day for 12 days. A control group(n ¼ 5) with size-matched tumors received human poly-clonal immunoglobulin G (IgG; Intratect; Biotest) at adose of 25 mg/kg. To measure bevacizumab plasmaconcentrations, plasma samples from 3 to 4 animalsper treatment group were collected after the i.p. applica-tion of 2 and 8 subsequent doses every other day, with theplasma obtained 2 days after last application. The plasmaconcentration of bevacizumab was determined by usingan ELISA for the quantitative detection of human anti-bodies in animal plasma. Briefly, a biotinylated mAbagainst human Fcg was bound to a streptavidin-coatedmicrotiter plate in the first step. By incubating plasmasamples and reference standard, bevacizumab binds tothe immobilized mAb. The bound construct can bedetected by digoxigenylated mAb against human Fcg(mAb-Dig) followed by anti-Dig-horseradish peroxidase(HRP) antibody conjugate (FAb<Dig>-HRP). ABTS solu-tion is used as the substrate for HRP.
Measurement of overall tumor growthTumor growth was monitored by in vivo epifluorescence
microscopy, and as soon as the RFP signal reached adiameter of approximately 1.5 mm (range, 1.2–1.9 mm),usually around day 14 to 20 after single cell implantation,anti-VEGF treatment with bevacizumab was started. Thiswas designated as day 0. Tumor volume was calculated onthe basis of the following equation:
Tumor size (mm2) ¼ (long axis) � (short axis) � P
As shown by us and by others, this methods allows toapproximate overall tumor growth (25, 28).
Survival analysisFor the survival study, the stereotactic injection of
5 � 105 U87-RFP cells was carried out after drilling aborehole. Cells were injected 1 mm lateral to the sagittalsinus into a depth of 2 mm, no cranial window wasprepared. Treatment (n ¼ 6 animals per treatment group)was initiated 5 days after tumor implantation. Experimentswere terminated when mice became moribund or died.
Dynamic in vivo multiphoton laser scanningmicroscopy
A MaiTai Titanium Sapphire laser (690–1,040 nm, 14 Wpump laser; Newport Spectra Physics) equipped with a 2-photon microscope (LSM 5 MP; Zeiss) was used for in vivomultiphoton laser scanning microscopy (MPLSM). A cus-tom-made microscopy stage allowing for stereotactic fixa-tion of the cranium was used (Narishige). Mice wereanesthetized by a mixture of O2 and 1% isoflurane andbody temperature of mice was held constant by using aheating pad. Images were acquired at an excitation wave-length of 750 nm. Laser power was limited to a minimum,not exceeding 3% of total power at the surface, and 50% in350 mm depth. At this power, no phototoxic damage tobrain tissue was detectable over the time course of inves-tigations. For each tumor, 3 adjacent regions were imagedthrough the cranial window and 133 images spared 3microns apart were collected from the brain surface produ-cing 650 � 650 � 400 mm volume stacks with a resolutionof 0.64 � 0.64 � 3 mm per pixel. These regions wererevisited and recorded on day 3, 6, 9, and 12.
To make sure that corresponding tumor regions werefollowed up over time, we used 2 different strategies: (i)allmiceweremountedon a computerized stereotactic stage,allowing for relocation of identical regions in x, y, and zdimension. (ii) To compensate for minor shifts because oftumor growth and cerebral edema, landmark vessels of thenormal brain and the tumor were identified and used forproper alignment of the regions of interest. MPLSM angio-graphy of glioblastoma vessels was done after i.v. injectionof 100 mL of fluorescein isothiocyanate (FITC)-labeled dex-tran (10 mg/mL, 2 mol/L Da MW, green). In a group of 4animals the observation period was extended to 25 days.
Analysis of tumor vasculatureThree regions showing both tumor cells and tumor
blood vessels were randomly selected at day 0 for everytumor. The 2 regions that could be followed over time withthe best image quality were subjected to three-dimensional(3D) reconstruction of the tumor vessels as well as analysisof the vascular network by using Imaris 6.1 (BitplaneScientific Software). Briefly, 3D reconstructions of 100images representing the region from 0 to 300 mm underthe brain surface were created. In corresponding regions ofinterest (400 � 400 � 300 mm), a semiautomated quanti-fication of vascular parameters (number of branch points,
Baumgarten et al.
Clin Cancer Res; 17(19) October 1, 2011 Clinical Cancer Research6194
on August 28, 2021. © 2011 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst July 25, 2011; DOI: 10.1158/1078-0432.CCR-10-1868

number of vessel segments, vessel diameter, intravascularvolume, and vascular surface) was done for all time pointsby using the filament tracer function of the software.Briefly, a wizard-based interface guides the automatic crea-tion of a tree-like filament on the basis of local intensitycontrast. Tracking proceeds from start points to endpointsand a vectorized backbone of the vascular bed is proposed.In a last step, the radius at each point is defined accordingto the local contrast ridge (for representative images seeSupplementary Fig. S1).
Dynamic interdependence of blood vessels and tumorcellsFor the detailed analysis of regional tumor volume and
regional vascular volume, a random tumor region of 200�100� 33 mmwas chosen on day 9. According to its vascularbranching pattern, the exact corresponding region wasidentified for day 6 and day 0. Because of tumor growthin 3D, these regions were recovered at varying Z-levelsduring the observation period. The volume of FITC–dex-tran-labeled vessels and the total volume of RFP-expressingtumor cells was determined in identical tumor regions byusing Imaris 6.1 (Bitplane Scientific Software).
Red blood cell velocityThe motion of red blood cells (RBC) was inferred from
line-scan measurements as described previously (33).Briefly, repetitive line scans of typically 15 mm along thecentral axis of a vessel were done with a spatial resolution of0.23 mmper pixel, a pixel dwell time of 10.2 ms and a recordlength of 3 seconds (for representative images see Supple-mentary Fig. S2). In a depth between 100 and 150 mm fromthe brain surface, RBC velocity was determined in 12vessels in 3 corresponding tumor regions before the onsetand on day 6 of the treatment. In addition, in 4 animalsbearing a cranial window but no tumor, RBC velocitieswere measured 3 weeks after cranial window implantation.
Microregional vascular permeabilityVascular permeability to bovine serum albumin (BSA)
was determined after i.v. injection of 0.1 mL FITC–BSA(Invitrogen). Immediately after i.v. injection of BSA, Z stackimages of 100 mm with 3 mm intervals were collected in adepth of �75 to �175 mm from the surface in 2 adjacentareas of interest (650� 650� 100 mm) every 4 minutes for20 minutes. The increase in extravasated fluorescence dyeintensity measured by using Imaris 6.1 (Bitplane ScientificSoftware) and was normalized by blood vessel surface areaby using the equation as described previously (25, 34).
In vitro proliferation assayIn vitro cell proliferation was determined by using a cell
proliferation assay according to the manufacturer’s instruc-tions (CellTiter 96 AQueous nonradioactive cell prolifera-tion Assay; Promega). Briefly, cells were incubated withdifferent concentrations (5–1,000 ng/mL) of bevacizumabor control IgG in the samevolume for 48hours. After addingthe CellTiter reagent, absorbance was measured at 490 nm
by using an ELISA reader. Results are presented asmean of 4replicate measurements. To determine the growth kineticsof U87 and U87-RFP (Supplemental Fig. S1A), 104 cells perwell were seeded in the same volume and were allowed togrow for different time intervals (12 hours, 2, 4, 6, and 8days) under standard conditions. After adding the CellTiterreagent, absorbance was measured as described above.
Western blot analysisWestern blot analysis was carried out by using a standard
protocol. Briefly, 50 mg protein were electroblotted on apolyvinylidene difluoride membrane. VEGF was detectedby using a rabbit polyclonal antibody directed against theN-terminus of human VEGF-A (sc-152, 1:50; Santa Cruztechnologies) and a secondary, alkaline phosphatase-con-jugated goat–anti-rabbit antibody (D0487, 1:2,000;Dako). As a separate loading control, we used a mono-clonal mouse antibody directed against a-tubulin (T6199,1:2,200; Sigma Aldrich) and a secondary goat-anti mouseantibody conjugated to alkaline phosphatase (31320,1:2,000; Thermo Scientific). Quantification of the inte-grated gray values of the VEGF band and the a-tubulinband was done by using ImageJ software.
Quantification of the RFP signal in vitroTo determine whether a correlation exists between U87-
RFP cell numbers and the fluorescence intensity of the RFPsignal,we seededU87-RFP cells at different numbers in clear96-well plates (Biosearch). Cells were allowed to adhere for12 hours, afterwards fluorescence determinations weremade by using a fluorescence microplate reader and a565 excitation filter anda590-nmemission filter (FLUOStarOptima; BMG Technologies). In a second subset of experi-ments, 5,000 U87-RFP cells were incubated with differentconcentrations (5–1,000ng/mL)of bevacizumabor controlIgG in the same volume for 48 hours. Subsequently fluor-escence was determined as described above.
Correlation of cell death and RFP fluorescenceintensity
To determine whether a loss of RFP fluorescence corre-lates with cell death, U78-RFP cells growing under standardconditions were heated at 67�C for 10 minutes, irradiatedwith 130 Gy, or left untreated. Thirty-six hours later, U87-RFP cells were harvested and diluted in PBS. A total of 105
cells of each group were incubated for 10 minutes withSYTOX Blue Dead Cell Stain (# S34857, final concentration2 mmol/L; Molecular probes) according to the man-ufacture’s instruction. Sytox is a high affinity blue fluores-cing nucleic acid stain that penetrates cells withcompromised plasma membranes. Subsequently, FACSanalysis was done to determine red fluorescence (RFPsignal) and blue fluorescence (cell death stain) by using aflow cytometer (MoFLo XDP cell sorter; Beckman Coulter).
StatisticsData are expressed asmean� SEM. To test for differences
between groups, the Kruskal–Wallis 1-way ANOVA and
Bevacizumab Effects on Gliomas In Vivo
www.aacrjournals.org Clin Cancer Res; 17(19) October 1, 2011 6195
on August 28, 2021. © 2011 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst July 25, 2011; DOI: 10.1158/1078-0432.CCR-10-1868

Student Newman Keuls as post hoc test were used. Forrepeated measurements, Friedman Repeated MeasuresANOVA on ranks or the Wilcoxon signed rank test wasapplied (SigmaStat 3.5 Software). Survival was assessed byplotting survival curves according to the Kaplan–Meiermethod; comparisons were carried out by using the log-rank test. The value of P < 0.05 was considered to bestatistically significant.
Results
Bevacizumab dose dependently inhibits tumorgrowth and increases survival
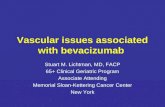
First, we examined the kinetics of tumor growth andtumor angiogenesis after cerebral implantation of 105 RFP-expressing human U87 glioma cells. Initially, implantedU87 glioma cells proliferated slowly. Within this period,the tumor vasculature was comprised mostly of preexistingbrain capillaries, many of them undergoing vascular remo-deling with enlargement (days 6 and 12 in Fig. 1A). Thefirst new blood vessels occurred from day 12 on. Once thetumor had reached a threshold diameter of 900 to 1,200mm, tumor growth was paralleled by extensive vascularremodeling and by the formation of new vessels (days19–30 in Fig. 1A). The onset of tumor angiogenesis wasfollowed by a more rapid tumor growth. The ability tofollow individual blood vessels in tumormicroregions overtime thus enabled us to clearly distinguish between newblood vessel formation (angiogenesis) and vascular remo-deling. Animals became moribund 2 to 5 weeks afterimplantation of tumor cells when tumors reached a meandiameter of 3.5 to 4.5mm (9.6–15.8mm2). Importantly, invitro growth rates of wild-type and DsRed2-transfectedcancer cell lines as well as VEGF-expression were equal(Supplementary Fig. S3A–C).
Next, we sought to compare the effects of 3 different andclinically meaningful doses of bevacizumab (which inhi-bits human ¼ tumor cell–derived VEGF-A). By giving 0.5,5, and 25 mg/kg bevacizumab i.p. every 2 days to mice,plasma concentration of 4.9 � 2.01 mg/mL, 22.7 � 8.25mg/mL, and 196.89 � 35.32 mg/mL were reached after 2applications. After 8 applications, plasma levels of 11.4mg/mL � 8.3 mg/mL, 76.3 � 13.1 mg/mL, and 341.3 � 99.4mg/mL were obtained (n ¼ 3–4 animals per group). Whencompared with published pharmacokinetic data fromhumans (35), the application of 0.5 mg/kg i.p. in miceresults in plasma concentrations that are achieved whenhumans are given 0.3 to 1 mg/kg bevacizumab i.v.; the 5mg/kg mouse dose corresponds to a 3 mg/kg human dose;and the 25 mg/kg mouse dose corresponds to a 15 mg/kghuman dose, approximately. Higher doses are required inmice because the half-life of bevacizumab is 3.5-fold lowerin mice (6 days in mice vs. 20 days in humans; refs. 36, 37),and the route of administration was different (i.p. vs. i.v.).In conclusion, the selected doses represent a subclinicaldose and 2 doses in the range that is used in the clinic.
A survival analysis showed that the mean survivalafter inoculation of 5 � 105 tumor cells is 21 � 2 days
in the control group, 32 � 5 days, 44 � 6, and 55 � 8 inanimals receiving 0.5, 5, and 25 mg/kg every other day(eod), respectively. Survival dose dependently increased,reaching significance in themedium- and high-dose groups(P < 0.05 vs. control, respectively).
To determine whether the survival benefit resulted froma reduced tumor growth, we determined the size of theoverall tumor as identified bymeasurement of the total RFPsignal over time. Bevacizumab at a dose of 5 and 25 mg/kgeod lead to a significant reduction of glioma growth, whencompared with animals receiving control IgG (Fig. 1C). Ontreatment days 6 and 12, mean tumor size was reduced by74% and 78% in animals receiving high-dose bevacizumaband by 58% and 64% in mice receiving an intermediatedose of 5 mg/kg. In contrast, treatment with low doses (0.5mg/kg) of bevacizumab did not significantly alter tumorgrowth (Fig. 1C). Importantly, even high doses of bevaci-zumab did not inhibit U87 proliferation (Fig. 1D) or alterthe RFP signal in vitro (Supplementary Fig. S4A).
Bevacizumab fails to induce glioma cell invasion inthe U87 model within a treatment period of 25 days
Some clinical and experimental evidence suggests thatmalignant gliomas continue to grow diffusely in the brainunder bevacizumab therapy (30, 38), including in U87xenograft models (39, 40). In our model, no aggressivegrowth pattern occurred during a treatment period of12 days in U87 xenografts, which normally grow withsharp borders to the normal brain (Fig. 1A). Even whentreatment was prolonged to 25 days, a true induction oflocal invasion by bevacizumab treatment could not bedetected. However, we did observe regions of the tumorborder that seemed to be less well defined due to the spreadof single tumor cells close to the main tumor mass (Fig. 1E,black arrows). The ability to monitor individual tumormicroregions over time allowed us to clarify that these cellsare remnants of regressing areas of themain tumor and thatthey themselves tend to regress over time.
Importantly, extensive characterization of the fluores-cence signal of U87-RFP in vitro confirms that (i) fluor-escence intensity indeed correlates with the number ofcells observed and is not affected by bevacizumab per se(see Supplementary Fig. S4A and B) and that (ii) the lossof RFP fluorescence signal in vitro corresponds to celldeath (Supplementary Fig. S5). The latter has alsobeen shown by us for other red fluorescent cancer cellsin vivo (41).
Bevacizumab effects on tumor blood vesselsTo gain insight into the dynamic effects of different doses
of bevacizumab on the tumor vasculature, we carried outan in-depth analysis of the tumor vascularization by usingintravital multiphoton microscopy of identical tumorregions over time. Before treatment, vessel morphologyin gliomas was highly heterogeneous (day 0 in Fig. 2A).In contrast to the normal cerebral vasculature, untreatedtumors displayed a chaotic network of tortuousblood vessels with fluctuating, often large diameters, a
Baumgarten et al.
Clin Cancer Res; 17(19) October 1, 2011 Clinical Cancer Research6196
on August 28, 2021. © 2011 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst July 25, 2011; DOI: 10.1158/1078-0432.CCR-10-1868

high vascular density, and lack of a hierarchicalnetwork (Fig. 2A). In control animals, tumor angiogramsof corresponding tumor regions showed a high vascularturnover (Fig. 2A, first panel): during an observation period
of 12 days, the formation of new tumor vessels and theregression of established ones happened continuously.Because of 3D tumor growth, vessels were recovered at avarying depth over the observation period and, in some
Figure 1. A, characteristic patternof glioma growth andangiogenesis imaged by in vivomultiphoton microscopy. Corticalvessels are highlighted in greenafter i.v. injection of FITC–dextran;U87-RFP cells are displayed inred. Images represent maximumintensity projections of the mousecortex from 0 to �350 mm atdifferent time points after singlecell implantation of 105 U87-RFPcells (scale bars 200 mm). B,treatment with bevacizumab dosedependently increased survival,reaching significance in themedium (5 mg/kg eod, blue line)and in the high (25 mg/kg eod) butnot at the low-dose group (0.5mg/kg eod, gray line), *, P < 0.05versus control (black line), n ¼ 6per group. C, bevacizumab dosedependently inhibits gliomagrowth in vivo (*, P < 0.05 vs.control, n ¼ 5 per group). Tumorsize of animals treated with controlantibodies (black line),bevacizumab 25 mg/kg eod(red line), 5 mg/kg eod (blue line),and 0.5 mg/kg eod (gray line). D,bevacizumab does not affectin vitro proliferation of U87 cells. E,shows a tumor border region overa time period of 25 days. Over thetime, the tumor border seems tobe less well defined because ofthe presence of vital single tumorcells (arrows) within areas in whichthe main tumor mass hasregressed. Images represent 3Dreconstructions (650 � 650 � 450mm) acquired by MPLSM.Respective top panels show both,tumor cells (red) and tumorvessels (green), bottom panelsshow tumor vessels only (scalebar 100 mm).
25 mg/kg
Control
5 mg/kg0.5 mg/kg
Bevacizumab
25 mg/kg
Control
5 mg/kg0.5 mg/kg
Bevacizumab
Therapy
vs. Contr.vs. Contr.
Day 6A
B
C
E
D
Day 30
Day 0 Day 3 Day 6 Day 12 Day 17 Day 25
Day 12 Day 19 Day 24
Bevacizumab Effects on Gliomas In Vivo
www.aacrjournals.org Clin Cancer Res; 17(19) October 1, 2011 6197
on August 28, 2021. © 2011 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst July 25, 2011; DOI: 10.1158/1078-0432.CCR-10-1868

cases, eventually escaped evaluation. Blood vessel diameterincreased and at late stages of tumor growth, vesselsappeared dilated and sinusoidal; the vascular densityremained high throughout the observation period.
Bevacizumab inhibited the formation of new tumorvessels, which resulted in a marked reduction of vascularturnover, leading to a steady decrease of overall tumorvessel density in all doses given (Fig. 2A). Compared withthe vascular network in control tumors, the vascular net-work that persisted despite treatment showed hierarchical
and much less excessive and chaotic branching patterns(Fig. 2A–C).
A quantification of the tumor angiograms confirmed thatbevacizumab induced a significant reduction of the vascu-lar volume, which reached a minimum at day 12 (Fig. 2C).The maximum extent of the reduction of vascular volumewas similar for the different doses of bevacizumab; how-ever, with a high dose of the drug, the inhibitory effectoccurred more rapidly after onset of treatment (Fig. 2C).The reduction in overall vascular volume was not because
25 mg/k g
A
B C
E F
D
Control
5 mg/kg 0.5 mg/kg
Bevacizumab
Figure 2. A, the effect of differentdoses of bevacizumab on thevascular phenotype of establishedU87 gliomas as assessed by invivo MPLSM. Note the dynamicalteration of the vascular bed incontrol tumors by high vascularturnover during the observationperiod. Bevacizumab treatmentleads to a stabilization of thevascular bed by inhibition of newblood vessel formation. Imagesrepresent 3D reconstructions(600 � 600 � 350 mm) ofcorresponding tumor angiogramsafter i.v. injection of FITC–dextranbefore (day 0) and on day 3, 6, 9,and 12 of treatment (scale bar 100mm). B, representative angiogramof the normal brain. C,quantification of vascular volume;D, mean vessel diameter; E,number of vessel branches(*, P < 0.05 vs. control, 2 regionsper animal, 5 animals per group);and F, vessel surface per vesselvolume (# P < 0.05 day 0 vs. day12, 2 regions per animal, 5 animalsper group).
Baumgarten et al.
Clin Cancer Res; 17(19) October 1, 2011 Clinical Cancer Research6198
on August 28, 2021. © 2011 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst July 25, 2011; DOI: 10.1158/1078-0432.CCR-10-1868

of a decrease in vascular diameter, as this parameterincreased in all groups during the experiment and wasonly affected at late stages by the high dose of bevacizumab(Fig. 2D). Bevacizumab therapy rather preferentiallypruned the small blood vessels of the tumor (Fig. 2A),which caused both a decrease in vascular volume and anincrease in the mean diameter. Consequently, bevacizu-mab rapidly reduced the number of vascular branchingpoints, and this was again independent of the dose(Fig. 2E). Extravasation of molecules from the bloodstreamby diffusion critically depends on the ratio of vessel surfaceper vessel volume (42). In mice treated with a high dose ofbevacizumab, the vessel surface per vessel volumeremained low over the entire course of the experiment(Fig. 2F), indicating a retention of a better vascular functionover time.
Bevacizumab treatment increases blood flow velocityand reduces vascular permeabilityTo determine the effects of bevacizumab on vascular
physiology, we determined blood flow velocity and vas-cular permeability in tumor vessels by intravital multi-photon microscopy.In tumor microvessels, RBC velocities were very low
compared with normal brain, which can contribute tohypoxia and difficulties in drug delivery within tumors(43). RBC velocities in arterioles and veins increased as afunction of the vascular diameter in normal brain; thisphysiologic dependency of blood flow velocity on vesseldiameter was completely disrupted in the tumor vascula-ture (Fig. 3A and B). This is in line with the concept thatabnormalities in both vasculature and blood viscosityincrease the resistance to blood flow in tumors and over-ride the physiologic interrelationship between RBC velo-cities and vessel geometry (44). Remarkably, treatmentwith bevacizumab dose dependently increased RBC velo-cities in gliomas (Fig. 3C) and partially reestablished theinterdependence of blood flow and vessel diameter (datanot shown).In control tumors, tumor vessels are abnormally perme-
able to albumin (Fig. 3C and D). Treatment with bevaci-zumab leads to a significant reduction of vascularpermeability in all 3 treatment doses (Fig. 3C).
Dynamic analysis of the interdependence of tumorcell and blood vessel regressionFinally, we aimed to take advantage of our novel animal
model to address the question whether or not bevacizumabcan cause glioma cell regression in vivo, and whether this isdue to its effects on tumor vasculature or independentthereof. Therefore, a tumor region of limited depth (33mm) was identified in all 3D at days 0, 6, and 9, andchanges of blood vessel and tumor cell volume weretracked over time in all 4 treatment groups (Fig. 4A–D).In contrast to Fig. 1B, in which the total tumor volume(including tumor cells, nontumor cells, vasculature, andintratumoral edema) was determined, we now measuredthe tumor cell volume only. Whereas both the intermediate
and the high dose of bevacizumab induced a similar netdecrease in vascular volume in these regions over time(Fig. 4E), only the high dose induced a rapid and pro-nounced reduction of tumor cell volume (Fig. 4F). Nosignificant reductions of tumor cell volumes were detectedin control animals (Fig. 4A and F) and in animals treatedwith a low dose of bevacizumab (Fig. 4D and F). This was afirst indication of an antitumor effect in addition to thevascular actions of bevacizumab when used in high doses.To analyze this discrepancy of antitumoral and antivasculareffects in more detail, we carried out an analysis of thespatiotemporal correlation of both tumor compartments inmice treated with the same high dose of bevacizumab(Fig. 5). On day 9 of treatment, in 6 of 10 tumor regions,the reduction of viable tumor cells in response to bevaci-zumab was preceded, at least paralleled by a decrease alsoin the vascular volume (Fig. 5A and B), suggesting that theantivascular action of the drug contributed to the reductionof viable tumor cells in these microregions. Notablythough, in 4 of 10 tumor regions, the antivascular andantitumor effect of bevacizumab seemed to be uncoupled:In 2 regions, bevacizumab triggered a substantial reductionin viable tumor cells without affecting overall vasculariza-tion (Fig. 5A and D), whereas there was no effect on tumorcell viability despite a substantial effect on tumor vascular-ization in another set of 2 microregions (Fig. 5A and C).
These findings have 3 major implications: (i) The anti-vascular effect of bevacizumab is most often paralleled byantitumoral effects, which supports the classical concept oftumor starvation by antiangiogenic therapy and proves thatbevacizumab does have the potency to reduce the numberof cancer cells in a glioma; (ii) Some microregions withinthe tumor manage to escape the antiangiogenic actions ofanti-VEGF treatment and continue to grow despite disin-tegration of the local microvascular network. (iii) Tumorcell viability can be impaired even without concomitantchanges of the local tumor vasculature morphology, sug-gesting that—in addition to its antivascular properties—bevacizumab-based anti-VEGF therapy also modulatestumor cell biology bymechanisms independent of vascularregression.
Discussion
In this study, we have directly addressed the effects ofdifferent doses of bevacizumab on tumor vessels, tumorgrowth, and tumor cell viability by using in vivo multi-photon microscopy of mouse glioma. Thus, for the firsttime, we were able to study dynamic interactions of bloodvessels and tumor cells in vivo and in real time during anti-VEGF therapy. We show here that the antiangiogenic effectof VEGF inhibition by bevacizumab occurs across the rangeof doses tested. Furthermore, normalization of vascularpermeability was observed with all doses; only normal-ization of blood flow velocity was dose dependent. How-ever, only higher, but not subclinical doses of bevacizumabalso reduced overall tumor growth, tumor cell viability, andprolonged survival. This indicates that blood vessel effects
Bevacizumab Effects on Gliomas In Vivo
www.aacrjournals.org Clin Cancer Res; 17(19) October 1, 2011 6199
on August 28, 2021. © 2011 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst July 25, 2011; DOI: 10.1158/1078-0432.CCR-10-1868

including vascular normalization occur with much smallerdoses than the effects on tumor cells, which has consider-able importance for future dosing considerations whenbevacizumab is used as monotherapy, or in combinationwith cytotoxic therapies for glioblastomas.
Until recently, antiangiogenic and antivascular effectswere considered the most prominent mechanism of action
of bevacizumab (45–48). Only with the introduction ofnovel imaging technologies, including epifluorescence andmultiphoton microscopy in combination with chronicwindow models, it has become obvious that the effectsof anti-VEGF therapy are likely to be more complex thaninitially anticipated (34, 41). Because of the previousinability to visualize of the dynamic events involved in
25 mg/kg
Control
5 mg/kg 0.5 mg/kg
Bevacizumab
#
# 25 mg/kg
Control
5 mg/kg 0.5 mg/kg
Bevacizumab
Normal brainA
B
D
CDay 0 Day 6
Day 0 Day 6
Figure 3. RBC velocities (VRBC) inrelation to the microvasculardiameter in the normal brain andestablished U87 gliomas (A). B,VRBC before and on day 6 oftreatment in control-treated (blackbars) and in bevacizumab-treatedanimals (red bars, 25 mg/kg eod;blue bars, 5 mg/kg eod; and graybars, 0.5 mg/kg eod). Note thedose-dependent increase of RBCvelocities by bevacizumab(#, P < 0.05 day 0 vs. day 6; day 6,*, P < 0.05 vs. control; n ¼ 12measurements in 5 animals pergroups). C, quantification of thevascular permeability in control(black bars) and in bevacizumab-treated animals (red bars,25 mg/kg eod; blue bars, 5 mg/kgeod; and gray bars, 0.5 mg/kgeod). The increased permeabilityof tumor vessels is reduced byall 3 doses of bevacizumab(#, P < 0.05 day 0 vs. day 6; day 6,*, P < 0.05 vs. control; n ¼ 2measurements in 5 animals pergroup). D, vascular permeability asassessed by the extravasation ofFITC–BSA. Images representmaximum intensity projections of�75 to �150 mm at day 6 aftertreatment with bevacizumab. Notethe dose-independent reductionof extravascular fluorescence 20minutes after i.v. injection of BSA.
Baumgarten et al.
Clin Cancer Res; 17(19) October 1, 2011 Clinical Cancer Research6200
on August 28, 2021. © 2011 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst July 25, 2011; DOI: 10.1158/1078-0432.CCR-10-1868

tumor growth and angiogenesis, another questionremained unsolved: does antiangiogenic treatment withbevacizumab also exert antitumor cell effects, because of orindependent from its antivascular properties? By usingintravital multiphoton microscopy, we show here thatanti-VEGF treatment substantially affects not only tumorvasculature but also glioma growth; high doses even lead toregression of tumor cells in distinct microregions. This is incontrast to recent animal studies showing an exclusiveantiedema (but not antitumor) effect of anti-VEGF tyrosinekinase therapy (28). However, it is in line with the markedinhibition of tumor growth seen with viral antisenseapproaches and the use of antibodies against endogenousVEGF (34, 48–52).Although these findings indicate that anti-VEGF may
have indirect antitumor potential in addition to its vascular
effects, the interdependence of the vascular and antitumoreffects of anti-VEGF strategies still is a matter of debate. Infact, there is increasing evidence suggesting that antitu-moral and antivascular effects might occur independentfrom each other. A recent study showed that the vasculargrowth factor receptor–targeted kinase inhibitor cediranibinduced rapid vascular normalization with a significantreduction of microvascular density and of vascular perme-ability leading to edema alleviation. The substantial effectson tumor vasculature were associated with prolongedsurvival; however, at the dose tested, tumor growthremained unaffected (28). This would fit to our findingfor the low dose of bevacizumab, which significantlyreduced tumor vasculature without affecting tumor growthand tumor cell viability. In contrast, animals receivingclinical doses of bevacizumab showed a decrease of tumor
Figure 4. Effect of different dosesof bevacizumab on tumor cellswithin established U87 gliomas.A–D, images represent 3Dreconstructions (600 � 600 � 33mm) of corresponding tumorregions before (day 0) and onday 6 and 9 of treatment withdifferent doses of bevacizumaband control IgG acquired byMPLSM. Respective top panelsshow both tumor cells (red) andtumor vessels (green); bottompanels show tumor vessels only(scale bar 100 mm). Quantificationof relative vascular volume (E) andrelative regional tumor volume (F).Note that tumorcell regression, butnot antivascular effects, is limitedto higher doses of bevacizumab(*, P < 0.05 vs. control; #, P < 0.05bevacizumab 25 mg/kg vs. 5mg/kg; n ¼ 2 regions in 5 animalsper group).
25 mg/kg
Control
5 mg/kg 0.5 mg/kg
Bevacizumab
Day 0 Day 6 Day 9
Day 0 Day 6 Day 9 Day 0 Day 6 Day 9
Day 0 Day 6 Day 9
A B
C D
E F
Bevacizumab Effects on Gliomas In Vivo
www.aacrjournals.org Clin Cancer Res; 17(19) October 1, 2011 6201
on August 28, 2021. © 2011 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst July 25, 2011; DOI: 10.1158/1078-0432.CCR-10-1868

growth and tumor cell viability as well as a reduction intumor vessels. The diversity that was observed in differentglioma microregions reflects the well-known morphologic,physiologic, and molecular heterogeneity of glioblastoma(53). Inmost of the tumormicroregions studied, tumor cellregression followed vascular regression, which is in accor-dance with the original hypothesis how antiangiogenictherapy should exert its effect (24). However, it is remark-able that a similar extent of vascular regression in the low-dose group did not result in significant tumor cell regres-sion. Moreover, even with the high dose, we still observeddistinct microregional uncoupling of its antitumoral andantivascular effects. Although we cannot complete rule outthat hypoxia occurs in areas without vascular regression,our present findings suggests that (i) the vascular effects ofanti-VEGF treatment do not necessarily translate into anti-tumor cell effect and that (ii) bevacizumab can cause tumorcell regression despite a lack of vascular regression in somemicroregions.
The mechanisms of the vessel-independent antitumorcell effects of bevacizumab in vivo remain elusive. Somehuman glioma cell lines (including U87), and cells isolatedfrom biopsy specimens express VEGF receptors, includingVEGFR-1/Flt-1, VEGFR-2/KDR, Neuropilin-1 (NRP-1), andNRP-2 (5, 54, 55). However, both the ligand VEGF-A andVEGFR2 neutralizing antibodies did not influence cellproliferation or invasion in in vitro assays (including inthis study), which argues against a relevant direct effect of
bevacizumab on tumor cells (56). Therefore, it seems mostlikely that anti-VEGF therapy modulates paracrine factorsof endothelial cells (or other cells of the brain parenchymaor progenitor cells; refs. 57, 58) in vivo. Correspondingly,studies have shown that VEGF-A inhibitors can inducetumor cell apoptosis by decreasing the levels of endothelialcell–derived paracrine factors promoting cell survival invitro (59). Those possible paracrine factors may, for exam-ple, include tissue factor Bcl-2 and VEGF-A itself (59, 60).Likewise, it has been shown for several other tumor entitiesthat modulation of VEGF receptor signaling blocks impor-tant functions of tumor cells in vivo despite the lack of aneffect on tumor cell proliferation in vitro, for example, inhuman leukemias (61, 62) and in human breast carcinoma(63). Furthermore, glioma stem cells reside in a perivas-cular niche (64) and rely on this local microenvironmentproviding survival signals (65). Interestingly, a recentreport identified endothelial nitric oxide as an importantfactor for glioma stem cell characteristic in the perivascularniche (66). This is of importance because bevacizumab hasbeen shown to reduce nitric oxide production of endothe-lial cells (60). Taken together, bevacizumab-induceddecrease of nitric oxide production might target gliomastem cells and thereby inhibit the ability of certain tumorregions to maintain a proliferative state.
Derived from in vivomicroscopical observations, RakeshJain suggested the concept of vascular normalizationaccording to which judicious application of antiangiogenic
Day 0 Day 6
A B
C D
Day 9
Day 0 Day 6 Day 9Day 0 Day 6 Day 9
Figure 5. A, quantification ofrelative changes in microregionalvascular volume and tumor cellviability at day 9 of treatment. In 6 of10 glioma regions (A; green ellipse),the decrease in the regionalvascular volume is paralleled orpreceded by a reduction of viabletumor cells in response tobevacizumabtreatment,whereas in4 of 10 glioma regions the effect ontumor cells and on the regionalvascular volume is uncoupled(A, black ellipse: vascularregression but no tumor cellregression; A, brown ellipse: tumorcell regression but no vascularregression). B–D, show tumorregions representing the 3 types.Note the synchronous blood vesseland tumor cell regression in B,whereas C shows vascularregression without tumor cellregression, and tumor cellregression without blood vesselregression in glioma microregionsin D. Images represent 3Dreconstructions (600 � 600 � 33mm) of corresponding tumorregions acquired by MPLSM.Respective top panels show both,tumor cells (red) and tumor vessels(green); bottom panels show tumorvessels only (scale bar 100 mm).
Baumgarten et al.
Clin Cancer Res; 17(19) October 1, 2011 Clinical Cancer Research6202
on August 28, 2021. © 2011 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst July 25, 2011; DOI: 10.1158/1078-0432.CCR-10-1868

therapy could transiently normalize the structurally andfunctionally abnormal tumor vasculature (26). This canlead to improved oxygenation of experimental gliomas,ultimately resulting in improved response to radiationtherapy but only during a time window (25). However,it remained unclear how different doses of an antiangio-genic agents influence the normalization phenomenon. Itwas hypothesized that there might be a too little and a toomuch of an agent when it comes to vascular normalization(26). Nevertheless, one can speculate that the doses ofantiangiogenic agents that exert maximum antitumoreffects are not the same that exert maximum normalizationeffects. Our results show that mice treated with bevacizu-mab reveal a morphologic and functional normalization oftumor vessels, which is evident even with a very low dose ofthe drug. A decrease in vascular permeability was noted inall treatment groups. However, the abnormally low bloodflow velocity of control tumors was increased only withhigher doses, suggesting that some features of vascularnormalization are indeed dose dependent.In conclusion, we show here that VEGF inhibition by
bevacizumab induces regression and normalization oftumor vasculature, but tumor cell regression becomesrelevant only at higher doses. The antitumor cell effectsoccur both dependent and independent of vascular regres-sion of the drug, suggesting a bevacizumab-induced mod-ulation of paracrine factors from the vasculature in sometumor microregions. These findings are clinically relevant:it is not clear yet whether bevacizumab should be used as asingle agent or in combination therapies in glioblastoma
(8, 9, 11) and what doses are optimal for both treatmentapproaches (14). Our results suggest that using lower dosesof bevacizumab can be sufficient to induce some extent ofvascular normalization in gliomas but have no antitumoreffect by itself. In contrast, with the caveat about a highertoxicity that might occur, higher doses, (e.g., 15 mg/kgevery 2 weeks in patients) might be most efficient, at leastfor monotherapy approaches, by adding antitumor celleffects.
Disclosure of Potential Conflicts of Interest
Y. Kienast is a full time employee at Roche since October, 2010. J. Hermshas received a commercial research grant from Roche for basic researchproject, and F. Winkler is an honoraria from Speakers Bureau (Roche,lecture, March 2010).
Acknowledgment
We thank Irene Kolm from Roche for the determination of Bevacizumabplasma concentrations, and Steffen Massberg for his creative input andsupport.
Grant Support
This study was supported by a grant from the Else Kroener-Fresenius-Stiftung (F. Winkler and S. Grau) and from the Deutsche Forschungsge-meinschaft (WI1930/4, F. Winkler).
The costs of publication of this article were defrayed in part by the paymentof page charges. This article must therefore be hereby marked advertisement inaccordance with 18 U.S.C. Section 1734 solely to indicate this fact.
Received July 14, 2010; revised June 13, 2011; accepted July 7, 2011;published OnlineFirst July 25, 2011.
References1. Stupp R, Mason WP, van den Bent MJ, Weller M, Fisher B, Taphoorn
MJ, et al. Radiotherapy plus concomitant and adjuvant temozolomidefor glioblastoma. N Engl J Med 2005;352:987–96.
2. Folkman J. Role of angiogenesis in tumor growth and metastasis.Semin Oncol 2002;29:15–8.
3. Plate KH, Breier G, Weich HA, Risau W. Vascular endothelial growthfactor is a potential tumour angiogenesis factor in human gliomas invivo. Nature 1992;359:845–8.
4. Chaudhry IH, O’Donovan DG, Brenchley PE, Reid H, Roberts IS.Vascular endothelial growth factor expression correlates with tumourgrade and vascularity in gliomas. Histopathology 2001;39:409–15.
5. Lamszus K, Ulbricht U, Matschke J, Brockmann MA, Fillbrandt R,Westphal M. Levels of soluble vascular endothelial growth factor(VEGF) receptor 1 in astrocytic tumors and its relation to malignancy,vascularity, and VEGF-A. Clin Cancer Res 2003;9:1399–405.
6. Norden AD, Drappatz J, Wen PY. Antiangiogenic therapy in malignantgliomas. Curr Opin Oncol 2008;20:652–61.
7. Vredenburgh JJ, Desjardins A, Herndon JE, Dowell JM, Reardon DA,Quinn JA, et al. Phase II trial of bevacizumab and irinotecan inrecurrent malignant glioma. Clin Cancer Res 2007;13:1253–9.
8. Friedman HS, Prados MD, Wen PY, Mikkelsen T, Schiff D, Abrey LE,et al. Bevacizumab alone and in combination with irinotecan inrecurrent glioblastoma. J Clin Oncol 2009;27:4733–40.
9. Kreisl TN, Kim L,Moore K, Duic P, Royce C, Stroud I, et al. Phase II trialof single-agent bevacizumab followed by bevacizumab plus irinote-can at tumor progression in recurrent glioblastoma. J Clin Oncol2009;27:740–5.
10. Raizer JJ, Grimm S, Chamberlain MC, Nicholas MK, Chandler JP,Muro K, et al. A phase 2 trial of single-agent bevacizumab given in an
every-3-week schedule for patients with recurrent high-grade glio-mas. Cancer 2010;116:5297–305.
11. Chamberlain MC, Johnston S. Bevacizumab for recurrent alkylator-refractory anaplastic oligodendroglioma. Cancer 2009;115:1734–43.
12. Vredenburgh JJ, Desjardins A, Herndon JE, Marcello J, Reardon DA,Quinn JA, et al. Bevacizumab plus irinotecan in recurrent glioblastomamultiforme. J Clin Oncol 2007;25:4722–9.
13. Cohen MH, Shen YL, Keegan P, Pazdur R. FDA drug approvalsummary: bevacizumab (Avastin) as treatment of recurrent glioblas-toma multiforme. Oncologist 2009;14:1131–8.
14. Wick W, Weller M, van den BM, Stupp R. Bevacizumab and recurrentmalignant gliomas: a European perspective. J Clin Oncol 2010;28:e188–9.
15. Nghiemphu PL, Liu W, Lee Y, Than T, Graham C, Lai A, et al.Bevacizumab and chemotherapy for recurrent glioblastoma: a sin-gle-institution experience. Neurology 2009;72:1217–22.
16. Wong ET, Gautam S, Malchow C, Lun M, Pan E, Brem S. Bevacizu-mab for recurrent glioblastoma multiforme: a meta-analysis. J NatlCompr Canc Netw 2011;9:403–7.
17. Miles DW, Chan A, Dirix LY, Cortes J, Pivot X, Tomczak P, et al. PhaseIII study of bevacizumab plus docetaxel compared with placebo plusdocetaxel for the first-line treatment of human epidermal growth factorreceptor 2-negative metastatic breast cancer. J Clin Oncol 2010;28:3239–47.
18. Johnson DH, Fehrenbacher L, Novotny WF, Herbst RS, NemunaitisJJ, Jablons DM, et al. Randomized phase II trial comparing bevaci-zumab plus carboplatin and paclitaxel with carboplatin and paclitaxelalone in previously untreated locally advanced or metastatic non-small-cell lung cancer. J Clin Oncol 2004;22:2184–91.
Bevacizumab Effects on Gliomas In Vivo
www.aacrjournals.org Clin Cancer Res; 17(19) October 1, 2011 6203
on August 28, 2021. © 2011 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst July 25, 2011; DOI: 10.1158/1078-0432.CCR-10-1868

19. Kabbinavar F, Hurwitz HI, Fehrenbacher L, Meropol NJ, Novotny WF,Lieberman G, et al. Phase II, randomized trial comparing bevacizumabplus fluorouracil (FU)/leucovorin (LV) with FU/LV alone in patients withmetastatic colorectal cancer. J Clin Oncol 2003;21:60–5.
20. Jain RK, Lee JJ, Hong D, Markman M, Gong J, Naing A, et al. Phase Ioncology studies: evidence that in the era of targeted therapiespatients on lower doses do not fare worse. Clin Cancer Res 2010;16:1289–7.
21. Rubin EH, Anderson KM. Finding the Right Dose for CancerTherapeutics–Can We Do Better? Clin Cancer Res 2010;16:1085–7.
22. Bonadonna G, Valagussa P. Dose-response effect of adjuvant che-motherapy in breast cancer. N Engl J Med 1981;304:10–5.
23. Cao Y. Off-tumor target–beneficial site for antiangiogenic cancertherapy? Nat Rev Clin Oncol 2010;7:604–8.
24. Folkman J. Tumor angiogenesis: therapeutic implications. N Engl JMed 1971;285:1182–6.
25. Winkler F, Kozin SV, Tong RT, Chae SS, Booth MF, Garkavtsev I,et al. Kinetics of vascular normalization by VEGFR2 blockadegoverns brain tumor response to radiation: role of oxygenation,angiopoietin-1, and matrix metalloproteinases. Cancer Cell 2004;6:553–63.
26. Jain RK. Normalization of tumor vasculature: an emerging concept inantiangiogenic therapy. Science 2005;307:58–62.
27. Batchelor TT, Sorensen AG, di Tomaso E, Zhang WT, Duda DG,Cohen KS, et al. AZD2171, a pan-VEGF receptor tyrosine kinaseinhibitor, normalizes tumor vasculature and alleviates edema in glio-blastoma patients. Cancer Cell 2007;11:83–95.
28. Kamoun WS, Ley CD, Farrar CT, Duyverman AM, Lahdenranta J,Lacorre DA, et al. Edema control by cediranib, a vascular endothelialgrowth factor receptor-targeted kinase inhibitor, prolongs survivaldespite persistent brain tumor growth in mice. J Clin Oncol 2009;27:2542–52.
29. Iwamoto FM, Abrey LE, Beal K, Gutin PH, Rosenblum MK, Reuter VE,et al. Patterns of relapse and prognosis after bevacizumab failure inrecurrent glioblastoma. Neurology 2009;73:1200–6.
30. Norden AD, YoungGS, Setayesh K, Muzikansky A, Klufas R, Ross GL,et al. Bevacizumab for recurrent malignant gliomas: efficacy, toxicity,and patterns of recurrence. Neurology 2008;70:779–87.
31. van den Bent MJ, Vogelbaum MA, Wen PY, Macdonald DR, ChangSM. End point assessment in gliomas: novel treatments limit useful-ness of classical Macdonald's Criteria. J Clin Oncol 2009;27:2905–8.
32. Norden AD, Drappatz J, Wen PY. Antiangiogenic therapies for high-grade glioma. Nat Rev Neurol 2009;5:610–20.
33. Kleinfeld D, Mitra PP, Helmchen F, Denk W. Fluctuations and stimu-lus-induced changes in blood flow observed in individual capillaries inlayers 2 through 4 of rat neocortex. Proc Natl Acad Sci U S A1998;95:15741–6.
34. Yuan F, Chen Y, Dellian M, Safabakhsh N, Ferrara N, Jain RK. Time-dependent vascular regression and permeability changes in estab-lished human tumor xenografts induced by an anti-vascular endothe-lial growth factor/vascular permeability factor antibody. Proc NatlAcad Sci U S A 1996;93:14765–70.
35. Jayson GC, Mulatero C, Ranson M, Zweit J, Jackson A, Broughton L,et al. Phase I investigation of recombinant anti-human vascularendothelial growth factor antibody in patients with advanced cancer.Eur J Cancer 2005;41:555–63.
36. Mordenti J, Thomsen K, Licko V, Chen H, Meng YG, Ferrara N.Efficacy and concentration-response of murine anti-VEGF monoclo-nal antibody in tumor-bearing mice and extrapolation to humans.Toxicol Pathol 1999;27:14–21.
37. Lu JF, Bruno R, Eppler S, Novotny W, Lum B, Gaudreault J. Clinicalpharmacokinetics of bevacizumab in patients with solid tumors.Cancer Chemother Pharmacol 2008;62:779–86.
38. Verhoeff JJ, van Tellingen O, Claes A, Stalpers LJ, van Linde ME,Richel DJ, et al. Concerns about anti-angiogenic treatmentin patients with glioblastoma multiforme. BMC Cancer 2009;9:444.
39. de Groot JF, Fuller G, Kumar AJ, Piao Y, Eterovic K, Ji Y, et al. Tumorinvasion after treatment of glioblastoma with bevacizumab: radio-
graphic and pathologic correlation in humans and mice. Neuro Oncol2010;12:233–42.
40. Lucio-Eterovic AK, Piao Y, de Groot JF. Mediators of glioblastomaresistance and invasion during antivascular endothelial growth factortherapy. Clin Cancer Res 2009;15:4589–99.
41. Kienast Y, Von Baumgarten L, Fuhrmann M, Klinkert WE, GoldbrunnerR, Herms J, et al. Real-time imaging reveals the single steps of brainmetastasis formation. Nat Med 2010;16:116–22.
42. Jain RK. Transport of molecules across tumor vasculature. CancerMetastasis Rev 1987;6:559–93.
43. Jain RK, di Tomaso E, Duda DG, Loeffler JS, Sorensen AG, Batch-elor TT. Angiogenesis in brain tumours. Nat Rev Neurosci 2007;8:610–22.
44. Jain RK, Munn LL, Fukumura D. Dissecting tumour pathophysiologyusing intravital microscopy. Nat Rev Cancer 2002;2:266–76.
45. Kim KJ, Li B, Winer J, Armanini M, Gillett N, Phillips HS, et al. Inhibitionof vascular endothelial growth factor-induced angiogenesis sup-presses tumour growth in vivo. Nature 1993;362:841–4.
46. Lee CG, Heijn M, di Tomaso E, Griffon-Etienne G, Ancukiewicz M,Koike C, et al. Anti-vascular endothelial growth factor treatmentaugments tumor radiation response under normoxic or hypoxic con-ditions. Cancer Res 2000;60:5565–70.
47. Rubenstein JL, Kim J, Ozawa T, ZhangM,Westphal M, Deen DF, et al.Anti-VEGF antibody treatment of glioblastoma prolongs survival butresults in increased vascular cooption. Neoplasia 2000;2:306–14.
48. Kunkel P, Ulbricht U, Bohlen P, Brockmann MA, Fillbrandt R,Stavrou D, et al. Inhibition of glioma angiogenesis and growth invivo by systemic treatment with a monoclonal antibody againstvascular endothelial growth factor receptor-2. Cancer Res 2001;61:6624–8.
49. Im SA, Gomez-Manzano C, Fueyo J, Liu TJ, Ke LD, Kim JS, et al.Antiangiogenesis treatment for gliomas: transfer of antisense-vascu-lar endothelial growth factor inhibits tumor growth in vivo. Cancer Res1999;59:895–900.
50. Dickson PV, Hamner JB, Sims TL, Fraga CH, Ng CY, Rajasekeran S,et al. Bevacizumab-induced transient remodeling of the vasculature inneuroblastoma xenografts results in improved delivery and efficacy ofsystemically administered chemotherapy. Clin Cancer Res 2007;13:3942–50.
51. Saleh M, Stacker SA, Wilks AF. Inhibition of growth of C6 glioma cellsin vivo by expression of antisense vascular endothelial growth factorsequence. Cancer Res 1996;56:393–401.
52. Cheng SY, Huang HJ, Nagane M, Ji XD, Wang D, Shih CC, et al.Suppression of glioblastoma angiogenicity and tumorigenicity byinhibition of endogenous expression of vascular endothelial growthfactor. Proc Natl Acad Sci U S A 1996;93:8502–7.
53. Park CK, Jung JH, Park SH, Jung HW, Cho BK. Multifarious proteomicsignatures and regional heterogeneity in glioblastomas. J Neurooncol2009;94:31–9.
54. Mentlein R, Forstreuter F, Mehdorn HM, Held-Feindt J. Functionalsignificance of vascular endothelial growth factor receptor expressionon human glioma cells. J Neurooncol 2004;67:9–18.
55. Steiner HH, Karcher S, Mueller MM, Nalbantis E, Kunze S, Herold-Mende C. Autocrine pathways of the vascular endothelial growthfactor (VEGF) in glioblastoma multiforme: clinical relevance ofradiation-induced increase of VEGF levels. J Neurooncol 2004;66:129–38.
56. Hong X, Jiang F, Kalkanis SN, Zhang ZG, Zhang X, Zheng X, et al.Decrease of endogenous vascular endothelial growth factor may notaffect glioma cell proliferation and invasion. J Exp Ther Oncol2007;6:219–29.
57. Lyden D, Hattori K, Dias S, Costa C, Blaikie P, Butros L, et al. Impairedrecruitment of bone-marrow-derived endothelial and hematopoieticprecursor cells blocks tumor angiogenesis and growth. Nat Med2001;7:1194–201.
58. Grunewald M, Avraham I, Dor Y, Bachar-Lustig E, Itin A, Jung S, et al.VEGF-induced adult neovascularization: recruitment, retention, androle of accessory cells. Cell 2006;124:175–89.
59. Kaneko T, Zhang Z, Mantellini MG, Karl E, Zeitlin B, Verhaegen M,et al. Bcl-2 orchestrates a cross-talk between endothelial and tumor
Baumgarten et al.
Clin Cancer Res; 17(19) October 1, 2011 Clinical Cancer Research6204
on August 28, 2021. © 2011 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst July 25, 2011; DOI: 10.1158/1078-0432.CCR-10-1868

cells that promotes tumor growth. Cancer Res 2007;67:9685–93.
60. Wang Y, Fei D, Vanderlaan M, Song A. Biological activity of bevaci-zumab, a humanized anti-VEGF antibody in vitro. Angiogenesis2004;7:335–45.
61. Dias S, Hattori K, Zhu Z, Heissig B, Choy M, Lane W, et al. Autocrinestimulation of VEGFR-2 activates human leukemic cell growth andmigration. J Clin Invest 2000;106:511–21.
62. Dias S, Hattori K, Heissig B, Zhu Z, Wu Y, Witte L, et al. Inhibitionof both paracrine and autocrine VEGF/VEGFR-2 signaling pathways isessential to induce long-term remission of xenotransplanted humanleukemias. Proc Natl Acad Sci U S A 2001;98:10857–62.
63. Wu Y, Zhong Z, Huber J, Bassi R, Finnerty B, Corcoran E, et al. Anti-vascular endothelial growth factor receptor-1 antagonist antibody asa therapeutic agent for cancer. Clin Cancer Res 2006;12:6573–84.
64. Calabrese C, Poppleton H, Kocak M, Hogg TL, Fuller C, Hamner B,et al. A perivascular niche for brain tumor stem cells. Cancer Cell2007;11:69–82.
65. Gilbertson RJ, Rich JN. Making a tumour's bed: glioblastomastem cells and the vascular niche. Nat Rev Cancer 2007;7:733–6.
66. Charles N, Ozawa T, Squatrito M, Bleau AM, Brennan CW, Hambard-zumyan D, et al. Perivascular nitric oxide activates notch signaling andpromotes stem-like character in PDGF-induced glioma cells. CellStem Cell 2010;6:141–52.
Bevacizumab Effects on Gliomas In Vivo
www.aacrjournals.org Clin Cancer Res; 17(19) October 1, 2011 6205
on August 28, 2021. © 2011 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst July 25, 2011; DOI: 10.1158/1078-0432.CCR-10-1868

2011;17:6192-6205. Published OnlineFirst July 25, 2011.Clin Cancer Res Louisa von Baumgarten, David Brucker, Anca Tirniceru, et al. Glioma Blood Vessels and Tumor CellsBevacizumab Has Differential and Dose-Dependent Effects on
Updated version
10.1158/1078-0432.CCR-10-1868doi:
Access the most recent version of this article at:
Material
Supplementary
http://clincancerres.aacrjournals.org/content/suppl/2011/09/23/1078-0432.CCR-10-1868.DC2 http://clincancerres.aacrjournals.org/content/suppl/2011/07/25/1078-0432.CCR-10-1868.DC1
Access the most recent supplemental material at:
Cited articles
http://clincancerres.aacrjournals.org/content/17/19/6192.full#ref-list-1
This article cites 66 articles, 31 of which you can access for free at:
Citing articles
http://clincancerres.aacrjournals.org/content/17/19/6192.full#related-urls
This article has been cited by 15 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://clincancerres.aacrjournals.org/content/17/19/6192To request permission to re-use all or part of this article, use this link
on August 28, 2021. © 2011 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst July 25, 2011; DOI: 10.1158/1078-0432.CCR-10-1868















![When to test for BRAF and what are the consequences? · III TRIBE study who were treated with FOLFOXIRI plus bevacizumab or FOLFIRI plus bevacizumab [33]. Even if BRAF mutation was](https://static.fdocuments.in/doc/165x107/5c72e51609d3f2b92e8c59a6/when-to-test-for-braf-and-what-are-the-consequences-iii-tribe-study-who-were.jpg)
