
Integrating School Mental Health and PBIS: Selecting Evidence-based Practices
Best Practicesin Mental Health
FM_FM 4/16/13 12:58 PM Page i

Best Practices in Mental Health
Editors in ChiefVikki L. Vandiver, DrPH, MSW Kevin Corcoran, PhD, JDProfessor and Associate Dean ProfessorPortland State University Portland State UniversitySchool of Social Work School of Social Work1800 SW 6th St/PO Box 751 1800 SW 6th St/PO Box 751Portland, OR 97207-0751 Portland, OR 97207-0751(503) 725-5007 (503) [email protected] [email protected]
Book Editor Editorial AssistantsRobert H. Keefe, PhD, ACSW Kristin BeersAssociate Professor Stephanie SundborgSchool of Social Work Portland State University685 Baldy HallUniversity at Buffalo PublisherState University of New York David C. FollmerBuffalo, NY 14260-1050 Lyceum Books, Inc.716/645-3381 ext. [email protected]
Best Practices in Mental HealthVolume 9, Number 1, March 2013© 2013 by Lyceum Books, Inc. All rights reserved.Best Practices in Mental Health is published January and July by Lyceum Books, Inc., 5758 S. Blackstone Ave., Chicago, IL 60637. The subscription rate is U.S. $40.00 for individualsand U.S. $90.00 for libraries and institutions. Copies for individuals are available for U.S. $20.00.For all purchases, add U.S. $15.00 for delivery outside of the United States.
Articles and advertisements in Best Practices in Mental Health do not constitute endorsement bythe editors, Portland State University, SUNY University at Buffalo, or Lyceum Books, Inc.
The full text of Best Practices in Mental Health will be found on EBSCO Publishing’s academicdatabase called Academic Search Premier. The journal is also indexed in CSA/SociologicalAbstracts, Journalseek, Ulrich’s Periodicals Directory, Child Welfare Information Gateway(selected/appropriate articles), Academic Search Complete, Academic Search Premier, Academic Search Research & Development, Biography Reference Bank, Social Sciences FullText, and PsycINFO.
For subscription and advertising inquiries, please contact the publisher by phone(773/643-1902) or email ([email protected]).
Printed in the United States of AmericaDate of Issue: March 2013International Standard Serial Number: 1553-555X
FM_FM 4/16/13 12:58 PM Page ii
Alean Al-KrenawiMemorial University of Newfoundland
Mary I. ArmstrongFlorida Mental Health Institute
Kia J. BentleyVirginia Commonwealth University
Daphne CainLouisiana State University
Grant CharlesUniversity of British Columbia
Monit CheungUniversity of Houston
Ira C. ColbyUniversity of Houston
Lena DominelliDurham University
Richard EdwardsRutgers, The State University of New Jersey
Christopher G. HudsonSalem State University
Sean JoeUniversity of Michigan
Stuart KirkUniversity of California, Los Angeles
David KondratUniversity of South Florida
Wynne Sandra KorrUniversity of Illinois, Urbana-Champaign
Craig Winston LeCroyArizona State University
Bruce NisbetBuffalo State University
Thomas O’HareBoston College
David PattersonUniversity of Tennessee
Maria PuigColorado State University
Mark RaggUniversity of Eastern Michigan
Ian F. ShawUniversity of York
Jackie SieppertUniversity of Calgary
Haluk SoydanUniversity of Southern California
Karen M. StallerUniversity of Michigan
Makmur SunusiMinistry of Social Affairs Republic of Indonesia
Bruce ThyerFlorida State University
Maria Elena Ramos TovarUniversidad Autonoma de Nuevo Leon
John J. VaccaSaint Joseph’s University
Jack C. WallLoyola University Chicago
Alex WashingtonCalifornia State University, Long Beach
Editorial Board
FM_FM 4/16/13 12:58 PM Page iii

FM_FM 4/16/13 12:58 PM Page iv

vii Editorial Policy and Submission Guidelines
xi Letter from the Editors: “Evidence” for Best PracticeKevin Corcoran and Vikki L. Vandiver
Articles
1 A Systematic and Empirical Review of Mindfulness Interventionswith Adolescents: A Potential Fit for Delinquency InterventionKatherine L. Montgomery, Johnny S. Kim, David W. Springer, and Joy A. Learman
20 Youthful Offender Diversion Project: YODACatheleen Jordan, Peter Lehmann, Kristin Whitehill, Lieu Huynh, Kingsley Chigbu,Richard Schoech, Jamie Cummings, and Debra Bezner
31 The Full Spectrum: Hispanic Understanding of AutismHeather Voelkel, Craig W. LeCroy, Lela Rankin Williams, and Jane Holschuh
47 Promotion of Holistic Development in University Students: A Credit-Bearing Course on Leadership and Intrapersonal DevelopmentDaniel T. L. Shek
62 Reducing Health Disparities for People with Serious Mental Illness: Development and Feasibility of a Peer Health Navigation InterventionJohn S. Brekke, Elizabeth Siantz, Rohini Pahwa, Erin Kelly, Louise Tallen, and Anthony Fulginiti
Best Practices inMental Health
VOL. 9No. 1MARCH
2013
FM_FM 4/16/13 12:58 PM Page v

Brief Report
83 Conceptual Underpinnings of the Evidence-Based Practice Sustainability IndexTrevor J. Manthey and Rick Goscha
Case Study
99 When Bambi Meets Godzilla: A Practitioner’s Experience Adapting and Implementing a Manualized Treatment in a Community Mental Health SettingJonathan B. Singer and Catherine M. Greeno
Book Reviews
117 Character Formation and Identity in Adolescence: Clinical and Developmental IssuesReviewed by Jed Metzger
118 Citizenship Social Work with Older PeopleReviewed by Jason Dauenhauer
120 Advocacy Practice for Social Justice, 2nd EditionReviewed by Pamela Viggiani
Website Review
123 Your Attention, Please: A Review of Selected Websites on Attention Deficit Hyperactivity DisordersKristin Beers and Stephanie Sundborg
vi Best Practices in Mental Health
FM_FM 4/16/13 12:58 PM Page vi

Best Practices inMental Health
EDITORIAL POLICY
AND SUBMISSION
GUIDELINES
Aims and Policies
Best Practices in Mental Health is a refereed publication intended for an interdisciplinary audience of
mental health practitioners, administrators, and scholars. The journal publishes original, practice-
focused articles that are in keeping with the best possible evidence about what works in clinical, com-
munity, and/or organizational settings. Each issue includes information on innovative programs, inter-
ventions, new research efforts, book reviews, and descriptions and links to relevant websites.
The journal seeks to provide readers with an array of articles on topics ranging from the micro
application of a single practice intervention, such as psychoeducation, to macro applications such as
accreditation standards. Manuscripts are solicited from the entire mental health community and also
invited from other educators, researchers, policy makers, and practitioners whose focus is on
strengthening the knowledge base of mental health practices.
Categories of Best Practices
Best practices is a term with a broad definition that has numerous applications. The journal reviews
four areas of mental health practices: (1) best practices, (2) emerging practices, (3) practice-based
evidence, and (4) evidence-based practice. We ask that contributors ensure submissions meet at least
one of these categories of best practices as described below.
Best practices for mental health can be described as a method or technique that has consistently
shown results superior to those achieved with other means and is often used as a benchmark for oth-
ers to base their practices on. Additionally, best practices guidelines are determined through a thor-
ough process that includes research findings, clinical experience, and implementation guidelines
which are then debated and discussed by panels of specialists including clinicians, researchers, pro-
gram administrators, and client advocates.
Emerging practices are defined as treatments and services that are promising, are less thoroughly
documented than evidence-based practices, and have a strong research foundation but fewer than
five scientifically rigorous published studies. Emerging practices are often administrative or clinical
practices that have proven effective at achieving a specific aim, hold promise for other organizations,
and show effectiveness in small-scale projects where research designs are less rigorous or self-report-
ing measures are used.
FM_FM 4/16/13 12:58 PM Page vii

Practice-based evidence is defined as evidence of real-world data collection and focuses heavily
on improving practice. Descriptions are focused on effectiveness and practice, and studies often
describe routine practices that have high external validity but little inferential generalizability.
Evidence-based practices are those interventions for which there is consistent scientific evidence
showing that they improve client outcomes, with one or more replications of the original studies.
Overall, best practices are broadly seen as activities, programs, and guidelines that have been cre-
ated based on careful identification and synthesis of the best available evidence in a particular field
of practice.
Types of Articles
Best Practices accepts regular articles and brief reports, both of which can include conceptual papers
(e.g., descriptive best practices), research reports (e.g., empirically supported best practices), and spe-
cialty topic literature reviews (e.g., best practices for transition-age youth). Anyone interested in sub-
mitting such material should contact the editors. From time to time, the editors will solicit articles on
special topics and will feature such special topics as consumer-selected best practices, commentaries,
and field notes. Book reviews are a regular feature of the journal and are usually solicited by the editors.
The following section describes the recommended format and procedures for conceptual and
research manuscripts and book reviews.
Conceptual articles. The format for conceptual articles is introduction, best practices program or
intervention description, preliminary findings, discussion (e.g., including implications for best prac-
tices), and conclusion. The introduction can include literature review, issues, problem statement, and
identification of best practice category. The program or intervention description can include theoret-
ical perspective, program description or design, components, steps for implementing best practice, or
curriculum description. Preliminary findings can reference evaluation efforts and results, and note
whether informed consent and institutional review board approval was obtained. The discussion sec-
tion can describe findings, limitations of the intervention or program, recommendations for future
development, and implications for best practices. The conclusion section pulls it all together and
refers to main findings or conclusions supported by the discussion.
Research reports. The standard format for research reports is introduction, methods, results, dis-
cussion (with implications for best practices), and conclusion. In the last paragraph of the introduction,
state the purpose of the research as either a statement or a research question, indicate type of study
design (e.g., experimental, survey), and identify which category of best practice this article represents.
Include descriptive data of participants or population, dates for original data collection, and statement
of whether informed consent or institutional review board approval was obtained. In the methods sec-
tion, describe the data analysis procedures in a manner understandable to nonstatisticians. In the
results section, report findings directly related to the research purpose or question. This section can
report numbers of all percentages (in either text or table) as well as statistically significant results (e.g.,
values, degrees of freedom, probability levels). The discussion section should describe limitations as
well as explicitly discuss the findings in relation to application and implications for best practices.
Book reviews. The journal’s intent is to publish book reviews that are relevant to readers interested
in resources for best practices in mental health. Books to be considered for review should be sent to
Robert H. Keefe, PhD, ACSW, School of Social Work, 685 Baldy Hall, University at Buffalo, State Uni-
versity of New York, Buffalo, NY 14260-1050, or [email protected]. Potential reviewers should
contact Professor Keefe.
viii Best Practices in Mental Health
FM_FM 4/16/13 12:58 PM Page viii

Submission of Manuscripts
General Requirements
Best Practices reviews material for publication on condition that it has not been previously published,
including electronic publication, and is not being reviewed for publication elsewhere. For peer review,
all submissions must:
1. Be sent electronically to [email protected] as one file folder containing multiple docu-
ments. For example, the folder must have separate e-files for the following:
• cover letter;
• title page with author names, affiliations, and contact information;
• article manuscript without author names on the title page, but including an abstract, key
words, full article text, references, and acknowledgments;
• tables and figures (if any), submitted as separate files, with a corresponding callout in the
text.
Files should be prepared using Microsoft Word and saved as .doc (not .docx) files. All tables
and figures must fit on the page with portrait (not landscape) orientation; PowerPoint figures
are not accepted. The entire article manuscript must be without author identification. E-mail
or phone inquiries may be made directly to either editor: Vikki L. Vandiver, [email protected],
503-725-5007; or Kevin Corcoran, [email protected], 503-962-0995.
2. Conform to the Publication Manual of the American Psychological Association, 6th edition
(APA) for citations and references only; text style should follow the Chicago Manual of Style,
16th edition. Please use person-first (e.g., person with schizophrenia, not schizophrenic;
research participants, not subjects) and nonsexist language.
3. Be double-spaced (including tables), using 12 point font (Times New Roman preferred) with 1-
inch margins. Do not use bold or underline. Number pages numbered in the upper right-hand
corner.
4. Conform to word and page limits. Regular articles should not exceed 5,000 words (about
twenty pages). Brief reports should not exceed 800 words (about four pages). Book reviews
should be about 600 words (about three pages).
5. Identify in the cover letter all authors and their contact information, include a statement claim-
ing that the manuscript is not under review elsewhere, and note which category the manu-
script should be reviewed under (best practices, emerging practices, practice-based evidence,
or evidence-based practice).
Arranging the Manuscript
Best Practices uses a blind review system, thus all manuscripts must have a separate title page that
can be removed when the manuscript is sent for review. As described above, please provide TWO title
pages, one with title of manuscript and all authors’ names, affiliations, and contact information; and
a second title page in the article manuscript with NO author identification.
Authors. Only principal writers should be listed as authors. Persons listed as authors must have
made substantial contributions to the article and must be able to take public responsibility for it.
Other contributors may be named in the acknowledgments. For each author, list no more than two
academic degrees or certifications and the primary current affiliation (including specific title and
department, agency, or university affiliation).
Editorial Policy and Submission Guidelines ix
FM_FM 4/16/13 12:58 PM Page ix

Acknowledgments. Acknowledgment of individuals or groups is limited to those who contributed
to the article’s intellectual or technical content. List all financial support, including grants and support
from foundations and/or the pharmaceutical industry. For grants, include the grant number and full
name of granting agency.
Abstract and key words. The abstract is meant to be a brief, succinct summary of the manuscript,
no longer than about 150 words. It is recommended that authors follow the format sections
described for conceptual or research papers (given above). Following the abstract, list key words that
characterize your manuscript (e.g., geriatric depression; home care; screening); please provide two or
three terms.
Manuscript. Whether your manuscript is a regular article (about twenty pages or 5,000 words) or
a brief report (about four pages or 800 words), please structure the sections using the guidelines
listed under conceptual or research.
Tables and figures. Include tables only when they present relevant numerical data more clearly
than can be done in text; all tables should be referenced in text. Please limit tables to one or two per
article. Figures can be used to illustrate a variety of relationships (e.g., logic models, flow charts, or
program diagrams). These should be formatted in Microsoft Word (using SmartArt, drawing tools, or
a text box), portrait orientation, no use of color, uncluttered, and clearly presented. Each table or
figure should have its own electronic file, clearly labeled. Be sure to indicate in the text approximately
where each table or figure should appear.
References. Please use care when preparing your article references. References cause the greatest
loss of time and productivity when your article is being reviewed, copy edited, and typeset. Limit ref-
erences to relevant published material cited in the text. Prior to submission of your article for review,
please check to see that spelling of names, titles, years of publication, up-to-date URLs, and page
numbers are correct and consistent. Please refer to previous issues of this journal for publishing style,
and consult the APA Publication Manual for any questions on how to prepare your references.
Review Process and Editorial Decision
Manuscripts submitted for publication are sent for blind peer review to three editorial board mem-
bers. Final decision for publication rests with the editors.
Timeline. The journal is published twice yearly (January and June). The peer review process takes
approximately one month, after which time the editors will communicate the editorial decision to the
author(s) along with a summary of information about the decision and, if appropriate, recommenda-
tions for revision of the manuscript for publication or resubmission for a second review. Once final
manuscripts are accepted and revisions (if needed) are completed, a future publication and issue date
will be provided to the author(s).
Revised manuscripts. Authors may be asked whether they wish to make suggested revisions, and
if so, a time frame will be given for turnaround.
x Best Practices in Mental Health
FM_FM 4/16/13 12:58 PM Page x

This journal was conceived from the need to develop and disseminate informationon best practices in mental health. To a measurable degree it has succeeded. Andyet, in the decade since its conceptualization much has changed in best practices.This has resulted in considerably more published articles, books, and manuals distinguishing what works (or seems to work based on probability) from whatseems not to work in the treatment of persons with mental health conditions.
One change has been the broadening of the scope of what is meant by bestpractices: that is, the amount of available evidence balanced against its probativeor persuasive value. A broader scope seems necessary, in part, because best prac-tice has always included evidence. The idea of using evidence in practice is notnew and has always been a part of clinical practice (Corcoran, 2007).
Historically, no example is more persuasive than the Greek practice of medi-cine. Their approach to health care was based on observations or data, that is, evi-dence. Although these observations were not highly accurate (i.e., valid), theywere consistent (i.e., reliable). Key to this approach were observations of blooddrying, resulting in the theory that there are four types of bodily fluids or humors:blood, phlegm, bile, and black bile. This was consistent with the Greeks’ quadraticworld view: four seasons, four components of the environment (hot, cold, wet, anddry), four directions (north, east, south, and west), four elements in the universe(earth, wind, fire, and water), and so forth (Barry, 2004). It all made perfect senseand was based on evidence.
It would be 600 years before further advancement was made, by way ofGalenic medicine (Galen, 130–200 CE), a mere tinkering with the Hippocraticnotions using a critically different method, known as active observations. Galen wasquite influential, and his procedures were considered the best practice throughoutthe Christian and Muslim worlds. Galenic medicine was evidence-based and treat-ments were derived from observations. With integrity, the theory of balance andimbalance in the body system (i.e., the four body humors being out of whack) pro-duced such interventions as bloodletting, sweating, urinating, defecating, vomit-ing, and other methods of purging to restore the balance between blood, phlegm,
Letter from the Editors“Evidence” for Best Practice
Kevin Corcoran and Vikki L. Vandiver
FM_FM 4/16/13 12:58 PM Page xi

bile, and black bile. Of these methods, the best practice soon became bloodletting,whereas vomiting, urinating, and defecating fell into disfavor. If tenacity is a cri-terion for knowledge (Rubin and Babbie, 2010), then there is something to be saidabout Galen and best practice, as both Near Eastern and Western medicine wouldwait another 1,500 years before any noticeable advancement would occur. Andyet, perhaps this illustrates that the problem with traditions is that they get old.
The defining issue of best practices, then, is not evidence per se, but the proba-tive value of that evidence when applied to the proper question. The challenge forresearchers and practitioners of best practice is to understand how sound evi-dence is established and to use practices for particular problems that are based onpersuasive evidence. Over the decades the gold standard has been the randomizedcontrolled trial, and rightfully so, but not without internal and external threats tovalidity.
Some best practices have had the benefit of extensive research, whereas recentinterventions for new or different mental health conditions, such as those foundat sites including the Substance Abuse and Mental Health Services Administra-tion, Robert Wood Johnson Foundation, and Hazelden & Dartmouth PsychiatricResearch Center, have not. In contrast, work with Indian youth using culturallyappropriate interventions is quite new (see Vandiver, 2013), but the evidence,although from less rigorous procedures such as quasi-experimental designs, ispromising and suggests an emerging best practice.
Vandiver (2013) delineates four ways of considering what is best practice:
1. research evidence proving that a practice works (i.e., evidence-based);2. practitioners’ opinions about what works in practice (i.e., clinical consensus
such as those produced by the Institute of Medicine);3. cultural and local context that determines if and how a practice works here
and now (i.e., practice-based evidence), along with a scientific frameworkthat incorporates culturally based interventions (again, practice-based evidence); and
4. guidelines or a general plan of action that requires specification to fit theparticular circumstances in which the system of care is being implemented.
All of these sources of best practice will be considered for publication in Best Prac-tices in Mental Health.
One type of evidence that the editors believe is slightly new to this journalappears in the inclusion of articles based on practice-based evidence. Althoughthe debate between evidence-based practice and practice-based evidence contin-ues, it is clear that both are of considerable value. It can be argued even to themost rigid empirical scientist that experience matters. In all likelihood, with expe-rience, scientists become much more proficient than they were when they enteredthe field. We improve because we observe our practices and refine our skills.
xii Best Practices in Mental Health
FM_FM 4/16/13 12:58 PM Page xii

Gladwell (2008) illustrates this concept in his delightful discussion of the10,000-hour rule. For various reasons it seems that 10,000 hours of practice isthe magic number of hours needed to make an expert. As all musicians, athletes,artists, and authors know, success results from practice, practice, and more prac-tice. This hypothesis does seem to work, and in every sense of the word, experienceis “practice-based evidence.” We hope to include exceptional pieces that illustratethis, along with articles using more rigorous methodologies. After all, the goal ofBest Practices in Mental Health is to develop and disseminate what seems to work.
To this end, the format of the journal has been changed. We intend to continuethe strong tradition of special issues once a year or so, and to organize the entriesto include an editorial, research articles, brief reports, book reviews, and a newsection by Kristin Beers and Stephanie Sundborg that reviews websites on a par-ticular topic. This section will be called Website Review, and the first entry is areview of sites about attention deficit hyperactivity disorders, which seems appro-priate because many of the articles in this issue concern youth and young adults.Finally, all authors will be asked to conclude with a section specifically addressingthe implications for best practice, with the intent of providing directions for prac-titioners. We welcome manuscripts of all types, and hope you find the new formatsatisfactory.
ReferencesBarry, J. M. (2004). The great influenza: The epic story of the deadliest plague in his-
tory. New York: Viking.Corcoran, K. (2007). From the scientific revolution to evidence-based practice:
Teaching the long journey of a short past. Research on Social Work Prac-tice, 17(5), 548–552.
Gladwell, M. (2008). Outliers: The story of success. New York: Back Bay Books.Rubin, A., & Babbie, E. (2010). Research methods for social work. Belmont, CA:
Brooks Cole/Cengage.Vandiver, V. L. (2013). Best practices in community mental health. Chicago: Lyceum
Books.
Letter from the Editors xiii
FM_FM 4/16/13 12:58 PM Page xiii

FM_FM 4/16/13 12:58 PM Page xiv

Mindfulness therapies have gained considerable attention recently in empirical litera-ture, revealing promise for the reduction of a variety of psychological and physiologicalsymptoms among adults. Studies have offered promising results regarding the efficacyof Acceptance and Commitment Therapy (ACT), Dialectical Behavior Therapy (DBT),Mindfulness-Based Cognitive Therapy (MBCT), and Mindfulness-Based Stress Reduc-tion (MBSR) for use with problems such as depression, anxiety disorders, borderlinepersonality traits, internalizing and externalizing problems, chronic pain, psychosis,and epilepsy. Only in recent years have researchers begun to investigate the impact ofmindfulness therapies on adolescent illnesses. To date, however, there has been no syn-thesis of research on mindfulness therapies with adolescents. Using specific inclusionand exclusion criteria, a systematic synthesis of the literature yielded a final sample offifteen studies (two ACT, twelve DBT, and one MBSR). When they were not reported inthe studies, effect sizes (Hedges’s g) were calculated for all outcome measures usingComprehensive Meta-Analysis 2.0 software. The majority of included studies reflectedmoderate to very large effect sizes regarding the impact of the mindfulness therapies onoutcome variables; however, only particular variables were significant. Findings fromthis systematic review offer a first step toward understanding the impact of mindful-ness therapies with adolescents.
Key words: Acceptance and Commitment Therapy; Dialectical Behavior Therapy;Mindfulness-Based Cognitive Therapy; Mindfulness-Based Stress Reduction Ther-apy; systematic review
“It is our own thoughts, inaccurate beliefs, unrealistic expectations, and insatiabledesires that obscure and distort our direct perceptions. Thinking is actually the
A Systematic and Empirical Review ofMindfulness Interventions with Adolescents: A Potential Fit for Delinquency Intervention
Katherine L. Montgomery, Johnny S. Kim, David W. Springer, andJoy A. Learman
Katherine L. Montgomery, MSSW, PhD, holds a post doctorate at George Warren Brown School ofSocial Work, Washington University, St. Louis, Missouri. Johnny S. Kim, PhD, is associate profes-sor at the University of Kansas. David W. Springer, PhD, is professor at University of Texas atAustin. Joy A. Learman, MSW, is a PhD candidate at the University of Texas at Austin.
© 2013 Lyceum Books, Inc., Best Practices in Mental Health, Vol. 9, No. 1, March 2013
Chapter 01_Chapter 01 4/16/13 11:02 AM Page 1

problem, not (as we often assume) the solution” (Semple & Lee, 2008, p. 64). Thisquote highlights the primary difference between the traditional cognitive behav-ioral therapies (CBTs) and mindfulness therapies. Although both assert that think-ing contributes to the problem, traditional cognitive-behavioral therapists putsubstantial emphasis on altering thinking as a means to change behavior (Craske,2009). Alternatively, the mindfulness therapies seek to alter individuals’ contextand relationship with their thinking rather than the actual thoughts (Greco &Hayes, 2008).
Mindfulness, or third-wave, behavioral therapies are relatively new and havegained popularity in research literature during the last two decades (Keng,Smoski, & Robins, 2011). These therapies have revealed particular promise for thereduction of a variety of psychological and physiological symptoms among adults(Keng et al., 2011; Montgomery, Kim, & Franklin, 2011). Specifically, studies have offered promising results regarding the efficacy of Acceptance and Commit-ment Therapy (ACT), Dialectical Behavior Therapy (DBT), Mindfulness-Based Cog-nitive Therapy (MBCT), and Mindfulness-Based Stress Reduction (MBSR) withissues such as depression (Grossman, Niemann, Schmidt, & Walach, 2004; Ma &Teasdale, 2004; Teasdale et al., 2000; Vowles & McCracken, 2008), anxiety dis-orders (Dalrymple & Herbert, 2007; Grossman et al., 2004), borderline personal-ity traits (Dimeff & Koerner, 2007), chronic pain (Dahl, Wilson, & Nilsson, 2004;Wicksell, Melin, Lekander, & Olsson, 2009), eating disorders (Wisniewski, Safer, &Chen, 2007), and epilepsy (Lundgren, Dahl, Melin, & Kies, 2006).
Only in recent years have researchers begun to investigate the impact of mind-fulness therapies on adolescent illnesses (O’Brien, Larson, & Murrell, 2008). Burke(2010) recently conducted a review of MBCT and MBSR interventions with bothchildren and adolescents. To date, however, there has been no systematic synthe-sis of research investigating all four mindfulness therapies with a focus on adoles-cents. Therefore, the primary purpose of this study is to offer an overview of eachthird-wave therapy, its utility with adolescents, and corresponding empirical sup-port by calculating effect sizes for treatment effects. An ancillary aim of thisreview is to explore the extent to which mindfulness therapies may offer delin-quency treatment providers a therapeutic approach to address identified limita-tions currently existing in the utilization of the most efficacious or evidence-baseddelinquency treatment interventions.
Background
Acceptance and Commitment Therapy
As reported by Fletcher and Hayes (2005), the primary aim of ACT is to fosterpsychological flexibility. Specifically, they define psychological flexibility as “theability to fully contact the present moment and the psychological reactions it pro-duces as a conscious person and to persist or change behavior in the situation inthe service of chosen values” (p. 319). Ultimately, ACT promotes psychologicalflexibility through six core processes: acceptance, presence in the moment, cogni-
2 Best Practices in Mental Health
Chapter 01_Chapter 01 4/16/13 11:02 AM Page 2

tive defusion, self as context, values, and committed action (Hayes, Luoma, Bond,Masuda, & Ellis, 2006). These six processes are considered to be interrelated andoften require the use of one process to fully explore another. Although overlap anda collective reliance on more than one of the processes are often necessary intreatment implementation, not all six constructs need to be utilized for effectiveintervention. Developmentally appropriate activities and metaphor exercisesbased on the ACT processes have been developed for the treatment of adolescents(e.g., Wicksell & Greco, 2008).
Research on the efficacy of ACT has primarily been dedicated to interventionwith adults. Over the past decade, researchers have reported on the promisingeffects of ACT with a variety of psychological and physiological health problemssuch as anxiety disorders (Dalrymple & Herbert, 2007; Woods, Wetterneck, &Flessner, 2006), depression (Vowles & McCracken, 2008; Vowles, Wetherell, &Sorrell, 2009), distress associated with psychotic symptoms (Gaudiano & Herbert,2006), chronic pain (Dahl et al., 2004; Vowles et al., 2009; Vowles & McCracken,2008; Wicksell et al., 2009), epilepsy (Lundgren et al., 2006), trichotillomania,chronic skin picking (Woods et al., 2006), and diabetes (Gregg, Callaghan, Hayes,& Glenn-Lawson, 2007).
Dialectical Behavior Therapy
Dialectical Behavior Therapy is based on the premise that a dialectic worldviewcan exist between clients’ mindfully accepting themselves and simultaneouslystriving for change (Linehan, 1993). As opposed to ACT, MBCT, and MBSR, DBT islargely influenced by traditional cognitive behavioral therapy and is employedthrough specific treatment stages with accompanying treatment goals (Dimeff &Koerner, 2007). For example, the goals associated with Stage 1 (achieving rea-sonable and immediate life expectancy, maintaining control of actions, and hav-ing adequate connection to treatment) are taught through skills training todevelop the following (Dimeff & Koerner, 2007):
• emotion regulation;• distress tolerance;• skillful responses to interpersonal situations;• observation, description, and participation skills in the absence of self-
judgment, while simultaneously remaining aware and focused on effectiveskills; and
• behavior management through utilizing strategies that are not self-injurious.
Initially developed to treat suicidal adult female patients diagnosed with bor-derline personality disorder (Linehan, 1993), DBT has also demonstrated a posi-tive impact on adults who have substance dependence with borderline personalitydisorder (McMain, Sayrs, Dimeff, & Linehan, 2007), eating disorders (Wisniewskiet al., 2007), and depression with personality disorder (Lynch & Cheavens, 2007).For adolescents, DBT consists of a combination of individual, group, and family
Mindfulness Interventions with Adolescents 3
Chapter 01_Chapter 01 4/16/13 11:02 AM Page 3

therapy and targets change for adolescents displaying borderline personality traits(Woodbury, Roy, & Indik, 2008). Rathus and Miller (2000) identified specificdialects central to the use of DBT with adolescents that would address the balancebetween (1) leniency and authoritarianism in the familial context, (2) pathologiz-ing normative behaviors and normalizing pathological behaviors, and (3) forcingautonomy and fostering dependence.
Mindfulness-Based Stress Reduction Therapy
Mindfulness-Based Stress Reduction was first developed in the 1970s for peoplewith a diverse range of physiological problems (Kabat-Zinn, 1990). Not considereda third-wave therapy, MBSR is the only intervention included in this review thatdoes not incorporate any behavioral techniques. The integration of mindfulnesspractice into Western medicine and health care has largely been credited to JonKabat-Zinn, the creator of MBSR (O’Brien et al., 2008). Unlike ACT and DBT, inwhich mindfulness is only a component of treatment, MBSR professionals considermindfulness techniques to be the primary method of treatment (Grossman et al.,2004). These mindfulness techniques are influenced by Buddhist mindfulness med-itation practices, but are offered in a secular context (Baer, 2003; Dryden & Still,2006; Kabat-Zinn, 1990). Delivering services in a group setting for eight weeklysessions, the MBSR therapist is an expert in mindfulness meditation who regularlypractices techniques individually (Kabat-Zinn, 1990, 2003; Segal, Williams, &Teasdale, 2002). Grossman and colleagues (2004) conducted a meta-analysis thatinvestigated the efficacy of MBSR with adults and revealed positive results withboth psychological and physiological health outcomes. They found a statisticallysignificant effect with both mental health outcomes (increased psychological well-being and decreased depression symptoms, anxiety symptoms, and affective per-ception of pain) and physical health outcomes (reduced medical symptoms, physi-cal pain, and physical impairment) for participants who received MBSR.
Age-appropriate techniques and language for this therapy have been developedfor children and adolescents. For example, Saltzman and Goldin (2008) detailedsome techniques they utilized during an eight-week MBSR group with youthenrolled in an after-school program. They described how they employed a mindfuleating exercise at the beginning of each group with apples, tangerines, or fig-filledcookies. The children were instructed to describe the texture, color, and smell ofthe snack before eating. When they ate the first bite, they were asked to close theireyes and notice how the texture felt in their mouth, how their teeth and tongueworked, and how the taste changed (Saltzman & Goldin, 2008). Exercises such asmindful eating in MBSR are employed to allow youth to purposefully slow downand become aware of a particular situation.
Mindfulness-Based Cognitive Therapy
Developed from MBSR, MBCT is considered to be an integration of mindfulnesstechniques and cognitive behavioral therapy (Segal et al., 2002). Different from
4 Best Practices in Mental Health
Chapter 01_Chapter 01 4/16/13 11:02 AM Page 4

the other three mindfulness therapies included in this review, MBCT was firstintended solely to prevent the relapse and recurrence of adult depression (Dimid-jian, Kleiber, & Segal, 2010). It is delivered through eight weekly two-hour grouptherapy sessions (Segal et al., 2002) and has shown promise with depressionrelapse (Ma & Teasdale, 2004; Teasdale et al., 2000) and anxiety symptomsamong adults diagnosed with bipolar disorder (Williams et al., 2008). Since itsinception, MBCT has been altered for youth diagnosed with anxiety disorders.Semple, Lee, and Miller (2006) highlight three primary structural changesbetween mindfulness-based cognitive therapy for children (MBCT-C) and tradi-tional MBCT:
1. treatment is delivered over twelve weeks in weekly ninety-minute group ses-sions
2. several experiential learning techniques are employed in each session toachieve developmentally appropriate engagement
3. treatment includes family involvement
Mindfulness and Delinquency Treatment
States spend approximately 7.1 million dollars each day housing juvenileoffenders in residential facilities (Justice Policy Institute, 2009). In efforts toreduce nationwide spending on residential care for adjudicated youth, great atten-tion has been given to the implementation of evidence-based practices (EBPs)through diversionary, community-based treatment programs (Greenwood,2008). Many EBPs for youth at risk of delinquency are grounded in a systems andecological perspective (Bronfenbrenner, 1979; von Bertalanffy, 1968), requiringchange in one or more of the systems (e.g., family, school, and neighborhood) withwhich the juvenile interacts. Current delinquency treatments with the strongestevidence base are Multisystemic Therapy (Henggeler, Melton, & Smith, 1992),Multisystemic Therapy for Youth with Problem Sexual Behaviors (Borduin,Henggeler, Blaske, & Stein, 1990), and Multidimensional Treatment Foster Care(Chamberlain, 1990). Although other EBPs for treating delinquency exist, theseare currently some of the only ones tested with youth offenders in randomizedcontrolled trials (RCTs).
Practitioners have experienced difficulty in replicating such community-basedtreatments with juvenile offenders in natural settings (Henggeler, 2003). Con-tributing to this problem is the lack of any standardized system for rating pro-grams (Greenwood & Edwards, 2011) and workforce capacity. Barriers to “scalingup” EBPs with juvenile offenders include:
• availability of resources necessary for a multilevel approach (Bond, Drake,McHugo, Rapp, & Whitley, 2009)
• clients’ severity and range of mental health disabilities• parents’ severity and range of mental health illnesses• lack of parental engagement in treatment (Greco & Hayes, 2008)
Mindfulness Interventions with Adolescents 5
Chapter 01_Chapter 01 4/16/13 11:02 AM Page 5

• difficulty associated with other systemic changes (school, church, peers, etc.)• treatment fidelity (Henggeler, 2003)• an understanding of which factors moderate treatment outcomes (Kazdin,
2004)
Mindfulness-based interventions are one potential treatment approach that couldameliorate some of the challenges associated with EBP implementation with juve-nile offenders.
Mindfulness therapies have a unique approach to treatment that may concep-tually address some of the identified gaps in delinquency intervention. Accordingto Erikson’s stages of development, adolescence is a period marked by the need toestablish one’s identity and self outside of the familial context (1950). Adolescentthought transitions from childhood into more abstract cognition that applieshypotheses and deductive reasoning to provide an ability to grasp the complex con-cepts associated with mindfulness (O’Brien et al., 2008). Further, Bowenian theo-rists assert that problematic outcomes within a family system are partly the resultof individuals’ inability to differentiate themselves from the family system (Walsh,2006). According to Walsh, delinquent youth often come from what Boweniantheorists would consider to be an enmeshed (undifferentiated) family system.
Research further highlights that problematic factors associated not only withthe family but also with peers, school, and community contribute to placing anadolescent at risk for engaging in delinquent behavior (Hawkins, Catalano, &Miller, 1992; Shader, 2004). For the client whose system (family, peers, school,and/or community) is too difficult to change or whose system refuses to partici-pate in treatment, or for the client who does not have access to the resources nec-essary to participate in one of the aforementioned multisystemic therapies, thereis little evidence suggesting alternate efficacious treatment.
Because mindfulness therapies teach the individual unique techniques thatencourage behavior change in the presence of difficult circumstances andthoughts, delinquent youth coming from a difficult system may benefit from thesetherapies by embracing and understanding their differentiated identity. Further,as mentioned previously, mindfulness therapies have revealed promise with adultpsychological and physiological outcomes, some of which are frequently consid-ered risk factors for delinquency. Thus, the ancillary aim of this review is toexplore the extent to which mindfulness therapies may offer a therapeuticapproach to address the needs of some delinquent youth, an approach that is cur-rently absent from the most efficacious systematic interventions.
Research Aims
The aims of this review are twofold. First, there is no systematic review thatinvestigates the efficacy of all four mindfulness therapies with adolescents. Thus,the authors aim to ascertain the level of efficacy of mindfulness therapies appliedto adolescent populations. Secondly, although a large evidence base exists for effi-cacious delinquency treatment, several gaps in implementing these EBPs with
6 Best Practices in Mental Health
Chapter 01_Chapter 01 4/16/13 11:02 AM Page 6

delinquent youth have been identified. Accordingly, this article will explore theextent to which mindfulness therapies for adolescents offer an approach foraddressing the existing EBP limitations, with the goal of examining the use ofmindfulness therapies with juvenile delinquents.
Methods
In order to conduct the systematic review, the authors searched the followingdatabases: CINAHL, Dissertation Abstracts International, ERIC, MEDLINE, andPsycINFO. Four groups of search terms were used:
1. Acceptance and Commitment Therapy and adolescen* or youth or teenage*2. Dialectical Behavior Therapy or Dialectical Behavioral Therapy and ado-
lescen* or youth or teenage*3. Mindfulness-Based Cognitive Therapy and adolescen* or youth or teenage*4. Mindfulness-Based Stress Reduction and adolescen* or youth or teenage*
As suggested by Littell, Corcoran, and Pillai (2008), for the most effective system-atic searches, the authors included dissertations, non-English publications, andarticles from various countries. When articles were not offered in English, theauthors contacted the original authors for an English translation of the results.Two authors conducted the initial search independently and fully concurred onthe initial search sample of 296 articles.
The final sample was identified by applying the following inclusion criteria tothe initial search sample: (1) studies must utilize one of the mindfulness therapieswith adolescents (ages twelve to eighteen); and (2) studies must employ a ran-domized controlled trial, quasi-experimental, or single-group pre-test/post-testdesign. These inclusion criteria reduced the final sample to fifteen studies. Thenboth authors independently coded the remaining fifteen studies and comparedcoding to resolve discrepancies.
When not reported in the articles, effect sizes (Hedges’s g) were calculated forall outcome measures using Comprehensive Meta-Analysis 2.0 software. Theseindividual effect sizes were then averaged together based on similar outcome con-structs. Effect sizes are reported for each individual study in the results section.When studies reported multiple follow-up points, the first follow-up point wasselected to help calculate effect sizes. Effect sizes were interpreted based on classi-fication by Cohen (1988), with 0.20 indicating a small effect size, 0.50 indicatingmedium, and 0.80 and above indicating large. All effect sizes were reported suchthat positive effect size estimates favored mindfulness therapies. A 95-percent con-fidence interval (CI) level was calculated for each study’s effect size measure(Lipsey & Wilson, 2001).
Because of the limited number of studies per mindfulness therapy and the var-ied outcomes targeted, studies were not combined in a traditional meta-analyticapproach. In addition, this decision not to combine study effect size estimatesallowed for the inclusion of several single-group repeated measure design studies
Mindfulness Interventions with Adolescents 7
Chapter 01_Chapter 01 4/16/13 11:02 AM Page 7

that could not be combined with independent group design studies in a meta-analysis (Lipsey & Wilson, 2001).
The authors chose to draw from concepts asserted by the ACT creators in theiroperational definition of outcomes associated with mental health. Because ACTtherapists do not focus on the label of a specific mental illness, but instead focus onan overall increased psychological flexibility or psychological well-being for allclients (Hayes et al., 2006), all mental health–related outcome effect sizes weregrouped and are reported as psychological well-being. Outcomes not deemed asmental health outcomes were reported individually.
Results
The initial search yielded 296 articles (46 ACT, 209 DBT, 14 MBCT-C, and 27MBSR). The authors attempted to contact the original authors for data when arti-cles did not contain sufficient data for effect size calculation. Studies employingRCT, quasi-experimental, or single-group pre-test/post-test designs utilizing one ofthe mindfulness therapies with adolescents (ages twelve to eighteen) wereincluded in the final sample of fifteen (two ACT, twelve DBT, and one MBSR).Although there were some studies (using qualitative and case study approaches)being conducted on the impact of MBCT-C with adolescents, no studies werefound that employed one of the aforementioned research designs.
From this final list of reviewed studies, four studies utilized an RCT design, fouremployed a quasi-experimental design, and seven utilized a single-group pre-test/post-test design. As seen in table 1, the majority of mindfulness therapies con-ducted with adolescents targeted outcomes associated with psychological well-being, particularly with regard to symptoms associated with depression, anxiety,and borderline personality disorder. Only one study (Biegel, Brown, Shapiro, &Schubert, 2009) used MBSR with adolescents. Medium-range effect size results (g = 0.424) for this RCT study were found regarding adolescent psychological well-being. Although the direction of the effect size was positive, the 95-percent confi-dence interval ranged from –0.034 to 0.882, indicating that the effect size is notstatistically different from zero. Thus, no difference in treatment effect between thecontrol and MBSR groups can be asserted.
The studies that investigated ACT’s efficacy with adolescents were the onlystudies that observed outcomes ancillary to psychological well-being. Wicksell,Melin, and Olsson (2007) used a single-group repeated measures design to exam-ine psychological well-being, school attendance, medication use, and pain impair-ment in their ACT study. Overall, a medium effect size (g = 0.488) was calculatedfor medication use, and large effect sizes were calculated for psychological well-being (g = 0.767), school attendance (g = 1.062), and pain impairment (g =1.158). All three of these large effect sizes were statistically significant based ontheir confidence intervals not containing zero. Wicksell and colleagues (2009) fol-lowed up with a more rigorous RCT study using ACT with adolescents. Theirresults indicated a small effect size for psychological well-being (g = 0.322), and alarge effect size (g = 0.680) was calculated for pain impairment. Although effectsizes were positive for both outcomes, the confidence intervals indicated no statis-tical difference.
8 Best Practices in Mental Health
Chapter 01_Chapter 01 4/16/13 11:02 AM Page 8

Mindfulness Interventions with Adolescents 9
Table 1 Adolescent Mindfulness Intervention Effect Sizes
Mindfulness-Based Stress Reduction N = 1
Citation Study design Outcome constructs Effect size(95% CI)
Biegel et al., 2009 RCT Psychological well-being(global functioning, state and trait anxiety, psychologicalstress, psychological well-being, depression, obsession-
compulsion, interpersonal sensitivity)
0.424(–0.034, 0.882)
Acceptance and Commitment Therapy N = 2
Dialectical Behavior Therapy N = 12
Wicksell et al.,2009
Wicksell et al.,2007
RCT
Single-grouppre/post
Psychological well-being(depression, internalizing/catastrophizing)
Pain impairment
Psychological well-being(depression, internalizing/catastrophizing)
School attendance
Medication use
Pain impairment
0.322(–0.392, 1.037)
0.680(–0.051, 1.412)
0.767(0.198, 1.336)
1.062(0.431, 1.693)
0.488(–0.037, 1.013)
1.158(0.504, 1.811)
Apsche et al.,2006
Cwik, 2006
Denaro, 2007
Goldstein et al.,2007
James et al., 2008
Katz et al., 2004
McDonell et al.,2010
Miller et al., 2000
Nelson-Gray et al.,2006
Rathus & Miller,2002
Wineman, 2009
Woodbury et al.,2008
RCT
RCT
Quasi-experimental
Single-grouppre/post
Single-grouppre/post
Quasi-experimental
Single-grouppre/post
Single-grouppre/post
Single-grouppre/post
Quasi-experimental
Quasi-experimental
Single-grouppre/post
Psychological well-being(depression, suicidal ideation)
Psychological well-being(mood regulation, depression, overall mental health
functioning)
Psychological well-being(suicidal ideation, depression, anxiety, anger)
Psychological well-being(suicidality, emotional dysregulation, mood symptomatology, depression)
Psychological well-being(borderline personality traits, depression, hopelessness,
global functioning)
Psychological well-being(depression, hopelessness, suicidal ideation)
Psychological well-being(global functioning, nonsuicidal self-injurious behavior)
Psychological well-being(borderline personality disorder symptoms:
confusion about self, impulsivity, emotional instability,interpersonal problems)
Psychological well-being(aggression, internalizing and externalizing problems,oppositional defiant disorder symptoms, depression)
Psychological well-being(suicide attempts, suicidal ideation, behavioral symptoms)
Psychological well-being(emotional awareness, emotional dysregulation,
depression, suicide risk)
Psychological well-being(suicidal ideation, impulsive-addictive behavior)
–0.438†(–1.289, 0.412)
0.138(–0.577, 0.853)
0.520(–0.419, 1.458)
0.638(–0.058, 1.335)
1.202(0.566, 1.838)
0.208(–0.325, 0.741)
0.801(0.575, 1.027)
0.942(0.495, 1.389)
0.487(0.115, 0.860)
0.800(0.128, 1.472)
0.448(–0.169, 1.065)
0.422(–0.004, 0.849)
† indicates comparison group did better than MBT.
Chapter 01_Chapter 01 4/16/13 11:02 AM Page 9

The mindfulness therapy with the most studies conducted with adolescentswas DBT. All DBT study outcomes included in this review coalesced around psy-chological well-being. Studies by Cwik (2006) and Apsche, Bass, and Houston(2006) were the only two DBT studies that employed an RCT design. Cwik (2006)reported having a small effect size (g = 0.138) for psychological well-being,whereas the other study reported a medium effect size (g = –0.0438) favoring theMode Deactivation Therapy (MDT) control group (Apsche et al., 2006). Neitherone of these studies was statistically significant based on the 95-percent confi-dence interval scores. Apsche and colleagues (2006) also examined physicalaggression, with results favoring the MDT control group of adolescents, but notenough statistical information was available to calculate an effect size for thismeasure.
Several studies used a quasi-experimental design to examine the effect of DBTon the psychological well-being of adolescents. Effect size results varied, as studiesrevealed one small effect size (g = 0.208, Katz, Cox, Gunasekara, & Miller, 2004),two medium effect sizes (g = 0.520, Denaro, 2007; g = 0.448, Wineman, 2009),and one large effect size (g = 0.800, Rathus & Miller, 2002). However, only thestudy by Rathus and Miller (2002) had a confidence interval that indicated differ-ence in treatment effect between the comparison and DBT group.
Half the DBT studies used a single-group repeated measures design, and psy-chological well-being effect size results were calculated for all six studies. Threestudies had medium effect sizes (g = 0.638, Goldstein, Axelson, Birmaher, & Brent,2007; g = 0.487, Nelson-Gray et al., 2006; g = 0.422, Woodbury et al., 2008).However, only the study by Nelson-Gray and colleagues was statistically signifi-cant. Three of the single-group design studies (g = 1.202, James, Taylor, Winmill,& Alfoadari, 2008; g = 0.801, McDonell et al., 2010; g = 0.942, Miller, Wyman,Huppert, Glassman, & Rathus, 2000) offered large statistically significant effectsize results. Each of these three findings was statistically significant.
Discussion
Best Practice with Adolescents
Mindfulness therapies, often considered third-wave behavioral therapies, havebecome popular over the previous decade in research literature and in the practicecommunity. Although substantial research has recently highlighted the efficacy ofparticular mindfulness therapies with various psychological and physiological ill-nesses, this review indicates that research on the efficacy of mindfulness therapieswith adolescents is still in its infancy. Nevertheless, this review offers insight intounderstanding and identifying unique interventions that may offer promise foradolescents who have been identified as difficult to treat.
Acceptance and Commitment Therapy
Of the mindfulness therapies, ACT studies incorporated a wider variety of out-comes. This is consistent with the ACT literature that has investigated the effi-
10 Best Practices in Mental Health
Chapter 01_Chapter 01 4/16/13 11:02 AM Page 10

cacy of ACT with adults who have many psychological and physiological prob-lems (Montgomery et al., 2011). At-risk adolescents, particularly those who areat risk of becoming delinquent, often display multiple internalizing and external-izing symptoms (Shader, 2004). Thus, intervening effectively with regard to allidentified problems for the juvenile delinquent has been deemed a difficult task(Greenwood, 2008). Although the review reveals that much more work is neededto understand the efficacy of ACT with adolescents, it may be an option to con-sider for youth who become involved in the juvenile justice system.
A medium effect size was calculated for medication use, whereas large effectsizes were computed for three other measures (psychological well-being, schoolattendance, and pain impairment; Wicksell et al., 2007). All three of these largeeffect sizes were statistically significant. However, when Wicksell and colleagues(2009) followed up with a more rigorous RCT study using ACT with adolescents,they found positive but nonsignificant effects. The more rigorous RCT study pro-duced nonsignificant smaller effects, highlighting the need for more research todetermine the efficacy of ACT with adolescent populations.
Dialectical Behavior Therapy
Consistent with the available research on adult mindfulness therapies, DBTresearch with adolescents is more robust than that for the other interventionsincluded in this review. Different from other mindfulness therapies, DBT focuseson outcomes associated with borderline personality traits (Linehan, 1993).Because this personality disorder has been considered difficult to treat, DBT hasgained considerable attention in both practice and research. Borderline person-ality disorder has been found in approximately one-fourth of delinquent boys(Eppright, Kashani, Robison, & Reid, 1993) and is correlated with antisocial per-sonality disorder among juvenile and criminal offenders (Taylor, James, Reeves, & Kistner, 2009). Further, Taylor and colleagues found that borderline personal-ity traits are associated with poorer clinical and psychosocial functioning indelinquent adolescents. Thus, this mindfulness therapy may be relevant for thisdifficult-to-treat population.
Of the four approaches examined in this review, the majority of the studiesexamined the effectiveness of DBT. However, half of these DBT studies used a single-group repeated measures design rather than a more rigorous researchmethodology such as RCT. Although two of the DBT studies were RCTs, neitherone was statistically significant based on the 95-percent confidence interval. Sev-eral DBT studies employed a quasi-experimental design to examine the effect ofDBT on psychological well-being among adolescents. Only one of the quasi-experimental studies (Rathus & Miller, 2002) produced statistically significantresults, indicating a significant difference in treatment effect between the com-parison and DBT groups. Half of the DBT studies used a single-group repeatedmeasures design, with four of these studies (James et al., 2008; McDonell et al.,2010; Miller et al., 2000; Nelson-Gray et al., 2006) revealing significant results.The findings on the efficacy of DBT with adolescents is mixed, and, as in the case
Mindfulness Interventions with Adolescents 11
Chapter 01_Chapter 01 4/16/13 11:02 AM Page 11

of ACT, additional research is necessary. The more rigorous RCTs did not producesignificant results, whereas four of the single-group repeated measures studiesdid reveal significant treatment effects.
Mindfulness-Based Stress Reduction and Mindfulness-Based Cognitive Therapy
Mindfulness-Based Stress Reduction Therapy was first created in the 1970s,and it is surprising that only one study met inclusion criteria for this review. Thisone MBSR study indicated that there was no difference in treatment effect betweenthe control and MBSR groups (Biegel et al., 2009). Additional research is neededto evaluate the use of MBSR with adolescent populations. There were also noMBCT-C studies that met the authors’ criteria for inclusion. Thus, the authors areunable to draw any conclusions about the effectiveness of MBCT-C based upontheir review.
Implications for the Treatment of Adolescents and Juvenile Delinquents
Based on this review, it appears at first glance that DBT may show the mostpromise among the mindfulness therapies examined for the treatment of adoles-cents. This assessment comes with two caveats, however. First, most of the positivetreatment effects and largest effect sizes in the studies included in this review wereproduced from less rigorous, single-group pre-test/post-test designs. Secondly,from a clinical perspective, DBT can be difficult to implement. It requires organi-zational support to ensure treatment fidelity, and is more challenging to use for anindependent practitioner. To illustrate, DBT’s treatment approach requires weeklytwo-hour skills training groups, weekly individual psychotherapy sessions,between-session telephone coaching support, and mandatory weekly consulta-tion team meetings for the clinician implementing the DBT treatment (Swenson,Torrey, & Koerner, 2002). Other researchers, such as Rizvi (2011), have noted thecomplexity and difficulty of implementing DBT, especially for novice clinicians.Guthrie (2006) also notes similar challenges when using DBT with adolescents.This raises questions about the transportability of DBT, particularly for the type ofsettings that typically provide treatment to juvenile delinquents, because it can bechallenging to hire and retain a qualified mental health professional in these set-tings. Additionally, these concerns are similar to the aforementioned problemsregarding the use of EBPs identified for delinquent populations.
In this review MBSR demonstrated a medium treatment effect that approachedstatistical significance. Moreover, findings from Wicksell and colleagues (2007,2009) showed promise for ACT. It appears that both MBSR and ACT may be morefeasible to implement with delinquent populations than DBT, and the treatmenteffects that they produced are not too different than what is typically reported forpsychosocial interventions in reviews of the adolescent treatment literature(Weisz & Jensen, 1999). Hence, because delinquent populations usually presentwith a variety of psychosocial problems that are considered very difficult to treat,
12 Best Practices in Mental Health
Chapter 01_Chapter 01 4/16/13 11:02 AM Page 12

mindfulness interventions may be beneficial to practitioners working with delin-quent populations.
Limitations
There are limitations to this study that inhibit the ability to analyze and inter-pret the data. First, it is important to note that this analysis takes the averagescores across several measures. Every time a score is averaged, its sensitivity andprecision are diminished. For example, in the Wicksell (2009) study, there werethree measures for pain with scores of 0.489, 0.559, and 0.993. The average ofthese three scores is 0.680. The medium effects of 0.489 and 0.559 both con-tained zero in their confidence interval, but the large effect of 0.993 did not. Yet,the average of the scores produced a confidence interval that contains zero, result-ing in a nonsignificant result, even for the large effect.
Second, there were several effect sizes (viz., Biegel et al., 2009; Goldstein et al.,2007; Wicksell et al., 2009; Woodbury et al., 2008) that approached statisticalsignificance (see table 1). This is related to the first limitation, as it is plausible thatthese effects did not reach significance as a result of averaging the measure scores.Additionally, the nonsignificant confidence interval findings in some of the effectsizes may be a function of the width of the confidence intervals, which could indi-cate that the study was small and low-powered, and resulting in the possibility ofa type II error in some cases (Davies, 2009). Also, many of the studies reviewedhad small sample sizes, which limit statistical power to detect treatment effects. Inaddition, the design of the studies reviewed was limited in external validity andthus generalizability.
Also, the studies included in this review were not limited to RCTs, and severalare open to several threats to internal validity. Additional research, employingstronger research designs, should be conducted before mindfulness therapies canbe considered sufficient treatment for delinquent adolescents.
Finally, there is a possibility that effect sizes were overestimated for single-grouprepeated measure designs (Lipsey & Wilson, 2001). Effect sizes calculated for theseless rigorous study designs may be misleading because they tend to be higher thanthose of the more rigorous experimental designs. Thus, some of the positive treat-ment effects reported above should be interpreted with caution.
Conclusion
Despite these limitations, this systematic review enhances the ability to criti-cally examine the extent to which mindfulness therapies may be useful in thetreatment of adolescents and juvenile delinquents. Based on this analysis, there ismixed support for ACT, DBT, and MBSR. Yet, clinically speaking, the more applic-able approaches appear to be ACT and MBSR. This is particularly true becausethey pertain to the treatment of juvenile delinquents, especially because they are likely to be more transportable than DBT given the barriers to scaling up
Mindfulness Interventions with Adolescents 13
Chapter 01_Chapter 01 4/16/13 11:02 AM Page 13

evidence-based approaches within juvenile justice treatment settings (e.g., fund-ing, staff resistance, capacity of agencies to support complex approaches, andworkforce availability; Greenwood & Edwards, 2011).
ReferencesApsche, J., Bass, C., & Houston, M. (2006). A one-year study of adolescent males
with aggression and problems of conduct and personality: A comparisonof MDT and DBT. International Journal of Behavioral Consultation and Ther-apy, 2(4), 544–552.
Baer, R. A. (2003). Mindfulness training as a clinical intervention: A conceptualand empirical review. Clinical Psychology: Science and Practice, 10(2),125–143.
Biegel, G., Brown, K., Shapiro, S., & Schubert, C. (2009). Mindfulness-basedstress reduction for the treatment of adolescent psychiatric outpatients:A randomized clinical trial. Journal of Consulting and Clinical Psychology,77(5), 855–866.
Bond, G. R., Drake, R. E., McHugo, G. J., Rapp, C. A., & Whitley, R. (2009). Strate-gies for improving fidelity in the National Evidence-Based Practices pro-ject. Research on Social Work Practice, 19(5), 569–581.
Borduin, C. M., Henggeler, S. W., Blaske, D. M., & Stein, R. (1990). Multisystemictreatment of adolescent sexual offenders. International Journal of OffenderTherapy and Comparative Criminology, 35(2), 105–114.
Bronfenbrenner, U. (1979). The ecology of human development. Cambridge, MA:Harvard University Press.
Burke, C. A. (2010). Mindfulness-based approaches with children and adoles-cents: A preliminary review of current research in an emergent field.Journal of Child and Family Studies, 19(2), 133–144.
Chamberlain, P. (1990). Comparative evaluation of specialized foster care forseriously delinquent youths: A first step. Community Alternatives: Interna-tional Journal of Family Care, 2(2), 21–36.
Cohen, J. (1988). Statistical power analysis for the behavioral sciences (2nd ed.).Hillsdale, NY: Lawrence Erlbaum.
Craske, M. G. (2009). Cognitive-behavioral therapy. Washington, DC: AmericanPsychological Association.
Cwik, M. (2006). A dialectical behavior therapy (DBT) skills training group forlearning disabled adolescents. Dissertation Abstracts International, 66,6266A.
Dahl, J., Wilson, K. G., & Nilsson, A. (2004). Acceptance and commitment ther-apy and the treatment of persons at risk for long-term disability resultingfrom stress and pain symptoms: A preliminary randomized trial. BehaviorTherapy, 35(4), 785–802.
Dalrymple, K. L., & Herbert, J. D. (2007). Acceptance and commitment therapyfor generalized social anxiety disorder: A pilot study. Behavior Modifica-tion, 31(5), 543–568.
14 Best Practices in Mental Health
Chapter 01_Chapter 01 4/16/13 11:02 AM Page 14

Davies, H. T. (2009). What are confidence intervals and p-values? RetrievedDecember 12, 2011, from http://www.whatisseries.co.uk/whatis.
Denaro, J. (2007). Effectiveness of dialectical behavior therapy in the treatmentof adolescent girls with borderline personality features in an outpatientcommunity mental health setting. Dissertation Abstracts International, 68,5564A.
Dimeff, L. A., & Koerner, K. (2007). Dialectical behavioral therapy in clinical prac-tice: Applications across disorders and settings. New York: Guilford Press.
Dimidjian, S., Kleiber, B. V., & Segal, Z. V. (2010). Mindfulness-based cognitivetherapy. In N. Kazantzis, M. A. Reinecke, & A. Freeman (Eds.), Cognitiveand behavioral therapies in clinical practice. New York: Guilford Press.
Dryden, W., & Still, A. (2006). Historical aspects of mindfulness and self-acceptance in psychotherapy. Journal of Rational-Emotive and Cognitive-Behavior Therapy, 24(1), 3–28.
Eppright, T. D., Kashani, J. H., Robison, B. D., & Reid, J. C. (1993). Comorbidity ofconduct disorder and personality disorders in an incarcerated juvenilepopulation. American Journal of Psychiatry, 150(8), 1233–1236.
Erikson, E. H. (1950). Childhood and society. New York: Norton.Fletcher, L., & Hayes, S. C. (2005). Relational frame theory, acceptance and com-
mitment therapy, and a functional analytic definition of mindfulness. Jour-nal of Rational-Emotive and Cognitive-Behavior Therapy, 23(4), 315–336.
Gaudiano, B. A., & Herbert, J. D. (2006). Acute treatment of inpatients with psychotic symptoms using acceptance and commitment therapy: Pilotresults. Behavior Research and Therapy, 44(3), 415–437.
Goldstein, T., Axelson, D., Birmaher, B., & Brent, D. (2007). Dialectical behaviortherapy for adolescents with bipolar disorder: A one-year open trial. Jour-nal of the American Academy of Child and Adolescent Psychiatry, 46(7),820–830.
Greco, L. A., & Hayes, S. C. (2008). Acceptance and mindfulness treatments for chil-dren and adolescents: A practitioner’s guide. Oakland, CA: New Harbinger.
Greenwood, P. (2008). Prevention and intervention programs for juvenile offenders. The Future of Children, 18(2), 185–210.
Greenwood, P. W., & Edwards, D. L. (2011). Evidence-based programs for at-riskyouth and juvenile offenders: A review of proven prevention and inter-vention models. In D. W. Springer & A. R. Roberts (Eds.), Juvenile justiceand delinquency (pp. 369–390). Boston: Jones and Bartlett.
Gregg, J. A., Callaghan, G. M., Hayes, S. C., & Glenn-Lawson, J. L. (2007).Improving diabetes self-management through acceptance, mindfulness,and values: A randomized controlled trial (a brief report). Journal ofCounseling and Clinical Psychology, 75(2), 336–343.
Grossman, P., Niemann, L., Schmidt, S., & Walach, H. (2004). Mindfulness-basedstress reduction and health benefits: A meta-analysis. Journal of Psycho-somatic Research, 57(1), 35–43.
Guthrie, D. M. (2006). Adolescent borderline personality disorder and dialecticalbehavior therapy. Praxis, 6, 35–43.
Mindfulness Interventions with Adolescents 15
Chapter 01_Chapter 01 4/16/13 11:02 AM Page 15

Hawkins, J. D., Catalano, R. F., & Miller, J. Y. (1992). Risk and protective factorsfor alcohol and other drug problems in adolescence and early adulthood:Implications for substance abuse prevention. Psychological Bulletin,112(1), 64–105.
Hayes, S. C., Luoma, J. B., Bond, F. W., Masuda, A., & Ellis, J. (2006). Acceptanceand commitment therapy: Model, processes and outcomes. BehaviorResearch and Therapy, 44(1), 1–25.
Henggeler, S. W. (2003). Advantages and disadvantages of multisystemic ther-apy and other evidence-based practices for treating juvenile offenders.Journal of Forensic Psychology Practice, 3(4), 53–59.
Henggeler, S. W., Melton, G. B., & Smith, L. A. (1992). Family preservation usingmultisystemic therapy: An effective alternative to incarcerating seriousjuvenile offenders. Journal of Consulting and Clinical Psychology, 60(6),953–961.
James, A. C., Taylor, A., Winmill, L., & Alfoadari, K. (2008). A preliminary studyof dialectical behavior therapy (DBT) with adolescent females demon-strating persistent, deliberate self-harm (DSH). Children and AdolescentMental Health, 13(3), 148–152.
Justice Policy Institute. (2009). The costs of confinement: Why good juvenile justicepolicies make good fiscal sense. Retrieved from http://www.justicepolicy.org/images/upload/09_05_REP_CostsOfConfinement_JJ_PS.pdf.
Kabat-Zinn, J. (1990). Full catastrophe living. New York: Hyperion Press.Kabat-Zinn, J. (2003). Coming to our senses: Healing ourselves and the world through
mindfulness. New York: Hyperion Press.Katz, L., Cox, B., Gunasekara, S., & Miller, A. (2004). Feasibility of dialectical
behavior therapy for suicidal adolescent inpatients. Journal of the Ameri-can Academy of Child and Adolescent Psychiatry, 43(3), 276–282.
Kazdin, A. E. (2004). Evidence-based treatments: Challenges and priorities forpractice and research. In B. Burns & K. Hoagwood (Eds.), Child and adolescent psychiatric clinics of North America (pp. 923–940). New York:Elsevier.
Keng, S., Smoski, M. J., & Robins, C. J. (2011). Effects of mindfulness on psycho-logical health: A review of empirical studies. Clinical Psychology Review,31(6), 1041–1056.
Linehan, M. M. (1993). Cognitive behavioral treatment of borderline personality dis-order. New York: Guilford Press.
Lipsey, M. W., & Wilson, D. B. (2001). Practical meta-analysis. Thousand Oaks,CA: Sage.
Littell, J. H., Corcoran, J., & Pillai, V. K. (2008). Systematic reviews and meta-analysis.New York: Oxford University Press.
Lundgren, T., Dahl, J., Melin, L., & Kies, B. (2006). Evaluation of acceptance andcommitment therapy for drug refractory epilepsy: A randomized con-trolled trial in South Africa, a pilot study. Epilepsia, 47(12), 2173–2179.
16 Best Practices in Mental Health
Chapter 01_Chapter 01 4/16/13 11:02 AM Page 16

Lynch, T. R., & Cheavens, J. S. (2007). Dialectical behavior therapy for depressionwith comorbid personality disorder: An extension of standard dialecticalbehavior therapy with a special emphasis on the treatment of olderadults. In L. A. Dimeff & K. Koerner (Eds.), Dialectical behavioral therapy in clinical practice: Applications across disorders and settings. New York: Guilford Press.
Ma, S. H., & Teasdale, J. D. (2004). Mindfulness-based cognitive therapy fordepression: Replication and exploration of differential relapse preventioneffects. Journal of Consulting and Clinical Psychology, 72(1), 31–40.
McDonell, M. G., Tarantino, J., Dubose, A. P., Matestic, P., Steinmetz, K., Galbreath, H., & McClellan, J. M. (2010). A pilot evaluation of dialecticalbehavioural therapy in adolescent long-term inpatient care. Child andAdolescent Mental Health, 15(4), 193–196.
McMain, S., Sayrs, J. H. R., Dimeff, L. A., & Linehan, M. M. (2007). Dialecticalbehavior therapy for individuals with borderline personality disorder andsubstance dependence. In L. A. Dimeff & K. Koerner (Eds.), Dialecticalbehavioral therapy in clinical practice: Applications across disorders and set-tings. New York: Guilford Press.
Miller, A., Wyman, S., Huppert, J., Glassman, S., & Rathus, J. (2000). Analysis ofbehavioral skills utilized by suicidal adolescents receiving dialecticalbehavior therapy. Cognitive and Behavioral Practice, 7(2), 183–187.
Montgomery, K. L., Kim, J., & Franklin, C. (2011). Acceptance and commitmenttherapy for psychological and physiological illnesses: A systematic reviewfor social workers. Health and Social Work, 36(3), 169–181.
Nelson-Gray, R., Keane, S., Hurst, R., Mitchell, J., Warburton, J., Chok, J., & Cobb,A. R. (2006). A modified DBT skills training program for oppositionaldefiant adolescents: Promising preliminary findings. Behaviour Researchand Therapy, 44(12), 1811–1820.
O’Brien, K. O., Larson, C. M., & Murrell, A. R. (2008). Third-wave behavior therapies for children and adolescents: Progress, challenges, and futuredirections. In L. A. Greco & S. C. Hayes (Eds.), Acceptance and mindfulnesstreatments for children and adolescents: A practitioner’s guide (pp. 15–35).Oakland, CA: New Harbinger.
Rathus, J., & Miller, A. (2002). Dialectical behavior therapy adapted for suicidaladolescents. Suicide and Life-Threatening Behavior, 32(2), 146–157.
Rathus, J. H., & Miller, A. (2000). Dialectical dilemmas in working with suicidaladolescents. Cognitive and Behavioral Practice, 7(4), 420–425.
Rizvi, S. L. (2011). Treatment failure in dialectical behavior therapy. Cognitive andBehavioral Practice, 18(3), 403–412.
Saltzman, A., & Goldin, P. (2008). Mindfulness-based stress reduction for school-age children. In S. C. Hayes & L. A. Greco (Eds.), Acceptance and mindful-ness interventions for children, adolescents and families (pp. 139–161). Oakland, CA: Context Press/New Harbinger.
Mindfulness Interventions with Adolescents 17
Chapter 01_Chapter 01 4/16/13 11:02 AM Page 17
Segal, Z. V., Williams, J. M. G., & Teasdale, J. D. (2002). Mindfulness-based cognitivetherapy for depression: A new approach to preventing relapse. New York: Guilford Press.
Semple, R. J., & Lee, J. (2008). Treating anxiety with mindfulness: Mindfulness-based cognitive therapy for children. In S. C. Hayes & L. A. Greco (Eds.),Acceptance and mindfulness interventions for children, adolescents and families(pp. 63–87). Oakland, CA: Context Press/New Harbinger.
Semple, R. J., Lee, J., & Miller, L. F. (2006). Mindfulness-based cognitive therapyfor children. In R. A. Baer (Ed.), Mindfulness-based treatment approaches:Clinician’s guide to evidence base and applications (pp. 143–166). Burlington,MA: Elsevier.
Shader, M. (2004). Risk factors for delinquency: An overview (NCJ 207540). Washington, DC: U.S. Department of Justice.
Swenson, C. R., Torrey, W. C., & Koerner, K. (2002). Implementing dialecticalbehavior therapy. Psychiatric Services, 53(2), 171–178.
Taylor, J., James, L. M., Reeves, M. D., & Kistner, J. A. (2009). Borderline person-ality traits are associated with poor clinical and psychosocial functioningin delinquent boys. Journal of Psychopathology and Behavioral Assessment,31(2), 94–103.
Teasdale, J. D., Segal, Z. V., Williams, J. M. G., Ridgeway, V., Soulsby, J., & Lau, M.(2000). Prevention of relapse/recurrence in major depression by mindfulness-based cognitive therapy. Journal of Consulting and ClinicalPsychology, 68(4), 615–623.
von Bertalanffy, L. (1968). General system theory: Foundations, development, appli-cations. New York: George Braziller.
Vowles, K. E., & McCracken, L. M. (2008). Acceptance and values-based actionin chronic pain: A study of treatment effectiveness and process. Journal ofConsulting and Clinical Psychology, 76(3), 397–407.
Vowles, K. E., Wetherell, J. L., & Sorrell, J. T. (2009). Targeting acceptance, mind-fulness, and values-based action in chronic pain: Findings of two prelimi-nary trials of an outpatient group-based intervention. Cognitive andBehavioral Practice, 16(1), 49–58.
Walsh, J. (2006). Theories for direct social work practice. Florence, KY: ThompsonBrooks/Cole.
Weisz, J. R., & Jensen, P. S. (1999). Efficacy and effectiveness of child and adoles-cent psychotherapy and pharmacotherapy. Mental Health ServicesResearch, 1(3), 125–157.
Wicksell, R. K., & Greco, L. A. (2008). Acceptance and commitment therapy forpediatric chronic pain. In L. A. Greco & S. C. Hayes (Eds.), Acceptance andmindfulness treatments for children and adolescents: A practitioner’s guide (pp. 89–113). Oakland, CA: New Harbinger.
Wicksell, R. K., Melin, L., Lekander, M., & Olsson, G. L. (2009). Evaluating theeffectiveness of exposure and acceptance strategies to improve function-ing and quality of life in longstanding pediatric pain: A randomized con-trolled trial. Pain, 141(3), 248–257.
18 Best Practices in Mental Health
Chapter 01_Chapter 01 4/16/13 11:02 AM Page 18
Wicksell, R., Melin, L., & Olsson, G. (2007). Exposure and acceptance in therehabilitation of adolescents with idiopathic chronic pain—a pilot study.European Journal of Pain, 11(3), 267–274.
Williams, J. M. G., Alatiq, Y., Crane, C., Barnhofer, T., Fennell, M. J. V., Duggan, D. S., . . . Goodwin, G. M. (2008). Mindfulness-based cognitive therapy(MBCT) in bipolar disorder: Preliminary evaluation of immediate effectson between-episode functioning. Journal of Affective Disorders, 107(1–3),275–279.
Wineman, P. (2009). The efficacy of a dialectical behavior therapy-based journal-writing group with inpatient adolescent females: Improving emotion regulation,depressive symptoms and suicidal ideation (Unpublished doctoral disserta-tion). Northeastern University, Boston, MA.
Wisniewski, L., Safer, D., & Chen, E. (2007). Dialectical behavior therapy and eating disorders. In L. A. Dimeff & K. Koerner (Eds.), Dialectical behavioraltherapy in clinical practice: Applications across disorders and settings. NewYork: Guilford Press.
Woodbury, K. A., Roy, R., & Indik, J. (2008). Dialectical behavioral therapy foradolescents with borderline features. In L. A. Greco & S. C. Hayes (Eds.),Acceptance and mindfulness treatments for children and adolescents: A practi-tioner’s guide. Oakland, CA: New Harbinger.
Woods, D. W., Wetterneck, C. T., & Flessner, C. A. (2006). A controlled evaluationof acceptance and commitment therapy plus habit reversal for trichotillo-mania. Behavior Research and Therapy, 44(5), 639–656.
Mindfulness Interventions with Adolescents 19
Chapter 01_Chapter 01 4/16/13 11:02 AM Page 19

A university-court collaboration developed a youth offender diversion project (YODA) inresponse to an ongoing trend of youth arrests for violence toward non-intimate-partnerfamily members (e.g., mothers or sisters) in Tarrant County, Texas. The YODA pro-gram is a three-phase approach using assessment, case management, and individual andfamily solution-focused brief therapy. This article reports on the benefits and process ofthe collaboration, as well as objectives for further study. Preliminary program evalua-tion results are promising.
Key words: case management; community-based treatment; diversion programs;family violence; juvenile justice; solution-focused brief therapy
This article describes a youth offender diversion project (YODA) that was devel-oped in response to an ongoing trend of youth arrests for violence toward non-intimate-partner family members (e.g., mothers and sisters) in Tarrant County,Texas. In September 2010, approximately 120 youth offenders charged withdomestic violence toward non-intimate-partner family members were awaitinghearing. Of concern was the effect of this behavior on adolescent and family devel-opment. Youth offenders are young persons typically aged seventeen throughtwenty-five, who usually live with adult caregivers and who have been chargedwith misdemeanor family violence. Before YODA, these youth offenders received
Youthful Offender Diversion Project: YODA
Catheleen Jordan, Peter Lehmann, Kristin Whitehill, Lieu Huynh, Kingsley Chigbu, Richard Schoech, Jamie Cummings, and Debra Bezner
Catheleen Jordan, PhD, is professor at the School of Social Work, University of Texas at Arling-ton. Also at the School of Social Work, University of Texas at Arlington, Peter Lehmann, PhD, isassociate professor, and Kristin Whitehill (Bolton), MSW and doctoral candidate, is a researchassistant. Lieu Huynh, MSSW, is clinical case manager at Texas Criminal Court #5, TarrantCounty, Texas. Kingsley Chigbu, MSW, is a doctoral candidate, and Richard Schoech, PhD, isresearch professor, Computer Science and Engineering at University of Texas at Arlington. JamieCummings, JD, is a judge, and Debra Bezner, MA, LPC, is a program coordinator at Texas Crimi-nal Court #5, Tarrant County, Texas. This article was supported by I-CAP funding from the AmonG. Carter Foundation.
© 2013 Lyceum Books, Inc., Best Practices in Mental Health, Vol. 9, No. 1, March 2013
Chapter 02_Chapter 02 4/16/13 11:02 AM Page 20

deferred adjudication and assignment to one-size-fits-all anger managementcourses, sometimes with career offenders. No systems of care existed to assess theparticular short- and/or long-term strengths and risks or sufficiency needs of theyouthful offender. Likewise, improvements in family functioning that might helppromote positive behaviors (e.g., good family ties and supportive relationships)were not addressed. Family involvement has been shown to be a critical require-ment for ending youth violence (Guerra, Kim, & Boxer, 2008). Consequently, asubstantial need existed to better understand the factors contributing to this grow-ing problem and to develop a mechanism to increase the likelihood that youth canend their violence and make a transition to a healthy independent adulthood.
To address this need, the YODA program was designed for these youth and theirfamilies and aimed to prevent future non-intimate-partner family violencethrough an innovative and collaborative community-based volunteer diversionprogram. YODA developed from a collaboration between Criminal Court #5 in Tar-rant County and the University of Texas at Arlington School of Social Work. Thisprogram requires an assessment of youth and family factors contributing to vio-lence, as well as case management and individual and family interventions to pre-vent future violence. This article will focus on the following topics:
• solution-focused brief therapy (SFBT) as diversion• the benefits of a collaborative community-based diversion program• the process used to establish a university-judicial relationship• program evaluation results• the potential for transferring the intervention and collaborative community
programming to other populations
Solution-Focused Brief Therapy as Diversion
Solution-focused brief therapy, which was chosen as the clinical basis of theYODA program intervention, is a strengths-based intervention. As a continuingresponse to treating aggression in adolescents, some researchers have added astrengths-based element to the requirements for successful treatment. Strengths-based approaches highlight and develop youth strengths and competencies toreduce risk (Guerra & Leaf, 2008). As part of the YODA project, a focus onstrengths attempts to “mobilize talents, knowledge, capacities, and resources inthe service of achieving clients’ goals and visions” (Saleebey, 2006, p. 1).Strengths-based approaches are grounded in the profession’s paradigm of helpingpeople achieve health and well-being. A greater emphasis is placed on findingwhat is right, effective, and strong within individuals as opposed to a focus onidentifying problems. In the following section, the authors advocate for the use ofSFBT as a strengths-based model of practice for the YODA diversion program.
Solution-Focused Brief Therapy and Supporting Evidence
Solution-focused brief therapy was developed by Steve de Shazer (1940–2005), Insoo Kim Berg (1934–2007), and colleagues beginning in the late 1970s
Youthful Offender Diversion Project: YODA 21
Chapter 02_Chapter 02 4/16/13 11:02 AM Page 21

in Milwaukee, Wisconsin (see, for example, Berg, 1994; Berg & Steiner, 2003; Berg& Dolan, 2001; de Shazer, 1985, 1988). It is future-focused and goal-directed, and it emphasizes potential solutions to the problems that bring clients to therapy.The SFBT approach assumes that all clients have some knowledge of what wouldmake their lives better, even though they may need (at times, considerable) help.Although everyone who seeks help already possesses at least the minimal skillsnecessary to create solutions, help is needed to describe the details of a better lifeby asking the miracle question in addition to carrying out new tasks. All clinicaltherapy is in the form of specialized conversations that can include client- andtherapist-approved tasks/assignments. With SFBT, the conversation can be aboutany number of problems the client brings, but with a focus on developing andachieving the client’s vision of solutions for a better future. A number of tech-niques and questions help to clarify those solutions and the means for achievingthem. These include but are not limited to looking for previous solutions andexceptions, coping and scaling questions, client goal setting, the miracle question,compliments, and inviting the client to do more of what works.
Supporting Empirical Evidence
Although the evidence base for SFBT is still preliminary (Corcoran & Pillai,2009), strides have been made in advancing the usefulness of SFBT. The followingis a summary of support for SFBT, including support relevant to the YODA project:
• The Office of Juvenile Justice and Delinquency Prevention (2008;www.ojjdp.gov) has recognized SFBT as a promising model of practice.
• Currently there are eighty-nine documented studies of SFBT (European BriefTherapy Association, 2010), including two meta-analyses, three systematicreviews of the literature, and eighty-three follow-up research-based papers.These studies include thirteen randomized/control group findings, thirtycomparison studies, and forty naturalistic studies summarizing a variety ofmental health issues.
Four SFBT studies, all with domestic violence batterer intervention programs,were found. Although none contain adolescent samples, the model and process ofthe client groups including content (e.g., violence against a significant other) maybe relevant for working with youthful offender populations.
The Benefits of a Collaborative Community-Based Diversion Program:YODA
The university-judicial collaboration generated a diversion program availableto youth offenders between the ages of seventeen and twenty-five. The programconsists of three phases using SFBT, a designated model of promise (Office of Juve-nile Justice and Delinquency Prevention, 2008). Solution-focused brief therapyhas not previously been used with this specific population. Phase 1 involves refer-
22 Best Practices in Mental Health
Chapter 02_Chapter 02 4/16/13 11:02 AM Page 22

ral from Tarrant County Court #5 to the University of Texas at Arlington (UTA)School of Social Work (SSW) Center for Clinical Social Work (referred to as theClinic) to assess self-sufficiency needs, mental health risks, and stressors. Follow-ing the referral, a multidimensional assessment looks at the extent to which fam-ily issues have contributed to past negative behaviors and how family strengthsmay contribute to greater positive outcomes. Case management to provide neededresources occurs in phase 1. Phase 1 assessment leads to the intervention plan forphases 2 and 3 by identifying youth and family needs.
Phase 2 consists of individual SFBT with the youth offender; case managementcontinues in this phase as needed to increase youth self-sufficiency behaviors andskills. Phase 3 includes family SFBT at the Clinic if the family agrees to participate.Phases 2 and 3 will eventually include a web-phone system, called teleherence, tooptimize client outcomes. The teleherence system will deliver messages andreminders through text messages or voice phone calls, ask questions, collect clientvoice messages and trigger alerts to staff, present counseling booster audios suchas motivational messages in the voice of the counselor, and flag potential problemsor opportunities for the case manager using smart algorithms.
Expected benefits of this collaborative effort include:
• diverting youth from the criminal justice system• providing an opportunity for charge dismissal through efforts of the youth
toward self-sufficient behaviors• assisting families with stressors to improve family relationships
Process Used to Establish a University-Community Collaboration
Establishing YODA required obtaining community support to fund the project,developing procedures for youth enrolled in the project, and measuring outcomes.
Funding the Project
In 2010, the UTA-SSW received a large grant from the Amon G. Carter Foun-dation. The purpose of this grant was to encourage partnerships between UTA-SSW faculty researchers and community agency personnel with the goal of pro-moting innovative research-practice collaborations, as well as improving the livesof individuals and families residing in Tarrant County.
Each year, grant proposals are developed by faculty-agency collaborators andsubmitted for review by a committee of nationally recognized experts in order todetermine which proposals will receive funding. The YODA program resulted froma partnership between Professor Peter Lehmann and Professor Catheleen Jordanat UTA-SSW, and Judge Jamie Cummings and her assistant, Debra Bezner, fromTarrant County Criminal Court #5. The project was funded in January 2011, andthe first clients enrolled in March 2011. Court personnel referred youth to the pro-ject and monitored progress. The university researchers supervised the adminis-tration of the intervention and the research component.
Youthful Offender Diversion Project: YODA 23
Chapter 02_Chapter 02 4/16/13 11:02 AM Page 23

Procedures
It is important to note that YODA is a voluntary program. Youth charged withassault in Tarrant County Criminal Court #5 may be offered the option of enter-ing the program, but not all youth are offered this option. Participants’ lawyers,district attorneys, and the judge decide who will be offered this option based onprior offenses, attitude and willingness to work toward change, and level of com-petency. Those who are offered the opportunity to enter the program are gener-ally presented with alternative plea arrangements negotiated by their lawyers.Next, the potential client meets with the case manager, receives an explanationof the program, and decides whether to join YODA or accept the plea. If the clientchooses to participate in the diversion program, he or she is provided with infor-mation about the requirements he or she must meet in order to remain enrolledand complete the program. One of these requirements is a strict attendance policy; clients are required to attend each session. If two sessions are missed andthe case manager believes the reasons for absence are invalid, the client isreported to the court and either dismissed from the program or sent to jail (thelength of jail time is determined by the judge). Compliance with the program is acondition of the client’s bond and therefore a condition of the client’s agreementwith the court. Furthermore, if the client is not making strides in SFBT sessionsoffered by the counselor and improvement is not being achieved, he or she is sub-ject to dismissal.
Upon enrollment in the program, clients are required to complete a compe-tency interview and assessment packet containing standardized measures(described further below). The assessments are completed within the first or sec-ond session with the case manager. Upon completion of assessments, the clientbegins SFBT with the case manager and continues routinely until completion ofthe program. Frequency of sessions is based on a subjective assessment by thecase manager regarding client need as well as his or her progress in achieving self-identified goals and goals identified by the case manager. Family therapy is a laststep in phase 3 if the assessment shows that it may be helpful and if family mem-bers agree to participate.
Measures
The outcome measures for YODA are classified as short- and long-term out-comes. Short-term outcomes include identification of problems, goal develop-ment, and initial steps toward achieving goals. Identification of problems and goaldevelopment are pivotal components of SFBT and are completed within the firsttwo sessions. If goals are not established, clients are unable to move forward withtreatment. All clients are required to identify problems and goals as conditions oftheir involvement in the program. If for some reason this is not done, clients arereferred back to the court for sentencing.
Short-term outcomes are assessed weekly by the client throughout treatmentusing a goal attainment scale. Clients are asked to rank progress toward their goals
24 Best Practices in Mental Health
Chapter 02_Chapter 02 4/16/13 11:02 AM Page 24

and objectives on a ten-point self-anchored scale. At the midway point in the pro-gram (generally around two to three months), clients report to the judge for a mid-term evaluation of their progress in terms of goal attainment as reported by thecase manager using the client’s self-reported data. Finally, upon completion of theprogram, the case manager provides the court with a similar updated evaluationof the client’s progress over the course of the program.
In terms of the short-term outcomes, it is important to emphasize that, in orderto complete the program, clients are not required to have achieved all of theirgoals. Some of the goals may take several years to complete (e.g., graduation fromhigh school or college), and the length of time to complete them would exceed thetime during which the client is enrolled in the program. However, the client mustdemonstrate progress toward achieving the objectives included in each goal beforecompletion of the program is considered.
Short-term outcomes also may include assessment, using standardized mea-sures, of the client’s level of self-sufficiency, resilience, aggression, family rela-tions, mental health, goal attainment, stress, and alcohol and substance abuse. Interms of middle outcomes, positive results would represent a shift from the base-line measurement. For example, through treatment it is hoped that levels ofaggression, substance abuse, mental health issues, and stress would decreasewhereas levels of resiliency, self-sufficiency, and family relations would all increaseor improve. Either of these results would be considered positive.
The long-term outcome for YODA is to reduce the occurrence of violent re-offense among the clients participating in the program. This is measured bysearching arrest records at both six months and one year after the program com-pletion date.
Below is a list of the measures used for short-term measurement:
• The Child and Youth Resilience Measure (CYRM): This measure containstwenty-eight items rated on a five-point Likert scale. Responses are sum-mated, with higher levels indicating higher levels of protective factors asso-ciated with resilient individuals.
• The Solution Building Inventory (SBI): This scale measures the client’s abilityto develop solutions and access both internal and external resources whenfaced with conflict. Fourteen items are scored on a five-point Likert scale.
• The Novaco Anger Scale and Provocation Inventory (NAS-PI): This is a two-partassessment containing eighty-five items rated on a three-point Likert scale.The NAS-PI assesses for anger as a problem of psychological functioning andphysical health as well as for therapeutic change.
• Multidimensional Adolescent Assessment Scale (MAAS): The MAAS comprisesfifteen subscales totaling 177 items. The items are ranked on a seven-pointLikert scale, and scores for each subscale are calculated separately. The sub-scales include problems with school, aggression, family relationship prob-lems, suicidal thoughts, feelings of guilt, confused thinking, disturbingthoughts, memory loss, alcohol abuse, and drug abuse.
Youthful Offender Diversion Project: YODA 25
Chapter 02_Chapter 02 4/16/13 11:02 AM Page 25

The assessments are completed during the first two sessions of enrollment inYODA and upon completion of the program. Change in scores from the pretest tothe posttest is used to measure program success.
Program Evaluation Results
The program evaluation provides a multidimensional view of YODA’s effective-ness. Both process and fidelity assessment as well as outcome evaluation sum-maries are discussed; focus is on the organization/services and clients. The processevaluation assesses the delivery of the program, and the outcome evaluationdetermines if the intended outcomes are in fact achieved. Although data collec-tion primarily consists of self-reports collected by the SFBT case manager, data col-lection and analysis are monitored and performed by the two faculty co-principalinvestigators and a PhD-level graduate assistant. This evaluation seeks to addressand offer implications and findings in three areas:
1. Has YODA been implemented according to plan?2. Does YODA operate in the intended manner?3. Is YODA meeting the intended outcomes?
Question 1: Implementation and Process Evaluation
Process evaluation addresses how well the program is being delivered to thetarget population. Implementation and process are evaluated on the basis of clientrecords and a bimonthly report of client contact.
The YODA staff and court personnel work side by side so that court records arereadily available. All youth in this age group who commit a crime are referred tothe court. The docket is reviewed once a month, and court personnel provide a listof the offenders to the YODA case manager. Nonattendance or noncompliance isdealt with through collaboration between YODA and court personnel. The processhas worked smoothly from the beginning, with most offenders who were offered anopportunity to join YODA accepting the opportunity and those who violated YODApolicy (i.e., were rearrested or did not attend required sessions) being removed.
Question 2: Program Fidelity
Program fidelity refers to whether the program is being delivered as intendedand in this case refers to the SFBT component. This portion of the evaluation isunder development. A fidelity measure has been developed (Lehmann, Jordan,Whitehill, Huynh, & Chigbu, 2012) for the clients to complete to determine if thetherapist/case manager is adequately delivering SFBT. The assessment is given tothe client at one randomly selected time during enrollment.
Sessions in which the assessment is administered will be video recorded. Thevideo recordings will then be microanalyzed to further determine if fidelity hasbeen achieved. Microanalysis dissects the session frame by frame and recordsresults. These results are then compared to results from the fidelity measure todetermine if correlation and consistency exist between the microanalyst’s percep-
26 Best Practices in Mental Health
Chapter 02_Chapter 02 4/16/13 11:02 AM Page 26

tion and the client’s perception of the delivery of the SFBT. Plans are for this to beimplemented in 2013.
Question 3: Outcome Evaluation
As of July 1, 2012 (fifteen months after the first youth entered the program),YODA had ninety-two clients enrolled in the program. All of the clients are youthaged seventeen to twenty-five and charged with assault of a non-intimate partner.Eighteen of the participants chose to leave the program and were rearrested or dis-missed for violating the attendance policy. Fifty participants had completed theprogram. Data presented are for the forty-nine clients who completed the mea-sures (one measure on one client is missing). The success rate for YODA was foundto be 80 percent. Case records revealed that all clients who remained in the pro-gram until completion attended the appropriate number of sessions and all butone completed a pre-test/post-test assessment packet. Demographics, short-termoutcomes, and long-term outcomes will be presented in the following sections.
Demographics. Demographic information is assessed at intake, and results arecomputed from the data sheet completed by each client during the initial assess-ment. It was found that 43 percent are Caucasian, 20 percent are Hispanic, 23percent are African American, 12 percent are biracial, and 2 percent are Asian.Male participants comprise the majority of the sample (53.1%); females accountfor 46.9 percent. Client ages ranged from seventeen to twenty-five, with a meanage of nineteen. The majority of clients are eighteen when they enter YODA. Sixty-seven percent of the clients are between the ages of seventeen and nineteen. Clienteducation varies from completion of eighth grade up to completion of some col-lege. Nearly half (48.9%) of clients are either enrolled in twelfth grade or havecompleted twelfth grade, whereas 26.5 percent are enrolled in or have completedsome college. The victim of the assault is primarily the mother (32.6%), followedby sister (22.4%); in spite of this, 59 percent of participants are living with theirvictim.
Short-Term Outcomes. Outcome data are based on the completed assessmentpackets at both pretest and posttest for the forty-nine clients who have completedthe program and the measures. Paired sample t-tests were used to assess ifchanges from pretest to posttest were statistically significant.
• MAAS: This scale (see table 1) measures a wide range of possible problemareas; it has two cutting scores: 30 and above indicates a clinical problem,and 70 and above indicates a catastrophic issue.
• SBI: The SBI is a fourteen-item questionnaire rated on a five-point Likertscale (see table 2). High scores on the SBI indicate better solution builders(Smock, McCollum, & Stevenson, 2010).
• CYRM: The CYRM assesses for processes of resilience (see table 2). It is atwenty-eight-item questionnaire rated on a five-point Likert scale. Higherscores indicate higher levels of resilience (Ungar, 2007).
Youthful Offender Diversion Project: YODA 27
Chapter 02_Chapter 02 4/16/13 11:02 AM Page 27

The NAS-PI (Novaco, 2003) is a two-part self-report questionnaire. It yields sixscores and contains eighty-five items (see table 3):
• Cognitive: Determined by responses given regarding engendering thoughtsthat may arise as a result of personal memories or meanings.
• Arousal: Focuses on the physical experience of the anger response.
28 Best Practices in Mental Health
Table 1 Means, Standard Deviations, and t-Test (N = 49)
MAAS Pretest Posttest Paired t-test
Mean SD Mean SD t df p
Depression 24.34 16.24 15.37 13.30 3.93 48 .000Self-esteem 23.15 14.08 16.63 12.20 3.79 48 .000Mother problems 33.65 23.78 18.86 21.25 5.07 48 .000Father problems 30.21 28.81 19.01 23.40 3.83 48 .000Personal stress 24.59 19.21 8.60 8.60 6.45 48 .000Friend problems 14.02 14.73 8.85 8.85 2.63 48 .006School problems 23.18 18.83 16.03 16.03 3.03 48 .002Aggression 22.58 18.05 9.18 15.49 6.53 48 .000Family problems 42.10 24.55 21.20 21.34 5.78 48 .000Suicide 8.89 15.90 1.39 4.36 3.34 48 .001Guilt 23.51 17.90 11.88 14.96 4.51 48 .000Confused thinking 24.49 26.62 13.03 14.43 3.72 48 .002Memory loss 20.95 21.09 12.24 14.42 3.19 48 .001Alcohol abuse 9.88 12.66 4.76 7.93 3.44 48 .001Drug abuse 6.32 12.08 1.19 5.86 3.41 48 .003
Table 2 Means, Standard Deviations, and t-Test for SBI and CYRM (N = 49)
Measure Pretest Posttest Paired t-test
Mean SD Mean SD t df p
SBI 59.18 8.67 65.84 4.88 –5.75 48 .000CYRM 108.01 17.90 120.00 13.47 –4.98 48 .000
Table 3 Means, Standard Deviations, and t-Test for NAS-PI
Novaco Pretest Posttest Paired t-test
Mean SD Mean SD t df p
Cognitive 45.73 12.50 36.08 11.49 6.34 48 .000Arousal 45.47 11.62 37.35 11.10 6.23 48 .000Behavior 47.27 11.95 37.59 9.14 5.74 48 .000NAS Total 46.12 12.65 35.55 10.78 6.75 48 .000Regulation 54.96 14.49 64.29 10.18 –4.14 48 .000PI Total 44.84 12.07 36.02 10.78 5.86 48 .000
Chapter 02_Chapter 02 4/16/13 11:02 AM Page 28

• Behavior: Asks about behaviors that are problematic or indicative of violence,including impulsive reactions.
• NAS Total: Cognitive + Arousal + Behavior.• Anger regulation: Asks about the adaptive aspects of the experience of anger
in terms of the ability to evaluate and direct angry responses in a construc-tive manner.
• Provocation inventory: Provides an index of anger intensity and generalityacross a range of provocations.
In sum, short-term outcomes were clinically significant in a positive direction. Thelong-term outcome is to keep YODA participants out of court and jail. To this date,none of the YODA program completers have reoffended.
Best Practice with Collaborative Community Programs
Evidence-based interventions are expected to transfer to other court systems bysimilar collaborations. The study provided information on innovative treatmentsfor families, as well as information to facilitate university-court collaborations.
Innovative Treatments
It should be noted that SFBT has not been used prior to this program with theYODA population. The three-phase approach is a unique design of assessment andtreatment. Assessment/case management builds toward individual treatment forthe youthful offender, and then the family is brought in for further work. To date,YODA is meeting short-term and long-term outcome goals as well as operating asintended. Clients have shown an increase in mental health, resilience, hope, andability to build solutions. Additionally, clients have shown a decrease in aggres-sion, along with drug and alcohol abuse.
University-Court Collaborations
This unique opportunity has provided a testing ground for a university-community collaboration. Of the clients who have successfully completed theprogram, court records indicate that none have reoffended in Tarrant County.
Future Aims
A future aim is to expand YODA into other areas and to continue to test YODAas an evidence-based intervention using more sophisticated analytical techniquesand including comparison samples. Toward this end, a National Institute of Jus-tice grant has been submitted for expansion of this program into Dallas County.Other program components to be expanded and studied include the teleherencecomponent (Schoech, 2010) and the family component (Lehmann et al., 2012).The program has been presented at both national and international conferencesin an effort to network with other like-minded researchers and practitioners.
Youthful Offender Diversion Project: YODA 29
Chapter 02_Chapter 02 4/16/13 11:02 AM Page 29

ReferencesBerg, I. K. (1994). Family-based services: A solution-focused approach. New York:
Norton.Berg, I. K., & Dolan, Y. (2001). Tales of solutions: A collection of hope-inspiring
stories. New York: Norton.Berg, I. K., & Steiner, T. (2003). Children’s solution work. New York: Norton.Corcoran, J., & Pillai, V. J. (2009). A review of the research on solution-focused
therapy. British Journal of Social Work, 39(2), 234–242.De Shazer, S. (1985). Keys to solution in brief therapy. New York: Norton.De Shazer, S. (1988). Clues: Investigating solutions in brief therapy. New York:
Norton.European Brief Therapy Association. (2010). Solution-focused brief therapy evalu-
ation list. Retrieved November 16, 2010, from http.blog.ebta.nu/resources.Guerra, N. G., Kim, T. E., & Boxer, P. (2008). What works: Best practices with
juvenile offenders. In R. D. Hoge, N. G. Guerra, & P. Boxer (Eds.), Treatingthe juvenile offender (pp. 79–102). New York: Guilford.
Guerra, N. G., & Leaf, C. (2008). Implementing treatment programs in commu-nity and institutional settings. In R. D. Hoge, N. G. Guerra, & P. Boxer(Eds.), Treating the juvenile offender (pp. 103–126). New York: Guilford.
Lehmann, P., Jordan, C., Whitehill, K., Huynh, L., & Chigbu, K. (2012). Solution-focused brief therapy and criminal offending: A family conference tool forwork in restorative justice. Journal of Systemic Therapies, 31(4), 49–62.
Novaco, R. W. (2003). The Novaco Anger Scale and Provocation Inventory Manual.Los Angeles: Western Psychological Services.
Office of Juvenile Justice and Delinquency Prevention. (2008). Solution-focusedbrief therapy. Retrieved November 15, 2012, from www.ojjdp.gov/.
Saleebey, D. (2006). The strengths perspective in social work practice (4th ed.).Boston: Pearson.
Schoech, R. (2010). What happens when human service information is con-nected globally. Paper presented at the 1st International Forum on Virtual Teaching and Cyber Psychology, School of Psychology, NationalAutonomous University of Mexico, Mexico City.
Smock, S. A., McCollum, E., & Stevenson, M. (2010). The development of thesolution-focused inventory. Journal of Marital and Family Therapy, 36(4),499–510.
Ungar, M. (2007). Playing at being bad: The hidden resilience of troubled teens.Toronto, ON: McClelland and Stewart.
30 Best Practices in Mental Health
Chapter 02_Chapter 02 4/16/13 11:02 AM Page 30

The purpose of this study is to explore the knowledge and attitudes about autism spec-trum disorders among Hispanics in the Southwest. The study also examines perceivedbarriers in obtaining resources, and preferences in accessing health care. Participants(N = 169) were surveyed using the Autism Awareness Survey, which was developedspecifically for this research. Significant differences were found between individualswith high acculturation and low acculturation in exposure to autism, knowledge aboutautism, perceived barriers to obtaining resources and health care, and attitudes towardpeople with autism. Additionally, the findings suggest that, although the surveyed pop-ulation was knowledgeable about the symptoms associated with autism, they were lessknowledgeable about the etiology and course of the disorder. The research underscoresthe serious need for both Spanish educational resources and Spanish-speaking healthcare providers to address the needs of Hispanics with regard to autism, especially forindividuals with low levels of acculturation.
Key words: acculturation; Hispanics; knowledge of autism; public perceptions
According to the Centers for Disease Control and Prevention (CDC), autism is adevelopmental disorder related to atypical biology and chemistry within the brain(Rice, 2009). Symptoms vary, but include problems with social skills such as mak-ing friends and showing empathy, as well as difficulty with verbal and nonverbalcommunication. Because an early, intensive, and appropriate treatment programgreatly improves the outlook for most people with autism, the CDC considers itcrucial that children be correctly diagnosed when they are still young, preferablybefore the age of three.
The Full Spectrum: Hispanic Understanding of Autism
Heather Voelkel, Craig W. LeCroy, Lela Rankin Williams, and JaneHolschuh
Heather Voelkel is an academic success specialist at the School of Social Work, Arizona State Uni-versity, Phoenix, Arizona. Also at the School of Social Work, Arizona State University, Phoenix,Arizona, Craig W. LeCroy, PhD, is professor; Lela Rankin Williams, PhD, is assistant professor; andJane Holschuh, PhD, is lecturer.
© 2013 Lyceum Books, Inc., Best Practices in Mental Health, Vol. 9, No. 1, March 2013
Chapter 03_Chapter 03 4/16/13 11:03 AM Page 31

Autism prevalence statistics in the United States reveal that about 1 child inevery 127 of Hispanic ethnicity has an autism spectrum disorder (CDC, 2012).The prevalence of this disorder in the general population is considerably higher:one out of eighty-eight children is diagnosed with autism. It is uncertain whetherHispanic children are actually less affected by autism or whether the lack of accessto appropriate health care and autism services among Hispanic families causesthis disparity in diagnosis (CDC, 2012; Global Autism Public Health, 2010).
Although it is understood that the prevalence of autism spectrum disorders(ASD) is dramatically increasing, current literature does not document Hispanicunderstanding or awareness of these disorders. Additionally, the literature doesnot indicate whether Hispanics with low levels of acculturation have more diffi-culty accessing health care services than Hispanics with high levels of accultura-tion. It is possible that families do not seek treatment or care because they do notunderstand the symptoms or they do not have access to information concerningautism in their preferred language. Due to the paucity of literature in this area,research on this topic will contribute to the knowledge base concerning Hispanicunderstanding of autism and will help agencies more effectively tailor their ser-vices to meet the needs of this specific population.
Review of Literature
Although the rate of autism diagnosis for Hispanics is lower than that of thegeneral population, the literature indicates that the lower rate of autism diagnosisfor Hispanics relative to the general population results from sociocultural and eco-nomic factors, which include cultural stigma attached to diagnosis, dense popula-tion in high-poverty areas with less access to care, fear of deportation, and lan-guage complications (Bearman & Fountain, 2011; Durkin et al., 2010; Rice,2009). It is important to note that the literature shows that Hispanics with highersocioeconomic status have the same diagnosis rate for autism as white non-Hispanics, which may indicate that the disparity in autism prevalence rates isgreatly dependent on access to high-quality health care (Bearman & Fountain,2011; Durkin et al., 2010). However, the research does not explore how an indi-vidual’s level of acculturation may affect the cultural and economic barriers toaccessing health care services.
Barriers to Care
According to the literature, a variety of issues act as barriers to Hispanic pop-ulations accessing health care resources, including but not limited to Hispanicattitudes toward a system they perceive to be prejudiced, a lack of culturally andlinguistically competent agencies and workers, and a lack of resources in areas of high need (Alvarado, 2005; Bearman & Fountain, 2011; Durkin et al., 2010;Flores, 1984; Flores, Abreu, Oliver, & Kastner, 1998; Graf, Blankenship, Sanchez,& Carlson, 2007; Guendelsberger, 1992; Kraemer, 2010).
32 Best Practices in Mental Health
Chapter 03_Chapter 03 4/16/13 11:03 AM Page 32

Alvarado (2005) reports that Hispanic families tend to distrust professionalsand authorities. The research suggests that this mistrust arises out of a fear ofdeportation and an aversion to being marginalized and discriminated against(Alvarado, 2005; Bearman & Fountain, 2011; Durkin et al., 2010; Flores, 1984;Graf et al., 2007; Kraemer, 2010). In particular, the study from Southern Califor-nia by Bearman and Fountain substantiates this distrust. This study shows a directcorrelation between heated political campaigns regarding immigration issues andlower diagnosis of ASD among Hispanic populations. Once the political fervor diesdown, diagnosis numbers rise. Although the impact of political repression on theuse of services by children in immigrant families is not specific to autism, this dis-order may be particularly vulnerable because the diagnosis is based on behavioralsymptoms (Bearman & Fountain, 2011; Mandell & Novak, 2005).
Further, inequalities in the U.S. health care system create the likelihood ofunderdiagnosis among children of low-income parents (Alvarado, 2005; Durkinet al., 2010; Kraemer, 2010). A study by Durkin et al. (2010) found that childrendiagnosed with autism spectrum disorders are less likely to reside in census blockgroups classified as areas of poverty, and more likely to live in block groups withhigher adult educational achievement and a higher median household income. Itis notable that the study also indicates that black and Hispanic children are morelikely to live in areas of poverty, which suggests that these children are systemati-cally less likely to be diagnosed with autism. The implication is that the lower over-all prevalence of autism among these population groups is correlated with thelack of appropriate medical attention because areas of higher poverty are lesslikely to offer high-quality medical services (Durkin et al., 2010; Mandell et al.,2009).
High-poverty communities in which children with autism spectrum disordersare identified are often unprepared to meet the children’s needs (Jacobson &Mulick, 2000; Mandell & Novak, 2005; Newschaffer & Curran, 2003). Schools in wealthy sectors are able to hire professionals proficient in assessing studentsand to offer superior facilities that cater to the particular needs of the students(Kraemer, 2010). Schools in poor sectors generally cannot afford to offer suchcare. Other facilities face a similar predicament: Hospitals, clinics, and social workagencies in these poorer areas do not have the staffing or funding to offer the fullspectrum of care (Alvarado, 2005; Kraemer, 2010). Alvarado and Kraemerreport that Hispanics are twice as likely to report long delays in waiting rooms andunresponsive health care workers. Even if the resources are available, Hispanicfamilies often lack the health insurance and transportation necessary to takeadvantage of these health care programs (Flores et al., 1998).
Many Mexican Americans report that the number one barrier to accessinghealth care services is the inability to communicate with health care professionals(Alvarado, 2005; Flores et al., 1998; Mandell & Novak, 2005). Although many ofthese Spanish-speaking individuals qualify for assistance, they often are unawareof the availability of services because they cannot communicate with those who
The Full Spectrum: Hispanic Understanding of Autism 33
Chapter 03_Chapter 03 4/16/13 11:03 AM Page 33

are knowledgeable about the programs or with the professionals on-site. Miscom-munications in a hospital setting can result in adverse health consequences,which include poor medical care, misdiagnosis, and inappropriate medication andhospitalization (Flores et al., 1998).
There are many gaps in the literature pertaining to Hispanic families and ASD.One area that merits further study is whether Hispanic populations are familiarwith autism and its symptoms. The literature does not address Hispanic awarenessof autism, nor does it discuss whether or how people from a Hispanic backgroundmay perceive the symptoms of autism differently from members of the main-stream white, non-Hispanic culture in the United States. Ethnic minorities may beless likely to view symptoms of autism as related to a health condition and, there-fore, may be less likely to seek care through public medical systems. Moreover, Hispanics may perceive autism as socially embarrassing and may be less likely to seek assistance. Additionally, the literature does not thoroughly examinewhether autism prevalence is truly higher among non-Hispanics or whether non-Hispanics are simply more frequently diagnosed. There has been insufficientresearch comparing the prevalence rates of autism diagnosis among Hispanicsand non-Hispanics of equal socioeconomic status. Finally, the literature does notaddress how acculturation levels of Hispanics may affect their awareness ofautism. Hispanic families that are more highly acculturated may have a betterunderstanding of autism than families that have recently immigrated to theUnited States. The identified sociocultural and economic barriers may be far moreinsurmountable for Hispanics with low levels of acculturation than for Hispanicswith high levels of acculturation.
The research described in this article will examine the relationship betweenacculturation and autism awareness, knowledge about symptoms associated withand etiology of autism, and attitudes toward individuals with autism. Addition-ally, the study will seek greater understanding concerning how Hispanics perceiveaccess to health care services.
Method
Instrumentation
The Autism Awareness Survey was constructed based in part on questions usedin previous studies (for example, British Social Attitudes Survey, Staniland, 2009;Questions about Disability Survey, Graf et al., 2007; and The Acculturation Rat-ing Scale for Mexican Americans–Short Form, Dawson, Crano, & Burgeon, 1996),as well as questions reflective of commonly held attitudes and understandingsconcerning autism.
The survey is composed of fifty-three questions and addresses people’s under-standing of key characteristics or behaviors associated with autism, exposure topeople with autism, awareness and attitudes toward health services, and accul-turation levels. Five yes-or-no questions and one fill-in-the-blank question at thebeginning of the survey seek to establish people’s exposure to autism (see table 1).
34 Best Practices in Mental Health
Chapter 03_Chapter 03 4/16/13 11:03 AM Page 34

The first and third sections of the survey consist of eighteen Likert scale questions(rated on a five-point scale of strongly disagree, disagree, neither agree nor disagree,agree, and strongly agree), which seek to determine perceived attitudes toward peo-ple with autism (see table 2) and perceived barriers to accessing resources andhealth care (see table 3). Twelve true or false questions ascertain levels of knowl-edge about autism (see table 4).
The Full Spectrum: Hispanic Understanding of Autism 35
Table 2 Responses to Items Related to Perceived Attitudes toward People with Autisma
NeitherStrongly agree nor Stronglyagree Disagree disagree Agree agree
Item % n % n % n % n % n
1. People with autism are (15.2) 25 (13.4) 22 (19.5) 32 (34.1) 56 (17.7) 29ignored by other people
2. People with autism are (9.8) 16 (11.0) 18 (15.2) 25 (39.0) 64 (25.0) 41isolated from other people
3. People with autism (11.1) 18 (35.2) 57 (24.7) 40 (24.7) 40 (4.3) 7stay at home
4. People with autism are (12.8) 21 (31.1) 51 (28.0) 46 (20.1) 44 (7.9) 13hidden from other people
5. People don’t know (7.8) 13 (10.2) 17 (15.1) 25 (48.2) 80 (18.7) 31what to say to people with autism
6. People are comfortable (16.9) 28 (29.5) 49 (28.9) 48 (22.3) 37 (2.4) 4around people with autism
7. People avoid interacting (6.6) 11 (17.5) 29 (33.1) 55 (31.9) 53 (10.8) 18with people with autism
8. People feel sorry for (12.7) 21 (16.3) 27 (16.3) 27 (36.7) 61 (18.1) 30people with autism
9. People don’t interact (12.2) 20 (26.8) 44 (23.2) 38 (28.7) 47 (9.1) 15with people with autism because they are too different
10. I believe that people (14.0) 23 (14.6) 25 (20.1) 33 (29.3) 48 (22.0) 36with autism are discriminated against because of their condition
aValid percentages are used in the table; three to seven responses are missing for each question.
Table 1 Response to Items Relating to Exposure to Autisma
Yes NoItem
% n % n
1. Have you ever heard of autism? (89.3) 150 (10.7) 182. Have you ever met anyone with autism? (63.7) 107 (36.3) 613. Have you ever read about autism in a magazine or newspaper? (59.8) 98 (40.2) 664. Have you ever heard anyone on television talk about autism? (82).0 137 (18).0 305. Do you know anyone with autism? (57.1) 92 (42.9) 69
aValid percentages are used in the table; one to five responses are missing for each question.
Chapter 03_Chapter 03 4/16/13 11:03 AM Page 35

Section four is an eleven-question acculturation rating scale that aims to estab-lish people’s level of acculturation to mainstream, English-speaking, white, non-Hispanic culture in the United States and includes questions related to language,activity preferences, and group identity (rated on a six-point scale of none, some-times, moderate, a lot or very often, very much, and all the time). This scale is based on the Acculturation Rating Scale for Mexican Americans–Short Form (Dawsonet al., 1996), which is a standardized measure specifically geared for the MexicanAmerican population and has strong reliability (α = .96).
Once the Autism Awareness Survey was completed, the researchers developeda Spanish version of the instrument to meet the linguistic needs of the intendedpopulation. A native-Spanish-speaking researcher completed the initial transla-
36 Best Practices in Mental Health
Table 3 Responses to Items Related to Perceived Barriers to Accessing Health Care
NeitherStrongly agree nor Stronglyagree Disagree disagree Agree agree
Item % n % n % n % n % n
1. If my child were diagnosed (12.2) 20 (0.6) 1 (12.2) 20 (39.6) 65 (15.2) 25with autism, I would know where to go for help
2. If my child were diagnosed (29.3) 48 (40.9) 67 (11.0) 18 (15.9) 26 (3.0) 5with autism, I would not use health services because my family is able to take care of the things I need
3. If I needed services for my (9.2) 15 (8.6) 14 (16.6) 27 (42.9) 70 (22.7) 37child with autism, I would be able to find health services that really care about my family
4. If my child were diagnosed (6.9) 11 (6.9) 11 (15.0) 24 (46.3) 74 (25.0) 40with autism, I would be able to get the care I needed for him or her
5. If my child were diagnosed (7.5) 12 (13.1) 21 (14.4) 23 (39.4) 63 (25.6) 41with autism, I would be concerned I wouldn’t be able to afford the care he or she needs
6. If my family needed help, (9.4) 15 (16.4) 26 (23.9) 38 (35.2) 56 (15.1) 24I would be concerned that professionals would not listen to my opinion
7. If my child were diagnosed (4.3) 7 (4.3) 7 (22.8) 37 (37.0) 60 (31.5) 51with autism, I would want the service professionals to speak Spanish
8. If my family needed help (5.0) 8 (16.1) 26 (22.4) 36 (37.3) 60 (19.3) 31from service professionals, I would be worried that they wouldn’t spend the time to provide me the help I needed
Chapter 03_Chapter 03 4/16/13 11:03 AM Page 36

tion of the survey. Two other native-Spanish-speaking professionals then reviewedthe survey, giving special attention to word choice (to incorporate local dialect)and sentence construction (to decrease the formality of the language). A forwardand backward translation of the survey instrument was also completed to mini-mize translation errors.
Statistical Analysis
The researchers completed a primarily exploratory analysis of the data. A reli-ability analysis was conducted and used to create five scales. First, a scale was cre-ated to address perceived barriers to accessing resources and health care, withhigher scores indicating greater perceived barriers (three items; α = .75):
• I would know where to go for help if my child were diagnosed with autism• I would be able to find health services that really care about my family• I would be able to get the care I need for my child
Next, a scale was created to examine preferences concerning health care services(four items; α = .68):
• I would want service professionals to speak Spanish• I would be concerned that I would not be able to afford health care if my child
were diagnosed with autism• I would be concerned that professionals would not listen to the family’s
opinion• I would be concerned that professionals wouldn’t spend the necessary time
to provide my family the help we needed
The Full Spectrum: Hispanic Understanding of Autism 37
Table 4 Responses to Item Related to Knowledge about Autism
True and false questionsa % correct
1 Most children with autism have difficulty reading facial expressions. (T) 65.02 With proper treatment, most children with autism outgrow the disorder. (F) 39.63 Children with autism often avoid eye contact. (T) 71.04 Children with autism often have unusual behavior patterns
(like flapping their arms or tapping). (T) 79.35 Children with autism often talk excessively about one or two topics. (T) 63.36 Emotional trauma plays a major role in causing autism. (F) 53.87 Children with autism generally prefer predictability. (T) 60.48 Children with autism are generally attuned to other people’s
feelings and emotions. (F) 42.09 Autism is caused by vaccinations. (F) 69.8
10 Autism is more frequently diagnosed in males than females. (T) 48.511 Children with autism tend to resist being held or touched. (T) 66.912 Autism is primarily a genetic disorder. (T) 36.1
aCorrect true (T) or false (F) answers are in parentheses.
Chapter 03_Chapter 03 4/16/13 11:03 AM Page 37

A third scale was used to investigate perceived negative attitudes toward peoplewith autism (ten items; α = .80). The items on this scale were modeled after a sur-vey by Graf and colleagues (2007), entitled Questions about Disability Survey.Items on this scale included people with autism are ignored by other people and peoplefeel sorry for people with autism.
The fourth scale examined the participant’s knowledge about the symptomsand etiology of autism (twelve items). The scale was a sum score of responses,with correct answers receiving a 1 and incorrect answers receiving a 0. Finally,the fifth scale addressed the respondent’s level of acculturation (Dawson et al.,1996) and included eleven items, α= .96. Items on this scale include I enjoy speak-ing English and my thinking is done in the Spanish language. More positive scores (rating 0 or above on the scale) indicate high levels of acculturation, whereas lowscores (rating below 0) indicate low levels of acculturation.
Independent t-tests were used to examine differences between the responses ofindividuals with high acculturation and those of individuals with low accultura-tion with respect to the variables that measure knowledge about autism, perceivednegative attitudes toward people with autism, perceived barriers that preventaccess to resources and health care, and preferences concerning health care ser-vices. Chi-square tests were used to compare individuals with high and low levelsof acculturation concerning exposure to people with autism.
Procedures
The research team consisted of one researcher and three research assistantswho are bilingual (Spanish and English) and one research assistant who is mono-lingual (Spanish). The research team created a list of public locations in a varietyof areas around Tucson, Arizona, with the intention of collecting data from indi-viduals with disparate socioeconomic, education, and acculturation levels. Someof the collection areas included grocery stores, fast food restaurants, departmentand outlet stores, and a local mall. Each member of the research team was respon-sible for several locations to cover a broad geographical area.
Inclusion criteria for the survey included age greater than eighteen and self-identification as Hispanic or Latino. The researchers asked potential participants ifthey spoke English or Spanish and if they would be interested in taking part in asurvey designed to help social service and health care agencies offer better care tothe population living in Southern Arizona. If the individual met the inclusion cri-teria, he or she was invited to complete the survey. Before completing the survey,participants were given an informed consent letter, as required by the InstitutionalReview Board. The researchers made themselves available to participants in orderto answer questions, read the surveys aloud if requested, and collect the surveys.Seven participants asked the researchers to read the survey aloud. In all sevencases, the Spanish version of the survey was requested. Two participants citedpoor vision and five participants cited low literacy as the reason for requesting thisaccommodation. After the survey was completed, the researchers held aside forty-
38 Best Practices in Mental Health
Chapter 03_Chapter 03 4/16/13 11:03 AM Page 38

one surveys from people who did not meet inclusion criteria. (One was set asidebecause the participant did not meet the age requirement; forty were set asidebecause the participants did not self-identify as Hispanic or Latino.)
Results
Of the 169 surveys completed by individuals who self-identified as Hispanic,108 (63.9%) were completed in Spanish and 61 (36.1%) were completed in Eng-lish. Of those individuals with high acculturation, 58.1 percent chose to com-plete the survey in English, whereas, of those individuals with low acculturation,only 13.4 percent chose to complete the survey in English. The results presentedbelow include statistics describing the demographics of the participants and sta-tistics of items related to exposure to autism. Additionally, frequency data andsignificant differences between responses of individuals with high acculturationand low acculturation are presented pertaining to attitudes toward people withautism, barriers to accessing resources and health services, and knowledge aboutautism.
Participant Demographics
Descriptive statistics examined the age, gender, education, employment, andmarital status of the participants. The sample was largely female (81.1%). Theyoungest participant was eighteen, whereas the oldest was seventy-nine. Themean age of participants was forty. In terms of marital status, 47.9 percent weremarried, 5.3 percent had a domestic partner, 32 percent were single, 7.1 percentwere divorced, 5.9 percent were separated, and 1.8 percent did not respond. Lev-els of education ranged from completion of grades one through five to completionof graduate-level work. Forty-four percent of the participants reported havingcompleted grade twelve or less. Of those with high acculturation, 70.9 percenthad completed at least some college, as compared to those with low acculturation,of whom only 40.2 percent had completed at least some college. With regard toemployment, 39.1 percent worked full time, 13.6 percent worked part time, 12.4percent were unemployed, 30.2 percent were homemakers, and 4.7 percent didnot respond to the question.
Exposure to Autism
The first section of the Autism Awareness Survey related to exposure to autism(see table 1). The overwhelming majority (89.3%) indicated that they had heard ofautism, whereas only 57.1 percent reported that they personally knew someonewith autism. Significantly more people reported having heard about autism ontelevision (82%) than having read about autism in a magazine or newspaper(59.8%). In response to the question, “What percentage of people do you think getautism?” the average response was 25.7 percent of the population, which is farabove the actual rate of diagnosis of 1 percent of the population.
The Full Spectrum: Hispanic Understanding of Autism 39
Chapter 03_Chapter 03 4/16/13 11:03 AM Page 39

Chi-square comparisons were performed to assess the differences in exposure toautism between individuals with high acculturation and individuals with lowacculturation. Significant differences were found in the responses of those withhigh acculturation and low acculturation for the question pertaining to havingmet someone with autism. The number of people with low acculturation who hadmet someone with autism (56.1%) was significantly lower than for those withhigh acculturation (71.8%), x2(1) = 4.45, p = .04, phi = .16. There was also a significant difference found in responses to the question about whether they hadread about autism in a magazine or newspaper. Those with low acculturation hadless affirmative responses (50.6%) than those with high acculturation (67.9%),x2(1) = 5.01, p = .02, phi = .18. A trend toward significance was found in the com-parisons of responses about personally knowing anyone with autism. Those withhigh acculturation reported knowing people with autism more often (64.3%)than those with low acculturation (50%), x2(1) = 3.33, p = .07, phi = .14. Therewere no significant differences between the responses of those with high accul-turation and those with low acculturation to the questions about having heard ofautism (89.4% vs. 89%) or hearing anyone on television talk about autism(79.8% vs. 84.1%).
Perceived Negative Attitudes
The responses in the section of the survey about perceived negative attitudestoward people with autism highlighted fairly strong views about how societyinteracts with people with autism (see table 2). Most notably, over 60 percent ofthe respondents agreed or strongly agreed that people don’t know what to say toindividuals with autism (66.9%) and that people with autism are isolated fromothers (64%). Additionally, more than half of the respondents agreed or stronglyagreed that people with autism are ignored by others (51.8%) and that people feelsorry for people with autism (54.8%). More than half of the respondents indicatedthat they believed that people with autism are discriminated against because oftheir condition (51.3%).
To determine if there were differences in perceived attitudes toward people withautism between individuals with high acculturation and individuals with lowacculturation, the questions concerning attitudes were examined using t-testanalysis. Significant differences were found between the responses of those withhigh acculturation and those with low acculturation (see figure 1). Individualswith low acculturation indicated that they perceived less negative attitudes towardpeople with autism (M = 3.03, SD = 0.69) than those with high acculturation (M = 3.40, SD = 0.70), t(164) = –3.44, p = .001.
Perceived Barriers and Preferences for Care
There were varied responses to the survey questions pertaining to perceivedbarriers to accessing resources and health care services (see table 3). The largestperceived barriers pertained to finances and language. More than 60 percent of
40 Best Practices in Mental Health
Chapter 03_Chapter 03 4/16/13 11:03 AM Page 40

the respondents agreed or strongly agreed that, if their child were diagnosed withautism, they would be concerned that they would not be able to afford the neces-sary health care services (65%) and that they would want the health care profes-sional to speak Spanish (68.5%). Additionally, 56.6 percent indicated that theywould be concerned that the health care provider would not spend the time nec-essary to provide the family with quality care. On the other hand, over half therespondents indicated that they would know where to go for help if their childwere diagnosed with autism (54.8%) and that they would feel confident that theywould be able to get the care they needed for the child (71.3%).
In order to examine differences in perceived barriers to accessing resources andhealth care services between individuals with high acculturation and individualswith low acculturation, the questions concerning access to resources and healthcare were examined using t-test analysis. Significant differences were foundbetween the responses of those with high acculturation and those with low accul-turation (see figure 1). Individuals with low acculturation indicated that they per-ceived more barriers in accessing resources and health care services (M = 2.70,SD = 1.01) than those with high acculturation (M = 2.27, SD = 0.96), t(161) =2.74, p = 0.07. On the other hand, there were no significant differences in theresponses of those with low acculturation (M = 3.65, SD = 0.85) and those withhigh acculturation (M = 3.50, SD = 0.79) regarding specific preferences abouthealth care services (see figure 1), t(160) = 1.16, p = .25.
The Full Spectrum: Hispanic Understanding of Autism 41
Figure 1 Comparison of Responses to Perceived Barriers, Preferences,and Negative Attitudes
Note: * indicates significant statistical differences in responses between individuals with high acculturationand individuals with low acculturation.
Resp
onse
s to
Lik
ert-
scal
e qu
estio
ns,
1 =
str
ongl
y di
sagr
eean
d 5
= s
tron
gly
agre
e
Perceived Barriers* Preferences Negative Attitudes*
LowAcculturation
HighAcculturation
Chapter 03_Chapter 03 4/16/13 11:03 AM Page 41

Knowledge about Autism
Results from the true and false section of the survey demonstrated that therespondent sample had some understanding of the symptoms associated withautism (see table 4). The majority were able to identify that children with autismhad difficulty reading facial expressions (65%), often avoid eye contact (71%),often have unusual behavior patterns (79.3%), talk excessively about one or twotopics (63.3%), prefer predictability (60.4%), and often resist being held ortouched (66.9%). However, only 42 percent of the respondents correctly indicatedthat children with autism are not generally attuned to other people’s feelings andemotions.
The sample responses also suggested that the etiology and course of autism isless well known among the survey participants. Many respondents (60.4%) incor-rectly believed that children with autism could outgrow the disorder and thattrauma plays a major role in causing autism (46.2%). Additionally, only 36.1 per-cent of the respondents recognized autism as a genetic disorder. It is notable, how-ever, that 69.8 percent did correctly identify that vaccines do not cause autism.
To determine if there were differences in responses between individuals withhigh and low acculturation, the questions concerning knowledge were examinedusing t-test analysis. Significant differences were found between the responses of those with high acculturation and those with low acculturation. Individualswith low acculturation on average demonstrated less knowledge about autism (M = 6.60, SD = 2.09) than those with high acculturation (M = 7.98, SD = 2.07),t(157) = –4.16, p = .001.
Discussion
Researchers have found that Hispanics in the United States perceive more bar-riers to accessing health care than their white, non-Hispanic contemporaries(Alvarado, 2005; Bearman & Fountain, 2011; Durkin et al., 2010; Flores, 1984;Flores et al., 1998; Graf et al., 2007; Guendelsberger, 1992; Kraemer, 2010). Theresults of this study build on past research by delineating significant differences inthe perceived barriers to care between Hispanics with low acculturation and His-panics with high acculturation. The findings are not surprising, but this studyclearly demonstrates that Hispanics with low acculturation perceive more barriersto accessing health care than those with high acculturation. Speculatively, it couldbe that Hispanics with high acculturation perceive fewer barriers to care becausethey can communicate more confidently in English with health care professionalsand have higher English literacy, meaning that they can access publicly dissemi-nated literature and information more easily.
This research additionally contributes information on the previously unexam-ined topic of Hispanics’ level of exposure to autism. Hispanics with low accultur-ation reported significantly less exposure to autism than Hispanics with highacculturation in their responses to the questions pertaining to having met some-one with autism, having read about autism, and personally knowing someone
42 Best Practices in Mental Health
Chapter 03_Chapter 03 4/16/13 11:03 AM Page 42

with autism. Interestingly, there were no significant differences in the responsesabout having heard of autism. This may indicate that some information concern-ing the disorder has effectively circulated to the Hispanic population. On the otherhand, the lack of direct contact with people with autism and the lack of exposureto written material concerning autism may indicate that Hispanics with lowacculturation have only a cursory understanding of autism, and that there needsto be more effort in offering education about the specifics of the disorder.
This supposition is supported by the data addressing knowledge about autism.Hispanics with low acculturation knew significantly less about autism than thosewith high acculturation. Although all the respondents had fairly accurate under-standing of the symptoms associated with autism, they had less knowledge aboutthe etiology and course of the disorder. More specifically, close to 60 percent ofthe survey participants inaccurately believed that those with autism would even-tually outgrow the disorder; only 36.1 percent knew that autism is a primarilygenetic disorder, and 46.2 percent believed that trauma plays a large role in caus-ing autism. This lack of knowledge concerning the etiology of autism may beindicative of a larger problem concerning the issue of culpability associated withautism. In other words, people feel that the parents of a child with autism musthave done something wrong in their parenting to somehow cause the disorder.This perception of culpability is problematic, not only because it is incorrect, butalso because it connects feelings of shame and guilt to autism such that familiesmay be less likely to seek help because they feel that society will blame them forthe problem.
The findings of this research correspond to and affirm the assertions ofAlvarado, Mandell and Novak, and others that language is the number one bar-rier that keeps Hispanics from accessing health care services. Even though thisstudy was conducted in a city close to the Mexican-American border where highlevels of multicultural awareness and outreach would be assumed, there remaingreat disparities in the accessibility of resources between people who have fluencyin the English language and those who do not. Moreover, this study again confirmsthe findings of Jacobson and Mulick, Mandell and Novak, and Newschaffer andCurran that the cost of health care is one of the primary barriers keeping peoplefrom accessing the health services they need.
Some limitations are evident with this study. First, the researchers used a sam-ple of convenience, which is a nonprobability approach; therefore, the responsesmay not be truly representative of the target population. Additionally, the smallnumber of participants limits the external validity and generalizablity of the study.Another limitation of the study is that the survey instrument was newly developedand therefore could be lacking validity. A final limitation of the research is that theSpanish translation of the survey may not use the most appropriate dialect for thepopulation surveyed, which may affect the participants’ understanding of thequestions and therefore influence the responses. To minimize this limitation,researchers did forward and backward translations of the survey and severalnative Spanish speakers collaborated to ensure the best possible word choice.
The Full Spectrum: Hispanic Understanding of Autism 43
Chapter 03_Chapter 03 4/16/13 11:03 AM Page 43

Best Practices for Working with Families with Autism
Although previous studies have examined perceived barriers that keep Hispan-ics from accessing health care, the strength of the research presented in this arti-cle is that, in addition to confirming the findings from prior studies, it alsoaddresses previously unexamined topics such as Hispanics’ exposure to autismand knowledge about the symptoms and etiology of autism, and it differentiatesbetween Hispanics with high and low levels of acculturation. This exploratorystudy can act as a foundation for further research, and it highlights the impor-tance of continued investigation concerning autism and the Hispanic population.
The implications of this research for social work and health care practitionersare far-reaching. Once again, it has been demonstrated that the primary barrierskeeping Hispanic families from accessing health care services are language andfinances—the same barriers that researchers have identified for this populationfor the last twenty years (Alvarado, 2005; Bearman & Fountain, 2011; Durkin etal., 2010; Flores, 1984; Flores et al., 1998; Guendelsberger, 1992; Kraemer,2010). It seems that there has been little progress in the development of culturallyappropriate and cost-efficient services. The cost of health care has been the topicof national debate, yet there has been no tangible movement to reduce the cost ofhealth services, particularly for the uninsured and underinsured. Additionally,with the upcoming, highly politicized changes to the diagnostic criteria for autismspectrum disorders within the Diagnostic and Statistical Manual for Mental Disorders(American Psychiatric Association, 2000), many families who currently receivesupport through the Department of Developmental Disabilities may cease to qual-ify for assistance, leaving the financial burden of care entirely on the family. Thisresearch again highlights the uncertainty felt by the general public and the needfor professionals to engage in national dialogue and advocacy for the marginalizedpopulations in our communities. This study supports the actions of practitionersas they consider the broader implications of their work and underscores the needfor advocacy in addressing social problems.
The other primary barrier to care pertains to language, that is, the lack ofSpanish-speaking health care professionals and the lack of Spanish informationand literature concerning autism. There are clear implications for mezzo-levelsocial work practice; in particular, health care programs need to broaden servicesthat address the specific cultural needs within their communities. In the South-west, this means making health care services equally accessible to English- andSpanish-speaking populations. Although it seems that this community is gener-ally aware of autism as a concept, education about autism, specifically aboutissues concerning culpability, is clearly necessary. Without addressing the stigmaof the disorder, vast numbers of those with autism spectrum disorders are unlikelyto receive the care they need during the prime treatment years, and will reachadulthood without the skills to effectively engage with the world around them.
44 Best Practices in Mental Health
Chapter 03_Chapter 03 4/16/13 11:03 AM Page 44

This research should remind health and education professionals of the uniqueneeds of the diverse populations within this country, which must be met withequitable and appropriate care.
ReferencesAlvarado, I. (2005). An analysis of the participation of immigrant Mexican mothers
in their child’s early intervention program (Doctoral dissertation). The Uni-versity of Georgia, Athens, Georgia. Retrieved from www.fcs.uga.edu/ss/docs/alvardo_maria_i_200512_phd.pdf.
American Psychiatric Association. (2000). Diagnostic and statistical manual ofmental disorders (4th ed., text rev.). Washington, DC: Author.
Bearman, P., & Fountain, C. (2011). Risk as a social context: Immigration policy and autism in California. Sociological Forum, 26(2), 215–240. doi: 10.1111/j.1573-7861.2011.01238.x.
Centers for Disease Control and Prevention. (2012). New data on autism spectrumdisorders. Retrieved from www.cdc.gov/features/countingautism.
Dawson, E. J., Crano, W. D., & Burgeon, M. (1996). Redefining the meaning andmeasurement of acculturation: Revisiting a novel methodologicalapproach. Journal of Intercultural Relations, 20(1), 97–114.
Durkin, M. S., Maenner M. J., Meaney, F. J., Levy, S. E., DiGuiseppi, C., Nicholas, J. S., . . . Schieve, L. A. (2010). Socioeconomic inequality in the preva-lence of autism spectrum disorder: Evidence from a U.S. cross-sectionalstudy. PLoS ONE, 5(7). e11551. doi: 10.1371/journal.pone.0011551.
Flores, E. (1984). Research on undocumented immigrants and public policy.International Migration Review, 18(3), 505–523.
Flores, G., Abreu, M., Oliver, M. A., & Kastner, B. (1998). Access barriers tohealth care for Latino children. Archives of Pediatric Adolescent Medicine,152(11), 19–25.
Global Autism Public Health. (2010). Autism Awareness Month highlighted byprogress in Mexico, Brazil and Aruba. Retrieved from http://www.autismspeaks.org/science/global-autism-public-health.
Graf, N., Blankenship, C., Sanchez, G., & Carlson, R. (2007). Living on the line:Mexican and Mexican American attitudes toward disability. RehabilitationCounseling Bulletin, 50(3), 153–165.
Guendelsberger, J. (1992). Access to citizenship for children born within thestate to foreign parents. The American Journal of Comparative Law, 40(2),379–429.
Jacobson, J., & Mulick, J. (2000). System and cost research issues in treatmentsfor people with autistic disorders. Journal of Autism and Developmental Disorders, 30(6), 585–593.
The Full Spectrum: Hispanic Understanding of Autism 45
Chapter 03_Chapter 03 4/16/13 11:03 AM Page 45

Kraemer, R. (2010). Special education placement factors for Latino students (Unpub-lished doctoral dissertation). University of Arizona, Tucson, AZ.
Mandell, D. S., & Novak, M. (2005). The role of culture in families’ treatmentdecisions for children with autism spectrum disorders. Mental Retardationand Developmental Disabilities Research Reviews, 11(2), 110–115. doi:10.1002/mrdd.20061.
Mandell, D. S., Wiggins, L. D., Carpenter, L. A., Daniels, J., DeGuiseppi, C., Durkin,M. S., . . . Kirby, R. S. (2009). Racial/ethnic disparities in the identifica-tion of children with autism spectrum disorders. American Journal of Public Health, 99(3), 493–498. doi: 10.2105/AJPH.2007.131243.
Newschaffer, C., & Curran, L. (2003). Autism: An emerging public health prob-lem. Public Health Reports, 118(5), 393–399.
Rice, C. (2009). Prevalence of autism spectrum disorders: Autism and developmentaldisabilities monitoring network, United States, 2006 (pp. 1–21). Washing-ton, DC: Department of Health and Human Services, Centers for DiseaseControl and Prevention.
Staniland, L. (2009). Public perceptions of disabled people: Evidence from the BritishSocial Attitude Survey. London: Office of Disability Issues. Retrieved fromwww.Odi.dwp.gov.uk/docs/res/ppdp.pdf.
46 Best Practices in Mental Health
Chapter 03_Chapter 03 4/16/13 11:03 AM Page 46

There is a need to reexamine how universities can promote holistic and balanced devel-opment of university students. Based on the positive youth development approach, it isargued that promotion of psychosocial competencies and positive mental health attrib-utes such as resilience, emotional competence, self-understanding, and interpersonalskills is an important strategy to facilitate holistic development of university studentsin Hong Kong. A credit-bearing course entitled Tomorrow’s Leaders was developed atThe Hong Kong Polytechnic University and piloted twice in response to this require-ment. Findings based on various evaluation strategies, including objective and subjectiveoutcome evaluations, process evaluation, and qualitative evaluation consistentlyshowed that this course was able to promote the psychosocial competencies and positivemental health of the students.
Key words: Chinese adolescents; formal curriculum; positive youth development;psychosocial competencies; university students
Developmental Problems in University Students and the Role of Universities
A survey of the literature showed that university students face many develop-mental issues. Shek and Wong (2011) reviewed developmental issues such asmental health problems, substance abuse, and egocentric behavior of university
Promotion of Holistic Development in University Students: A Credit-Bearing Course onLeadership and Intrapersonal Development
Daniel T. L. Shek
Daniel T. L. Shek, PhD, BBS, JP, is chair professor in the Department of Applied Social Sciences,Hong Kong Polytechnic University. The development of the course Tomorrow’s Leaders and theevaluation study were financially supported by Hong Kong Polytechnic University via the Teach-ing Development Grant and the funding for the 3-3-4 new curriculum. The author would also liketo thank the Wofoo Foundation for the establishment of several scholarships for outstanding stu-dents taking the course. Members of the Curriculum Development Team include Daniel Shek,Rachel Sun, Yat Hung Chui, Dorcas Allen, Ceci Ma, Lu Yu, Yida Chung, Yammy Chak, Pik FongTsui, Moon Law, and Winnie Fung.
© 2013 Lyceum Books, Inc., Best Practices in Mental Health, Vol. 9, No. 1, March 2013
Chapter 04_Chapter 04 4/16/13 11:03 AM Page 47

students. Several phenomena were revealed by the review. First, there were men-tal health issues confronting university students. For example, Blanco et al.(2008) found that the prevalence rates for alcohol use and personality disordersin university students were 20.4 and 17.7 percent, respectively. As Mowbray et al.(2006) pointed out, “averaging across a number of studies, it appears that approx-imately 12–18% of students on college campuses have a diagnosable mental dis-order” (p. 227). Suicide was the second leading cause of death among college stu-dents in the United States after homicides and accidents (Barrios, Everett, Simon,& Brener, 2000).
Second, there was a gradual drop in empathy and rising narcissistic personal-ity characteristics among university students. For example, studies revealed thatthere was an overall increase in narcissism across the cohorts of university stu-dents (Twenge & Foster, 2008; Twenge, Konrath, Foster, Campbell, & Bushman,2008). There were also research findings showing that university students havebecome more self-focused and financially oriented, but less engaged in socialresponsibility and civic participation. In a recent New York Times article titled “Students Are Different Now,” Bips (2010) asserted that “students now are lessmature and often not ready for the responsibility of being in college . . . many stu-dents today lack the resilience and are unable to summon strategies to cope . . .many students are often not prepared to be young ‘adults’ with all the responsi-bilities of life.”
With particular reference to Hong Kong, Shek (2010) highlighted several phe-nomena regarding the development of university students in Hong Kong. First,research findings show that the mental health of university students is a concern.For example, Wong, Cheung, Chan, Ma, and Tang (2006) showed that the rates ofpsychological morbidity in first-year postsecondary (tertiary) education studentsin Hong Kong were high. In a study conducted by the Hong Kong Tertiary Insti-tutions Health Care Working Group (2007), roughly half of the respondents dis-played excessive anxiety problems. In fact, there are findings indicating thatroughly one-fifth of young people in Hong Kong have various mental health con-cerns (Shek, Ma, & Sun, 2011).
In another recent review of developmental issues in university students, Shekand Cheung (in press) highlighted that there are several issues that deserve atten-tion. First, there are behavioral and lifestyle issues in university students in HongKong. Findings showed that alcoholism among university students in Hong Konggradually worsens throughout their university lives. Additional evidence showedthat viewing pornography on the Internet was prevalent among male universitystudents in Hong Kong. Moreover, university students encountered sleeping prob-lems: 68.6 percent of students had insomnia and 40 percent rated their sleepquality as poor. Finally, research showed that dating violence in Hong Kong uni-versity students was more prevalent than reported in other countries.
Mental health issues in university students also deserve attention. Chan,Tiwari, Leung, Ho, and Cerulli (2007) found that the rate of suicidal ideation
48 Best Practices in Mental Health
Chapter 04_Chapter 04 4/16/13 11:03 AM Page 48

among a university student sample was 41 percent, which was higher than thepercentage reported in the Western literature. Regarding depression, Song et al.(2008) compared Hong Kong students with Beijing students and found that moreHong Kong students suffered from depressive symptoms. University students hadpersonal goal and self-confidence problems, and they showed materialistic andpragmatic values. Finally, there were signs of egocentrism and lack of civicresponsibilities in university students.
With reference to the above-mentioned problems, universities have an obviousresponsibility to help students to develop holistically. It has been suggested thatcontemporary universities are unable to help students develop in a holistic man-ner. In the past two decades, books criticizing higher education have been pub-lished. In his book entitled The Closing of the American Mind, Bloom (1987) pointedout that the decline in emphasis on humanities, overemphasis on moral relativismand postmodernism, and disconnection between contemporary students and spir-itual and cultural roots (especially those in the Great Books) in contemporary uni-versities have adversely affected the total development of students. In his bookentitled The University in Ruins, Readings (1997) pointed out that the changingnature of universities has transited from the preservation of national culture toquantitative but empty benchmarks on excellence. Criticisms of contemporaryuniversities can also be found in Wilshire’s book The Moral Collapse of the Univer-sity (1990). His view is that academic professionalism and careerism have beenoveremphasized and that education, as well as the needs of the teachers and stu-dents, has been underemphasized.
In his book Our Underachieving Colleges, former Harvard president Derek Bok(2006) examined learning in undergraduate education. He concluded that stu-dents must catch up on critical thinking, quantitative skills, and moral reasoningto become well-informed citizens. In another book, Excellence without a Soul, HarryLewis, former dean and professor of Harvard University, argued that the funda-mental purpose of the university has been forgotten and its mission lost (2006).Lewis opined that general education courses lacked vision and mission, and thatstudents could not gain autonomy, resilience, and a sense of responsibility fromuniversity education. He also warned of the predominance of money as the dri-ving force for education, decision making, and consumer satisfaction. In short,one of Lewis’s key messages is that universities fail to nurture the holistic develop-ment of university students.
In a special issue focusing on contemporary tertiary education, Dalton andCrosby (2006) argued that the inner lives of university students are grosslyneglected in university education and that university education programs fail tohelp students to “make internal connections to the defining beliefs and purposesin their lives . . . since they do not reach that part of students’ lives where thingsreally matter” (p. 1). Astin and Sax (1998) also pointed out that there was anoveremphasis on intellectual outcomes but negligence toward holistic develop-ment in university students.
Promotion of Holistic Development in University Students 49
Chapter 04_Chapter 04 4/16/13 11:03 AM Page 49

The Quest for Holistic Development in University Students
Traditional mainstream adolescent developmental theories (e.g., Freudian the-ories) commonly focus on the developmental problems of adolescents. In responseto such theories, which emphasize adolescent pathologies, theorists in the fields ofpositive psychology and positive youth development (PYD) have argued that it isimportant to look at the bright side and the potentials of young people. Accordingto Damon (2004), in contrast to approaches that focus on youth developmentalissues such as depression and substance abuse, positive youth developmentemphasizes the talents, strengths, interests, and future potentials of children andadolescents. It also emphasizes the principle that “problem-free is not fully pre-pared” (Pittman, 1991) and developmental assets such as psychosocial compe-tencies are important in children and adolescents.
A survey of the literature shows that various PYD models propose differentdevelopmental assets or psychosocial competencies. Benson (1997) highlightedthe importance to adolescents of developing forty developmental assets, includingsocial competence (e.g., planning and decision making, interpersonal compe-tence, resistance skills, and peaceful conflict resolution) and positive identity (e.g.,sense of purpose, self-esteem, and positive view of personal future). Weissberg andO’Brien (2004) proposed that it is important to promote social-emotional compe-tencies, such as self-awareness, social awareness, self-management, relationshipskills, and responsible actions, to be nurtured in young people. Graczyk et al.(2000) similarly argued that the promotion of social and emotional learning (SEL)in adolescents is important. In the context of higher education, Bok (2006)asserted that university students should be nurtured to develop psychosocial skills,including communication, critical thinking, moral reasoning, preparation for cit-izenship, living with diversity, living in a global society, and preparation for work.
The concept of developmental assets such as psychosocial competence isclosely related to the concept of mental health or psychological well-being.According to Ryan and Deci (2001), psychological well-being is defined as “opti-mal psychological functioning and experience” (p. 142). The importance of thepositive dimension of mental health (i.e., not just absence of psychological prob-lems) is also highlighted by the World Health Organization (WHO; 2011), whichdefines mental health as
a state of well-being in which every individual realizes his or her own poten-tial, can cope with the normal stresses of life, can work productively and fruit-fully, and is able to make a contribution to her or his community. . . . The posi-tive dimension of mental health is stressed in WHO’s definition of health ascontained in its constitution: “Health is a state of complete physical, mentaland social well-being and not merely the absence of disease or infirmity.”
Obviously, developmental assets such as psychosocial competencies are integralcomponents of the positive dimension of mental health.
50 Best Practices in Mental Health
Chapter 04_Chapter 04 4/16/13 11:03 AM Page 50

Development of a Course on Tomorrow’s Leaders for Hong Kong University
Under the new four-year undergraduate curriculum at the Hong Kong Poly-technic University, students admitted in 2012 will be required to complete arequirement in leadership and intrapersonal development. A course entitledTomorrow’s Leaders was developed to help students fulfill this requirement. It isexpected that, after taking this course, students will accomplish the followinglearning outcomes:
1. understand and integrate theories, research, and concepts on the basicqualities (particularly intrapersonal and interpersonal qualities) of effectiveleaders in the Chinese context;
2. develop self-awareness and self-understanding;3. acquire interpersonal skills;4. develop self-reflection skills in their learning; and5. recognize the importance of an active pursuit of knowledge as it relates to
intrapersonal and interpersonal leadership qualities.
Several positive youth development constructs, including self-understanding;resilience; cognitive, social, emotional, and moral competence; spirituality; posi-tive identity; interpersonal relationships; and self-leadership are included in thiscourse. The course syllabus is shown in table 1 (Shek, 2012).
Promotion of Holistic Development in University Students 51
Table 1 Syllabus for the Course Tomorrow’s Leaders
Topic Subject Content
1 An overview of the personal attributes of effective leaders: role of self-understandingand interpersonal relationship qualities.
Required reading: Hogan, R., & Kaiser, R. B. (2005). What we know about leader-ship. Review of General Psychology, 9(2), 169–180.
2 Self-understanding: personality traits conducive to successful leadership.Required reading: Shek, D. T. L. (2010). Nurturing holistic development of univer-
sity students in Hong Kong: Where are we and where should we go? Scientific WorldJournal, 10, 563–575.
3 Emotional competence: awareness and understanding of emotions, emotionalquotient (EQ), role of emotional management in effective leadership, and mentalhealth.
Required reading: Lau, P. S. (2006). Emotional competence as a positive youthdevelopment construct: Conceptual bases and implications for curriculum develop-ment. International Journal of Adolescent Medicine and Health, 18(3), 355–362.
4 Cognitive competence: different types of thinking, higher order thinking, experientiallearning, role of cognitive competence in effective leadership, and effective leaders asteachers.
Required reading: Moseley, D., Elliott, J., Gregson, M., & Higgins, S. (2005). Think-ing skills frameworks for use in education and training. British Educational ResearchJournal, 31(3), 367–390.
Chapter 04_Chapter 04 4/16/13 11:03 AM Page 51

52 Best Practices in Mental Health
Table 1 Syllabus for the Course Tomorrow’s Leaders—(Continued)
Topic Subject Content
5 Resilience: stresses faced by adolescents, life adversities, coping with life stresses,adversity quotient (AQ), and role of resilience in effective leadership.
Required reading: Lee, T. Y. (2006). Resilience as a positive youth developmentconstruct: Conceptual bases and implications for curriculum development. Interna-tional Journal of Adolescent Medicine and Health, 18(3), 475–482.
6 Spirituality: meaning in life and adolescent development, spirituality and mentalhealth, role of spirituality in effective leadership, and servant leadership.
Required reading: Lau, P. S. (2006). Spirituality as a positive youth developmentconstruct: Conceptual bases and implications for curriculum development. Interna-tional Journal of Adolescent Medicine and Health, 18(3), 363–370.
7 Ethics and morality: moral issues and moral competence, role of ethics and moralityin effective leadership, integrity and responsibility and effective leadership.
Required reading: Park, N., & Peterson, C. (2009). Character strengths: Researchand practice. Journal of College and Character, 10(4), 1–10.
8 Social competence: basic social competence skills, ability to build up positive humanrelationships, role of social competence in effective leadership, and egocentric men-tality as a block to effective leadership.
Required reading: Ma, H. K. (2006). Social competence as a positive youth devel-opment construct: Conceptual bases and implications for curriculum development.International Journal of Adolescent Medicine and Health, 18(3), 379–385.
9 Positive and healthy identity: self-identity, self-esteem, and self-concept; self-discrepancies; role of self-concept in leadership; and self-leadership.
Required reading: Tsang, S. K. M., & Yip, F. Y. Y. (2006). Positive identity as a positive youth development construct: Conceptual bases and implications for curricu-lum development. International Journal of Adolescent Medicine and Health, 18(3),459–466.
10 Interpersonal communication: theories, concepts, and skills of interpersonalcommunication, and role of communication skills in effective leadership.
Required reading: de Vries, R. E., Bakker-Pieper, A., Siberg, R. A., van Gameren, K.,& Vlug, M. (2009). The content and dimensionality of communication styles. Com-munication Research, 36(2), 178–206.
11 Interpersonal conflict; role of conflict resolution in effective leadership, team building,relationship quality, and effective leadership.
Required reading: Barki, H., & Hartwick, J. (2004). Conceptualizing the constructof interpersonal conflict. The International Journal of Conflict Management, 15(3),216–244.
12 Personal integrity and sense of responsibility in effective leaders; egocentricism inuniversity students.
Required reading: Thomas, J. C. (2008). Ethical integrity in leadership and organi-zational moral culture. Leadership, 4(4), 419–442.
13 Self-leadership, mental health, and effective leadership.Required reading: Dolbier, C. L., Soderstrom, M., & Steinhardt, M. A. (2001). The
relationships between self-leadership and enhanced psychological, health and workoutcomes. Journal of Psychology, 135(5), 469–485.
Chapter 04_Chapter 04 4/16/13 11:03 AM Page 52

Evaluation of Tomorrow’s Leaders
Tomorrow’s Leaders was offered to four classes of students in the 2011–12school year. In Pilot Study 1, 268 students participated in the course. In PilotStudy 2, 195 students enrolled in four classes. Systematic evaluation was per-formed using various evaluation mechanisms, including objective outcome evalu-ation, post-lecture and post-course subjective outcome evaluation, process evalu-ation, and qualitative evaluation. The evaluation findings are presented in thefollowing sections.
Objective Outcome Evaluation
In Pilot Study 1, pre-test and post-test data utilizing the Chinese Positive YouthDevelopment Scale (CPYDS) were collected from fifty students taking the course.The CPYDS is a validated instrument that assesses various aspects of positiveyouth development, including bonding; resilience; cognitive, emotional, behav-ioral, moral, and social competence; self-determination; self-efficacy; positiveidentity; spirituality; prosocial norms; and prosocial involvement. Relevantdomains of the CPYDS were used in this study. Results showed that participantshad significant increases in scores in the domains of emotional, cognitive, andbehavioral competence; self-determination; and positive identity. They also hadsignificant increases in several composite scores (Shek & Sun, 2012e).
In Pilot Study 2, a quasi-experimental study with an experimental group (N = 195) and a control group (N = 71) was conducted to examine the effective-ness of the course. The two groups were comparable in terms of gender ratio, age,and family background characteristics. Analyses of covariance, controlling forpre-test differences between the two groups, showed that the experimental groupgenerally exhibited higher levels of psychosocial competence in terms of a com-posite variable including resilience; social, emotional, cognitive, and behavioralcompetence; self-determination; self-efficacy; and beliefs in the future. The studysuggests that this course can promote critical thinking, interpersonal competence,problem solving, lifelong learning, and ethical leadership in Chinese universitystudents in Hong Kong (Shek, Sun, Tsien-Wong, Cheng, & Yim, in press).
Subjective Outcome Evaluation (Post-Lecture Evaluation)
To evaluate their perceptions of the lectures, students were invited to respondto a twelve-item post-lecture questionnaire after each lecture (except the last lec-ture) in Pilot Study 1. A total of 2,039 post-lecture subjective outcome evaluationforms were collected following lectures 1 through 13. The post-lecture evaluationquestionnaire was found to possess good psychometric properties. Results showedthat the students generally had positive perceptions of the lecture content, classatmosphere, and teacher attributes. With reference to the global evaluation of the
Promotion of Holistic Development in University Students 53
Chapter 04_Chapter 04 4/16/13 11:03 AM Page 53

subject, 93 and 90 percent of students gave positive evaluations of the teacherand subject, respectively. Subject, class, and teacher attributes were found to bepredictive of the overall satisfaction with the lecture and the teacher (Shek, 2012).
In Pilot Study 2, students were similarly invited to respond to a twelve-itempost-lecture questionnaire after the first thirteen lectures (N = 195 students with2,012 questionnaires collected). Results showed that students generally had posi-tive perceptions of the subject, class, and teacher attributes, and the overall eval-uation was very positive. More than 93 percent of the respondents had a positiveglobal evaluation of the subject and the teacher. Through factor analyses, threefactors were abstracted from the scale (subject attributes, class attributes, andteacher attributes). The total scale and subscales were internally consistent. It wasalso found that subject, class, and teacher attributes were significant predictors ofperceived benefits of the subject (Shek & Sun, in press-b).
Subjective Outcome Evaluation (Post-Course Evaluation)
In Pilot Study 1, subjective outcome evaluation data based on a validatedinstrument were collected from 189 students after completion of the course. Thestudents generally had positive perceptions of the program and instructors, withmore than 90 percent of the participants indicating that they were satisfied withthe program and that they perceived the program was helpful to them in thedomains of holistic development and leadership. For example, 94 percent of thestudents felt that the subject had helped them to achieve self-reflection, and 93percent commented that the subject promoted their overall development. Signifi-cant correlations among perceived quality of the program, perceived quality ofinstructors, and perceived program benefits were found (Shek & Sun, 2012d).
In Pilot Study 2, 195 students responded to the thirty-seven-item SubjectiveOutcome Evaluation Scale (SOES) after completion of the course. Results showedthat students generally had positive perceptions of the program and instructors,with more than 90 percent of the participants indicating that they were satisfiedwith the program. Almost all participants felt that the subject had helped themdevelop their intrapersonal and interpersonal competence. In both pilot studies,factor analyses showed that three factors (course, instructor, and benefits) wereabstracted from the scale. The total scale and the subscales were found to be inter-nally consistent (Shek & Sun, in press-a).
Process Evaluation
In Pilot Study 1, process evaluation was carried out for fourteen lectures tounderstand the quality of the program implementation. Based on systematicobservations by two observers, results showed that the average level of programadherence was high (85.71%), with high ratings given to student interest, class-room control, use of interactive delivery method, use of strategies to enhance stu-dent motivation, opportunity for reflection, degree of achievement of the objec-
54 Best Practices in Mental Health
Chapter 04_Chapter 04 4/16/13 11:03 AM Page 54

tives, quality of preparation, overall implementation quality, and success of imple-mentation. Various aspects of the program implementation contributed to thehigh quality and success of the program (Shek & Sun, 2012c).
In the second piloting exercise, process evaluation was carried out for nineteenlectures, with each lecture observed by two independent observers. Resultsshowed that interrater reliability was generally high. Regarding ratings for thequality of program implementation, results showed that quality of implementa-tion as assessed by the two observers was generally high. In addition, bothobservers generally regarded the program implementation as successful. Highprogram fidelity (average degree of program adherence = 94.9%) was also found.Classroom management, time management, and achievement of the teachingunit’s objectives were significant predictors of overall quality and success of theprogram (Shek & Sun, in press-c).
Qualitative Evaluation (Personal Reflection)
In Pilot Study 1, students were invited to use qualitative descriptors andmetaphors to describe their experiences in the course. Based on the reflections of189 students, results showed that most participants used positive descriptors(such as self-understanding, interesting, motivating, meaningful, and enlighten-ing) and positive metaphors (such as meaningful tours, compass, star, and super-star) to describe the course. Several scholarship holders were also invited to writedown their personal reflections. Results showed that the students liked the course,and they identified many positive attributes of the course. They also appreciatedthe instructors, and they felt that the course contributed to various aspects oftheir development (Shek & Sun, 2012f).
In Pilot Study 2, three qualitative studies based on the reflections of the partic-ipants were conducted. In the first study, students were invited to use threedescriptors and a metaphor to describe their experiences at the end of the course(Shek, in press). Based on the reflections of 143 students, results showed that 94.4percent of the descriptors used by informants were positive (e.g., helpful to devel-opment, useful/helpful, reflective, inspiring, and impressive). For the metaphorsused to describe the subject, 92.7 percent were positive (e.g., enjoyable, meaning-ful, interesting, interactive, or relaxing course; path to future; breakthrough; mile-stone; and turning point).
In the second study, students were invited to write personal reflections aboutthe subject. Based on the reflections of 104 students, data were separately ana-lyzed by two independent raters. Reliability analyses revealed that the coding ofreflections had high intra- and interrater reliability. Results showed that the infor-mants were generally positive about the subject and lecturers, and that they per-ceived that the subject promoted their overall development in various domains.
Finally, five recipients of Wofoo Foundation Scholarships were invited to writereflective journals regarding their experiences in taking this course. The students
Promotion of Holistic Development in University Students 55
Chapter 04_Chapter 04 4/16/13 11:03 AM Page 55

believed there was a need for this course, and they felt that the course was benefi-cial to their development. Additionally, they pointed out that they liked the courseand instructors, and they identified many positive attributes of the course and itsimplementation. Respondents also perceived the course to be beneficial to theirdevelopment. Some of the narratives are included below:
• “I learned a lot from this GE course. . . . We built up friendships and shareddifferent points of view through discussion. In the lectures, the lecturer . . .allowed us to interact and communicate with classmates. We thought andreflected on our own experiences of our life. Now, Tomorrow’s Leaders to meis not only a noun, but also something we could achieve in the future.”
• “In my major, there are only lectures and tutorials. After the lecturers fin-ished what they wanted to say, they left. . . . But in Tomorrow’s Leaders therewere many interactions, which shocked me at the very beginning. Nearlyeveryone has to share what they think and feel during the lesson. . . . This issomething I can never encounter if I haven’t taken this course, Also, themost interesting part was the worksheet. . . . These few pieces of paper canhelp me find my truth and know about myself. I have the deepest feelingwhen I was filling the worksheet about my strengths, weaknesses and ideal-self. I would like to find out the answers.”
• “The lectures that I like most . . . are ‘Self-understanding’ and ‘Resilience.’For ‘Self-understanding,’ it provided a chance for us to rethink ourselves. Ithink it was a valuable opportunity to understanding our strengths andweaknesses. . . . After understanding ourselves, it is a chance to let us acceptand strive for change. Then, I believe that it is easier to be a good leader andcommunicate with others after the change. For ‘Resilience,’ I learned that wecan convert difficulties into opportunities. Now in my mind, difficulties arejust time to make decisions and time to prove that I have the ability to solveproblems. . . . Last but not least, I liked the in-class activities, videos, and sto-ries provided by the instructor. It got me involved in the class and to cooper-ate with different people. . . . And also, it is valuable to meet other people fromdifferent programs, such as engineering and social work. It is good to under-stand them and know more about their values, which are very different frommine.”
Qualitative Evaluation (Focus Group Interviews)
In Pilot Study 1, five focus groups (N = 23 students) were conducted to under-stand the feelings and views of the students taking the course. Results showed thatstudents generally had positive perceptions of the course content, the class, andthe lecturers, and almost all students felt that the course could promote theirreflection and self-understanding. All students also held the view that there was aneed to have this course in their university study (Shek & Sun, 2012b).
56 Best Practices in Mental Health
Chapter 04_Chapter 04 4/16/13 11:03 AM Page 56

In Pilot Study 2, twenty-three randomly selected students participated in fourfocus group interviews. The students generally felt that the subject was very help-ful to their development and that there was a strong need to offer this course. Theyalso enjoyed the course very much. Some related narratives are as follows:
• “The course was interactive. It was well-designed with clear structure ofwhich you could pace with the rundown of the lecture.”
• “I liked the ‘Stars’ of the videos which had a modeling effect on me, especiallyon the self-development and personal growth.”
• “I thought that the course should be organized for the university students atan earlier stage so that they could know more about the formation of per-sonality and different competences. . . . All of these had good match with theframework of positive youth development concept.”
• “After the lecture on emotional competence, I always reminded myself to betolerant of my family. Besides, you might have problem in working with oth-ers if you could not handle your emotion.”
• “Before I took the course, . . . I looked at things from my perspective. Ithought about myself first—it was your fault but not my fault. I am a per-fectionist. I do not like other people intruding in my life and I am very stub-born. In particular, I always have quarrels with my mum and I do not under-stand her feelings. In the past, I simply ignored her and thought it was herbusiness if she worried about me . . . but now I will stand in my mom’s per-spective to look at things. I think our relationship has improved. My mumsaid that our relationship had improved. In the past, we would stop talkingwhen we were unhappy. Now, we would communicate and I would under-stand her feelings.”
Best Practice for Youth Development
This article has outlined the development of a course entitled Tomorrow’s Lead-ers for students to fulfill the leadership and intrapersonal development require-ment of the four-year undergraduate curriculum at the Hong Kong PolytechnicUniversity. The course was piloted twice, with the use of a wide range of evalua-tion strategies. Overall, the evaluation findings are overwhelmingly positive. Withspecific reference to objective outcome evaluation, students showed positivechanges after taking the course, and the positive changes were more pronouncedin students in the experimental group than those in the control group.
With reference to the nonexperimental evaluation findings, students generallyhad positive perceptions of the course and the instructors, and they agreed thatthe program could promote their psychosocial competence in areas such asresilience, positive identity, and overall positive development. Shek and Wong(2011) pointed out that adolescent developmental issues would not disappearovernight, and that existing strategies to cope with the problem are not consistent
Promotion of Holistic Development in University Students 57
Chapter 04_Chapter 04 4/16/13 11:03 AM Page 57

with the basic principles of public health. A review of the literature shows thatpositive youth development programs are very popular in high school settings(Catalano et al., 2012). Surprisingly, validated and systematic positive youthdevelopment programs are rare in higher education. The findings suggest that theuse of a credit-bearing course to promote the holistic development of universitystudents is a promising approach (Shek et al., 2012).
These two pilot studies and the related evaluation further reinforce the impor-tance of nurturing developmental assets such as psychosocial competence in pro-moting holistic development and the positive component of mental health inyoung people. Actually, Tomorrow’s Leaders can be regarded as a university ver-sion of the Project P.A.T.H.S. initiative in Hong Kong. To promote holistic develop-ment among Hong Kong adolescents, the Hong Kong Jockey Club Charities Trustlaunched a project entitled P.A.T.H.S. to Adulthood: A Jockey Club YouthEnhancement Scheme (Project P.A.T.H.S.), with an aggregated earmarked grantof HK$750 million. To date, more than 200,000 secondary school students frommore than 280 secondary schools have joined the program. Triangulation of var-ious types of evaluation data clearly showed that the project was able to promotepositive development and reduce problem behavior in grade seven to grade ninestudents (Shek & Sun, 2012a).
Of course, there are several limitations of the two pilot studies. First, althougha quasi-experimental design was used in the second pilot study, it is important touse a true experimental design to evaluate the program. In particular, the use ofrandomized clinical trials and independent groups of researchers at several siteswould be helpful. Second, because the current findings are basically cross-sectional or short-term, there is a need to conduct longitudinal studies. This isimportant because there is a need to assess the impact of the program in real lifesettings. Third, involvement of observers observing the students taking this coursewould provide an additional perspective in understanding the program’s effect.Finally, to enhance the generalizability of the findings, the subject should beoffered in other settings involving different types of students.
ReferencesAstin, A. W., & Sax, L. J. (1998). How undergraduates are affected by service
participation. Journal of College Student Development, 39(3), 251–263.Barrios, L. C., Everett, S. A., Simon, T. R., & Brener, N. D. (2000). Suicide ideation
among U.S. college students: Assocations with other injury risk behavior.Journal of American College Health, 48(5), 195–198.
Benson, P. L. (1997). All kids are our kids: What communities must do to raise caringand responsible children and adolescents. San Francisco: Jossey-Bass.
Bips, L. (2010). Students are different now. New York Times. Retrieved fromhttp://www.nytimes.com/roomfordebate/2010/10/11/have-college-freshmen-changed/students-are-different-now.
58 Best Practices in Mental Health
Chapter 04_Chapter 04 4/16/13 11:03 AM Page 58

Blanco, C., Okuda, M., Wright, C., Hasin, D. S., Grant, B. F., Liu, S. S., & Olfson, M.(2008). Mental health of college students and their non-college-attendingpeers: Results from the national epidemiologic study on alcohol andrelated conditions. Archives of General Psychiatry, 65(12), 1429–1437.
Bloom, A. (1987). The closing of the American mind. New York: Simon and Schuster.Bok, D. (2006). Our underachieving colleges: A candid look at how much students
learn and why they should be learning more. Princeton, NJ: Princeton University Press.
Catalano, R. F., Fagan, A. A., Gavin, L. E., Greenberg, M. T., Irwin, C. E., Ross, D. A., & Shek, D. T. L. (2012). Worldwide application of prevention science inadolescent health. Lancet, 379(9826), 1653–1664.
Chan, K. L., Tiwari, A., Leung, W. C., Ho, H. W. Y., & Cerulli, C. (2007). Commoncorrelates of suicidal ideation and physical assault among male andfemale university students in Hong Kong. Violence and Victims, 22(3),290–303.
Dalton, J., & Crosby, P. (2006). The neglected inner lives of college students. Jour-nal of College and Character, 7(8), 1–2.
Damon, W. (2004). What is positive youth development? Annals of the AmericanAcademy of Political and Social Science, 591(1), 13–24.
Graczyk, P. A., Weissberg, R. P., Payton, J. W., Elias, M. J., Greenberg, M. T., &Zins, J. E. (2000). Criteria for evaluating the quality of school-basedsocial and emotional learning programs. In R. Bar-On & J. D. A. Parker(Eds.), The handbook of emotional intelligence: Theory, development, assess-ment, and application at home, school and in the workplace (pp. 391–409).San Francisco: Jossey-Bass.
Hong Kong Tertiary Institutions Health Care Working Group. (2007). Researchshowed that roughly half of university students in Hong Kong have anxiety problems. [Press release]. Hong Kong: Li Ka Shing Faculty ofMedicine, University of Hong Kong.
Keyes, C. L. M., Shmofkin, D., & Ryff, C. D. (2002). Optimizing well-being: Theempirical encounter of two traditions. Journal of Personality and SocialPsychology, 82(6), 1007–1022.
Lewis, H. R. (2006). Excellence without a soul: How a great university forgot educa-tion. New York: Public Affairs Publishing.
Mowbray, C. T., Megivern, D., Mandiberg, J. M., Strauss, S., Stein, C. H., Collins, K.,. . . Lett, R. (2006). Campus mental health services: Recommendationsfor change. American Journal of Orthopsychiatry, 76(2), 226.
Pittman, K. J. (1991). Promoting youth development: Strengthening the role ofyouth-serving and community organizations. Report prepared for the U.S.Department of Agriculture Extension Services. Washington, DC: Centerfor Youth Development and Policy Research.
Readings, B. (1997). The university in ruins. Cambridge, MA: Harvard UniversityPress.
Promotion of Holistic Development in University Students 59
Chapter 04_Chapter 04 4/16/13 11:03 AM Page 59
Ryan, R. M., & Deci, E. L. (2001). To be happy or to be self-fulfilled: A review ofresearch on hedonic and eudaimonic well-being. In S. Fiske (Ed.), Annualreview of psychology (Vol. 52, pp. 141–166). Palo Alto, CA: AnnualReview, Inc.
Shek, D. T. L. (2010). Nurturing holistic development of university students inHong Kong: Where are we and where should we go? Scientific World Jour-nal, 10, 563–575.
Shek, D. T. L. (2012). Development of a positive youth development subject in auniversity context in Hong Kong. International Journal on Disability andHuman Development, 11(3), 173–179.
Shek, D. T. L. (in press). Reflections of Chinese students on a university subjecton leadership and intrapersonal development. International Journal on Disability and Human Development.
Shek, D. T. L., & Cheung, B. P. M. (in press). Developmental issues of universitystudents in Hong Kong. International Journal of Adolescent Medicine andHealth.
Shek, D. T. L., Ma, H. K., & Sun, R. C. F. (2011). A brief overview of adolescentdevelopmental problems in Hong Kong. Scientific World Journal, 11,2243–2256.
Shek, D. T. L., & Sun, R. C. F. (2012a). Epilogue: The Project P.A.T.H.S. in HongKong: Lessons learned and implications for positive youth development programs. Scientific World Journal, 2012, Article ID 687536. doi: 10.1100/2012/687536.
Shek, D. T. L., & Sun, R. C. F. (2012b). Focus group evaluation of a positive youthdevelopment course in a university in Hong Kong. International Journal onDisability and Human Development, 11(3), 249–254.
Shek, D. T. L., & Sun, R. C. F. (2012c). Process evaluation of a positive youthdevelopment course in a university setting in Hong Kong. InternationalJournal on Disability and Human Development, 11(3), 235–241.
Shek, D. T. L., & Sun, R. C. F. (2012d). Promoting leadership and intrapersonalcompetence in university students: What can we learn from Hong Kong?International Journal on Disability and Human Development, 11(3),221–228.
Shek, D. T. L., & Sun, R. C. F. (2012e). Promoting psychosocial competencies inuniversity students: Evaluation based on a one group pretest-posttestdesign. International Journal on Disability and Human Development, 11(3),229–234.
Shek, D. T. L., & Sun, R. C. F. (2012f). Qualitative evaluation of a positive youthdevelopment course in a university setting in Hong Kong. InternationalJournal on Disability and Human Development, 11(3), 243–248.
Shek, D. T. L., & Sun, R. C. F. (in press-a). Post-course subjective outcome evalua-tion of a course promoting leadership and intrapersonal development inuniversity students in Hong Kong. International Journal on Disability andHuman Development.
60 Best Practices in Mental Health
Chapter 04_Chapter 04 4/16/13 11:03 AM Page 60

Shek, D. T. L., & Sun, R. C. F. (in press-b). Post-lecture evaluation of a universitycourse on leadership and intrapersonal development. International Journalon Disability and Human Development.
Shek, D. T. L., & Sun, R. C. F. (in press-c). Process evaluation of a leadership andintrapersonal development subject for university students. InternationalJournal on Disability and Human Development.
Shek, D. T. L., Sun, R. C. F., Chui, Y. H., Lit, S. W., Yuen, W. W., Chung, Y., & Ngai,S. W. (2012). Development and evaluation of a positive youth develop-ment course for university students in Hong Kong. Scientific World Jour-nal, 2012, Article ID 263731. doi:10.1100/2012/263731.
Shek, D. T. L., Sun, R. C. F., Tsien-Wong, T. B. K., Cheng, C. T., & Yim, H. Y. (inpress). Objective outcome evaluation of a leadership and intrapersonaldevelopment subject for university students. International Journal on Disability and Human Development.
Shek, D. T. L., & Wong, K. K. (2011). Do adolescent developmental issues disap-pear overnight? Reflections about holistic development in university students. Scientific World Journal, 11, 353–361.
Song, Y., Huang, Y., Liu, D., Kwan, J. S. H., Zhang, F., Sham, P. C., & Tang, S. W.(2008). Depression in college: Depressive symptoms and personality factors in Beijing and Hong Kong college freshmen. Comprehensive Psychiatry, 49(5), 496–502.
Twenge, J. M., & Foster, J. D. (2008). Mapping the scale of the narcissism epi-demic: Increases in narcissism 2002–2007 within ethnic groups. Journalof Research in Personality, 42(6), 1619–1622.
Twenge, J. M., Konrath, S., Foster, J. D., Campbell, W. K., & Bushman, B. J.(2008). Egos inflating over time: A cross-temporal meta-analysis of thenarcissistic personality inventory. Journal of Personality, 76(4), 875–901.
Weissberg, R. P., & O’Brien, M. U. (2004). What works in school-based social andemotional learning programs for positive youth development. Annals ofthe American Academy of Political and Social Science, 591(1), 86–97.
Wilshire, B. (1990). The moral collapse of the university. New York: SUNY Press.Wong, J. G. W. S., Cheung, E. P. T., Chan, K. K. C., Ma, K. K. M., & Tang, S. W.
(2006). Web-based survey of depression, anxiety and stress in first-yeartertiary education students in Hong Kong. Australian and New ZealandJournal of Psychiatry, 40(9), 777–782.
World Health Organization. (2011). Mental health: A state of well-being.Retrieved from http://www.who.int/features/factfiles/mental_health/en/index.html.
Promotion of Holistic Development in University Students 61
Chapter 04_Chapter 04 4/16/13 11:03 AM Page 61

People with serious mental illness die, on average, twenty-five years earlier than thosein the population without a serious mental illness. This disparity is largely due to treat-able medical conditions that remain unaddressed due to factors at the client, treatment,provider, clinic, and system levels of health and mental health service delivery. Thisarticle describes the development, initial implementation, and feasibility of the Bridge,a peer-staffed care linkage model situated in a mental health clinic that addresses barri-ers at multiple levels of service delivery by connecting clients to physical health servicesand developing client skills that result in self-management of health care. The Bridgewas developed collaboratively with interventionists, clinic staff, and mental health peersand relies largely on an in vivo approach.
Key words: health; health disparities; health navigation; intervention; seriousmental illness
People living with serious mental illness in the United States die, on average,twenty-five years earlier than those without a serious mental illness, largely due topreventable medical conditions and suboptimal medical care (Parks, Svendsen,Singer, & Foti, 2006). Studies have found a higher incidence of certain physicaldisorders, such as diabetes (Dickerson et al., 2006; Lester, Tritter, & Sorohan,2005), obesity (Parks et al., 2006), high cholesterol or dyslipidemia (Dalmau,Bergman, & Brismar, 1997), metabolic and cardiovascular problems (Brunero &Lamont, 2010; Deakin et al., 2010), and cancer (Brown, 1998), among people
Reducing Health Disparities for People with SeriousMental Illness: Development and Feasibility of aPeer Health Navigation Intervention
John S. Brekke, Elizabeth Siantz, Rohini Pahwa, Erin Kelly, Louise Tallen, and Anthony Fulginiti
John S. Brekke, PhD, is professor at the School of Social Work, University of Southern California,Los Angeles. Also at the School of Social Work, University of Southern California, Los Angeles,Elizabeth Siantz, MSW, is a PhD student; Rohini Pahwa, MSW, is a PhD candidate; Louise Tallen,PhD, is project manager; and Anthony Fulginiti, MSW, is a PhD student. Erin Kelly, PhD, is post-doctoral fellow at the Health Services Research Center, University of California, Los Angeles. Thispilot study was funded with support from the UniHealth Foundation, and the Los Angeles BasinClinical Translational Science Institute at the University of Southern California.
© 2013 Lyceum Books, Inc., Best Practices in Mental Health, Vol. 9, No. 1, March 2013
Chapter 05_Chapter 05 4/16/13 11:04 AM Page 62

with serious mental illness. When combined with a serious mental illness, physi-cal illness can lead to other health conditions (Dickerson et al., 2005) and to aquality of life lower than that of both the general population and individuals withmental illness alone (Desai, Rosenheck, Druss, & Pearlin, 2002; Dickerson et al.,2008). These negative health consequences can affect other recovery goals suchas housing, vocational training, and education (Bazelon Center for Mental HealthLaw [BCMHL], 2004).
Individuals with serious mental illness also face numerous barriers to accessand use of health care services needed to prevent and manage chronic diseases atmultiple levels of the service delivery system (De Hert et al., 2011; Druss, Rask, &Katon, 2008). At the system level, the chasm between the health and mentalhealth care systems impedes access to care in both systems and reduces coordina-tion of services (Miller, Druss, Dombrowski, & Rosenheck, 2003). Environmentalbarriers include difficulties in finding a specialist, long waits in clinics, trans-portation difficulties, geographical distance, and cost (Dickerson et al., 2003;Jeste, Gladsjo, Lindamer, & Lacro, 1996). Provider-level barriers for people withserious mental illness include limited training of mental health professionals inattending to their physical health concerns (Brown, 1998), limited training of pri-mary care physicians in working with people with serious mental illness (Leigh,Stewart, & Mallios, 2006), and the stigma endured during encounters with healthproviders (Goldberg et al., 2007). At the individual level, additional barriers mayresult from mistrust of the system, lack of knowledge and resources, and behav-ioral or cognitive challenges in understanding and accessing services, along witheducational, cultural, and language hurdles (Bradford, Coleman, & Cunningham,2007; Cohen & Krauss, 2003; Dickey, Normand, Weiss, Drake, & Azeni, 2002).
The high incidence of comorbid diseases among people with serious mental ill-ness contributes to the high cost of health care for those who receive specialtymental health services (BCMHL, 2004), leading to increasing demands for solu-tions, nationally and internationally (Hedberg & Skärsäter, 2009; Kane, 2009;Maj, 2009; Shattell, Donnelly, Scheyett, & Cuddeback, 2011). The integration ofhealth and mental health services is a means to address the fragmentation ofhealth and mental health service systems (Anderson & Knickman, 2001; Druss et al., 2008; Goldberg, 1999). This article will discuss the conceptual model,development, and feasibility of an innovative community-based health navigatorintervention for people living with serious mental illness.
Models for Integrating Services
The Bazelon Center for Mental Health Law (2004) has identified the followingmodels for integrating health and mental health services for individuals with seri-ous mental illness: (1) embedding of health care providers within mental healthprograms, (2) full-service health and mental health delivery programs housed inthe same agency, and (3) collaboration between independent health and mentalhealth providers. The first two models involve co-situated care, and the third is a
Reducing Health Disparities for People with Serious Mental Illness 63
Chapter 05_Chapter 05 4/16/13 11:04 AM Page 63

care linkage model. These approaches address different barriers to care. Althoughco-situated approaches would appear to address more barriers, they require sig-nificant change in both health care policy and the structure and financing of ser-vice delivery (Goldberg, 1999). For example, although co-situated service pro-grams show some impact, they are still challenged by separate funding streams forhealth and mental health services. Another barrier to integration is the differencein reimbursement plans for health and mental health services (BCMHL, 2004).Even with Medicaid, individuals with serious mental illness are served throughfee-for-service arrangements, whereas physical health is addressed via managedcare services (Goldberg, 1999). Moreover, integrating care contracts does not necessarily result in more integrated and efficient services (Laws, Gabriel, &McFarland, 2002; Stroul, Pires, & Armstrong, 2001; Vogel, 2001).
The third model, care linkage, improves collaboration between independenthealth and mental health providers and could be implemented in the context ofmany existing financing and service structure arrangements. One randomizedstudy has shown increased utilization of primary care service by individuals withserious mental illness, increased preventative care visits, and better health out-comes when separate health and mental health services are coordinated by anurse case manager (Druss, von Esenwein, et al., 2010). Although care linkagedoes not require co-situated health and mental health care, the use of highly paidprofessionals may introduce other cost considerations.
Care Linkage and Peer Providers
A promising alternative to care linkage provided by professionals is the use ofpeer providers to deliver these services (New Freedom Commission on MentalHealth, 2003). Peer providers bring their own experience of living with a mentalillness to assist clients with serious mental illness. Peers are one of the most rapidlygrowing segments of the mental health workforce in the United States (Druss,Zhao, et al., 2010), and peer-run interventions are becoming prominent in therecovery literature (Rosenick & Rosenheck, 2008; Solomon, 2004). Peers can betrained to work in a variety of settings to promote recovery and wellness (Cook,2005; Davidson et al., 1999; Davidson, Chinman, Sells, & Rowe, 2006; Rosenick& Rosenheck, 2008; Solomon, 2004), and potentially offer more cost-effective ser-vices than other options (Battaglia, Roloff, Posner, & Freund, 2007; Jandorf et al.,2006; Steinberg et al., 2006). Furthermore, this peer provider option can offertraining and employment opportunities to persons with serious mental illness andprovide them with a stronger role and voice within these systems, a key goal of theRecovery Movement.
Peer interventions build on the experience and sensitivities of peers to focus onpractical issues of access and utilization of health services. For example, individu-als with a history of cancer have been used to help women with breast canceraccess services (Darnell, 2007; Dohan & Schrag, 2005). Similarly, HIV/AIDS
64 Best Practices in Mental Health
Chapter 05_Chapter 05 4/16/13 11:04 AM Page 64

services have applied this model to reduce barriers to service utilization (Bradfordet al., 2007), and such models are thought to be an effective strategy for address-ing obstacles to accessing health care services. At present, only one randomizedpilot trial, in which trained peers led manualized group pyschoeducation classeson chronic disease management for participants with serious mental illness, hasbeen completed (Druss, Zhao, et al., 2010). Compared to participants whoreceived treatment as usual, participants who completed the course showedhigher rates of utilizing primary care services (68.4% vs. 51.9%), more patientengagement in self-managing their health and health care, and higher quality ofphysical health. These results, although promising, may also suggest that patientsmay require significantly more assistance to see substantial improvements in well-being.
Given the potential benefits of a care linkage model with peer providers, theauthors developed and implemented an intensive, individualized, peer health nav-igator intervention to facilitate access to physical health care for people diagnosedwith serious mental illness who are engaged in the publicly funded mental healthsystem in Los Angeles.
Theoretical Framework for Peer Health Navigation
Improving the physical health of people living with serious mental illness is acomplex challenge, resulting from numerous factors at the levels of the individual,the provider, the health care system, and the broader geographic and sociopoliti-cal environment. A sound conceptual framework is important for organizing themultiple factors that contribute to the use of health services and the physicalhealth status of people living with serious mental illness, and can provide a roadmap for addressing factors to be targeted by an intervention.
The conceptual model underlying this intervention tailors Gelberg, Andersen,and Leake’s (2000) Behavioral Model of Health Service Use for Vulnerable Popu-lations (BMHSUVP) for those with serious mental illness. Gelberg and colleaguesposit that health services usage is determined by a combination of predisposingcharacteristics (demographic, social structure, and health beliefs), enablingresources (personal/family and community), need for care (perceived and evalu-ated), and personal health care habits (diet, exercise, and self-care). Importantly,this model includes not only factors that lead to health care utilization, but alsofactors that influence the effectiveness of those services. To tailor this model forthose with serious mental illness, a series of focus groups and interviews was con-ducted with clients, staff, and administrators from health care and mental healthcare agencies. Based on the information obtained in these interviews, it becameapparent that the BMHSUVP model omits some important factors that suppresshealth service utilization among those with serious mental illness—namely severepsychiatric symptoms, stigma, and system bifurcation. The adapted theoreticalmodel is shown in figure 1.
Reducing Health Disparities for People with Serious Mental Illness 65
Chapter 05_Chapter 05 4/16/13 11:04 AM Page 65
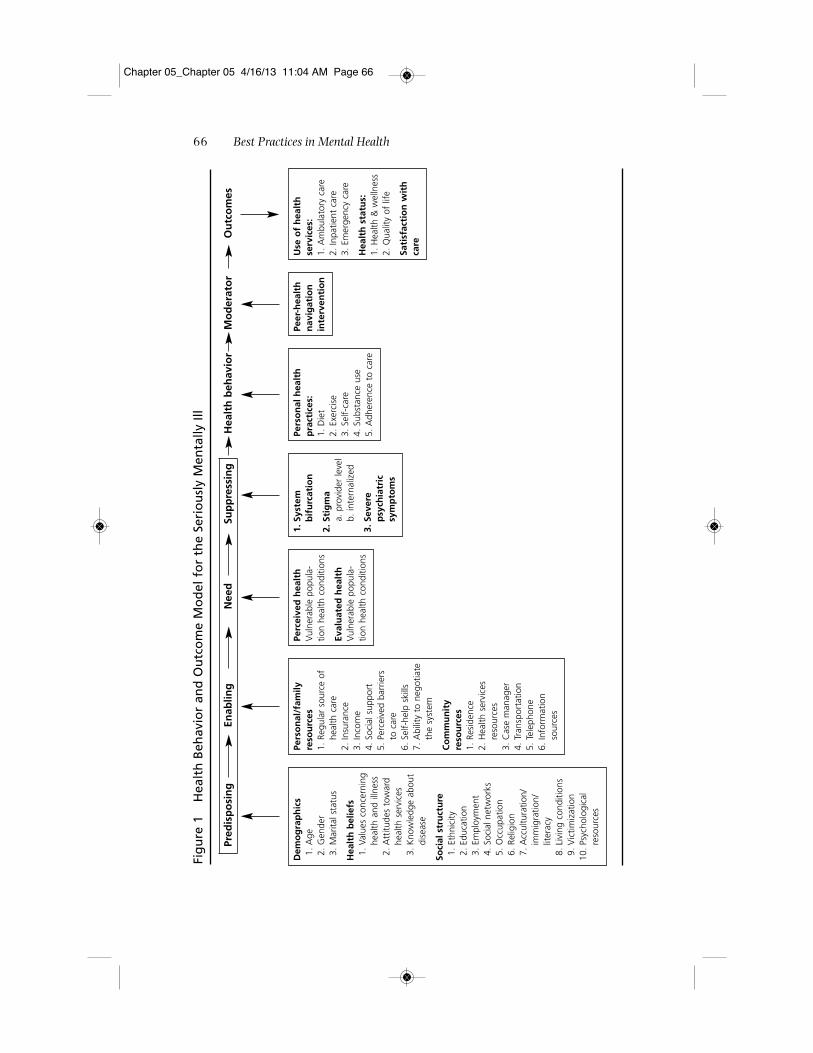
66 Best Practices in Mental Health
Fig
ure
1
Hea
lth
Beh
avio
r an
d O
utc
om
e M
od
el f
or
the
Seri
ou
sly
Men
tally
Ill
Pred
isp
osi
ng
Enab
ling
Nee
dSu
pp
ress
ing
Hea
lth
beh
avio
rM
od
erat
or
Ou
tco
mes
Dem
og
rap
hic
s1.
Age
2. G
ende
r3.
Mar
ital s
tatu
s
Hea
lth
bel
iefs
1. V
alue
s co
ncer
ning
heal
th a
nd il
lnes
s2.
Att
itude
s to
war
dhe
alth
ser
vice
s3.
Kno
wle
dge
abou
tdi
seas
e
Soci
al s
tru
ctu
re1.
Eth
nici
ty2.
Edu
catio
n3.
Em
ploy
men
t4.
Soc
ial n
etw
orks
5. O
ccup
atio
n6.
Rel
igio
n7.
Acc
ultu
ratio
n/im
mig
ratio
n/lit
erac
y8.
Liv
ing
cond
ition
s9.
Vic
timiz
atio
n10
. Psy
chol
ogic
alre
sour
ces
Pers
on
al/f
amily
reso
urc
es1.
Reg
ular
sou
rce
ofhe
alth
car
e2.
Insu
ranc
e3.
Inco
me
4. S
ocia
l sup
port
5. P
erce
ived
bar
riers
to c
are
6. S
elf-
help
ski
lls7.
Abi
lity
to n
egot
iate
the
syst
em
Co
mm
un
ity
reso
urc
es1.
Res
iden
ce2.
Hea
lth s
ervi
ces
reso
urce
s3.
Cas
e m
anag
er4.
Tra
nspo
rtat
ion
5. T
elep
hone
6. In
form
atio
nso
urce
s
Perc
eive
d h
ealt
hVu
lner
able
pop
ula-
tion
heal
th c
ondi
tions
Eval
uat
ed h
ealt
hVu
lner
able
pop
ula-
tion
heal
th c
ondi
tions
1. S
yste
m
bif
urc
atio
n
2. S
tig
ma
a. p
rovi
der
leve
lb.
inte
rnal
ized
3. S
ever
e p
sych
iatr
ic
sym
pto
ms
Pers
on
al h
ealt
hp
ract
ices
:1.
Die
t2.
Exe
rcis
e3.
Sel
f-ca
re4.
Sub
stan
ce u
se5.
Adh
eren
ce t
o ca
re
Peer
-hea
lth
nav
igat
ion
inte
rven
tio
n
Use
of
hea
lth
se
rvic
es:
1. A
mbu
lato
ry c
are
2. In
patie
nt c
are
3. E
mer
genc
y ca
re
Hea
lth
sta
tus:
1. H
ealth
& w
elln
ess
2. Q
ualit
y of
life
Sati
sfac
tio
n w
ith
care
Chapter 05_Chapter 05 4/16/13 11:04 AM Page 66

The model’s predisposing domain includes participant demographics such asage, gender, and marital status; health beliefs including values concerning healthand illness; attitudes toward health services and knowledge of disease; factorsrelated to social structure including ethnicity, level of education, employment sta-tus, social networks, occupation, religion, acculturation, immigration status, lit-eracy, living conditions, victimization, and psychological resources (e.g., mastery,coping, self-esteem, cognitive ability, and substance abuse). Even if services are accessed, clients with serious mental illness may be predisposed to negativeexperiences with physicians as symptoms of their disorder, and cognitive deficitscan make communication more difficult and stressful (Berren, Santiago, Zent, &Carbone, 1999).
The enabling domain includes personal and community characteristicsrequired for the health care interaction to take place (Gelberg et al., 2000). Theproposed model includes personal and family resources such as access to a regu-lar source of care, insurance, income, social support, perceived barriers to care,self-help skills, ability to negotiate the system, and community resources such asestablishing residence and availability of health services, case management,transportation, telephone, and other information sources.
The need domain includes self-assessment or professional assessment thathealth services are required to treat health conditions specific to an adult livingwith serious mental illness. Clients’ perceptions and clinicians’ evaluations oftheir clients’ physical health status may be influenced by the presence of seriousmental illness (Gelberg et al., 2000). Physical health treatment and preventivecare such as cervical screenings, mammograms, and immunizations (Carney,Allen, & Doebbeling, 2002; Druss, Rosenheck, Desai, & Perlin, 2002) may be givensecondary priority relative to care for active psychiatric symptoms, maintainingstable housing, and financial insecurity (BCMHL, 2004).
Personal health behaviors play an important role in service needs (Gelberg etal., 2000). Diet, exercise habits, self-care habits, and substance use can have pow-erful influences on health status (Compton, Daumit, & Druss, 2006). Even ifhealth habits are not poor, increased morbidity and mortality associated with seri-ous mental illness can be traced, in part, to second-generation antipsychotic med-ications currently used to treat this condition. Studies have linked weight gain,dyslipidemia, diabetes, insulin resistance, and metabolic syndromes to these med-ications (Gianfrancesco, Grogg, Mahmoud, Wang, & Nasrallah, 2002; Hippisley-Cox, Vinogradova, Coupland, & Parker, 2007; Kreyenbuhl, 1999). Clients may bereluctant to seek out medical care due to concerns that they will be judged orblamed by their physicians for their self-care habits, motivational deficits, and lowself-esteem (Dickerson et al., 2006). Moreover, clients who have difficulties inthese domains are particularly likely to have difficulty adhering to treatmentregimes or following a physician’s instructions.
Stigma has a pervasive influence on the receipt of health care among thosewith serious mental illness. Stigma refers to imputed personal characteristics thatidentify persons as being undesirably different from normal, and may result in
Reducing Health Disparities for People with Serious Mental Illness 67
Chapter 05_Chapter 05 4/16/13 11:04 AM Page 67

negative self-attributions as well as devaluation by others (Link & Phelan, 2001).When the stigma is mental illness, negative attitudes can lead to avoidance anddiscrimination on the grounds of perceived unacceptability or inferiority. The con-sequences of stigma can include decreased life opportunities, loss of independentfunctioning, and decreased use of physical health services among people livingwith serious mental illness (BCMHL, 2004). Moreover, recognizing oneself as amember of the devalued group can have negative effects on one’s self-concept(Link, 1987; Link & Phelan, 2001; Scheff, 1994) and lead to fear of discrimina-tion and feelings of shame. Physical health providers are not immune to stigma-tizing attitudes and behaviors toward individuals with serious mental illness(Goldberg et al., 2007). These attitudes may be rooted in the fear of unpredictablebehavior and concern with regard to an individual’s noncompliance with treat-ment. Some primary care providers report concerns that people with serious men-tal illness may become bizarre, agitated, disorganized, or even violent in their wait-ing rooms (BCMHL, 2004). These negative attitudes can cause individuals livingwith serious mental illness to receive poor quality of care from the physical healthcommunity (Goldberg et al., 2007).
System bifurcation is the separation of physical and mental health services,which poses a serious issue for those with chronic mental and physical healthissues. At a system level, at least four types of separation between mental andphysical health care may exacerbate the problems for persons with serious mentalillness:
1. geographic, or lack of colocated medical and mental health services;2. financial, including but not limited to separate funding streams for medical
and mental health services;3. organizational, or difficulty in sharing information and expertise across
these systems; and4. cultural, or provider focus on particular symptoms or disorders rather than
on the persons with those problems (Druss & Newcomer, 2007).
Bifurcation discourages people with a mental illness from accessing and utiliz-ing services (Lieberman & Coburn, 1986). Current insurance policies reinforcethis bifurcation because neither Medicare nor Medicaid pays for two services onthe same visit. The Los Angeles County Department of Health Services has sug-gested that the cost of treating a person with serious mental illness can be tentimes that of treating a client without mental illness in a public health clinicbecause clinics are paid a flat fee regardless of case complexity. This provides littleincentive for doctors or clinics to treat those with serious mental illness. Mentalhealth professionals are unable to provide health services, as physical health careis beyond their scope of practice or training and is not reimbursed by mentalhealth funding streams (Brown, 1998). Hence, even colocated services requiremultiple visits and pose structural barriers to adequate care, and in addition to thefiscal divide, the separation of the professional cultures of physical and mental
68 Best Practices in Mental Health
Chapter 05_Chapter 05 4/16/13 11:04 AM Page 68

health systems can cause mutual mistrust and rivalry (BCMHL, 2004). Differ-ences between physical and mental health care provision can also exist in terms ofinformation storage and sharing, software compatibility, privacy rules, and pro-fessional standards.
This understanding of the multifaceted challenges of integrating health andmental health care for the population with serious mental illness led to the devel-opment of the Bridge peer health navigator intervention.
The Bridge: A Peer Health Navigator Intervention
The Bridge health navigator intervention was developed using a collaborativeapproach including the members of the research team, service providers, andpeers. The intervention was based on the model, presented above, of the barriersthat lead to problematic health access, utilization, and outcomes for people livingwith serious mental illness. The model addresses system bifurcation and practi-tioner issues, and is designed to assist clients regardless of their symptom severityor functional level. The use of peer intervention can help ameliorate stigma forclients, as peer experiences with mental illness may provide a common ground tobuild rapport, an essential component of this type of intervention. The Bridgeintervention moderates the impact of the factors that impede both service utiliza-tion and health outcomes by strengthening the enabling factors and amelioratingthe suppressing factors. The four components of the intervention are assessmentand planning, coordinated linkages, consumer education, and cognitve-behavioralstrategies. A central goal of the Bridge is to give clients the skills and experiencenecessary to self-manage their health care activities to the greatest degree possibleafter the intervention ends.
Assessing and Planning
In order to plan what assistance is needed, the navigator takes the clientthrough a thorough assessment of his or her health status, current use of healthservices, and experience with accessing and using health services, as well as bar-riers encountered. This process results in a collaborative health navigation plan,which includes the client’s health care and wellness goals (Mueser et al., 2006). Astep-by-step strategy is then developed to guide the goal-directed activity and toprovide a basis for monitoring progress. This activity increases clients’ awarenessof their health care needs and their history of health care service use, whichincreases their motivation to participate in navigation and self-managementstrategies.
Coordinated Linkages
Based on an integrated care linkage model (BCMHL, 2004), coordinated link-ages consist of several activities that assist clients as they navigate the health caresystem, including helping them make appointments, communicate with a range of
Reducing Health Disparities for People with Serious Mental Illness 69
Chapter 05_Chapter 05 4/16/13 11:04 AM Page 69

medical care providers, and ensure follow-up care; handling pharmacy and spe-cialty care issues; and ensuring adherence to medical treatment plans. This modelwas drawn partly from patient navigation interventions developed for people withcancer and people with HIV (Battaglia et al., 2007; Bradford et al., 2007; Darnell,2007; Dohan & Schrag, 2005; Jeste et al., 1996; Steinberg et al., 2006). Peer nav-igator experiences, with both their mental illness and their navigation of physicalhealth and mental health services, make them uniquely sensitive to and aware ofchallenges their peers face. The method is also based on the principles of AssertiveCommunity Treatment (Stein & Test, 1980; Test et al., 1991), in that an in vivoapproach to linkage and training activities is stressed. Compared to models thatpredominantly use a classroom training approach, (e.g., Goldberg et al., 2013), theBridge features an in vivo approach that develops self-management skills in real-world health care settings. The in vivo approach is important because these real-world health care settings are ideal for teaching and learning self-managementskills that are sustainable.
Consumer Education
The third intervention component is consumer education, which is based onprinciples of patient education (Prohaska & Lorig, 2000). Patient education is the-oretically rooted in the health belief model, in which an individual’s response toillness is rooted in his or her beliefs about health and health care. Hence, provid-ing knowledge to alter health beliefs can lead to better subjective perceptions ofhealth and better decisions about illness and its management (Goldman & Quinn,1988; Prohaska & Lorig, 2000). For the current intervention, the consumer edu-cation component includes education about the health care system, how to part-ner with medical providers, treatment compliance, self-advocacy, appropriateinteraction skills, and health and wellness issues (such as regular health care, diet,and exercise), as well as education about health benefits and entitlements.
Cognitive-Behavioral Strategies
The fourth intervention component is the use of cognitive-behavioral strate-gies to support behavior change and maintenance with regard to health care uti-lization, and is based on cognitive-behavioral and social learning theory (Dobson& Hamilton, 2002). Central to the intervention is a method for guiding the behav-ioral work, which is expressed explicitly and succinctly as for them, with them, bythem. Using behavioral strategies of modeling, role playing, coaching, and fading,peer navigators enhance client skill development, using a systematic process thatentails gradually shifting navigation activities to the client (fading) with the aim ofmaximizing the client’s management of his or her health care to the greatestextent possible.
As an example, making a medical appointment by phone can be challenging.At first, the navigator makes the appointment with the client watching and lis-
70 Best Practices in Mental Health
Chapter 05_Chapter 05 4/16/13 11:04 AM Page 70

tening on speaker phone (for them, or modeling). The next time, the client makesthe call with the navigator present as a coach, or as the receptionist in a role play(with them, or coaching). Finally, the navigator fades and lets the client make thephone call independently (by them) while continuing to act as a reinforcer, sup-porter, or collaborative problem solver if complications arise. Although theauthors prefer in vivo coaching and learning, role playing can also be done ifclients have sufficient skill. These strategies are complemented by user-friendlyself-instructional and self-help cognitive-behavioral strategy guides for the peernavigator. This training method is used for all skill building aspects of the inter-vention and becomes the foundation for self-management.
In addition to these four components, the intervention also addresses screeningand engagement, intervention target points, the intervention timeline, and out-comes.
Screening and Client Engagement
The Bridge intervention is based on appropriate screening and engagement.The authors have developed a six-item screening tool that targets current healthproblems and health service use. The tool is designed so that an inclusionaryresponse on any one of the six items indicates the need for health navigation. Thescreen can be administered in a self-report or interview format (in person or byphone). It has been used by health navigators, by case managers, and by staff aspart of agency intake forms. Once a positive screen occurs, the navigator meetswith the client (ideally in person) and uses an engagement script that details thenavigator intervention, the roles of the navigator and the client, the activities thatwill occur, and the timeline. One agency has used orientation groups to screen andengage clients.
Intervention Target Points
In practice, there are eight challenge points, identified as critical junctures byprior research and focus groups, at which peer navigators may intervene to facili-tate successful health care utilization. Figure 2 presents these points for interven-tion as well as the navigator role at each point. As can be seen, they range fromclient awareness of health care needs, through resource location, to follow-upcare.
Intervention Timeline
The Bridge is implemented in two phases. Phase one is characterized by fre-quent in-person contact between the peer health navigator and the client. This isan intensive four-month phase during which the navigator engages and helps theclient complete an initial assessment, collaborates with the client to develop healthand wellness goals and create a navigation plan, works with the client toward
Reducing Health Disparities for People with Serious Mental Illness 71
Chapter 05_Chapter 05 4/16/13 11:04 AM Page 71

72 Best Practices in Mental Health
Fig
ure
2
Bri
dg
e H
ealt
h N
avig
ato
r In
terv
enti
on
Co
nsu
mer
ch
alle
ng
e p
oin
ts t
o s
ucc
essf
ul h
ealt
h c
are
ou
tco
mes
Nav
igat
or
role
Hea
lth
an
dw
elln
ess
nee
ds
Co
nsu
mer
awar
enes
sSc
ann
ing
en
viro
nm
enta
lre
sou
rces
Init
ial
pro
vid
erco
nta
ct
Get
tin
g t
o t
he
app
oin
tmen
tW
aiti
ng
ro
om
exp
erie
nce
Exam
ro
om
exp
erie
nce
Trea
tmen
tp
lan
an
dfo
llow
-up
1. W
ork
with
serv
ice
coor
dina
tors
and
men
tal
heal
thpr
ovid
ers
toas
sess
co
nsum
erne
ed f
or
navi
gatio
n.
2. C
ondu
cthe
alth
car
ese
rvic
e sc
reen
ing
with
cons
umer
s.
3. H
elp
with
insu
ranc
e be
nefit
s as
nece
ssar
y.
1. C
ondu
cthe
alth
and
wel
lnes
sas
sess
men
tsw
ith
cons
umer
s.
2. W
ork
with
cons
umer
s to
set
heal
th a
ndw
elln
ess
goal
san
d th
e m
eans
to a
chie
veth
ose
goal
s.
3. P
rovi
de h
ealth
educ
atio
n ta
ilore
d to
cons
umer
’sgo
als.
1. F
ind
prov
ider
san
d/or
hea
lthcl
inic
s.
2. D
evel
op
rela
tions
hips
with
pro
vide
rsan
d cl
inic
s.
3. F
ind
insu
ranc
ean
d/or
be
nefit
s in
form
atio
n.
1. A
ssis
t w
ithm
akin
gap
poin
tmen
ts(r
ole
play
an
d in
viv
o).
2. C
oach
co
nsum
er in
mak
ing
appo
intm
ents
.
1. P
rovi
deap
poin
tmen
tre
min
ders
.
2. A
ssis
t w
ith
and
coac
hre
gard
ing
tran
spor
tatio
nne
eds.
1. H
elp
with
prov
ider
form
s.
2. M
odel
in
tera
ctio
nsw
ith s
taff
and
othe
r pa
tient
s (r
ole
play
and
invi
vo).
3. C
oach
in
tera
ctio
nsw
ith s
taff
and
patie
nts
(invi
vo).
4. A
ct a
s st
igm
a bu
ffer
.
1. M
odel
in
tera
ctio
nsw
ith m
edic
alpe
rson
nel
(rol
e pl
ay
and
in v
ivo)
.
2. C
oach
in
tera
ctio
nsw
ith m
edic
alpe
rson
nel (
invi
vo).
3. H
elp
cons
umer
com
mun
icat
ene
eds.
4. A
ct a
s st
igm
a bu
ffer
.
1. A
ssis
t w
ithtr
eatm
ent
com
plia
nce,
trea
tmen
tpl
an,
follo
w-
up o
r sp
ecia
lty
care
, an
d pr
escr
iptio
ns.
Chapter 05_Chapter 05 4/16/13 11:04 AM Page 72

achieving the goals, helps the client navigate through the health care system, andprovides active health education and skill building to shape and reinforce positivebehavior and move the client toward more independence. An in vivo navigationapproach is preferred for modeling and coaching, although this depends on clientpreference and skill. This means that navigators routinely accompany clients ondoctor, pharmacy, and lab visits in order to build their competence and indepen-dence, and to help with the transition to self-management.
Phase two is a two-month step-down phase in which clients’ health activitiesbecome increasingly more independent. In phase two, the health navigator con-nects with the client via phone or in person once a week or as needed to check onhis or her progress; help troubleshoot emerging health-care-related issues; andprovide support for the client to facilitate progress toward established goals, revisegoals, or set new goals. The length of phase two depends on the needs of the clientas some clients require step-down support for longer than others.
Although a timetable has been offered for the intervention, it is a general guide-line and subject to variation based on the intensity of client need. The authorshave found that individualization of both phases is critical, as clients progress atdifferent rates in learning the skills for autonomous health navigation and self-management.
Outcomes
Outcomes targeted by the Bridge intervention have been classified as proximalor distal. Proximal health outcomes include increased use of ambulatory and out-patient care, decreased usage of emergency room and urgent care health services,improved health status, increased health care self-efficacy, greater satisfactionwith health care, and higher health-related quality of life. Distal outcomes includebetter general life satisfaction, improved functional outcomes, and higher self-esteem.
Feasibility Test of the Bridge
Clinic Sites
The Bridge peer health navigator intervention was implemented at two outpa-tient mental health clinics in Los Angeles. Both sites are part of a large contractprovider called Pacific Clinics that serves 3,500 clients annually and has largenumbers of clients in need of assistance with coordinating health care services.The sites were selected because of their willingness and capacity to participate inimplementing this pilot intervention. The clients were enrolled in full-service part-nerships that targeted the most functionally impaired and highest users of mentalhealth services, those with histories of homelessness, or those most in need ofengagement in intensive mental health services. The intervention featured lowcaseloads (20:1) and was based on an Assertive Community Treatment approach(Gilmer, Stefancic, Manning, Ettner, & Tsemberis, 2010).
Reducing Health Disparities for People with Serious Mental Illness 73
Chapter 05_Chapter 05 4/16/13 11:04 AM Page 73

Peer Navigator Qualifications
Because the peer navigator is a crucial component of this intervention, mem-bers of the research team and service providers reviewed the qualificationsrequired to be a successful navigator. Several local agencies offer a comprehensivepeer mental health worker training program that combines ten weeks of class-room instruction with six weeks of intensive internship at a mental health agency.It was agreed that peer health navigators should participate in an official trainingprogram to learn the skills necessary for working in a mental health clinic setting.Other mutually approved qualifications for a peer navigator were good communi-cation skills, flexibility, ability to work well in a variety of settings, capacity todevelop rapport with peers, and comfort in communicating with mental healthand medical professionals.
Navigator Training
Peer health navigator training was initially conducted at one of the participat-ing sites. The navigator was placed at the site and worked with different teams. Hespent two months shadowing clinic nurses, team leaders, and service providers toget a sense of the operation, workflow, and ethos of the clinic. After this two-month period, the navigator began working with clients to pilot test the assess-ment tools and began testing the navigator model. During this time, he received in-depth training with the research team about the health navigator model and thetheory supporting it, background on understanding the scope of the problem, set-ting boundaries, avoiding dual relationships, setting up a supervision plan, deal-ing with stress on the job, and becoming integrated into the staff culture of theclinic.
Manual Development
Using information gathered from the needs assessment combined with thestage model of manual development (Carroll & Nuro, 2002), the authors havemanualized the Bridge intervention. The stage model proposes three differentstages for manual development (Carroll & Nuro, 2002; Carroll & Rounsaville,2008). The advantage of this model is that it leads to a manual that is well testedin a variety of settings and with different populations. A drawback is the length oftime needed to move from bench to clinic, which contributes to a disconnectbetween research and practice that needs to be addressed (Dobson & Hamilton,2002; Moras, 2002). Thus, the authors used a modified version of the stagemodel, which emphasizes working closely and continuously with practitioners toensure that the manual is applicable to the real world and to allow it to be dissem-inated more quickly (Moras, 2002). To do this, a manual development workinggroup was created, including members of the research team, clinic staff, and thehealth navigator. This working group method allowed the authors to receive con-tinuous feedback on the manual contents, and resulted in ongoing refinement andimproved utility in a real-world setting.
74 Best Practices in Mental Health
Chapter 05_Chapter 05 4/16/13 11:04 AM Page 74

The manual includes detailed instructions, scripts, and forms for screening,engagement, assessment, goal setting, planning for medical visits (physician, lab,or pharmacy), post-visit review, and monitoring progress. It also explicates the forthem, with them, by them training method and offers client education material.
Fidelity and Monitoring
The authors have developed protocols for establishing and maintaining fidelityto the Bridge, as well as strategies for monitoring the extent of implementation atan agency. The fidelity tool consists of rating the navigator’s competence inaccomplishing the critical elements of the intervention. This evaluation is basedon in vivo observation, verbal case descriptions, and record review. The extent ofimplementation is monitored via a software program that requires the navigatorto list both client contacts and contacts on behalf of the client, as well as the loca-tion, length, and topic of each contact.
Results from Pilot Data
Preliminary data on the feasibility, outcomes, and implementation of the Bridgehave been obtained from seven clients who received the intervention during thisearly developmental phase. Concerning outcomes, data have been received fromfour clients who completed baseline and follow-up assessments after six months ofthe intervention. These four clients showed positive changes in the total number ofcurrent health problems (baseline M = 6.5, SD = 0.7; follow-up M = 4.0, SD = 0.8;Mann-Whitney z = –2.4, p < .03) and an increase in the number of health screen-ings in the previous six months (baseline M = 1.75, SD = 1.00, follow-up M = 4.25, SD = 1.9; Mann-Whitney z = 2.1, p < .06). The number of medical hos-pital admissions began low and stayed low, as did the number of emergency roomvisits for physical problems. There was a decline in the number of outpatient visitsto primary care providers in the previous six months (baseline M = 6.5, SD = 4.6;follow-up M = 3.3, SD = 3.4) that was not statistically significant. According to thenavigator, this reduction was due to better follow-up care procedures that reducedvisits for the same health problems over time. Based on these highly preliminarydata, there is some suggestion that the intervention could be related to improvedhealth status and more appropriate use of outpatient services.
Pilot data on the quantity of client contacts were also analyzed. Of the sevenfully engaged clients, the average contacts made with or on their behalf were 2.3per week, with a range of 1.4 to 2.8 contacts per week. Eighty percent of the con-tacts were with the client, and 20 percent were with another person on behalf ofthe client. These contacts spread somewhat evenly between in-person (60%) andphone contacts (40%). Based on field notes kept by the navigator, the duration ofthe contacts ranged from under five minutes to over four hours. The navigatorreported that he moved to the step-down phase with all clients, during which the contacts decreased by over 75 percent as clients transitioned to more self-management of their health care.
Reducing Health Disparities for People with Serious Mental Illness 75
Chapter 05_Chapter 05 4/16/13 11:04 AM Page 75

The range of health-related issues among pilot clients was enormous. Six ofseven clients had not had any routine care from a primary care physician in sev-eral years. Most identified their psychiatrist as their primary medical care doctor.Only one individual had had an eye exam in the previous five years. Only oneclient had a regular dentist. One individual had ongoing foot lesions that resultedin repeated hospitalizations due to inadequate treatment follow-up. Most clientsused the hospital as their routine health care provider. The navigator securedhealth benefits for one undocumented Latino and accompanied most clients ondoctor visits. During these visits issues ranged from communication problemswith nurses and doctors to difficulties handing the waiting room and exam roomexperiences. There were also frequent problems with treatment compliance thatresulted in ongoing and increasingly serious health problems and overuse ofemergency services. One individual was too anxious to take public transportationto the medical clinic, so the navigator first accompanied her and sat next to her onthe bus; on subsequent trips he sat several seats behind her, and then he drovebehind the bus as she rode alone, all to encourage independence through reducednavigator presence.
Best Practice for Work with Persons with Severe Mental Illness
There were many navigator contacts to ensure follow-up care and treatmentcompliance. Pharmacy interactions and managing multiple medications werefound to be common difficulties for clients. Pharmacy personnel were pleased towork with the navigator as they reported challenges in working with individualswith serious mental illness. Health care physicians and nurses were generally wel-coming to the navigator and most often allowed him into the examining room.Once they had worked with the navigator, physicians actively engaged his servicesand felt he improved the effectiveness of the medical visit.
Because the work can be stressful, supervision and support of the peer naviga-tor is a crucial aspect of this intervention. To address this, the peer health naviga-tor met weekly, or as needed, with the project manager to debrief, talk about whatwas working and not working, and discuss any troubling situations. The healthnavigator also participated in weekly team meetings to discuss navigation-relatedissues with the project team.
Agency Integration
The authors have found that working closely with mental health agency staffis critical to adequately integrating peer health navigation into the agency clinicalmodel. For example, staff suggested that the peer health navigator be included inteam meetings, and that goals and treatment plans be shared (considering com-pliance issues) so that coordination and integration could be achieved. Otherforms of inclusion and communication have developed over time that facilitate theintegration of health navigator services. If mental health agencies have not previ-ously integrated peers into their approach, professional staff are required to takeon additional work.
76 Best Practices in Mental Health
Chapter 05_Chapter 05 4/16/13 11:04 AM Page 76

Next Steps
The purpose of this article was to describe the development, implementation,and feasibility of a peer health navigator intervention called the Bridge. Theauthors developed the Bridge peer health navigator intervention for many rea-sons. Several service models have been advocated for dealing with the physicalhealth of those with serious mental illnesses, yet models of care that integrate carethrough co-situation of services require multiple structural and financial changesto the existing health care system. A care linkage model, such as the Bridge,improves collaboration between independent health and mental health providers,and can be used in the context of many existing financing and service structurearrangements. The use of peer health navigators is an emerging best practice foraddressing health needs of people living with serious mental illness. There is accu-mulating evidence that peer-based services can improve outcomes in health andin other aspects of recovery among people living with serious mental illness, andare also cost effective (Rosenick & Rosenheck, 2008).
The results from the feasibility work reported here are encouraging. Theauthors are currently analyzing data from a small randomized trial (n = 24) ofthe Bridge intervention, and are refining the treatment manual. They are alsoworking on an agency implementation and sustainability protocol, which will bemanualized to deal with both administrative and intervention integration issuesat the staff level, and they have developed protocols for training new peer healthnavigators. Nonpeer paraprofessionals and professionals have recently beentrained in the Bridge intervention, but the use of professionals has proven difficultdue to cost considerations. Finally, the Bridge intervention was developed using apopulation with serious mental illness that was very functionally impaired andliving in an urban area. As the effectiveness of this intervention is investigatedfurther, it will be important to consider the degree to which the intensity of theintervention and its in vivo approach are required for other less challenged popu-lations and settings.
ReferencesAnderson, G., & Knickman, J. R. (2001). Changing the chronic care system to
meet people’s needs. Health Affairs, 20(6), 146–160.Battaglia, T. A., Roloff, K., Posner, M. A., & Freund, K. M. (2007). Improving
follow-up to abnormal breast cancer screening in an urban population: A patient navigation intervention. Cancer, 109(Suppl. 2), 359–367.
Bazelon Center for Mental Health Law. (2004). Get it together: How to integratephysical and mental health care for people with serious mental disorders.Washington, DC: Author. Retrieved from http://www.bazelon.org/News-Publications/Publications/.
Berren, M. R., Santiago, J. M., Zent, M. R., & Carbone, C. P. (1999). Health careutilization by persons with severe and persistent mental illness. Psychi-atric Services, 50(4), 559–561.
Reducing Health Disparities for People with Serious Mental Illness 77
Chapter 05_Chapter 05 4/16/13 11:04 AM Page 77

Bradford, J. B., Coleman, S., & Cunningham, W. (2007). HIV system navigation:An emerging model to improve HIV care access. AIDS patient care andSTDs, 21(Suppl. 1), S49–S58.
Brown, V. (1998). Untreated physical health problems among women diagnosedwith serious mental illness. Journal of the American Medical Women’s Asso-ciation, 53(4), 159–160.
Brunero, S., & Lamont, S. (2010). Health behaviour beliefs and physical healthrisk factors for cardiovascular disease in an outpatient sample of con-sumers with a severe mental illness: A cross-sectional survey. Interna-tional Journal of Nursing, 47(6), 753–760.
Carney, C. P., Allen, J., & Doebbeling, B. N. (2002). Receipt of clinical preventivemedical services among psychiatric patients. Psychiatric Services, 53(8),1028–1030.
Carroll, K. M., & Nuro, K. F. (2002). One size cannot fit all: A stage model for psychotherapy manual development. Clinical Psychology: Science and Practice, 9(4), 396–406.
Carroll, K. M., & Rounsaville, B. J. (2008). Efficacy and effectiveness in develop-ing treatment manuals. In A. M. Nezu & C. M. Nezu (Eds.), Evidence-basedoutcomes research: A practical guide to conducting randomized controlled trialsfor psychosocial interventions (pp. 219–243). New York: Oxford UniversityPress.
Cohen, J. W., & Krauss, N. A. (2003). Spending and service use among peoplewith the fifteen most costly medical conditions. Health Affairs, 22(2),129–138.
Compton, M. T., Daumit, G. L., & Druss, B. G. (2006). Cigarette smoking andoverweight/obesity among individuals with serious mental illnesses: A preventive perspective. Harvard Review of Psychiatry, 14(4), 212–222.
Cook, J. A. (2005). “Patient-centered” and “consumer-directed” mental health services.Report repared for the Institute of Medicine, Committee on Crossing theQuality Chasm–Adaptation to Mental Health and Addictive Disorders.University of Illinois at Chicago.
Dalmau, A., Bergman, B., & Brismar, B. (1997). Somatic morbidity in schizo-phrenia—A case control study. Public Health, 111(6), 393–397.
Darnell, J. S. (2007). Patient navigation: A call to action. Social Work, 52(1),81–84.
Davidson, L., Chinman, M., Kloos, B., Weingarten, R., Stayner, D., & Tebes, J. K.(1999). Peer support among individuals with severe mental illness: A review of the evidence. Clinical Psychology: Science and Practice, 6(2),165–187.
Davidson, L., Chinman, M., Sells, D., & Rowe, M. (2006). Peer support amongadults with serious mental illness: A report from the field. SchizophreniaBulletin, 32(3), 443–450.
78 Best Practices in Mental Health
Chapter 05_Chapter 05 4/16/13 11:04 AM Page 78

Deakin, B., Ferrier, N., Holt, R. I. G., Millar, H., Nutt, D., Reynolds, G., . . . Taylor, D.(2010). The physical health challenges in patients with severe mental ill-ness: Cardiovascular and metabolic risks. Journal of Psychopharmacology,24(Suppl. 1), 1–8.
De Hert, M., Correll, C. U., Bobes, J., Cetkovich-Bakmas, M., Cohen, D., Asai, I., . . .Leucht, S. (2011). Physical illness in patients with severe mental disor-ders. I. Prevalence, impact of medications and disparities in health care.World Psychiatry, 10(1), 52–77.
Desai, M. M., Rosenheck, R. A., Druss, B. G., & Perlin, J. B. (2002). Mental disor-ders and quality of diabetes care in the veterans health administration.American Journal of Psychiatry, 159(9), 1584–1590.
Dickerson, F. B., Brown, C. H., Daumit, G. L., Lijuan, F., Goldberg, R. W.,Wohlheiter, K., & Dixon, L. B. (2006). Health status of individuals withserious mental illness. Schizophrenia Bulletin, 32(3), 584–589.
Dickerson, F. B., Brown, C. H., Fang, L., Goldberg, R. W., Kreyenbuhl, J.,Wohlheiter, K., & Dixon, L. B. (2008). Quality of life in individuals withserious mental illness and type 2 diabetes. Psychosomatics, 49(2),109–114.
Dickerson, F. B., Goldberg, R. W., Brown, C. H., Kreyenbuhl, J., Wohlheiter, K.,Fang, L., . . . Dixon, L. B. (2005). Diabetes knowledge among personswith serious mental illness and type 2 diabetes. Psychosomatics, 46(5),418–424.
Dickerson, F. B., McNary, S. W., Brown, C. H., Kreyenbuhl, J., Goldberg, R. W., &Dixon, L. B. (2003). Somatic healthcare utilization among adults withserious mental illness who are receiving community psychiatric services.Medical Care, 41(4), 560–570.
Dickey, B., Normand, S. T., Weiss, R. D., Drake, R. E., & Azeni, H. (2002). Medicalmorbidity, mental illness, and substance use disorders. Medical Illness andSevere Mental Illness, 53(7), 861–867.
Dobson, K. S., & Hamilton, K. E. (2002). The stage model for psychotherapymanual development: A valuable tool for promoting evidence-based practice. Clinical Psychology: Science and Practice, 9(4), 407–409.
Dohan, D., & Schrag, D. (2005). Using navigators to improve care of underservedpatients. Cancer, 104(4), 848–855.
Druss, B., & Newcomer, J. (2007). Challenges and solutions to integrating mentaland physical health care. Journal of Clinical Psychiatry, 68(4), e09.
Druss, B. G., Rask, K., & Katon, W. J. (2008). Major depression, depression treat-ment and quality of primary medical care. General Hospital Psychiatry,30(1), 20–25.
Druss, B. G., Rosenheck, R. A., Desai, M. M., & Perlin, J. B. (2002). Quality of preventive medical care for patients with mental disorders. Medical Care,40(2), 129–136.
Reducing Health Disparities for People with Serious Mental Illness 79
Chapter 05_Chapter 05 4/16/13 11:04 AM Page 79

Druss, B. G., von Esenwein, S. A., Compton, M. T., Rask, K. J., Zhao, L., & Parker,R. M. (2010). A randomized trial of medical care management for com-munity mental health settings: The primary care access, referral, andevaluation (PCARE) study. American Journal of Psychiatry, 167(2),151–159.
Druss, B. G., Zhao, L., von Esenwein, S., Bona, J. R., Fricks, L., Jenkins-Tucker, S.,. . . Lorig, K. (2010). The Health and Recovery Peer (HARP) Program: A peer-led intervention to improve medical self-management for personswith serious mental illness. Schizophrenia Research, 118(1–3), 264–270.
Gelberg, L., Andersen, R. M., & Leake, B. D. (2000). The behavioral model forvulnerable populations: Application to medical care use and outcomes forhomeless people. Health Services Research, 34(6), 1273–1302.
Gianfrancesco, F. D., Grogg, A. L., Mahmoud, R. A., Wang, R., & Nasrallah, H. A.(2002). Differential effects of risperidone, olanzapine, clozapine, and con-ventional antipsychotic on type 2 diabetes: Findings from a large healthplan database. Journal of Clinical Psychiatry, 63(10), 920–930.
Gilmer, T., Stefancic, A., Manning, W., Ettner, S., & Tsemberis, S. (2010). Effect offull-service partnerships on homelessness, use and costs of mental healthservices, and quality of life among adults with serious mental illness.Archives of General Psychiatry, 67(6), 645–652.
Goldberg, R. J. (1999). Financial incentives influencing the integration of mentalhealth care and primary care. Psychiatric Services, 50, 1071–1075.
Goldberg, R. W., Dickerson, F., Lucksted, A., Brown, C. H., Weber, E., Tenhula, W. N., . . . Dixon, L. B. (2013). Living well: An intervention to improveself-management of medical illness for individuals with serious mentalillness. Psychiatric Services, 64(1), 51–57.
Goldberg, R. W., Kreyenbuhl, J. A., Medoff, D. R., Dickerson, F. B., Wohlheiter, K.,Fang, L. J., . . . Dixon, L. B. (2007). Quality of diabetes care among adultswith serious mental illness. Psychiatric Services, 58(4), 536–543.
Goldman, C. R., & Quinn, F. (1988). Effects of a patient education program in the treatment of schizophrenia. Hospital Community Psychiatry, 39(3),282–286.
Hedberg, I., & Skärsäter, I. (2009). The importance of health for persons withpsychiatric disabilities. Journal of Psychiatric and Mental Health Nursing,16(5), 455–461.
Hippisley-Cox, J., Vinogradova, Y., Coupland, C., & Parker, C. (2007). Risk ofmalignancy in patients with schizophrenia or bipolar disorder: Nestedcase-control study. Archives of General Psychiatry, 64(12), 1368–1376.
Jandorf, L., Fatone, A., Borker, P. V., Levin, M., Esmond, W., Brenner, B., . . .Redd, W. H. (2006). Creating alliances to improve cancer preventionand detection among urban medically underserved minority groups.Cancer, 107(Suppl. 8), 2043–2051.
Jeste, D. V., Gladsjo, J. A., Lindamer, L. A., & Lacro, J. P. (1996). Medical comor-bidity in schizophrenia. Schizophrenia Bulletin, 22(3), 413–430.
80 Best Practices in Mental Health
Chapter 05_Chapter 05 4/16/13 11:04 AM Page 80

Kane, J. M. (2009). Creating a health care team to manage chronic medical ill-nesses in patients with severe mental illness: The public policy perspec-tive. Journal of Clincal Psychiatry, 70(Suppl. 3), 37–42.
Kreyenbuhl, J. A. (1999). Correlates of psychopharmacologic treatment outcomes forschizophrenia (Doctoral dissertation). Retrieved from http://hdl.handle.net/10713/1240.
Laws, K., Gabriel, R., & McFarland, B. (2002). Integration and its discontents:Substance abuse treatment in the Oregon health plan. Health Affairs,21(4), 284–289.
Leigh, H., Stewart, D., & Mallios, R. (2006). Mental health and psychiatry train-ing in primary care residency programs. II. What skills and diagnoses aretaught, how adequate, and what affects training directors’ satisfaction?General Hospital Psychiatry, 28(3), 195–204.
Lester, H. E., Tritter, J. Q., & Sorohan, H. (2005). Providing primary care for people with serious mental illness: Focus group study. British MedicalJournal, 330(7500), 1122–1128.
Lieberman, A. A., & Coburn, A. F-. (1986). The health of the chronically men-tally ill: A review of the literature. Community Mental Health Journal,22(2), 104–116.
Link, B. G. (1987). Understanding labeling effects in the area of mental disor-ders: An assessment of the effects of rejection. American SociologicalReview, 52, 96–112.
Link, B. G., & Phelan, J. C. (2001). Conceptualizing stigma. Annual Review of Sociology, 27, 363–385.
Maj, M. (2009). Physical health care in persons with severe mental illness: A public health and ethical priority. World Psychiatry, 8(1), 1–2.
Miller, C. L., Druss, B. G., Dombrowski, E. A., & Rosenheck, R. A. (2003). Barriersto primary medical care among patients at a community mental healthcenter. Psychiatric Services, 54(8), 1158–1160.
Moras, K. (2002). A tool to advance the effectiveness and dissemination ofempirically supported psychotherapies and the NIMH public healthresearch agenda. Clinical Psychology: Science and Practice, 9(4), 425–430.
Mueser, K. T., Meyer, P. S., Penn, D. L., Clancy, R., Clancy, D. M., & Salyers, M. P.(2006). The illness management and recovery program: Rationale, devel-opment, and preliminary findings. Schizophrenia Bulletin, 32(Suppl. 1),S32–S43.
New Freedom Commission on Mental Health. (2003). Achieving the promise:Transforming mental health care in America. Final report (DHHS Pub. No.SMA-03-3832). Rockville, MD: Author.
Parks, J., Svendsen, D., Singer, P., & Foti, M. E. (2006). Morbidity and mortality inpeople with serious mental illness. Alexandria, VA: National Association ofState Mental Health Program Directors (NASMHPD) Medical DirectorsCouncil. Accessed at http://www.nasmhpd.org/docs/publications/MDCdocs/ MortalityandMorbidityFinalReport08.18.08.pdf.
Reducing Health Disparities for People with Serious Mental Illness 81
Chapter 05_Chapter 05 4/16/13 11:04 AM Page 81

Prohaska, T. R., & Lorig, K. (2000). The role of theory in patient education. In K. Lorig (Ed.), Patient education: A practical approach (3rd ed.). ThousandOaks, CA: Sage.
Rosenick, S. G., & Rosenheck, R. A. (2008). Integrating peer-provided services: A quasi-experimental study of recovery orientation, confidence, andempowerment. Psychiatric Services, 59(11), 1307–1314.
Scheff, T. (1994). Being mentally ill: A sociological theory (3rd ed.). Chicago:Aldine.
Shattell, M. M., Donnelly, N., Scheyett, A., & Cuddeback, G. S. (2011). Assertivecommunity treatment and the physical health needs of persons withsevere mental illness: Issues around integration of mental health andphysical health. Journal of American Psychiatric Nurses Association, 17(1),57–63.
Solomon, P. (2004). Peer support/peer provided services underlying processes,benefits, and critical ingredients. Psychiatric Rehabilitation Journal, 27(4),392–401.
Stein, L. I., & Test, M. A. (1980). An alternative to mental health treatment. I.Conceptual model, treatment program, and clinical evaluation. Archivesof General Psychiatry, 37(4), 392–397.
Steinberg, M. L., Fremont, A., Khan, D. C., Huang, D., Knapp, H., Karaman, D., . . .Streeter, O. E. (2006). Lay patient navigator program implementation forequal access to cancer care and clinical trials. Cancer, 107(11), 2669–2677.
Stroul, B. A., Pires, S. A., & Armstrong, M. (2001). Healthcare Reform TrackingProject: Tracking state managed care reforms as they affect children and adoles-cents with behavioral health disorders and their families: 2000 State Survey.Research and Training Center for Children’s Mental Health, Departmentof Child and Family Studies, Louis de la Parte Florida Mental Health Insti-tute, University of South Florida.
Test, M. A., Knoedler, W. H., Allness, D. J., Burke, S. S., Brown, R. L., & Wallisch,L. S. (1991). Long-term community care through an assertive continu-ous treatment team. In C. A. Tamminga and S. C. Schulz (Eds.), Advancesin neuropsychiatry and psychopharmacology: Schizophrenia research (Vol. 1,pp. 239–246). New York: Raven Press.
Vogel, C. (2001). Mental health “boundaries” in Medicaid managed care. Princeton,NJ: Mathematics Policy Research, Inc.
82 Best Practices in Mental Health
Chapter 05_Chapter 05 4/16/13 11:04 AM Page 82

Implementation of evidence-based practices (EBPs) and emerging best practices is animportant component of providing effective mental health services. If EBPs are notimplemented properly, their efficacy is reduced. Implementation efforts are in vain ifprograms cannot sustain the EBP after initial startup or after achieving fidelity. There-fore, sustainability is an essential element of implementation. This article details a con-ceptual framework for the development of the EBP Sustainability Index, a scale beingpiloted at the University of Kansas that helps measure whether programs are at risk ofdiscontinuing an implemented EBP. Forewarning about possible discontinuance allowsconsultants, staff, and administrators to develop plans to ensure sustainability ratherthan de-adoption.
Key words: evidence-based practice; framework; implementation; sustainability
Sustainability is essential to adequate implementation of evidence-based practices(EBPs) in mental health. If EBPs are not sustained, the positive outcomes associ-ated with the mental health practice will likely diminish. Implementation sciencerefers to the study of elements influencing the distribution, implementation, andsustainability of EBPs. Fortunately, significant progress has been made in develop-ing frameworks and strategies for adequate implementation of an EBP at start-up(McHugo et al., 2007). However, knowledge about how to sustain an EBP overtime is lacking. Issues such as financial backing, supervisory and staffing prob-lems, organizational structure, and incompatible policies all influence whether anEBP remains in place.
Brief Report:
Conceptual Underpinnings of the Evidence-Based Practice Sustainability Index
Trevor J. Manthey and Rick Goscha
Trevor J. Manthey, MSW, is consultant trainer and graduate research assistant in the Office ofMental Health Research and Training, University of Kansas School of Social Welfare, Lawrence,Kansas. Rick Goscha, MSW, PhD, is director of the Office of Mental Health Research and Train-ing, University of Kansas School of Social Welfare, Lawrence, Kansas.
© 2013 Lyceum Books, Inc., Best Practices in Mental Health, Vol. 9, No. 1, March 2013
Chapter 06_Chapter 06 4/16/13 11:04 AM Page 83

To address this issue, the University of Kansas School of Social Welfare is pilot-ing an EBP Sustainability Index (SI). The SI is used to determine whether an EBPis at risk of being discontinued. This article will describe the background contextleading to development of the SI, an operational definition of sustainability, andthe conceptual underpinnings of each assessment item.
Background
Effective implementation and maintenance of mental health EBPs are primaryconcerns for social work and many other human service fields (Aarons, Hurlburt,& Horwitz, 2011; Bellamy, Bledsoe, & Traube, 2006; Farkas, Gagne, Anthony, &Chamberlin, 2005; Gotham, 2004; McHugh & Barlow, 2010; McNeese & Thyer,2008; Proctor et al., 2009). Empirical support undergirds evidence-based andemerging best practices to verify that they provide effective outcomes and services.However, there is also increasing evidence that service improvement is as muchinfluenced by the process of implementation as it is by the practices that are cho-sen for implementation (Drake, Bond, & Essock, 2009). Conducting training is notsufficient to teach the complex skills that are often required for EBPs (Fixsen,Blase, Naoom, & Wallace, 2009). This finding has been replicated in many fieldsincluding health care (Grol & Grimshaw, 1999) and mental health (Drake et al.,2009), and in systematic reviews of implementation efforts across a variety offields (Naoom, Blase, Friedman, & Wallace, 2005). Since the 1970s, research hasindicated that the train and hope approach to implementation (i.e., conducting atraining and then hoping that skills are retained or that a model is implemented;Stokes & Baer, 1977) is not effective.
In the human services domain, EBP implementation is generally considered tobe more complex than in other domains “because they [the EBPs] are deliveredthrough the actions of individuals and organizations, which exist within complex,multi-layered social contexts” (Aarons et al., 2011, p. 5). Therefore, multicompo-nent implementation strategies are needed to address the challenges of effectiveimplementation (Fixsen et al., 2009; Glisson & Schoenwald, 2005; Grimshaw etal., 2001; Grol & Grimshaw, 1999).
Over the last twelve years, the University of Kansas School of Social Welfare hascollaborated with Dartmouth College and other organizations throughout theUnited States to complete the largest study to date of the implementation of EBPsfor individuals with psychiatric disabilities (Bond, Drake, McHugo, Rapp, & Whitley,2009; Drake et al., 2001; McHugo et al., 2007; Torrey et al., 2001; Torrey, Lynde,& Gorman, 2005). In this project, termed the National EBP Project, researchersdeveloped and then tested a comprehensive EBP implementation approach thatincluded the following features (Torrey, Finnerty, Evans, & Wyzik, 2003):
• consultation to the state mental health authority• consultation to community mental health center administrators• a kickoff presentation to the provider organization• provision of the EBP tool kit to the organization
84 Best Practices in Mental Health
Chapter 06_Chapter 06 4/16/13 11:04 AM Page 84

• initial skill training for practitioners• ongoing site consultation• systematic fidelity monitoring
Fidelity monitoring included two steps:
1. fidelity assessments based on daylong site visits by a pair of independentfidelity assessors who, guided by fidelity scale criteria, conduct structuredinterviews, observe team meetings and interventions, and review medicalrecords; and
2. fidelity review meetings with agency leaders in which assessors give oraland written feedback on quality of implementation (Bond et al., 2009).
In Kansas, five mental health evidence-based or emerging best practices wereimplemented using this National EBP Project implementation approach:
1. Supported Employment (Bond, 2007; Manthey, Rapp, Carlson, Holter, &Davis, 2012)
2. Integrated Dual Disorder Treatment (Wieder & Kruszynski, 2007)3. Strengths Model Case Management (Rapp & Goscha, 2011)4. Family Pyscho-education (Polio, North, & Osborne, 2002)5. Supported Education (Manthey, 2011; Mowbray et al., 2005)
Additional efforts are underway to use the national EBP implementation approachfor additional practices: supported housing (Grant & Westhues, 2010), illnessmanagement and recovery (Salyers, Rollins, McGuire, & Gearhart, 2009), andCommonGround shared decision making (Deegan, 2007).
At the national level, this implementation model was tested at more than fiftysites across eight states. At each site at least one EBP was implemented. Each sitewas followed for a two-year period using a combination of qualitative and quanti-tative methodologies. Outcomes were assessed at baseline and at six-month inter-vals for two years by using EBP fidelity scales and other measures. None of thesites attained high fidelity at baseline; however, most sites increased fidelity scoresduring the first year and attained high fidelity scores at or within two years(McHugo et al., 2007).
Data from the national EBP implementation project have led to more than fiftyarticles published in peer-reviewed journals. These include articles that report onthe overall implementation outcomes across EBPs (Bond et al., 2009; McHugo etal., 2007; Rapp, Goscha, & Carlson, 2010) and on findings for specific models.These articles reveal a wide range of accomplishments including successful imple-mentation and the associated results that each EBP was intended to achieve.
Although the overall findings from the National EBP Project have been encour-aging, some broad studies noted barriers to successful implementation and sustainability (e.g., Rapp et al., 2008; Rapp et al., 2009). In addition, many
Brief Report 85
Chapter 06_Chapter 06 4/16/13 11:04 AM Page 85

researchers studying individual EBPs noted potential sustainability concerns thatwere consistent across practices. For instance, it was found that outcome trackingand clear feedback loops were important for the implementation of IntegratedDual Disorder Treatment (Chandler, 2009), Supported Employment (Marshall,Rapp, Becker, & Bond, 2008), and Assertive Community Treatment (Bjorklund,Monroe-DeVita, Reed, Toulon, & Morse, 2009).
In addition, in one relevant mixed methods study, both qualitative and quanti-tative findings suggested that there were at least five warning signs that may indi-cate that an organization may de-adopt a practice (Massatti, Sweeney, Panzano, &Roth, 2008):
1. lack of financial resources2. indications that external agents do not support the organization’s imple-
mentation effort3. problems related to attracting and retaining qualified staff4. indications that the practice does not fit well either with employee knowl-
edge and skills or with the organization’s mission and treatment philosophy5. reports that the practice is neither easy to implement nor seen as a perma-
nent part of the organization’s regular service offerings
Similar themes were repeated and recognized by other researchers (e.g., Blasinsky,Goldman, & Unutzer, 2006; Jansen, Van Den Bosch, & Volberda, 2005; Rapp et al.,2010). Although there are scales such as the General Organizational Index (Sub-stance Abuse and Mental Health Services Administration, 2002) that help assessan organization’s readiness for EBP implementation, there are no scales yet devel-oped that focus on a program’s ability to sustain a practice.
In order to address these sustainability issues, researchers at the University ofKansas School of Social Welfare created the EBP Sustainability Index. Items on thesustainability index were developed by assessing national EBP studies, reviewingthe implementation and sustainability literature, and receiving feedback fromconsultants and trainers who helped implement EBPs in the field.
Operationalizing Sustainability
In order to clearly demarcate the difference between implementation and sus-tainability, it is important to clearly define the two terms. Wiltsey-Stirman (2010)conducted a systematic review of sustainability that included forty studies acrossmany fields of human service. It was found that definitions diverged greatly andmany researchers did not operationalize sustainability at all. Implementation isdefined as helping a program meet the standards for high fidelity to an EBP model.Implementation usually lasts between one and two years, and typically involvesstructural changes, staff skill development, and modification of organizationalprocesses to support the practice. Most programs will need significant on-site con-sultation and training during the first year of implementation. Consultation and
86 Best Practices in Mental Health
Chapter 06_Chapter 06 4/16/13 11:04 AM Page 86

training activities tend to taper off during the second year of implementation, andare often focused on refining staff skills and solidifying supports within the agencyto continue the practice.
On the other hand, sustainability can be interpreted as maintaining an EBP overa long period of time. The sustainability stage occurs after initial consultation/technical assistance has ended or has been greatly curtailed. A program will usu-ally enter a sustainability stage two years after initial start-up or after practicefidelity has been achieved. After the second year, fidelity assessments decrease fromonce every six months to once per year and consultation is truncated. It is at thistime that sustainability begins. Appropriate and effective implementation of anEBP can be time consuming and expensive.
Because social work and other human service arenas often face problems withsustainability that can lead to de-adoption (Massatti et al., 2008), it is importantto identify methods to sustain EBPs that do not require the intensive efforts thatoccur during initial implementation. It is hoped that, through noninvasive assess-ment, the SI will provide specific information that can lead to cost-effective andtargeted interventions that enable EBPs to be sustained.
Conceptual Underpinnings of the Sustainability Index
There are two primary ways in which a program may fail to sustain an EBP:EBP drift and EBP de-adoption. Even when the initial implementation is success-ful, programs have a tendency to drift away from EBP fidelity (e.g., Bond, 1991).Drifting away from model fidelity is not simply discontinuing an EBP; it is a naturalphenomenon that occurs when programs slowly start to change their practiceover time. The reasons for drift can be diverse; examples include cost cutting;changes in policy from local, state, or federal lawmakers; or reverting to previousways of conducting service. Examples of EBPs that have experienced drift and itsassociated reduction in effectiveness include Assertive Community Treatment(ACT) and the Individual Placement and Support (IPS) employment model. Inboth cases, when the program moved away from high fidelity, the model becameless effective (e.g., Bond, 1991; Bond, 2007; Godfrey, 2010; Rosenheck & Mares,2007; Schneider et al., 2009).
Programmatic drift can be assessed by conducting annual fidelity assessmentsof the EBP that has been implemented. Corrective actions can then be taken toensure adherence to high-quality standards. Unfortunately, some organizationsdo not continue conducting fidelity reviews (annually or otherwise) after the ini-tial period of implementation. In addition, most fidelity scales assess for internalprogrammatic structures/skills specific to an EBP rather than for external influ-ences that may result in EBP discontinuance. It is anticipated that the sustainabil-ity index will provide insight into both EBP drift and EBP discontinuation. Itassesses six broad domains: finances, staffing, policies, structure, quality improve-ment, supervision, and staff skills. Table 1 describes some of the underlying con-ceptual underpinnings for the SI.
Brief Report 87
Chapter 06_Chapter 06 4/16/13 11:04 AM Page 87

88 Best Practices in Mental Health
Table 1 Conceptual Underpinnings of the SI and Corresponding Assessment
Item Conceptual underpinning SI assessment
Finances
Staffing
Policies
Structure
Qualityimprovement
Supervision
Staff skills
A primary reason for difficulty in sustaining isinadequate sources of funding.
Adequate staffing is an essential componentof continued EBP maintenance (e.g., Massattiet al., 2008; Wieder & Kruszynski, 2007). Sig-nificant turnover at key agency positions canbe detrimental to an EBP (Aarons, Sommer-feld, Hecht, Silovsky, & Chaffin, 2009).
Several studies have noted the importance ofstate and federal level policies and support,as well as more local cross-system coordina-tion policies in order to achieve adequateimplementation (Isett et al., 2007; Magna-bosco, 2006; Van de Ven & Chu, 2000).Internal policies are also important influenceson EBP maintenance.
Many studies have indicated that ensuringcompatible organizational structures is imper-ative to ensure that a practice is adequatelysustained (Isett et al., 2007; Magnabosco,2006), including mechanisms to keep the EBPon the organizational agenda and having anEBP champion.
There is a wealth of evidence indicating thatcontinued quality improvement through train-ing, consultation/technical assistance, feed-back loops, and fidelity reviews is importantwhen implementing and sustaining an EBP(e.g. Bond, McHugo, Becker, Rapp, & Whitley,2008; Marshall et al., 2008; Marty, Rapp,McHugo, & Whitley, 2008).
There is increasing recognition in the EBP literature of the role of the supervisor inincreasing the ability for practitioners to mas-ter the skills needed within a particular EBP(Becker et al., 2007; Blakely & Dziadosz,2007; Fixsen et al., 2009; Marshall et al.,2008). There is also evidence that, whensupervisors and other leaders systematicallyendorse and support an EBP, it is likely to sus-tain longer (e.g., Solberg et al., 2000).
Even when organizational structures are inplace to support an EBP, the specific skillsassociated with an EBP may still be lacking(e.g., Herschell, Kolko, Baumann, & Davis,2010; Moser, Deluca, Bond, & Rollins, 2004).Additional support needs to be in place toensure that supervisors, frontline staff, andothers in the organization have the skills toimplement the practice (Rapp et al., 2009).
The SI assesses whether there have beenperceived or real financial concerns withinthe past six months and whether theagency can continue to support the EBP.The SI also assesses whether there is confi-dence that the organization will be able tofind resources to continue the EBP in thefuture despite financial constraints.
The SI assesses whether there has beenfrontline staff or supervisory or upper-leveladministration turnover in the past sixmonths.
The SI assesses both internal and externalpolicy changes over the past six months. Inthe case of internal policies, the SI attemptsto determine if conflicting policies exist orhave been newly developed. Any changesin policy that may conflict with servicedelivery through the EBP are assessed.
The SI documents several aspects of organi-zational structure. Any organizational orstructural changes that conflict with the EBPare assessed. The SI also assesses whetherthere are mechanisms in place to keep theEBP on the organizational agenda and wellrooted in the organization’s infrastructure.The SI also determines if there is an EBPchampion on staff with specific responsibil-ity to support the continuation of the EBP.
The SI assesses whether outcomes aretracked, shared, distributed, and discussedwith staff members. The SI also assesseswhether specific actions are taken toimprove client outcomes. Annual fidelityreviews provide a means for tracking anEBP’s quality. The SI assesses whether ornot recommendations from the last fidelityreview have been enacted.
The SI assesses three important supervisorybehaviors that relate to improving practiceskills of an EBP. This includes reviewing EBPtools completed by individual staff, provid-ing field mentoring, and giving staff spe-cific feedback on use of EBP tools andmethods. The SI assesses not only theoccurrence of these behaviors but their fre-quency of occurrence.
The SI assesses what percentage of staffmembers are proficient using EBP skills,tools, and/or methods (based on the EBP’sfidelity criteria). It assesses whether teammembers have received training related tothe EBP over the past six months. It alsoassesses the amount of consultationreceived by the team or supervisors in thepast six months.
Chapter 06_Chapter 06 4/16/13 11:04 AM Page 88

Sustaining Best Practices
Although the SI has not yet been validated, it is currently being piloted at sitesimplementing evidence-based practices and emerging best practices in Kansas. Itwill continue to be revised based on piloting research. The SI is assessed by the EBPconsultant and trainer during regularly scheduled fidelity reviews using informa-tion obtained from organizational leadership, supervisors, frontline staff, and written agency materials. It is considered an additional body of information, alongwith the fidelity review report, for organization leadership to use when makingdecisions related to the EBP.
Conceptually the SI was developed to assess concerns that have already beendiscovered and articulated in the peer-reviewed implementation science literature.It is meant to be nonintrusive and to point to targeted interventions that help towarn of potential drift and/or discontinuation. It can be considered a preventativemeasure that helps create cost-effective plans for maintaining innovative and evidence-based practices to improve the lives of the people social workers serve. Ifthese practices are not sustained, individuals may be harmed when helpful ser-vices are discontinued midstream. Ensuring the continuation of beneficial EBPshelps safeguard continuity of services and the outcomes that individuals bothwant and need.
ReferencesAarons, G. A., Hurlburt, M., & Horwitz, S. M. (2011). Advancing a conceptual
model of evidence-based practice implementation in public service sec-tors. Administrative Policy in Mental Health, 38(1), 4–23.
Aarons, G. A., Sommerfeld, D. H., Hecht, D. B., Silovsky, J. F., & Chaffin, M. J.(2009). The impact of evidence-based practice implementation andfidelity monitoring on staff turnover: Evidence for a protective effect.Journal of Consulting and Clinical Psychology, 77(2), 270–280.
Becker, D. R., Baker, S. R., Carlson, L., Flint, R., Howell, R., Lindsay, S., . . . Drake,R. E. (2007). Critical strategies for implementing supported employment.Journal of Vocational Rehabilitation, 27(1), 13–20.
Bellamy, J. L., Bledsoe, S. E., & Traube, D. E. (2006). The current state of evidence-based practice in social work: A review of the literature and qualitativeanalysis of expert interviews. Journal of Evidence-Based Social Work, 3(1),23–48.
Bjorklund, R. W., Monroe-DeVita, M., Reed, D., Toulon, A., & Morse, G. (2009).Washington State’s initiative to disseminate and implement high-fidelityACT teams. Psychiatric Services, 60(1), 24–27.
Blakely, T. J., & Dziadosz, G. M. (2007). Creating an agency integrated treatmentprogram for co-occurring disorders. American Journal of Psychiatric Reha-bilitation, 10(1), 1–18.
Blasinsky, M., Goldman, H. H., & Unutzer, J. (2006). Project impact: A report onthe barriers and facilitators to sustainability. Administration and Policy inMental Health and Mental Health Services Research, 33(6), 718–729.
Brief Report 89
Chapter 06_Chapter 06 4/16/13 11:04 AM Page 89

Bond, G. R. (1991). Variations in an assertive outreach model. New Directions forMental Health Services, 52, 65–80.
Bond, G. R. (2007). Modest implementation efforts, modest fidelity, and modestoutcomes. Psychiatric Services, 58(3), 334.
Bond, G., Drake, R., McHugo, G., Rapp, C., & Whitley, R. (2009). Strategies forimproving fidelity in the national evidence-based practices project.Research on Social Work Practice, 19(5), 569–581.
Bond, G. R., McHugo, G. J., Becker, D. R., Rapp, C. A., & Whitley, R. (2008).Fidelity of supported employment: Lessons learned from the NationalEvidence-Based Practice Project. Psychiatric Rehabilitation Journal, 31(4),300–305.
Chandler, D. (2009). Implementation of integrated dual disorders treatment ineight California programs. American Journal of Psychiatric Rehabilitation,12(4), 330–351.
Deegan, P. E. (2007). The lived experience of using psychiatric medication in therecovery process and a shared decision-making program to support it.Psychiatric Rehabilitation Journal, 31(1), 62–69.
Drake, R. E., Bond, G. R., & Essock, S. M. (2009). Implementing evidence-basedpractices for people with schizophrenia. Schizophrenia Bulletin, 35(4),704–713.
Drake, R. E., Goldman, H. H., Leff, H. S., Lehman, A. F., Dixon, L., Mueser, K. T., &Torrey, W. C. (2001). Implementing evidence-based practices in routinemental health service settings. Psychiatric Services, 52(2), 179–182.
Farkas, M., Gagne, C., Anthony, W., & Chamberlin, J. (2005). Implementingrecovery oriented evidence based programs: Identifying the criticaldimensions. Community Mental Health Journal, 41(2), 141–158.
Fixsen, D., Blase, K., Naoom, S., & Wallace, F. (2009). Core implementation com-ponents. Research on Social Work Practice, 19(5), 531.
Fixsen, D. L., Naoom, S. F., Blase, K. A., Friedman, R. M., & Wallace, F. (2005).Implementation research: A synthesis of the literature. Tampa, FL: Universityof South Florida, Louis de la Parte Florida Mental Health Institute, theNational Implementation Research Network.
Glisson, C., & Schoenwald, S. (2005). The ARC organizational and communityintervention strategy for implementing evidence-based children’s mentalhealth treatments. Mental Health Services Research, 7(4), 243–259.
Grant, J. G., & Westhues, A. (2010). Choice and outcome in mental health sup-ported housing. Psychiatric Rehabilitation Journal, 33(3), 232–235.
Grimshaw, J., Shirran, L., Thomas, R., Mowatt, G., Fraser, C., Bero, L., . . .O’Brien, M. A. (2001). Changing provider behavior: An overview of systematic reviews of interventions. Medical Care, 39(8), II2–II45.
Godfrey, J. L. (2010). Re-implementing assertive community treatment: One agency’schallenge of meeting state standards (Unpublished doctoral dissertation).Purdue University, Indianapolis, IN.
90 Best Practices in Mental Health
Chapter 06_Chapter 06 4/16/13 11:04 AM Page 90

Gotham, H. J. (2004). Diffusion of mental health and substance abuse treat-ments: Development, dissemination, and implementation. Clinical Psychology: Science and Practice, 11(2), 160–176.
Grol, R., & Grimshaw, J. (1999). Evidence-based implementation of evidence-based medicine. The Joint Commission Journal on Quality Improvement,25(10), 503.
Herschell, A. D., Kolko, D. J., Baumann, B. L., & Davis, A. C. (2010). The role oftherapist training in the implementation of psychosocial treatments: A review and critique with recommendations. Clinical Psychology Review,30(4), 448–466.
Isett, K. R., Burnam, M. A., Coleman-Beattie, B., Hyde, P. S., Morrissey, J. P.,Magnabosco, J., . . . Goldman, H. H. (2007). The state policy context ofimplementation issues for evidence-based practices in mental health.Psychiatric Services, 58(7), 914–921.
Jansen, J., Van Den Bosch, F. A. S., & Volberda, H. W. (2005). Managing potentialand realized absorptive capacity: How do organizational antecedentsmatter? Academy of Management Journal, 48(6), 999–1015.
Magnabosco, J. L. (2006). Innovations in mental health services implementa-tion: A report on state-level data from the U.S. Evidence-Based PracticesProject. Implementation Science, 1(13), 1–13.
Manthey, T. (2011). Using motivational interviewing to increase retention insupported education. American Journal of Psychiatric Rehabilitation, 14(2),120–136.
Manthey, T. J., Rapp, C. A., Carlson, L., Holter, M. C., & Davis, J. K. (2012). Theperceived importance of integrated supported education and employ-ment services. Journal of Rehabilitation, 78(1), 16–24.
Marshall, T., Rapp, C. A., Becker, D. R., & Bond, G. R. (2008). Key factors forimplementing supported employment. Psychiatric Services, 59(8),886–892.
Marty, D., Rapp, C., McHugo, G., & Whitley, R. (2008). Factors influencing consumer outcome monitoring in implementation of evidence-basedpractices: Results from the National EBP Project. Administrative Policy inMental Health, 35(3), 204–211.
Massatti, R. R., Sweeney, H. A., Panzano, P. C., & Roth, D. (2008). The de-adoptionof innovative mental health practices (IMHP): Why organizations choosenot to sustain an IMHP. Administration Policy in Mental Health, 35(1–2),50–65.
McHugh, R. K., & Barlow, D. H. (2010). The dissemination and implementationof evidence-based psychosocial treatments: A review of current efforts.American Psychologist, 65(2), 73–84.
McHugo, G. J., Drake, R. E., Whitley, R., Bond, G. R., Campbell, K., Rapp, C. A., . . .Finnerty, M. T. (2007). Fidelity outcomes in the National Evidence-BasedPractices Project. Psychiatric Services, 58(10), 1279–1284.
Brief Report 91
Chapter 06_Chapter 06 4/16/13 11:04 AM Page 91

McNeese, C. A., & Thyer, B. A. (2008). Evidence-based practice and social work.Journal of Evidence-Based Practice, 1(1), 7–25.
Moser, L. L., Deluca, N. L., Bond, G. R., & Rollins, A. L. (2004). Implementing evidence-based psychosocial practices: Lessons learned from statewideimplementation of two practices. CNS Spectator, 9(12), 926–936, 942.
Mowbray, C. T., Collins, M. E., Bellamy, C. D., Megivern, D. A., Bybee, D., & Szilvagyi, S. (2005). Supported education for adults with psychiatric disabilities: An innovation for social work and psychosocial rehabilitationpractice. Social Work, 50(1), 7–20.
Polio, D. E., North, C. S., & Osborne, V. A. (2002). Family-responsive psycho-education groups for families with a member with mental illness: Pilotresults. Community Mental Health Journal, 38(5), 413–421.
Proctor, E. K., Lansyerk, J., Aarons, G., Chambers, D., Glisson, C., & Mittman, B.(2009). Implementation research in mental health services: An emerg-ing science with conceptual, methodological, and training challenges.Administration and Policy in Mental Health Services Research, 36(1), 24–34.
Rapp, C. A., Etzel-Wise, D., Marty, D., Coffman, M., Carlson, L., Asher, D., . . .Holter, M. (2008). Evidence-based practice implementation strategies:Results of a qualitative study. Community Mental Health Journal, 44(3),213–224.
Rapp, C. A., Etzel-Wise, D., Marty, D., Coffman, M., Carlson, L., Asher, D., . . .Holter, M. (2009). Barriers to evidence-based practice implementation:Results of a qualitative study. Community Mental Health Journal, 46(2),112–118.
Rapp, C. A., & Goscha, R. J. (2011). The strengths model: Case management withpeople with psychiatric disabilities. New York: Oxford University Press.
Rapp, C. A., Goscha, R. J., & Carlson, L. S. (2010). Evidence-based practice imple-mentation in Kansas. Community Mental Health Journal, 46(5), 461–465.
Rosenheck, R. A., & Mares, A. S. (2007). Dissemination of supported employ-ment for homeless veterans with psychiatric and/or addiction disorders:Two-year client outcomes. Psychiatric Services, 58(3), 325–333.
Salyers, M. P., Rollins, A. L., McGuire, A. B., & Gearhart, T. (2009). Barriers andfacilitators in implementing illness management and recovery for con-sumers with severe mental illness: Trainee perspectives. AdministrativePolicy in Mental Health, 36(2), 102–111.
Schneider, J., Slade, J., Secker, J., Rinaldi, M., Boyce, M., Johnson, R., . . . Grove, B.(2009). SESAMI study of employment support for people with severemental health problems: 12-month outcomes. Health and Social Care inthe Community, 17(2), 151–158.
Solberg, L. I., Brekke, M. L., Fazio, C. J., Fowles, J., Jacobsen, D. N., Kottke, T. E., . . .Rolnick, S. J. (2000). Lessons from experienced guideline implementers:Attend to many factors and use multiple strategies. Joint Commission Journal on Quality Improvement, 26(4), 171–188.
92 Best Practices in Mental Health
Chapter 06_Chapter 06 4/16/13 11:04 AM Page 92

Stokes, T. F., & Baer, D. M. (1977). An implicit technology of generalization. Journal of Applied Behavior Analysis, 10(2), 349–367.
Substance Abuse and Mental Health Services Administration. (2002). Using general organizational index for evidence-based practices. Retrieved January2012 from http://www.ncebpcenter.org/pdfs/ACTGOI.pdf.
Torrey, W. C., Drake, R. E., Dixon, L., Burns, B. J., Rush, A. J., Clark, R. E., &Klatzker, D. (2001). Implementing evidence-based practices for personswith severe mental illness. Psychiatric Services, 52(1), 45–50.
Torrey, W. C., Finnerty, M., Evans, A., & Wyzik, P. F. (2003). Strategies for leadingthe implementation of evidence-based practices. Psychiatric Clinics ofNorth America, 26(4), 883–897.
Torrey, W. C., Lynde, D. W., & Gorman, P. (2005). Promoting the implementationof practices that are supported by research: The National ImplementingEvidence-Based Practice Project. Child and Adolescent Psychiatric Clinics ofNorth America, 14(2), 297–306.
Van de Ven, A. H., & Chu, Y. (2000). A psychometric assessment of the Min-nesota innovation survey. In A. H. Van de Ven, H. L. Angle, & M. S. Poole(Eds.), Research on the management of innovation: The Minnesota Studies(pp. 55–103). New York: Oxford University Press.
Wieder, B. L., & Kruszynski, R. (2007). The salience of staffing in IDDT imple-mentation: One agency’s experience. American Journal of Psychiatric Reha-bilitation, 10(2), 103–112.
Wiltsey-Stirman, S. (2010, December 17). Sustainability research: A review of con-ceptualizations, methods, and findings. Paper presented at the DartmouthPRC Research Seminar, Lebanon, NH.
Brief Report 93
Chapter 06_Chapter 06 4/16/13 11:04 AM Page 93
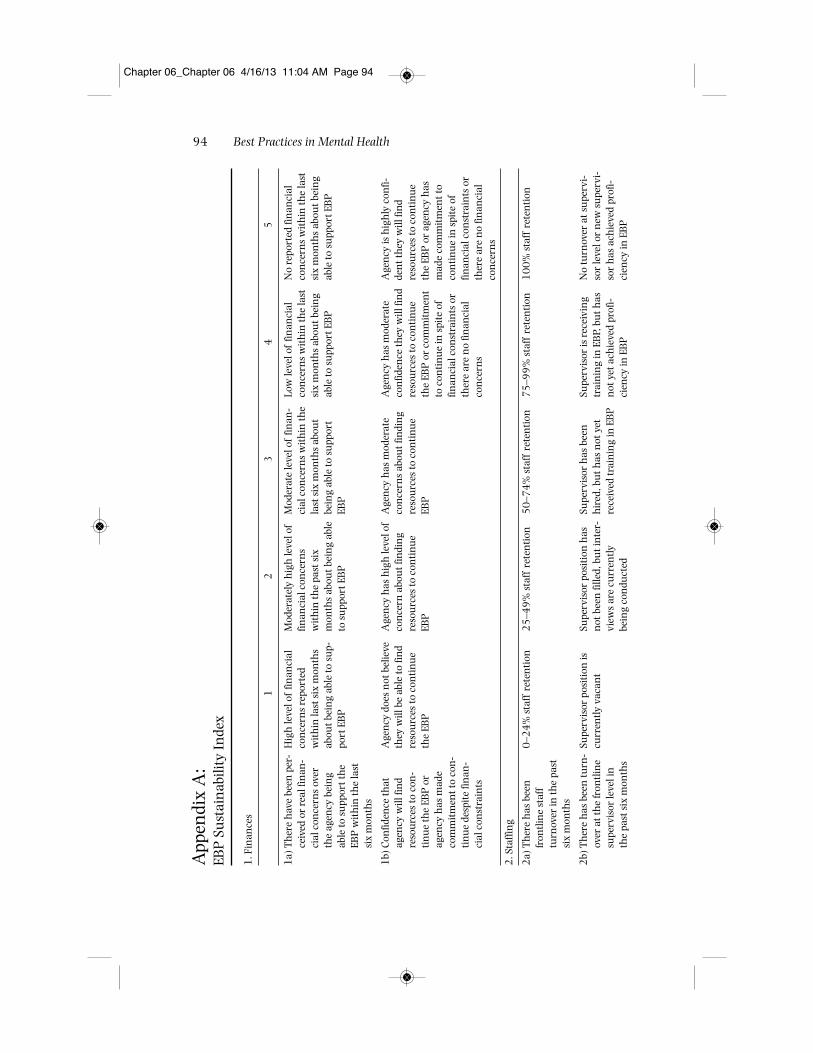
94 Best Practices in Mental Health
App
endi
x A
:EB
P S
ust
ain
abili
ty In
dex
1. F
inan
ces
12
34
5
1a)
Th
ere
hav
e be
en p
er-
ceiv
ed o
r re
al fi
nan
-ci
al c
once
rns
over
the
agen
cy b
ein
gab
le to
su
ppor
t th
eEB
P w
ith
in th
e la
stsi
x m
onth
s
1b)
Con
fiden
ce th
atag
ency
will
fin
dre
sou
rces
to c
on-
tinu
e th
e EB
P o
rag
ency
has
mad
eco
mm
itm
ent t
o co
n-
tinu
e de
spit
e fin
an-
cial
con
stra
ints
2. S
taffi
ng
2a)
Th
ere
has
bee
nfr
ontl
ine
staf
ftu
rnov
er in
the
past
six
mon
ths
2b)
Th
ere
has
bee
n tu
rn-
over
at t
he
fron
tlin
esu
perv
isor
leve
l in
the
past
six
mon
ths
Hig
h le
vel o
f fin
anci
alco
nce
rns
repo
rted
wit
hin
last
six
mon
ths
abou
t bei
ng
able
to s
up-
port
EB
P
Age
ncy
doe
s n
ot b
elie
veth
ey w
ill b
e ab
le to
fin
dre
sou
rces
to c
onti
nue
the
EBP
0–2
4%
sta
ff r
eten
tion
Supe
rvis
or p
osit
ion
iscu
rren
tly v
acan
t
Mod
erat
ely
hig
h le
vel o
ffin
anci
al c
once
rns
wit
hin
the
past
six
mon
ths
abou
t bei
ng
able
to s
upp
ort E
BP
Age
ncy
has
hig
h le
vel o
fco
nce
rn a
bou
t fin
din
gre
sou
rces
to c
onti
nue
EBP
25
–49
% s
taff
ret
enti
on
Supe
rvis
or p
osit
ion
has
not
bee
n fi
lled,
bu
t in
ter-
view
s ar
e cu
rren
tlybe
ing
con
duct
ed
Mod
erat
e le
vel o
f fin
an-
cial
con
cern
s w
ith
in th
ela
st s
ix m
onth
s ab
out
bein
g ab
le to
su
ppor
tEB
P
Age
ncy
has
mod
erat
eco
nce
rns
abou
t fin
din
gre
sou
rces
to c
onti
nue
EBP
50
–74
% s
taff
ret
enti
on
Supe
rvis
or h
as b
een
hir
ed, b
ut h
as n
ot y
etre
ceiv
ed tr
ain
ing
in E
BP
Low
leve
l of
finan
cial
con
cern
s w
ith
in th
e la
stsi
x m
onth
s ab
out b
ein
gab
le to
su
ppor
t EB
P
Age
ncy
has
mod
erat
eco
nfid
ence
they
will
fin
dre
sou
rces
to c
onti
nue
the
EBP
or
com
mit
men
tto
con
tinu
e in
spi
te o
ffin
anci
al c
onst
rain
ts o
rth
ere
are
no
finan
cial
con
cern
s
75
–99
% s
taff
ret
enti
on
Supe
rvis
or is
rec
eivi
ng
trai
nin
g in
EB
P, b
ut h
asn
ot y
et a
chie
ved
prof
i-ci
ency
in E
BP
No
repo
rted
fin
anci
alco
nce
rns
wit
hin
the
last
six
mon
ths
abou
t bei
ng
able
to s
upp
ort E
BP
Age
ncy
is h
igh
ly c
onfi-
den
t th
ey w
ill fi
nd
reso
urc
es to
con
tinu
eth
e EB
P o
r ag
ency
has
mad
e co
mm
itm
ent t
oco
nti
nue
in s
pite
of
finan
cial
con
stra
ints
or
ther
e ar
e n
o fin
anci
alco
nce
rns
10
0%
sta
ff r
eten
tion
No
turn
over
at s
upe
rvi-
sor
leve
l or
new
su
perv
i-so
r h
as a
chie
ved
prof
i-ci
ency
in E
BP
Chapter 06_Chapter 06 4/16/13 11:04 AM Page 94
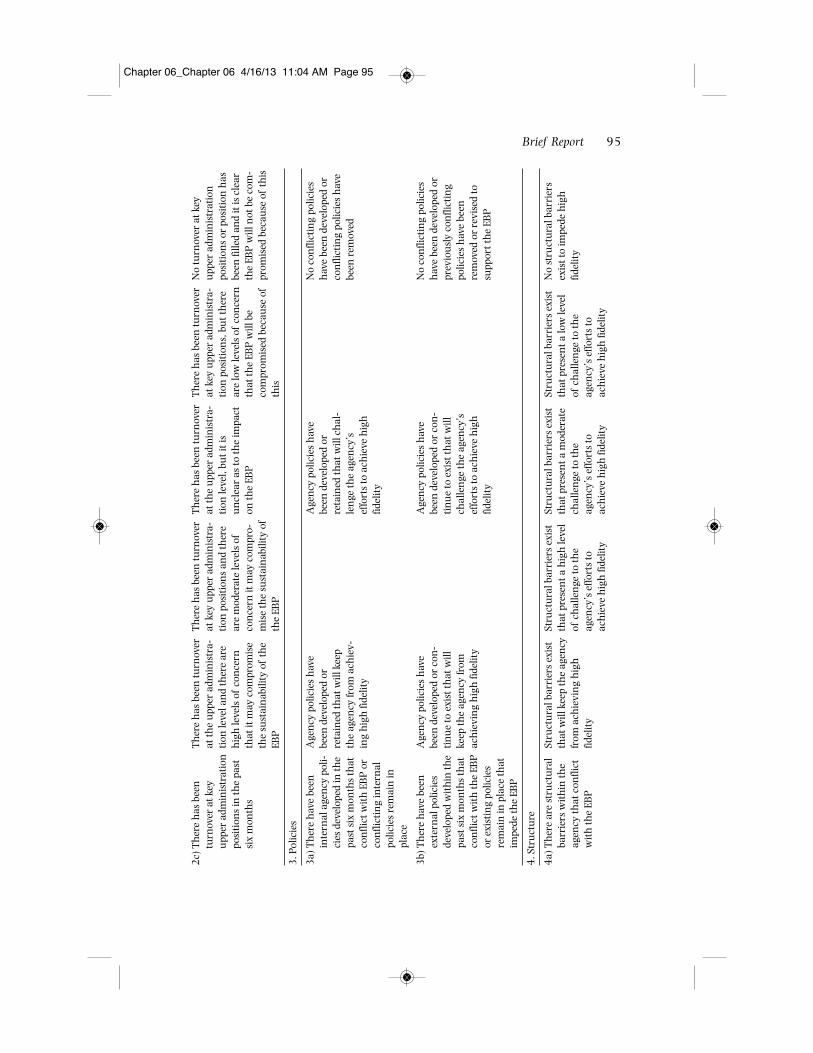
Brief Report 95
2c)
Th
ere
has
bee
ntu
rnov
er a
t key
upp
er a
dmin
istr
atio
npo
siti
ons
in th
e pa
stsi
x m
onth
s
3. P
olic
ies
3a)
Th
ere
hav
e be
enin
tern
al a
gen
cy p
oli-
cies
dev
elop
ed in
the
past
six
mon
ths
that
con
flict
wit
h E
BP
or
con
flict
ing
inte
rnal
polic
ies
rem
ain
inpl
ace
3b)
Th
ere
hav
e be
enex
tern
al p
olic
ies
deve
lope
d w
ith
in th
epa
st s
ix m
onth
s th
atco
nfli
ct w
ith
the
EBP
or e
xist
ing
polic
ies
rem
ain
in p
lace
that
impe
de th
e EB
P
4. S
tru
ctu
re
4a)
Th
ere
are
stru
ctu
ral
barr
iers
wit
hin
the
agen
cy th
at c
onfli
ctw
ith
the
EBP
Th
ere
has
bee
n tu
rnov
erat
the
upp
er a
dmin
istr
a-ti
on le
vel a
nd
ther
e ar
eh
igh
leve
ls o
f co
nce
rnth
at it
may
com
prom
ise
the
sust
ain
abili
ty o
f th
eEB
P
Age
ncy
pol
icie
s h
ave
been
dev
elop
ed o
rre
tain
ed th
at w
ill k
eep
the
agen
cy fr
om a
chie
v-in
g h
igh
fide
lity
Age
ncy
pol
icie
s h
ave
been
dev
elop
ed o
r co
n-
tin
ue
to e
xist
that
will
keep
the
agen
cy fr
omac
hie
vin
g h
igh
fide
lity
Stru
ctu
ral b
arri
ers
exis
tth
at w
ill k
eep
the
agen
cyfr
om a
chie
vin
g h
igh
fidel
ity
Th
ere
has
bee
n tu
rnov
erat
key
upp
er a
dmin
istr
a-ti
on p
osit
ion
s an
d th
ere
are
mod
erat
e le
vels
of
con
cern
it m
ay c
ompr
o-m
ise
the
sust
ain
abili
ty o
fth
e EB
P
Stru
ctu
ral b
arri
ers
exis
tth
at p
rese
nt a
hig
h le
vel
of c
hal
len
ge to
the
agen
cy’s
effo
rts
toac
hie
ve h
igh
fide
lity
Th
ere
has
bee
n tu
rnov
erat
the
upp
er a
dmin
istr
a-ti
on le
vel,
but i
t is
un
clea
r as
to th
e im
pact
on th
e EB
P
Age
ncy
pol
icie
s h
ave
been
dev
elop
ed o
rre
tain
ed th
at w
ill c
hal
-le
nge
the
agen
cy’s
effo
rts
to a
chie
ve h
igh
fidel
ity
Age
ncy
pol
icie
s h
ave
been
dev
elop
ed o
r co
n-
tinu
e to
exi
st th
at w
illch
alle
nge
the
agen
cy’s
effo
rts
to a
chie
ve h
igh
fidel
ity
Stru
ctu
ral b
arri
ers
exis
tth
at p
rese
nt a
mod
erat
ech
alle
nge
to th
eag
ency
’s e
ffort
s to
ach
ieve
hig
h fi
delit
y
Th
ere
has
bee
n tu
rnov
erat
key
upp
er a
dmin
istr
a-ti
on p
osit
ion
s, b
ut t
her
ear
e lo
w le
vels
of
con
cern
that
the
EBP
will
be
com
prom
ised
bec
ause
of
this
Stru
ctu
ral b
arri
ers
exis
tth
at p
rese
nt a
low
leve
lof
ch
alle
nge
to th
eag
ency
’s e
ffort
s to
ach
ieve
hig
h fi
delit
y
No
turn
over
at k
eyu
pper
adm
inis
trat
ion
posi
tion
s or
pos
itio
n h
asbe
en fi
lled
and
it is
cle
arth
e EB
P w
ill n
ot b
e co
m-
prom
ised
bec
ause
of
this
No
con
flict
ing
polic
ies
hav
e be
en d
evel
oped
or
con
flict
ing
polic
ies
hav
ebe
en r
emov
ed
No
con
flict
ing
polic
ies
hav
e be
en d
evel
oped
or
prev
iou
sly
con
flict
ing
polic
ies
hav
e be
enre
mov
ed o
r re
vise
d to
supp
ort t
he
EBP
No
stru
ctu
ral b
arri
ers
exis
t to
impe
de h
igh
fidel
ity
Chapter 06_Chapter 06 4/16/13 11:04 AM Page 95

96 Best Practices in Mental Health
App
endi
x A
—(C
onti
nued
)
12
34
5
4b)
Mec
han
ism
in p
lace
to k
eep
EBP
on
the
orga
niz
atio
nal
agen
da
4c)
Pre
sen
ce o
f EB
Pch
ampi
on w
ith
spe
-ci
fic fu
nct
ion
s to
supp
ort c
onti
nu
a-ti
on o
f EB
P
5. Q
ual
ity
Impr
ovem
ent
5a)
Rec
omm
enda
tion
sfr
om la
st fi
delit
yre
view
that
hav
ebe
en e
nac
ted
5b)
Fre
quen
cy th
at s
pe-
cific
act
ion
s ar
eta
ken
to im
prov
ecl
ien
t ou
tcom
es fr
omre
view
ing
data
wit
hst
aff
6. S
upe
rvis
or
6a)
Fre
quen
cy th
atsu
perv
isor
rev
iew
sto
ols
wit
h s
taff
No
stra
tegi
es e
xist
toke
ep E
BP
on
org
aniz
a-ti
onal
age
nda
No
EBP
ch
ampi
on
pres
ent
Non
e of
the
reco
mm
en-
dati
ons
hav
e be
enen
acte
d
Nev
er
Supe
rvis
or s
pen
ds le
ssth
an 3
0 m
inu
tes
per
wee
k re
view
ing
EBP
tool
s
At l
east
on
e st
rate
gy is
in p
lace
to k
eep
EBP
on
orga
niz
atio
nal
age
nda
EBP
ch
ampi
on p
rese
nt,
but w
ith
no
pow
er to
influ
ence
dec
isio
ns
mad
ere
late
d to
EB
P s
ust
ain
-ab
ility
A fe
w o
f th
e re
com
men
-da
tion
s h
ave
been
enac
ted,
bu
t cri
tica
l rec
-om
men
dati
ons
hav
e n
otye
t bee
n a
ddre
ssed
Supe
rvis
or s
pen
ds3
0–5
9 m
inu
tes
per
wee
kre
view
ing
EBP
tool
s
At l
east
two
stra
tegi
esar
e in
pla
ce to
kee
p EB
Pon
org
aniz
atio
nal
agen
da
EBP
ch
ampi
on p
rese
nt,
but o
nly
indi
rect
influ
-en
ce o
n d
ecis
ion
s m
ade
rela
ted
to E
BP
su
stai
n-
abili
ty
Mos
t of
the
reco
mm
en-
dati
ons
hav
e be
enen
acte
d w
ith
dis
cuss
ion
occu
rrin
g on
the
oth
ers
Act
ion
s ar
e ta
ken
occ
a-si
onal
ly, b
ut n
ot in
any
syst
emat
ic m
ann
er
Supe
rvis
or s
pen
ds6
0–8
9 m
inu
tes
per
wee
kre
view
ing
EBP
tool
s
At l
east
thre
e st
rate
gies
are
in p
lace
to k
eep
EBP
on o
rgan
izat
ion
alag
enda
EBP
ch
ampi
on p
rese
nt
wit
h m
oder
ate
pow
er to
influ
ence
key
dec
isio
ns
rela
ted
to E
BP
su
stai
n-
abili
ty
Mos
t rec
omm
enda
tion
sh
ave
been
en
acte
d or
asp
ecifi
c pl
an is
in p
lace
to e
nac
t th
ose
that
hav
en
ot
Supe
rvis
or s
pen
ds9
0–1
19
min
ute
s pe
rw
eek
revi
ewin
g EB
Pto
ols
Fou
r or
mor
e st
rate
gies
are
in p
lace
to k
eep
EBP
on o
rgan
izat
ion
alag
enda
EBP
ch
ampi
on p
rese
nt
wit
h s
ubs
tan
tial
pow
erto
influ
ence
key
dec
i-si
ons
rela
ted
to E
BP
su
stai
nab
ility
All
reco
mm
enda
tion
sh
ave
been
en
acte
d
At l
east
qu
arte
rly
Supe
rvis
or s
pen
ds a
tle
ast t
wo
hou
rs p
er w
eek
revi
ewin
g EB
P to
ols
Chapter 06_Chapter 06 4/16/13 11:04 AM Page 96
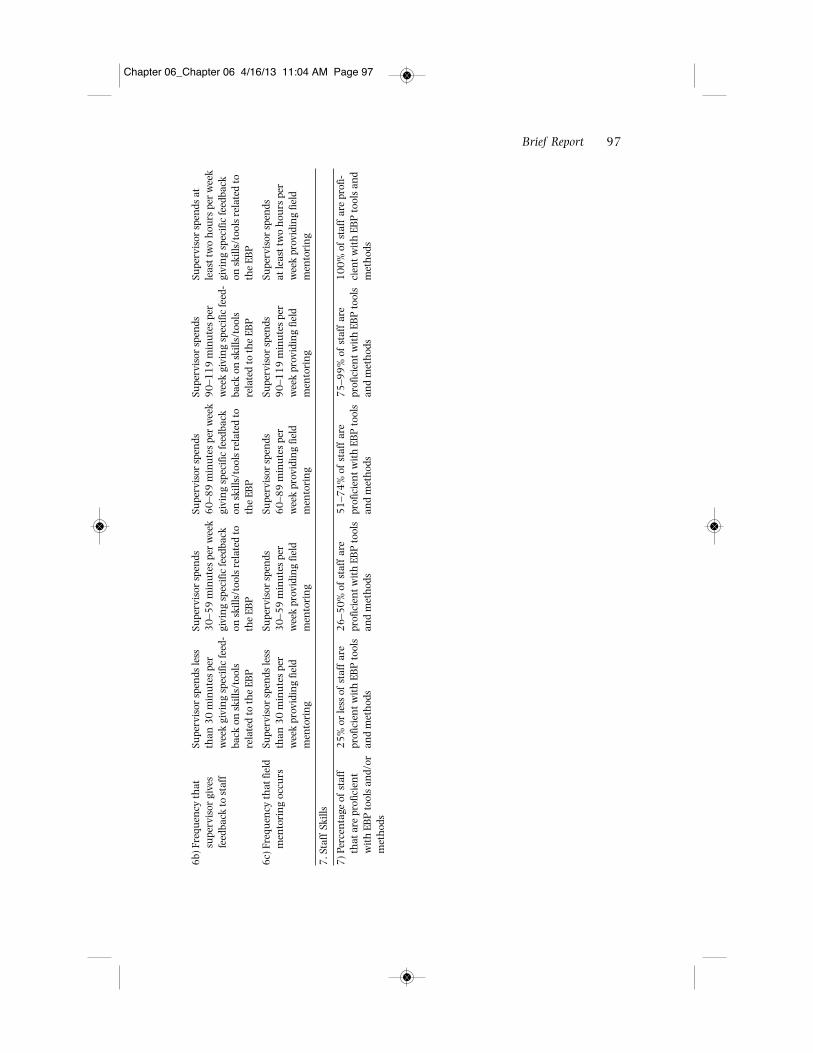
Brief Report 97
6b)
Fre
quen
cy th
atsu
perv
isor
giv
esfe
edba
ck to
sta
ff
6c)
Fre
quen
cy th
at fi
eld
men
tori
ng
occu
rs
7. S
taff
Ski
lls
7) P
erce
nta
ge o
f st
aff
that
are
pro
ficie
nt
wit
h E
BP
tool
s an
d/or
met
hod
s
Supe
rvis
or s
pen
ds le
ssth
an 3
0 m
inu
tes
per
wee
k gi
vin
g sp
ecifi
c fe
ed-
back
on
ski
lls/t
ools
rela
ted
to th
e EB
P
Supe
rvis
or s
pen
ds le
ssth
an 3
0 m
inu
tes
per
wee
k pr
ovid
ing
field
men
tori
ng
25
% o
r le
ss o
f st
aff
are
prof
icie
nt w
ith
EB
P to
ols
and
met
hod
s
Supe
rvis
or s
pen
ds3
0–5
9 m
inu
tes
per
wee
kgi
vin
g sp
ecifi
c fe
edba
ckon
ski
lls/t
ools
rel
ated
toth
e EB
P
Supe
rvis
or s
pen
ds3
0–5
9 m
inu
tes
per
wee
k pr
ovid
ing
field
men
tori
ng
26
–50
% o
f st
aff
are
prof
icie
nt w
ith
EB
P to
ols
and
met
hod
s
Supe
rvis
or s
pen
ds6
0–8
9 m
inu
tes
per
wee
kgi
vin
g sp
ecifi
c fe
edba
ckon
ski
lls/t
ools
rel
ated
toth
e EB
P
Supe
rvis
or s
pen
ds6
0–8
9 m
inu
tes
per
wee
k pr
ovid
ing
field
men
tori
ng
51
–74
% o
f st
aff
are
prof
icie
nt w
ith
EB
P to
ols
and
met
hod
s
Supe
rvis
or s
pen
ds9
0–1
19
min
ute
s pe
rw
eek
givi
ng
spec
ific
feed
-ba
ck o
n s
kills
/too
lsre
late
d to
the
EBP
Supe
rvis
or s
pen
ds9
0–1
19
min
ute
s pe
rw
eek
prov
idin
g fie
ldm
ento
rin
g
75
–99
% o
f st
aff
are
prof
icie
nt w
ith
EB
P to
ols
and
met
hod
s
Supe
rvis
or s
pen
ds a
tle
ast t
wo
hou
rs p
er w
eek
givi
ng
spec
ific
feed
back
on s
kills
/too
ls r
elat
ed to
the
EBP
Supe
rvis
or s
pen
ds
at le
ast t
wo
hou
rs p
erw
eek
prov
idin
g fie
ldm
ento
rin
g
10
0%
of
staf
f ar
e pr
ofi-
cien
t wit
h E
BP
tool
s an
dm
eth
ods
Chapter 06_Chapter 06 4/16/13 11:04 AM Page 97
Chapter 06_Chapter 06 4/16/13 11:04 AM Page 98
The profession of social work has codified the use of research-informed or evidence-based practice as both a basic educational competency and an expectation of ethicalpractice. Although there is debate as to what constitutes evidence, manualized treat-ments that have undergone rigorous empirical scrutiny are considered by many to bethe gold standard for evidence-based or empirically supported treatment (EST). Dissem-inating ESTs into the real world requires that clinicians learn and use the treatmentmanual. Although the challenges of implementing ESTs across systems or agencies arewell documented, little is known about the experiences of individual clinicians whoattempt to learn and implement a manualized treatment in a community mental healthsetting. The purpose of this article is to discuss one clinician’s experience using a treat-ment manual, to identify benefits and challenges, and to provide recommendations topractitioners and treatment development researchers about developing and using treat-ment manuals in the real world.
Key words: adolescent; community mental health; evidence-based practice; fam-ily therapy; treatment manual
The profession of social work has codified the use of research-informed/evidence-based practice as both a basic educational competency (Council on Social WorkEducation, 2008) and an expectation of ethical practice (National Association ofSocial Workers, 2008). Although there is debate as to what constitutes evidence(see Drisko & Grady, 2012) and what factors contribute to the best client out-comes (cf. Addis & Cardemil, 2005; Duncan & Miller. 2005), treatments that havebeen validated in well-controlled studies in which participants are randomlyassigned to different treatment conditions have long been considered the gold
Case Study:
When Bambi Meets Godzilla: A Practitioner’sExperience Adopting and Implementing aManualized Treatment in a Community Mental Health Setting
Jonathan B. Singer and Catherine M. Greeno
Jonathan B. Singer, PhD, LCSW, is assistant professor, School of Social Work, Temple University,Philadelphia. Catherine M. Greeno, PhD, is associate professor, School of Social Work, Universityof Pittsburgh, Pittsburgh, PA.
© 2013 Lyceum Books, Inc., Best Practices in Mental Health, Vol. 9, No. 1, March 2013
Chapter 07_Chapter 07 4/16/13 11:05 AM Page 99

standard for clinical practice. These treatments are referred to as empirically sup-ported treatments (ESTs), evidence-based therapies (EBTs), empirically validatedtherapies (EVTs), or less precisely, evidence-based practices (EBPs).
In order for an intervention to be empirically tested, the developers must spec-ify the conceptual, procedural, and structural boundaries of a treatment (i.e.,what is being done and why it is being done; Addis & Cardemil, 2005; Henggeler& Schoenwald, 2002). This information is contained in a treatment manual. Thetreatment manual has been a basic component of psychotherapy research sincethe 1960s (Duncan, Nicol, & Ager, 2004). Since the 1990s, it has been either cel-ebrated as a tool for disseminating ESTs and improving clinical practice or vilifiedas imposing an impersonal and impractical treatment that does not reflect real-world problems (Godley, White, Diamond, Passetti, & Titus, 2001). Althoughtreatment manuals are only one component of an EST, the most common form of learning about and becoming trained in ESTs is by reading these manuals (Herschell, Kolko, Baumann, Abigail, & Davis, 2010).
The challenges of widespread implementation of manualized treatments arewell documented (Chorpita, Becker, & Daleiden, 2007; Godley et al., 2001; LeCroy,2008). Some of the challenges are philosophical, such as clinician distrust of treat-ments developed in the lab, or beliefs that client outcomes have less to do with spe-cific interventions and more to do with therapist effects and the therapeutic rela-tionship. Other challenges are pragmatic, such as the quality and detail of thedissemination plan, time required to be certified in an EST, and cost effectiveness ofimplementing an EST compared to that of continuing to provide treatment-as-usual. Even when those barriers have been overcome, implementation challengesarise at every level of the service delivery system:
Variables influencing treatment fidelity, including the quality of the treatmentmanual, can be conceptualized from a social ecological framework. Practi-tioners are embedded in quality assurance systems (e.g., manuals, supervi-sion), which are embedded within organizations, which are embedded withincommunity contexts. Variables at each level of analysis influence practitionerbehavior and, in many cases, can undermine the intents of the best conceivedtreatment manual. (Henggeler & Schoenwald, 2002, p. 419)
The Institute of Medicine (2001) estimated that, once a treatment has an evidence base, it takes seventeen years for the intervention to make its way intoclinical practice. Recognizing the need to reduce the time and increase the num-ber of mental health providers trained in ESTs, public health authorities haverecently allocated over $2 billion dollars to improve dissemination efforts and todevelop best practices for disseminating ESTs (see McHugh & Barlow, 2010, for areview).
Therapist Experiences Using Treatment Manuals
Although the challenges of deploying an EST system-wide are daunting, thechallenges faced by a sole practitioner attempting to use a treatment manual in a
100 Best Practices in Mental Health
Chapter 07_Chapter 07 4/16/13 11:05 AM Page 100

community mental health setting may be greater. If a practitioner follows profes-sional standards (Council on Social Work Education, 2008; National Associationof Social Workers, 2008) and, through a process of determining the best inter-vention for the client (e.g., Parrish & Rubin, 2011), decides that the best treatmentis an EST, he or she will be faced with a number of questions (Chorpita et al.,2007):
• Can the manual be accessed, and if so, are there financial or other barriers toobtaining it? Northey and Hodgson (2008) reported that the costs of imple-menting manualized treatment for couples or families ranged from approxi-mately $1,000 for Emotion-Focused Couple Therapy to $30,000 for multi-systemic therapy (MST). If an agency is able to implement MST for $30,000and save $100,000 on more intensive services, then it is good value for themoney. For the independent practitioner, however, purchasing a $40 to $60treatment manual is an easy and affordable way of becoming familiar with atreatment.
• Will knowledge, skills, time, and agency support be available to implementthe EST? If, for example, the clinician finds that Dialectical Behavior Therapy(DBT) offers the most empirical support for a self-harming client who has adiagnosis of borderline personality disorder, he or she will soon find that DBTis actually a multicomponent treatment that assumes an integrated systemof care among a team of providers. Alternately, if a clinician is in an out-patient setting, and a manual has been developed for group therapy in aninpatient or partial hospitalization program, there may be challenges inestablishing groups, finding space, or overcoming other structural factorsthat would complicate the implementation of the manual.
• Even if the practitioner is able to find a manual intended for the client andagency setting, how will he or she determine whether the client’s outcomesresult from the treatment prescribed in the manual or from other factors?Even in the most rigorous randomized clinical trial in which therapists aretrained to fidelity and receive regular supervision, not all clients improve.Furthermore, there are those who argue that treatment outcomes have moreto do with nonspecific or common factors than with the techniques and pro-cedure included in the treatment manual (Duncan & Miller, 2005).
In addition to the practical challenges of finding and implementing a treatmentmanual, the clinician will discover that very little has been written by practition-ers with regard to their experience in implementing a manual-based treatment(Stegall & Nangle, 2005). Although there is a large body of literature that dis-cusses dissemination of ESTs, only one study has evaluated clinicians’ experiencesin implementing such a treatment (Godley et al., 2001).
Godley et al. (2001) examined interviews with nineteen therapists and casemanagers who used manualized approaches to treatment of cannabis abuse dur-ing a large randomized field experiment. The authors concluded that nearly all ofthese therapists and case managers had positive experiences with the treatment
Case Study 101
Chapter 07_Chapter 07 4/16/13 11:05 AM Page 101

manuals. They reported that manuals were easy to use, provided useful structure,helped the clinician to focus treatment, and allowed for creativity and flexibility.Challenges to working with the manualized treatment include managing behav-ioral problems not addressed in the manuals, adapting complex or inappropriatelyadvanced material, establishing guidelines for working with parents even whenthey are not included in the manual, and maintaining children’s focus whenteaching specific skills. The clinicians discussed the importance of clinical super-vision in implementing the manual-guided treatments. The authors concludedthat, despite clinicians’ positive experience with the treatment, clinician feedbackis essential in improving the value and utility of the treatment manual.
To contribute to the knowledge base about implementing manualized treat-ments, this article will describe the experience of a clinical social worker attempt-ing to implement Problem-Solving Communication Training (PSCT; Robin, Bedway,& Gilroy, 1994) in a community mental health agency. This article is neither a clin-ical case study, which seeks to provide an exemplar for treating a problem, nor anevaluation of a specific treatment, which seeks to demonstrate the effectiveness ofone approach relative to another. This article is more similar to autoethnography(Sparkes, 2000), in that it provides a context—the specifics of the case and thefocus of the treatment—in order to focus on the first author’s (JBS’s) experienceusing a treatment manual in a community setting. By critically evaluating thisexperience, the authors hope to help clinicians make more informed decisionsabout whether to obtain and use treatment manuals and to help treatment devel-opment researchers produce manuals that are more user friendly.
Intervention
Summary of Problem-Solving Communication Training
Problem-Solving Communication Training was one of ten treatment manualsincluded in LeCroy’s (1994) Handbook of Child and Adolescent Treatment Manuals.The treatment manual provided a theoretical overview, defined key terms, andrecommended training procedures (including supervision). Robin, Bedway, andGilroy (1994) described PSCT as a highly directive, twelve-session, behavioralfamily systems intervention intended to resolve parent-adolescent conflict. Thetreatment manual focused on teaching problem-solving skills, improving commu-nication skills, and addressing cognitive distortions.
Problem-Solving Communication Training is a four-phase treatment: engage-ment (sessions 1 through 3), skill building (sessions 4 through 7), conflict resolu-tion (sessions 8 through 10), and termination (sessions 11 and 12). For each ses-sion, the authors specified the goals, provided details about how to achieve thegoals, included sample dialogue and suggested wording for introducing conceptsor topics, recommended or included goal-specific measures or homework, andgave instructions on how to end the session. Additionally, the authors provided acontext for using the treatment manual. They advised the reader that not all fam-ilies would need all of the modules included in the manual, and that the manual
102 Best Practices in Mental Health
Chapter 07_Chapter 07 4/16/13 11:05 AM Page 102

could not cover every variation of parent-adolescent conflict. They also specifiedthat the manual was intended for trained clinicians who were familiar with fam-ily systems work. Consistent with these requirements, the clinician who imple-mented PSCT is a licensed clinical social worker who has extensive experienceworking with families. As a bonus, he taught the PSCT treatment manual dis-cussed in this article in a master’s-level clinical social work practice course.
The following is a brief summary of the presenting problem and description ofthe treatment, identifying the session goals and what worked and did not work,followed by a discussion of the clinician’s experience in each session. The casestudy concludes with detailed recommendations for clinicians, treatment develop-ment researchers, and educators. The personal pronoun I has been used through-out the case study to indicate that only one author (JBS) delivered the treatment.
Presenting Problem
Ms. D. self-referred to the agency to request services for herself and her fourteen-year-old son Craig. During the intake phone call, Ms. D described her family life as “one big argument.” She reported feeling very stressed, noting that she was asingle parent, held two part-time minimum-wage jobs, and was responsible fortaking care of her ailing mother. She stated that she blamed herself for her son’sproblems: “If I could spend more time with him he wouldn’t be so angry.” Ms. Ddescribed her son as bright and a good student. He had few friends and partici-pated in no extracurricular activities, “unless you think of video games asextracurricular.” She stated that he had no psychiatric diagnoses, was not on med-ications, and had no known medical problems. She reported that Craig refused tocomply with parental requests. She stated, “He tells me what to do—it is almostlike he wants to be the one in charge.”
Decision to Use the PSCT Treatment Manual
Ms. D described parent-child conflict and problems with the family structure(i.e., son taking on an executive role). I was familiar with PSCT because I hadtaught it in a graduate-level clinical practice social work course as a way ofdemonstrating problem-solving skills and providing students with an example ofa treatment manual. The problems that the mother described were consistent withthe treatment manual. I was eager to apply an empirically supported treatmentand put into practice something that I had used with my students.
Overview of Treatment
I met with the family for a total of thirteen sessions. The first five sessionsaddressed the material in the treatment manual and resulted in some reduction inconflict and some improvement in problem-solving skills. Between the fifth andsixth session, Ms. D’s mother died. The focus of treatment shifted to individualbereavement counseling for Ms. D for the six weeks following her mother’s death.We ended services with two family sessions.
Case Study 103
Chapter 07_Chapter 07 4/16/13 11:05 AM Page 103

Implementing the Treatment Manual in the Real World
Phase I. Engagement, Session 1: Build Rapport
PSCT goals. PSCT goals for this session are to establish rapport with the family;identify deficits in problem-solving skills, cognitive distortions, and family struc-ture problems; establish a shared view of the family problem; and motivate thefamily to participate in treatment. Materials needed are the Review of NegativeCommunication handout and the Unreasonable Beliefs handout (included in themanual), as well as a self-report questionnaire for homework (not included in themanual).
What worked. The treatment manual provided helpful sample dialogue todemonstrate what a model discussion about problem-solving skills looked like, andgave questions to assess for deficits in communication skills. Because the manualhad a specific theoretical foundation, including questions that were theoreticallyconsistent was very helpful. The family had difficulty identifying skill deficits, andthe manual helped to navigate the clinical waters.
What did not work. The biggest challenges in session 1 were maintaining rap-port while trying to follow the details of the manual, adopting the expert tone, andusing the required handouts.
The need to follow the manual made it hard to establish rapport with the fam-ily. The manual provided a specific order for addressing issues and specific lan-guage with which to describe the process to the family. Although I had taught thistreatment manual in clinical practice elective, I was not familiar enough with it toconduct the session without referring to the text. This had the paradoxical effectof interfering with the first goal: to establish rapport with the family.
Taking the expert role was counter to my training as a solution-focused thera-pist. Throughout the treatment, I was expected to define problems, have the fam-ily choose from preselected options, and frame both the problem (deficits in com-munication skills and distorted cognitions) and the solution. In order to be faithfulto the model, I found myself questioning my clinical choices and fighting againstthe tone and direction of the manual.
Handouts were difficult to use. Neither handout was included in session 1;instead, they were located in sessions 5 and 8, respectively. The handouts were notintended to be stand-alone, ready-to-use documents. In order for the handouts to beuseful, I could either retype them or try to enlarge them on the copy machine; nei-ther was a practical option given my time constraints and unreliable copy machine.The third handout, the homework assignment, was not included in the manual.
Phase I. Engagement, Session 2: Individual/Family Assessment
PSCT goals. Goals for this session are to establish rapport with the adolescent,assess psychopathology and cognitive functioning, obtain a developmental history,and assess marital interaction and family impact of adolescent-parent conflict.
104 Best Practices in Mental Health
Chapter 07_Chapter 07 4/16/13 11:05 AM Page 104

What worked. The treatment manual provided an outline of topics to includein the adolescent and adult interview and gave examples of rapport-building state-ments. Because the content was not prescriptive, I was able to use my existing clin-ical skills to establish rapport with the adolescent and parent.
What did not work. The biggest challenges in session 2 were assessing for psy-chopathology and cognitive functioning, having individual sessions with the childand parent, and collecting self-report measures from session 1.
Although one of the goals of the session was assessing for psychopathologyand cognitive functioning, the manual stated that “a detailed discussion of suchassessment goes beyond this manual. Consult Mash and Terdal (1988)” (p. 100).The expectation that I would have the time or resources to access this book wasunreasonable. The manual did not clarify whether the treatment should be modi-fied if clients present with deficits in cognitive functioning or psychopathology.
The individual session with Ms. D conflicted with two agency policies:
1. I could not have an individual session with Ms. D because agency policy pro-hibited children from being left alone in the waiting room.
2. We agreed to have the session over the phone, which violated agency policybecause I could not bill for therapy by phone.
The treatment manual advised that, if the parent/child did not complete the self-report measures in between sessions, he or she should complete them while sittingin the waiting room. However, because the self-report measure was not includedin the manual, and because the child was not allowed to be in the waiting roomalone, I never collected this information. This omission proved to be problematic inlater sessions.
Phase I. Engagement, Session 3: Contracting and Preparation for Change
PSCT goals. Goals for this session are to establish treatment goals, determinethe extent to which the family needs training in each component, and inform thefamily of the therapist’s conceptualization of their problems. Materials neededconsist of the Agreement for Action (AfA) form (included in the manual).
What worked. The AfA specified the targets of treatment. In theory, this madeit easier to maintain treatment fidelity.
What did not work. The biggest challenges in session 3 were using the AfAand taking an expert stance with the family. There were three problems with theAfA:
1. It was not formatted for copying. The hour I spent retyping the form helpedme to become familiar with it, but was time that could have been spentcatching up on paperwork or having a billable session.
Case Study 105
Chapter 07_Chapter 07 4/16/13 11:05 AM Page 105
2. The AfA was a one-size-fits-all list of problems that served as the PSCTtreatment plan. I could not use it as a treatment plan, however, because ouragency required personalized treatment plans that include information noton the AfA.
3. The family disliked the AfA because some of the action steps did not applyto them.
In part because of my solution-focused training, I was uncomfortable framing theproblem for the family and telling them what to do differently. It is likely that thefamily’s distrust of the AfA was in part a reflection of my own discomfort.
Phase II. Skill Building, Session 4: Problem-Solving Training
PSCT goals. Goals for this session are to present and teach problem solving,teach the family to use a problem-solving worksheet, and give the family a suc-cessful experience resolving a meaningful disagreement. Materials are limited tothe problem-solving worksheet (included).
What worked. The child and parent responded well to the structure of theproblem-solving model. I was familiar with problem solving, so the content in themanual was value-added to my existing skills. The worksheet was appropriate forcopying.
What did not work. The problem-solving session was supposed to revolvearound an issue that the family identified on the session 1 Issues Checklist.Because I never assigned it, we spent ten minutes figuring out which issue we weregoing to talk about. This limited the amount of time we had to problem solve. Thefamily was compliant, but the problem solving seemed sterile and academic. I wasconcerned that there was something else going on that we were not talking about,but did not feel comfortable deviating from the manual.
Phase II. Skill Building, Session 5: Communication Training
PSCT goals. The goals for this session are to increase family members’ aware-ness of their negative communication habits and their effect on the parent-childrelationship, identify the most important negative communication habit, teachpositive communication, and assign positive communication homework. Materi-als needed consisted of the Negative Communication handout (provided).
What worked. The manual included a handout suitable for copying. The fam-ily was very engaged with the content. They found the discussion of their nega-tive communication to be very entertaining. I had a great deal of experienceaddressing problematic communication, so I was very comfortable with the clin-ical territory.
106 Best Practices in Mental Health
Chapter 07_Chapter 07 4/16/13 11:05 AM Page 106

What did not work. In this session, there was nothing that did not work. Wewere able to address all of the content in the session, and it was favorably receivedby the family. I finally felt that I had found my groove with the treatment manualand the family was responding appropriately.
Intrusions of the Real World into the Manualized Treatment
Sessions 6 through 12Between sessions 5 and 6, Ms. D’s mother died. After the funeral, Ms. D
reported that her son had been rude and disrespectful. She reported feeling angryand frustrated with his behavior and her lack of control as a parent, as well asoverwhelming sadness. To their credit, the authors of PSCT provided instructionon how clinicians could address crises. They defined crisis as a breakdown in com-munication skills, failure to implement an agreed-upon solution, or a situation inwhich emotions were running high.
This intrusion of the real world seemed to be a perfect opportunity to apply thePSCT intervention, especially because Ms. D was finally willing to hold her sonaccountable for his actions. However, it quickly became apparent that teachingproblem-solving skills was far less important than recognizing Ms. D’s need to process the loss of her mother. Therefore the focus of treatment changed fromparent-child conflict to bereavement. After six weeks of individual treatment, Ms.D started working with a grief and loss counselor. Although I was willing to continue to work with the family, they were no longer interested in services. Theparent-child conflict that had been the focus of treatment had disappeared. Con-sequently, the PSCT intervention was no longer appropriate.
Session 13. Termination
PSCT goals. The goals for this session are to review treatment goals andprogress and prepare the family for continued application of skills.
What worked. The termination plan described in the manual was very similarto my usual termination session. Ms. D and Craig shared a laugh when wereviewed their conflicts from the beginning of services. Although they were nowfew and far between, the changes appeared to be more a function of shifting fam-ily dynamics than the skills we addressed in the PSCT intervention.
What did not work. The manual recommends spacing sessions two to threeweeks apart. Although the family was willing to do this, the agency’s requirementthat I fill all available slots with clients meant that I could not leave a two-week gapbetween termination sessions.
Best Practice with Manualized Interventions
One of the most basic questions that drive practitioners and interventionresearchers is how clinicians can best help their clients. A compelling answer is to
Case Study 107
Chapter 07_Chapter 07 4/16/13 11:05 AM Page 107

implement ESTs, which are grounded in theory; have well-defined targets of treat-ment; have withstood scrutiny from clients, clinicians, the developer, and otherresearchers; and have demonstrated efficacy in reducing symptoms and improvingfunctioning. Some have argued that it is unethical not to deliver an EST if oneexists that matches a client’s presenting problem(s) (Myers & Thyer, 1997). How-ever, for the clinician whose experience was described in this article, the anticipatedbenefit of the EST was outweighed by the numerous challenges he faced in imple-menting the treatment manual, including incompatibility with agency structureand billing requirements, unreasonable expectations of the clinician’s knowledgeand skills, and incomplete documentation. Although some of the agency-levelchallenges would certainly be addressed in a system-wide adoption of an EST(McHugh & Barlow, 2010), for independent clinicians, these challenges make suc-cessful implementation of a treatment manual in a community setting unrealistic.
Benefits of Using the Treatment Manual
If independent clinicians are not likely to deliver manualized treatments tofidelity, is there a benefit to using a treatment manual in the community? LeCroy(2008) argues that clinicians should have the access and opportunity to use treat-ment manuals because, unlike research articles that report on the treatment thathas been found to be more effective, treatment manuals actually describe what thetreatment looks like and how to deliver it. This information increases the likelihoodthat clinicians will be able to deliver well-conceptualized and effective treatmentsto clients who present with a variety of issues (LeCroy, 2008). Consistent withLeCroy and the findings by Godley et al. (2001), the treatment manual providedthe clinician with a useful structure, helped to focus his treatment, and helped himto learn new treatment techniques. As a community clinician responsible for treat-ing clients who presented with a variety of psychosocial problems, many of whombounced from crisis to crisis, the clinician was accustomed to taking an eclecticapproach that revolved around putting out fires. Although the structure of themanual was challenging, it provided a welcome stability and focus to treatment.The PSCT manual provided a theoretically grounded framework for conceptualiz-ing problems, and helped the clinician to think about what his treatment wouldlook like over the course of many weeks, rather than just one at a time. Because hewanted to provide the best services for his clients, following the manual providedreassurance that he was doing right by them. The inclusion of dialogue and exam-ples to demonstrate the process of teaching communication skills helped him tolearn a technique that was applicable beyond the treatment manual. The inclusionof a section on crisis management was excellent. Treatment manuals that ignorecrises fail to acknowledge the experience of most clients in clinical settings.
Challenges of Using the Treatment Manual
As noted earlier, the failure to transfer ESTs from the lab to the field is well documented. This is problematic from a public health perspective because ESTs areseen as a primary component of high-quality health care. Public health agencies
108 Best Practices in Mental Health
Chapter 07_Chapter 07 4/16/13 11:05 AM Page 108

in the United States recently allocated $2 billion to improve dissemination efforts(McHugh & Barlow, 2010). In part this is because the most widely used model ofdisseminating ESTs to community mental health clinicians—reading treatmentmanuals—has been found insufficient to produce sustained, long-lasting changein practitioner knowledge and skill (Herschell et al., 2010). Because manualizedtreatments are so difficult to learn and deliver with fidelity, some have argued thatsole practitioners should not attempt to use treatment manuals (Henggeler &Schoenwald, 2002). Despite the benefits described above, the challenges associ-ated with implementing the PSCT significantly outweighed the benefits. Theremainder of the article will list these challenges and provide recommendationsfor clinicians and treatment development researchers.
Lack of AccessIt is nearly impossible to find out which manualized treatments exist and which
manuals are available; if more than one manual addresses the same problem,there is no system to determine which manual is most appropriate. The clinicianhappened to be familiar with PSCT because he had used it as a teaching tool in anMSW program. Without that very rare circumstance, he would never havethought to use a treatment manual.
The following recommendations may help to address the challenges that havebeen identified:
1. Clinicians should become familiar with compendia of treatment manuals(e.g., Barlow, 2007; LeCroy, 2008) so that they can connect client needwith existing ESTs.
2. Research articles should list the name of the treatment manual used in theclinical trial; they should also indicate whether the manual is available, andunder what circumstances it can be obtained. This will make it easier forclinicians to be informed consumers. Social media and social networkingcan be used to provide resources for clinicians. Examples include podcasts toprovide a “treatment manual on tape” experience; a YouTube channel withshort videos demonstrating key components of the treatment; and a Face-book or Google+ site where clinicians using the manual can find a supportcommunity, get updates on treatment-specific publications and informationon background readings, and learn about upcoming trainings and otherresources. Existing dissemination networks, such as the National Center forChild Traumatic Stress (2007), should be made available to solo communitypractitioners, rather than systematically excluding them. Self-directedtraining, workshops, consultation, and supervision have all been found toimprove a therapist’s knowledge of and skill with an EST beyond what canbe acquired simply by reading a treatment manual (Herschell et al., 2010).
Incompatibility with Agency StructureThe treatment manual used in the case study did not conform to agency regu-
lations regarding intake, assessment, or treatment plan development. It assumed
Case Study 109
Chapter 07_Chapter 07 4/16/13 11:05 AM Page 109

that the decision to use the manual had been made prior to meeting the family.Although this fits clinical research protocols in which therapists treat only clientswho meet criteria specified by the manual, it does not work in community prac-tice, in which clients are assigned to clinicians who have an opening, rather thanto clinicians who provide a specific type of treatment. It will never be certain thata treatment manual will fit a new client’s problems.
Following are some suggestions for dealing with these issues:
1. Clinicians should determine whether the treatment manual is compatiblewith agency requirements for populations served (e.g., adults, parents, orchildren), modalities (e.g., individual, couple, family, and group therapy),and diagnoses or psychosocial problems (e.g., is the clinician allowed to pro-vide services to someone who does not meet criteria for a diagnosis?). Theclinician found that the PSCT treatment manual used in the case study tar-geted family problems, not an individual diagnosis. If his agency had man-dated that treatment follow specific diagnoses rather than problem areas(e.g., problem-solving and communication training), he would not havebeen able to use PSCT.
2. Treatment manuals should spell out in simple language indications andcontraindications for using the treatment with specific psychosocial prob-lems and/or diagnoses, populations, and practice settings. In clinical trials,inclusion and exclusion criteria are managed by the research team, not theclinical team. This information needs to be included in the treatment man-ual. Information about successful implementation in a community setting(i.e., effectiveness trial) should also be included. It should be assumed thatthe treatment manual will be used after intake and assessment, rather thanfrom the beginning of treatment. Although clinical trials are set up so thatonly clients who meet criteria for the treatment are consented into thestudy, decisions in community practice are made after clients enter the sys-tem. The treatment manual should specify whether it is appropriate for usein agencies or organizations whose staff does not have mental health train-ing (e.g., child welfare systems), or in agencies that use a recovery model orare consumer-led programs (Hardiman, Theriot, & Hodges, 2005).
Financial UntenabilityThe treatment manual did not consider agency expectations for clinician bill-
able hours. Not only did the clinician have to provide services that were not billable,but he could not bill for the hours per week he spent reviewing the manual, mak-ing handouts, and preparing for the session. Because he still had to meet his bill-able hours, the time spent on the manual was essentially an in-kind donation to theagency. This is an unrealistic expectation.
Following are recommendations for dealing with this challenge:
1. Clinicians should determine if the treatment is billable before committing tothe treatment. It is unlikely that the treatment manual can be implemented
110 Best Practices in Mental Health
Chapter 07_Chapter 07 4/16/13 11:05 AM Page 110

with less than one hour of preparation for each hour in session with theclient. This could include discussing the manual with a supervisor or a peersupervision group, reviewing the material in advance of the session, andidentifying what worked and what did not work after the session.
2. It is important to identify the type of funding streams that will reimburse forthe EST. Treatment manuals should clearly identify CPT codes that corre-spond to sessions. If there are no known funding streams, or if the treat-ment does not correspond to existing CPT codes, the manual should clarifythat. When face-to-face billable hours are the primary way that agenciesevaluate clinician productivity, unbillable time required by most manuals(e.g., intensive clinical supervision, fidelity checks through video reviewand adherence checklists, and clinician training to competency) is likely tobe discouraged by the agency, or resisted by the clinician unless he or shecan be credited with the time needed to learn the manual (Henggeler &Schoenwald, 2002).
Unreasonable Expectations of Clinician’s Skills and KnowledgeThe treatment manual assumed that the clinician had knowledge of key com-
ponents of therapy, or that the clinician would be able to get additional instruc-tion, training, and/or supervision. A widely cited barrier to implementation ofESTs in community practice is the need for extensive training (Henggeler &Schoenwald, 2002). In the PSCT manual used in the case study, the authorswrote that the treatment was intended for a clinician or advanced student (Robinet al., 1994, p. 92). Two pages later, however, they stated that the procedure out-lined in the manual required prior experience with families and adolescents, andthat supervision is needed for effective implementation. Even if the clinician hadhad the time and money to hire an additional supervisor (which he did not), itmay have been unrealistic to assume that he would find one with experience inPSCT.
Following are recommendations for dealing with these issues:
1. Clinicians should review the manual to determine whether their clinicaltraining and theoretical orientation/practice framework will enable them toeffectively deliver the intervention. Matching a treatment manual to theclinician’s practice framework will increase the clinician’s belief in thevalue of the manual and his or her confidence in the treatment provided.Although the majority of clinicians identify as eclectic, it is likely that mosthave one or two dominant practice perspectives (e.g., they focus on affect,behaviors, or cognitions; emphasize the roots of a problem, either interper-sonal or cognitive, or emphasize current functioning), The clinician in thisarticle found himself fighting against the expectation that the PSCT thera-pist would take an expert role, formulate the problem for the family, and pre-scribe solutions. He learned that unlearning how to be solution focused wasjust as hard as learning PSCT (Palmer-Olson, 2007, cited in Sandberg &Knestel, 2011).
Case Study 111
Chapter 07_Chapter 07 4/16/13 11:05 AM Page 111

2. Treatment manuals should be designed with the intention that most clini-cians will have the skills necessary to use them. A multimillion-dollar studythat produces a detailed theoretically grounded and empirically tested treat-ment approach is only as valuable as a graduate student’s term paper if nei-ther can be used by clinicians. Although the standard protocol in treatmentdevelopment is to fully evaluate the treatment in a lab setting prior to test-ing it in the community, Chorpita (2002) and others have argued forincluding community feedback as early as possible in the process. Once thetreatment protocol has been drafted and used in a pilot study, feedback fromcommunity-based clinicians should be obtained as quickly as possible,using either individuals or focus groups. Questions that should be includedare
• Are treatment goals consistent with agency mandate?• Does the order of the treatment make sense?• Is there sufficient explanation?• How could the treatment manual be made more user friendly?
If the feedback is that the manual is too structured, too complicated, or too con-fusing, treatment development researchers owe it to clinicians and their clients tomake it easier to use. There could be two treatment manuals, one for researchstudies and one for the community, both of which emphasize the same activeingredients. If the researcher starts with the assumption that community practi-tioners will not have access to time or funds to become certified in a treatment, orto treatment-certified supervisors, then they can incorporate into the communityversion of the manual more clinical instruction, including case studies, sampledialogue, and examples of what not to do. The manual would then serve as both aguide and a resource, rather than a prescription for treatment (Escudero, 2012).
Incomplete DocumentationThe treatment manual used in the case study did not include handouts that
were suitable for copying, and in one case did not include an essential homeworkassignment. The best devised dissemination plan (e.g., McHugh & Barlow, 2010)will fail if the treatment manual is written with the researcher, not the clinician,in mind. (Note that the second edition of LeCroy’s (2008) Handbook of Evidence-Based Treatment Manuals for Children and Adolescents includes more reproduciblehandouts and is much more user friendly than the first edition, where the clinicianfound the PSCT treatment manual.)
Suggestions for improvement include the following:
1. Clinicians should review the treatment manual for missing components(e.g., assigned homework) or handouts that are not suitable for copying.
2. Researchers should ensure that all required materials are in ready-to-useformats (e.g., clean handouts that can be photocopied) or should includereference to a website where clinicians can download the documents. Exist-
112 Best Practices in Mental Health
Chapter 07_Chapter 07 4/16/13 11:05 AM Page 112

ing psychometric properties include detailed scoring and interpretationinstructions for outcome measures. If the outcome measures are notincluded in the manual, there should be an explanation (e.g., the materialsare restricted by copyright or need to be purchased separately). Researchersshould know that most independent practitioners will not have the time orresources to obtain additional measures. If the treatment manual cannotinclude the measures used in the research, the authors should includeproxy measures that enable clinicians to gather comparable and useful out-come data.
Conclusion
Although the treatment with Ms. D and her son was not a textbook example ofsuccessful manualized intervention, the experience of trying to implement themanual was clinically useful and shed light on some of the strengths and limita-tions of trying to implement a treatment manual in a community mental healthsetting. Until researchers develop manuals specifically for clinicians—and the sys-tems within which they must provide services—these manuals will not be a con-duit through which to disseminate ESTs. Clinicians who decide to use a treatmentmanual should know that, despite the popular notion that these manuals can beimplemented off the shelf, all will have to be modified to fit client need and agencypolicies and procedures. Although modification will likely mean that the clinicianis not delivering the treatment with fidelity, being trained to deliver the treatmentwith fidelity is unrealistic for most community clinicians.
Adopting and implementing a treatment manual is not the only way to answerthe question of how a clinician can best help clients. However, if clinicians aremade aware of the benefits and challenges associated with implementation andthey are willing to provide feedback to the authors of the treatment manual, andif researchers are willing to make the needed modifications, then well-written andeasily accessible treatment manuals can become a valuable tool in the effort toprovide the best services possible to clients (LeCroy, 2008).
ReferencesAddis, M. E., & Cardemil, E. (2005). Psychotherapy manuals can improve out-
comes. In J. Norcross, L. E. Beutler, & R. Levant (Eds.), Evidence-based practices in mental health: Debate and dialogue on the fundamental questions(pp. 131–139). Washington, DC: American Psychological Association.
Barlow, D. H. (2007). Clinical handbook of psychological disorders: A step-by-steptreatment manual (4th ed.). New York: Guilford Press.
Chorpita, B. F. (2002). Treatment manuals for the real world: Where do we buildthem? Clinical Psychology: Science and Practice, 9, 431–433.
Chorpita, B. F., Becker, K. D., & Daleiden, E. L. (2007). Understanding the com-mon elements of evidence-based practice: Misconceptions and clinicalexamples. Journal of the American Academy of Child and Adolescent Psychia-try, 46(5), 647−652. doi: 10.1097/chi.0b013e318033ff71.
Case Study 113
Chapter 07_Chapter 07 4/16/13 11:05 AM Page 113

Council on Social Work Education. (2008). Educational policy and accreditationstandards. Alexandria, VA: Author.
Duncan, A. E. S., Nicol, M. M., & Ager, A. (2004). Factors that constitute a good cognitive behavioural treatment manual: A Delphi study. Behav-ioural and Cognitive Psychotherapy, 32(2), 199–213. doi: 10.1017/S135246580400116X.
Duncan, B. L., & Miller, S. D. (2005). Treatment manuals do not improve out-comes. In J. Norcross, L. E. Beutler, & R. Levant (Eds.), Evidence-based practices in mental health: Debate and dialogue on the fundamental questions(pp. 140–149). Washington, DC: American Psychological Association.
Drisko, J. W., & Grady, M. D. (2012). Evidence-based practice in clinical social work.New York: Springer.
Escudero, V. (2012). Reconsidering the “heresy” of using treatment manuals.Journal of Family Therapy, 34(1), 106–113. doi: 10.1111/j.1467–6427.2011.00581.x.
Godley, S. H., White, W. L., Diamond, G., Passetti, L., & Titus, J. C. (2001). Thera-pist reactions to manual-guided therapies for the treatment of adolescentmarijuana users. Clinical Psychology: Science and Practice, 8(4), 405–417.doi:10.1093/clipsy.8.4.405.
Hardiman, E. R., Theriot, M. T., & Hodges, J. Q. (2005). Evidence-based practicein mental health: Implications and challenges for consumer-run pro-grams. Best Practices in Mental Health, 1(1), 105–122.
Henggeler, S. W., & Schoenwald, S. K. (2002). Treatment manuals: Necessary,but far from sufficient. Clinical Psychology: Science and Practice, 9(4),419–420.
Herschell, A. B., Kolko, D. J., Baumann, B. L., Abigail, C., & Davis, A. C. (2010).The role of therapist training in the implementation of psychosocialtreatments: A review and critique with recommendations. Clinical Psychology Review, 30(4), 448–466. doi: 10.1016/j.cpr.2010.02.005.
Institute of Medicine. (2001). Crossing the quality chasm: A new health system forthe 21st century. Washington, DC: National Academy Press.
LeCroy, C. W. (1994). Handbook of child and adolescent treatment manuals. NewYork: Lexington Books.
LeCroy, C. W. (2008). Handbook of evidence-based treatment manuals for childrenand adolescents (2nd ed.). New York: Oxford University Press.
McHugh, R., & Barlow, D. H. (2010). The dissemination and implementation ofevidence-based psychological treatments: A review of current efforts.American Psychologist, 65(2), 73–84. doi:10.1037/a0018121.
Myers, L., & Thyer, B. (1997). Should social work clients have the right to effec-tive treatment? Social Work, 42, 288–298. doi: 10.1093/sw/42.3.288.
National Association of Social Workers. (2008). Code of ethics of the NationalAssociation of Social Workers. Washington, DC: Author.
114 Best Practices in Mental Health
Chapter 07_Chapter 07 4/16/13 11:05 AM Page 114

National Center for Child Traumatic Stress. (2007, March). Learning collaborativeinformation packet. Retrieved from http://www.nctsnet.org/nctsn_assets/pdfs/lc_info_packet_3-22-07.pdf.
Northey, W. F., & Hodgson, J. (2008). Keys to implementing empirically supportedtherapies. Journal of Family Psychotherapy, 19(1), 50–84. doi: 10.1080/08975350801904189.
Parrish, D. E., & Rubin, A. (2011). An effective model for continuing educationtraining in evidence-based practice. Research on Social Work Practice,21(1), 77–87. doi: 10.1177/1049731509359187.
Robin, A. L., Bedway, M., & Gilroy, M. (1994). Problem-solving communicationtraining. In C. W. LeCroy (Ed.), Handbook of child and adolescent treatmentmanuals. New York: The Free Press.
Sandberg, J. G., & Knestel, A. (2011). The experience of learning emotionallyfocused couples therapy. Journal of Marital and Family Therapy, 37(4),393–410. doi: 10.1111/j.1752–0606.2011.00254.x.
Sparkes, A. C. (2000). Autoethnography and narratives of self: Reflections oncriteria in action. Sociology of Sport Journal, 17(1), 21–43.
Stegall, S. D., & Nangle, D. W. (2005). Successes and failures in the implemen-tation of a manualized treatment for childhood depression in an out-patient setting. Clinical Case Studies, 4(3), 227–245. doi: 10.1177/1534650103259718.
Case Study 115
Chapter 07_Chapter 07 4/16/13 11:05 AM Page 115

Chapter 07_Chapter 07 4/16/13 11:05 AM Page 116

Character Formation and Identity in Adolescence: Clinical and Developmental IssuesRandolph L. LucenteLyceum Books, Chicago, 2012
168 pages (paperback), $39.95, ISBN 978-1-933478-69-2
Reviewed by Jed Metzger
Character Formation and Identity in Adolescence provides an integrated approach toadolescent development and the various depth-oriented psychoanalytic psycho-therapies. Scholarly and well organized, this book interweaves case vignettes withtheoretical exploration across the adolescent developmental process. Lucente hasan advanced understanding of adolescent development as well as Freudian psy-chologies of ego, object, and self.
The clarity and depth of this book make it an invaluable resource for practi-tioners providing depth-oriented psychoanalytic psychotherapy. Each chaptermakes an important contribution. The book requires a comprehensive knowledgeof development and classical treatment, and therefore will be most useful to eitherdoctoral-level students or experienced practitioners. Additionally, althoughLucente states that the text is offered to bridge classical psychoanalytic psy-chotherapy with postmodern approaches, this reviewer found that the theoreticaland case illustration remained strongly structural.
Chapter 1 focuses on adolescent development and the clinical process. Thematerial is presented from a classical perspective, and is detailed and wellresearched. The treatment approaches mirror the developmental thinking, withemphasis on insight-oriented intervention. The chapter is organized around
Book Reviews
Jed Metzger, PhD, LCSW, is associate professor of social work at Nazareth College in Rochester,New York.
© 2013 Lyceum Books, Inc., Best Practices in Mental Health, Vol. 9, No. 1, March 2013
Chapter 08_Chapter 08 4/16/13 11:05 AM Page 117

identity formation, the development of an ego ideal, and character formation andconcludes with an interesting discussion of intersubjectivity.
Chapter 2, “Narcissism, Character Formation, and Separation-individuation,”begins by framing these concerns against an ego psychological understanding, butquickly moves to introduce self psychology. The integration of the neurobiology ofthe adolescent developmental process is described, followed by a lengthy case pre-sentation illustrating the aforementioned concepts and perspectives.
Chapter 3 takes on splitting, differentiation, and identity. Lucente uses objectrelations theory and ego psychology to frame the therapeutic and developmentalissues. There is an interesting discussion on how transference unfolds, with a vari-ety of perspectives offered. Lucente ultimately rejects the Freudian assessment ofthe transference, favoring a more ego mastery understanding.
Chapter 4 discusses affect regulation and the true self. Here the case and theo-retical presentations are put forward from an intersubjective lens. As the chaptertitle attests, there is a strong application of British object relations theory. The finalchapter presents evidence in support of the book’s approach. A wheel of awarenessmodel is offered to build an evidence base for this form of clinical inquiry.
In sum, this is a well-researched and well-written book. It will be most useful foradvanced practitioners or doctoral students who work from a classical model.Although, as mentioned earlier, the book does not seem to bridge into postmodernapproaches, as Lucente suggests, it would be interesting to see whether a postmod-ern approach could in fact be integrated into the classical structural approaches.
Citizenship Social Work with Older PeopleMalcolm PayneLyceum Books, Chicago, 2012
208 pages (paperback), $36.95, ISBN 978-1-935871-08-8
Reviewed by Jason Dauenhauer
Malcolm Payne’s book Citizenship Social Work with Older People encourages readersto be mindful of the value and importance of aging adults in a global society. Theauthor argues that elders are not afforded the same rights as younger people withregard to active participation and engagement in social relationships. This nega-tive perspective toward aging is fostered by economic development theories inwhich elders are no longer seen as productive, contributing members of society.The author’s purpose for writing this book is to promote critical and creative socialwork skills related to older people in many parts of the world. To enhance thebook’s utility, he has included links to a variety of supplemental Internet resourcesin addition to traditional peer-reviewed scholarly resources.
118 Best Practices in Mental Health
Jason Dauenhauer, PhD, MSW, is associate professor and chairperson, Department of SocialWork, College at Brockport, State University of New York, Brockport, New York.
Chapter 08_Chapter 08 4/16/13 11:05 AM Page 118

The first chapter provides an overview of aging issues while grounding thereader in the author’s principles of citizenship social work—fostering social par-ticipation of all people and promoting societal responsibility for citizens. Readersare encouraged to examine the powerful effects of attitudes toward aging and howthese attitudes translate into social policy and practices. This is reinforced byincluding numerous short case examples, contrasting the experiences of olderadults who are the same chronological age, yet have significantly different lifeexperiences, as well as exercises to promote reflection. Most importantly, thestrengths and weaknesses of aging-related theory are described while keeping thereader focused on social work’s responsibility to recognize the balance of individ-ual, cultural, and large-scale economic social factors that influence the behaviorof older adults.
Chapter 2 describes the increasing trend of service integration for older adultsthat focuses on holistic social work practice to promote independence and dignitywithin and across service systems. Numerous case examples highlight methods ofservice integration and the role of social workers who promote age-proof individu-alized care coordination within communities and service systems. Social work stu-dents and seasoned practitioners alike will be reminded of the importance of theirrole as advocates and agents of change, helping elders to remain engaged as con-tributors to society and not relegated to what the author terms “health care andsocial care ghettos.” The author provides clear definitions of and distinctionsbetween social care and social work within diverse settings. Many useful resourcesare provided as well as examples of different systems of service provision for olderadults in various countries.
Chapter 3 focuses on social work skills with older people, providing a goodoverview of the social work assessment and intervention process and highlightingcase scenarios that are common and relevant (e.g., grief/loss, grandparent caregiving, sexual orientation, and falls). The following two chapters highlight criticalsocial work practice and creativity. The author justifies the need for social workproviders to think critically when engaging with elders, their families, andproviders to assess needs and identify solutions. He encourages practitioners toavoid and/or and to move toward and/also—a very simple, but meaningful way toavoid limitations imposed by structured policies and practices. He also asserts theneed for social workers to promote creative outlets for older adults in various set-tings and provides examples.
The latter portion of the book focuses on groups and macro-practice with olderadults followed by aging-specific topics that relate to social exclusion. The finalchapter emphasizes the inequalities faced by older adults with different life experi-ences, health issues, economic resources, and education. Importantly, the authorconnects these issues to ageism and the role of social work practitioners to advo-cate for social and economic justice and fairness with regard to the provision ofservices. Strategies for safeguarding vulnerable older adults (e.g., elders at risk ofabuse) and special considerations for end-of-life and bereavement issues areincluded.
Book Reviews 119
Chapter 08_Chapter 08 4/16/13 11:05 AM Page 119

In summary, Citizenship Social Work with Older People provides current informa-tion and strategies for social workers who are increasingly engaged in service pro-vision for older adults in many industrialized parts of the world, especially theEuropean Union, the United Kingdom, and the United States. The central theme ofcitizenship social work, with a focus on aging, is grounded in the ethics of thesocial work.
This compendium can be used as a text for a social work practice course onaging, or as a supplemental text for a service-learning course. It reinforces manyof the gero-competencies established by the Council on Social Work Education,and describes current Internet-based resources that provide a global perspectiveon social work and aging. Students will be inspired by the author’s passion fortraining a future generation of social workers who are critically and creativelymindful that older people have a right, and society has a responsibility, to keep thispopulation meaningfully engaged within the community.
Advocacy Practice for Social Justice, 2nd EditionRichard HoeferLyceum Books, Chicago, 2012
256 pages (paperback), $39.95, ISBN 978-1-935871-07-1
Reviewed by Pamela Viggiani
The second edition of Advocacy Practice for Social Justice presents a strong case forincluding advocacy at all levels of social work practice. Hoefer provides a straight-forward and easily readable guide to help students and professionals think aboutand incorporate advocacy into their practice. He reminds students and practition-ers that social work has both a strong history and a current mandate to advocatefor social justice. Hoefer grounds his argument for including advocacy in socialwork practice firmly in the profession’s value base and its ethics. He argues that,when social workers’ values are considered by policy makers, the result is “greatersocial justice across the country and perhaps even in the world” (p. 23).
This book takes the reader from an understanding of advocacy and social jus-tice and its primacy in social work to a model of how to incorporate advocacy intoeveryday practice. Eight of the ten chapters lay out a logical model for social workadvocacy. Chapter 1 presents Hoefer’s unified model for advocacy practice for com-parison with the generalist social work model. His six-step model pairs nicely withthe generalist model of engagement through follow-up.
Each step of Hoefer’s model is fully explicated in chapters 3 through 8. Histhoughtful pairing of his advocacy model with the generalist model allows socialworkers to understand the model as part of good practice rather than as a special-ized practice area.
120 Best Practices in Mental Health
Pamela Viggiani, PhD, LMSW, is associate professor at Nazareth College, Rochester, New York.
Chapter 08_Chapter 08 4/16/13 11:05 AM Page 120

The remaining two chapters provide grounding for advocacy. Chapter 9 pro-vides a basic argument for social workers to strive for social justice and to use advo-cacy to obtain that end. Chapter 10 offers a short overview of the history of socialwork’s advocacy efforts throughout the twentieth century and into the first decadeof the twenty-first century, while calling for the continuation of advocacy in socialwork today. Hoefer reiterates that his book’s major thrust is to present “advocacyas a problem-solving practice technique with steps similar to other practice tech-niques” that “can and should be used in many situations and places . . . in dealingwith client problems at micro-, mezzo-, and macrolevels” (p. 211).
Hoefer’s utilization of case study illustrates the application of his advocacymodel. In the first chapter, for example, he takes a micro-level case and shows howthe advocacy model would work to effectively relieve both the client’s short- andlong-term problems by addressing clinical and social justice concerns. Hoefer alsoincludes tables and graphics that compare, highlight important points, and sim-plify complex concepts. Although his discussion questions and exercises at the endof each chapter may be too basic for many, the annotated references at the end ofeach chapter will allow readers to broaden and deepen their knowledge of topicsdiscussed in the chapters.
Overall, Advocacy Practice for Social Justice is a useful guide for social work prac-titioners and students. The straightforward and readable format is likely to attractreaders and keep their attention. For an instructor, it is a useful text in that it viewsadvocacy as a part of ethical social work at micro-, mezzo-, and macrolevels ofpractice and easily incorporates advocacy strategies across the practice curricu-lum. Hoefer furthers social work’s primary mission, to “enhance human well-being and help meet the basic human needs of all people, with particular attentionto the needs and empowerment of people who are vulnerable, oppressed, and liv-ing in poverty” (Code of Ethics of the National Association of Social Workers,1996, http://www.socialworkers.org/pubs/code/code.asp).
Book Reviews 121
Chapter 08_Chapter 08 4/16/13 11:05 AM Page 121

Chapter 08_Chapter 08 4/16/13 11:05 AM Page 122

The purpose of this article is to provide reviews of some of the key websites on a topicgermane to the current issue of Best Practices in Mental Health. Because a numberof articles in this issue concern youth, sites on attention deficit hyperactivity disorders(ADHD) were selected. Sites will be organized by government, general, and membershiporganizations.
Government Websites
Centers for Disease Control and Prevention: http://www.cdc.gov/ncbddd/adhd/
The Centers for Disease Control and Prevention (CDC) website on ADHD isvery user friendly, and will appeal to the general public. Pictures and icons makenavigating the site very easy. With an apparent goal of educating the publicabout ADHD, this site provides research, data, and statistics, recommended arti-cles, and avenues for accessing more information including conferences andworkshops. This site provides a personal touch with stories from people livingwith ADHD.
Mayo Clinic: http://www.mayoclinic.com/health/adhd/DS00275
The Mayo Clinic site on ADHD provides a basic but helpful overview of the dis-order. It provides information on symptoms, causes, risk factors, complications,diagnosis, and treatment. Additionally, the site includes pages on lifestyle andhome remedies and alternative treatments, which provide tips for managingsymptoms outside of medication management. This site would be appropriate forthose looking to gain a basic understanding of ADHD.
Website Review:
Your Attention Please: A Review of Selected Websiteson Attention Deficit Hyperactivity Disorders
Kristin Beers and Stephanie Sundborg
Kristin Beers is an MSW student at Portland State University, Portland, Oregon. Stephanie Sund-borg, MS, is a PhD student at Portland State University, Portland, Oregon.
© 2013 Lyceum Books, Inc., Best Practices in Mental Health, Vol. 9, No. 1, March 2013
Chapter 09_Chapter 09 4/16/13 11:08 AM Page 123

National Institute of Mental Health: http://www.nimh.nih.gov/health/publications/attention-deficit-hyperactivity-disorder/
Like the Mayo Clinic website, the National Institute of Mental Health (NIMH)ADHD site provides basic, easy-to-read information about ADHD; however, NIMHextends beyond symptom, diagnosis, and treatment to discuss co-occurring disor-ders, strategies for working with schools, and information about adult ADHD.Information from NIMH is also available in print, which makes it a useful tool forhealth and mental health providers, as well as schools and support centers.
PubMed Health: http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0002518/
This website outlines causes, risk factors, symptoms, and treatment for ADHD.It contains information helpful to both parents and practitioners, as well as initialsteps for diagnosing ADHD in children. The Signs and Tests section outlines thecriteria for diagnosing ADHD, which is particularly helpful because ADHD is oftenmisdiagnosed or undiagnosed. The Treatment section addresses various treatmentmethodologies including medication and behavior therapy.
General Websites
Shire US Inc.: http://www.adhdandyou.com/
This easy-to-navigate website provides targeted information for individualswith ADHD, their parents/families, and professionals. Each section contains infor-mation relevant to a particular group, with a focus on managing the disorder.There is an extensive resource section with tools and information. The site isupdated regularly with new information.
National Resource Center on AD/HD: http://www.help4adhd.org/
Funded by the CDC and sponsored by Children and Adults with AttentionDeficit Disorder, this website offers information on the science behind ADHD,along with resources and support. Targeting individuals (or their families) withADHD, this site covers topics from dealing with the educational, legal, and insur-ance systems to practical concerns regarding workplace issues and maintainingsocial relationships. The information is provided through a variety of methodsincluding webinars, podcasts, and a live help line.
Membership Websites
Attention Deficit Disorder Association (ADDA): http://www.add.org/
The ADDA is a membership association that provides information andresources for adults with ADHD. The site provides little information about the dis-order itself, but offers updates on legislation and advocacy opportunities, andinformation about support groups, as well as scholarship information for collegestudents. Much of the website is easily accessible; however, newsletters and webi-nars are for members only.
124 Best Practices in Mental Health
Chapter 09_Chapter 09 4/16/13 11:08 AM Page 124

Children and Adults with Attention Deficit/Hyperactivity Disorder (CHADD):http://www.chadd.org/
The CHADD organization website is one of the more comprehensive and acces-sible, offering information about ADHD in children, teens, and young adults, aswell as adults. It outlines information about symptoms, diagnosis, treatment, andcoexisting disorders; resources including local support groups, research, and aprofessional directory; and information about conferences and trainings. With theexception of information directed toward the organization’s members, the websiteis easy to navigate and gives links to additional information and assistancethrough the National Resource Center on ADHD.
The Attention Deficit Disorder (ADD)/ADHD Support Site:http://www.attentiondeficit-add-adhd.com/
This site provides basic, summarized information on a wide range of topics.Topics include overviews of child and adult ADHD; information about potentialside effects of commonly prescribed medications; research and literature on thedisorder; and information on nutrition and ADHD, school resources, and summercamps for children with ADHD. Much of the website is focused on medication sideeffects, nutrition, and literature.
Website Review 125
Chapter 09_Chapter 09 4/16/13 11:08 AM Page 125

Since1988SOCIAL WORK PUBLISHER
YourLYCEUMB O O K S , I N C .
5758 S. Blackstone, Chicago, IL 60637
4 EASY WAYS TO ORDERE m a i l : l y c e u m @ l y c e u m b o o k s . c o mCall: 1 - 7 7 3 - 6 4 3 - 1 9 0 2Fax: 1 - 7 7 3 - 6 4 3 - 1 9 0 3We b : w w w. l y c e u m b o o k s . c o m / s h o p
Best Practices at Your Finger TipsAn Easy-to-Use Text with Ready-to-Implement Approaches
Preface Introduction - What are Best Practices and WhyShould We Care? Vikki L. Vandiver
Part I Behavioral Healthcare Oriented Best Practices1. Integrated Treatment for People with Co-Occurring Mental Illness and Substance Use Disorder Madeleine S. Rafferty & Robert Drake
2. Nonmedical Roles in Psychopharmacotherapy Kia J. Bentley & Joseph Walsh
3. Illness Management and Recovery Kim T. Mueser & Susan Gingerich
4. Best Practices for Improving the Health of Personswith Serious Mental Illness and Comorbid Physical Conditions Sara Bressi Nath
5. Harm Reduction in Mental Health Practice Katie Witkiewitz, Justin Walthers, & G. Alan Marlatt
Part II Community Oriented Best Practices6. Tribal Best Practices: A Native American Horsemanship Program for Indian Youth John Spence & Vikki L. Vandiver
7. Assertive Community Treatment Michelle P. Salyers, Sam Tsemberis, & Laura Stull
8. Supported Housing Yin-Ling Irene Wong & Sungkyu Lee
9. Housing First: Homelessness, Recovery, and Community Integration Sam Tsemberis & Benjamin Henwood
10. Supported Employment Marina Kukla & Gary R. Bond
Part III Empowerment Oriented Best Practices11. Spirituality and Mental Health
David Derezotes12. Recovery Oriented Services
Victoria Stanhope & Phyllis Solomon13. Motivational Interviewing
Alan B. McGuire & Tim D. Gearhart14. Best Practices for Family Caregivers of Peoplewith Severe Mental Illness Susan E. Mason
Part IV Educationally Oriented Best Practices15. Psychiatric Rehabilitation
William Anthony, Rick Forbess, & Kathleen Furlong-Norman
16. Supported Education Karen V. Unger17. Psychoeducation Joseph Walsh
Part V Children and Youth Oriented Best Practices18. Early Intervention for Youth Psychosis: The Australian Model Patrick McGorry & Sherilyn Goldstone
19. Best Practices in Children’s Mental Health Peter Nguyen
Part VI Organizationally Oriented Best Practices:Pulling It All Together 20. Sanctuary Model Sandra Bloom
Concluding RemarksAre We There Yet? Ensuring Quality Best PracticesVikki L. Vandiver
CONTENTS
2013 paperback, 332 pages, ISBN 978-1-935871-04-0, $49.95
“Best Practices in Community Mental Health offers a broad andwell-researched overview of the contemporary issues facing thecommunity mental health field and its consumers. Each chapter is authored by well-known writers and researchers in their field.”
—Rick Trammell, Argosy University, Hawaii
Each chapter features: •Background information and theory •Steps for implementation •Review of available evidence •Glossary of terms •Suggestions for further reading
BPMH Ads1_Layout 1 2/20/13 1:24 PM Page 1

Since1988SOCIAL WORK PUBLISHER
YourLYCEUMB O O K S , I N C .
5758 S. Blackstone, Chicago, IL 60637
4 EASY WAYS TO ORDERE m a i l : l y c e u m @ l y c e u m b o o k s . c o mCall: 1 - 7 7 3 - 6 4 3 - 1 9 0 2Fax: 1 - 7 7 3 - 6 4 3 - 1 9 0 3We b : w w w. l y c e u m b o o k s . c o m / s h o p
New from Lyceum BooksThe Recovery Philosophy and Direct Social Work Practice
2013 paperback, 257 pages, ISBN 978-1-935871-23-1, $37.95
“This book is a handbook on social work’s naturalcompatibility with recovery perspectives onmental illness. It is timely, packed with the knowledge and practices necessary for clinicalsocial workers to function successfully within the recovery approach and, above all, speaks to students and practitioners about their role in relation to consumers. I think this book is excellent.”
—Daniel Salhani, University of British Columbia,Okanagan
Joseph Walsh’s new book gives a clear, practice-oriented approach to social work using the recovery philosophy. The book provides in-depth examples of recovery practice withpersons who have schizophrenia, depression, bipolar disorder, and autism spectrum disorders. The recovery philosophy offers clients a path to wellness, hope, self-direction,and social inclusion, and gives social workers a new way to serve and empower their clients.
Features� A practice-based approach, with content on the dynamics of the social worker/consumer relationship and clinical endings in recovery work
� History and definitions of several models of recovery� Summaries and discussion questions following each chapter
Scan QR code to see full description, and the expanded table of contents!
BPMH Ads1_Layout 1 2/20/13 1:24 PM Page 2

Since1988SOCIAL WORK PUBLISHER
YourLYCEUMB O O K S , I N C .
5758 S. Blackstone, Chicago, IL 60637
4 EASY WAYS TO ORDEREma i l : l y ceum@lyceumbook s . comCall: 1 -773 -643 -1902Fax: 1 -773 -643 -1903Web : www. l yceumbook s . com/shop
Self Care for Social Workers by Way of the Kitchen
BSW and MSW students have a lot on their plate, but unfortunately that doesn't always include healthy meals. This two-year cooking guide can help any social work student(or professor) incorporate tasty, healthy meals into their busylives. With recipes contributed from over fifty social work educators, Corcoran's cookbook adds a lot more flavor and fun to the idea of self care!
2013 paperback, 304 pages, ISBN 978-1-933478-94-4, $29.95
Best Practices in the Classroom Environment
Whether you are a graduate student or a tenure-track professor, this book willhelp you identify your teachingstrengths and provide you with the tools to successfully share and buildknowledge within the classroom setting.
2013 paperback, 70 pages, ISBN 978-1-935871-28-6, $19.95
This guidebook illustrates how to integrate affective learning into the class-room experience, which helps nurturestudents into scientifically sophisticated,and client-centered practitionersgrounded in discipline and compassion.
2011 paperback, 192 pages, ISBN 978-1-933478-45-6, $34.95
BPMH Ads2_Layout 1 2/20/13 1:26 PM Page 1

METHOD OF PAYMENT:
� Visa � MasterCard � American Express � Check (enclosed)
Card number _____________________________________________________________ Exp. date __________________
Card holder signaure ____________________________________________________________________________________
Daytime phone ________________________________________________________________________________________
SHIP TO:
Name ______________________________________________________________________________________________
Company (for Institutions/Libraries) ______________________________________________________________________
Address ____________________________________________________________________________________________
City / State / ZIP ______________________________________ Country__________________________________________
Phone ____________________________________________ Email address* __________________________________
Mail: Complete and return this order form with payment to:
Lyceum Books, Inc.
5758 S. Blackstone Ave.
Chicago, IL 60637
Phone: 773-643-1902
e-mail: [email protected]
web: http://lyceumbooks.com/MentalHJournal.htm
Since1988SOCIAL WORK PUBLISHER
YourLYCEUMB O O K S , I N C .
5758 S. Blackstone, Chicago, IL 60637
Facebook@LyceumBooks
Twitter@LyceumBooks
Order Your Subscription to Best Practices in Mental HealthToday!
FOUR WAYS TO ORDER
Individual Subscription: US $40.00 (add US $15.00 for international shipping)
Institutional/Library Subscription: US $90.00 (add US $15.00 for international shipping)
To subscribe to Best Practices in Mental Health for one year (two issues), contact Lyceum Books.
MH OrderForm_MH OrderForm 2/12/13 10:13 AM Page 1


















