Best Practice JCEM Screening Neonatal y usar solamente de TSH.pdf
13
6 Neonatal TSH screening: is it a sensitive and reliable tool for monitoring iodine status in populations? Mu Li, PhD, Senior Lecturer a, * , Creswell J. Eastman, MD, Clinical Professor, Vice Chairman of ICCIDD and Regional Coordinator Asia Pacific Region b,1 a School of Public Health, the University of Sydney, Sydney, NSW 2006, Australia b Sydney Medical School, the University of Sydney, Sydney, NSW 2006, Australia Keywords: newborns thyr oid stimula ting hormone (or thyr otropin ) monitoring iodine deficiency Iodine deficiency is the most common cause of preventable brain damage in the newborn. The indicator s for ass essing iodine nutr itional stat us include urinary iodine exc reti on, thyroid size, thyroid stimulat ing hor mone (TS H) and thyroglobul in (T g) concentrati ons in the blood. Neonat al TSH concentra tion is increased when the supply of thyroid hormone and iodine from the maternal circulation to the foetus has been compromised. The Worl d Healt h Organiza tion (WHO) has sugges ted that when a sensitive assay is used on samples collected 3–4 days after birth, a <3% frequency of TSH concentrations >5 mIU l 1 indicates iodine sufficiency in a population. However, many studies have attempted to apply the fre quency of neonat al TSH val ues >5 mIU l 1 in determining population iodine status and monitoring intervention programmes, and although some have proven to be successful , most have provided conflicting or uncertain data. This is due to the man y tec hni cal iss ues that remain unr esolve d on the use of neonatal TSH screening for moni tor ing iodine stat us, making it doubtful as a sensitive and reliable quantitative tool. More research is required to resolve these issues. In the interim, WHO should consider wit hdr awing its cur rent gui del ines for neonat al TSH screening for monitoring iodine deficiency in populations. Crown Copyright 2009 Published by Elsevier Ltd. All rights reserved. * Tel.: þ61 2 9351 5996; Fax: þ61 2 9351 5049. E-mail addresses: muli@health.usyd.edu.au (M. Li), ceastman@me d.usyd.edu.au (C.J. Eastman). 1 Tel.: þ61 2 9439 9396; Fax: þ61 2 9436 1505. Contents lists available at ScienceDirect Best Practice & Research Clinical Endocrinology & Metabolism journal homepage: www.elsevier.com/locate/beem 1521-690X/$ – see front matter Crown Copyright 2009 Published by Elsevier Ltd. All rights reserved. doi:10.1016/j.beem.2009.08.007 Best Practice & Research Clinical Endocrinology & Metabolism 24 (2010) 63–75
-
Upload
erickmattos -
Category
Documents
-
view
216 -
download
0
Transcript of Best Practice JCEM Screening Neonatal y usar solamente de TSH.pdf

8/10/2019 Best Practice JCEM Screening Neonatal y usar solamente de TSH.pdf
http://slidepdf.com/reader/full/best-practice-jcem-screening-neonatal-y-usar-solamente-de-tshpdf 1/13
6
Neonatal TSH screening: is it a sensitive and reliable tool formonitoring iodine status in populations?
Mu Li, PhD, Senior Lecturer a,*, Creswell J. Eastman, MD, Clinical Professor,
Vice Chairman of ICCIDD and Regional Coordinator Asia Pacific Region b,
1
a School of Public Health, the University of Sydney, Sydney, NSW 2006, Australiab Sydney Medical School, the University of Sydney, Sydney, NSW 2006, Australia
Keywords:
newborns
thyroid stimulating hormone (or thyrotropin)
monitoring
iodine deficiency
Iodine deficiency is the most common cause of preventable brain
damage in the newborn. The indicators for assessing iodine
nutritional status include urinary iodine excretion, thyroid size,
thyroid stimulating hormone (TSH) and thyroglobulin (Tg)
concentrations in the blood. Neonatal TSH concentration is
increased when the supply of thyroid hormone and iodine fromthe maternal circulation to the foetus has been compromised. The
World Health Organization (WHO) has suggested that when
a sensitive assay is used on samples collected 3–4 days after birth,
a <3% frequency of TSH concentrations >5 mIU l1 indicates iodine
sufficiency in a population. However, many studies have attempted
to apply the frequency of neonatal TSH values >5 mIU l1 in
determining population iodine status and monitoring intervention
programmes, and although some have proven to be successful,
most have provided conflicting or uncertain data. This is due to the
many technical issues that remain unresolved on the use of
neonatal TSH screening for monitoring iodine status, making it
doubtful as a sensitive and reliable quantitative tool. More research
is required to resolve these issues. In the interim, WHO should
consider withdrawing its current guidelines for neonatal TSH
screening for monitoring iodine deficiency in populations.
Crown Copyright 2009 Published by Elsevier Ltd. All rights
reserved.
* Tel.: þ61 2 9351 5996; Fax: þ61 2 9351 5049.
E-mail addresses: [email protected] (M. Li), [email protected] (C.J. Eastman).1 Tel.: þ61 2 9439 9396; Fax: þ61 2 9436 1505.
Contents lists available at ScienceDirect
Best Practice & Research Clinical
Endocrinology & Metabolismj o u r n a l h o m e p a g e : w w w . e l s e v i e r . c o m / lo c a t e / b e e m
1521-690X/$ – see front matter Crown Copyright 2009 Published by Elsevier Ltd. All rights reserved.
doi:10.1016/j.beem.2009.08.007
Best Practice & Research Clinical Endocrinology & Metabolism 24 (2010) 63–75

8/10/2019 Best Practice JCEM Screening Neonatal y usar solamente de TSH.pdf
http://slidepdf.com/reader/full/best-practice-jcem-screening-neonatal-y-usar-solamente-de-tshpdf 2/13
Iodine nutrition in pregnant women and newborns
Iodine requirement in pregnancy
Iodine of maternal origin is essential for foetal and neonatal brain development. At a population and
global level, iodine deficiency is theleading cause of preventablemental handicap.At an individual level,the developing brain is extremely vulnerable to even minor degrees of maternal hypothyroxinaemia
secondary to iodine deficiency or maternal thyroid disease. Even mild, clinically unrecognisable,
hypothyroxinaemia can cause serious irreversible neuromotor deficits rendering a child handicapped
for life.1 The invisibility of the deficiency during pregnancy and neonatal development makes it all the
more dangerous in both developing and developed societies. Despite enormous efforts to conquer
iodine deficiency, it remains a serious public health problem. The World Health Organisation (WHO)
estimates that almost 2 billion people worldwide, comprising over 300 million children in 54 countries,
still have inadequate iodine intake.2 The United Nations Children’s Fund (UNICEF) estimates that
presently over 38 million newborns annually are not protected from iodine deficiency.3
Pregnancydemands a largeincrease in iodinerequirementsprincipally to keep pacewith theincreased
maternal thyroidal productionof thyroxine(T4).The maternal thyroidhormone pool (chiefly T4) increaseson average by 50% due to the need to saturate the increased thyroxine-binding globulin produced by the
liver and maintain a normal free T4 concentration. Increased T4 production is facilitated by enhanced
thyroidal stimulation from human chorionic gonadotropin during early pregnancy.4 Additional demands
on the thyroid come from passage of T4 from mother to foetus and increased degradation of T4 by the
placenta.4 Enhanced renal clearance of iodine during pregnancy results in maternal wastage of iodineand
contributes to the demand for increased iodine intake. While the foetal thyroid commences synthesis of
thyroid hormone at the end of the first or early second trimester, most of the T4 in the foetal circulation is
derived from maternal passage until very late in pregnancy. In addition to maternal transfer of T4 to the
foetus, there is also transfer of iodine in the latter weeks of gestation. Although the precise quantity of this
transfer has yet tobe established, it isestimated to bein the range of 50–75 mg per day, based on the known
requirement of 90 mg per day in the neonates and infants (0–12 months).6
The recommended daily intake (RDI) of iodine in the non-pregnant state is 150 mg, increasing to
250 mg during pregnancy.5,6 The infant will require around 90–100 mg iodine per day, mandating
a requirement of approximately 250 mg iodine daily in the breastfeeding mother.5,6 The iodine content
of human breast milk varies with maternal iodine intake, emphasising the need to ensure iodine intake
is boosted during lactation to protect the infant from hypothyroxinaemia.
Monitoring of iodine intake and use during pregnancy and lactation in mothers remains a contro-
versial and poorly researched issue. Urinary iodine excretion, serum concentrations of free T4, TSH and
thyroglobulin (Tg) provide direct or indirect indices of thyroid function and iodine intake during
pregnancy. Each of these tests is prone to methodological problems and artefactual interference during
pregnancy. The simplest test at a population level, but not in an individual, is the urinary iodine
excretion concentration (UIC). Most of the iodine absorbed through the gut is eventually excreted inthe urine. One can calculate iodine intake using the simple assumption that 90% of intake is excreted
within the next 24 h. The current convention of judging UIC measurements in pregnant women against
non-pregnant adults is misleading. If the RDI for iodine during pregnancy is 250 mg per day, then this
intake would correspond to a UIC of 150 mg l1.4
Physiology and pathophysiology of use of iodine in the foetus and neonate
An adequate iodine intake in the mother is essential for the normal synthesis of maternal and foetal
thyroid hormones important for foetal brain development.7,8 Insufficient iodine supply from the
mother can result in a decreased synthesis of both T4 and 30,3,5-triiodothyronine (T3), with an
increased concentration of TSH in the newborn. In most cases, the impaired thyroid function due toiodine deficiency is transient.9 Infants, especially if born prematurely, are susceptible to transient
hypothyroxinaemia10, a condition characterised by a transient elevation of newborn TSH level in
conjunction with a normal T4 concentration. It occurs at higher frequency in mild-to-moderate iodine-
deficient environments.11
M. Li, C.J. Eastman / Best Practice & Research Clinical Endocrinology & Metabolism 24 (2010) 63–7564

8/10/2019 Best Practice JCEM Screening Neonatal y usar solamente de TSH.pdf
http://slidepdf.com/reader/full/best-practice-jcem-screening-neonatal-y-usar-solamente-de-tshpdf 3/13
Neonatal TSH screening
Neonatal screening for Congenital Hypothyroidism
The incidence of sporadic congenital hypothyroidism (CH) is around 1 in 3000 to 1 in 4000 live
births.11,12 The symptoms and signs of sporadic congenital hypothyroidism are often non-specific and,unless tested for biochemically, CH will be frequently overlooked, resulting in irreparable neurological
damage from thyroid hormone deficiency during this crucial period of brain development. To address
this problem and permit early detection and implementation of thyroid hormone therapy, systematic
screening programmes for thyroid function were introduced in many countries in the early 1970s.11,13
The initial screening method was measurement of T4 in heel-prick blood samples. This has been
superseded by measurement of thyrotropin (TSH) in most programmes around the world. Convincing
arguments can be made for the superiority of either one of these tests as the primary screening
method. The major disadvantage of using TSH is that it will not detect central (hypothalamic or
pituitary) hypothyroidism, a rare disorder occurring in approximately 1 in 20 000 neonates, that can be
picked up by T4 testing. TSH testing does detect subclinical or transient primary hypothyroidism that
will be missed by T4 screening and may cause brain damage.12
TSH testing results in neonates born in iodine-deficient environments
The newborn thyroid has limited iodine stores, and even mild deficiency during pregnancy will
compromise neonatal thyroidal secretion of T4 causing increased pituitary TSH secretion. It follows
that an elevated TSH in the neonate is a sensitive indicator of an inadequate supply of thyroid hormone
to the developing brain. This principle underpins the application of newborn TSH screening as an
indicator of maternal and hence population iodine nutrition. Thus, neonatal TSH screening may be
a powerful and underused tool in monitoring iodine nutrition in mothers and babies. However,
multiple factors other than maternal iodine status can influence measurement of newborn TSH,
including prematurity, the timing of the heel-prick collection, maternal or newborn exposure toiodine-containing antiseptics (povidone), the collection paper employed for the bloodspot and the TSH
assay methodology. Consequently, the original recommendations of categorising the severity of iodine
deficiency using measurement of neonatal TSH promulgated by WHO in 199414 (Table 1) have not been
included in the more recent recommendations.6,15 The Swiss experience showed neonatal TSH was
sensitive to even marginal improvement of iodine nutrition status of pregnant women, following the
increase of iodine concentration in iodised salt. This was demonstrated in the reduction of the
frequency of newborn TSH values >5 mIU l1 from 2.9% to 1.7%.16
Newborn TSH screening as a tool for assessing iodine deficiency
Monitoring tool in iodine-deficient environments
In contrast to sporadic CH, elevated TSH levels, accompanied by either normal or low T4 levels occur
much more commonly in neonates born in iodine-deficient environments. Studies performed in the
1980s in Zaire and India, where iodine deficiency is endemic, confirmed neonatal TSH concentrations
were grossly elevated in the cord blood of the offspring of mothers suffering from moderate-to-severe
Table 1
WHO/ICCIDD/UNICEF Indicators for Assessing Iodine Deficiency Disorders.
Indicator Target
population
Severity of public health problem (prevalence)
Mild Moderate Severe
Thyroid volume >97 centile by ultrasound SACa
5.0–19.9% 20.0–29.9% 30%Median urinary iodine level (mg/L) SAC 50–99 20–49 <20
TSH >5 mIU/l whole blood Newborns 3.0–19.9% 20.0–39.9% 40%
Adapted from WHO/NUT/94.6, 1994 (14).a School aged children
M. Li, C.J. Eastman / Best Practice & Research Clinical Endocrinology & Metabolism 24 (2010) 63–75 65

8/10/2019 Best Practice JCEM Screening Neonatal y usar solamente de TSH.pdf
http://slidepdf.com/reader/full/best-practice-jcem-screening-neonatal-y-usar-solamente-de-tshpdf 4/13
iodine deficiency.17–19 From these studies, neonatal TSH screening was put forward as a population-
monitoring tool for iodine deficiency, in addition to its role as a case-detection tool for diagnosing
individual neonates with congenital hypothyroidism.20
Delange advocated neonatal thyroid screening as an indicator of the degree of iodine deficiency at
a population level and as a monitoring tool in programmes of iodine supplementation.20,21 In his
reviews, Delange concluded that neonatal TSH screening is the only indicator that allows prediction of a possible impairment of mental development.20,21 However, in the context of declining urinary iodine
concentration reported from several countries, where the frequency of TSH >5 mIU l1 is often below
3%, it is uncertain whether neonatal TSH screening results can truly reflect the current iodine intake
trend in these populations.22,23
Published reports of neonatal TSH screening for monitoring population iodine nutrition
Table 2 is a summary of published reports using TSH screening for assessment of iodine-deficiency
status or monitoring theoutcome of iodine prophylaxis programmes in countries or sub-national regions,
with reference to the WHO criteria.6,14,15 One good example is in southeast Poland, where Tylek-
Lemanska24 and colleagues were able to demonstrate that, from the CH screening programme, with thereintroduction of iodised kitchen salt in 1992, the prevalence of neonatal TSH results 5 mIU l1 dropped
from above 20% in 1991 to just over 5% between 1995 and 2000. There have been other examples of using
newborn TSH screening to assess iodine-deficiency status.16,25–37 In Thailand, with the application of
a geographic information system to their neonatal TSH screening programme, which covers 760 000 live
births annually (94% of total), it is possible to identify iodine deficiency down to the sub-district level.37
In Table 2, reported studies are listed under three categories, according to the timing and nature of
the blood samples. Majority of the published reports have employed dried blood spot samples
collected >48 h after birth, as recommended for neonatal screening for CH. Greater than 3% of TSH
>5 mIU l1 is the arbitrary indicator for iodine deficiency in a population.6,15 Some studies have used
dried cord blood spots, particularly the two multi-nation studies by Sullivan30 and Copeland,34 which
also used TSH >5 mIU l1
as the cut off. Other studies used cord blood serum samples. In addition,multiple methods, and the same technique by different assay manufacturers, have been used. In the
following, we look at these issues closely to see how they may impact on the TSH test results.
Influencing factors of newborn TSH measurements
Maternal iodine status
Maternal iodine nutrition and thyroid function status can have significant impact on foetal and
newborns’ TSH levels.38 In a study comparing maternal and neonatal thyroid status in Nigeria,39 it was
found that women from a known iodine-deficient area (Saki) had significantly lower UIC levels and
higher goitre rates compared with women from the control area. Their plasma total T3 (TT3) and total
T4 (TT4) were lower and TSH was higher than the values of the controls, although they did not reachthe statistically significant level. The mean plasma neonatal TSH of babies from Saki, however, was
significantly higher than the control value.
Data from newborn screening in Europe have shown that the frequency of serum TSH >50 mU ml1
(mIU l1) for recall was inversely related to maternal urinary iodine level. 9 This was further evidenced
by the Costante study,31 which showed a negative relationship between the frequency of TSH
>11 mU ml1 (mIU l1), the 97% cut off of neonatal TSH and the median UIC of schoolchildren living in
the same area (r2¼ 0.86, P ¼ 0.007). A study conducted in the West Black Sea area of Turkey showed
that the maternal median UIC was different for mothers living in three different cities (from 31 mg l1 to
75 mg l1). The proportion of neonatal heel blood TSH >5 mIU l1 and the median neonatal Tg
concentration correlated inversely with the maternal UIC.36 A study of a cohort of 253 healthy pregnant
women in Hong Kong has clearly demonstrated that mothers had lower urinary iodine levels givingbirth to infants with higher TSH level, compared with mothers with normal urinary iodine excretion
levels. Furthermore, women, who had given birth to infants with cord blood serum TSH >16 mIU l1,
had significantly lower urinary iodine concentrations and serum FT4 levels compared with mothers
who had given birth to newborns with normal TSH levels.40 A recent study from three districts of
M. Li, C.J. Eastman / Best Practice & Research Clinical Endocrinology & Metabolism 24 (2010) 63–7566

8/10/2019 Best Practice JCEM Screening Neonatal y usar solamente de TSH.pdf
http://slidepdf.com/reader/full/best-practice-jcem-screening-neonatal-y-usar-solamente-de-tshpdf 5/13
Table 2
Reported Neonatal TSH with Reference to Iodine Deficiency.
Country/Region Settings Sample size Frequency (%) Method UIE (m
Dried blood spot collected >48 hours after birth (>5 mIU/L)
Italy/Calabria Neonatal screening
program
22,384 14.4 Fluroimmunoassay
(DELFIA neonatal TSH kit Wallac, Finland)
65.6 (
Belgium/Brussels Neonatal screeningprogram
308,614 4.5
Estonia Neonatal screening
program
20,021 17.7 Fluroimmunoassay
(DELFIA neonatal TSH kit)
65b (S
Poland/Cracow Neonatal screening
program
634,179 20–5.7 Fluroimmunoassay (FIA) and
Luminoimmunoassay (LIA)
Argentina/Buenos Aires Neonatal screening
program
1,500 2.7 Immuno-flurometric assay
(IFMA, DELFIA neonatal
TSH kit Wallac)
143 (
30.0 IRMA (DPC)
Turkey/West Black
Sea Area
Neonatal screening
program
18,606 26.7 RIA (DPC, USA) Moth
neona
Switzerland Neonatal screening
program
259,035 2.9 (1992–98) Time-resolved
Fluroimmunoassay
Moth
249 (
SC
115 (
141 (
218,665 1.7 (1999–2004)
Ireland Neonatal screening
program
73,019 3.64–2.35
(1995–2006)
Dissociation-enhanced
fluroimmunoassay (DELFIA)
45–68
(preg
Thailand Neonatal screening
program
550,927 13.54 (2003) ELISA
543,121 15.28 (2004)
639,583 21.55 (2005)
766,392 19.56 (2006)
Australia/Sydney Teaching Hospital 1,316 8.1, 5.4 Dissociation-enhanced
fluroimmunoassay
(DELFIA Wallac, Finland)
109 (
1,457
USA/Atlanta Hospital 28 42.9 ELISA (Enzaplate N-TSH, Ciba
Corning Japan)
282
Australia/NSW Public hospitals
and local community
health centres
815 2.2 Fluroimmunoassay
(Auto DELFIA Wallac)
Moth
Thailand/Songkhla District hospitals 236 8.9 Immunoradiometric assay Gesta
75.5
28–30
34–36
72.1

8/10/2019 Best Practice JCEM Screening Neonatal y usar solamente de TSH.pdf
http://slidepdf.com/reader/full/best-practice-jcem-screening-neonatal-y-usar-solamente-de-tshpdf 6/13
Table 2 (continued)
Country/Region Settings Sample size Frequency (%) Method UIE (m
Dried cord blood spot sample collected at delivery (>5 mIU/L)
Malaysia/Kuching Major hospitals 195 52 ELISA (Spectra-Screen TSH,
IEM Diagnostics, USA)
33 (m
Philippines/Manila Major hospitals 750 32 ELISA (Spectra-Screen TSH,
IEM Diagnostics, USA)
40b (S
Pakistan/Islamabad
Quetta
Lahore
Karachi
Major hospitals 201
279
256
148
76
65
80
69
ELISA (Spectra-Screen TSH,
IEM Diagnostics, USA)
Kyrgyzstan
Bishkek
Osh
Major hospitals 90
92
74
47
ELISA (Spectra-Screen TSH,
IEM Diagnostics, USA)
30 (S
Bangladesh Local hospitals 208 84 ELISA (Enzaplate N-TSH,
Ciba Corning Japan)
96 (m
73 (S
Guatemala Local hospitals 141 58 ELISA ((Enzaplate N-TSH,
Ciba Corning Japan)
120 (
181 (
USA Local hospitals 243 82 ELISA (Enzaplate N-TSH,
Ciba Corning Japan)
105 (
282 (Argentina/Buenos Aires Neonatal screening
program
186 11.3 Immuno-fluorometric assay
(DELFIA Wallac, Finland)
143 (
Cord blood serum collected at delivery (>10 mIU/L unless specified)
Thailand/Chiangmai
Nan
Bangkok
Provincial and
district hospitals
Teaching hospital
(Bangkok)
10,150
8,603
7,688
20.0
15.3
7.2
Immunoradiometric assay
(Department of Health
Science, Thailand)
64b
Hong Kong Teaching hospital 253 22 Immunochemilumino-metric
assay (ACS Ciba Corning
Diagnostic Corp, USA)
z122
Sudan/Omdurman Local hospital 76 70d TR-FIA (DELFIA Wallac, Finland)
Turkey/Kayseri Teaching hospital 70 27.1 IRMA (Amersham, UK) 30.2 (
India/West Bengal Local hospital 267 2.9
d
ELISA (Pathozyme Diagnostics, India) 144 (Thailand/Bangkok Neonatal screening
programs
5,114 31e Electro-chemiluminescence immunoassay
(Roche Diagnostics, Germany)
85
a School aged children.b Indirectly quoted data.c and from personal communication.d TSH > 5 mIU/L.e TSH > 11.2 mIU/L.

8/10/2019 Best Practice JCEM Screening Neonatal y usar solamente de TSH.pdf
http://slidepdf.com/reader/full/best-practice-jcem-screening-neonatal-y-usar-solamente-de-tshpdf 7/13
Songkhla, southern Thailand has revealed a negative correlation between neonatal TSH concentrations
and urinary iodine concentrations in their mothers, although it failed to reach a statistical significant
level (r ¼0.10, P ¼ 0.068).41 Studies from Australia and Denmark with mild-to-borderline iodine
deficiency, however, could not find the expected negative correlation between neonatal whole blood
TSH and maternal UIC.42–44
Although WHO recommends that the iodine intake in pregnancy should be increased to 250 mg perday to ensure a corresponding urinary iodine level of 150 mg l1,6 this has been challenged by a recent
Thai study that found a decrease in the median urinary iodine concentration in pregnant women did
not directly impact on the median newborn TSH concentration. Despite that median maternal UIC level
has more than halved in the Dan Sai district, northern Thailand in 2003 compared with 1998
(106 mg l1 from 249 mg l1) and the median maternal UIC in Bangkok was as low as 85 mg l1, there was
no substantial difference in cord blood serum TSH concentrations in the corresponding newborns.22
A number of studies have used measurement of Tg as part of the assessment of neonatal thyroid
function in relation to iodine status. Kung’s study in Hong Kong40 showed there were significant
differences in both neonatal TSH and Tg of babies born to mothers who had UIC <0.44 mmol l1
(50 mg l1) or >0.79 mmol l1 (100 mg l1). Furthermore, in neonates with TSH >16 mIU l1 their Tg
levels were significantly higher than those with TSH levels <16 mIU l1 (32.0 vs. 25.6, P < 0.05). Thestudy in the West Black Sea area of Turkey showed a positive relationship between percentage neonatal
TSH >5 mIU l1 and median Tg (r ¼ 0.51, P < 0.01).36
Mode of delivery
Many studies have explored the impact of delivery characteristics on neonatal TSH levels, partic-
ularly in cord blood. This is most relevant in countries where cord blood, either serum or dried blood
spot, is used for the neonatal thyroid screening. The reports are still controversial. Neonates born with
assisted vaginal delivery, including vacuum or forceps extraction, were reported to have higher TSH
values than those of normal vaginal delivery.45–47 Furthermore, newborns by vaginal delivery had
higher TSH levels compared with babies delivered by caesarean section.45–48 This may relate to stress
associated with vaginal delivery.47
Studies in Japan and Sudan, however, found no difference innewborn TSH levels in relation to vaginal delivery, assisted or non-assisted, or caesarean section, and
they claimed that the TSH was less influenced by perinatal factors. 49,50
An interesting study from Sydney, Australia, described a phenomenon that newborns delivered by
caesarean section were more likely to have TSH levels >5 mIU l1 on day 3 after birth than those born
by vaginal delivery.51 There could be a number of implications of this finding. First, more babies
delivered by caesarean section were born before 37 weeks’ gestation, so their thyroid glands might be
less mature in handling topical iodine used to prepare for the caesarean section. 51 Second, Sydney is
a mild iodine-deficient area.43,52,53 As discussed further in this article, iodine deficiency might exac-
erbate the ability of the thyroid to handle excessive iodine in preterm babies. Third, based on the
guidelines, most reported heel blood samples were collected between day 2 and 4; this phenomenon
could, therefore, have an impact on the results of TSH screening and IDD monitoring. Last, the numberof babies delivered by caesarean section is increasing in many countries, suggesting this should be
taken into consideration in interpreting neonatal TSH results.
Time of sampling: cord blood vs. heel blood taken in the first few days of life
The recommended time of sampling for screening of CH is before day 5 of life. It is most highly
desirable at 48 h to 4 days due to the neonatal TSH surge in the first 24 h after birth.12,54,55 Some
neonatal screening programmes use cord blood samples collected at delivery for convenience or for
better acceptance of the test by parents.40,56 In some countries, both cord blood and heel blood samples
are used to achieve higher coverage.29,57 Another issue has been the early discharge of mothers and
babies within 48 h of birth for various reasons, including cultural practices in some countries where
women return home within 24 h after giving birth.
58,59
Samples collected at different times havepresented a major challenge for setting the appropriate cut-off points for neonatal screening. Evidence
shows that the mean TSH level sampled less than 24 h after birth was significantly higher than the mean
TSH level of neonates after the first 24 h.59,60 This poses an even bigger challenge for monitoring IDD
programmes, as we are looking at a narrowly defined level, that is, <3% of neonates TSH >5 mIU l1.
M. Li, C.J. Eastman / Best Practice & Research Clinical Endocrinology & Metabolism 24 (2010) 63–75 69

8/10/2019 Best Practice JCEM Screening Neonatal y usar solamente de TSH.pdf
http://slidepdf.com/reader/full/best-practice-jcem-screening-neonatal-y-usar-solamente-de-tshpdf 8/13
In a study from the United States, Lott and colleagues60 analysed results from 16144 newborn blood
samples collected between<24 h and>95 h of life in 24-h intervals and found that the mean TSH levels
progressively reduced from 15.20 mIU l1 to 3.24 mIU l1, highlighting the necessity of establishing the
age-dependent cut-off values. Other studies also showed the median TSH levels of samples collected in
the days beyond 48 h after birth were significantly lower than the level in cord blood,34,61 suggested that
it was inappropriate to apply the same cut-off point for samples collected at different time points. This isparticularly important in assessing the iodine-deficiency status when cord blood spot samples are used,
but the same criteria still apply as for blood spot samples collected>48 h after birth. This could lead to
overestimation of the problem if the results were looked at in isolation from other indicators. Using TSH
>5 mIUl1 as the cut-off, Copeland34 found the proportion of TSH concentrations above this cut-off in
dried cord blood varied between 58% in Guatemala and 84% in Bangladesh, which is much higher than
the reported results using dried heel-prick blood spots collected >48 h throughout the world.
Furthermore, there was a marked discrepancy between neonatal TSH and other iodine-deficiency
indicators, namely urinary iodine excretion level and total goitre rates in schoolchildren. For instance, in
Bangladesh, 84% neonates had TSH >5 mIU l1, while median UIC in schoolchildren was 73 mg l1 and
26% of children had enlarged thyroids by ultrasound, indicating mild-to-moderate iodine deficiency. In
Guatemala, the UIC of schoolchildren was in the normal range (181 mg l1) and 15% children hadpalpable goitre, but the proportion of neonatal TSH values >5 mIU l1, however, was as high as 58%.
Maternal or neonatal exposure to iodine-containing antiseptics
Maternal or neonatal exposure to iodine-containing antiseptics is a common cause of transient
hyperthyrotropinaemia and/or hypothyroidism in newborns.11,62–66 Only a few newborn TSH screening
programmes, however, have reported information on maternal or neonatal exposure to iodine-con-
taining antiseptics before or during delivery.24,34,36,67 Copeland34 reported that a very high percentage
(82%) of newborns at the Crawford Long Hospital in Atlanta, Georgia, in the United States, had cord
blood TSH levels above 5 mIU l1. This was partially attributed to maternal exposure to beta-iodine-
containing antiseptics prior to birth, including intravenous infusion, epidural insertion and catheter-
isation. Simsek confirmed that all hospitals in the area of their study used povidone as a local skinantiseptic in mothers or in newborns.36 Telek-Lemanska24 commented that information on the use of
iodine-containing disinfectants was not available. This is likely to be the case for many screening
programmes where the information was either not collected or not well managed and reported.
One study from Poland, in particular, is of interest as it highlights the strong influence of using
iodine-containing antiseptics in obstetric practice on the results of TSH screening.67 Based on a survey,
there were 71% of obstetric clinics in 1998 and 58% in year 2000 in Poland using iodine as a skin
disinfectant. When the neonatal TSH data was examined for the ‘iodine-free hospitals’ and those using
iodine-containing antiseptics separately, the authors found more than a threefold increase in TSH
levels greater than the cut-off (15 mIU l1) in the hospitals using iodine. Many reported cases of
transient perinatal hyperthyrotropinaemia resulting from iodine exposure occurred in countries where
there was mild-to-moderate iodine deficiency.65
A recent study in an iodine-replete area of Iran hasshowed that povidone disinfection at delivery did not affect TSH measurement from cord dried blood
spot or the rate of hyperthyrotropinaemia among mature and normal-birth-weight neonates.48
Instead of exposure to iodine-containing antiseptic products, a study from Denmark44 found 41% of
the neonates whose mothers were exposed to regular daily iodine-containing supplements during
pregnancy had cord blood serum TSH level greater than 10 mIU l1, compared with 31% in the non-
iodine-supplemented control group. The median urinary iodine excretion of mothers (60 mg l1 in I
group vs. 34.5 mg l1 in non-I group) and babies (63 mg l1 in I group vs. 31 mg l1 in non-I group), clearly
indicating that the iodine supplement was inadequate and both mothers and babies in the supple-
mented group were still mildly iodine deficient. The authors have postulated that iodine deficiency
might predispose the foetal and neonatal thyroid gland to the inhibitory effect of an excessive iodine
load on thyroid hormone synthesis, leading to elevated neonatal TSH concentrations.
Type of samples: dried cord blood spot vs. cord blood serum vs. dried heel blood spot
In a small study in Japan, Fuse and colleagues49 found that there was a significant linear correlation of
the TSH concentration in dried cord blood spots and cord venous blood samples in the same neonate,
M. Li, C.J. Eastman / Best Practice & Research Clinical Endocrinology & Metabolism 24 (2010) 63–7570
8/10/2019 Best Practice JCEM Screening Neonatal y usar solamente de TSH.pdf
http://slidepdf.com/reader/full/best-practice-jcem-screening-neonatal-y-usar-solamente-de-tshpdf 9/13
suggesting that the cord blood collected on filter paper might be a feasible alternative for a TSH screening
programme using cord blood. This was supported by a study in southwest China, an iodine-deficient
endemic area.45 The study showed that there was not only a good correlation of TSH levels between the
dried cord blood spots and the cord venous blood samples (r ¼ 0.84, P < 0.01) but also a good correlation
between the dried cord blood and dried heel blood obtained 3–5 days after birth (r ¼0.67, P < 0.01).
In a larger-scale study involving seven provinces in China, it was shown that while the medianurinary iodine excretion level in pregnant women was within the optimal range (246 mg l1), signifi-
cant variations were found in dried cord blood spot TSH levels. Furthermore, the TSH levels were also
significantly affected by the type of delivery.68 The authors concluded that the neonatal dried cord
blood TSH was influenced by many factors; therefore, it was not a suitable indicator for IDDs
surveillance in areas where iodine nutrition was adequate.68 In Thailand, both dried blood spot
collected from 48 h (national programme)37 and cord blood serum (in Ramathibodi Hospital,
Bangkok)22 are used for the neonatal TSH screening. Comparing data from the two programmes, it has
been concluded that the whole blood collected from a heel prick on day 3 was not sensitive enough to
assess the status of iodine nutrition in neonates.22
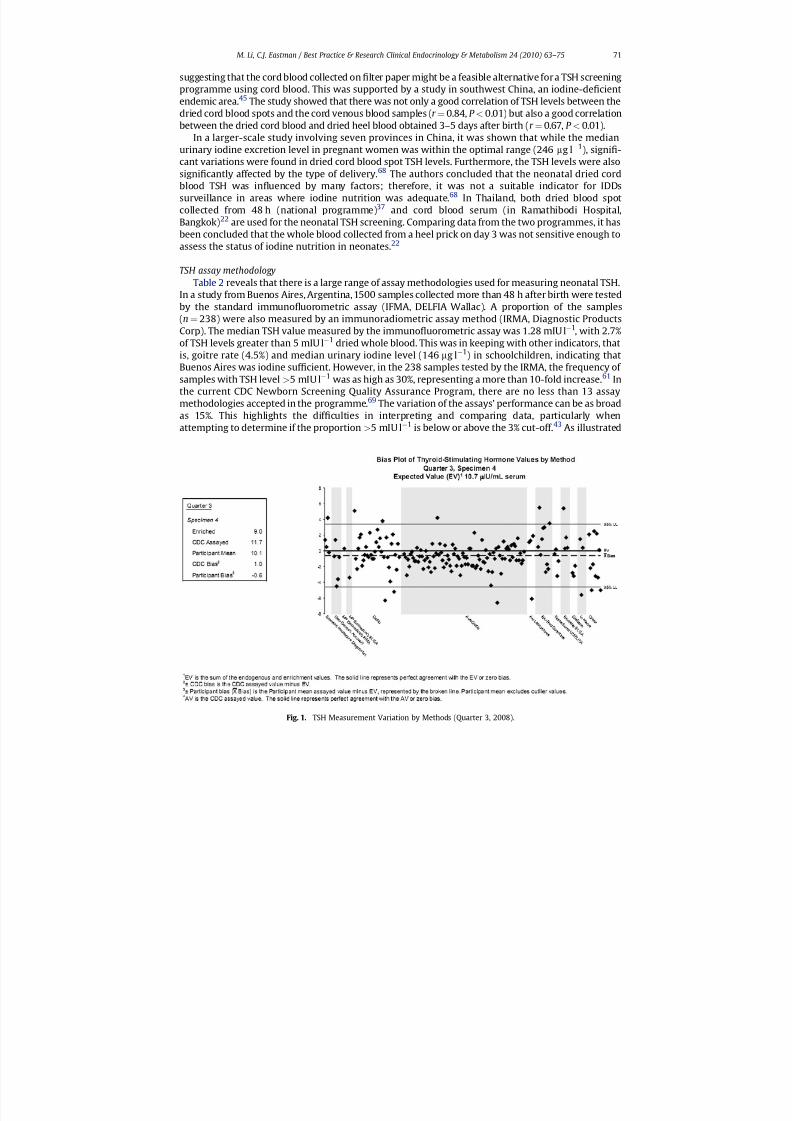
TSH assay methodologyTable 2 reveals that there is a large range of assay methodologies used for measuring neonatal TSH.
In a study from Buenos Aires, Argentina, 1500 samples collected more than 48 h after birth were tested
by the standard immunofluorometric assay (IFMA, DELFIA Wallac). A proportion of the samples
(n¼ 238) were also measured by an immunoradiometric assay method (IRMA, Diagnostic Products
Corp). The median TSH value measured by the immunofluorometric assay was 1.28 mIU l1, with 2.7%
of TSH levels greater than 5 mIU l1 dried whole blood. This was in keeping with other indicators, that
is, goitre rate (4.5%) and median urinary iodine level (146 mg l1) in schoolchildren, indicating that
Buenos Aires was iodine sufficient. However, in the 238 samples tested by the IRMA, the frequency of
samples with TSH level >5 mIU l1 was as high as 30%, representing a more than 10-fold increase.61 In
the current CDC Newborn Screening Quality Assurance Program, there are no less than 13 assay
methodologies accepted in the programme.69
The variation of the assays’ performance can be as broadas 15%. This highlights the difficulties in interpreting and comparing data, particularly when
attempting to determine if the proportion >5 mIU l1 is below or above the 3% cut-off.43 As illustrated
Fig. 1. TSH Measurement Variation by Methods (Quarter 3, 2008).
M. Li, C.J. Eastman / Best Practice & Research Clinical Endocrinology & Metabolism 24 (2010) 63–75 71

8/10/2019 Best Practice JCEM Screening Neonatal y usar solamente de TSH.pdf
http://slidepdf.com/reader/full/best-practice-jcem-screening-neonatal-y-usar-solamente-de-tshpdf 10/13
in Fig. 1, there is a wide range of variation among the assays. More importantly, these assay are
designed to detect CH, which are usually optimised at higher cut-off values (10–20 mIU l1) than
needed for assessing iodine nutritional status (5 mIU l1). This has been demonstrated by Elnagar32
that there was a poor correlation of the TSH levels obtained from serum and dried blood spot below
5 mIU l1 in the DELFIA TSH ultra assay.
In conclusion, despite what is recommended in the WHO/UNICEF/ICCIDD guidelines and someencouraging successes in countries such as Belgium and Switzerland, there are still some serious
technical issues in relation to using the frequency of neonatal TSH values greater than 5 mIU l1 as
a tool for assessing population iodine nutrition status and monitoring iodine deficiency control pro-
grammes confidently. To establish valid guidelines for neonatal TSH screening in these situations, more
research is required with adherence to standardised protocols to minimise the large number of
variables that can influence the neonatal TSH concentration.
References
*1. Zimmermann MB, Jooste PL & Pandav CS. Iodine deficiency disorders. Lancet 2008; 372: 1251–1262.2. Andersson M, Takkouche B, Ines Egli I et al. Current global iodine status and progress over the last decade towards the
elimination of iodine deficiency. Bulletin of the World Health Organisation 2005; 83: 518–525.3. The United Nations Children’s Fund. Sustainable elimination of iodine deficiency. New York: UNICEF, 2008.4. Glinoer D. The importance of iodine nutrition during pregnancy. Public Health Nutrition 2007; 10: 1542–1546.
Practice points
The neonatal TSH should only be used as one of the indicators for assessing the status of iodine nutrition in a population if the screening system is robust, adheres to a strict protocol
with strict quality assurance and the data is routinely collected for the primary purpose of
screening for CH.
Neonatal TSH should not be used as the sole indicator for monitoring iodine deficiency
control programs, especially when samples are collected less than 48 hours after birth, as
there are no established reference intervals.
The current WHO/UNICEF/ICCIDD criteria for iodine deficiency, i.e. >3% of neonatal TSH
greater than 5 mIU/L, does not specify assay methods when this should be an essential
requirement. Marked variation in assay results question the validity of these data. It is
important to bear this in mind when interpreting or comparing neonatal TSH results by
different methods.
The continuing decline of iodine intake in many developed countries warrants closer
monitoring of the subtle increases in neonatal TSH levels, even when the proportion of TSH
>5 mIU/L that may be less than 3%.
It appears that the neonatal TSH measurement may not be a reliable monitoring tool for
iodine deficiency control programs due to the many potential confounding factors which may
discredit the data and its interpretation. WHO should reconsider their published guidelines
until these issues have been resolved.
Research agenda
Continuing research is necessary to explore sensitive and reliable indicators for assessing
mild to moderate iodine deficiency conditions and monitoring intervention programs.
Further research is required to establish the recommended cut off levels for using mixed
dried cord blood spot samples, as they are used in many countries where heel prick blood
sample collection is not possible.
Research is needed to quantify the variations among different assay methods in order to
guide the interpretation and comparison of the neonatal TSH data.
M. Li, C.J. Eastman / Best Practice & Research Clinical Endocrinology & Metabolism 24 (2010) 63–7572
8/10/2019 Best Practice JCEM Screening Neonatal y usar solamente de TSH.pdf
http://slidepdf.com/reader/full/best-practice-jcem-screening-neonatal-y-usar-solamente-de-tshpdf 11/13
5. Untoro J, Mangasaryan N, de Benoist B et al. Reaching optimal iodine nutrition in pregnant and lactating women andyoung children: programmatic recommendations. Public Health Nutrition 2007; 10: 1527–1529.
*6. WHO Assessment of iodine deficiency disorders and monitoring their elimination: a guide for programme managers. 3rd ed.Geneva: WHO, 2007. Available from: http://whqlibdoc.who.int/publications/2007/9789241595827_eng.pdf .
7. Morreale de Escobar G, Obregon MJ & Escobar del Rey F. Is neuropsychological development related to maternal hypo-thyrodism, or maternal hypothyroxinemia? Journal of Clinical Endocrinology and Metabolism 2000; 85: 3975–3987.
8. Morreale de Escobar G, Obregon MJ & Escobar del Rey F. Role of thyroid hormone during early brain development.European Journal of Endocrinology 2004; 151: U25–U37.9. Delange F. The disorders induced by iodine deficiency. Thyroid 1994; 4: 107–128.
10. Delange F, Dalhem A, Bourdoux P et al. Increased risk of primary hypothyroidism in preterm infants. Journal of Pediatrics
1984; 105: 462–469.*11. Delange F. Neonatal screening for congenital hypothyroidism: results and perspectives. Hormone Research 1997; 48:
51–61.12. American Academy of Pediatrics, Rose SR, Section on Endocrinology and Committee on Genetics, American Thyroid
Association, Brown RS, Public Health Committee, Lawson Wilkins Pediatric Endocrine Society, Foley T, Kaplowitz PB, KayeCI et al. Update of newborn screening and therapy for congenital hypothyroidism. Pediatrics 2006; 117: 2290–2303.
13. Dussault JH. The anecdotal history of screening for congenital hypothyroidism. Journal of Clinical Endocrinology andMetabolism 1999; 84: 4332–4334.
14. WHO Indicators for assessing iodine deficiency disorders and their control through salt iodisation. Geneva: WHO, 1994. WHO/NUT/94.6.
15. WHO Assessment of iodine deficiency disorders and monitoring for their elimination – a guide for program managers . 2nd ed.
Geneva: WHO, 2001. Available from: http://www.who.int/nutrition/publications/en/idd_assessment_monitoring_elimination.pdf .
*16. Zimmermann MB, Aeberli I, Toni Torresani T et al. Increasing the iodine concentration in the Swiss iodized salt programmarkedly improved iodine status in pregnant women and children: a 5-y prospective national study. American Journal of Clinical Nutrition 2005; 82: 388–392.
17. Thilly CH, Delange F, Lagasse R et al. Fetal hypothyroidism and maternal thyroid status in severe endemic goitre. Journal of Clinical Endocrinology and Metabolism 1978; 47: 354–360.
18. Delange F, Iteke FB & Ermans AM. Nutritional factors involved in the goitrogenic action of cassava . Canada: InternationalDevelopment Research Centre, 1982. 1–100.
19. Kochupillai N, Pandav CS, Godbole MM et al. Iodine deficiency and neonatal hypothyroidism. Bulletin of the World HealthOrganisation 1986; 64: 547–551.
*20. Delange F. Screening for congenital hypothyroidism used as an indicator of the degree of iodine deficiency and of itscontrol. Thyroid 1998; 8: 1185–1192.
21. Delange F. Neonatal thyroid screening as a monitoring tool for the control of iodine deficiency. Acta Paediatrics Supplement 1999; 88: 21–24.
*22. Rajatanavin R. Iodine deficiency in pregnant women and neonates in Thailand. Public Health Nutrition 2007; 10: 1602–1605.
*23. Burns R, Mayne PD, O’Herlihy C et al. Can neonatal TSH screening reflect trends in population iodine intake? Thyroid 2008;18: 883–888.
24. Tylek-Lemanska D, Rybakowa M, Kumorowicz-Kopiec M et al. Iodine deficiency disorders incidence in neonates based onthe experience with mass screening for congenital hypothyroidism in southeast Poland in the years 1985–2000. Journal of
Endocrinological Investigation 2003; 26(Suppl. 2): 32–38.25. Wa chter W, Mvungi MG, Triebel E et al. Iodine deficiency, hypothyroidism, and endemic goitre in southern Tanzania. A
survey showing the positive effects of iodised oil injections by TSH determination in dried blood spots. Journal of Epidemiology and Community Health 1985; 39: 263–270.
26. Carta Sorcini M, Diodato A, Fazzini C et al. Influence of environmental iodine deficiency on neonatal thyroid screeningresults. Journal of Endocrinological Investigation 1988; 11: 309–312.
27. Delange F, Bourdoux P, Laurence M et al. Neonatal thyroid function in iodine deficiency. In: Delange F, Dunn J & Glinoer D(eds.). Iodine deficiency in Europe: a continuing concern. New York: Plenum Publishing, 1993, pp. 199–209.
28. Nordenberg D, Sullivan K, Maberly G et al. Congenital hypothyroid screening programs and the sensitive thyrotropinassay: strategies for the surveillance of iodine deficiency disorders. In: Delange F, Dunn J & Glinoer D (eds.). Iodine defi-ciency in Europe: a continuing concern. New York: Plenum Publishing, 1993, pp. 211–217.
29. Rajatanavin R, Unachak K, Winichakoon P et al. Neonatal thyrotropin profile as an index for severity of iodine deficiencyand surveillance of iodine prophylactic program. Thyroid 1997; 7: 599–604.
30. Sullivan KM, May W, Nordenberg D et al. Use of thyroid stimulating hormone testing in newborns to identify iodinedeficiency. Journal of Nutrition 1997; 127: 55–58.
*31. Costante G, Grasso L, Ludovico O et al. The statistical analysis of neonatal TSH results from congenital hypothyroidismscreening programs provides a useful tool for the characterization of moderate iodine deficiency regions. Journal of Endocrinological Investigation 1997; 20: 251–256.
32. Elnagar B, Gebre-Medhin M, Larsson A et al. Iodine nutrition in Sudan: determination of thyroid-stimulating hormone infilter paper blood samples. Scandinavian Journal of Clinical Laboratory Investigation 1997; 57: 175–181.
33. Mikelsaar RV & Viikmaa M. Neonatal thyroid-stimulating hormone screening as an indirect method for the assessment of iodine deficiency in Estonia. Hormone Research 1999; 52: 284–286.
34. Copeland DL, Sullivan KM, Houston R et al. Comparison of neonatal thyroid-stimulating hormone levels and indicators of
iodine deficiency in schoolchildren. Public Health Nutrition 2002; 5: 81–87.35. Kurtoglu S, Akcakus M, Kocaoglu C et al. Iodine status remains critical in mother and infant in Central Anatolia (Kayseri) of
Turkey. European Journal of Nutrition 2004; 43: 297–303.36. Simsek E, Karabay M & Kocabay K. Neonatal screening for congenital hypothyroidism in West Black Sea area, Turkey.
International Journal of Clinical Practice 2005; 59: 336–341.
M. Li, C.J. Eastman / Best Practice & Research Clinical Endocrinology & Metabolism 24 (2010) 63–75 73

8/10/2019 Best Practice JCEM Screening Neonatal y usar solamente de TSH.pdf
http://slidepdf.com/reader/full/best-practice-jcem-screening-neonatal-y-usar-solamente-de-tshpdf 12/13
37. Charoensiriwatana W, Srijantr P, Janejai N et al. Application of geographic information system in TSH neonatal screeningfor monitoring of iodine deficiency areas in Thailand. Southeast Asian Journal of Tropical Medicine and Public Health 2008;39: 362–367.
*38. Glinoer D. The regulation of thyroid function during normal pregnancy: importance of the iodine nutrition status. Best Practice & Research Clinical Endocrinology & Metabolism 2004; 18: 133–152.
39. Ojule AC & Osotimehin BO. Maternal and neonatal thyroid status in Saki, Nigeria. African Journal of Medicine and Medical
Sciences 1998; 27: 57–61.40. Kung AW, Lao TT, Low LC et al. Iodine insufficiency and neonatal hyperthyrotropinaemia in Hong Kong. Clinical Endo-
crinology (Oxford) 1997; 46: 315–319.41. Jaruratanasirikul S, Sangsupawanich P, Koranantakul O et al. Maternal iodine status and neonatal thyroid-stimulating
hormone concentration: a community survey in Songkhla, southern Thailand. Public Health Nutrition 2009; doi:10.1017/S1368980009005205.
42. Travers CA, Guttikonda K, Norton CA et al. Iodine status in pregnant women and their newborns: are our babies at risk of iodine deficiency? Medical Journal of Australia 2006; 184: 617–620.
43. McElduff A, McElduff P, Gunton JE et al. Neonatal thyroid-stimulating hormone concentrations in northern Sydney:further indications of mild iodine deficiency? Medical Journal of Australia 2002; 176: 317–320.
44. Nøhr SB & Laurberg P. Opposite variations in maternal and neonatal thyroid function induced by iodine supplementationduring pregnancy. Journal of Clinical Endocrinology and Metabolism 2000; 85: 623–627.
45. Shi LX, Ma QL & Zhang JX. Influence of perinatal factors and sampling methods on thyroid stimulating hormone andthyroid hormone levels in cord blood. Zhonghua Fu Chan Ke Za Zhi 1994; 29: 714–716 [Article in Chinese].
46. Rashmi Seth A, Sekhri T et al. Effect of perinatal factors on cord blood thyroid stimulating hormone levels. Journal of
Pediatric Endocrinology and Metabolism 2007; 20: 59–64.47. Herbstman J, Apelberg BJ, Witter FR et al. Maternal, infant, and delivery factors associated with neonatal thyroid hormone
status. Thyroid 2008; 18: 67–76.48. Ordookhani A, Pearce EN, Mirmiran P et al. The effect of type of delivery and povidone-iodine application at delivery on
cord dried-blood-specimen thyrotropin level and the rate of hyperthyrotropinemia in mature and normal-birth-weightneonates residing in an iodine-replete area: report of Tehran Province, 1998–2005. Thyroid 2007; 17: 1097–1102.
49. Fuse Y, Wakae E, Nemoto Y et al. Influence of perinatal factors and sampling methods on TSH and thyroid hormone levelsin cord blood. Endocrinologia Japonica 1991; 38: 297–302.
50. Eltom A, Eltom M, Idris M et al. Thyroid function in the newborn in relation to maternal thyroid status during labour ina mild iodine deficiency endemic area in Sudan. Clinical Endocrinology (Oxford) 2001; 55: 485–490.
51. McElduff A, McElduff P, Wiley V et al. Neonatal thyrotropin as measured in a congenital hypothyroidism screeningprogram: influence of the mode of delivery. Journal of Clinical Endocrinology and Metabolism 2005; 90: 6361–6363.
52. Gunton JE, Hams G, Fiegert M et al. Iodine deficiency in ambulatory participants at a Sydney teaching hospital: is Australiatruly iodine replete? Medical Journal of Australia 1999; 171: 467–470.
53. Li M, Ma G, Boyages SC et al. Re-emergence of iodine deficiency in Australia. Asia Pacific Journal of Clinical Nutrition 2001;10: 200–203.
54. Working Group on Neonatal Screening of the European Society for Paediatric Endocrinology. Revised guidelines forneonatal screening programmes for primary congenital hypothyroidism. Hormone Research 1999; 52: 49–52.
55. American Academy of Pediatrics Section on Endocrinology and Committee on Genetics & American Thyroid AssociationCommittee on Public Health. Newborn screening for congenital hypothyroidism: recommended guidelines. Pediatrics1993; 91: 1203–1209.
56. Ogunkeye OO, Roluga AI & Khan FA. Resetting the detection level of cord blood thyroid stimulating hormone (TSH) for thediagnosis of congenital hypothyroidism. Journal of Tropical Pediatrics 2008; 54: 74–77.
57. Vela M, Gamboa S, Loera-Luna A et al. Neonatal screening for congenital hypothyroidism in Mexico: experience, obstacles,and strategies. Journal of Medical Screening 1999; 6: 77–79.
58. Elbualy M, Bold A, De Silva V et al. Congenital hypothyroid screening: the Oman experience. Journal of Tropical Pediatrics1998; 4 4: 81–83.
59. Feleke Y, Enquoselassie F, Deneke F et al. Neonatal congenital hypothyroidism screening in Addis Ababa, Ethiopia. Eastern
African Medical Journal 2000; 77: 377–381.
60. Lott JA, Sardovia-Iyer M, Speakman KS et al. Age-dependent cutoff values in screening newborns for hypothyroidism.Clinical Biochemistry 2004; 37: 791–797.*61. Grun eiro-Papendieck L, Chiesa A, Mendez V et al. Neonatal TSH levels as an index of iodine sufficiency: differences related
to time of screening sampling and methodology. Hormone Research 2004; 62: 272–276.62. Theodoropoulos T, Braverman LE & Vagenakis AG. Iodide-induced hypothyroidism: a potential hazard during perinatal
life. Science 1979; 205: 502–503.63. Fisher DA & Klein AH. Thyroid development and disorders of thyroid function in the newborn. New England Journal of
Medicine 1981; 304: 702–712.64. Gru ters A, l’Allemand D, Heidemann PH et al. Incidence of iodine contamination in neonatal transient hyper-
thyrotropinemia. European Journal of Pediatrics 1983; 140: 299–300.65. Robuschi G, Montermini M, Alboni A et al. Cord blood iodothyronine and thyrotropin concentrations in newborns of
mothers exposed to povidone iodine in the last trimester. Journal of Endocrinological Investigation 1987; 10:183–186.
66. Novaes Junior M, Biancalana MM, Garcia SA et al. Elevation of cord blood TSH concentration in newborn infants of mothers exposed to acute povidone iodine during delivery. Journal of Endocrinological Investigation 1994; 17:
805–808.67. O1tarzewski M & Szymborski J. Neonatal hypothyroid screening in monitoring of iodine deficiency and iodine supple-
mentation in Poland. Journal of Endocrinological Investigation 2003; 26(Suppl. 2): 27–31.68. Dong H & Zheng Q. Study on the neonate umbilical cord blood thyroid stimulating hormone level in the universal iodized
salt areas and its application. Zhonghua Liu Xing Bing Xue Za Zhi 2002; 23: 250–253 [article in Chinese].
M. Li, C.J. Eastman / Best Practice & Research Clinical Endocrinology & Metabolism 24 (2010) 63–7574

8/10/2019 Best Practice JCEM Screening Neonatal y usar solamente de TSH.pdf
http://slidepdf.com/reader/full/best-practice-jcem-screening-neonatal-y-usar-solamente-de-tshpdf 13/13
69. Department of Health and Human Services & Centre for Disease Prevention and Control. Newborn Screening QualityAssurance Program 2008 Annual Summary Report. Available from: http://www.cdc.gov/labstandards/pdf/nsqap/nsqap_summaryreport_2009.pdf ; January 2009.
70. Chakraborty I, Chatterjee S, Bhadra D et al. Iodine deficiency disorders among the pregnant women in a rural hospital of West Bengal. Indian Journal of Medical Research 2006; 123: 825–829.
M. Li, C.J. Eastman / Best Practice & Research Clinical Endocrinology & Metabolism 24 (2010) 63–75 75