Benign and Malignant
8
Sacrococcygeal teratomas are impor tant tumors of early infancy and child hood. In order to clarify some of the problems which are regularly encoun tered in the diagnosis and treatment of these tumors, our experience with 49 sacrococcygeal teratomas has been com pared with a review of 54 cases from the literature. Clinical features which differentiate the malignant from the benign teratomas have been found to relate closely to the age of the patient at the time of discovery of the tumor and to the presence or absence of the symptoms of bowel or bladder obstruc tion. The surgical procedures necessary for the removal of the benign tera tomas, the use of combination methods for treatment of the malignant tumors, and the prognosis for cure in both groups of tumors are outlined in this report. Presenting Symptoms Contrary to what might be expected, the majority of benign sacrococcygeal teratomas produce no functional diffi culties even when there is a consider able intrapelvic extension. Progressive growth filling the whole pelvis may cause mild obstructive symptoms, but when the obstruction is severe, the tu Dr. Donnellan is Attending Surgeon, The Chil dren's Memorial Hospital, and Assistant Professor of Surgery, Northwestern University Medical School, Chicago, Illinois. Dr. Swenson is Surgeon-in-Chief, The Children's Memorial Hospital, and Professor of Surgery. Northwestern University Medical School. Abridged and reprinted from SURGERY: 64: 834- 846, 1968. mor is usually malignant, involving the presacral nerve plexuses and the viscer al walls. Bowel or bladder dysfunction, pain on defecation, discomfort during standing, and particularly the presence of vascular or lymphatic obstruction all suggest the diagnosis of malignancy (Table 1). In the group of 30 malignant tumors, 24 produced bowel or bladder dysfunc tion or both together. Of the 73 benign teratomas, only 5 had produced such symptoms. While it may be argued that the majority of the tumors are removed in infancy before the obstruction be comes severe, we have been impressed with the paucity of symptoms of the benign teratomas even when they are very bulky. By contrast, one of the infants with a relatively small malig nant growth was born with marked pitting edema of the leg and rectal ob struction resulting from pelvic inva sion. (Fig. 1.) Fig. 1. Malignant sacrococcygeal teratoma in newborn infant. Note pouting of anus and swelling of right leg. 344 Benign and Malignant Sacrococcygeal Teratomas William L. Donnellan, M.D., and Orvar Swenson, M.D.
-
Upload
bembie-purwono -
Category
Documents
-
view
36 -
download
3
Transcript of Benign and Malignant

Sacrococcygeal teratomas are important tumors of early infancy and childhood. In order to clarify some of theproblems which are regularly encountered in the diagnosis and treatment ofthese tumors, our experience with 49sacrococcygeal teratomas has been compared with a review of 54 cases fromthe literature. Clinical features whichdifferentiate the malignant from thebenign teratomas have been found torelate closely to the age of the patientat the time of discovery of the tumorand to the presence or absence of thesymptoms of bowel or bladder obstruction. The surgical procedures necessaryfor the removal of the benign teratomas, the use of combination methodsfor treatment of the malignant tumors,and the prognosis for cure in bothgroups of tumors are outlined in thisreport.
Presenting SymptomsContrary to what might be expected,
the majority of benign sacrococcygealteratomas produce no functional difficulties even when there is a considerable intrapelvic extension. Progressivegrowth filling the whole pelvis maycause mild obstructive symptoms, butwhen the obstruction is severe, the tu
Dr. Donnellan is Attending Surgeon, The Children's Memorial Hospital, and Assistant Professorof Surgery, Northwestern University MedicalSchool, Chicago, Illinois.
Dr. Swenson is Surgeon-in-Chief, The Children'sMemorial Hospital, and Professor of Surgery.Northwestern University Medical School.
Abridged and reprinted from SURGERY: 64: 834-846, 1968.
mor is usually malignant, involving thepresacral nerve plexuses and the visceral walls. Bowel or bladder dysfunction,pain on defecation, discomfort duringstanding, and particularly the presenceof vascular or lymphatic obstruction allsuggest the diagnosis of malignancy(Table 1).
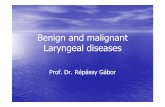
In the group of 30 malignant tumors,24 produced bowel or bladder dysfunction or both together. Of the 73 benignteratomas, only 5 had produced suchsymptoms. While it may be argued thatthe majority of the tumors are removedin infancy before the obstruction becomes severe, we have been impressedwith the paucity of symptoms of thebenign teratomas even when they arevery bulky. By contrast, one of theinfants with a relatively small malignant growth was born with markedpitting edema of the leg and rectal obstruction resulting from pelvic invasion. (Fig. 1.)
Fig. 1. Malignant sacrococcygeal teratoma innewborn infant. Note pouting of anus andswelling of right leg.
344
Benign and MalignantSacrococcygeal Teratomas
William L. Donnellan, M.D.,and Orvar Swenson, M.D.

MalignantPresenceofmassBenign(percent)TotalBirth
to 2 months718(10.1)79After
2 months.. ++222 (91.7)24
TABLE 1—SYMPTOMSPRODUCED BY SACROCOCCYGEALTERATOMAS
Malignant(30 cases)
915
24
11
4
6
Benign
Symptoms (73 cases)
Pelvic obstruction
Bowel obstruction + 1
Bowel and bladder 4
Total 5
Pain 2*
Circulatory obstruction —¿�
Inguinal lymph node metastases —¿�
* Pain associated with infection and abscess formation in bofh cases.
TABLE2—INCIDENCEOF MALIGNANCY BY AGE AT DISCOVERYOF THE TUMOR
Malignancy and Age of DiscoveryThe age of the patient at first dis
covery of the tumor provides a goodpreliminary differentiation between thebenign and malignant teratomas. Of79 teratomas presenting as a mass atbirth, 8 were malignant or later becamemalignant, an incidence of 10.1 percent. In tumors discovered after theage of 2 months, 22 out of 24 weremalignant, an incidence of 91.7 percent.
Table 2 indicates the time of appearance of the benign and malignant teratomas. We have chosen to separate thegroups into those tumors discoveredafter the age of two months and thosewhich were evident before that time.
Although figures for malignancy aslow as 9 percent and as high as 41.8percent have been presented, most authors agree that about one third ofsacrococcygeal teratomas are malignant.'2 In the present series, 30 of the103 tumors were malignant. This incidence of 29.1 percent malignancy isbased on actual infiltrative extension ordistant metastases, and not upon thediagnosis of “¿�potentialmalignancy―derived from histological findings ofhighly primitive tissues.
Although it is frequently stated thatsacrococcygeal teratomas should be removed as early as possible in infancyin order to forestall their malignant
345

Type of tumor No. ofcasesPercentBenign
1866.7Malignant9*33.3Total
27100.0*
Five of these showed no progression until the developmentofobvious
malignancy.TABLE
4—RELATIONSHIPOF MALIGNANCY TOAGEANDSEXAge
MaleFemaleDiscovered
atbirthBenign1952Malignant
55Discovered
after 2monthsBenign
02Malignant
1010
TABLE3—INCIDENCEOF MALIGNANCY IN TUMORS PRESENTAT BIRTH ANDOPERATEDAFTERTHE AGE OF 4 MONTHS
transformation, this occurrence is notcommon.' In the corribined group ofcases, 27 teratomas were discovered atbirth but were not operated upon untilafter the age of 4 months. Eighteen(66.7 percent) of these remained benign, and 9 (33.3 percent) were malignant. Only 4 tumors which were judgedto be benign at birth on the basis oftheir size and appearance were subsequently found to be malignant, an incidence of 15 percent in late-operatedcases. (Table 3.)
Sex RatioAs noted by others, the benign tera
tomas occur in females in a ratio of 4to 1. The malignant tumors show nosuch predilection for the female. Fifteen of the patients with malignantteratomas were males, and fifteen werefemales. These figures become moresignificant when they are related to theage at which the tumor was discovered.A moderate-sized or bulky tumor whichis present at birth in a female child,and which has caused no obstructivesymptoms, is almost certainly benign.It will be cured by adequate removal,
@a,.pdif it is left alone the likelihood1!iat it will become malignant is notgreat. (Table 4.)
Pathology of SacrococcygealTeratomas
GROSS APPEARANCE. Benign sacro
coccygeal teratomas present as tumormasses which may be external to thepelvic cavity or wholly within the presacral space. Usually, however, theyshow a combination of both types ofgrowth. They are all closely associatedwith the coccyx and lower sacrum, andmust be regarded as lying above orwithin the origin of the levator animuscles. A few tumors will grow outward and come to hang on a pedicle.Five of the cases showed such an appearance, and all were benign andhighly organized. The malignant tumors, on the other hand, are primarilyintrapelvic. When both internal andexternal growth occur, the presacral orpelvic component usually progressesthrough the posterior portion of thelevator ani muscle in a dumbbellfashion. This probability must be bornein mind during operative treatment of
346

adherent to surrounding structures. Inmany of the tumors, large cysts containing cloudy fluid are seen to alternate with areas of a mushy or rubberyconsistency throughout which myriadsof smaller cysts are visible.
The malignant teratomas are generally firm to hard in consistency, thoughthis alone will not distinguish themfrom benign teratomas. Infrequentlythe malignant component lies in theintrapelvic portion of a benign cysticteratoma, and only the presence offirmer masses about the anus and lowerrectum suggests the diagnosis of malignancy. When there are inguinal nodemetastases, malignancy is obvious. Fiveof the 30 malignant teratomas had developed distant metastases to lung,liver, brain, bone, and other sites atthe time of death, and 29 were locallyinvasive at the time of operation. Inonly 2 of the malignant tumors wascomplete excision thought to have beenaccomplished. All the rest involved pelvic structures to such an extent thattheir removal was judged impossible,and only a biopsy could be done.
MICROSCOPIC PATHOLOGY. The benign
sacrococcygeal teratomas may be divided into two classes. The most frequent is the “¿�adult―type, in whichtissue masses markedly similar to thoseof normal structures may be seen. Thecommon tissues are those of the respiratory, gastrointestinal, and nervoussystems, but structures which mimicany organ of the normal body may befound. In the most mature teratomas,ciliated bronchial epithelium and submucosa are surrounded by smoothmuscle and cartilage, contain normalgoblet cells, and may be found in thevicinity of pulmonary alveoli. The gastrointestinal elements are often madeup of small bowel or colonic mucosawith a surrounding musculature and anormal complement of argentaffine cells.It is not unusual to find well-developedsympathetic ganglia and autonomic
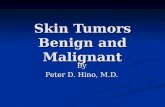
Fig. 2. Cut surface of a typical benign sacro@coccygeal teratoma.
sacrococcygeab teratomas.The external surface of the growth
is usually smooth, the result of stretching of the gluteal muscles and skin overits cystic masses. Not infrequently theskin is hemangiomatous and discolored.Less frequently there is considerableulceration and infection of the surfaceof the tumor. When ulceration occursin association with a hemangiomatouscomponent, severe bleeding may resultwhich places the baby in jeopardy. Ifthere is a large intrapelvic extension,the anus is displaced forward and isdistorted. The perineum is stretchedout over the mass and bulges downward. Sometimes only one buttock isenlarged, the tumor having extendedlaterally over the iliac wing and underthe gluteus muscles. In such cases, ithas often grown through the lessersciatic notch, and there is a large intrapelvic component. If inflammation occurs within such an intrapelvic teratoma, the tumor may be firmly adherent to the rectum and the walls of thepelvis.
The cut surface of the benign sacrococcygeal teratoma has a variegatedcombination of solid and cystic areas.(Fig. 2.) There is usually a well-defined fibrous capsule, though it may be
347

—¿�@ @s4•@@
I,, n.t:@_@
ganglion cells scattered throughout thetumor. “¿�Brain―tissue is frequent, butBetz cells appear never to be present.We have not found them in any of the22 cases available to us for study andhave not encountered any such a description in the literature. (Fig. 3.)
In more primitive teratomas the capabilities for near-normal organizationare largely absent, and various tissuesare seen to form structures which areonly vaguely related to normal bodycomponents. Cystic and glandular ele
-\@@
@ —¿�_i.
@@ .--.T,-:
@V@@;:@
F@1'
Si' @--@
rt—@r' 14@
:@ ‘¿�s-.. ‘¿�@N@lhi@
@•¿�@@
..@ ç@@Sb
,@
/1'@'

TABLE5—TYPESOF MALIGNANT ELEMENTSIN 30 CASES
Type No. of cases
Total carcinoma . 22
Adenocarcinoma
Papillary adenocarcinoma ‘¿�‘¿� . ‘¿�
Undifferentiated carcinoma
Embryonal or undifferentiated sarcoma
Rhabdomyosarcoma
Hemangioendothelioma
Type not stated . , 2
9
74
32
ments may be present, but they arenot surrounded by submucosal andmuscular coats, and their organ patterns are not well differentiated. Forexample, a single layer of cells maymimic the respiratory mucosa, but thenormal muscular coat and cartilage areabsent.
The stroma of the sacrococcygeabteratomas is composed of well-developedfibrous tissue or of a gelatinous myxomatous material in which steblate cellslie in a basophibic matrix. This latter issometimes differentiated into cartilaginous masses with a more eosinophibicmatric containing swollen cartilagecells. There appears to be no prognosticsignificance to the presence of any ofthese different types of stroma, andoften they are admixed; calcificationwithin the teratomata likewise has noprognostic implications.
Whether or not fully formed organsare present within the sacrococcygeabteratomas is disputed.' Our own material does not contain any sacrococcygeal tumor with webb-developed organformation, but in the reports from theliterature the presence of “¿�30cm. ofnormal intestine,― of limb components,and of well-formed teeth have beendocumented.5' In these tumors, thepresence of other abortive structurestypical of the teratomata confirms thediagnosis.
The most frequent type of malignancy is an adenocarcinoma. (Fig. 4.)The terminology varies with different
authors, but 10 of the 30 malignanttumors were described as adenocarcinomas, and 8 contained papillary elements. Other malignant teratomas wereclassified as embryonal carcinomas,embryonal sarcomas, “¿�teratocarcinoma,― rhabdomyosarcoma, undifferentiated sarcoma, and hemangioendothelioma. Whether or not all of these weretruly teratomatous in nature may bedisputed, as in some cases only one ortwo cystic elements were identified inthe histologic preparations. (Table 5.)
Different Diagnosis ofSacrococcygealMasses
The sacrococcygeal region is the seatof frequent developmental anomaliesand persistent embryonic rests. Tumorformation arises as a result of boththese circumstances. A report from theMayo Clinic in 1953 has detailed thedifferential diagnosis of presacraltumor formation in an analysis of 161cases.' The tumors may be of congenital, inflammatory, neurogenic, osseous,and miscellaneous origin. They includeteratomas and dermoid cysts, chordomas, ependymomas, anterior spina bifida with myebomeningocele, lipomataassociated with meningocebes, giantcell tumors of the sacrum, sarcomas ofvarious types, mucoid carcinomas, angiomas, and rarely, coccygeal gliomas.Perirectal abscesses must also be included in the differential diagnosis,since infection of the cystic or malignant tumor may closely mimic this condition.
349

In infants and children the list ofsacrococcygeal growths may be reducedconsiderably. The sacrococcygeal teratomas are the most frequent tumors inthe caudal region, followed by dermoidcysts, anterior myelomeningoceles, Iipomas, perirectal abscesses, sarcomas,and angiomas. We believe, with Gross,that nearly all of the true tumors ininfancy should be included in the teratoma group, for their treatment issimilar, and it is possible to demonstrate tissues of all three germ layersin almost all of them.' The rare growthswhich arise in the postanal gut andrelated embryonic rests, the so-calledenterocystomas, are usually cystic andgrossly identical to the true teratomasand appear to have similar malignantpotentialities.'
Prognosisand TreatmentTHE BENIGN TERATOMAS. In the pres
ent combined series, there were no recurrences in 51 cases in which the removal of a benign sacrococcygealteratoma was thought to have beencomplete, and in which the coccyx wasexcised. Benson has discussed a case ofmalignant recurrence one year afterapparently complete removal of a benign teratoma, and it is possible thatsmall anterior extensions of these tumors may become malignant.―' In oneof the cases from the literature, a solidportion of tumor was found to be malignant anteriorly while the remainderwas typically benign.'1
With any tumor mass about thebuttocks, no matter how small it mayappear to be, the probability of deepextension must be borne in mind.
The important principles of the operative approach are the placing of theincision, the preservation of the attenuated gluteus muscles in their bowerhalf, careful exploration of the presacrab space, and repair of the normalanorectal anatomy after the tumor hasbeen removed. Removal of the coccyxis of course essential since the tera
toma is intimately associated with itsanterior surface in nearly every case.
Roentgen therapy in the benign teratomas is not only useless, but it mayresult in death. One patient in theseries was treated with X-ray therapypostoperatively and died 3 months lateras the result of infection and necrosisof the perineab region. Malignancy wasnoted in one case 10 months after preoperative X-ray therapy of a barge benign tumor. Since the possibility of theinduction of malignancy in unstabletissues by X-irradiation cannot be discounted entirely, this form of treatment of benign teratomas should bediscouraged.
THE MALIGNANT TERATOMAS. Treat
ment of the malignant sacrococcygeabteratomas is a formidable undertaking.Our records show only one cure. Thiswas accomplished by simple excision ofthe coccyx together with a 3 cm. rhabdomyosarcoma containing teratomatouselements. Goodman has reported “¿�control―of a malignant sacrococcygeal teratoma with pulmonary metastases bycombined X-ray, surgical, and chemotherapeutic attacks. His patient, a 16-month-old girl, died 13 months afterthe beginning of therapy.1' In most ofthe cases of sacrococcygeal malignancydeath occurs within one year of discovery of the tumor.
DiscussionSince the classic report of Gross and
his associates in 1951, the sacrococcygeab teratomas and their clinical features have been increasingly well recognized.― The markedly poorer prognosis of teratomas discovered after theage of three months was emphasized,and it was noted that the smaller tumors often show a greater likelihood ofmalignancy than do the barge bulky tumors. Of 29 operated tumors whichwere discovered at birth in their series,only 2 subsequently recurred with metastases, an incidence of 6.9 percent.This figure is similar to our findings
350

in the 78 patients in whom a sacrococcygeal mass was discovered at birth.*Of these, 7 developed malignancy, anincidence of 9 percent. When the criteria for the presence of a benign teratoma were applied, however, only 6percent of patients developed malignancy even though operation was delayed beyond 4 months.
It appears clear that when facilitiesare available for the safe excision of asacrococcygeal teratoma in a small infant, operation should be undertakenwithout delay. Despite the probabilitythat the tumor will remain benign,there is always the chance that its unstable tissues may go on to malignantdegeneration. The real problem in themalignant sacrococcygeal teratomas isthe discovery of small lesions beforethey have begun to disseminate. Whileit is possible that a fatal outcome incases of malignant teratomata has already been determined at the time ofthe child's birth, we believe that someof them may be amenable to cure. Certainly routine rectal examination in infants and children should be made apart of every physical evaluation, fortime and again the complaints of difficulty in sitting, in defecation, and finably in urination have been noted tohave been present for months prior tothe diagnosis of an obvious malignantteratoma. The parents of such childrenare often reassured by their physicianswithout a rectal examination havingbeen done. Since nearly all of the teratoid tumors arise at the tip or in theinner surface of the coccyx, an areawhich is easily palpable on rectal examination, it should be possible to discover them far earlier than has beenthe case in the past. The newer approaches of combined X-ray treatment,chemotherapy, and surgical excisionhave not been curative in the bate
* One case was obviously malignant at birth and
was not considered in this number.
stages of the disease when these children are usually seen, but they maybe of greater value if an earlier diagnosis can be made.
SummarySacrococcygeal tumors which are
present at birth are usually benign. Ifthe growth appears after two months ofage, however, it is almost always malignant. Symptoms of bowel or bladderdysfunction increase the likelihood thatthe tumor is malignant.
The coccyx must be removed in everycase. If this is not done the recurrencerate is 31.3 percent.
During dissection for removal of thebenign teratomas, all muscle must bescrupulously preserved. Both the levator ani and the gluteus muscles arestretched and thinned by the tumorgrowth. If portions of these musclesare excised with the tumor, seriouscosmetic and functional defects mayoccur.
References1. Chaffin, L.: Clinical aspects of sacrococcygealteratomas. Surg., Gynec. & Obst. 69: 337-341, 1989.
2. Hatteland, K., and Knutrud, 0.: Sacrococcygealteratoma in children. Acta chir. scandinav. 119:444-452, 1960.
3. Hickey, R. C., and Layton, J. M.: Sacrococcygeal teratoma. Emphasis on the biological historyand early therapy. Cancer 7: 1081-1048, 1954.
4. Willis, R. A.: The Borderland of Embryologyand Pathology. London: Butterworth & Co., Ltd..1958, P. 447.
5. Hansmann, G. H., and Berne. C. J.: Sacrococcygeal teratomas. Arch. Surg. 25: 1090-1097, 1932.
6. Nicholson, G. W.: Studies on tumour formation;a sacrococcygeal teratoma with 3 metacarpal bonesand digits. Guy's Hosp. Rep. 87: 46-106, 1937.
7. Mayo, C. W.; Baker, G. S., and Smith, L. R.:Presacral tumors. Differential diagnosis and report of a case. Proc. Staff Meet., Mayo Clin. 28:616-622, 1953.
8. Gross, R. E.: Clatworthy, H. W., Jr., andMeeker, m. A., Jr.: Sacrococcygeal teratomas ininfants and children. Surg., Gynec. & Obst. 92:341-354, 1951.
9. Gius, J. A., and Stout, A. P.: Perianal cysts ofvestigial origin. Arch. Surg. 87: 268-287, 1988.
10. Benson, C.: Discussion.―
11. Renner, R. H., and Good.sitt. E.: Sacrococcygealteratoma. Report of a case of double tumor in anewborn infant. Am. J. Cancer 24: 617-625, 1985.
12. Schilling. A.; Ulfohn, A.; Aybar, 0., et al.:Enzyme-alterable alkylating agents. IV. Treatmentof cancer in children with repetitive massive dosesof S-46, protecting the extremity marrow bytourniquets. Cancer 16: 727-736, 1963.
351