![[Salesforce] Perforce - Enablers of Rampant Growth](https://static.fdocuments.in/doc/165x107/546d6a48b4af9f8e2c8b54d7/salesforce-perforce-enablers-of-rampant-growth.jpg)
behind the screen - Robert Wood Johnson Medical...
7
behind the screen the newsletter of the department of anesthesia Volume 1 • Number 1 FEATURED RESEARCHER Dr. Cohen talks about greenhouses and gravity SRBA: A New DRUG A review of the first selective relaxant binding agent A HISTORY LeSSON How $50K started this department & Much more...new faculty...ongoing research...international meetings...
Transcript of behind the screen - Robert Wood Johnson Medical...

behind the screenthe newsletter of the department of anesthesia
Volume 1 • Number 1
Featured researcherdr. cohen talks about greenhouses and gravity
SRBA: A New DRUGa review of the first selective relaxant binding agent
A HISTORY LeSSONhow $50K started this department
& Much more...new faculty...ongoing research...international meetings...

2 3behind the screen behind the screen
“He liked to sit leaning back,” Dr. Shaul Cohen explains, “like this,” as he mimics the movement in his chair. “I was in the army then,” he adds as he continues his story.
Born in Israel, Dr. Cohen served a total of four years in the military. He had deferred these until after he had completed training at the Medical School of the Hebrew University in Jerusalem in the early 70s. “I was just waiting for the movie to start when I heard the announcement: ‘Is there a medic here?’” The soldier in the recumbent position had been bitten in the neck by a poisonous snake—rampant in the area. Dr. Cohen and a few of his colleagues ran to assist. In the field and with limited equipment, they quickly in-tubated his trachea, securing his airway. They delivered antivenom and rushed the soldier to safety. And this was all prior to his complet-ing his anesthesia residency.
Currently the director of Obstetric Anesthesia and previously everything from a captain in the army to the chairman of an anesthesia department, Dr. Cohen has accomplished several life-times’ worth of accolades. All who have worked with Dr. Cohen know that his ed-ucational pearls are punctu-ated with stories such as the one above.
Dr. Cohen trained with Dr. Gertie Marx, who is often credited as the principle advocate for the use of epidural anesthesia to ease pain for routine deliveries at a time when an-esthesia was reserved only for Cesar-ean sections. Since his fellowship in obstetric anesthesia, Dr. Cohen has authored hundreds of studies that have improved patient safety.
A dural puncture headache is a known complication of placing an
epidural catheter. The needle, ad-vanced through the space between vertebrae, must end with its tip in-side the bony spinal canal but out-side the dura mater: too far and it may cause cerebral spinal fluid (CSF) to leak, which may result in a head-ache. Most anesthetists use a loss-of-resistance technique to find this tiny space; they slowly advance the needle while intermittently attempting to pump a small amount of air through
the needle with a syringe, carefully at-tempting to discern when the air can easily pass—a sign that the tip is in the epidural space.
Dr. Cohen noted that sometimes this technique failed; there would be no loss of resistance to air, but ad-vancing the catheter caused it to en-ter the dural space. He had a theory: as the needle is advanced, the lumen gets clogged with tissue, plugging it, preventing the anesthesiologist from
being able to squeeze air into the epi-dural space. “You cannot assume,“ he quickly adds, “without doing the study.” And that is exactly what he did. He enrolled 500 parturients into the study. One group had epidur-als placed the traditional way, while the other had one key difference: between every few millimeters of advancing the needle, the stylette (a fine plastic wire) was placed back in the hollow needle to clear it. In this
group, the incidence of a dural puncture decreased to 0.4%, a sixfold difference. The benefit is so great that he trains every resident that passes through the obstetrics rotation this technique. “You cannot make it zero,” Dr. Cohen makes sure to note as he explains how small adhesions may still obliterate the epidural space and cause the anesthesiologist to cause a CSF leak.
“For those cases,” he con-tinues, “we can offer a sphe-nopalatine ganglion block,” a minimally invasive technique that palliates the strong head-ache that accompanies a dural puncture. A recent study he performed showed that it can avoid having to place an epi-dural blood patch: the tradi-tional treatment, but also one that carries a much higher risk of infection than this block.
Currently, he is work-ing on several studies, one of which—the gravity tech-
nique—relies on the free flow of the epidural infusate to open this space to improve patient satisfaction and analgesia. Outside the hospital, Dr. Cohen is just as active. He carries two smart phones to show off pic-tures of scores of tropical flowers that bloom in his home greenhouse. “It’s what helps me stay above ground,” he comments about his hobby. And when does he expect to retire? He an-swers very bluntly: “Never.”
Letters I began my role as Program Director (PD) just a few short months ago. During
this time, several concerns have arisen, contributing to the growth of several new gray hairs on my head!
The support of the faculty has eased considerably my transition in the PD role. The CA-1 residents gave us rave reviews on the content and presentation of the basic science lectures. And our efforts were not in vain, as evidenced by the outstanding scores on their first metrics exam!
We also give a wonderful round of applause to our recent graduates. The written board pass rate was 100%! We wish them continued success in their careers.
I am very much indebted to the Faculty for all your efforts in establishing a dynamic and productive educational environment for all of the residents.
Thank You!Kang Rah, MD
It is my distinct pleasure to present the inaugural edition of behind the screen, the official newsletter of the Department of Anesthesiology of Rutgers, The State University of New Jersey!
We hope to improve communication among all members of the Department via this medium. We may share all manner of information and gather feedback on the common issues that matter to us as clinicians, academicians, educators and members of the health care community.
Everyone’s voice is important. We encourage your participation and your contribution!
Christine W. Hunter, MDChair
Today we incorporate a new face to our already busy, but not-so-visible department with the addition of this newsletter of the Department of Anesthesiology at Rutgers Robert Wood Johnson Medical School. Too often we hear from friends, the public, and even colleagues: “What does an anesthesiologist do?” We hope that with this new informational tool, we can help spread the word on issues related to anesthesia within our institution and the practice as a whole. In the coming issues, we shall delve into multiple topics related to the educational, informational, and research-oriented missions of our Department and its sections: critical care, cardiac, obstetric, pediatric, perioperative ultrasound, acute and chronic pain, and regional. We shall also show you that our jobs don’t end when the drapes come down. We hope that this periodical will serve as a communication tool for our colleagues as well as for patients and their relatives. We welcome notices regarding exciting activities, research projects, and personal announcements from our colleagues that they would like to share with the department. We extend an invitation to patients who would like to share their experience with our department as well.
We appreciate this opportunity to shine a light on the Department.
The Editors
behind the screen
Featured researcher: Dr. Shaul Cohen
Enrique PantinQuiana Fraizer
Ashley GlorNeethu Kumar
Sagar S. MungekarDiane Ridley
Editor-in-ChiefAssociate EditorAssociate EditorAssociate EditorAssociate EditorAssociate Editor
Department of AnesthesiaRutgers Robert Wood Johnson Medical School
Clinical Academic Building 3100125 Paterson Street
New Brunswick, New Jersey 08901-1962United States of America
Unless otherwise noted, all content is copyright by and the intellectual property of behind the screen and may not be copied, reproduced, distributed, or displayed without express permission. The information contained herein is neither intended nor implied to be a substitute for profes-sional medical advice; rather, it is provided for educational purposes only. The views expressed are not necessarily those of the Medical School or Rutgers, the State Uni-versity of New Jersey. Informed consent was obtained as required. Correspondence may be directed to the address above or electronically to the addresses on the back cover. ©2013
by Sagar S. Mungekar
Cover photo and art by Sagar S. Mungekar
Photo: Sagar S. Mungekar
Photo: Sagar S. Mungekar
Photo: Enrique Pantin

4 5behind the screen behind the screen
Sugammadex is a new class of medications called selective relaxant binding agents (SRBAs). This medica-tion acts to encapsulate free circulat-ing steroidal nondepolarizing neuro-muscular blocking agents, decreasing the amount interacting at the recep-tor sites.
The sugammadex structure con-tains 8 glucose molecules with nega-tively charged side chains. The ring with a lipophilic interior binds to aminosteroid relaxants with a 1:1 ra-tio, removing the relaxant from the neuromuscular junction. The resul-tant complex lacks relaxing proper-ties and is excreted within 24 hours via the kidneys (96%), expiration and feces (0.02%); the remaining is slowly decomposed in the liver. This binding has a very high association rate, rendering the incidence of resid-ual block extremely low while avoid-ing the side-effects associated with traditional reversal agents. Sugam-madex shows the highest affinity for rocuronium, then vecuronium, and the lowest for pancuronium.
Sugammadex is meant only for single-dose use. The recommended dose depends on the level of neuro-muscular blockade (NMB) to be re-versed, with smaller doses needed for a light block compared with a deep block. For routine reversal, if spon-taneous recovery from a light NMB (reappearance of T2) with rocuroni-um or vecuronium has occurred, a sugammadex dose of 2 mg·kg-1 is recommended. A sugammadex 4 mg·kg-1 dose is recommended if
recovery has reached 1 to 2 post-te-tanic counts (profound NMB) after rocuronium or vecuronium. For the immediate reversal of NMB, a su-gammadex dose of 16 mg·kg-1 at 3 minutes after the administration of rocuronium is recommended. Pre-cautionary measures should be taken in the severely renal impaired, until more data is available.
The most frequently reported adverse events in clinical trials of su-gammadex were hypotension, QTc prolongation (>400 ms), broncho-spasm, constipation, hyperactivity, and dysgeusia (altered taste sensa-tion).
Sugammadex has been dem-onstrated to be highly effective and generally well tolerated during Phase I–III testing. Sugammadex was ap-
proved by the European Commission in July 2008 for routine reversal of rocuronium or vecuronium and for immediate reversal of rocuronium in adults, and for routine reversal fol-lowing rocuronium in children and adolescents. In the US, sugamma-dex was issued a not approvable–let-ter by the FDA in August 2008. The FDA cited concerns over potential hypersensitivity reactions which was based on data from one volunteer who displayed clinical evidence of hypersensitivity during the infusion of a 32 mg·kg-1 dose and the retro-spective identification of six potential hypersensitivity reactions in previous studies.
In summary, sugammadex has an onset ten times faster than neostig-mine and three than edrophonium, very low incidence of side effects, and can be used even when deep neuro-muscular block is present. It has been widely used in adults and children in Europe, Australia, Iceland, New Zea-land, and some countries in South America with great success. Some practitioners no longer use other means of reversal. Its main limita-tion, by far, has been related to its high price.
Hot topics: A novel reversal agent and... Numerous studies have shown
glycemic control in patients under-going coronary artery bypass grafting (CABG) with diabetes mellitus and those with hyperglycemia decreases the risk of perioperative morbid-ity and mortality and improves long term survival.
In 2005, Gandhi et al. looked at the effects of intensive intraopera-tive insulin therapy in 400 elective patients undergoing CABG. Patients were prospectively randomized to a continuous insulin (glucose 80–100 mg·dL-1) or a conventional group with (glucose less than 200 mg·dL-1) using intermittent boluses of IV in-sulin. The incidence of diabetes was 20% in both groups. There was no difference between the groups in the composite incidence of death, sternal wound infections, prolonged venti-lation, cardiac arrhythmias, strokes, ICU or hospital stay, and renal failure within 30 days of surgery. Patients in the aggressive glycemic control had significantly lower mean intraopera-tive glucose levels (114 mg·dL-1 vs. 157 mg·dL-1; p < .01), however there was no difference in glucose levels 24 hours postoperatively. In addition, in the aggressive insulin therapy there was an increased tendency for more deaths and strokes.
Some of the limitations of this study include both groups received intense insulin therapy immediately postoperatively therefore it was hard to distinguish between aggressive glycemic control versus intermittent insulin therapy; the study included both patients with diabetes and non-diabetic patients. In the intermittent insulin bolus group, the average glu-cose levels 24 hours postoperatively was less than 180 mg·dL-1; therefore, this group achieved the same degree of glycemic control as the continuous insulin therapy group.
This finding suggested that tight glycemic control might also be ben-eficial in nondiabetic patients during
CABG surgery. In 2011, Szekely et al. also supported this finding in their study of 550 patients undergoing primary CABG surgery. In this mul-ticenter series of patients, there was increased in hospital mortality in nondiabetic patients associated with 48 hours postoperative glucose levels greater than 250 mg·dL-1 However, within the nondiabetic group 25% were treated with a perioperative in-sulin infusion compared with 84.4% of the diabetic patients.
It is now believed tight glyce-mic control is beneficial in both dia-betic and nondiabetic undergoing CABG surgery. Although studies have shown glucose levels less than 180 mg·dL-1 reduces morbidity and mor-tality in patients undergoing CABG, the optimal range of glucose levels is not clear. In the study by Van den Ber-ghe et al., blood glucose levels were maintained 80–100 mg·dL-1 and there was no effect on morbidity and mortality in patients who had under-gone a CABG and spent less than 3 days in the ICU.
Lazar et al. looked at effects of a more aggressive regimen for glycemic control in diabetics. Patients were prospectively randomized to aggres-sive (90–120 mg·dL-1) or moderate (120–180 mg·dL-1) glycemic con-trol. More aggressive glycemic con-trol did not have any significant im-provement in clinical outcomes that could not otherwise be achieved with more moderate control. Bhamidipati et al. also showed the least amount of morbidity and mortality was with moderate glycemic control (120–179 mg·dL-1) in diabetic patients under-going CABG.
The American College of Physi-cians now recommends a moderate glucose level of 140–200 mg·dL-1 in surgical and medical ICU patients. Future studies in this area will help further determine the most optimal level of glycemic control in patients undergoing CABG.
Evidence-based medicine is the cornerstone of our practice. Keeping up with scientific advancements
helps us offer the best care to our patients. For this is-sue, Dr. Neethu Kumar has reviewed the current liter-ature and provided us with viewpoints on two issues: one that is a new solution to an old problem, and the other, a concept revisited.
by Neethu Kumar
Abrishami A, Ho J, Wong J et al. Sugammadex, a selective reversal medication for prevent-ing postoperative residual neuromuscular blockade (review). Cochrane Database Syst. Rev. 2009; 7(4), CD007362
Aniskevich, S; Leone, B; Brull, S. Sugammadex: a novel approach to reversal of neuromuscu-lar blockade. Expert Rev Neurother 2011; 11:185-98
Fink, H; Hollman, MW. Myths and facts in neu-romuscular pharmacology. New devel-opments in reversing neuromuscular blockade. Minerva Anestesiologica. 2012; 78:473-82
Sokół-Kobielska, E. Sugammadex—indications and clinical use. Anaesthesiol Intensive Ther. 2013; 45:106–10
Szekely A, Levin J, Miao Y, et al. Impact of hy-perglycemia on perioperative mortality af-ter coronary artery bypass graft surgery. J Thorac Cardiovasc Surg 2011; 142:430–7.
Gandhi GY, Nuttall GA, Abel ND, et al. Inten-sive intraoperative insulin therapy versus conventional glucose management dur-ing cardiac surgery. Ann Intern Med 2007; 146:233–42.
Lazar, A. How important is glycemic control dur-ing coronary artery bypass?. Advances in Surgery. 2023; 46: 219-35.
Lazar HL, McDonnell M, Chipkin S, et al. The So-ciety of Thoracic Surgeons practice guide-line series: blood glucose management during adult cardiac surgery. Ann Thorac Surg. 2009; 87:663–9.
Lazar HL, McDonnell M, Chipkin S, et al. Effects of aggressive versus moderate glycemic control on clinical outcomes in diabetic coronary artery bypass graft patients. Ann Surg 2011; 254(3):458–64.
Bhamidipati CM, LaPar DJ, Stukenborg GJ, et al. Superiority of moderate control of hyper-glycemia to tight control in patients un-dergoing coronary artery bypass grafting. J Thorac Cardiovasc Surg 2010; 141:1–9.
Qaseem A, Humphrey LL, Chou R, et al. For the Clinical Guidelines Committee of the American College of Physicians. Use of intensive insulin therapy for the manage-ment of glycemic control in hospitalized patients. A clinical practice guideline from the American College of Physicians. Ann Intern Med 2011; 154:260–7.
...the glycemic control debate
References and suggested reading
Sugammadex, a derivative of γ-cyclodextrin, is depicted as a space-filling model. The lipophilic core (hydrogen atoms, white spheres) encapsulates the aminosteroid rocuronium (not shown) while the hydrophilic exterior (sodium atoms, purple spheres) increases blood solubility.
Image in public domain
16th World Congress of AnaesthesiologistsAugust 28–September 2, 2-14
Hong Kong Convention and Exhibition Centre
6 7behind the screen behind the screen
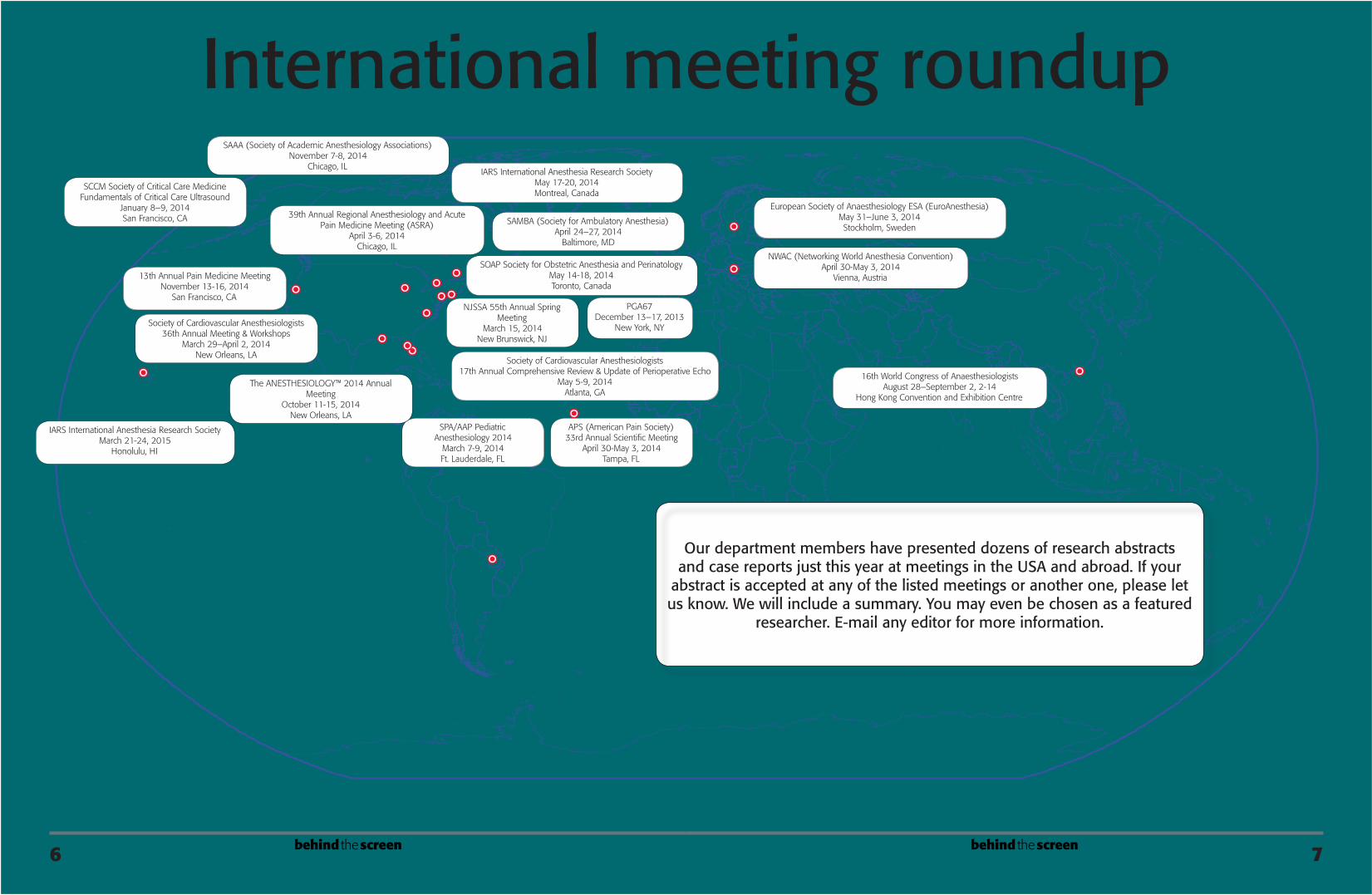
International meeting roundup
Our department members have presented dozens of research abstracts and case reports just this year at meetings in the USA and abroad. If your
abstract is accepted at any of the listed meetings or another one, please let us know. We will include a summary. You may even be chosen as a featured
researcher. E-mail any editor for more information.
PGA67December 13–17, 2013
New York, NY
SCCM Society of Critical Care MedicineFundamentals of Critical Care Ultrasound
January 8–9, 2014San Francisco, CA
SPA/AAP Pediatric Anesthesiology 2014
March 7-9, 2014Ft. Lauderdale, FL
NJSSA 55th Annual Spring Meeting
March 15, 2014New Brunswick, NJ
Society of Cardiovascular Anesthesiologists36th Annual Meeting & Workshops
March 29–April 2, 2014New Orleans, LA
39th Annual Regional Anesthesiology and Acute Pain Medicine Meeting (ASRA)
April 3-6, 2014Chicago, IL
APS (American Pain Society) 33rd Annual Scientific Meeting
April 30-May 3, 2014Tampa, FL
NWAC (Networking World Anesthesia Convention)April 30-May 3, 2014
Vienna, Austria
Society of Cardiovascular Anesthesiologists17th Annual Comprehensive Review & Update of Perioperative Echo
May 5-9, 2014Atlanta, GA
SOAP Society for Obstetric Anesthesia and PerinatologyMay 14-18, 2014Toronto, Canada
IARS International Anesthesia Research SocietyMay 17-20, 2014Montreal, Canada
European Society of Anaesthesiology ESA (EuroAnesthesia)May 31–June 3, 2014Stockholm, Sweden
SAMBA (Society for Ambulatory Anesthesia)April 24–27, 2014
Baltimore, MD
The ANESTHESIOLOGY™ 2014 Annual Meeting
October 11-15, 2014New Orleans, LA
SAAA (Society of Academic Anesthesiology Associations)November 7-8, 2014
Chicago, IL
13th Annual Pain Medicine MeetingNovember 13-16, 2014
San Francisco, CA
IARS International Anesthesia Research SocietyMarch 21-24, 2015
Honolulu, HI

9behind the screen8 behind the screen
Anesthesia patient safety out-comes are based on the combined efforts of many individuals within the anesthesia care team. Robert Wood Johnson University Hospital (RWJUH) is no exception. The anes-thesia care team consists of anesthe-siologists, certified registered nurse Anesthetists (CRNAs), residents and anesthesia technicians (ATs). Anes-thesia technicians provide the nec-essary tools, support, and expertise needed to help the anesthesia care team perform their job safely and successfully. They assist the anesthe-sia care team in all phases of patient care: preoperative, intraoperative and postoperative.
There are several educational programs that have helped ATs ob-tain the necessary critical skills and knowledge that they need to be suc-cessful in this field. The American So-ciety of Anesthesia Technologists and Technician (ASATT) is one. Founded in 1989, ASATT is an organization that focuses primarily on the educa-tion of anesthesia technologists and technicians. ASATT also provides
Anesthesia technicians
Stanley Sowa, or “Stan the man”, as some would call him, has played a very special role in the Anesthesia department at Robert Wood Johnson Univer-sity Hospital. Stan was unique because he worked every other weekend faithfully until he retired in 2013. He has made a great dif-ference in the lives of so many in-cluding his coworkers. We honor him for that.
Stanley Sowa attended the Alexian Brother Nursing School in Chicago and graduated in 1966. He also attended and grad-uated from Jersey Shore Medical Center (JSMC) School of Anesthe-sia in 1971. After graduating, he became the Director of the school until they closed. Stan began his journey working weekends here at
Stan the man
The word “anesthesia”, also writ-ten “anaesthesia” is derived from the Greek αν- (an-) meaning “without”; and αἴσθησις (aisthesis) meaning “sensation”. Simply said, it means “without sensation”. The first written known use of the word goes back to 1721, when it appeared in Nathan Bailey’s Universal Etymological Eng-lish Dictionary. The search for pain control can be traced far back in his-tory. Sleep potions were described by Homer in the Odyssey, but it was
standards of practice guidelines that help with AT daily practice.
Here at RWJUH we have a team of nineteen ATs who are responsible for coverage in the following areas: main operating rooms, pediatric op-erating rooms, labor and delivery, ra-diology department, cardiac catheter-ization laboratory, endoscopy suites, as well as other areas where acute an-esthesia care is provided (emergency rooms, intensive care units, and hos-pital floors). The ATs help ensure that patient safety is the department’s pri-ority.
really not until 1824 when a young British doctor, Henry Hill Hickman, was able to anesthetize successfully animals using a gas called nitrous oxide. He had many detractors, and failed to convince the French Acad-emy on its potential on humans and fell in disgrace.
In January 1842, Crawford W. Long used ether to remove a neck tu-mor from James Venable in Georgia, but his experience went mostly un-noticed. Soon thereafter, he had to stop using ether when he was almost killed by the people of his town. The first successful public anesthetic dem-onstration was done by William T. G. Morton using ether on October 16, 1846 in the amphitheater of Massa-chusetts General Hospital. He anes-thetized Mr. Gilbert Abbott. He be-gan by saying, “doctor, your patient is ready”, a phrase uttered to his day by anesthesiologists. Once Dr. Warren finished removing the neck tumor and the patient awoke without recol-lection of pain, he told the audience “Gentlemen, this is no humbug”.
The discovery of surgical anes-thesia is considered by many as the biggest contribution the USA has made to medicine.
What is anesthesia?
by Quiana Frazier
by Enrique Pantin
by Quiana Frazier Robert Wood Johnson University Hospital when it was “Middlesex General Hospital” in 1977.
In 1984 he became affiliated with the University of Medicine and Dentistry (UMDNJ) and the rest is history.
Stan currently resides in Shark River Hills, New Jersey with his wife, daughters, son-in-law, grandchildren and a host of ani-mals that he adopts from Bruce Springsteen’s farm. We would like to congratulate Stan on his retire-ment. He has been a dedicated and appreciated member of the anesthesia team for over 30 years and we are happy that he will have the opportunity to spend time with his family. We wish him nothing but the best as he embarks on his next venture.
Stanley Sowa is seen here earlier this year holding a copper kettle, a device invented in the 1950s that was used to deliver a standard volume of inhaled anesthetic vapor to the patient.
Photo: Stanley Sowa
New faculty membersPhoto: Sagar S. Mungekar
Dr. Gina George, born and raised on Long Island, New York, complet-ed an accelerated seven-year medical program at New York College of Os-teopathic Medicine in Old Westbury, NY after which time she completed her internship at North Shore Uni-versity Hospital. She then continued her training with us in an anesthesia residency. She started working at Rut-gers Robert Wood Johnson University Hospital on August 2013.
Photo: Sagar S. Mungekar
Dr. Jayesh Thaker, graduated from the State of Gujarat Medical School in Gujarat, India, completed in 1996 his anesthesia residency at Brookdale Medical Center, New York. He has worked in two states, New York and New Jersey, and came back to us on October 2013 to work shar-ing time at our ambulatory center and Rutgers Robert Wood Johnson University Hospital. We welcome back Dr. Thaker!
Photo: Sagar S. Mungekar
Dr. Jessica Perez, graduated from Ross University School of Medicine, Dominica, West Indies, did her anes-thesia residency at St. Barnabas Medi-cal Center, and went to Children’s Hospital of Michigan where she com-pleted a pediatric anesthesiology fel-lowship in June 2013. She joined our Pediatric Anesthesia Team in July of this year.
Photo: Enrique Pantin
Dr. Melissa Wu, completed her undergraduate school at Rutgers in 2003. She attended medical school and completed her anesthesia resi-dency at Rutgers Robert Wood John-son Medical School, (formerly UMD-NJ), graduating in June 2013. She started working at Rutgers Robert Wood Johnson University Hospital in August 2013.
Photo: Sagar S. Mungekar
Dr. Christine Curcio, joined our practice in July 2013 as part of the Pediatric Anesthesia team. Dr. Curcio completed her internship and anes-thesia residency at Stony Brook Uni-versity Hospital in Stony Brook, NY in 2012 and went on to complete a fellowship in pediatric anesthesia at University of Michigan’s Mott Chil-dren’s Hospital in 2013.

10 11behind the screen behind the screen
One of the consequences of this realization became plans for a medi-cal school to be built on the Piscat-away campus of Rutgers University. It was envisioned that this would be a two-year school that would feed medical schools in the North-east with third-year clinically ready medical students. This idea was quite contentious; in only a short time it evolved into a traditional four-year school.
The original plan had also called for a medium-sized hospital to be built from the foundation up on the Busch campus. But as has often happened in New Jersey history, the state ran out of money. The hospital, which originally was supposed to have between 200 and 300 beds, was shaved back to 150 beds, then to 70 beds, and finally to no beds. Resident clinical experience therefore was out-sourced to smaller hospitals around the area.
The two large hospitals in New Brunswick—St. Peter’s Medical Cen-ter and Middlesex General Hospi-tal—were enlisted for the bulk of clinical training. At that time they both had around 300 beds and were not considered to be on par with hospitals in New York and Philadel-phia. Individual practitioners and small partnerships controlled both hospitals. They both had long tradi-tions of service to the community, with St. Peter’s in particular having a modest but real reputation as an obstetric and neonatal center. The lo-cal community of medical practitio-ners viewed the arrival of the medical school as a potential imposition and a rival for the patient population.
It should be noted here that the general feeling of the community was
that the two hospitals were fine for routine work, but for services such as pediatric surgery or cancer care, the New Jersey Turnpike beckoned in one direction to Children’s Hospi-tal of Philadelphia, and in the other direction to Sloan-Kettering of New York City.
There was some indication that during the 70s, Middlesex General Hospital was in ill financial health. This reality, coupled with the need for an inexpensive clinical campus, morphed into a grand bargain that in a complex contract gave the medical school the right to appoint the chiefs of service of the various specialties at Middlesex in return for state support for items such as house staff salaries (for a vastly increased number of interns and residents) and improve-ments to the physical plant. One of the major carve-outs, which was left to be determined, was the status of the anesthesia department, which had functioned as a private practice for many decades.
When the medical school started an open-heart program in the late 70s, the private anesthesia practice refused to cover these long and dif-ficult cases, which led the surgery department to set up a section of anesthesia within itself, and hire out-side anesthesiologists. It also led to a global agreement between the private anesthesiologists and the surgery de-partment—signed off by the dean at the time—that the ten rooms in the operating suite at Middlesex would be divided such that daily, the private practice was expected to cover seven rooms and the University, three, in-cluding the open-heart room.
Since the private practice group contained five anesthesiologists and
two nurse anesthetists, this meant that they committed their entire ros-ter irrespective of call status to work every day, with the nurse anesthe-tists’ nominally being supervised by an anesthesiologist who was simul-taneously administering anesthesia. Lunch breaks and calls of nature were answered by either delaying case starts in the private practice rooms or turning the case over to “Dr. Ventila-tor” with the anesthesia caregiver’s out of the room for between ten to thirty minutes.
Toward the end of the 70s, the Dean initiated a search for a chairman of anesthesia, upon whose arrival the section of anesthesia as a subdivision of the surgery department would it-self become a full department.
The search went on for nearly four years, and was the longest in the history of the medical school up to that time and for many years after.
The first appointed chairman was Dr. Sanford L. Klein, DDS, MD, who came from the University of Iowa, although he had grown up and have been educated in New York City, graduating from training programs in Albany, New York, and Philadelphia. Dr. Klein was also a two-year veteran of the United States Army, and had spent nearly eight years at the Univer-sity of Iowa Hospital ending with a four-year stint as the clinical director of the operating room suite in one of the larger hospitals in the United States.
Dr. Klein was appointed chair in August of 1983, and arrived in New Jersey with his family in October just in time to leave for that year’s Ameri-can Society of Anesthesia Conference to recruit new faculty members.
As a gift, the surgery department gave the department of anesthesia $50,000 in cash, and an accounts re-ceivable valued at a quarter million dollars. A naïve Dr. Klein thought
that this was a very satisfactory situ-ation; however, almost immediately it became apparent that the depart-ment was expected to serve primarily as adjuncts to the open-heart room by the surgery department. This led to many colorful disagreements, and some unstable solutions such as hir-ing cardiac anesthesiologists per diem from New York and Philadel-phia to perform the open-heart cases when the department’s load in its other rooms became unmanageable. Because many of the open-heart pro-cedures were being done on patients insured by Medicare, the departments found itself in the position of paying more to the outside contractors than it took in by billing.
The situation was partially allevi-ated by immediately hiring five nurse anesthetists to help carry the load. Many months of high volume nego-tiations and vituperative discussions would pass before arriving at an equi-librium with the Surgery department.
Meantime, the private practice was creating its own freestanding surgicenters in East Brunswick and conflict escalated as it appeared they expected surgeons from Middlesex to take patients from that hospital to their new center.
Negotiations were entered rather fitfully in a scheme for the Univer-sity to buy out the private practice. Their initial negotiating position was based upon a buyout of 17 years. The university’s position was a five-year buyout, which led to many tense mo-ments in the operating room, partic-ularly when matters of the standard of care were brought up. To further complicate an already tangled and complex situation, the Department of Anesthesia pushed ahead to estab-lish an anesthesia residency. The first residents, a group of four started on July 1, 1985…
The history of our department by Sanford Klein
continued on page 11Watch for the continuation of this story
in the following issue of behind the screen.
In the late 1960s it was recognized that the number of medical schools in New Jersey compared to neigh-
boring states, and in particular, to the size of the popu-lation, was woefully inadequate.
General announcementsby Alann Solina
A multi-disciplinary RWJ-specific Regulating Compliance Committee is in the works to ensure compliance with all regulating agencies: JCAHO, Department of Health, and CMS. Representatives from anesthesia, surgery, pharmacy, nursing, and ancillary support will collaborate to keep the whole of perioperative services compliant and up to date on all new and existing compliance regulations.
Pediatricsby Valerie McRae
A new pediatric order set will be integrated into SCM. All preoperative (e.g. oral midazolam) and postoperative medications will be included (pain medi-cations, respiratory treatments, etc.) in a patient-specific weight-based formula.
Coming soon is the grand opening of the new pediatric operating rooms located in the Bristol Myers Squibb Chil-dren’s Hospital on the seventh floor. There are four large operating rooms and two smaller procedure rooms, one of which will be used for pediatric endos-copy. The other procedure room is slated for cases such as lumbar punctures with chemotherapy. All pediatric surgeons will perform all surgical cases upstairs, but major trauma cases will still be per-formed in the main operating room area in the first floor.
Endoscopyby Dennis Hall
Many endoscopists are instituting a split preparation for patients whose pro-cedure times are scheduled to begin after noon. This allows for a better colonic preparation for colonoscopy. The second dose of preparation should be 4 hours prior to start time and is 8–16 oz. of clear liquid, keeping within the NPO guide-lines for procedure: 4 hours for clears.
Cardiac anesthesia
One of the original founding sur-geons of RWJ’s cardiothoracic Surgery Di-vision in the Department of Surgery, Dr. Peter Scholz has retired.
A new cardiothoracic surgeon, Dr Aziz Ghali, who comes from Loma Linda University in California started to work with us. He has been hired to replace Dr. Thomas W. Prendergast as our heart transplant surgeon. Dr. Prendergast left us to work at Jersey City Medical Center a few months ago but has continued to provide heart transplant care at RWJ.
Iloprost a synthetic analog of prosta-cyclin is now being utilized inhaled as an adjunct to or in some cases as a replace-ment for nitric oxide in patients with pul-monary hypertension undergoing cardiac surgery. It is commercially available in 1 mL ampules at two different concentra-tions: 10 and 20 mg·mL-1, and can be stored at room temperature. Dosage initi-ated for cardiac surgery is 2.5 or 5 mg. De-livered via nebulizer, prostaglandins have been shown to have comparable efficacy and hemodynamic effects to inhaled ni-tric oxide at a fraction of the cost.
Neuroanesthesiaby Christine Hunter and Christian McDonough
The department has seen an increase of 50% in the volume of interventional neurosurgical cases just during summer 2013. These cases are mainly done in the neuroradiology suites in the radiol-ogy department. State of the art develop-ments in the treatment of aneurysms have patients and surgeons flocking to these minimally invasive techniques. One such technique-Pipeline Embolization Device-is allowing treatment for some of the most complex and dangerous brain aneu-rysms. This wire mesh cylindrical device made of a nickel-cobalt chromium alloy is endovascularly placed across the neck of the aneurysm redirecting blood flow away from the aneurysm. This will allow the remaining blood in the aneurysm to form a blood clot which prevents the rup-ture of the aneurysm.
Off-site anesthesiaRoom 9 in Special procedures in the
radiology department has a new Mega-tron-like monitor that moves freely from the ceiling and is located directly in front of the anesthesia machine.
There is a portable end-tidal CO2 ma-chine located in the endoscopy depart-ment for all off-site location that require anesthesia, but are not equipped with such monitoring.
Memorandacompiled by Ashley Glor
Photo: Sagar S. Mungekar; Logo, seal, and marks are property of Rutgers, the State University of New Jersey

Department of Anesthesia Chairman
Christine Hunter, MD
Vice-ChairmanAlann Solina, MD
FacultyRose Alloteh, MD
Sylvania Barsoum, MDStefanie Berman, MDMordy Bermann, MD
Oak Chi, MDRenu Chhokra, MD
Antonio Chiricolo, MDShaul Cohen, MD
Christine Curcio, MDVincent DeAngelis, MD
Howard Denenberg, MDJohn Denny, MDGina George, DO
Steven Ginsberg, MDJeremy Grayson, MDWilliam Grubb, MD
Dennis Hall, MDSam Kiel, MDGeza Kiss, MD
Christian McDonough, MDValerie McRae, MDTejal Mehta, MD
Scott Mellender, MDEnrique Pantin, MD
Jessica Perez, MDKang Rah, MD
Diane Ridley, MDAshraf Sakr, MDShruti Shah, MDRyan Sison, MD
Laurie Spina, MDMark Stein, MD
Jamie Taylor, MDJames Tse, MD, PhD
Boris Veksler, MDMonty Wang, MDMelissa Wu, MDDora Zuker, MD
Chief Anesthesia ResidentsAndrew Burr, DOHeather Skiff, DO
ResidentsCandy Anim, MD
Gianna Casini, MDMohammad Chaudhry, MD
David Delatte, MDAliraza Dinani, MD
Amanda Doucette, MDViviana Freire, MDSabrina Haque, MDAysha Hasan, MDThomas Jan, MD
Matthew Johnson, MDRobert Jongco, MD
Alexander Kahan, MDAnkit Kapadia, MD
Ibraheem Khan, MDJane Kim, MD
Carolyn Kloepping, MDNeethu Kumar, MDJacques Lorthé, MD
Christian Mabry, MDQuynh Mai, MD
Sagar S. Mungekar, MDNeeraj Nanavati, MD
Arpit Patel, MDErica Patel, MDBrian Raffel, DOSana Shaikh, MD
Mengmeng Shen, MDTatyana Shkolnikova, MD
Trishna Upadhyay, MD
Certified Registered Nurse AnesthetistsTemitope AjibadeDaphne AnudonYvelise Bargman
Bruno Beja-UmukoroKatherine Glass
Ashley GlorOrlando Gopez*
Kristen KellyTanya Milask
Sharon MorganKatie Novak
Stacey PaulusAndrew PrusanAlex Rozhitsky
Elzbieta SamojlukAnthony Smith
Kenneth TruesdaleAnesthesia Technicians
Ahmed BanguraDoreen Bell Jade Barnes‡Luz CamachoEbonee Clark
Quiana Frazier†Kenie Lebron‡Gwendolyn LeeHanan Malek Jorge Mancera
Cecil “Chris” McFarlaneLinda OrtutayShevon ParksIgnacio Rivera
Katrina Sinkfield‡Andrea Sroczynski
Deon TaylorKeith Taylor
Gwendelyen “Mamma” Wells
* Chief CRNA† Anesthesia manager‡ Lead anesthesia technician E-mail editor: [email protected]
AdministratorsVirginia Freemanrecchia
Elaine IwachiwWendy Kuziemski
Valerie LisottoHelen Lowry
Ann Marie LozanoDiane Plona
Danielle PlylerBen Schoen
Doreen M. Stillwell


















