BBEEYYOONNDD TTRRAAIINNIINNGG · 2013-10-06 · Mastering Endurance, Health and Life B eenn...
14
B B E E Y Y O O N N D D T T R R A A I I N N I I N N G G Mastering Endurance, Health and Life Ben Greenfield
Transcript of BBEEYYOONNDD TTRRAAIINNIINNGG · 2013-10-06 · Mastering Endurance, Health and Life B eenn...

BBEEYYOONNDD TTRRAAIINNIINNGG Mastering Endurance, Health and Life
BBeenn GGrreeeennffiieelldd

I experienced my first "PVC" when I was in the middle of an 18 mile training
run for Ironman Hawaii.
To prepare my body and mind for the rigors of the Kona lava fields, I had chosen to go
pound the pavement at 4pm in the afternoon on a blistering 97 degree day in my hometown
of Spokane, Washington. At about mile 15, with my throat parched and my body
overheating, I paused for a quick sip of water from the drinking station beside the trail. But
as I bent down to take a drink, something suddenly felt very wrong in my chest.
My heart skipped a beat.
Several times.
Here I was exposed in the scorching heat, 3 miles from home, and my body's primary
internal engine - the organ that literally decides whether I live or I die - seemed to be
seriously malfunctioning.
If I had been lost in the tunes of .mp3 player, my labored breathing or the beat of my feet on
the ground, I probably wouldn't have even noticed this cardiovascular electrical short-
circuit. But I was lucky enough to have not been moving when my heart decided to flip-flop.
And I definitely noticed.
So I walked home. Slowly.
-----------------------------------------------
Let's back up for a second.
After all, a PVC may sound like something out of a science fiction novel or a do-it-yourself
household plumbing guide.
But PVC actually stands for "Premature Ventricular Contraction", and you're about to learn
how it happens.
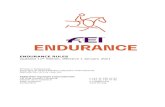
Every time your heart squeezes blood out to the rest of your body, it requires an electrical
impulse. In a normal electrical conduction, impulses originate from an area in the top right
corner of the heart known as the "sinus node" (see picture below). The electricity then
spreads across the upper two chambers of the heart (the atria), and is then transmitted to
the lower two chambers (the ventricles) through the "atrioventricular node".

During a normal heartbeat, your heart's ventricles contract blood out to your entire body
after your heart's atria have helped to fill them. In this way, the ventricles can pump the
maximum amount of blood both to the lungs and to the rest of the body.
So how can this electrical misfiring happen?
Every piece of tissue in your heart is electrically active. This means that all heart tissue can
conduct electricity. However, all heart tissue can not only conduct electricity, but can also
generate electricity. Normally, your heart tissue is conducting electricity generated by the
sinus node. However, occasionally it will generate electricity on it's own as well - and when
this happens a premature contraction results.
So when a PVC happens, your heartbeat is not initiated by your sinoatrial node (your body's
normal heartbeat initiator), but rather by special fibers in your ventricles that are triggered
by the atrioventricular node, bypassing the normal method of electrical stimulation. This
means your ventricles contract first - before your atria have optimally filled the ventricles
with blood.
And this not only means that blood circulation of oxygen and nutrients is way less efficient,
but it also means that you can feel things like palpitations, skipped beats, extra heart
contraction, irregular heart rhythm, slight chest pain, a feeling of faintness and fatigue, or
shortness of breath.
Now before you have a PVC panic attack, please allow me to make something
very clear: the occasional PVC is actually common.
That's right - nearly everybody has a skipped or extra heartbeat every now and then. As a
matter of fact, cardiac electrophysiologist and cyclist Dr. John Mandrola, in a very good
blog post on PVC's, says that PVC's are the second most common rhythm problem he sees

(he points out that a related electrical abnormality called an atrial arrhythmia, also known
as a "heart flutter" is the most common).
In that same post, Dr. Mandrola also points out a few other interesting facts, including:
1. In an overwhelming majority of people, especially those with normal heart structure,
PVCs are benign - which means that the extra beats do not actually indicate heart
disease or any other serious and immediately threatening issue...
2. The normal person has about 100,000 heartbeats per day (athletes with slow
heartbeats would have fewer heartbeats than this), and only people with more than
20,000 PVCs per day are actually at risk for developing cardiomyopathy (weak heart).
That means about 20% of the time, you'd be experiencing PVC's - and trust me - you'd
probably know it if this were the case.
3. PVC's might indicate training excess. Here's exactly what Dr. Mandrola says about
this:
"I see this often in athletes. It might happen during a big training block or
immediately afterwards. Of course, my theory is that PVCs associate with excess
inflammation. The reason I see inflammation as the link is because PVCs often occur
in patients who are exposed to stress. The middle-aged person going through a
divorce, the doctor embroiled in a lawsuit, the minister who takes care of everyone
but himself, the grad student during exams. The theme here is that PVCs tend to
cluster at times of high inflammation–be it physical, mental or emotional..."
"Recently, a cycling friend told me his PVCs had resolved almost as soon as he
stopped training for races. He still rides, fast at times, but doesn‟t „train.‟ (I‟m not
advocating not racing; it‟s just an anecdote.)"
4. PVC's could potentially be aggravated by dietary deficiencies. For example, Dr.
Mandrola says that he has had some patients report benefit from magnesium
supplementation, and Dr. Mark Sircus said the same thing when I interviewed him on
the podcast episode "The Shocking Information About A Compound That
Pharmaceutical Companies Really Don’t Want You to Know About." I referenced that
episode again in a follow-up audio recording I did entitled "How To Avoid Sudden
Heart Attacks While Running". While electrolytes may matter less than Gatorade
would have you to believe, they're certainly important for heart health and electrical
conductivity in hard charging athletes, and in an era of mineral-depleted diets and
excessive stress and over-exercise, I suspect deficiencies such as magnesium are a
much bigger contributor to the problem than many people might think (yet another
reason why I slather my body with magnesium oil after every hard workout).

In a nutshell, you can think of PVC's as a canary in the mine. As a matter of fact,
in this helpful forum discussion on MedHelp, it's pointed out that two conditions are known
to cause PVCs during exercise - one is coronary artery disease and the other is myocarditis
(heart "inflammation"), and both are often aggravated by excess adrenaline (e.g. stress
and/or overtraining) and poor exercise conditions. But in the absence of these two factors,
PVC's may actually be no big deal at all.
--------------------------------------------
Now of course, there are other potential cardiovascular concerns that go above and beyond
palpitations or PVC's. From leaky valves to an enlarged heart wall, I discuss many of these
other heart issues in the chapter "Are Endurance Sports Unhealthy".
In that chapter, I also address potentially disturbing findings by researchers like Dr. James
O' Keefe (famous for his TED Talk video "Run for your life! At a comfortable pace, and not
too far."), and point out the balanced evidence on the other side of the fence produced by
Armi Legge in his articles "Does Cardio Cause Heart Disease" and "10 Reasons Why a Large
Athlete’s Heart is Usually Not Dangerous".
Ultimately, if you don't have time to read the links above, the take-away message is this:
Even though exercise is generally good for your health and your
heart, there's some evidence that high amounts of exercise - especially long
bouts of endurance exercise - could potentially be bad for your heart,
especially when combined with lifestyle stress, difficult exercise conditions
such as extreme heat, nutrient and electrolyte depletion, and genetic risk
factors for heart disease.
And with my combination of PVC's, my history of intense and often excessive exercise, and
my very high cortisol levels from a fast-paced lifestyle, I didn't want to take any chances.
So what action did I personally take?
It was this sage advice from the Dr. Mandrola article on PVC's that led me to take the next
step:
"A basic medical evaluation can exclude significant structural heart disease."
In other words, there must be some kind of a test or medical evaluation of my heart that
could tell me whether or not I was at risk of dropping dead during my next Ironman and

leaving behind a lonely wife and two fatherless boys - or whether my PVC's were simply
normal and harmless occurrences.
It was this line of thinking that got me on the phone with the Spokane Heart Institute to
schedule an appointment with local cyclist and cardiologist named Dr. Timothy Bishop.
--------------------------------------------
Dr. Bishop is a slim, fit, bespectacled man, and I could tell as soon as he walked into the
room that he was a seasoned cyclist and health enthusiast. In other words, this wasn't some
out-of-shape doc who didn't know a running shoe from a loafer.
I inwardly pumped my fist that I got hooked up with a doc who knew exercise, and then I
proceeded to spill the beans on my heart palpitations, my concerns, the James O' Keefe
findings, and the recent Wall Street Journal article "The Exercise Equivalent of a
Cheeseburger". I also filled Dr. Bishop in on the fact that I am an author writing a book on
endurance sports, and specifically interested in the potentially deleterious effect of exercise
on the heart, including the potential for increased risk of arrhythmias and coronary artery
disease in athletes who participate in extreme endurance events.
Dr. Bishop was very careful to lay out both sides of the "exercise is bad for your heart"
argument.
And he really knew his stuff.
He explained all the recent findings and recently published data on potential for heart risks
in endurance athletes, laid out both sides of the argument in a balanced way, and ended by
emphasizing that in most cases, in a relatively sedentary society, we're probably doing more
harm than good by warning people away from exercising.
In other words, the last thing a couch potato needs to hear is that if they go for a long walk
they're going to have a heart attack.
Point well taken.
"But Dr. Bishop," I explained, "Let's just say, hypothetically, that a guy like me who has
been beating up his body for 10 years wanted to get some peace of mind? Can't I just get
some tests to find out if there are any issues with my heart?"

The doctor pushed up his glasses, "Ben - if you were showing serious signs of heart
problems, I'd be happy to test you. But if I ran a battery of expensive medical tests on every
person who waltzed in wanting to get their heart evaluated out of sheer curiosity, I would
technically be practicing medicine irresponsibly and potentially misusing the medical
system and simply racking up unnecessary expenses."
Once again, point well taken.
But I kept pressing, "But doctor, let's just say, hypothetically, that I were going to get tested
to get some peace of mind. What would you do?"
Dr. Bishop then took a deep dive into the rabbit hole, explaining the huge battery of
available heart testing options, including:
1. A CT scan of the heart, in which you get injected with an intravenous dye
(iodine) and then your heart is scanned using a high speed CT scanner, allowing
the assessment of blood flow to their heart muscle, and visualization of the heart
anatomy, coronary circulation, calcium buildup in the arteries, and detailed
information about vessels surrounding and coming in and out of the heart
(which includes the aorta, pulmonary veins, and arteries).
2. An exercise electrocardiogram, also known as a stress ECG, which provides
information about how the heart responds to exertion. It usually involves
walking on a treadmill or pedaling a stationary bike at increasing levels of
difficulty, while your heart's electrical activity, heart rate, and blood pressure
are monitored - and is especially good at detecting PVC's or other arrhythmias.
3. A transthoracic echocardiogram, which is a heart test similar to X-ray, but
without the radiation. The procedure uses the same technology used to evaluate
a baby's health before birth (AKA an ultrasound). A hand-held device called a
transducer is placed on the chest and transmits high frequency sound waves
which bounce off the heart structures, producing images and sounds that can be
used by the doctor to detect heart damage, wall thickness, heart size, valve
function or significant scarring (admittedly, this test won't pick up some of the
less significant scarring raised in some of the concerning articles about mild
heart scarring from endurance exercise, but will at least show areas of serious
damage).
4. Cardiac catheterization (also called cardiac cath or coronary angiogram),
which is a relatively invasive imaging procedure in which a long, narrow tube
called a catheter is inserted into a blood vessel in your arm or leg and guided to
your heart with the aid of a special X-ray machine. Contrast dye is injected
through the catheter so that X-ray videos of your valves, coronary arteries, and
heart chambers can be created.

5. MRI (magnetic resonance imaging). An MRI uses large magnets and radio-
frequency waves to produce pictures of the body's internal structures. This
technique obtains information about the heart as it is beating, creating images
of the heart throughout its pumping cycle. Although expensive and a bit more
difficult to get, an MRI can evaluate the anatomy and function of the structures
of the chest, including the heart, lungs, major vessels, and pericardium (the
outside lining of the heart). It is also used to determine the presence of diseases
such as coronary artery disease, pericardial disease, cardiac tumors, heart
valve disease, heart muscle disease (cardiomyopathy), and congenital heart
disease. A sample of an image from an MRI is below:

At this point, my head was spinning with the options. I had originally figured we
could just do something as simple as throw me on a treadmill, have me run for a little while
with a few cables attached to my chest, and call it good.
I leaned forward in the office chair, "OK, doc, so let's say I want to find out if I've actually
done any damage to my heart over the past few years, and discover if I maybe, just might
happen to be one of these walking statistics who has a perfect storm going on in my chest
that could lead to me dropping dead during Ironman Hawaii in 4 weeks? What could I do?"
Turns out the options were:
A) fly to some extremely expensive concierge medical facility, like the Princeton Longevity
Center, and pay some booka bucks for whatever test I'd care to throw money at (I wasn't
extremely keen to explain that expense to my wife)...
B) call around to a variety of medical research institutes or academic institutions such as
University of Washington and try to get into a heart study in which they use an MRI or
one of the other fancier tests...
C) stay in my own backyard and get tested by Dr. Bishop at the Spokane Heart Institute
using their standard heart preventive testing equipment - namely a stress ECG and an
echocardiogram...
Option C was sounding like a reality, and like something I may be able to actually pull off in
a timely fashion before Ironman, so I pressed on...
"So Dr. Bishop, if we just take into consideration those heart palpitations I had during my
long run, we could technically justify doing some like an ECG and ultrasound, right?"
Having filled me in on all the options, the reality of the situation, the fact that I was
probably just fine, and potential expenses associated with the test, Dr. Bishop finally gave
in. He nodded yes.
And just like that, within 5 minutes I was outside in the hallway scheduling with the
receptionist to show up at the downtown hospital that Friday at the ungodly hour of
7:00am for a heart ultrasound and a treadmill stress test.
-----------------------------------------

That Friday, my alarm blared at 5:30am. I rolled out of bed, and opted for a cup of
decaffeinated coffee, just to avoid any potential effects of caffeine on my heart rhythm, then
hopped in my pickup truck and headed downtown.
The ultrasound came first, and it was actually a bit surreal to both feel my heart in my chest,
but also see it up there on the computer screen. Up to this point, my only experience with
the stereotypical black and white ultrasound monitor was having watched my twin baby
boys wriggle around in mom's tummy. And now it was my heart up there on the screen
instead, wriggling, churning, pumping, sucking, pushing, pulling and pumping in my chest
as the ultrasound technician darted his magic wand around my chest - measuring valve size,
wall thickness, and the size of my four primary heart chambers -the right and left atria and
right and left ventricle.
The ultrasound (AKA transthoracic echocardiogram) looks like this:
Within 30 minutes, the technician was finished and my heart was all measured up.
Next, came the treadmill stress test, which was a bit more involved than simply lying on a
table while a technician gave me a free chest massage.
For this test, I stripped down to my running shorts, threw on my running shoes, shocked
the nurses with my resting heart rate of 29 beats per minute, and then had 8 "leads"
attached to my chest and abdomen to measure electrical activity in my heart while I ran on

the treadmill - beginning at an easy pace and progressing in speed and incline to gradually
harder intensities until I reached close to maximum capacity.
I suspected I was perhaps not the stereotypical test subject for the Spokane Heart Institute
when the nurses began discussing whether or not the treadmill was actually going to go any
faster or higher.
In other words, they'd never seen anyone take this test to the red-hot intensity I took it.
But I really wanted to push to the limits and ensure my heart was truly "stressed" during
this test. After all, I didn't want useless, walk-in-the-park data. So I stared at the cold wall
and pounded away for 21 and half minutes - up to an 18% incline on the treadmill.
That's not my focused mugshot in the photo below, but it's a pretty good picture of what a
treadmill stress test actually looks like once you're all hooked up to the cables (albeit in the
early stages, before the real torture begins).
And that was it.
Within 2 hours, I was all wrapped up, and headed over to my follow-up meeting with Dr.
Bishop, who was waiting with all my results in hand.

-----------------------------------------
So what did we actually find out?
Dr. Bishop summed things up pretty quickly in his post-test meeting with me. It went like
this:
1. The ultrasound showed that my heart was structurally sound with zero concerning
defects. The technician actually described my heart as a "textbook image" (I kept my
fingers crossed that he wasn't talking about the bad part of the textbook).
2. The ultrasound did indeed show that I have a mildly enlarged right and left atrium (the
upper heart chambers), but the size is still completely typical and well within range of a
normal "athlete's heart"*. My left and right ventricle and heart wall thickness were within
normal limits, with no evidence of significant scarring.
3. During the exercise stress test, I achieved 19.2 METS which according to the report,
represents a "new Spokane Cardiology record for exercise tolerance". Although there were
occasional PVC's during the test, they were completely benign, normal and within limits,
and there were no exercise-induced arrhythmias or heart rhythm changes concerning for
myocardial ischemia (e.g. I wasn't going to drop dead of a heart attack from the type of
rhythms I experience at high exercise intensities).
4. One of my heart valves - the pulmonic valve - show trace "regurgitation", or just a bit of
backflow, which Dr. Bishop explained was completely normal and quite common, with no
cause for concern.
And then, we shook hands, he told me to swing by anytime if I had more
questions, and I was happily driving home for breakfast.
*As you can read in the well-researched post on athlete's heart at Impruvism.com, there is
no evidence showing that an enlarged athlete‟s heart leads to long-term disease
progression, cardiovascular disability, or sudden cardiac death - as is backed up in a
paper by Dr. Barry Maron, the author of this excellent review on athlete‟s heart. The idea
that extreme athlete‟s heart could be harmful in some cases “is perhaps unlikely but at this
time cannot be excluded with certainty.” There‟s also little evidence that having an
enlarged heart is going to make you much healthier. It‟s unlikely that a marathon runner
is going to have a healthier heart than someone who lifts weights a few times a week and
stays active with other light activity. So ultimately, there‟s not much evidence having a
large, athlete‟s heart is bad or good for you.

Finally, you might be wondering about the actual cost of all this testing. At the time of this
writing, I haven't received the final bill, nor do I know how much of the damage my
catastrophic health insurance will pick up vs. what I'll end up needing to personally shell
out of my Health Savings Account, but I have to admit...
...the peace of mind from testing my heart was well worth it, no matter what
the cost. When I'm charging down the lava fields during Ironman Hawaii next
week, it will be nice to know that my ticker is going to keep on ticking.
-----------------------------------------
So when it comes to whether or not endurance exercise is bad for your heart, what's the
final take-away message for you and me?
A) Ultimately, it doesn't look like ten years of extreme endurance exercise, including
oodles of bodybuilding, hardcore, marathon-esque workouts, marathons, long distance
cycling, high intensity interval training and Ironman triathlon has done much damage at
all to my heart. I've got arteries like firehoses, actually - and extremely low resting heart
rate, low blood pressure and a normal heart structure.
B) If you're experiencing heart palpitations or you're worried about other heart issues, the
most important steps you can take are to minimize lifestyle stress, take care to recover
properly after your exercise sessions, avoid overtraining and underrecovery,
consume adequate water, nutrients, vitamins, antioxidants, and
electrolytes (especially magnesium) and accept the fact that you may be taking risks by
putting your body into stressed-out "running from a lion" mode when you're in
excessively hot conditions.
C) If you really want true peace of mind, go get a test like I did. You may need to press a
little to actually get your doctor to order one. Heck, you may even need to make things
sound just slightly worse than they actually are if it helps you get the preventive test
you're looking for. If money isn't an issue and you want the gold standard heart test, find
a longevity institute or concierge medical facility and opt for a full body CT Scan or gated
MRI. But if you need something quick, convenient and not quite as costly, you can get a
heck of a lot of information from a stress EKG and echocardiogram like I did.
Finally, if you want the nitty-gritty details and to download the full .pdf results and official
medical report from my visit with Dr. Bishop - as well as see my follow-up heart scan and
treadmill stress test results - then here's how you can do it:

I just published the entire medical report on BenGreenfieldFitness Premium
channel, and you can click here to go Premium and to check it out
now. Premium is just ten bucks *a year* and includes a secret vault with
dozens of other hidden articles, videos and podcasts that you can access from
your phone, your tablet and your computer. If you want to dig into the nitty-
gritty medical report, see what the results of a hard stress EKG looks like, get
more details on the structure of the heart of a guy who's been beating himself
up with endurance sports for the past decade, are still curious about the
results of the whole heart testing process, or just want more insider content,
I'd highly recommend you click here to go Premium.
And thanks for reading!
To Your Health,
Ben Greenfield
-----------------------------------------