Basic principles of treatment of breaks of he overhead extremities and spine.
21
Basic principles of Basic principles of treatment of breaks treatment of breaks of he overhead of he overhead extremities and extremities and spine. spine. Tutor: Kostiv S. Ya. Tutor: Kostiv S. Ya.
-
Upload
mackensie-short -
Category
Documents
-
view
36 -
download
0
description
Basic principles of treatment of breaks of he overhead extremities and spine. Tutor: Kostiv S. Ya. SPINAL TRAUMA. C1 Fractures. The upper cervical spine is defined by the 2 most cephalad cervical vertebrae, C1 (the atlas) and C2 (the axis) - PowerPoint PPT Presentation
Transcript of Basic principles of treatment of breaks of he overhead extremities and spine.

Basic principles of Basic principles of treatment of breaks treatment of breaks
of he overhead of he overhead extremities and spine.extremities and spine.
Tutor: Kostiv S. Ya.Tutor: Kostiv S. Ya.

SPINAL TRAUMASPINAL TRAUMA

C1 FracturesC1 Fractures
• The upper cervical spine is defined by the 2 The upper cervical spine is defined by the 2 most cephalad cervical vertebrae, C1 (the most cephalad cervical vertebrae, C1 (the atlas) and C2 (the axis)atlas) and C2 (the axis)
• Jefferson originally described this type of C1 Jefferson originally described this type of C1 fracture in 1920. The principal treatment is fracture in 1920. The principal treatment is with a halo and vest or cast, which remains with a halo and vest or cast, which remains an effective current treatment for many of an effective current treatment for many of these fractures.these fractures.
• Fractures of the atlas compromise 25% of Fractures of the atlas compromise 25% of atlantoaxial complex bony injuries, 10% of atlantoaxial complex bony injuries, 10% of cervical spine injuries, and 2% of all spine cervical spine injuries, and 2% of all spine injuriesinjuries

EtiologyEtiology• The Jefferson fracture most commonly occurs as the The Jefferson fracture most commonly occurs as the
result of axial loading on the head through the result of axial loading on the head through the occiput, leading to a burst-type fracture of C1. Diving occiput, leading to a burst-type fracture of C1. Diving is the most frequent cause of this fracture, when it is the most frequent cause of this fracture, when it results from striking the head on an obstacle in results from striking the head on an obstacle in shallow water; hence, the national program "Feet shallow water; hence, the national program "Feet first, first time" (North American Spine Society, 2005) first, first time" (North American Spine Society, 2005) provides a motto for diving in unknown waters or provides a motto for diving in unknown waters or shallow collections of water and has been an effective shallow collections of water and has been an effective deterrent. The next most frequent cause of this deterrent. The next most frequent cause of this fracture is being thrown up against the roof of a fracture is being thrown up against the roof of a motor vehicle, a car or bus, or even an aircraft, and motor vehicle, a car or bus, or even an aircraft, and the forces are distributed to the body through the the forces are distributed to the body through the neck. The third most frequent cause of these injuries neck. The third most frequent cause of these injuries is falls onto the head, except in toddlers, who are is falls onto the head, except in toddlers, who are predisposed to injury from falls because of their predisposed to injury from falls because of their disproportionate head size.disproportionate head size.

ClinicalClinical
• Patients with a complete spinal cord injury and Patients with a complete spinal cord injury and no neurologic function continue to have only no neurologic function continue to have only sensation on the face and motor control of the sensation on the face and motor control of the facial muscles from the cranial nerves. A facial muscles from the cranial nerves. A tracheostomy is essential because the patient tracheostomy is essential because the patient requires respiratory assistance and a volume requires respiratory assistance and a volume respirator. If the C3-5 area is intact, the phrenic respirator. If the C3-5 area is intact, the phrenic nerve may often be stimulated to contract the nerve may often be stimulated to contract the diaphragm. If stimulation of the phrenic nerve diaphragm. If stimulation of the phrenic nerve does not contract the diaphragm, then the does not contract the diaphragm, then the spinal cord is no longer functioning; the cell spinal cord is no longer functioning; the cell body is dead, and a phrenic electrical stimulator body is dead, and a phrenic electrical stimulator is not effective.is not effective.
Imaging StudiesImaging Studies
• Cervical spine radiographs Cervical spine radiographs • ArteriographyArteriography
Medical therapyMedical therapy• Patients with C1 fractures customarily have some form Patients with C1 fractures customarily have some form
of trauma; thus, they need to be immediately stabilized of trauma; thus, they need to be immediately stabilized at the scene, which requires the customary attention to at the scene, which requires the customary attention to the ABCs (airway, breathing, and circulation). If the the ABCs (airway, breathing, and circulation). If the airway is compromised or air exchange is inadequate, airway is compromised or air exchange is inadequate, intubation without moving the head is crucial (C-spine intubation without moving the head is crucial (C-spine protection). Careful evaluation and frequent protection). Careful evaluation and frequent reassessment is needed because the patient may have reassessment is needed because the patient may have sustained a concussion with the impact to the head (the sustained a concussion with the impact to the head (the common injury that produces the C1 fracture) and, common injury that produces the C1 fracture) and, because of a clouded sensorium, may not be able to be because of a clouded sensorium, may not be able to be fully evaluated or to report neck pain. Patients with a fully evaluated or to report neck pain. Patients with a diminished alertness and orientation should carefully diminished alertness and orientation should carefully undergo imaging studies to exclude underlying undergo imaging studies to exclude underlying pathology.pathology.

Surgical therapySurgical therapy
• Treatment of the C1 fracture consists of Treatment of the C1 fracture consists of stabilization or immobilization in a satisfactorily stabilization or immobilization in a satisfactorily reduced position to allow reliable healing. This reduced position to allow reliable healing. This illustrates the necessity of identifying illustrates the necessity of identifying associated injuries; for example, if a Jefferson associated injuries; for example, if a Jefferson fracture is identified but an associated odontoid fracture is identified but an associated odontoid fracture, transverse ligament fracture, or other fracture, transverse ligament fracture, or other problem is present, then halo treatment may be problem is present, then halo treatment may be modified or less successful. The transverse modified or less successful. The transverse ligament is not necessarily expected to heal ligament is not necessarily expected to heal tightly or reliably, although a bony fracture tightly or reliably, although a bony fracture would be expected to have mechanical integrity would be expected to have mechanical integrity restored when healedrestored when healed

Fracture of the C1 ring may result in lateral Fracture of the C1 ring may result in lateral displacement and subsequent overhang on the displacement and subsequent overhang on the
open mouth view in radiographsopen mouth view in radiographs

Computed tomography Computed tomography scanning is often best to scanning is often best to
visualize C1 ring fracturesvisualize C1 ring fractures

Computed tomography sagittal Computed tomography sagittal views can be used to evaluate the views can be used to evaluate the
atlantodens interval or to visualize atlantodens interval or to visualize C1 fractures.C1 fractures.
C2 FracturesC2 Fractures• Cervical spine (C-spine) injuries are the most feared Cervical spine (C-spine) injuries are the most feared
of all spinal injuries because of the potential for of all spinal injuries because of the potential for significant deleterious sequelae. Correlation is noted significant deleterious sequelae. Correlation is noted between the level of injury and morbidity/mortality between the level of injury and morbidity/mortality (ie, the higher the level of the C-spine injury - the (ie, the higher the level of the C-spine injury - the higher the morbidity and mortality). Craniocervical higher the morbidity and mortality). Craniocervical junction injuries are the deadliest.junction injuries are the deadliest.
• As many as 10% of unconscious patients who present As many as 10% of unconscious patients who present to the emergency department following a motor to the emergency department following a motor vehicle accident (MVA) have C-spine pathology. vehicle accident (MVA) have C-spine pathology. MVAs and falls are responsible for the bulk of C2 MVAs and falls are responsible for the bulk of C2 fractures. The clinical manifestations range from fractures. The clinical manifestations range from asymptomatic to frank paralysis. This article focuses asymptomatic to frank paralysis. This article focuses on the uniqueness of and the most common types of on the uniqueness of and the most common types of traumatic C2 (axis) fractures.traumatic C2 (axis) fractures.
Neurologic assessment of Neurologic assessment of C2 fractures (C2 nerve C2 fractures (C2 nerve
root)root)• Motor: Muscles that have a contribution from Motor: Muscles that have a contribution from
the C2 nerve root include the the C2 nerve root include the sternocleidomastoid, trapezius, longus capitis, sternocleidomastoid, trapezius, longus capitis, longus colli, rectus capitis anterior, splenius longus colli, rectus capitis anterior, splenius capitis, splenius cervicis, and semispinalis capitis, splenius cervicis, and semispinalis capitis. capitis.
• Sensory: The posterior scalp, anterolateral Sensory: The posterior scalp, anterolateral neck, anteroinferior and posteroinferior neck, anteroinferior and posteroinferior external ear and C2 sensory innervation sites. external ear and C2 sensory innervation sites.
• Reflexes: For the sternocleidomastoid (SCM) Reflexes: For the sternocleidomastoid (SCM) reflex, tap on the clavicular end and the reflex, tap on the clavicular end and the muscle contracts.muscle contracts.

Clinical examination Clinical examination includes the following:includes the following:
• Observe and palpate for deformities and Observe and palpate for deformities and step-offs step-offs
• Muscle strength and tone of upper and Muscle strength and tone of upper and lower extremities lower extremities
• Sensory testing of upper and lower Sensory testing of upper and lower extremities extremities
• Rectal examination Rectal examination • Shrugging the shoulders to test trapezius Shrugging the shoulders to test trapezius
muscle muscle • Observe for torticollisObserve for torticollis
Odontoid fracturesOdontoid fractures• Type I fracture Type I fracture • A type I fracture (less than 5% of cases) is an oblique fracture through A type I fracture (less than 5% of cases) is an oblique fracture through
the upper part of the odontoid process.the upper part of the odontoid process.• This type of fracture occasionally is associated with gross instability This type of fracture occasionally is associated with gross instability
due to traction forces applied to, and subsequent injury of, the apical due to traction forces applied to, and subsequent injury of, the apical and/or alar ligaments.and/or alar ligaments.
• This is an avulsion injury to the tip of the odontoid and is usually This is an avulsion injury to the tip of the odontoid and is usually stable.stable.
• Type II fracture: A type II fracture (more than 60% of cases) is a Type II fracture: A type II fracture (more than 60% of cases) is a fracture occurring at the base of the odontoid as it attaches to the fracture occurring at the base of the odontoid as it attaches to the body of C2 (see Image 1).body of C2 (see Image 1).
• Type III fracture Type III fracture • A type III fracture (30% of cases) occurs when the fracture line A type III fracture (30% of cases) occurs when the fracture line
extends through the body of the axis.extends through the body of the axis.• The fracture line can extend laterally into the superior articular facet The fracture line can extend laterally into the superior articular facet
for the atlas.for the atlas.• Another type of odontoid process fracture is a vertical fracture Another type of odontoid process fracture is a vertical fracture
through the odontoid process and body of the axis (less than 5% of through the odontoid process and body of the axis (less than 5% of cases). This type of fracture often is considered a variant of a cases). This type of fracture often is considered a variant of a traumatic spondylolisthesis of C2, which is discussed below.traumatic spondylolisthesis of C2, which is discussed below.
• C2 lateral mass fracturesC2 lateral mass fractures• C2 extension teardrop fracturesC2 extension teardrop fractures
Traumatic spondylolisthesis Traumatic spondylolisthesis of C2 (hangman fracture)of C2 (hangman fracture)
• Type I fractures Type I fractures • Type I fractures (29%) are bilateral pedicle fractures with less than 3 mm of anterior C2 body Type I fractures (29%) are bilateral pedicle fractures with less than 3 mm of anterior C2 body
displacement and no angulation.displacement and no angulation.• The mechanism of this injury is hyperextension with concomitant axial loading and a force sufficient The mechanism of this injury is hyperextension with concomitant axial loading and a force sufficient
enough to cause the fracture but not enough to disrupt the anterior longitudinal ligament (ALL), posterior enough to cause the fracture but not enough to disrupt the anterior longitudinal ligament (ALL), posterior longitudinal ligament (PLL), nor the C2/C3 disk.longitudinal ligament (PLL), nor the C2/C3 disk.
• The integrity of the C2/C3 disk, ALL, and PLL determines the stability of the injury, and with these The integrity of the C2/C3 disk, ALL, and PLL determines the stability of the injury, and with these elements intact, the injury is considered stable.elements intact, the injury is considered stable.
• Commonly associated concomitant injuries are C1 posterior arch fractures, C1 lateral mass fractures, and Commonly associated concomitant injuries are C1 posterior arch fractures, C1 lateral mass fractures, and odontoid fractures.odontoid fractures.
• Type II fractures Type II fractures • Type II fractures (56%) demonstrate significant displacement and angulation.Type II fractures (56%) demonstrate significant displacement and angulation.• The mechanism of this injury is 2-fold; hyperextension with concomitant axial loading, followed by flexion The mechanism of this injury is 2-fold; hyperextension with concomitant axial loading, followed by flexion
with concomitant axial compression.with concomitant axial compression.• The resultant injury pattern is bilateral pedicle fractures with slight disruption of the ALL and significant The resultant injury pattern is bilateral pedicle fractures with slight disruption of the ALL and significant
disruption of the PLL and C2/C3 disk. This injury is considered unstable.disruption of the PLL and C2/C3 disk. This injury is considered unstable.• A wedge compression fracture of C3 is the most common associated injury.A wedge compression fracture of C3 is the most common associated injury.• Type IIA fractures Type IIA fractures • Type IIA fractures (6%) demonstrate no anterior displacement, but there is severe angulation.Type IIA fractures (6%) demonstrate no anterior displacement, but there is severe angulation.• The mechanism for this injury is flexion with concomitant distraction. The resultant injury pattern is The mechanism for this injury is flexion with concomitant distraction. The resultant injury pattern is
bilateral pedicle fractures with C2/C3 disk disruption and some degree of insult to the PLL. This is an bilateral pedicle fractures with C2/C3 disk disruption and some degree of insult to the PLL. This is an unstable fracture.unstable fracture.
• Radiographs taken while the patient is in cervical traction demonstrate an increase in the C2/C3 posterior Radiographs taken while the patient is in cervical traction demonstrate an increase in the C2/C3 posterior disk space.disk space.
• Type III fractures Type III fractures • Type III fractures (9%) demonstrate severe displacement and severe angulation.Type III fractures (9%) demonstrate severe displacement and severe angulation.• The mechanism of this injury is flexion with concomitant axial compression.The mechanism of this injury is flexion with concomitant axial compression.• The resultant injury pattern demonstrates not only bilateral pedicle fractures with C2/C3 disk disruption, The resultant injury pattern demonstrates not only bilateral pedicle fractures with C2/C3 disk disruption,
but also concomitant unilateral or bilateral C2/C3 facet dislocations.but also concomitant unilateral or bilateral C2/C3 facet dislocations.• Varying degrees of injury occur to the ALL and PLL. This is an unstable fracture.Varying degrees of injury occur to the ALL and PLL. This is an unstable fracture.• A relatively high incidence of mortality and morbidity is noted with this injury, particularly neurologic A relatively high incidence of mortality and morbidity is noted with this injury, particularly neurologic
sequela.sequela.
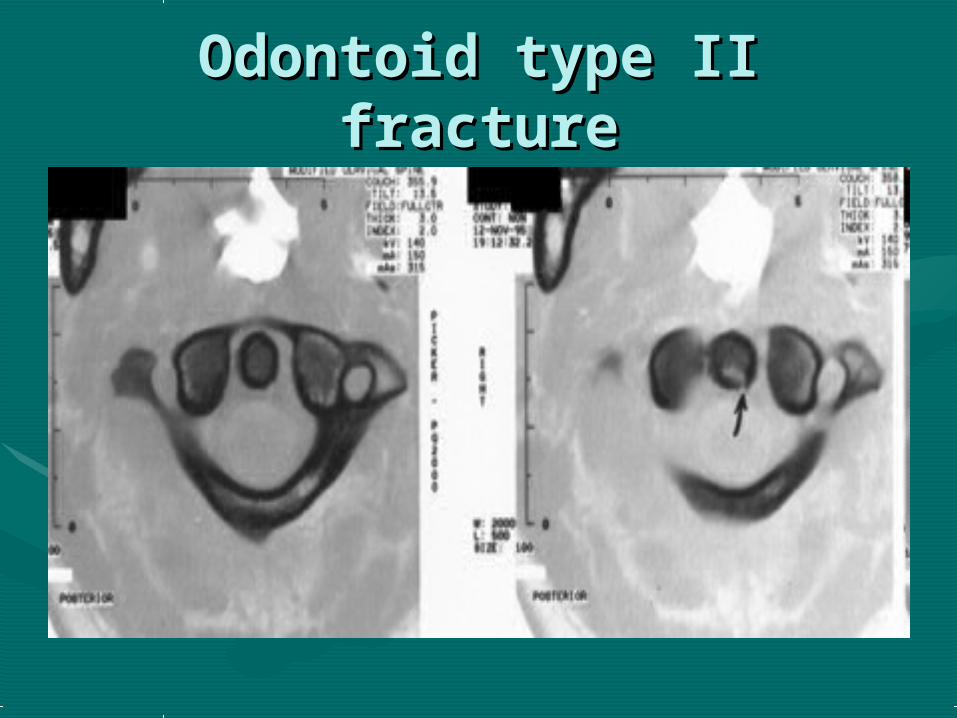
Odontoid type II fractureOdontoid type II fracture
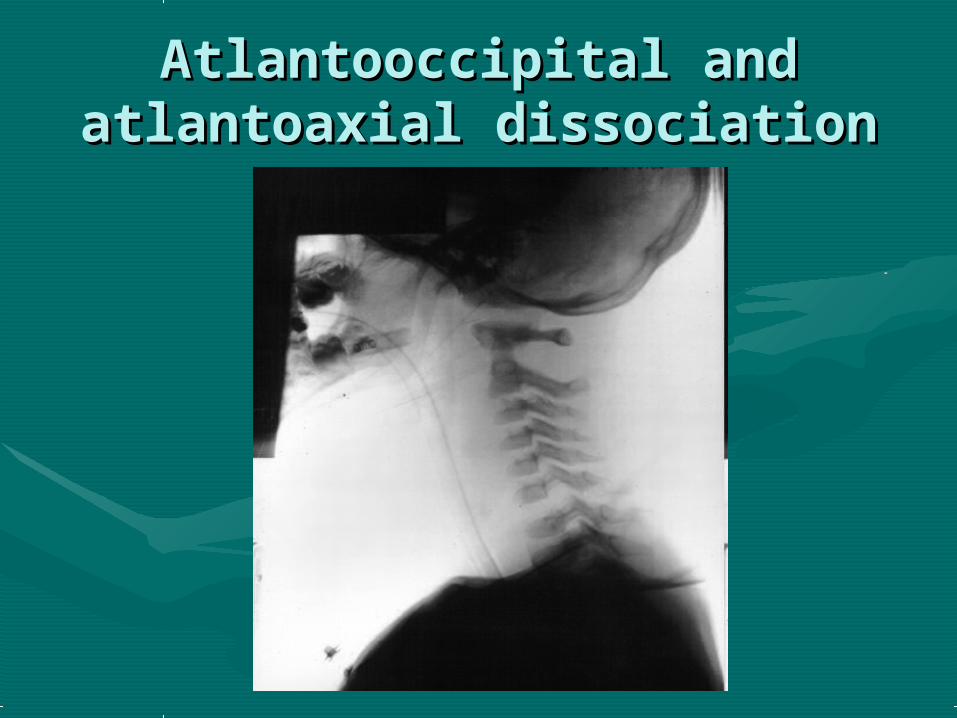
Atlantooccipital and Atlantooccipital and atlantoaxial dissociationatlantoaxial dissociation
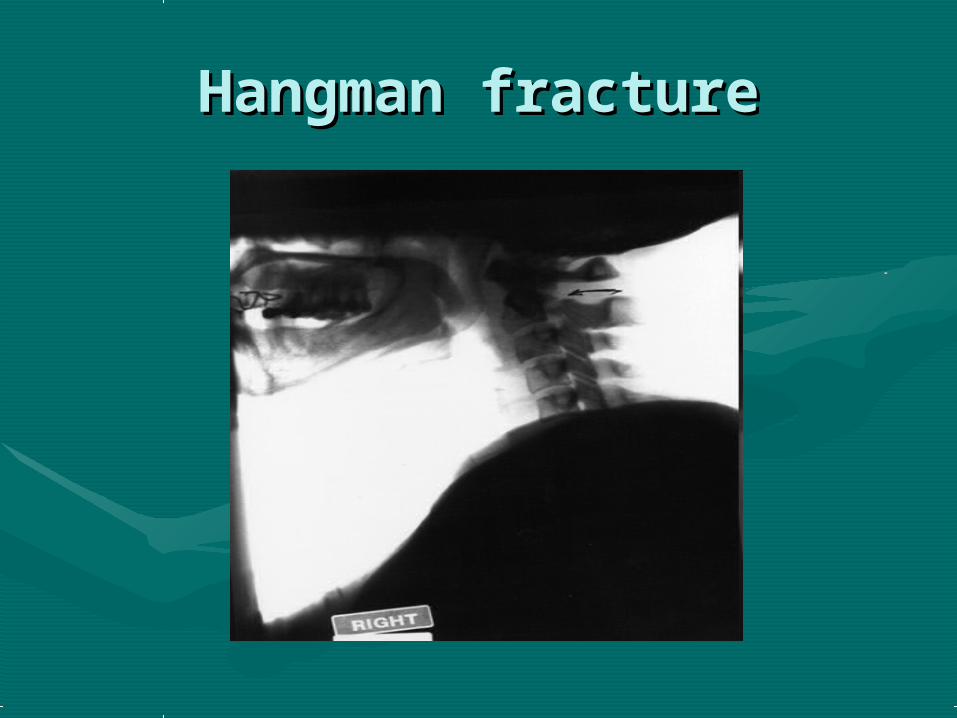
Hangman fractureHangman fracture

Three types of C2 odontoid fractures: type I is an Three types of C2 odontoid fractures: type I is an oblique fracture through the upper part of the odontoid oblique fracture through the upper part of the odontoid
process; type II is a fracture occurring at the base of process; type II is a fracture occurring at the base of the odontoid as it attaches to the body of C2; type III the odontoid as it attaches to the body of C2; type III
occurs when the fracture line extends through the body occurs when the fracture line extends through the body of the axis.of the axis.