Basic principles of endodontics
57
-
Upload
tess-boto -
Category
Health & Medicine
-
view
556 -
download
5
description
smear layer
Transcript of Basic principles of endodontics



I ASEPSIS AND INFECTION CONTROLII TERMINOLOGYIII OBJECTIVES OF INFECTION CONTROLIV PRINCIPLES OF INFECTON CONTROLV PATIENT EVALUATONVI PATIENT PREPARATIONVII PREPARATION OF THE OPERATORY (INFECTION CONTROL)VII CLASSIFICATION OF INSTRUMENT STERILIZATION - CRITICAL ITEMS -SEMI CRITICAL ITEMS - NON CRITICAL ITEMSIX PREOPERATIVE STERILIZATION AND DISINFECTIONX BARRIER TECHNIQUESXI ROCEDURAL TECHNIQUES (TOOTH ISOLATION)XII IMMUNIZATION

ASEPSIS AND INFECTION CONTROL
Endodontics has long emphasize the importance of aseptic techniques using sterilized instruments, disinfecting solutions such as sodium hypochlorite and rubber dam barriers. Traditionally Hepatitis B has been the benchmark disease on which infection control has been based. In an office that treats 20 patient a day the personnel can expect to encounter active carrier of Hepatitis B virus (HBV) every 7 working days. In addition one can expect exposure to a patient with oral herpes and unknown number of patient infected with Human immuno deficiency virus(HIV).

The transmission route of HIV /HBV is primarily through the exchange of blood. Percutaneous injury to the dentist is the most direct patient-to-dentist transmission method. Percutaneous injuries to dentist are caused by burs (37%), syringe needle(30%), sharp instruments(21%), orthodontic wires(6%), suture needles(3%), scalpel blades(1%), and other object(2%).
Dental Professionals are exposed to wide variety of microorganisms, in the blood and saliva of the patient, making infection control procedure outmost importance. The common goal of infection control is to eliminate or reduce number of microbes shared between the people. The procedures of infection control must not only protect patient and the dental team from contracting infections during dental procedures, but also reduce the number of microorganism in the immediate dental environment to the lowest level possible.

STERILIZATION- the process that destroys all types and forms of microorganism,including viruses,bacteria fungi, and bacterial endospores. Applies to instruments not on skin where antiseptic can only be achieved. Includes: steam autoclave, dry heat, chemical vapor under pressure, ethylene oxide gas, and immersion in liquid chemical disinfectant / sterilizers.
DISINFECTIONS- a process less lethal than sterilization it means reducing the number of viable microorganism present in a sample.
Three levels: -High level disinfection- a process that can kill some
but not necessarily all, bacterial spores. It is tuberculocidal, and if the disinfectant is capable of destroying bacterial spores it is termed as sporicidal.

- Intermediate level of disinfection - a process that is capable of killing mycobacterium tuberculosis, HBV and HIV it may not be capable of killing bacterial spores.
- Low level disinfection- kills most bacteria, some fungi, and some viruses. It does not kill M.tuberculosis or bacterial spore.
BACTERICIDAL- a process or an agent that destroys bacteria. BACTERIOSTATIC- a process or an agent that inhibits growth or
multiplication of bacteria. CONTAMINATION- the introduction of an infectious agent into an
area. BIOMEDICAL WASTE - waste that has been generally or has been
used in the diagnosis, treatment, or immunization of human being or animals. May contain infectious agents and may pose substantial threat to health.

BIOHAZARDOUS WASTE – also called infectious waste or biomedical waste, is any waste containing infectious materials or potentially infectious substance. Includes laboratory waste, specimens sent to a laboratory for microbiologic analysis, surgical specimen, recognizable fluid and blood elements and sharps.
MEDICAL SOLID WASTE – empty specimen containers, bandages or dressings containing nonliquid blood, surgical globes, treated biohazard waste, and other materials that are not biohazardous.
ANTISEPTIC – a chemical agent that is applied to living tissue to kill microbes.
DISINFECTANT- a chemical or physical agent that is applied to inanimate object to kill microbes.

III OBJECTIVES OF INFECTION CONTROLIII OBJECTIVES OF INFECTION CONTROL
1. Decrease the number of pathogenic microbes to the level where normal body resistance mechanisms can prevent infection. 2. Break the cycle of infection from dentist, assistant and patient and eliminate cross contamination. 3. Treat all patients and instruments as though they could transmit an infectious disease. 4. Protect patient and personnel from infection and protect all dental personnel from the threat of malpractice.

1. Appreciation of basic microbiology and mode of disease transmission.
2. Conscientious hygiene including appropriate hand washing and cleaning of work area, equipments and materials in dental office.
3. Use of recommended sterilization and disinfection procedure.
4. Use of disposable or sterilizable equipments. 5. Surveillance of potentially capable and occasionally
acquired infection.

The identification of patient with transmissible diseases and of those belonging to high risk group is essential before treatment begins.
According to the Center for Disease Control and Prevention (CDC), however because the medical history and examination cannot reliably identify all patients with bloodborne pathogens, blood and body fluid precautions should be consistently used for all patient. The concept stresses that all patients should be assumed to be infectious for HIV and other bloodborne pathogens. The medical history is only an adjunct to patient’s background and cannot be considered a totally inclusive source of information.

PATIENT EVALUATION
In the daily practice of Endodontics, one must frequently re-evaluate the patient’s medical history at least on a yearly basis. With the recent advances in the treatment of medically compromised patients, a greater number of patients will enter the office with immuno-compromised conditions, cardiovascular susceptibility, and a host of other physical limitations that may require special attention. Consultation with attending physicians is most important in proper care of such patient.

Regardless of the specifics of the case, the clinician is responsible for explaining the nature of the treatment and informing the patient of any risks, the prognosis, and other pertinent facts. Because of bad publicity and hearsay, root canal treatment is reputed to be a horrifying experience. Consequently, some patients may be reluctant, anxious, or even fearful of undergoing root canal treatment. Thus it is imperative that the clinician educate the patient before treatment (i.e., “informing before performing”) to allay concerns and minimize misconceptions. Good clinician and patient relationships are built on effective communication. Sufficient evidence suggests that clinicians who establish warm, caring relationships with their patients through effective case presentation are perceived more favorably. These clinicians also have a more positive impact on the patient’s anxiety, knowledge, and compliance than those who maintain impersonal, noncommunicative relationships. Most patients experience increased anxiety while in the dental chair. However, a simple but informative case presentation that answers all questions reduces patient anxiety and solidifies the patient’s trust in the clinician.

Because all dental health care personnel (DHCP), including those not directly involved in patient care, are at risk for exposure to a host of infectious organisms (e.g., influenza; upper respiratory disease; tuberculosis (TB); herpes; hepatitis B, C, D; acquired immunodeficiency syndrome [AIDS]), effective infection control procedures must be used to minimize the risk of cross contamination in the work environment.

1. The ADA and CDC recommend that all DHCP with a potential occupational exposure to blood or other potentially infectious material be vaccinated against hepatitis B.
2. A thorough patient medical history, which includes specific questions about hepatitis, AIDS, current illnesses, unintentional weight loss, lymphadenopathy, and oral soft-tissue lesions, must be taken and updated at subsequent appointments. All patents should be screened for latex allergies, and they should be referred if an allergy is suspected.

3. Dental personnel must wear protective attire and use proper barrier techniques. The standard requires the employer to ensure that employees use personal protective equipment (PPE) and that such protection is provided at no cost to the employee a. Disposable latex or vinyl gloves must be worn when contact with body fluids or mucous membranes is anticipated or when touching potentially contaminated surfaces; they may not be washed for reuse. OSHA requires that gloves be replaced after each patient contact, when torn, or when punctured. If their integrity is not compromised, sturdy, unlined utility gloves for cleaning instruments and surfaces may be decontaminated for reuse. Polyethylene gloves may be worn over treatment gloves to prevent contamination of objects, such as drawers, light handles, or charts.

b. Hands, wrists, and lower forearms must be washed with either a nonantimicrobial soap or antimicrobial soap and water when hands are visibly soiled, after bare-handed touching of inanimate objects likely to be contaminated, before and after treating each patient, before donning gloves, and immediately after removing gloves. An antimicrobial surgical hand scrub should be used for surgical procedures before donning sterile gloves. The standard requires that any body area that has contact with a potentially infectious material, including saliva, must be washed immediately after contact. It is strongly recommended that hand lotions that do not affect glove integrity be used to prevent dryness associated with handwashing. Sinks should have electronic, elbow-, foot-, or knee-action faucet controls for asepsis and ease of function.

c. Masks and protective eyewear with solid side shields or chin-length face shields are required when splashes or sprays of potentially infectious materials are anticipated and during all instrument and environmental cleanup activities. When a face mask is removed, it should be handled by the elastic or cloth strings, not by the mask itself. It is further suggested that the patient wear protective eyewear.
d. Protective clothing, either reusable or disposable, must be worn when clothing or skin is likely to be exposed to body fluids, and it should be changed when visibly soiled or penetrated by fluids.

e. Patients’ clothing should be protected from splatter and caustic materials, such as sodium hypochlorite, with waist-length plastic coverings overlaid with disposable patient bibs.
f. High-volume evacuation greatly reduces the number of bacteria in dental aerosols and should be employed when using the high-speed handpiece, water spray, or ultrasonics.
g. Use of the dental dam as a protective barrier is mandatory for nonsurgical root canal treatment, and failure to use this barrier is considered to be below standard care.

4 Contaminated disposable sharps (e.g., syringes, needles, scalpel blades) and contaminated reusable sharps (e.g., endodontic files) must be placed into separate, leak-proof, closable, puncture-resistant containers. These containers should be colored red or labeled “BIOHAZARD,” and they should be marked with the biohazard symbol. a. The clinician should take the following steps when handling contaminated endodontic files: With tweezers, place used files in glass beaker containing a nonphenolic disinfectant and detergent holding solution. At the end of the day, discard solution and rinse with tap water. Add ultrasonic cleaning solution, and place beaker in ultrasonic bath until thoroughly clean (i.e., 5 to 15 minutes). Discard ultrasonic solution, and rinse with tap water. Pour contents of beaker onto clean towel, and use tweezers to place clean files into metal box for sterilization. Files with any visible debris should be separately sterilized. Once sterilized, these files can be picked up by hand and debrided using 2 × 2 inch sponges. Once cleaned, files should be returned to metal box for sterilization.

b. Generally the standard prohibits bending or recapping of anesthesia needles. However, during endodontic treatment, reinjection of the same patient is often necessary, so recapping is essential. Recapping with a one-handed scoop method and using a mechanical device are the only permissible techniques; needles must not be recapped by using both hands or directing the needle point toward any part of the body. Shearing or breaking of contaminated needles should never be permitted.
5. Countertops and operatory surfaces, such as light handles, radiograph unit heads, chair switches, and any other surface likely to become contaminated with potentially infectious materials, can be either covered or disinfected. Protective coverings (e.g., clear plastic wrap, special plastic sleeves, aluminum oil) can be used. These coverings should be changed between patients and when they become contaminated.

6 Contaminated radiographic film packets must be handled in a way that prevents cross contamination. Contamination of the film (when it is removed from the packet) and subsequent contamination of the processing equipment can be prevented either by properly handling the film as it is removed from the contaminated packet or by preventing the contamination of the packet during use. After exposure, “overgloves” should be placed over contaminated gloves to prevent cross contamination of processing equipment or darkroom surfaces.
7 In conjunction with the previously mentioned guidelines for infection control, a mouth rinse of 0.12% chlorhexidine gluconate, such as Peridex (Procter & Gamble, Cincinnati), is suggested before treatment. This rinse will minimize the number of microbes in the mouth and, consequently, in any splatter or aerosols generated during treatment. It should be noted, however, that such mouth rinses have not proved to reduce the incidence of clinical infections.

8. After treatment, all instruments and burs must be cleaned and sterilized by sterilizers monitored with biologic indicators. Cassettes, packs, or trays should be rewrapped in original wrap, and individually packaged instruments should be placed in a covered container. Air and water syringes must be flushed, cleaned, and sterilized. handpieces and “prophy” angles be heat sterilized between patients. Before sterilization, all handpieces should be wiped with an EPA-registered disinfectant. In addition, highspeed handpieces should be run for a minimum of 30 seconds to discharge water and air, with spray directed into a high-volume evacuation system. Dental unit water lines should be periodically flushed with water or a 1:10 dilution of 5.25% sodium hypochlorite (NaOCl) to reduce biofilm formation.

The categorization of instruments depends on the contact with different tissue types to determine whether sterilization or disinfection is required.
1. Critical items- instruments that touch sterile areas of the body or enter the vascular system and those that penetrate the oral mucosa. eg scalpels, curettes, burs, and files. Must be sterilized and store in appropriate package, single use items must be properly discarded.
2. Semi critical items- instruments that touch membrane but do not penetrate tissues. eg. Amalgam condenser and saliva ejector. This items should be sterilized; however, if it is not feasible, high level disinfection is required.

3. Non critical items- those items that do not come in contact with oral mucosa but are touched by saliva or blood-contaminated hands while treating patients. eg. Light switches, counter tops,and drawer pulls on cabinets. These areas should be properly disinfected.

Sterilization methods that are generally accepted in dentistry:1. Steam under pressure - Autoclaving the typical method of sterilization for most health care facilities.
The usual cycle is 30 minutes at 250° F (121° C) at 15 psi. Flash sterilization at high temperatures of 273° F (134° C) for 10 minutes and 30 psi is also approved. The Statim brand autoclave uses the higher temperatures to reduce cycle time.
Advantages: - better penetration of moist heat - instruments can be wrapped prior to sterilization, increases
shelf life of instruments. - does not destroy cotton or cloth produts - most dental instruments can be autoclaved

Disadvantages:
- dulling and corrosion of sharp instruments - item sensitive to elevated temperature and
moisture cannot be effectively autoclaved. - damage to plastic and rubber products. - instruments need to be air dried at the end of cycle.


2. Chemical vapor sterilization – Chemclave Chemiclave uses a solution of 72% ethanol and 0.23%
formaldehyde in place of water in its “autoclave.” This avoids the instrument corrosion typical of steam autoclaves. They use 270° F (132° C) at 20 psi for 20 minutes, including drying time. Arguably a longer cycle time may be needed to meet guidelines for safety margins. Ventilation or filtration is required to handle formaldehyde fumes. Chemiclave chemicals can dissolve into liquids, so liquids should be steam autoclaved.

Advantage: - fast turn around time and better protection of
carbon steel bur.Disadvantage: - odor that is release when chemicals are heated.


3. Dry heat sterilization Dry heat sterilizers, either still air in an oven or forced air,
also avoid corrosion of instruments. After preheating the instruments to sterilizing temperature, still air models provide sterility in 1 hour at 375° F (191° C). The Cox sterilizer uses forced hot air of the same temperature and sterilizes in 6 minutes. Wrapped pack increase the time needed for processing. Hot air sterilizers may require special wraps
Disadvantage: - long sterilization time


In-operatory sterilizers were once popular among clinicians for decontaminating instruments during treatment. Such sterilizers achieved 450° F (218° C), and typical cycles were a few seconds for metal instruments. Glass beads or salt were used to transfer dry heat to endodontic canal instruments. These sterilizers are no longer approved for use because of the possibility that practitioners relied on them for sterilization between patients. One study found that they were ineffective at killing spores on cotton and paper products. Endodontic instruments used for recapitulation in a canal as it is progressively decontaminated may be disinfected chemically.


Following patient treatment, barriers should be removed and surfaces disinfected. Aerosols generated by dental care can land anywhere, so all surfaces that may be touched during treatment of the next patient should be disinfected. Special attention should be given to instrument holders and hoses. Door and drawer pulls should be included in the disinfection routine or covered with barriers. Pens, pencils, and even patient charts should be considered contaminated. Disinfection of the treatment room includes wiping all surfaces to be used with an appropriate disinfectant.


Disinfection- is added to the method for preventing cross contamination in which sterilization is not possible
Chlorine Dioxide disinfects instruments and operatory surface in 1 to 3 mins. when
used correctly. Requires no rinsing and leaves no residue after use. Disadvantages are corrosion of easily oxidized metals and the need for fresh solutions for each disinfection process.
Sodium Hypochlorite suitable for surface disinfection than for instruments sterilization
because of its high corrosive action on metals. Disinfection can occur in 3 to 30 mins.depending on the amount of debris present. Dilusion 1:1to 1:5

Iodophors Iodophors are broad spectrum disinfectant that is effective againts a host
of pathogens, including HBV, M. tuberculosis, poliovirus, and helpers simple virus. One of the inherent advantages of the compound is the slow release of elemental iodine to enhance the bactericidal activity. Dilution 1:213 of soft or distilled water hard water inactivates the iodophor. Biocidal activity occurs within 30 mins.
Alcohols Not accepted by ADA for disinfection of surface or instruments.
Quarternary Ammonium Compounds This group of compounds including benzalkonium chloride, is no longer
recommended for instrument or surface disinfection. All quarternary ammonium compounds have been disapproved by the ADA for use in dentistry.

Barrier techniques in infection control address the quantity factor in disease prevention. This may encompass protection of the body surfaces, protection of the environmental surfaces, or blockage of bacteria from the source.
Gloves provide the patient with protection from contamination of
microorganisms on the practitioners hands and protect dental health care workers from contaminations by the patients blood and saliva.
Handwashing hands should be washed before gloves are placed and after
gloves are removed bec. the integrity of the glove is not dependable.

Face masks The face masks is an important barrier providing protection from
inhalation of aerosols generated by high speed handpiece and air water syringes. Should remain dry to prevent transmission of organisms through moisture penetration.
Eyeglasses Protective eye ware is highly beneficial for dental care providers and
for the patient. Helpers virus infection of the eye and infection from hepatitis B are possible consequences of viral contact with the eye.
Clothing The general recommendations for clinic wear include reusable or
disposable gowns and laboratory coats or uniforms with long sleeves. Head covers are also recommended during procedures that result in splashing blood or other body fluids.

The use of the rubber dam is mandatory in root canal treatment. Developed in the nineteenth century by S.C. Barnum, the rubber dam has evolved from a system that was designed to isolate teeth for placement of gold foil to one of sophistication for the ultimate protection of both patient and clinician. The advantages and absolute necessity of the rubber dam must always take precedence over convenience and expediency. When properly placed, the rubber dam facilitates treatment by isolating the tooth from obstacles (e.g., saliva, tongue) that can disrupt any procedure. Proper rubber dam placement can be done quickly and will enhance the entire procedure.

The rubber dam is used in endodontics because it ensures the following
1. Patient is protected from aspiration or from the swallowing of instruments, tooth debris, medicaments, and irrigating solutions.
2. Clinician is protected from litigation because of patient aspiration or swallowing of an endodontic file. Routine placement of the rubber dam is considered the standard of care.
3. A surgically clean operating field is isolated from saliva, hemorrhage, and other tissue fluids. The dam reduces the risk of cross contamination of the root canal system, and it provides an excellent barrier to the potential spread of infectious agents. It is a required component of any infection control program.
4. Soft tissues are retracted and protected.
5. Visibility is improved. The rubber dam provides a dry field and reduces mirror fogging.
6. Efficiency is increased. The rubber dam minimizes patient conversation during treatment and the need for frequent rinsing.

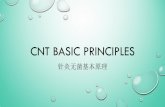
Components of rubber dam: The mainstay of the rubber dam system is the dam
itself. These autoclavable sheets of thin, flat latex come in various thicknesses (e.g., thin, medium, heavy, extraheavy, special heavy) and in two different sizes (5 × 5 inches and 6 × 6 inches).
Another component of the rubber dam system is the rubber dam frame, which is designed to retract and stabilize the dam. Both metal and plastic frames are available, but plastic frames are recommended for endodontic procedures. They appear radiolucent, do not mask key areas on working films, and do not have to be removed before film placement.

Rubber Dam Rubber Dam Frame

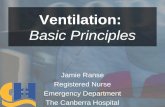
Methods of Rubber Dam PlacementThe method of dam placement is to position the bow of
the clamp through the hole in the dam and place the rubber over the wings of the clamp (a winged clamp is required).The forceps stretch the clamp to maintain the position of the clamp in the dam, and the dam is attached to the plastic frame, allowing for the placement of the dam, clamp, and frame in one motion. Once the clamp is secured on the tooth, the dam is teased under the wings of the clamp with a plastic instrument.

A, Rubber dam, clamp, and frame. B, Dam, clamp, and frame carried to mouth as one unit and placed over the tooth. C,
Clamp in place with four-point contact and rubber tucked under the wings.

Another method is to place the clamp, usually wingless, on the tooth and then stretch the dam over the clamped tooth .This method offers the advantage of enabling the clinician to see exactly where the jaws of the clamp engage the tooth, thus avoiding possible impingement on the gingival tissues. Gentle finger pressure on the buccal and lingual apron of the clamp before the dam is placed can be used to test how securely the clamp fits. Variations of this method include placing the clamp and dam first, followed by the frame, or placing the rubber dam first, followed by the clamp and then the frame.

A, After the clamp is placed, the dam is attached to the frame and gently stretched over the clamped tooth with the index
finger of each hand. B, Clamp is tested for a secure fit with gentle finger pressure (alternately) on the buccal and lingual aspects of the
clamp apron.

Insti-Dam is a disposable dam system available in both latex and nonlatex. A, Bendable flexible frame allows for easy
placement. B, Use of Insti-Dam during endodontic treatment. (Courtesy Zirc Company, Buffalo, MN.)

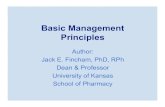
A third method, the split-dam technique, may be used to isolate anterior teeth without using a rubber dam clamp. Not only is this technique useful when there is insufficient crown structure, as in the case of horizontal fractures, but also it prevents the possibility of the jaws of the clamp chipping the margins of teeth restored with porcelain crowns or laminates. Studies on the effects of retainers on porcelain-fused-to-metal restorations and tooth structure itself have demonstrated that there can be significant damage to cervical porcelain, as well as to dentin and cementum, even when the clamp is properly stabilized. Thus for teeth with porcelain restorations, ligation with dental floss is recommended as an alternate method to retract the dam and tissues, or the adjacent tooth can be clamped.

Split-dam technique. A, Premolar clamp on maxillary central incisor along with ligation on the maxillary canine prevents
dam slippage and aids in dam retraction during endodontic treatment on broken-down maxillary lateral incisor. B, Split dam used during
post removal and retreatment of a maxillary central incisor. (A Courtesy Dr. James L. Gutmann. B Courtesy Dr. Francisco A. Banchs.)

Rubber dam clamps are color coded for ease in identification. (Courtesy Coltene/Whaledent, Inc., Cuyahoga Falls,
OH.)

Hepatitis B is a major health hazard for dental health personnel. Because of this risk, the ADA Council on Therapeutics and the CDC have recommended that all dental personnel involved in patient care can receive the hepatitis B vaccine if they do not already immunity as a result of previous exposure to virus.
Two types:1. plasma-derived HB vaccine2. recombinant DNA HB vaccine
Vaccine plays an important role in infection control process but many blood borne pathogens exist for which there is presently no vaccine including HIV. Proper infection control procedure are therefore important to prevent transmission of any pathogens.

PATHWAYS OF THE PULP 9th EDITION INTERNET
Text book of endodontics by: Nisha Garg and Amit Garg Endodontics 5th edition by: Ingle and Bacland


THANK YOU AND GOOD DAY