Basic Insulin Pumping
71
Basic Insulin Pumping Stephen W. Ponder MD, FAAP, CDE Endocrinologist Baylor Scott and White Healthcare
-
Upload
stephen-mabry -
Category
Health & Medicine
-
view
249 -
download
0
Transcript of Basic Insulin Pumping
Basic Insulin PumpingStephen W. Ponder MD, FAAP, CDE
Endocrinologist
Baylor Scott and White Healthcare

What is an insulin pump?
A programmable electromechanical device capable of delivering variable doses of rapid-acting insulin through a temporarily implanted catheter.

Display Screen
Pump Case (removed)
Cartridge(insulin reservoir)
Lithium
AA Battery
Electronics(behind screen)
Control buttons
Anatomy of an Insulin Pump
Display Screen
Pump Case (removed)
Cartridge(insulin reservoir)
Lithium
AA Battery
Electronics(behind screen)
Control buttons
Anatomy of an Insulin PumpAnatomy of an Insulin Pump

What are potential benefits of a pump?
• Flexibility in scheduling meals and activities
• Better manage unexpected changes in routine
• Eliminate need for frequent insulin shots
• Improved blood sugar control

Why we strive for better control
Keeping a lower A1C
over time lowers the
chance of diabetes
complications
There is NO magic
A1C that helps. Any
improvement counts!

What Lowers The A1c
Frequent BG checks *
Frequent boluses *
Rapid insulin *
Accurate carb counting *
Easier bolus calculations *
Easy history *
Basal can be adjusted to match need *
Bolus based on carbs and BG *
Properly set doses --> Pump Formulas
* Where a pump helps

What are the challenges of an insulin pump?
• Being attached to a device 24/7
• Everyday activities • Bathing/showering• Clothing• Sleeping• Pets?
• Remembering to use it properly
• Not thinking enough before using it

Is the insulin pump better than shots?
• Depends on how they are used
• A pump is a choice
• If age is a consideration, it can be better than shots (small kids)

Pump Myths
• My child or teen will have perfect blood sugar control once on the pump.
• The pump will prevent all complications
• Pump therapy will be easier and will take less time.
• My child or teen won’t have to monitor as much
Infusium, the Greek god of Pumps

GIGO Garbage in…Garbage out…
Most pump wearers have non-physiologic settings in their pumps.
This creates significant errors in dosing.
All pump settings should be selected from standard formulas and readjusted through BG testing

Does insurance cover a pump?
• Yes, in Texas. Including Medicaid
• No for Omnipod and Snap Pump (Medicare only)

What should I know to use an insulin pump?
• Basic diabetes survival skills
• Check BG levels frequently each day/use a CGM
• Mastery of hyperglycemia/sick day/ketone self care
• Appreciate how carbs, exercise, stress, and insulin affect each other
• Be able to stay focused and follow through well
• Have the ability to troubleshoot and problem-solve situations
• Remember what works, learn from what fails

Which insulins work with a pump?
• Rapid acting insulin (Novolog, Humalog, Apidra)
• Fast-acting insulin (Regular Human insulin) • Slower insulin, requires adjustments
• Talk with doc before switching
• Never use cloudy insulin (N, 70/30, or 75/25)
• Never use Lantus or Levemir

How soon can I start using an insulin pump?
• Right after diagnosis, but usually after basic diabetes training is complete
• Quality pre-pump education is needed before “button-pushing” training
• Ongoing training and updates are essential to the best outcomes

Can the pump measure my sugar level?
• Not the pump per se, but we now have CGM-enabled insulin pumps
• Still require BG checks to verify reading on the pump screen
• The pump cannot dose insulin based on the sensor reading

How long can I disconnect from the pump?
• Usually no longer than 2 hours, sometimes less
• Check BG before and after disconnecting
• Depending on circumstances, could take an insulin dose before disconnecting and wait longer before reattaching

Can I get off the pump and back on later?
• Yes, absolutely
• Learn how to properly start switch over from a pump to shots based on how long it takes for the insulin pump’s insulin to wear off and the injected insulin starts to work.
• It takes about 2 hours for a basal rate insulin dose to stop working
• It takes 2-4 hours for a Lantus or Levemir dose to start working

Does the pump automatically give me more insulin for a high BG?• No, not yet
• CGM-enabled pumps may suspend basal delivery for low BG

What is the “untethered” regimen?
• Taking Lantus or Levemir BY INJECTION each day and using the pump just to take insulin for meals or correction.
• Requires still wearing and changing an infusion site every 3 days.
• Still must keep up with the pump.

Can I fly with a pump?
• Yes
• Domestically, no problems
• Internationally, might need doc letter

What if my child doesn’t want a pump?
• Depends on age. Toddlers say no to everything, but adapt
• Older children (school age) should agree to use them
• But never force or cajole someone to use an insulin pump
What are ways to get started on a pump?
• After proper reflection and preparation
• Take preparatory classes on pump theory, carb counting
• Saline start optional, but can make transition in kids easier
• Set aside time for “button pushing” training when possible
• Unfortunately the only training might be at start up
• Expect close follow up by training staff after start up
• Remember what Homer Simpson said…

What is the infusion site like? Does it hurt?
• Small plastic catheter that inserts under the skin (not into a vein)
• Is placed by the user or parent
• Can be placed just about anywhere except over a bone or joint
• Ice packs or topical numbing agents can be used to manage insertion discomfort
• Different catheters insert at either a 90 or 30 degree angle

How often should I change my site?
• At least every 3 days
• Change the reservoir too
• Rotate infusion sites to minimize scarring or fatty buildup

When should I worry about an infusion site?
• If it’s tender, looks red or irritated or oozing anything
• If the BG level two hours after insertion continues to rise (check)
• If pump occlusion alarms occur
• If you see any blood or pink material in the catheter or tubing
• If you can smell insulin around the site
• If BG levels don’t respond to insulin doses like they usually do
• Anytime high BG is present and ketones (correct with injection)
• Whenever nausea or vomiting occurs (check BG and ketones ASAP)
• When in doubt, change it out!

Unexplained high…explained
Culprit: bad pump site
First discovered…
Corrected all by injection

What is a basal rate?
• The rate of delivery of insulin through a pump that is intended to match or mimic the natural production of insulin throughout the day by a working pancreas.
• The pump may be programmed to change basal rate delivery based on time of day
• Multiple basal rates are possible.
• The purpose of a basal rate is to• Keep high sugars and high ketones from forming when not eating
carbs• Maintain BG levels on a steady trend, not necessarily drop or raise BG
levels

0.75 U/hr
Starting a basal rate
B A S A L
Example:
Pre-pump TDD = 48 units
75% of 48 units = 36 units (some reduce TDD)
50% of 36 units = 18 units
18 divided into 24 hours = 0.75 U/hr
timetime

. . ..
..
..
..
2 hours150 mg/dl
80 mg/dl
135 mg/dl
glu
cose
0.75 U/hr B A S A L
timetime
94 mg/dl
Testing a basal segment
145 mg/dl
2 hours 2 hours
105 mg/dl
fasting

What is a bolus?
• A bolus is a dose of insulin given by shot or a pump. If given by pump it can be delivered all at once, or over a defined period of time (extended bolus or square wave bolus). It can also be divided into a portion given at once and the rest given over a defined period of time (combination bolus or dual wave bolus).
• A bolus is programmed by the pump user or parent.
• The purpose of an insulin bolus is to provide insulin for metabolizing carbohydrate containing foods or drinks, and/or to lower a blood sugar level that is out of a desired target range.

Timing of Bolus Insulin vs. food GI level or BG
-30 -15 0 15 30
Minutes from meal
OK
Low G.I.
Mod
High G.I.
High BG
Low BG

How are basal rate/carb factor/correction ratios calculated?
• Several formulas/charts have been created to help estimate a starting dose of rapid-acting insulin for:• Basal rate
• Carbohydrate coverage
• Correction insulin dosing
• Insulin on Board
• It’s important to know that these are ONLY ESTIMATES and their action may and will vary from day to day and sometimes within the same day. They are IMPRECISE but still helpful

6
time
0.75 U/hr
Insulin to Carb [I : CHO] ratio
B A S A L I N S U L I N
. . ..
..
.
.
..
..
2 hours
time
180 mg/dl
80 mg/dl
125 mg/dl 150mg/dl
Example: 1 to 10
60 grams CHO / 10
60 / 10 = 6
6
“Acceptable” = “target” +/- 30 mg/dl
glu
cose
bo
lus
CH
O

. . ..
..
.
.
..
..
2 hours155 mg/dl
95 mg/dl
125 mg/dl
glu
cose
0.75 U/hr
timetime
60 mg/dl
Bolus for a measured amount of carbs
Testing a bolus
145 mg/dl
215 mg/dl
B A S A L

How is an insulin correction factor calculated?
• This is from an empirical formula originally created by Dr. Paul Davidson in Atlanta Georgia in the 1980’s
• It’s based on dividing the average total daily insulin needs (in units) into the number 1800, 1900 or 2000 (pick one).
• For example. 30 units total daily insulin dose. 1800/30 = 60
• 60 suggests that 1 unit of rapid acting insulin will lower BG by 60 mg/dl in 2-3 hours. The +/- is 30 mg/dl
• This is just a starting point and MUST be proven with BG checks done often enough to verify it’s close enough
• This is always changing with age, size, gender and diabetes duration

5
time
0.75 U/hr
“Correction” dose
B A S A L I N S U L I N
. . ..
..
.
.
..
..
2 hours
time
180 mg/dl
80 mg/dl
250 mg/dl
110 mg/dl
Example: 1 to 25
Actual – target / 25
250 – 125 / 25 = 5
5
“Acceptable” = “target” +/- 30 mg/dl
glu
cose
bo
lus

What does the insulin on board mean?
• A way to estimate the time (in hours), that a bolus dose of rapid acting insulin works before the sugar lowering effect is all gone.
• Example: IOB of 4 hours, IOB of 3.5 hours
• Range is 2-8 hours, usually 3-5 hours
• It’s an estimate only, larger doses last longer than smaller ones.

0.75 U/hr
Unused insulin (Duration of insulin)
7 Units6 Units
B A S A L
timetime
6 Units
4-6 hours
“Stacking effect”

1 hr 2 hr 3 hr 4 hr
1 units 0.7 0.4 0.1 0
2 units 1.4 0.8 0.2 0
3 units 2.1 1.2 0.3 0
4 units 2.8 1.6 0.4 0
5 units 3.5 2.0 0.5 0
6 units 4.2 2.4 0.6 0
7 units 4.9 2.8 0.7 0
8 units 5.6 3.2 0.8 0
9 units 6.3 3.6 0.9 0
10 units
7.0 4.0 1.0 0
Insulin left at 1,2,3 and 4 hours after a dose of Humalog or Novolog
Units left to work after:Dose given
Th
e u
nu
sed
in
suli
n r
ule

DIAs on current pumps can be set from 2 to 8 hours.
An inaccurate DIA can significantly affect control.
Mudaliar et al: Diabetes Care, 22: 1501, 1999
Recommendations for DIA times

. . ..
..
.
.
..
..
2 hours
180 mg/dl
80 mg/dl
125 mg/dl
glu
cose
0.75 U/hr
timetime
60 mg/dl
Exercise or other strenuous activity
Temp basal rates
B A S A L

. . ..
..
.
.
..
..
2 hours
180 mg/dl
80 mg/dl
125 mg/dl
glu
cose
0.75 U/hr B A S A L
timetime
90 mg/dl
Exercise or other strenuous activity
40% reduction
Temp basal rates

Basal-Bolus insulin regimens require…
attention to detail
frequent glucose monitoring
lots of decision making
teamwork to succeed!
thinking like a pancreas

How do I know my pump settings are right?
• Assuming carbs are counted properly and insulin dosed on time and basal rate(s) is/are correct: • Before breakfast blood sugars will average in a proper target range (80-120
mg/dl)
• After meal (2-3 hours) blood sugar levels will be 140-180 mg/dl
• Blood sugars in the absence of food or snack will track steady and not drift
• 2-3 hours after a correction insulin dose the values will be near target
• The A1C results will be in your desired target range (7% or lower)
• If the above is not happening don’t assume first that the pump is the problem. Look at your method and self care practices first.

When should I change my pump settings?
• When you have ruled out OTHER reasons for poor control FIRST• Missed boluses• Delayed boluses• Eating carbs but not covering• Poor counting of carbs• Not checking BG often enough to make a proper analysis
• When A1C is increasing over 7% (maybe 8% depending on age)
• When careful review of properly collected BG data suggests the need at any time, and other reasons (above) have been eliminated

How can a “pump system” malfunction?
• Software
• Hardware• Reservoir leak• Tubing leak• Air bubbles• Dislodged site• Poorly inserted site• Tunneling
• User• Failure to bolus• Late to bolus• Not blousing at all

What if my skin reacts to the adhesive?
• Try different adhesives as barriers
• Flonase?

How do I know what I should change?
• At first you will need help
• Resist making changes to the pump settings. Look at your self care practices first (insulin timing, carb counts, do you always correct?)
• Discuss with your pump trainer/CDE/NP/PA/endo
• In general, look at how often corrections are being used. If a lot, then a dose change might be needed (assuming proper carb counts)
• Insulin dose ranges are wide in kids and adults. In general most people need 30-40% of their total daily insulin needs as basal, with the rest given as boluses. A high basal percentage could indicate missed insulin boluses in teens.

Should only my doc make pump changes?
• In most cases yes, at least at first
• You can be trained to make independent changes to pump settings
• When making changes, be conservative at first (10% changes)
• Wait long enough to see a distinct improvement based on BG data
• Remember, pump settings are estimates at best

What if my teen is misusing the pump?
• Ask if they would like to take a break from the pump
• Try to share more self care duties with them
• Decide if the pump really is helping or enabling bad behaviors
• Discuss other options with your endo (untethered?

What are underused features of a pump?
• Bolus history – check when boluses were done
• Bolus reminder alarms – to remind user to dose
• BG check alarms – to remind user to check BG after site change
• Dose calculators – estimate insulin dose based on BG and carb
• Auto-off features – shuts off pump if no buttons pushed in x hrs

Ponder’s Pumping Principles1. An insulin pump is no better or worse than
the human being attached to it
2. Master carb counting first BEFORE pumping
3. Age does not limit who can pump insulin
4. Garbage in, garbage out: beware of the “pump and dump” phenomenon
5. A good pump doctor behaves like a coach
6. Simple is a good place to start, but pumping skills MUST advance over time
7. A good insulin pumper troubleshoots and problem solves daily. It’s all about mastering the PROCESS of pumping
8. Technology changes; people don’t
9. Self-consistency is a virtue
10. Everyone’s blood sugar fluxes; seek out your own sugar patterns in the “chaos”
11. Success is always a relative thing
12. Don’t ever be afraid to start over

Pump problems, etc…

Oh no. Not Mystery Boluses!

Straight versus angled infusion sets








Air in infusion tubing

Air in luer lock hub

120 U of air

Defective tubing connections

Subcutaneous layer
Muscle tissue
Dermal layer
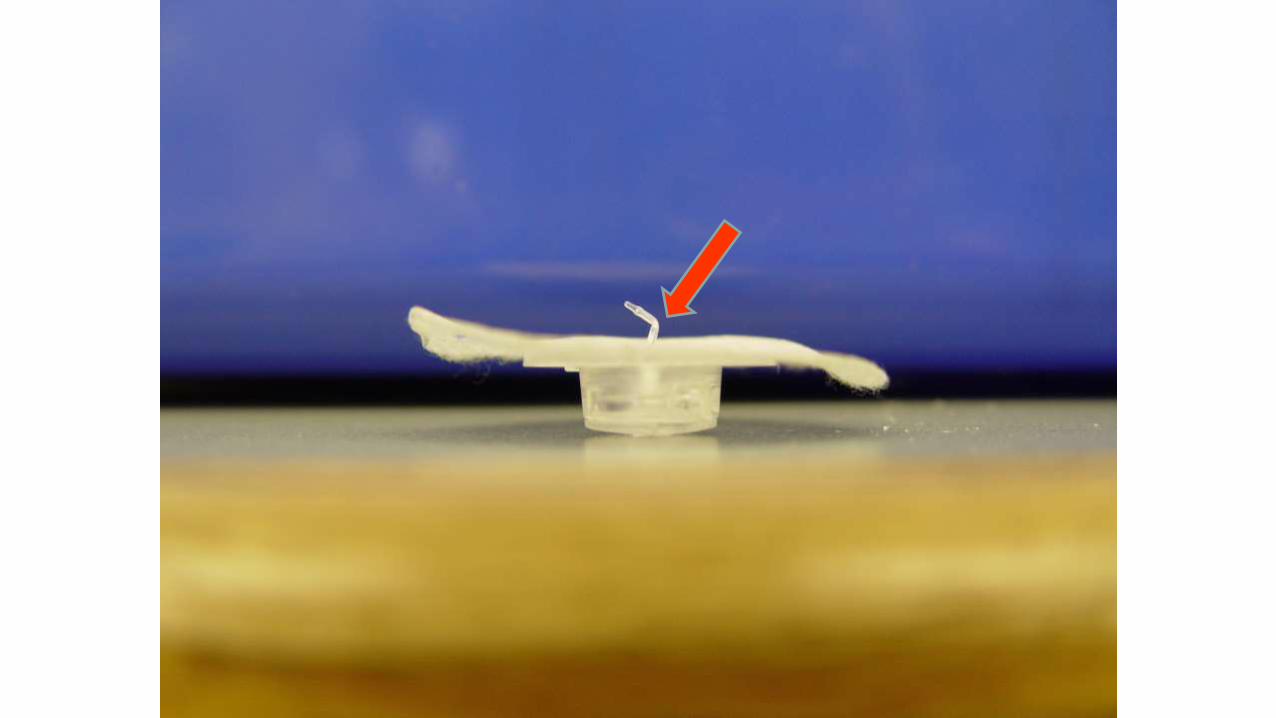
“Tunneling” A problem with Teflon infusion sets
Back-leakage occurs due to a slightly dislodged catheter
High BG is the only sign
Tennis players, golfers and other vigorous activities
Solution: Make a tape “sandwich”, use metal sets

Tunneling

Tunneling and CGM “pickup”
154 mg/dl 5 units Novolog
“tunneling”
30 degree angled site is 2 days old

Thank you.I hope you learned
something!