Radiographic Evaluation of a Pulmonary Embolism Dr Mohamed El Safwany, MD.
Upload
nigel-peregrine-allenCategory
view
218download
1
BASIC CONCEPTS IN DIAGNOSTIC IMAGING
Dr Mohamed El Safwany, MD.

Intended learning outcome
• The student should learn at the end of this lecture Basic concepts in radiological Imaging.

Outline
• Introduction• X-Rays• Fluoroscopy• CT• MR• Innovative Modalities

Modalities Available in Radiology
• Plain Film / X-Ray/Mammography
• Fluoroscopy
• Ultrasound
• CT
• MRI
• Nuclear Medicine/Molecular Imaging
• Angiography/Interventional

X-Rays
• Discovered in 1895 and still used today
• Most widely performed imaging exam
• X Rays are emitted and detected in cassette
• Cassette can generate either a film or a digital image
• Films are kept ‘on file’ or in a digital archive

Most Useful Applications for Plain X-Rays
• Chest
• Musculoskeletal
• Abdomen: limited usefulness

Fluoroscopy
• Utilizes X-Rays
• Real-time imaging
• Utilizes image intensifier
• Involves use of contrast agents

Main Uses of Fluoroscopy
• Gastrointestinal Imaging
• Genitourinary Imaging
• Angiography
• Other– Intraoperative– Foreign body removal– Musculoskeletal
Gastrointestional Fluoroscopy
• Esophogram/Barium Swallow
• Modified Barium Swallow/Dysphgiagram
• Upper GI
• Small Bowel Series
• Enteroclysis
• Contrast Enema
• Defecography

Single Contrast vs Double Contrast
• Single Contrast– Generally uses just thin Barium– Distends lumen with high density material– Easier for patient/less mucosal detail
• Double Contrast/Air Contrast– Thick barium coats lumen– Effervescent tablets ingested to distend lumen with air– Produces ‘see-through’ images with greater mucosal
detail – Greater sensitivity for small lesions, polyps, ulcers

Single ContrastBarium Enema
Double ContrastBarium Enema
Single Contrast vs Double Contrast

Contrast Materials for GI Exams
• Barium Sulfate– Thick: used in double contrast studies– Thin: used in single and double contrast exams– Paste: mod Ba swallow and defogography
• Gastrograffin– Full stregnth: rarely used– Dilute

Gastrograffin Swallow StudyBarrium Swallow Study
Barium vs Gastrograffin

Barium Sulfate
• Most widely used
• Better images than gastrograffin
• ‘Chalky taste’
• Peritonitis may develop if perforation
• If delayed transit, may form concretions in colon

Gastrograffin
• Water soluble• Foul Taste• Poor mucosal coating
– Basically used for R/O obstruction
• Won’t cause peritonitis if perforation• May cause severe chemical pneumonitis if aspirated• Osmotic pressure draws fluid into bowel lumen
– Progressive distention in small bowel obstruction– ‘Therapeutic’ enema in constipation

Patient Factors in GI Fluoroscopy
• Ability to ingest contrast– In order to get high quality images, a relatively large
volume of contrast needs to be ingested fairly quickly
• Mobility– Multiple positions required for GI exams, particularly
double contrast exams.– Limited mobility = less diagnostic images
• Weight– Tables have weight limits– Requires maximal radiographic technique and exposure is
often suboptimal

Esophogram or Barium Swallow
• Evaluates pharynx and esophagus
• Limited evaluation of stomach
• Double or Single Contrast
• Mucosal contour and Motility

Modified Barium Swallow
• AKA Dysphagiagram and at Carle “cookie swallow”
• Performed with Speech Pathologist• Barium administered in various bolus
consistencies ranging from liquid to solid• Evaluates swallowing mechanism• Evaluates for aspiration• Performed on videotape

Modified Barium Swallow

Upper GI Exam
• Evaluates esophagus, stomach and duodenum
• Double or Single Contrast
• Can be combined with small bowel series
• Largely replaced by endoscopy and cross-sectional imaging
• Fairly insensitive

Small Bowel Series
• Patient drinks 2 cups of thin Ba
• Overhead films obtained at routine intervals
• The Ba column is followed through until it reaches the colon
• Transit time, mucosal contour, bowel loop distribution are evaluated.
• Insensitive for small masses

Small Bowel Series
Small Bowel Enteroclysis
• “Double Contrast Small Bowel Series• NGT placed at duodenal-jejunal junction• Ba injected followed by methylcellulose• See-through appearance to small bowel• Greater sensitivity for small masses and
mucosal lesions• Patient discomfort related to NGT and
diarrhea

Contrast Enemas
• Barium or Gastrograffin
• Double contrast or single contrast
• Generally less sensitive than endoscopy
• Requires bowel prep to assess for mucosal lesions
• Requires some element of patient cooperation

Single ContrastBarium Enema
Double ContrastBarium Enema
Contrast Enemas

Defecogram
• Barium paste is inserted into rectum
• Patient is asked to defecate under fluoroscopy
• Ano-rectal and pelvic floor dynamics can be assessed
• Rectocele, intussusception, pelvic floor relaxation, stress incontinence

Genitourinary Fluoroscopy
• Cystogram
• Voiding cystourethrogram
• Retrograde urethrogram
• Hysterosalpingogram

Cystogram
• Usually in adult patients
• Looking for tear or intraluminal mass
• Catheter placed and bladder filled with contrast to capacity: usually 300-500 ml.
• Spot films obtained when full
• Post void film: usually overhead
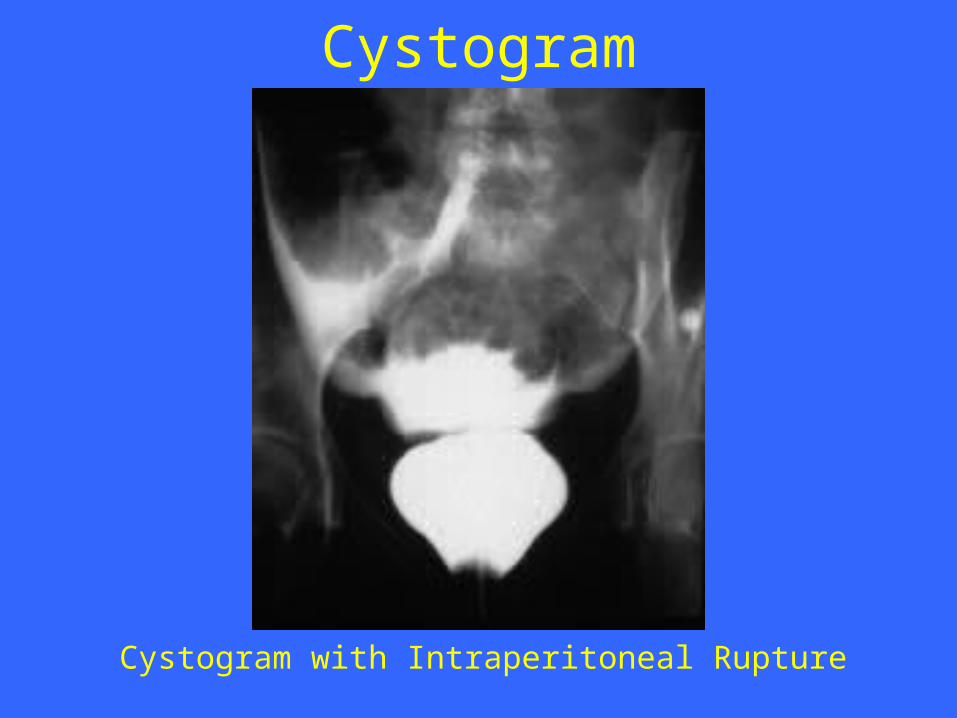
Cystogram with Intraperitoneal Rupture
Cystogram

Voiding CystourethrogramVCUG
• Usually in children with history of UTI
• Searching for vesicoureteral reflux
• In males, evaluate for urethral abnormalities: posterior urethral valves
• Same as cystogram except when full patient voids under fluoro with spot films

Retrograde UrethrogramRUG
• Male patients
• Pelvic Trauma
• Post-infectious: STD- looking for stricture
• Different techniques
• Meatus occluded and contrast injected into urethra under fluoro

Retrograde UrethrogramRUG

Hysterosalpingogram
• Used to evaluate endometrial canal and fallopian tubes
• Infertility and uterine anomalies
• Dye injected into cervical os under fluoro
• Injection continued with goal to opacify the fallopian tubes and spill contrast into peritoneum

Musculoskeletal Fluoroscopy
• Fracture/Dislocation reduction
• Hardware placement in the OR
• Flexion/Extension views of c-spine
• Arthrography– May be performed in conjunction with MRI or
CT

Techniques Relevant to MSK Radiology
• Radiography (routine and specialized views)
• CT
• MRI
• US
• Densitometry
• Interventional procedures (arthrography, percutaneous biopsy/vertebroplasty)
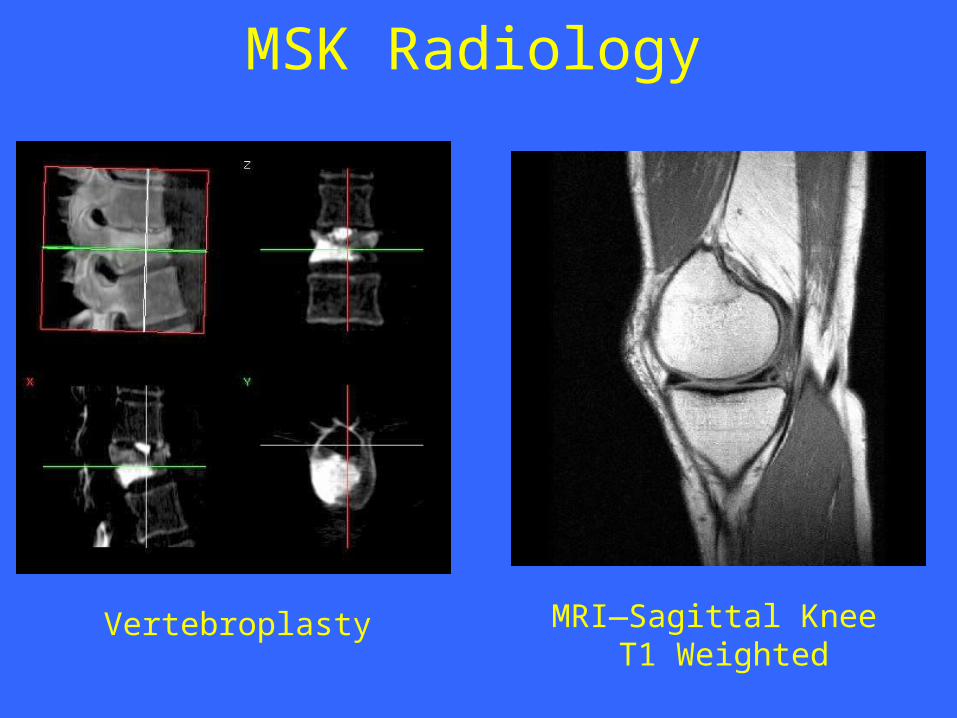
MRI—Sagittal Knee T1 Weighted
MSK Radiology
Vertebroplasty

Computed Tomography (CT)• Cross Sectional imaging modality
• Mobile X-ray tube that rotates around a pt
• Slices of X-ray transmission data reconstructed to generate image
• Data displayed in multiple window settings (lungs parenchyma, bone, etc.)
• Density measurements/Hounsfield Units analyze chemical component of tissue
• HU: -150-0 = fat, 0 = water, 0-20 = serous fluid, 45-75 = blood,
100-1000 = bone/calcium

CT Contrast Agents• Intravenous contrast---iodinated
Differentiate blood vessels vs. vascular internal organs
• Enteric contrast---barium
Differentiate bowel vs. intra-abdominal fluid/masses
• Rectal contrast
• Retrograde urinary bladder contrast

CT Applications• Neuro-imaging
-Acute head trauma, acute intracranial hemorrhage
-Low sensitivity for early ischemic stroke, intracranial metastatic disease, white matter degenerative disease
• Head and Neck imaging-Soft tissue of neck, paranasal sinuses, temporal
bone imaging, orbital wall imaging

CT Applications• Body Imaging
-Chest, Abdomen, Pelvis (with enteric and IV contrast)
• Pulmonary nodules, Renal Calculi (without contrast)
• Acute appendicitis (with enteric and IV contrast)
• Specialized protocols:
-Liver masses, pancreatic tissue, renal masses, adrenal masses

CT Applications• Acute Abdomen
-decrease rate of false laparotomy procedures
• Trauma Spine Imaging (cervical, thoracic, lumbar)
• Other osseous structures (pelvis, extremities)
• Vascular Imaging
-CT angiography--- i.e. coronary arteries

CTAxial, with oral contrast in stomach

CT PET PET/CT

CTA(CT Angiography)
CT Cardiac Imaging
The Power of CT

Magnetic Resonance Imaging (MRI)
• Multi-planar scanning
• Without ionizing radiation
• Images generated using powerful magnets and pulsed radio waves passing through the body
• Data from Pt’s body used to generate image
• Field strength of magnets 0.3-3.0 Tesla

MR Contrast Agents• Intravenous contrast---Gadolinium chelate-
based contrast agents
• Gadolinium is a paramagnetic lanthanide that is toxic as a free metal
• Contrast to evaluate BBB, intracranial edema and hemorrhage
• Novel agents being developed as tagged Monoclonal antibodies for Molecular Imaging

MR Applications• Neuro-imaging
-Excellent tool due to high soft tissue contrast resolution
-Abundant water content of CNS allows for imaging soft intracranial tissue
• Head and Neck imaging-Multi-planar capability allows for monitoring
extent of disease
-Differentiating subtle soft tissue boundaries of head and neck

MRIAxial, T2-Weighted


MR Applications
• Body Imaging
-Thorax: mediastinal, hilar, chest wall abnormalities
• Limited lung imaging due to artifacts
• New advances in breast imaging
• Potentials for cardiac MRI with coronary MR angiography


MRIBreast Imaging

MR Applications
• MSK Imaging
- High sensitivity for neoplastic, inflammatory, and traumatic conditions of bone and soft tissue
- T1-weighted---fluid collections and abnormalities in fatty marrow
- T2-weighted---lesions in both marrow and soft tissue

MRISagittal, T1-Weighted

Innovative Modalities• Constantly evolving face of radiology
• New contrast agents for CT and MR
• Molecular Imaging
- Imaging molecular events---enzymatic activity, receptor binding, cellular events
• Interventional Radiology and Interventional Neuroradiology
Text Book
• David Sutton’s Radiology
• Clark’s Radiographic positioning and techniques

Assignment
• Two students will be selected for assignment.

Question
• Describe importance of Hysterosalpingeogram?

Thank You
60