
Basic Assumptions (Caramazza, 1984) Neurological specificity: organization of the mind parallels...
20
Basic Assumptions (Caramazza, 1984) • Neurological specificity: organization of the mind parallels organization of the brain (monist philosophy) • modularity of mind (functional) = modularity of brain (anatomical) • Transparency: the pattern of spared and impaired performance of the patient can lead to valid conclusions about the nature and function of the impaired processing components • brain damage allows one to spot more easily the workings of processes that are “opaque” in normal’s flawless performance • Subtractivity: performance of the brain damaged patient is just like the normal, intact cognitive system minus those components that were damaged by the injury. • does not mean that behavioral compensation does not occur (using functions of intact modules to compensate for damaged ones) • but, implies that the mature brain does not develop new cognitive modules following injury (substantial reorganization) • Modularity…functional and anatomical
-
Upload
edith-wilkerson -
Category
Documents
-
view
226 -
download
0
Transcript of Basic Assumptions (Caramazza, 1984) Neurological specificity: organization of the mind parallels...

Basic Assumptions (Caramazza, 1984)
• Neurological specificity: organization of the mind parallels organization of the brain (monist philosophy)
• modularity of mind (functional) = modularity of brain (anatomical)
• Transparency: the pattern of spared and impaired performance of the patient can lead to valid conclusions about the nature and function of the impaired processing components
• brain damage allows one to spot more easily the workings of processes that are “opaque” in normal’s flawless performance
• Subtractivity: performance of the brain damaged patient is just like the normal, intact cognitive system minus those components that were damaged by the injury.
• does not mean that behavioral compensation does not occur (using functions of intact modules to compensate for damaged ones)
• but, implies that the mature brain does not develop new cognitive modules following injury (substantial reorganization)
• Modularity…functional and anatomical

A hierarchy of modules• Basic Modules:
– carry out a single type of computation– no interaction with other modules until finished with it’s
process
Transducer 2: Cochlea (audition)
Input Module 2a
Mod 2b Mod 2c
Transducer 1:Retina (vision)
Input Module 1a
Mod 1c Mod 1b
Central system
• Central systems: non-modular, receive input from multiple basic modules

Modularity: “Definitions”• Fodor, Modularity of Mind, 1983
– Informational encapsulation: module functions in isolation from processes going on elsewhere; makes them more efficient
– Autonomous: does not share processes with other modules– Domain specificity: each module can only process one
particular type of input (not a gatekeeper)– Mandatory (Automatic) and Fast– Innate: determined by genetics (nature)– Hardwired: not affected by nurture
• Modularity, as adopted by cognitive neuropsychology– Domain Specificity– Informational encapsulation
• can be selectively impaired (single/double dissociations)• remains intact in the face of gross intellectual decline
(dementia)• not affected by beliefs, desires, or expectations (Coltheart)

Task Dissociation Logic
Association: Patient X shows a deficits on task A and B
• Patient X’s damage could have impaired a single functional module shared by task A and B
0
1
2
3
4
5
6
Task A Task B
# errors • Patient X’s damage could have impaired two separate functional modules
–Modules could be anatomically adjacent (e.g., Gerstmann’s syndrome), or not, if damage is widespread

Task Dissociation Logic
• Single dissociation: Patient X (case or group) is significantly more impaired on Task A than Task B relative to a control group.
Stronger
0
1
2
3
4
5
6
Task A Task B
# errors
Weaker
0
1
2
3
4
5
6
Task A Task B
Patient XControl
• Dissociations are considered to be “stronger” if:
• Task A and B are of equal difficulty (avoid “resource artifact”)• Patient(s) is/are “normal” (as good as controls) on one task.

Task Dissociation Logic• Double dissociation: Patient X (case or group) is
more impaired on Task A than B (relative to controls); Patient Y (case or group) is more impaired on Task B than A. – Considered “gold standardgold standard” of cognitive neuropsychology
research
Weaker
0
1
2
3
4
5
6
Task A Task B
Patient XControl Patient Y
Stronger
0
1
2
3
4
5
6
Task A Task B
# errors

Alternatives to modularity
• Connectionist architectures– Processing is graded, distributed and interactive– Conceptually more similar to neural populations– When distributed systems are “lesioned” they can
sometimes simulate neuropsychological impairment(Farah & McCelland, 1991; Farah, 1994)
black box module vs.

Alternatives to modularity
• Compromise:• Distributed systems inside of modular boxes
• “Cascading” processes
Methods: Case vs. Group Studies
• Case Studies: assess behavior of an individual subject who demonstrates a highly specific pattern of deficits
Vs.• Group Studies: assess average performance of a
group of patients similar with respect to area of brain damage, etiology or disorder (i.e., amnesia, anomia).
Case Studies• Advantages (argued by advocates):
– often provides evidence of highly specific cognitive modules– fine-grained analysis (conjunctions of results from multiple tasks) can be used to
develop highly sophisticated models of cognitive systems– less susceptible to Type II error
• Disadvantages (argued by detractors): – diffuse etiologies make localization difficult (where is the “neuro” in this type of
neuropsychology?)• localization of cognitive function to particular brain regions is secondary (“radical
view”), or even unimportant (“ultra” view)• why should brain damage fractionate along cognitive lines?
– questionable generalizability and replicability• “selection bias” : select patients on the basis of whether they demonstrate a particular
deficit as proof of a theory that the deficit represents a modules • problems with Type I error• how do you know whether a single individual is truly representative of the “normal”
population (premorbidly atypical subjects)

Group Studies• a priori grouping: small groups (N > 15) pre-selected to
have overlapping/ homogeneous lesion or disorder– If system is modular it is only important there is a region of overlapping
damage, not that there is heterogeneity outside this region
6 subjects:
5 subjects:

A priori grouping
• Advantages: – good localization– good generalizability/predictability– some heterogeneity in patients means that when if effect is found
it must be a large and robust enough effect to overcome the “uncontrolled” variance.
• Disadvantages: – inter-subject variability could lead to Type II error– even if homogeneous with regard to lesion or clinical disorder,
may not be homogeneous with regard to experimental tests– don’t give enough behavioral tests to get at the heart of the
problem

Group Studies• a posteriori grouping: large groups (N < 15) with more
heterogeneous lesions, grouped by behavior
Left frontal damage…a) With apraxia of speech b) Without apraxia of speech

A posteriori grouping• Advantages:
– reduces between-subject variability by using it as blocking variable
• Disadvantages: – like case-studies, this “advantage” depends on use of multiple tests
and specificity of those tests (how good they are at tapping into dissociable behaviors)

Sources of variance
• Neurological– Age– No two brains are exactly alike (like snowflakes?)
– Occult brain conditions (undetected brain damage)– Differences in lesion size– Differences in pre-morbid organization– Differences in post-morbid plasticity
• High-resolution structural and functional imaging can provide some insight into these sources

Sources of variance
• Behavioral– Different approaches to the assessment task
• distraction, strategy, motivation
CONTROL
Dig
it-M
onito
ring
(% C
orre
ct)
50403020100
110
100
90
80
70
60
STBI
50403020100
110
100
90
80
70
60
Encoding-biassubgroup
Digit-bias subgroup
Memory Performance (% Correct)Memory Performance (% Correct) 0
20
40
60
% C
orr
ect
Focused Divided
*
Control
All STBI
*
*
Encoding-bias STBI
Digit-bias STBI

Sources of variance• Behavioral
– Different approaches to the assessment task:• personality differences, cultural differences
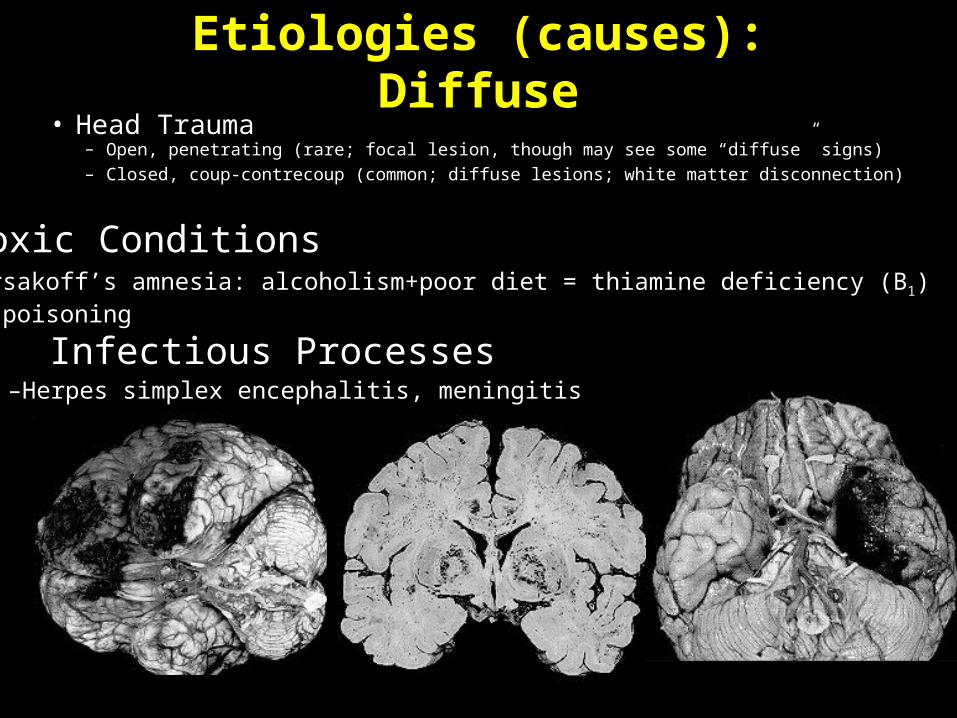
Etiologies (causes): Diffuse• Head Trauma
– Open, penetrating (rare; focal lesion, though may see some “diffuse” signs)– Closed, coup-contrecoup (common; diffuse lesions; white matter disconnection)
• Toxic Conditions–Korsakoff’s amnesia: alcoholism+poor diet = thiamine deficiency (B1) –CO poisoning
• Infectious Processes–Herpes simplex encephalitis, meningitis

Etiology (causes): Focal• Vascular Disorders*(best for group studies)
– Cerebro-vascular accident (CVA): hemorrhagic (aneurysm) or obstructive– Oxygen deprivation (anoxia/ischemia) and apoptosis (cellular suicide)
• Surgical Resection– Tumors– Epilepsy– AVM



















