Basic Airway Management
32
Airway Management
description
airway management
Transcript of Basic Airway Management

Airway Management

Objectives• Recognize signs of a threatened airway
• Manual techniques for establishing an airway
• Manual techniques of mask ventilation without or with suspected cervical spine injuryinjury
• Preparation and perform endotracheal intubation and phramacologic therapy
• Be familiar with airway adjuncts (laryngeal mask airway, combitube)

Introduction• ABC of resuscitation
• Focus is to ensure the airway is open, assess patient breathing and support gas exchange
• Secondary goal is preservation of cardiovascular stability and the prevention of cardiovascular stability and the prevention of aspiration
• Healthcare providers must be skilled in manually supporting the airway and providing the essential process of oxygenation and ventilation

Assessment• First step : Assess airway patency and
spontaneous breathing. Look, listen and feelfor air movement.
• Observe the level of consciousness and determine if respiratory efforts are absent determine if respiratory efforts are absent proceed to manual support and assist ventilation while preparing to establish the airway
• Identify injury (e.g possible cervical spine fracture)
• Observe chest expansion, to assess respiratory muscle activity and adequate ventilation

Assessment• Observe for suprasternal, supraclavicular or
intercostal retraction, tracheal tug or nasal flaring that represent respiratory distress
• Auscultate over the neck and chest for breath sounds. Complete airway obstruction if there sounds. Complete airway obstruction if there is chest movement but breath sound are absent. Incomplete obstruction if we hear snoring, stridor, gurgling or noisy breathing.
• Assess the protective airway reflexes (cough and gag). Absence of protective reflexes need for airway support.

Oxygen supplementation• Nasal cannula O2 100% 0,5-5 lt/m (FiO2 0,40-
0,50)
• Venturi mask O2 100% 6lt/m
• Aerosol face mask
• Reservoar face mask (rebreathing or non rebreathing


Airway obstruction :
The majority of preventable deaths
following trauma occur as a result of airway
Airway obstruction
following trauma occur as a result of airway
obstruction.
Obstruction may occur at any point within
the airway, from the upper airways to the
bronchi deep within the chest.

Common causes of airway obstruction
Upper Airway
- tongue (due to unconsciousness)
- soft tissue swelling
- blood, vomit
- direct injury
Larynx (voice box) Larynx (voice box)
- foreign material, direct injury, soft tissue swelling
Lower Airway
- secretions, oedema, blood
- bronchospasm
- aspiration of gastric contents

LOOK for chest/abdominal movement
LISTEN at mouth and nose for breath sounds and
abnormal noises
FEEL at mouth and nose for expired air
Recognition of airway obstruction
FEEL at mouth and nose for expired air
Abnormal sounds in airway obstruction
Snoring - due to obstruction of upper airway by
the tongue
Gurgling - due to obstruction of upper airway by
liquids (blood, vomit)
Wheezing - due to narrowing of the lower airways
Complete airway obstruction is silent.

For pediatric patients• Common causes of airway obstruction is
upper airway infection (e.g viral croup, bacterial tracheitis, epiglottitis)
• Airway obstruction in semiconscious child is posterior displacement of tongue and collapse posterior displacement of tongue and collapse of hypopharynx
• Infant until 6 month age is obligate nose-breather, suctioning the nares can be useful in cleaning the airway.

Manual methods to establish an airway• Initial step to assure a patent airway in a
spontaneously breathing patient without possible injury to the cervical spine is Triple airway maneuver : neck extension, elevation of mandible (jaw thrust), mouth openingof mandible (jaw thrust), mouth opening

Manual in-line stabilisation of the c-spine
Head tilt (NOT if c-spine injury)
Chin lift with manual in-line stabilisation of the c-
spine
Opening the airway
spine
Jaw thrust with manual in-line stabilisation of the
c-spine
Suction with manual in-line stabilisation of the c-
spine


Mouth to mouth ventilation

Oral airways
Will stimulate vomiting and movement in
conscious or semi-conscious casualties
This may result in;
worsening airway problems
cervical spine compromise


Nasal airways
Will cause bleeding from the nose in a large
number of cases.
This will result in worsening airway problems so use
only as a last resort.

Manual Mask Ventilation• Indication :
- Patient is apneic
- Spontaneous tidal volume is inadequate
- Reduce the work of breating- Reduce the work of breating
- Hypoxemia due to poor spontaneous
ventilation


Manual Mask Ventilation
• Single handed method, left hand hold the mask placement, bag reservoir compressed by right hand
• Observe the chest expansion and auscultation• Observe the chest expansion and auscultation
• Listen for any gas leaks around the mask
• If patient apneic ventilation is performed 12-16 times per minute. If spontaneous breathing ventilation synchronized with patient inspiratory efforts
• Oxygen 100% at flow rate 15 l/minute

Cricoid pressure

Manual Mask Ventilation• If no cervical spine injury, the operator can do
slight neck extension, mandibular elevation and gentle downward pressure the mask on the face
• If cervical spine injury is suspected the • If cervical spine injury is suspected the operator should not do neck extension, may choose two handed for mask placement but assure no neck movement

Endotracheal intubation• Indication :
- airway protection
- relief of obstruction
- mechanical ventilation & oxygen - mechanical ventilation & oxygen
therapy
- respiratory failure
- shock
- hyperventilation for intracranial
hypertension
- reducing work of breathing
- facilitation of suctioning/pulmonary toilet





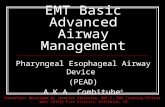
Laryngeal Mask


Combitube

Thank you