
Baseline Silent Cerebral Infarctio in thne Asymptomatic...
9
1122 Baseline Silent Cerebral Infarction in the Asymptomatic Carotid Atherosclerosis Study Thomas Brott, MD; Thomas Tomsick, MD; William Feinberg, MD; Constance Johnson, MD; Jose Biller, MD; Joseph Broderick, MD; Michael Kelly, MD; James Frey, MD; Skai Schwartz, MA; Christine Blum, RN, MSN; J.J. Nelson, MSPH; Lloyd Chambless, PhD; James Toole, MD, for the Asymptomatic Carotid Atherosclerosis Study Investigators Background and Purpose In a group of patients with high- grade asymptomatic carotid artery stenosis, we prospectively determined the prevalence and radiological characteristics of clinically asymptomatic brain infarction evident on computed tomography. Risk factors and extent of carotid disease were also determined. Methods Patients randomized into the Asymptomatic Ca- rotid Atherosclerosis Study (ACAS) underwent a neurological history, a detailed stroke/transient ischemic attack question- naire, and a detailed neurological examination. Computed tomography scans were examined by standardized criteria developed as part of a quality-control program supervised by a neuroradiologist. The presence, location, and size of all cere- bral infarctions evident by computed tomography were determined. Results Among 1132 patients, 848 had no history of stroke or transient ischemic attack. One hundred twenty-six patients (15%) had a silent infarct; 95 (11%) had one, 24 (3%) had two, W ith the development of high-resolution brain imaging, the limitations of the neurological history and examination in identifying brain pathology have become increasingly apparent. Today the diagnosis of transient ischemic attack (TIA) may be associated with imaging evidence for cerebral infarction by brain computed tomography (CT)'- 7 or by magnetic resonance imaging (MRI). 8 Thus the imaging diagnosis of cerebral infarction is increasingly made for patients evaluated by CT or MRI in the absence of typical symptoms or signs of stroke (eg, patients evaluated for dementia or headache). The Asymptomatic Carotid Atherosclerosis Study (ACAS) 9 is a multicenter, randomized trial comparing carotid endarterectomy plus medical therapy with med- ical therapy alone for treatment of hemodynamically significant but asymptomatic carotid artery stenosis. We Received November 30, 1993; final revision received March 3, 1994; accepted March 4, 1994. From the University of Cincinnati Medical Center, Ohio (T.B., T.T., J.Broderick, C.B.); Arizona Health Sciences Center, Tucson, Ariz (W.F.); Francis Scott Key Medical Center, Baltimore, Md (C.J.); Northwestern University Medical School, Chicago, 111 (j.Biller); Loyola University Medical Center, Maywood, III (M.K.); Barrow Neurological Institute, Phoenix, Ariz (J.F.); Uni- versity of North Carolina at Chapel Hill (S.S., J.J.N., L.C.); and The Bowman Gray School of Medicine, Wake Forest University, Winston-Salem, NC (J.T.). Correspondence to Thomas Brott, MD, Dept of Neurology, University of Cincinnati Medical Center, 231 Bethesda Ave, Cincinnati, OH 45267-0525. and 7 (1%) had three or more infarcts. The infarct size was small and deep for 117 patients (72%), less than one-half lobe for 45 (28%), and one-half to less than one lobe for 1 (0.5%). The silent infarcts were evenly distributed ipsilaterally and contralaterally to the study artery but were significantly more frequent in the right hemisphere (P<.05). Factors associated with silent infarction were abnormal gait (/ > <.001), abnormal deep tendon reflexes or plantar responses (P=.O38), but not degree of carotid stenosis. Silent infarction was less frequent among this totally asymptomatic cohort (15%) compared with those with transient ischemic attacks (34/139, 25%; P<.001). Conclusions Silent infarction in the setting of asymptomatic carotid stenosis is not uncommon, but silent infarctions are rarely sizable. The clinical significance of silent cerebral in- farction in patients with asymptomatic carotid artery stenosis has yet to be established. (Stroke. 1994;25:1122-1129.) Key Words • carotid artery diseases • cerebral infarction • clinical trials believe this cohort is at high risk for symptomatic ischemic stroke and hypothesized that the cohort may also be at high risk for asymptomatic, "silent" stroke. We report the baseline CT scan characteristics obtained for patients enrolled in the ACAS trial without a history of stroke. The number, size, and location of the silent cerebral infarcts are described. The potential relations of silent cerebral infarction to stroke risk factors, the neurological examination, and the degree of carotid stenosis are addressed. Subjects and Methods ACAS is a multicenter, randomized trial of carotid endar- terectomy for asymptomatic, hemodynamically significant ca- rotid artery stenosis. Patient enrollment ended in December 1993. To be eligible, patients had to be between the ages of 40 and 79 years and had to have a unilateral or bilateral surgically accessible stenosis of the common or internal carotid artery of at least 60% (determined by criteria that have been previously described). 9 ' 10 A TIA/stroke questionnaire was administered to each patient to supplement the neurological history and standardized neurological examination." Patients were also given the Folstein Mini-Mental Status test. Candidates did not qualify if a history of TIA or stroke ipsilateral to the study artery was detected or if a history of vertebrobasilar distribu- tion TIA or stroke was detected. Other exclusions were serious cardiac, respiratory, or neoplastic disease that would limit survival to 5 years or less; focal seizures within the last 2 years; confounding neurological illness causing transient deficits; uncontrolled hypertension; warfarin use; previous ipsilateral carotid surgery or cervical region radiation; intolerance for by guest on July 9, 2018 http://stroke.ahajournals.org/ Downloaded from
Transcript of Baseline Silent Cerebral Infarctio in thne Asymptomatic...
1122
Baseline Silent Cerebral Infarction in theAsymptomatic Carotid Atherosclerosis Study
Thomas Brott, MD; Thomas Tomsick, MD; William Feinberg, MD; Constance Johnson, MD;
Jose Biller, MD; Joseph Broderick, MD; Michael Kelly, MD; James Frey, MD; Skai Schwartz, MA;Christine Blum, RN, MSN; J.J. Nelson, MSPH; Lloyd Chambless, PhD; James Toole, MD, for
the Asymptomatic Carotid Atherosclerosis Study Investigators
Background and Purpose In a group of patients with high-grade asymptomatic carotid artery stenosis, we prospectivelydetermined the prevalence and radiological characteristics ofclinically asymptomatic brain infarction evident on computedtomography. Risk factors and extent of carotid disease werealso determined.
Methods Patients randomized into the Asymptomatic Ca-rotid Atherosclerosis Study (ACAS) underwent a neurologicalhistory, a detailed stroke/transient ischemic attack question-naire, and a detailed neurological examination. Computedtomography scans were examined by standardized criteriadeveloped as part of a quality-control program supervised by aneuroradiologist. The presence, location, and size of all cere-bral infarctions evident by computed tomography weredetermined.
Results Among 1132 patients, 848 had no history of strokeor transient ischemic attack. One hundred twenty-six patients(15%) had a silent infarct; 95 (11%) had one, 24 (3%) had two,
With the development of high-resolution brainimaging, the limitations of the neurologicalhistory and examination in identifying brain
pathology have become increasingly apparent. Todaythe diagnosis of transient ischemic attack (TIA) may beassociated with imaging evidence for cerebral infarctionby brain computed tomography (CT)'-7 or by magneticresonance imaging (MRI).8 Thus the imaging diagnosisof cerebral infarction is increasingly made for patientsevaluated by CT or MRI in the absence of typicalsymptoms or signs of stroke (eg, patients evaluated fordementia or headache).
The Asymptomatic Carotid Atherosclerosis Study(ACAS)9 is a multicenter, randomized trial comparingcarotid endarterectomy plus medical therapy with med-ical therapy alone for treatment of hemodynamicallysignificant but asymptomatic carotid artery stenosis. We
Received November 30, 1993; final revision received March 3,1994; accepted March 4, 1994.
From the University of Cincinnati Medical Center, Ohio (T.B.,T.T., J.Broderick, C.B.); Arizona Health Sciences Center, Tucson,Ariz (W.F.); Francis Scott Key Medical Center, Baltimore, Md(C.J.); Northwestern University Medical School, Chicago, 111(j.Biller); Loyola University Medical Center, Maywood, III(M.K.); Barrow Neurological Institute, Phoenix, Ariz (J.F.); Uni-versity of North Carolina at Chapel Hill (S.S., J.J.N., L.C.); andThe Bowman Gray School of Medicine, Wake Forest University,Winston-Salem, NC (J.T.).
Correspondence to Thomas Brott, MD, Dept of Neurology,University of Cincinnati Medical Center, 231 Bethesda Ave,Cincinnati, OH 45267-0525.
and 7 (1%) had three or more infarcts. The infarct size wassmall and deep for 117 patients (72%), less than one-half lobefor 45 (28%), and one-half to less than one lobe for 1 (0.5%).
The silent infarcts were evenly distributed ipsilaterally andcontralaterally to the study artery but were significantly morefrequent in the right hemisphere (P<.05). Factors associatedwith silent infarction were abnormal gait (/><.001), abnormaldeep tendon reflexes or plantar responses (P=.O38), but notdegree of carotid stenosis. Silent infarction was less frequentamong this totally asymptomatic cohort (15%) compared withthose with transient ischemic attacks (34/139, 25%; P<.001).
Conclusions Silent infarction in the setting of asymptomaticcarotid stenosis is not uncommon, but silent infarctions arerarely sizable. The clinical significance of silent cerebral in-farction in patients with asymptomatic carotid artery stenosishas yet to be established. (Stroke. 1994;25:1122-1129.)
Key Words • carotid artery diseases • cerebral infarction• clinical trials
believe this cohort is at high risk for symptomaticischemic stroke and hypothesized that the cohort mayalso be at high risk for asymptomatic, "silent" stroke.We report the baseline CT scan characteristics obtainedfor patients enrolled in the ACAS trial without a historyof stroke. The number, size, and location of the silentcerebral infarcts are described. The potential relationsof silent cerebral infarction to stroke risk factors, theneurological examination, and the degree of carotidstenosis are addressed.
Subjects and MethodsACAS is a multicenter, randomized trial of carotid endar-
terectomy for asymptomatic, hemodynamically significant ca-rotid artery stenosis. Patient enrollment ended in December1993. To be eligible, patients had to be between the ages of 40and 79 years and had to have a unilateral or bilateral surgicallyaccessible stenosis of the common or internal carotid artery ofat least 60% (determined by criteria that have been previouslydescribed).9'10 A TIA/stroke questionnaire was administeredto each patient to supplement the neurological history andstandardized neurological examination." Patients were alsogiven the Folstein Mini-Mental Status test. Candidates did notqualify if a history of TIA or stroke ipsilateral to the studyartery was detected or if a history of vertebrobasilar distribu-tion TIA or stroke was detected. Other exclusions were seriouscardiac, respiratory, or neoplastic disease that would limitsurvival to 5 years or less; focal seizures within the last 2 years;confounding neurological illness causing transient deficits;uncontrolled hypertension; warfarin use; previous ipsilateralcarotid surgery or cervical region radiation; intolerance for
by guest on July 9, 2018http://stroke.ahajournals.org/
Dow
nloaded from
Brott et al Baseline Silent Cerebral Infarction in ACAS 1123
aspirin; other factors that could be contraindications forsurgery or prevent 5-year follow-up; and confounding majorneurological examination abnormalities in the distribution ofthe ACAS artery (eg, a patient with cerebral palsy was noteligible if a major hemiparesis was present, ipsilateral to theACAS artery, but was eligible if the hemiparesis was modest).
Each patient randomized into ACAS underwent brain CTexamination at baseline and will have another CT at the timeof any end point and at the time of study exit. The baseline CTscans were obtained after the neurological histories and exam-inations were carried out and after randomization, except inthose circumstances where a CT had been performed within 3months before randomization and was available for analysis. ACT lesion played no role in eligibility or randomization. TheCT examinations were noncontrast and followed similar butnot identical imaging protocols. For the most part, the CTexaminations were performed with 10-mm slice thicknessreconstructed on a 512x512 matrix with 15° orbital-meatalangle slices; a window level of 50 and a window width of 100Hounsfield units were used.
Silent infarcts were defined as any circumscribed low atten-uation consistent with cerebral infarction (ie, infarct by CT)occurring in any cerebral location in patients without a historyof stroke. The vascular distribution of each infarct was deter-mined after the method of Damasio,12 and arterial distributiontemplates were used. For a qualitative estimate of lesionvolume, a cerebral lobe was used as the unit of measurement.Lesions were then subdivided into four categories: small anddeep, less than one-half lobe, up to one lobe, and larger thanone lobe. Lesion size was also assessed by an estimate of thevolume of low attenuation by CT.
A CT quality-control program was carried out to attain adegree of uniformity in the readings. Before the beginning ofrecruitment, each center received five scans, chosen to includesome difficult or potentially ambiguous diagnostic problems.The readings from the centers were then compared with thoseof the study neuroradiologist (T.T.). Potential reasons fordisagreement were communicated to the local center reader.In addition to this initial test, ongoing monitoring continues.The CT scan films and completed CT scan forms for the firstfive randomized patients from each center were submitted tothe central neuroradiologist for blind rereading. Again, poten-tial explanations for disagreements were determined by thecentral neuroradiologist and communicated to the localreader. This process was repeated 1 year after a center beganrecruitment as well as on three additional occasions.
The results from the CT quality-control program and fromthe baseline CT scan readings were analyzed at the ACASStatistical Coordinating Center. A x2 t e s t was used when all ofthe cell sizes in the 2x2 table were 10 or greater. When anycell size was less than 10, a Fisher's exact test was used instead.All tests were two sided, and significance was declared whenthe rounded probability value was less than .05. No adjust-ments for multiple comparisons were made.
ResultsCharacteristics of the ACAS population with no
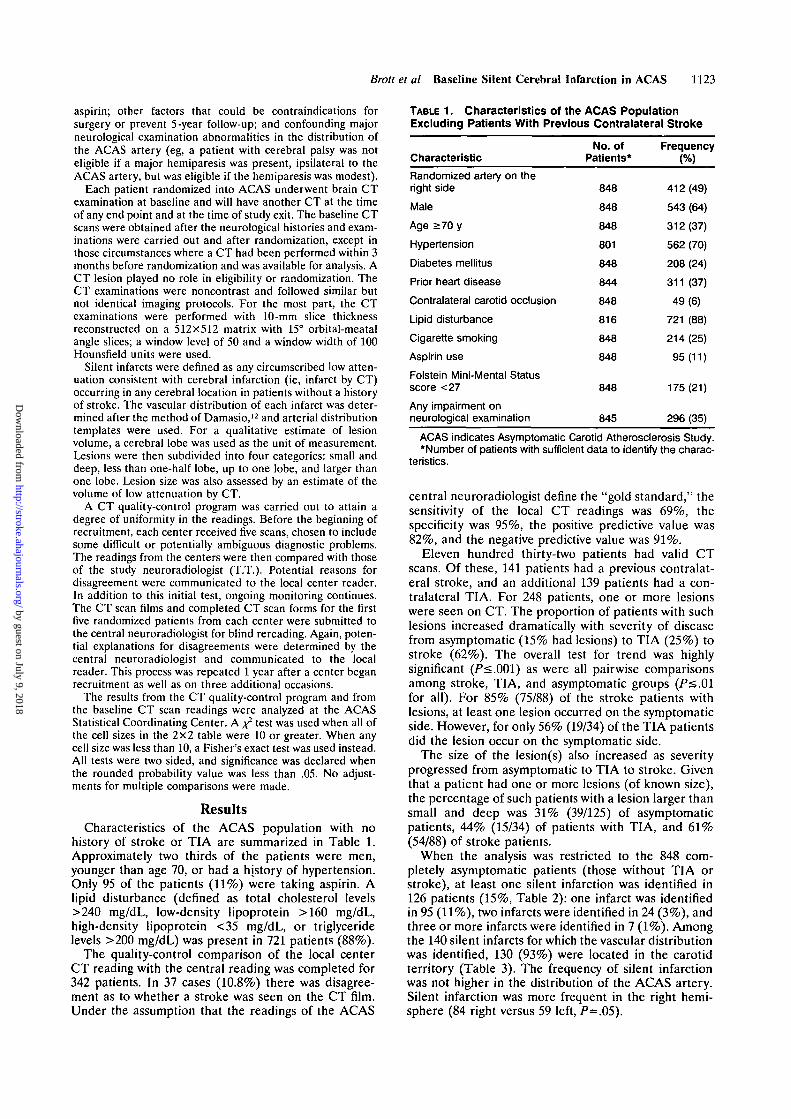
history of stroke or TIA are summarized in Table 1.Approximately two thirds of the patients were men,younger than age 70, or had a history of hypertension.Only 95 of the patients (11%) were taking aspirin. Alipid disturbance (defined as total cholesterol levels>240 mg/dL, low-density lipoprotein >160 mg/dL,high-density lipoprotein <35 mg/dL, or triglyceridelevels >200 mg/dL) was present in 721 patients (88%).
The quality-control comparison of the local centerCT reading with the central reading was completed for342 patients. In 37 cases (10.8%) there was disagree-ment as to whether a stroke was seen on the CT film.Under the assumption that the readings of the ACAS
TABLE 1. Characteristics of the ACAS PopulationExcluding Patients With Previous Contralateral Stroke
Characteristic
Randomized artery on theright side
Male
Age >70 y
Hypertension
Diabetes mellitus
Prior heart disease
Contralateral carotid occlusion
Lipid disturbance
Cigarette smoking
Aspirin use
Folstein Mini-Mental Statusscore <27
Any impairment onneurological examination
No. ofPatients*
848
848
848
801
848
844
848
816
848
848
848
845
Frequency(%)
412(49)
543 (64)
312(37)
562 (70)
208 (24)
311 (37)
49(6)
721 (88)
214(25)
95 (11)
175(21)
296 (35)
ACAS indicates Asymptomatic Carotid Atherosclerosis Study.*Number of patients with sufficient data to identify the charac-
teristics.
central neuroradiologist define the "gold standard," thesensitivity of the local CT readings was 69%, thespecificity was 95%, the positive predictive value was82%, and the negative predictive value was 91%.
Eleven hundred thirty-two patients had valid CTscans. Of these, 141 patients had a previous contralat-eral stroke, and an additional 139 patients had a con-tralateral TIA. For 248 patients, one or more lesionswere seen on CT. The proportion of patients with suchlesions increased dramatically with severity of diseasefrom asymptomatic (15% had lesions) to TIA (25%) tostroke (62%). The overall test for trend was highlysignificant (P<.001) as were all pairwise comparisonsamong stroke, TIA, and asymptomatic groups (P<.01for all). For 85% (75/88) of the stroke patients withlesions, at least one lesion occurred on the symptomaticside. However, for only 56% (19/34) of the TIA patientsdid the lesion occur on the symptomatic side.
The size of the lesion(s) also increased as severityprogressed from asymptomatic to TIA to stroke. Giventhat a patient had one or more lesions (of known size),the percentage of such patients with a lesion larger thansmall and deep was 31% (39/125) of asymptomaticpatients, 44% (15/34) of patients with TIA, and 61%(54/88) of stroke patients.
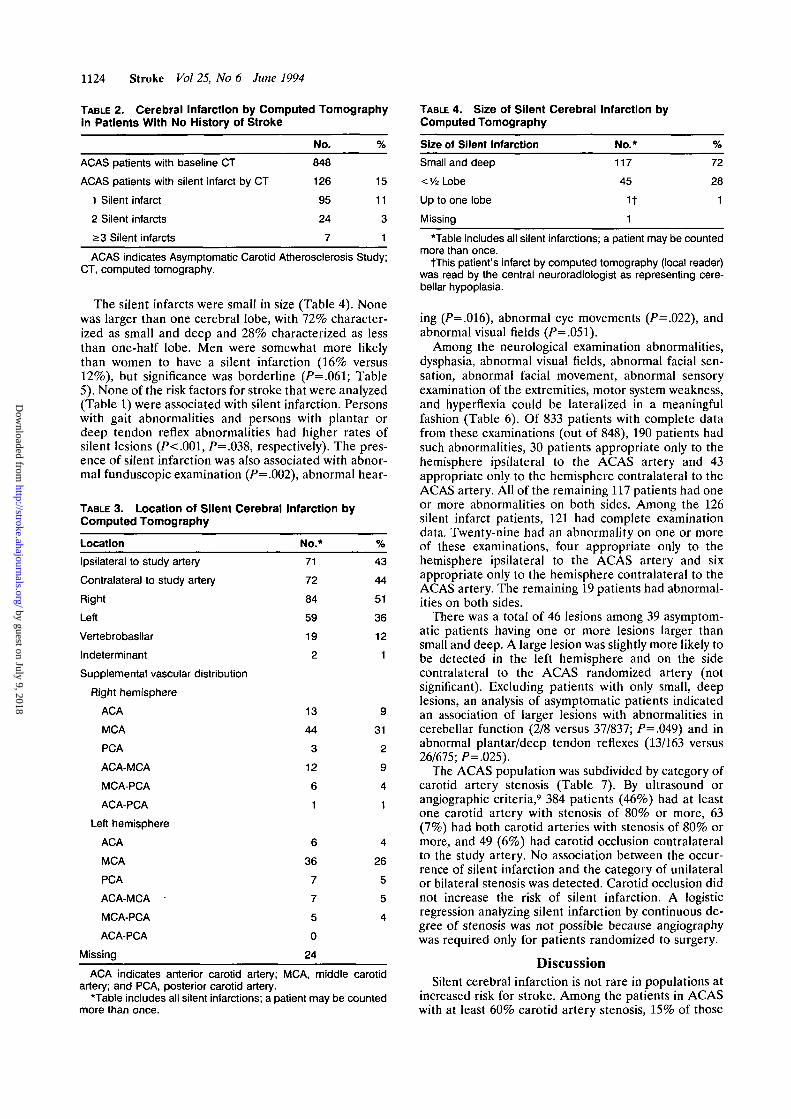
When the analysis was restricted to the 848 com-pletely asymptomatic patients (those without TIA orstroke), at least one silent infarction was identified in126 patients (15%, Table 2): one infarct was identifiedin 95 (11%), two infarcts were identified in 24 (3%), andthree or more infarcts were identified in 7 (1%). Amongthe 140 silent infarcts for which the vascular distributionwas identified, 130 (93%) were located in the carotidterritory (Table 3). The frequency of silent infarctionwas not higher in the distribution of the ACAS artery.Silent infarction was more frequent in the right hemi-sphere (84 right versus 59 left, />=.05).
by guest on July 9, 2018http://stroke.ahajournals.org/
Dow
nloaded from
1124 Stroke Vol 25, No 6 June 1994
TABLE 2. Cerebral Infarction by Computed Tomographyin Patients With No History of Stroke
No. %
ACAS patients with baseline CT 848
ACAS patients with silent infarct by CT 126 15
1 Silent infarct 95 11
2 Silent infarcts 24 3
>3 Silent infarcts 7 1
ACAS indicates Asymptomatic Carotid Atherosclerosis Study;CT, computed tomography.
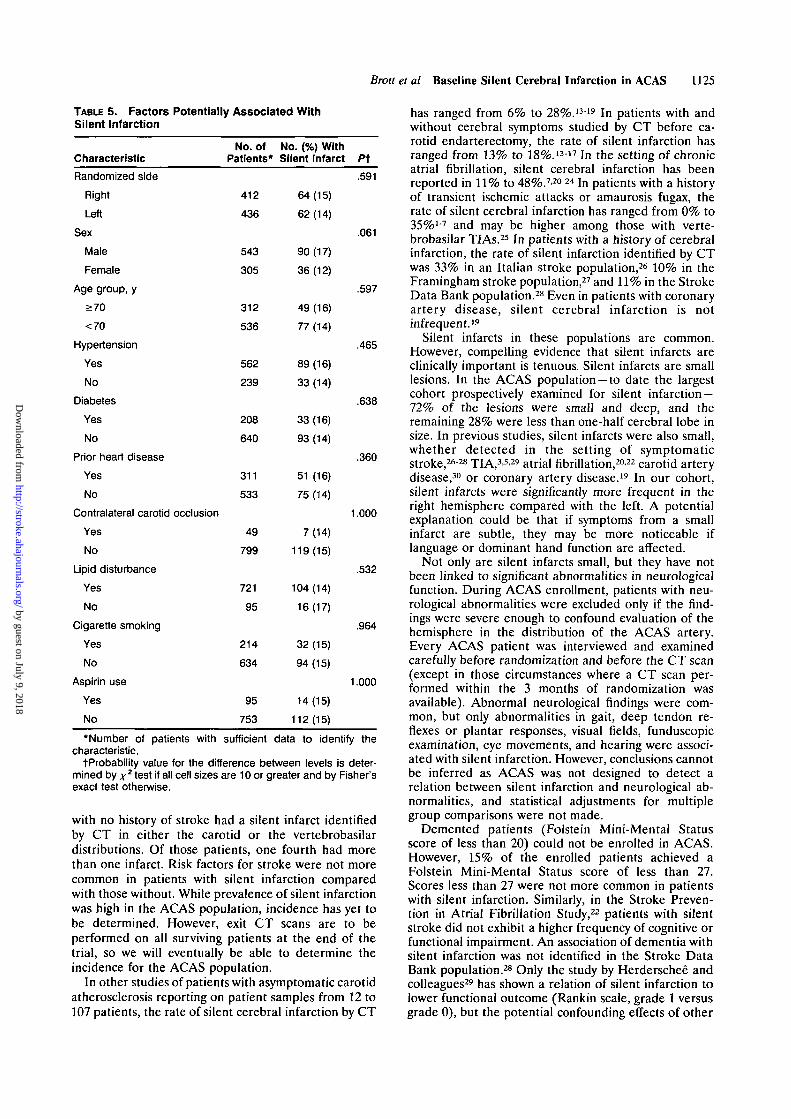
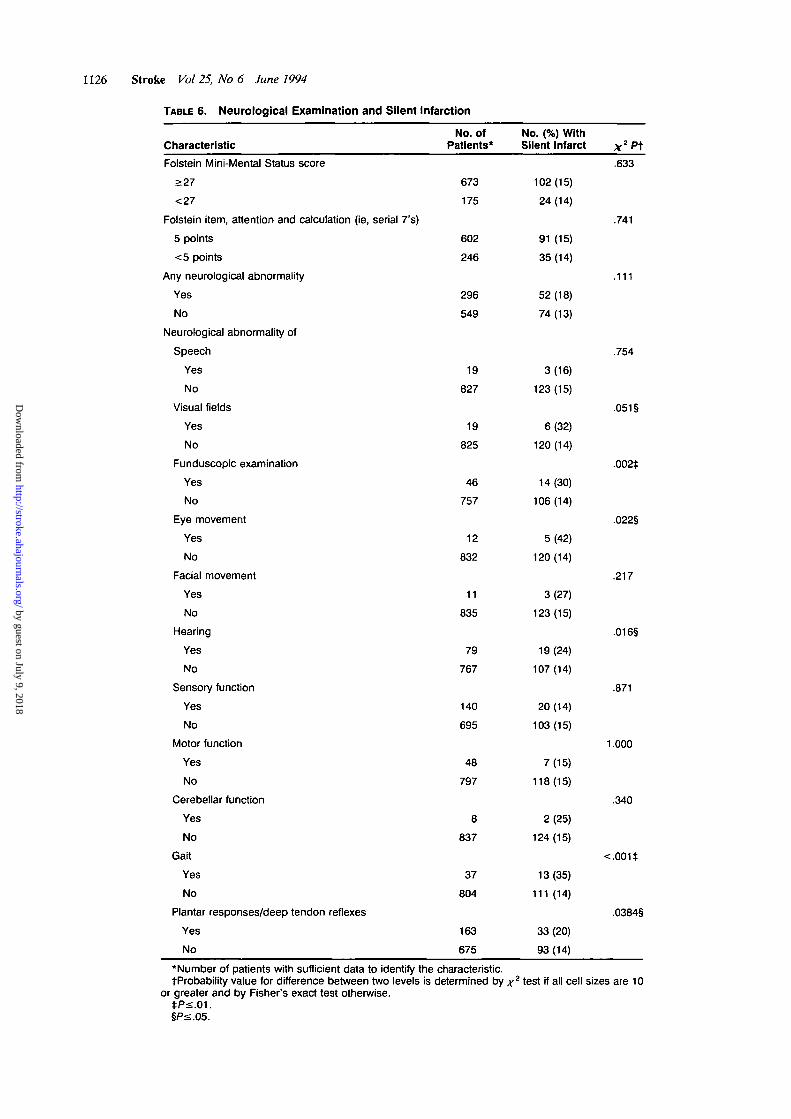
The silent infarcts were small in size (Table 4). Nonewas larger than one cerebral lobe, with 72% character-ized as small and deep and 28% characterized as lessthan one-half lobe. Men were somewhat more likelythan women to have a silent infarction (16% versus12%), but significance was borderline (P=.O61; Table5). None of the risk factors for stroke that were analyzed(Table 1) were associated with silent infarction. Personswith gait abnormalities and persons with plantar ordeep tendon reflex abnormalities had higher rates ofsilent lesions (P<.001, P=.O38, respectively). The pres-ence of silent infarction was also associated with abnor-mal funduscopic examination (P=.OO2), abnormal hear-
TABLE 3. Location of Silent Cerebral Infarction byComputed Tomography
TABLE 4. Size of Silent Cerebral Infarction byComputed Tomography
Size of Silent Infarction No.*
Location
Ipsilateral to study artery
Contralateral to study artery
Right
Left
Vertebrobasilar
Indeterminant
Supplemental vascular distribution
Right hemisphere
ACA
MCA
PCA
ACA-MCA
MCA-PCA
ACA-PCA
Left hemisphere
ACA
MCA
PCA
ACA-MCA •
MCA-PCA
ACA-PCA
Missing
No.*
71
72
84
59
19
2
13
44
3
12
6
1
6
36
7
7
5
0
24
%
43
44
51
36
12
1
9
31
2
9
4
1
4
26
5
5
4
Small and deep
< 1/2 Lobe
Up to one lobe
Missing
117
45
1t1
72
28
1
ACA indicates anterior carotid artery; MCA, middle carotidartery; and PCA, posterior carotid artery.
*Table includes all silent infarctions; a patient may be countedmore than once.
*Table includes all silent infarctions; a patient may be countedmore than once.
tThis patient's infarct by computed tomography (local reader)was read by the central neuroradiologist as representing cere-bellar hypoplasia.
ing (/>=.O16), abnormal eye movements (P=.O22), andabnormal visual fields (P=.O51).
Among the neurological examination abnormalities,dysphasia, abnormal visual fields, abnormal facial sen-sation, abnormal facial movement, abnormal sensoryexamination of the extremities, motor system weakness,and hyperflexia could be lateralized in a meaningfulfashion (Table 6). Of 833 patients with complete datafrom these examinations (out of 848), 190 patients hadsuch abnormalities, 30 patients appropriate only to thehemisphere ipsilateral to the ACAS artery and 43appropriate only to the hemisphere contralateral to theACAS artery. All of the remaining 117 patients had oneor more abnormalities on both sides. Among the 126silent infarct patients, 121 had complete examinationdata. Twenty-nine had an abnormality on one or moreof these examinations, four appropriate only to thehemisphere ipsilateral to the ACAS artery and sixappropriate only to the hemisphere contralateral to theACAS artery. The remaining 19 patients had abnormal-ities on both sides.
There was a total of 46 lesions among 39 asymptom-atic patients having one or more lesions larger thansmall and deep. A large lesion was slightly more likely tobe detected in the left hemisphere and on the sidecontralateral to the ACAS randomized artery (notsignificant). Excluding patients with only small, deeplesions, an analysis of asymptomatic patients indicatedan association of larger lesions with abnormalities incerebellar function (2/8 versus 37/837; P=.O49) and inabnormal plantar/deep tendon reflexes (13/163 versus26/675; P=.025).
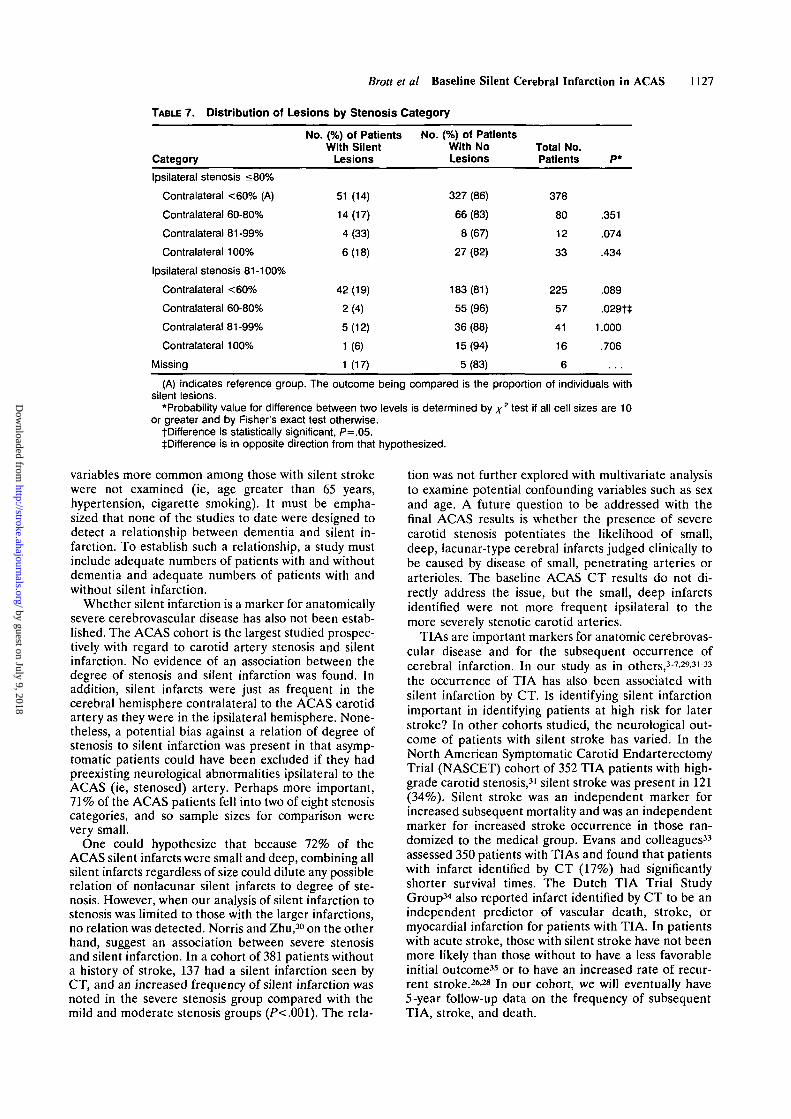
The ACAS population was subdivided by category ofcarotid artery stenosis (Table 7). By ultrasound orangiographic criteria,9 384 patients (46%) had at leastone carotid artery with stenosis of 80% or more, 63(7%) had both carotid arteries with stenosis of 80% ormore, and 49 (6%) had carotid occlusion contralateralto the study artery. No association between the occur-rence of silent infarction and the category of unilateralor bilateral stenosis was detected. Carotid occlusion didnot increase the risk of silent infarction. A logisticregression analyzing silent infarction by continuous de-gree of stenosis was not possible because angiographywas required only for patients randomized to surgery.
DiscussionSilent cerebral infarction is not rare in populations at
increased risk for stroke. Among the patients in ACASwith at least 60% carotid artery stenosis, 15% of those
by guest on July 9, 2018http://stroke.ahajournals.org/
Dow
nloaded from
Brott et al Baseline Silent Cerebral Infarction in ACAS 1125
TABLE 5. Factors Potentially Associated WithSilent Infarction
Characteristic
Randomized side
Right
Left
Sex
Male
Female
Age group, y
>70
<70
Hypertension
Yes
No
Diabetes
Yes
No
Prior heart disease
Yes
No
Contralateral carotid occlusion
Yes
No
Lipid disturbance
Yes
No
Cigarette smoking
Yes
No
Aspirin use
Yes
No
No. ofPatients*
412
436
543
305
312
536
562
239
208
640
311
533
49
799
721
95
214
634
95
753
No. (%) WithSilent Infarct
64(15)
62 (14)
90 (17)
36 (12)
49 (16)
77 (14)
89(16)
33(14)
33(16)
93(14)
51 (16)
75 (14)
7(14)
119(15)
104(14)
16(17)
32 (15)
94 (15)
14(15)
112 (15)
Pt.591
.061
.597
.465
.638
.360
1.000
.532
.964
1.000
*Number of patients with sufficient data to identify thecharacteristic.
tProbability value for the difference between levels is deter-mined by x2 test if all cell sizes are 10 or greater and by Fisher'sexact test otherwise.
with no history of stroke had a silent infarct identifiedby CT in either the carotid or the vertebrobasilardistributions. Of those patients, one fourth had morethan one infarct. Risk factors for stroke were not morecommon in patients with silent infarction comparedwith those without. While prevalence of silent infarctionwas high in the ACAS population, incidence has yet tobe determined. However, exit CT scans are to beperformed on all surviving patients at the end of thetrial, so we will eventually be able to determine theincidence for the ACAS population.
In other studies of patients with asymptomatic carotidatherosclerosis reporting on patient samples from 12 to107 patients, the rate of silent cerebral infarction by CT
has ranged from 6% to 28%.1319 In patients with andwithout cerebral symptoms studied by CT before ca-rotid endarterectomy, the rate of silent infarction hasranged from 13% to 18%.1317 In the setting of chronicatrial fibrillation, silent cerebral infarction has beenreported in 11% to 48%.7-20-24 In patients with a historyof transient ischemic attacks or amaurosis fugax, therate of silent cerebral infarction has ranged from 0% to35%'-7 and may be higher among those with verte-brobasilar TIAs.25 In patients with a history of cerebralinfarction, the rate of silent infarction identified by CTwas 33% in an Italian stroke population,26 10% in theFramingham stroke population,27 and 11% in the StrokeData Bank population.28 Even in patients with coronaryartery disease, silent cerebral infarction is notinfrequent.19
Silent infarcts in these populations are common.However, compelling evidence that silent infarcts areclinically important is tenuous. Silent infarcts are smalllesions. In the ACAS population —to date the largestcohort prospectively examined for silent infarction —72% of the lesions were small and deep, and theremaining 28% were less than one-half cerebral lobe insize. In previous studies, silent infarcts were also small,whether detected in the setting of symptomaticstroke,2628TIA,3-5-29 atrial fibrillation,2022 carotid arterydisease,30 or coronary artery disease.19 In our cohort,silent infarcts were significantly more frequent in theright hemisphere compared with the left. A potentialexplanation could be that if symptoms from a smallinfarct are subtle, they may be more noticeable iflanguage or dominant hand function are affected.
Not only are silent infarcts small, but they have notbeen linked to significant abnormalities in neurologicalfunction. During ACAS enrollment, patients with neu-rological abnormalities were excluded only if the find-ings were severe enough to confound evaluation of thehemisphere in the distribution of the ACAS artery.Every ACAS patient was interviewed and examinedcarefully before randomization and before the CT scan(except in those circumstances where a CT scan per-formed within the 3 months of randomization wasavailable). Abnormal neurological findings were com-mon, but only abnormalities in gait, deep tendon re-flexes or plantar responses, visual fields, funduscopicexamination, eye movements, and hearing were associ-ated with silent infarction. However, conclusions cannotbe inferred as ACAS was not designed to detect arelation between silent infarction and neurological ab-normalities, and statistical adjustments for multiplegroup comparisons were not made.
Demented patients (Folstein Mini-Mental Statusscore of less than 20) could not be enrolled in ACAS.However, 15% of the enrolled patients achieved aFolstein Mini-Mental Status score of less than 27.Scores less than 27 were not more common in patientswith silent infarction. Similarly, in the Stroke Preven-tion in Atrial Fibrillation Study,22 patients with silentstroke did not exhibit a higher frequency of cognitive orfunctional impairment. An association of dementia withsilent infarction was not identified in the Stroke DataBank population.28 Only the study by Herderschee andcolleagues29 has shown a relation of silent infarction tolower functional outcome (Rankin scale, grade 1 versusgrade 0), but the potential confounding effects of other
by guest on July 9, 2018http://stroke.ahajournals.org/
Dow
nloaded from
1126 Stroke Vol 25, No 6 June 1994
TABLE 6. Neurological Examination and Silent Infarction
Characteristic
Folstein Mini-Mental Status score
>27
<27
Folstein item, attention and calculation (ie, serial 7's)
5 points
<5 points
Any neurological abnormality
Yes
No
Neurological abnormality of
Speech
Yes
No
Visual fields
Yes
No
Funduscopic examination
Yes
No
Eye movement
Yes
No
Facial movement
Yes
No
Hearing
Yes
No
Sensory function
Yes
No
Motor function
Yes
No
Cerebellar function
Yes
No
Gait
Yes
No
Plantar responses/deep tendon reflexes
Yes
No
No. OfPatients*
673
175
602
246
296
549
19
827
19
825
46
757
12
832
11
835
79
767
140
695
48
797
8
837
37
804
163
675
No. (%) WithSilent Infarct
102(15)
24(14)
91 (15)
35 (14)
52 (18)
74 (13)
3(16)
123(15)
6(32)
120(14)
14(30)
106 (14)
5(42)
120 (14)
3(27)
123(15)
19 (24)
107(14)
20 (14)
103(15)
7(15)
118(15)
2(25)
124(15)
13(35)
111 (14)
33 (20)
93(14)
X2Pt.633
.741
.111
.754
.051§
.002*
.022§
.217
.016§
.871
1.000
.340
<.001t
.0384§
*Number of patients with sufficient data to identify the characteristic.tProbability value for difference between two levels is determined by x2 test if all cell sizes are 10
or greater and by Fisher's exact test otherwise.tP<.01.§P<.05.
by guest on July 9, 2018http://stroke.ahajournals.org/
Dow
nloaded from
Brott et al Baseline Silent Cerebral Infarction in ACAS 1127
TABLE 7. Distribution of Lesions by Stenosis Category
Category
Ipsilateral stenosis <80%
Contralateral <60% (A)
Contralateral 60-80%
Contralateral 81-99%
Contralateral 100%
Ipsilateral stenosis 81-100%
Contralateral <60%
Contralateral 60-80%
Contralateral 81-99%
Contralateral 100%
Missing
No. (%) of PatientsWith Silent
Lesions
51 (14)
14(17)
4(33)
6(18)
42(19)
2(4)
5(12)
1 (6)
1 (17)
No. (%) of PatientsWith NoLesions
327 (86)
66 (83)
8(67)
27 (82)
183(81)
55 (96)
36 (88)
15(94)
5(83)
Total No.Patients
378
80
12
33
225
57
41
16
6
P*
.351
.074
.434
.089
.029t*
1.000
.706
(A) indicates reference group. The outcome being compared is the proportion of individuals withsilent lesions.
*Probability value for difference between two levels is determined by x2 t e s t if all cell sizes are 10or greater and by Fisher's exact test otherwise.
tDifference is statistically significant, P=.O5.^Difference is in opposite direction from that hypothesized.
variables more common among those with silent strokewere not examined (ie, age greater than 65 years,hypertension, cigarette smoking). It must be empha-sized that none of the studies to date were designed todetect a relationship between dementia and silent in-farction. To establish such a relationship, a study mustinclude adequate numbers of patients with and withoutdementia and adequate numbers of patients with andwithout silent infarction.
Whether silent infarction is a marker for anatomicallysevere cerebrovascular disease has also not been estab-lished. The ACAS cohort is the largest studied prospec-tively with regard to carotid artery stenosis and silentinfarction. No evidence of an association between thedegree of stenosis and silent infarction was found. Inaddition, silent infarcts were just as frequent in thecerebral hemisphere contralateral to the ACAS carotidartery as they were in the ipsilateral hemisphere. None-theless, a potential bias against a relation of degree ofstenosis to silent infarction was present in that asymp-tomatic patients could have been excluded if they hadpreexisting neurological abnormalities ipsilateral to theACAS (ie, stenosed) artery. Perhaps more important,71% of the ACAS patients fell into two of eight stenosiscategories, and so sample sizes for comparison werevery small.
One could hypothesize that because 72% of theACAS silent infarcts were small and deep, combining allsilent infarcts regardless of size could dilute any possiblerelation of nonlacunar silent infarcts to degree of ste-nosis. However, when our analysis of silent infarction tostenosis was limited to those with the larger infarctions,no relation was detected. Norris and Zhu,30 on the otherhand, suggest an association between severe stenosisand silent infarction. In a cohort of 381 patients withouta history of stroke, 137 had a silent infarction seen byCT, and an increased frequency of silent infarction wasnoted in the severe stenosis group compared with themild and moderate stenosis groups (P<.001). The rela-
tion was not further explored with multivariate analysisto examine potential confounding variables such as sexand age. A future question to be addressed with thefinal ACAS results is whether the presence of severecarotid stenosis potentiates the likelihood of small,deep, lacunar-type cerebral infarcts judged clinically tobe caused by disease of small, penetrating arteries orarterioles. The baseline ACAS CT results do not di-rectly address the issue, but the small, deep infarctsidentified were not more frequent ipsilateral to themore severely stenotic carotid arteries.
TIAs are important markers for anatomic cerebrovas-cular disease and for the subsequent occurrence ofcerebral infarction. In our study as in others,3-7.293133
the occurrence of TIA has also been associated withsilent infarction by CT. Is identifying silent infarctionimportant in identifying patients at high risk for laterstroke? In other cohorts studied, the neurological out-come of patients with silent stroke has varied. In theNorth American Symptomatic Carotid EndarterectomyTrial (NASCET) cohort of 352 TIA patients with high-grade carotid stenosis,31 silent stroke was present in 121(34%). Silent stroke was an independent marker forincreased subsequent mortality and was an independentmarker for increased stroke occurrence in those ran-domized to the medical group. Evans and colleagues33
assessed 350 patients with TIAs and found that patientswith infarct identified by CT (17%) had significantlyshorter survival times. The Dutch TIA Trial StudyGroup34 also reported infarct identified by CT to be anindependent predictor of vascular death, stroke, ormyocardial infarction for patients with TIA. In patientswith acute stroke, those with silent stroke have not beenmore likely than those without to have a less favorableinitial outcome35 or to have an increased rate of recur-rent stroke.2628 In our cohort, we will eventually have5-year follow-up data on the frequency of subsequentTIA, stroke, and death.
by guest on July 9, 2018http://stroke.ahajournals.org/
Dow
nloaded from
1128 Stroke Vol 25, No 6 June 1994
Perhaps identifying silent infarction is important withregard to perioperative risk in patients undergoingcarotid endarterectomy. The surgical results in ACASand NASCET have yet to be analyzed in this regard.Results of other studies have been conflicting, withsome reports identifying an association of preoperativesilent stroke to perioperative neurological deficit,14 andother reports not identifying an association.I3-1518-36
Because the frequency of perioperative stroke in thesereports was low, the relation of silent infarction toperioperative stroke, even if present, may be impossibleto detect without a large, multicenter study (eg, ACAS).
We conclude that silent strokes are common inpatients with high-grade asymptomatic carotid stenosis,particularly men. Silent stroke may be more common inpatients with abnormalities in gait, deep tendon reflexesor planar responses, visual fields, funduscopic examina-tion, eye movements, or hearing. Nonetheless, the clin-ical significance of silent cerebral infarction is difficultto detect, perhaps in large part because of the small sizeof the lesions. The ACAS results indicate that a detailedneurological history or examination rarely misses clini-cally important ischemic brain lesions. However, assuggested, it remains to be seen whether silent infarc-tion identified by CT may be a marker for future stroke,either perioperatively or in the long term.
AcknowledgmentThis study was supported by National Institute of Neurolog-
ical Disorders and Stroke grant NS-22611-07.
Appendix. Participants in the ACAS Group asof October 1, 1993
The participating clinical centers (CT readers followed byclinic coordinators) and central units are as follows:
Arizona (University of), Tucson, Ariz: William Feinberg,MD; Joachim Seeger, MD; Denise Bruck; Brenda Void; JoanLaguna.
Arkansas (University of), Little Rock, Ark: MichaelChesser, MD; Lee Archer, MD; Jess R. Nickols, MD; ColetteMacDonald.
Barrow Neurological Institute, Phoenix, Ariz: John Hodak,MD; Richard Flom, MD; Sonna Hunsley; Heidi Jahnke.
Bowman Gray School of Medicine, Winston-Salem, NC:David Lefkowitz, MD; Jean Satterfield.
California, Los Angeles (University of), Los Angeles, Calif:Stanley Cohen, MD; Bruce Jacobs, MD; Richard Holgate,MD; Brad Joabour, MD; Kathy Walden; Candace Vescera.
California Pacific Medical Center, San Francisco, Calif:Robert Bernstein, MD; Pat Radosevich; Peggy McCormick;Linda Elias.
Cleveland Clinic, Cleveland, Ohio: Anthony Furlan, MD;Bernadine Bryerton.
Cincinnati (University of), Cincinnati, Ohio: Thomas Brott,MD; Thomas Tomsick, MD; Laura Sauerbeck; Chriss Blum.
Columbia University, New York, NY: J.P. Mohr, MD;George Petty, MD; Richard Libman, MD; Randolph Mar-shall, MD; Annette Cruz; Tina Gonzalez; Anilda Cabrera,MD.
Francis Scott Key Medical Center, Baltimore, Md: Con-stance Johnson, MD; Christopher Early, MD; Brenda Stone;Mairi Pat Maguire.
Harbin Clinic, Rome, Ga: Jay Schecter, MD; RaymondCapps, MD; Jeffrey Glass, MD; Nell Farrar.
Henry Ford Hospital, Detroit, Mich: Serish Patel, MD; JudyWilczewski; Wendy Robertson; Sheila Daley.
Hershey Medical Center, Hershey, Pa: Cindy Janesky, MD;Jon Meilstrup, MD; Diane Friedman; Florence Smith.
Hopital de L'Enfant Jesus, Quebec City, Canada: FernandBedard, MD; Charlotte Benguigui.
Iowa (University of), Iowa City, Iowa: Harold Adams, MD;Jose Biller, MD; Betsy Love, MD; Brigette Bendixen, MD;Lynn Vining; Dawn Karboski; Karla Grimsman.
Kentucky (University of), Lexington, Ky: Charles Lee, MD;Byron Young, MD; Creed Pettigrew, MD; Robert Dempsey,MD; Ruthie Sadler; Linda Rice; Louise Diana; Artie Norton.
Lehigh Valley Hospital, Allentown, Pa: Zwu-Shin Lin, MD;Joan Langenecker; Donna Jenny.
Loyola University, Maywood, 111: Michael Kelly, MD; SudhaGupta, MD; Katy Burke.
Marshfield Clinic, Marshfield, Wis: John Warner, MD;Sandy Lobner.
Medical College of Virginia, Richmond, Va: John Taylor,MD; Ann Cockrell; Chris Conway.
Mississippi (University of), Jackson, Miss: Robert Smith,MD; Robin Brown.
New England Medical Center, Boston, Mass: Louis Caplan,MD; Loretta Barron.
New Jersey (University of Medicine & Dentistry), Newark,NJ: Fred Weisbrot, MD; Stephen Kamin, MD; Tom Back;Carolyn Rogers.
New Mexico (University of), Albuquerque, NM: AskielBruno, MD; Edie Johnson; Susan Steel.
Northwestern University Medical School, Chicago, III: JoseBiller, MD; James Yao, MD; Linda Chadwick.
Ocshner Clinic, New Orleans, La: Richard Hughes, MD;Bruce Lepler, MD; Vicki Lang; Cheryl Benoit; Vicki Cahanin.
Oregon Health Sciences, Portland, Ore: Lloyd Taylor, MD;Bruce Coull, MD; Lucy Whitaker; Ron Dalman, MD.
Roanoke Neurological Center, Roanoke, Va: Don Bivins,MD; Candy Foley.
Rochester (University of), Rochester, NY: Richard Green,MD; Dahne Cohen, MD; Joanne McNamara.
St. John's Mercy Medical Center, St Louis, Mo: RichardLevine, MD; Joseph Hurley, MD; Mary Wilcox; ClaireBlackburn.
Singing River Hospital, Pascagoula, Miss: Roland Mestayer,MD; Cindy Almond.
University of Texas Southwestern Medical Center at Dallas(Tex): G. Patrick Clagett, MD; Hal Unwin, MD; WilsonBryan, MD; Chris Matkins.
Sunnybrook Hospital, Toronto, Ontario, Canada: PerryCooper, MD; David Rowed, MD; Beverley Bowyer.
Tennessee (University of) Memphis, Tenn: James Robert-son, MD; Ken Vasu, MD; J. Acker, MD; Angeleah Bradley;Judy Riley; Joan Connell; Mary Ann Giampapa; ConnieTaylor; Nan Stahl; Terrye Thomas; Susan Bennett.
University Hospital, London, Ontario, Canada: Allan Fox,MD; Cheryl Mayer; Carole White.
Victoria Hospital, London, Ontario, Canada: Leo Assis,MD; W. Pexman, MD; Leslie Paddock; Barb Tate.
Virginia Mason Clinic, Seattle, Wash: Robert Crane, MD;Sandy Harris; Kathy Butter-Levy.
Yale University School of Medicine, New Haven, Conn:Larry Brass, MD; Perre Fayad, MD; Bauer Sumpio, MD;Anne Lovejoy; Donna Kisiel.
Operations CenterDepartment of Neurology, Bowman Gray School of Medi-
cine, Wake Forest University, Winston-Salem, NC: James F.Toole, MD (Principal Investigator); Virginia J. Howard,MSPH; Suzanne Purvis; Dee Dee Vernon; Kelley Needham;Pam Beck; Marty Dozier; David Lefkowitz, MD; GeorgeHoward, DrPh; Karla Essick.
Statistical Coordinating CenterDepartment of Biostatistics, University of North Carolina at
Chapel Hill, Chapel Hill, NC: Lloyd E. Chambless, PhD
by guest on July 9, 2018http://stroke.ahajournals.org/
Dow
nloaded from
Brott et al Baseline Silent Cerebral Infarction in ACAS 1129
(Principal Investigator); J.J. Nelson, MSPH; Ernestine Bland;James Locklear.
References1. Bogousslavsky J, Regli F. Cerebral infarction with transient signs
(CITS): do TIAs correspond to small deep infarcts in internalcarotid artery occlusion? Stroke. 1984;15:536-539.
2. Perrone P, Candelise L, Scotti G, DeGrandi C, Scialfa G. CTevaluation in patients with transient ischemic attack: correlationbetween clinical and angiographic findings. Eur Neurol. 1979;18:217-221.
3. Calandre L, Gomara S, Bermejo F, Millan JM, del Pozo G. ClinicalCT correlations in TIA, RIND, and strokes with minimumresiduum. Stroke. 1984;15:663-666.
4. Nicolaides A, Kalodiki E, Ramaswami G, Geroulakos G, Stevens J.The significance of cerebral infarcts on CT scans in patients withtransient ischaemic attack. In: Bernstein EF, Callow AD, Nico-laides AN, Shifran EG, eds. Cerebral Revascularization. London,England: Med-Orion Publishing Co; 1993:159-178.
5. Koudstaal PJ, vanGijn J, Lodder J, Frenken WGM, Vermeulen M,Franke CL, Hijdra A, Bulens C, Dutch Transient Ischemic AttackStudy Group. Transient ischemic attacks with and without arelevant infarct on computed tomographic scans cannot be distin-guished clinically. Arch Neurol. 1991;48:916-920.
6. Murros KE, Evans GW, Toole JF, Howard G, Rose LA. Cerebralinfarction in patients with transient ischemic attacks. J Neurol.1989;236:182-184.
7. Mounier-Vehier F, Leys D, Rondepierre P, Godefroy O, Pruvo JP.Silent infarcts in patients with ischemic stroke are related to ageand size of the left atrium. Stroke. 1993;24:1347-1351.
8. Fujikawa T, Yamawaki S, Touhouda Y. Incidence of silent cerebralinfarction in patients with major depression. Stroke. 1993;24:1631-1634.
9. The Asymptomatic Carotid Atherosclerosis Study Group. Studydesign for randomized prospective trial of carotid endarterectomyfor asymptomatic atherosclerosis. Stroke. 1989;20:844-849.
10. Howard VS, Grizzle J, Diener HC, Hobson RW II, Mayberg MR,Toole JR. Comparison of multicenter study designs for investi-gation of carotid endarterectomy efficacy. Stroke. 1992;23:583-593.
11. Lefkowitz DS, Brust JC, Goldman L, Johnson JL, Toole JF,Howard V, Chambless L. A pilot study of the end point verificationsystem in the Asymptomatic Carotid Atherosclerosis Study.J Stroke Cerebrovasc Dis. 1992;2:92-99.
12. Damasio H. Vascular territories defined by computed tomography.In: Wood JH, ed. Cerebral Blood Flow. New York, NY:McGraw-Hill; 1987:324-332.
13. Sise MJ, Sedwitz MM, Rowley WR, Shackford SR. Prospectiveanalysis of carotid endarterectomy and silent cerebral infarction in97 patients. Stroke. 1989;20:329-332.
14. Graber JN, Vollman RW, Johnson WC, Levine H, Butler R, ScottRM, Nabseth DC. Stroke after carotid endarterectomy: risk aspredicted by preoperative computerized tomography. Am J Surg.1984;147:492-497.
15. Ricotta JJ, Ouriel K, Green RM, DeWeese JA. Use of comput-erized cerebral tomography in selection of patients for elective andurgent carotid endarterectomy. Ann Surg. 1985;202:783-787.
16. Street DL, O'Brien MS, Ricotta JJ, Ekholm SE, Ouriel K, GreenRM, DeWeese JA. Observations on cerebral computed tomographyin patients having carotid endarterectomy. J Vase Surg. 1988;7:798-801.
17. Berguer R, Sieggreen MY, Lazo A, Hodakowski GT. The silentbrain infarct in carotid surgery. J Vase Surg. 1986;3:442-447.
18. Martin JD, Valentine RJ, Myers SI, Rossi MB, Patterson CB,Clagett GP. Is routine CT scanning necessary in the preoperativeevaluation of patients undergoing carotid endarterectomy? J VaseSurg. 1991;14:267-270.
19. Tanaka H, Sueyoshi K, Nishino M, Ishida M, Fukunaga R, Abe H.Silent brain infarction and coronary artery disease in Japanesepatients. Arch Neurol. 1993;50:706-709.
20. Petersen P, Madsen EB, Brun B, Pedersen F, Glydensted C,Boysen G. Silent cerebral infarction in chronic atrial fibrillation.Stroke. 1987;18:1098-1100.
21. Petersen P, Pedersen F, Johnsen A, Madsen EB, Brun B, BoysenG, Gotfredsen J. Cerebral computed tomography in paroxysmalatrial fibrillation. Acta Neurol Scand. 1989;79:482-486.
22. Feinberg WM, Seeger JF, Carmody RF, Anderson DC, Hart RG,Pearce LA. Epidemiologic features of asymptomatic cerebralinfarction in patients with nonvalvular atrial fibrillation. ArchIntern Med. 1990;150:2340-2344.
23. Kempster PA, Gerraty RP, Gates PC. Asymptomatic cerebralinfarction in patients with chronic atrial fibrillation. Stroke. 1988;19:955-957.
24. Ezekowitz MD, Bridgers S, James K, Nazarian SM, Gornick CC,Shabetai R, Kurtzke J, VAMC West Haven, Conn. Subclinicalcerebral infarction in patients with chronic nonvalvular atrial fibril-lation. Circulation. 1989;80(supp II):II-404. Abstract.
25. Nicolaides AN, Papadakis K, Gngg M, Al-Kutoubi A, WilliamsMA, Deacon DFS. Data from CT scans: the significance of silentcerebral infarction and atrophy. In: Bernstein EF, ed. AmaurosisFugax. New York, NY: Springer-Verlag; 1988:200-226.
26. Ricci S, Grazia M, LaRosa F, Righetti E, Duca E, Caputo N. Silentbrain infarctions in patients with first-ever stroke: a community-basedstudy in Umbria, Italy. Stroke. 1993;24:647-651.
27. Kase CS, Wolf PA, Chodosh EH, Zacker HB, Kelly-Hayes M,Kannel WB, D'Agostino R, Scampini L. Prevalence of silent strokein patients presenting with initial stroke: the Framingham Study.Stroke. 1989;20:850-852.
28. Chodosh EH, Foulkes MA, Kase CS, Wolf PA, Mohr JP, Hier DB,Price TR, Furtado JG Jr. Silent stroke in the NINCDS Stroke DataBank. Neurology. 1988;38:1674-1679.
29. Herderschee D, Hijdra A, Algra A, Koudstaal PJ, Kappelle LJ, vanGijn J, the Dutch TIA Trial Study Group. Silent stroke in patientswith transient ischemic attack or minor ischemic stroke. Stroke.1992;23:1220-1224.
30. Norris JW, Zhu CZ. Silent stroke and carotid stenosis. Stroke.1992;23:483-485.
31. Streifler JY, Fox AJ, Wong CJ, Hachinski VC, Barnett HJM, forthe NASCET Group. Importance of "silent" brain infarctions inTIA patients with high-grade carotid stenosis: results fromNASCET. Neurology. 1992;42(suppl 3):204. Abstract.
32. Weisberg LA. Computerized tomographic abnormalities inpatients with hemispheric transient ischemic attacks. South Med J.1986;79:804-807.
33. Evans GW, Howard G, Murros KE, Rose LA, Toole JF. Cerebralinfarction verified by cranial computed tomography and prognosisfor survival following transient ischemic attack. Stroke. 1991;22:431-436.
34. The Dutch TIA Trial Study Group. Predictors of major vascularevents in patients with a transient ischemic attack or nondisablingstroke. Stroke. 1993;24:527-531.
35. Jorgensen HS, Nakayama H, Raaschou HO, Gam J, Olsen TS.Silent infarction in acute stroke patients. Prevalence, localization,risk factors, and clinical significance: the Copenhagen StrokeStudy. Stroke. 1994;25:97-104.
36. Habozit B. The silent brain infarct before and after carotidsurgery. Ann Vase Surg. 1990;4:485-489.
by guest on July 9, 2018http://stroke.ahajournals.org/
Dow
nloaded from

and C BlumT Brott, T Tomsick, W Feinberg, C Johnson, J Biller, J Broderick, M Kelly, J Frey, S Schwartz
Baseline silent cerebral infarction in the Asymptomatic Carotid Atherosclerosis Study.
Print ISSN: 0039-2499. Online ISSN: 1524-4628 Copyright © 1994 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Stroke doi: 10.1161/01.STR.25.6.1122
1994;25:1122-1129Stroke.
http://stroke.ahajournals.org/content/25/6/1122World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://stroke.ahajournals.org//subscriptions/
is online at: Stroke Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer available in the
Permissions in the middle column of the Web page under Services. Further information about this process isOnce the online version of the published article for which permission is being requested is located, click Request
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.Stroke Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on July 9, 2018http://stroke.ahajournals.org/
Dow
nloaded from


![Improved Speech Reconstruction from Silent Videosynthesis using predicted spectrogram magnitude, including Tacotron (Wang et al.) [43] for speech synthesis, and the baseline model](https://static.fdocuments.in/doc/165x107/5ea3ce25fda4e52d8c1de6a1/improved-speech-reconstruction-from-silent-synthesis-using-predicted-spectrogram.jpg)















