Base Metal Alloys
37
Base metal alloys Presented by Harsha vardhan k.v
-
Upload
harsha-reddy -
Category
Documents
-
view
232 -
download
3
description
base metal alloys in prosthodontics
Transcript of Base Metal Alloys
Base metal alloys
Base metal alloys
Presented byHarsha vardhan k.vDept of ProsthodonticsSVSIDS
ContentsIntroductionHistoryReview of literatureClassificationDesirable properties of base metalsComposition of base metalsImportant alloysCasting proceeduresGuidelines for Clinical selection of alloysConclusionReferences
Introduction
Base metal- a metal that readily oxidises or dissolves to release ionsAlloy- is a metal containing two (or ) more elements, at least one of which is a metal and all of which are mutually soluble in Molten State The twentieth century generated substantially new changes to dental AlloysThe major factors that are driving new developments are
Economy.Performance.Aesthetics.A brief description of the evolution base metal alloys is appropriate to understand the rationale for the development of such wide varieties.
History700BC Etuscans and Egyptians made gold wires
Fig-1 1907 The Lost-Wax technique was introduced by William H.Taggart It led to the casting of inlays, onlays, crowns, fixed partial dentures.
1933 Cobalt-Chromium Partial Denture Alloys
Base metal removable partial denture alloys were introduced in the1930s. Since that time both nickel-chromium and cobalt-chromium formulations have become increasingly popular compared with conventional type IV gold alloys which previously were the predominant metals used for such prostheses. The obvious advantages of the base metal alloys are their lighter weight greater stiffness(elastic modulus). By 1978 the price of gold was increasing so rapidly that attention was focused on the noble metal alloys to reduce the noble metal content yet retain the advantages of the noble metals for dental use.
1959 Porcelain-Fused-to-Metal ProcessIn the late 1950s, a breakthrough occurred in dental technology that was to influence significantly the fabrication of dental restorations. This was the successful veneering of a metal substructure with dental porcelain. Requirement was felt for dental alloys which could bond to porcelain and had high melting range. Until that time, dental porcelain had a markedly lower coefficient of thermal expansion than did gold alloys. This thermal mismatch often led to cracking of the porcelain which made it impossible to attain a bond between the two structural components. It was found that adding both platinum and palladium to gold lowered the coefficient of thermal expansion/contraction of the alloy sufficiently to ensure physical compatibility between the porcelain veneer and the meal substructure. Weinstein et al. demonstrated that both the fusion temperature of palladium-based and gold-based alloys and the thermal expansion of the porcelains could be modified to produce thermally compatible metal-ceramic prostheses. The melting range of metal-ceramic alloys must be sufficiently high to permit firing of the porcelain onto the gold-based alloys without deforming the metal substructure.
1971 Gold Standard In 1971 US withdrew the gold standard and Gold then became a commodity freely traded on the open markets. deregulation of gold prices ----the price of gold increased years. Hence in some alloys, gold was replaced with palladium. In other alloys, palladium eliminated gold entirely.This also lead to the progressive increase in the usage of non precious metals. The obvious advantages of the base metal alloys are their lighter weight greater stiffness(elastic modulus)Background on Cold WorkingThe temperature at which the deformation takes place is an important determinant of the final properties. If the temperature is relatively low with respect to the melting point of the material (less than 0.3 of the melting point), the deformation process is termed "cold working". A material that is plastically deformed at temperatures above 0.6 of the melting point is said to be hot worked. There are significant differences between the effects of cold and hot working on the properties and structure of materials.While cold-working a metal will tend to increase its strength, other properties such as ductility or corrosion resistance may be negatively affected. Therefore, to remove internal stresses of cold work, it is sometimes desirable to heat treat the metal after cold working. If this heat treatment, or annealing, is conducted at a sufficiently high temperature, a reduction of the stress necessary to further deform the material may be achieved as recrystallization occurs. This experiment introduces us to the relationship between cold work and recrystallization processes and their associated properties.During cold-working, it may take a considerable amount of energy to affect the change in size and shape. Some of the energy expended will appear in the form of heat. A considerable amount of the energy will also be stored in the material. This stored energy is associated with the defects created during the deformation. The free energy of the worked metal will be increased by approximately the amount represented by the stored energy. The most important result of cold working, which accompanies this increase in the number of defects, is strain hardening. Strain hardening is the increase in the yield stress of the metal after it has been deformed. This makes it more difficult to further deform the material. The increase in yield stress comes from the fact that deformation results in a higher density of dislocations. The strain fields around the dislocations most often repel one another, limiting dislocation movement.
REVIEW OF LITERATUREP.J Brockhurst and R.W.S Canon in 1981 examined the requirements of alloys for metal-ceramic crowns and bridgework and discussed the functional requirements and manipulative behavior as well as cost of alternatives to high gold alloys. They concluded that base metal alloys functioned satisfactorily as compared to high noble alloys provided proper dental lab procedures were employed. Nickel and beryllium did not appear to be health hazards for them.J. Robert Kelly and Thomas C.Rose in 1983 discussed the various physical properties, biocompatibility, porcelain bonding and corrosion resistance of various non precious alloys and concluded that though the manipulation of non precious alloys is technique sensitive and exacting, their better physical properties and clinical performance merited consideration. They were of the opinion that beryllium was not a health hazard provided proper exhaust and ventilation was used in the dental lab and that the allergenic potential of nickel needed further research.M. Bagby, S.J Marshall and G.W Marshall in 1990 reviewed the literature on metal ceramic bio compatibility. They discussed the various tests to predict thermo mechanical compatibility and also for measuring compatibility at the metal ceramic interface.Russel R. Wang and Aaron Fenton in 1996 reviewed the literature on Titanium for prosthodontic applications. They described the development and properties of titanium for the purpose of evaluating the present status and future trends in its use.Selcuk Oruc and Ybrahim Tulunoglu in 2000 evaluated the marginal and inner fit of metal ceramic restorations and frameworks made with a Nickel-Chromium alloy (Remanium CS) and a commercially pure Titanium (Rematitan). They concluded that the fit of base metal alloy metal ceramic crowns was better than the commercially pure Titanium metal ceramic crowns. However both the artificial crowns were clinically acceptable.John C. Wataha in 2002 discussed the properties that are relevant to proper selection of an alloy for a given clinical problem. He summarized the various alloys available till date and their classification and also provided simple guidelines to help dentists choose appropriate alloys for their practices .ClassificationIn 1984 ADA proposed simple classification for dental casting alloys. Three categories, are described; High Noble (HN) Noble (N) and Predominantly base metal ( PB). High Noble Metal (HN) -Contains 40 WT % Au, 60 WT % of the noble metal elements ( Au + Ir + Pt + Rh+Ru) Noble Metal (N)- Contains 25 WT% of noble metal elements Predominantly Base Metal (PB)-Contains 25WT% of Noble metal Elements.
The ADA has adopted symbols for each of these classes of alloys to aid the practitioner in knowing to which category a given alloy belongs
In 1927, the Bureau of standards established gold Casting alloy types I through 4 according to composition, Based on 1989 revision of specification No - 5 by the ADA, the four alloy types are classified by their physical properties & not by their compositions Type I - (Low strength) - small inlays, easily burnished & subject to very slight stress. The minimum yield strength(YS) is 80mpa and minimum percent elongation(PE) is 18%Type 2- (medium strength) castings subjected to moderate stress, including 3/4 crowns, abutments, pontics, & full crowns.YS-180mpa and PE-10%Type 3 -( high strength) - castings subjected to high stress, including onlays, copings, abutments, pontics, full crowns, & short span fpd's.YS-270mpa PE-5%Type 4- (extra high strength) - castings subjected to high stresses, including denture base bars & clasps, long span fpd's endodontic posts & cones, thin veneer crowns & rpds. YS 360mpa PE-3%
Classification of Alloys for all FULL Metal restorations, Metal - ceramic restoration and partial dentures:-
It divided all the availible metals into three major catagories.. Highnoble alloys Noble alloys and Predominantly base metal alloys
Metal type All metal prosthesis Metal ceramic prosthesis Partial denture frameworks
Highnoble alloysAu-Ag-PdAu-Ag-Pd-Cu Metal Ceramic AlloysPure AUAu- Pt-Pd(5-12%wt AG)Au-Pd-Ag(more than 12%) Au- Pd. ( No Ag) Au-Ag-Pd-Cu
Noble alloys Ag-Pd-Au-CuAg-PdMetal Ceramic alloys Pd- Au Pd-Au-AgPd-AgPd-Cu-ga Pd-Ga-Ag ------------------
Predominantly base metal Ti - Al - V Pure Ti Ni - Cr - Mo- Be Co-Cr-Mo Co-Cr-W Pure TiTi - Al - V Ni-Cr-Mo-Be Ni-Cr-Mo Co-Cr-Mo Co-Cr-WTi - Al - V Ni-Cr-Mo-Be Ni-Cr-Mo Co-Cr-Mo Co-Cr-W
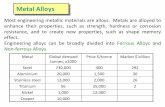
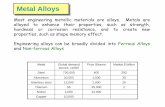
Emphasising on predominantly base metal alloys say that
J.C. Wataha, R.L. Messer / Dent Clin N Am 48 (2004) 499512 Alloy type Solidus-liquidus (C) Color Phasestructure Elasticmodulus(static, GPa Vickers hardness(kg/mm2) Yield strength(tension,0.2%, MPa)
Ni-Cr-Be 11601270 White Multiple 192 350 325
Ni-Cr 13301390 White Multiple 159 350 310
Ni-high-Cr 12501310 White Multiple 205 205 180
Co-Cr 12151300 White Multiple 155 155 390
The first three groups are closely related in composition and many physical properties but are fundamentally different in their corrosion properties. These alloys may be manufactured with or without trace amounts (0.1 wt %) of carbon. When used for cast restorations, these alloys generally do not contain carbon. However, when used for partial denture frameworks carbon is generally added carbon is a potent enhancer of yield strength and hardness (but not modulus) Metal An element whose atomic structure readily loses electrons to form positively charged ions, and which exhibits metallic bonding (through a spatial extension of valence electrons), opacity, good light reflectance from a polished surface and high electrical and thermal conductivity.Grain A microscopic single crystal in the microstructure of a metallic materialWhen a molten alloy cools to the solid state, crystals form around tiny nuclei. As the temperature drops, these crystals grow until the crystal boundaries meet each other in the solid state. At this point each crystals called a grain and the boundaries between crystal are grain boundaries. Small grains have been found to improve the elongation and tensile strength of cast gold alloys. In general a grain size of 30 micron or less has been reported to be desirable in dental alloys. Grain size vary from10 to 1000micron. Under normal conditions, the grain structure ofalloys is not visible and special acid etching and magnification are generally necessary to view grains.Phase structureAlloys can either be single phase or multiple phase. Single phase alloys have essentially the same composition throughout whereas multiple phase alloys have areas of composition that differ by microstructural location. Whether an alloy is single or multiple phase is dependent on the solubility of the alloy elements. If all elements are completely mutually soluble in solid state (eg Au, Pd, Cu) then the alloy will be single phase. If some elements are not soluble in one another (eg Au Pt) then alloy may be multiple phase. Phase structure affects the corrosion, strength and etching characteristics of alloys. In general multiple phase alloys are prone to higher corrosion rates than single phase alloys because of galvanic effects between the microscopic areas of different compositions
Desirable properties Biocompatibility.The material must tolerate oral fluids and not release am harmful products into the oral environmentBeryllium ---potentially toxic---hazardousNickel---allergenic potentialAn Investigation of the Cytotoxic Effects of Dental Casting Alloys Ahmad S. Al-Hiyasat et.al Int J Prosthodont 2003;16:812 Material and method Ten specimen of each high-noble alloy (Bioherador N) andsix commercially available base-metal alloys, includingfour Ni-Cr alloys (Remanium CS,Heranium NA, Wiron 99, CB Soft),one Co-Cr alloy (Wirobond C), and one Cu-based alloy (Thermobond) placed in 24-well tissue culture plates togetherwith a suspension containing Balb/C 3T3 fibroblasts (5 105 cells/mL). After 3 days of incubation at 37C, cell viability was determined Conclusion of the studyThe cytotoxicity of casting alloys tested in this study was markedly affected by their composition. Differences were found in the cytotoxicity of alloys classified within the same category. The presence of Cu in the composition of the alloy adversely affected cell viability. Corrosion Resistance.Corrosion is the physical dissolution of a material in an environment. Corrosion resistance is derived from the material components being either too noble to react in the oral environment (e.g., gold and palladium) or by the ability of one or more of the metallic elements to form an adherent passivating surface film, which inhibits any subsurface reaction (e.g., chromium in Ni-Cr and Co-Cr alloys and titanium in commercially pure titanium [CP Ti) and in Ti-6AI-4V alloy). Tarnish Resistance.Tarnish is a thin film of a surface deposit or an interaction layer that is adherent to the metal surface. These films are generally found on gold alloys with relatively high silver content or on silver alloysMetals are generally more susceptible to such attacks because of electrochemical reactions.Corrosion resistance is derived either by the component being too noble to react in the oral environment(E.g.: gold, palladium) or by its ability to form an adherent passivating surface film which inhibits any subsurface reactions( E.g.: Co-Cr, Ni-Cr and Co-Cr alloys and Ti alloys in CP Ti and in Ti-6Al-4V alloys). Allergenic Components in Casting Alloys.The concern for allergicreactions to dental materials gained momentum in the 1980s. AlthoughPresence of chromium --corrosion resistance some broad-based claims have been unsubstantiated, the subject is important from materials science and legal standpoints. Obviously, a restorative material should not cause adverse health consequences to a patient. Toxic materials are eliminated by regulation and sound business practices. Allergic reactions, however, are peculiar to the individual patient, and the practicing dentist has an obligation, morally and legally, to minimize this risk. The patient's "right-to-know" extends to having some knowledge of what is being placed into their bodies. Laws in some states are explicit in this respect. It is wise for the dentist to maintain a record of the material used for each restoration or prosthesis, as well as an understanding of any known allergies stated by the patientBe` concerntration for dental alloys rarely exceeds 2% by weightHowever Studies have shown that the parameter to evaluate its toxicity is the atomic concerntration rather than weight %Acc. To OSHA(occupational health and safety administration) exposure to `Be` should be limited to 2g/cu.mm and that of Ni is 15g/cu.mmMOFFA et.al 1973 advocated the use of proper exhaust and ventilation Aesthetics.Considerable controversy exists over the optimal balance among the properties of aesthetics, fit, abrasive potential, clinical survivability, and cost of cast metal prostheses compared with direct-filling restorations, ceramic-based prostheses (all-ceramic and metal-ceramic), and resin-veneered prostheses Considerable controversy exists over esthetics with regards to base metal alloys Studies showed that base metal alloys form dark oxide layer which is un esthetic Also cause blue or gray discoloration of subgingiva unlike noble metals Thermal Properties.For metal-ceramic restorations, the alloys or metals must have closely matching thermal expansion to be compatible with a given porcelain, and they must tolerate high processing temperatures Compensation for Solidification. To achieve accurately fitting cast inlays, onlays, crowns and more complex frameworks of prostheses, compensation for casting shrinkage from the solidus temperature to room temperature must be achieved either through computer-generated oversized dies or through controlled mold expansion. In addition, the fit of a cemented prosthesis must be tailored to accommodate the layersofbonding adhesive (if used) and the luting cement High melting range-high shrinkage Casting shrinkage= thermal shrinkage + solidification shrinkage Compensation for casting shrinkage must be achieved by oversized dies or through controlled mold expansion. CASTABILITY: To achieve accurate details in a cast framework or prosthesis, the molten metal must be able to wet the investment mold material very well (demonstrated by a sufficiently low contact angle) and flow into the most intricate regions of the mold without any appreciable interaction with the investment and without forming porosity within the surface or subsurface regions. The castability ofsome base metals is extremely challenging in this regard, because these alloys tend to readily form oxides or interact chemically with the mold wall during the casting process. In addition, these cast alloys tend to be more difficult to separate from the casting investment after cooling to room temperatureThe molten metal must be able to wet the investment mold material very well (decreased contact angle) and flow into the most intricate regions of the mold without any appreciable interaction with the investment and without forming porosity.. WHITLOCK et.al1985 measured % castability values of 14 metal ceramic alloys Of which
4Ni-Cr-Be7Ni based alloys without Be3gold basedResults werewith Be was 43-92%Without Be was 10-67% Finishing of Cast Metal.Cutting, grinding, finishing, and polishing of some metals is quite demanding, and extra time is required to produce a satisfactory surface finish. Hardness, ductility (percent elongation),and ultimate strength are important properties in this regard. The hardness of an alloy is a good primary indicator of cutting and grinding difficulty, and this property varies widely among the current casting metals. For example, Co-Cr and Ni-Cr alloys are quite hard compared with other metals, as seen in the following listing of Vickers hardness numbers: Co-Cr, 450 to 650; Ni-Cr, 330 to 400; Ti-6A1-4V, 320; tooth enamel, 300 to 400; Porcelain Bonding.To achieve a sound chemical bond to ceramic veneering materials, a substrate metal must be able to form a thin, adherent oxide, preferably one that is light in color so that it does not interfere with the aesthetic potential of the ceramic. The metal must have a thermal expansion/contraction coefficient that is closely matched to that of the porcelain. Stresses that develop in the ceramic adjacent to the metal/ceramic interface can enhance the fracture resistance of a metal-ceramic prosthesis (if the stresses are predominantly compressive in nature), or they can increase the susceptibility to crack formation (if they are predominantly tensile in nature Economic Considerations.The cost of metals used for single-unit prostheses or as frameworks for fixed or removable partial dentures is a function of the metal density and the cost per unit mass. For example, compared with a palladium alloy having a density of 11g/cm3, a gold alloy with a density of 18 g/cm3 will cost 164% (18/11 x100) more for the same volume and unit cost of metal.Composition of base metalsCHROMIUM: Chromium content is responsible for the tarnish resistance and stainless properties of these alloys. When the chromium of an alloy is over 29% the alloy is more difficult to cast becauseIt forms a brittle phase known as the sigma phase. Passivation12% of chromiumCOBALT AND NICKEL: They are some what interchangeable to a certain extent. Cobalt increases the elastic modulus, strength and hardness of the alloy more than nickel does. Nickel may increase ductility. CARBON CONTENT; The hardness of cobalt based alloys is increased by the increased content of carbon. Reduces ductility A change in the carbon content in the order of 0.2 % in these alloys changes their properties to such an extent that the alloy would no longer be usable in dentistryMOLYBDENUM: The presence of 3-6% molybdenum contributes to the strength of the alloy. decreases the thermal expansion coefficient ALUMINIUM:Al in Ni containing alloys forms a compound of Nickel and Aluminium (Ni3-Al).This compound increases the ultimate tensile and yield strength.BERYLLIUM: 1 % of this element to Nickel based alloys reduces the fusion range of the alloy by about 100 degree Celsius. It also aids in solid solution hardening. It improves the casting characteristics which possibly aid in porcelain bondingSILICON AND MANGANESE: These are added to increase the castability of base metal alloys. They primarily prevent oxidation of other elements during melting. When the nitrogen content of the final alloy is more than 0.1 % the castings loose some of their ductilityNICKEL-CHROMIUM ALLOYS Most Ni - Cr alloys for crowns & FPDs contains 61 - 81% Ni, 11 - 27 % Cr and 2- 5% Mo. By 1981, the percentage of laboratories using these base metal alloys increased to 70%, because of the unstable price of noble metals during this period. The Ni-Cr-Be alloys have retained their popularity despite the potential toxicity of beryllium and the allergenic potentialofnickel. In some regional areas, an increase in the use of palladium alloys has been observed.This section has been prepared to provide a critical assessment of the risks and benefits of base metal alloys when compared with gold-based or palladium based alloys for metal-ceramic prostheses. One might inquire why the Ni-Cr and Ni-Cr-Be alloys retain their popularity despite the known toxicity of beryllium as well as the allergenic potential ofnickel, are examples of potential nickel allergies on the hand of an individual who has had frequent exposure to nickel metal.There are several reasons for the use of nickel-chromium alloys in dentistry. Nickel is combined with chromium to form a highly corrosion resistant alloy.2. Ni-Cr alloys became popular in the early 1980s as low cost metals ($2 to $3 per conventional avoirdupois ounce) when the price ofgold rose to more than $500 per troy ounce. Because metal-ceramic restorations made with Ni-Cr-Be alloys have exhibited high success rates from the mid-1980s to the present, many dentists have continued to use these alloys.3. Alloys such as Ticonium 100 have been used in removable partial denture frameworks for many years with few reports of allergic reactions. However, it is believed that palatal epithelium may be more resistant to allergic reactions (contact dermatitis) than gingival sulcular epithelium.4. The Ni-Cr and Ni-Cr-Be alloys are relatively inexpensive compared with high noble or noble alloys. The priceofnickel-based alloys is stable, unlike the price of palladium-based alloys.5. Although beryllium is a toxic metal, dentists and patients should not be affected because the main risk occurs primarily in the vapor form, which is a concern for technicians who melt and cast large quantities of Ni-Cr-Be alloys without adequate ventilation or fume hoods in the melting area.6. Nickel alloys have excellent mechanical properties, such as high elastic modulus (stiffness), high hardness, and a reasonably high elongation (ductility).Since the development of cobalt-chromium alloys for cast dental appliances in 1928 and the subsequent introduction of nickel-chromium and nickel-cobalt-chromium alloys in later years, base metal alloys have demonstrated widespread acceptance in the United States as the predominant choice for the fabrication of removable partial denture frame works. Compared with Type IV gold alloys, cobalt-based alloys and nickel-based alloys feature lower cost, lower density, higher modulus of elasticity, higher hardness, and comparable clinical resistance to tarnish and corrosion. However, a comparison between nickel-based alloys and noble metal alloys designed for metal-ceramic crowns and fixed partial dentures (FPD) is more complex. Relatively small compositional differences or certain base metal additions such as beryllium, silicon, boron, and aluminum produce significant changes in base metal alloy microstructures and properties, which could affect the bond strength of ceramics to the metal oxide layer that is required to achieve chemical bonding.The majority of nickel-chromium alloys for crowns and FPD prostheses contain 61 wt% to 81 wt% nickel, 11 wt% to 27 wt% chromium and 2wt% to 4 wt% molybdenum. These alloys may also contain one or more of the following elements: aluminum, beryllium, boron, carbon, cobalt, copper, cerium, gallium, iron, manganese, niobium, silicon, tin, titanium, and zirconium. The cobalt-chromium alloys typically contain53 wt% to 67 wt% cobalt, 25 wt% to 32 wt% chromium, and 2 wt% to 6wt% molybdenum, which could affect the metal-ceramic bond strengthVitallium(Co-Cr-Mo)1939 Dr.Strock placed vitallium screws into human bone and called them `venable screws`As it resulted in formation of bone around metallic implantThough they failed There are several reasons for the use of nickel chromium and/or cobalt chromium alloys in dentistry These alloys are highly corrosion resistant as they are combined with Chromium Cost effectiveness Alloys such as Ticonium 100(Ni-Cr) have been used in removable partial denture frameworks for many years with few reports of allergic reactions. these alloys have excellent mechanical properties such as high elastic modulus, high hardness, high sag resistance and a reasonably high elongation (ductility)Lower density Because of higher modulus ,in metal ceramic prosthesis it is considered that a coping thickness can be reduced to 0.1mm and also the thickness of connector to as much as half butJones et.al connector thickness should not be reduced morethan 16% and reduction of coping thickness should not be done to 0.1mm Contrary to jones findings, finite element analysis studies proved that 0.1mm thick coping is acceptible and has slight effect On the other hand it is also important the realize the limitations of these alloys, These alloys are more difficult to cast and presolder The ability to obtain acceptable fitting castings may require special procedures to adequately compensate for the higher solidification shrinkage Potential for porcelain delamination as a result of separation of poorly adherent oxide layerfrom the metal substrate. Finishing and polishing require special procedures and is not easy either in the lab or at chair side. Removal of defective restorations may take time. Repair of crowns with fractured porcelain veneers which may be simply performed on noble metal substrates using pin-retained facings or metal ceramic onlays, is more difficult to accomplish in base metal frameworks.Few other important base metal alloys are 18-8 austinite form of stainless steel 18%cr and 8%ni orthodontic wires Elgiloy Co-Cr-Ni titanium/ TMA- titanium-molybdenum-aluminium Nitinol (nickel titanium Naval Ordnance Laborator) developed by Buehler This alloy system exhibits shape memory effect (SME) and super-elasticity, giving it a unusual set of mechanical properties
Titanium and Titanium AlloysThe use of commercially pure titanium (CP Ti) and titanium alloys increased significantly over the last two decades of the twentieth century. These metals can be used for all-metal and metal-ceramic prostheses, as well as for implants and removable partial denture frame works. Titanium is considered the most biocompatible metal used for dental prostheses. Because of the unique properties oftitanium, and especially its biocompatibility, it does not fall within the classification of base metals. It is worthy of a separate class of metals. According to the American Society for Testing and Materials(ASTM), there are five unalloyed grades of CP Ti (Grades 1-4, and Grade 7), based on the concentration of oxygen (0.18 wt% to 0.40 wt%) and iron (0.2 wt% to 0.5 wt%). Other impurities include nitrogen (0.03 wt% to 0.05 wt%), carbon (0.1 wt%), and hydrogen (0.015 wt%).Grade 1 CP Ti is the purest and softest form. It has a moderately high tensile strength (Grade 1 CP Ti, 240 MPa; Grade 4 CP Ti, 515 MPa),moderately high stiffness (elastic modulus, 117 GPa), low density(4.51 g/cm3), and low thermal expansion coefficient (9.4 x10-6/C).The elastic modulus of CP Ti is comparable to that of tooth enamel and noble alloys, but it is lower than that of other base metals. CP Tiis very resistant to tarnish and corrosion. The corrosion protection is derived from a thin (10 nm) passivating oxide film that forms spontaneously. However, because the oxidation rate of titanium increases markedly above 900 C, it is desirable to use ultralow-fusing porcelains (sintering temperature less than 850 C) for titanium-ceramic prostheses. A porcelain sintering temperature below 800 C is desirable to minimize oxidation and to avoid the conversion of alpha phase to the higher-temperature beta phase discussed in the following.Titanium has a high melting point (1668 C), and a special casting machine with arc-melting capability and an argon atmosphere is typically used, along with a compatible casting investment, to ensure acceptable capability. Because of reaction with the investment, a very hard so-called case having a thickness of approximately 150mforms at the surface of cast dental titanium alloys.For cast CP Ti, the HV increases from a bulk value of nearly 200 to approximately 650 at a depth of 25m below the surface, and special tools are required in the dental laboratory for finishing and adjusting CP Ti castings. Because of the presence of thecase, special surface modifications of cast titanium, using caustic NaOH based solutions or silicon nitride coatings, have been employed to improve the bond between cast CP Ti and dental porcelain.Titanium has the highest melting temperature of all metals used for metal ceramic prostheses and is highly resistant to sag deformation of metal frameworks at porcelain sintering temperatures.This high melting point is accompanied by a relatively low thermal expansion coefficient, and special low-expansion dental porcelains are necessary for bonding to titanium. Commercially pure titanium undergoes an allotropic transformation from a hexagonal close-packed crystal structure (phase) at 885 Cto a body-centered crystal structure (phase). Four possible types oftitanium alloys can be produced:, near-,, and. A alloywill form no phase on cooling. A near- phase alloy will formlimited phase on cooling. An - alloy will contain phase at room temperature and may contain retained phase and/or transformed phase. A alloy will retain the (3 phase on cooling, and it can precipitate other phases as well during heat treatment. Vanadium, which has a bcc structure, is one of the alloying elements that is isomorphous with the phase and is a phase stabilizer, that is, causing the transformation from phase to phase to occur at lower temperatures on cooling. Aluminum, which is an a phase stabilizer (i.e., causing the transformation of a phase to phase to occur at a higher temperature on heating), is included in a and near- alloys. Aluminum, tin, and zirconium are soluble in both the and phases. The most widely used titanium alloy in dentistry and for general commercial applications is Ti-6Al-4V, which is an- alloy. Although this alloy has greater strength than CP Ti, it is not as attractive from a biocompatibility point of view because of some concerns about health hazards from the slow release of aluminum and vanadium atoms in vivo Dr. Wilhelm kroll 1936 invented useful metallurgical processes for the commercial production of titanium metal and hence he is called the father of titanium industry. In early researches Bothe and Leventhal found that the response of bone to titanium was better than that of the previous alloys of Vitallium Branemark took this concept further and found that titanium implanted to the upper and lower jaws of dogs could withstand several years of loading without any change in stability, and without the tissue reactions shown to other materials at that time. His concept of intra-osseous implantation, where the bone was in a functional structural connection with a load-bearing implant, was later termed osseointegration. Since that time, the use of titanium and its alloys is increasing in many dental applications A special casting machine with arc melting capability and argon atmosphere is used along with a compatible investment are used to ensure acceptable castability. A pressure vacuum casting system with separate chamberAL2O3 MgO based investments are used
Guidelines for Clinical selection of alloys Considering oral health of patient and long term success, selection of casting alloys should be made primarily by the practitioner with consultation from the dental laboratory Customised approachmedical considerations like hypersensitivity to metals The physical requirements of the alloy --highest modulus of elasticity and less shrinkage is advisable The tensile strength is important if the restoration involves connectors between multiple units Color
Conclusion: - Choosing an alloy for prosthodontics applications is a formidable task. Selecting an alloy based on its color should be avoided unless all other factors are equal. One should know the complete composition of alloy and avoid elements to which patient is allergic. Single phase alloys should be preferred over multiphased. One should try to keep a track of alloys used in the patient. Alloys should be chosen from companies which research and manufacture their own alloys. These companies will be able to provide the most accurate information, the best service and best answers when the problems arise. Alloys which have been tested to elemental release and corrosion and have lowest possible release of elements should be used. Focus should be on long term clinical performance and long term costs ofrestorations. Clinical situations like esthetics, occlusion, space, allergy etc should be considered while selecting an alloy. Finally one should remember that clinician is ultimately responsible for the safety and efficacy of any restoration. Hence Selection of alloy should not be left to the lab, but should be meticulously selected according to the case in consultation with the lab.
References Anusavice-science of dental materials craigs restorative dental materials-12th edition Wataha JC. Alloys for prosthodontic restorations. J Prosthet Dent 2002;87:35183. Base Metal Alloys Used for Dental Restorations and Implants Michael Roach, MS Dent Clin N Am 51 (2007) 603627Casting alloys John C. Wataha, DMD, PhD*, Regina L. Messer, PhD Dent Clin N Am 48 (2004) 499512 The effects of recasting on the cytotoxicity of base metal alloys Ahmad S. Al-Hiyasat, BDS, MScD, PhD,a and Homa Darmani, BSc, PhDb(J Prosthet Dent 2005;93:158-63.)