Barriers to managing chronic illness among urban households in coastal Kenya
20
BARRIERS TO MANAGING CHRONIC ILLNESS AMONG URBAN HOUSEHOLDS IN COASTAL KENYA y THOMAS PORTER 1 * , JANE CHUMA 2 and CATHERINE MOLYNEUX 2,3 1 Oxford Deanery Public Health, Oxford, UK 2 Kenya Medical Research Institute (KEMRI) Wellcome Trust Research Programme, Kilifi, Kenya 3 University of Oxford, Oxford, UK Abstract: The burden of chronic illnesses is rising throughout the world but information on barriers to managing such diseases in developing countries is scarce. Qualitative data from focus group discussions and interview transcripts from a longitudinal study involving 22 households in urban, coastal Kenya were analysed. Themes around barriers to chronic illness care were identified and a conceptual framework developed which described relation- ships between these themes. The main barrier to chronic illness management was the cost of care. Other barriers identified were patient knowledge and beliefs, stigma, quality and trust in providers and long care pathways. Household resilience was adversely affected by chronic illness, further reducing households’ ability to cope with illness. Policy options to address the barriers identified are discussed. Copyright # 2009 John Wiley & Sons, Ltd. Keywords: chronic illness; barriers; coping strategies; household; Kenya; policy; healthcare 1 INTRODUCTION The burden of chronic illnesses is rising in developing countries (Strong et al., 2005). Although there is a paucity of epidemiological data for sub-Saharan Africa (Mufunda et al., 2006), estimates for non-communicable diseases (NCDs) may be used as a proxy for Journal of International Development J. Int. Dev. 21, 271–290 (2009) Published online 4 February 2009 in Wiley InterScience (www.interscience.wiley.com) DOI: 10.1002/jid.1552 *Correspondence to: Dr Thomas Porter, Specialist Registrar in Public Health, Oxford Deanery Public Health, Richards Building, Old Road Campus, Oxford, OX3 7LG, United Kingdom. E-mail: [email protected] y This paper is published with the permission of the Director of KEMRI. Thomas Porter carried out the qualitative and quantitative analyses presented in this paper, and wrote the paper draft. Catherine Molyneux and Jane Chuma conducted the original ATP study. Catherine Molyneux gave comments and corrections on the draft. Thomas Porter received a salary from the Oxford Deanery Public Health programme, with travel and accomodation costs for the study paid for by a stipend from the University of Oxford Global Health Science MSc programme. The original study was funded through a Fellowship awarded to Catherine Molyneux by the Wellcome Trust, UK and supported by the Kenya Medical Research Institute. The authors have no declared competing interests. Copyright # 2009 John Wiley & Sons, Ltd.
-
Upload
thomas-porter -
Category
Documents
-
view
212 -
download
0
Transcript of Barriers to managing chronic illness among urban households in coastal Kenya

Journal of International Development
J. Int. Dev. 21, 271–290 (2009)
Published online 4 February 2009 in Wiley InterScience
(www.interscience.wiley.com) DOI: 10.1002/jid.1552
BARRIERS TO MANAGING CHRONICILLNESS AMONG URBAN HOUSEHOLDS
IN COASTAL KENYAy
THOMAS PORTER1*, JANE CHUMA2 and CATHERINE MOLYNEUX2,3
1Oxford Deanery Public Health, Oxford, UK2Kenya Medical Research Institute (KEMRI) Wellcome Trust Research Programme, Kilifi, Kenya
3University of Oxford, Oxford, UK
Abstract: The burden of chronic illnesses is rising throughout the world but information on
barriers to managing such diseases in developing countries is scarce. Qualitative data from
focus group discussions and interview transcripts from a longitudinal study involving
22 households in urban, coastal Kenya were analysed. Themes around barriers to chronic
illness care were identified and a conceptual framework developed which described relation-
ships between these themes. The main barrier to chronic illness management was the cost of
care. Other barriers identified were patient knowledge and beliefs, stigma, quality and trust in
providers and long care pathways. Household resilience was adversely affected by chronic
illness, further reducing households’ ability to cope with illness. Policy options to address the
barriers identified are discussed. Copyright # 2009 John Wiley & Sons, Ltd.
Keywords: chronic illness; barriers; coping strategies; household; Kenya; policy; healthcare
1 INTRODUCTION
The burden of chronic illnesses is rising in developing countries (Strong et al., 2005).
Although there is a paucity of epidemiological data for sub-Saharan Africa (Mufunda et al.,
2006), estimates for non-communicable diseases (NCDs) may be used as a proxy for
*Correspondence to: Dr Thomas Porter, Specialist Registrar in Public Health, Oxford Deanery Public Health,Richards Building, Old Road Campus, Oxford, OX3 7LG, United Kingdom. E-mail: [email protected] paper is published with the permission of the Director of KEMRI. Thomas Porter carried out the qualitativeand quantitative analyses presented in this paper, and wrote the paper draft. Catherine Molyneux and Jane Chumaconducted the original ATP study. Catherine Molyneux gave comments and corrections on the draft. ThomasPorter received a salary from the Oxford Deanery Public Health programme, with travel and accomodation costsfor the study paid for by a stipend from the University of Oxford Global Health Science MSc programme. Theoriginal study was funded through a Fellowship awarded to Catherine Molyneux by the Wellcome Trust, UK andsupported by the Kenya Medical Research Institute. The authors have no declared competing interests.
Copyright # 2009 John Wiley & Sons, Ltd.

272 T. Porter et al.
chronic illness, although this is not without problems (the NCD definition includes acute
illnesses such as appendicitis and excludes chronic illness due to infection, such as
tuberculosis and HIV). In 2002 NCDs were estimated to account for 18 per cent of total
disability-adjusted life years (DALYs) in the region and by 2020 this is projected to have
nearly doubled to 32 per cent (Murray and Lopez, 1997; WHO, 2002a). In Kenya NCDs
accounted for 20 per cent of total DALYs in 2002 (WHO, 2002b). In addition to the
suffering associated with chronic illness, the financial burden is high (Su et al., 2006;
WHO, 2005).
The rising incidence and prevalence of chronic illnesses is partly due to population
expansion and ageing but is also the consequence of increasing prevalence of risk factors
and behaviours for long-term illnesses, such as urbanisation (Harpham and Stephens, 1991;
Wang et al., 2005). Other factors are likely to become increasingly prominent, such as the
use of therapies with the potential to delay mortality in some illnesses (e.g. antiretroviral
therapy in HIV).
The majority of health systems in developing countries were designed to manage acute,
especially infectious, illnesses (Wagner et al., 1996; WHO, 2002c), with little literature on
managing chronic illness in resource-poor settings (Unwin et al., 2001; El Ansari, 2006).
The Chronic Care Model (CCM) suggested that optimal chronic disease management
would result from success in six areas: community resources and policies; healthcare
organisations; self-management support (assisting patients and families to manage their
illnesses day-to-day); delivery system design; decision support; and clinical information
systems (Wagner, 1998; Bodenheimer et al., 2002). Whilst the CCM has generally been
successful where implemented (Tsai et al., 2005; Adams et al., 2007), its reliance on
information systems and motivated patients able to access care, makes it primarily suited
to developed countries. In 2002 the World Health Organisation published the innovative
care for chronic conditions (ICCC) framework, partly based on the CCM, which
recognised broader determinants including local community involvement and national
leadership and policies, making it more suitable for use in developing countries (WHO,
2002c).
There are few data available on the barriers to chronic illness management at the
household level in resource-poor settings, with most papers focusing on supply-side (i.e.
healthcare organisation) issues (e.g. Birbeck, 2000; Furber et al., 2004). The household
unit is important because it is at this level that most costs are ultimately borne and decisions
about treatment-seeking made (Berman et al., 1994). Poor management of long-term
illnesses, in comparison with that of acute illnesses, has a greater potential for prolonged
and ongoing impact on families’ livelihoods; a clearer understanding of the barriers to
management would enable the development of targeted interventions to improve chronic
illness management in these settings.
This paper presents data from a larger study which investigated household illness-related
treatment-seeking behaviour, costs, coping mechanisms and impoverishment (Chuma
et al., 2006, 2007; Molyneux et al., 2007, and papers in this issue by Chuma et al., and
Molyneux et al.). The aims of the current analysis were to describe household management
of chronic illnesses in urban Kenya and barriers to successful management. At the
household level, these were generally barriers to accessing care, and to self-management
by the patient. A comparison of the results with the existing literature in this field is
presented, along with their applicability to other settings. Relevant proposals in a recent
strategy document by the Government of Kenya, the National Health Sector Strategic Plan
(NHSSP), are reviewed in light of the present findings.
Copyright # 2009 John Wiley & Sons, Ltd. J. Int. Dev. 21, 271–290 (2009)
DOI: 10.1002/jid

Barriers to Managing Chronic Illness in Kenya 273
2 METHODS
2.1 Study Setting and Design
The original study was carried out in 2003/2004 in Kilifi District, the second poorest
district in Kenya, to investigate households’ ability to pay (ATP) for healthcare in both
urban and rural environments, initially focusing on costs for malaria treatment. It included
two large cross-sectional surveys of 870 adults; focus group discussions (FGDs); health
provider interviews; and an in-depth longitudinal study involving over 60 households. The
study was approved by local, national and international research ethics committees
(Chuma et al., 2007).
As part of the ATP study, a longitudinal study of 31 households, and 12 FGDs, took place
in the urban setting of Mtwapa. Mtwapa is a rapidly expanding town on the Kenyan coast,
10 km north of Mombasa, with a population of �70 000. The town is served by three
government hospitals, two government health centres, and one government dispensary.
There are also numerous private pharmacies, clinics and hospitals, as well as small general
shops selling basic medication. Although the area is considered urban, in practice some
neighbourhoods are more characteristic of rural settlements.
Households were selected for the case study through the cross-sectional survey, based
on their socioeconomic status (SES, derived from monthly per capita expenditure and
asset ownership), and average monthly health expenditure. Households were
categorised into low, medium and high SES; and low, medium and high health
expenditure. Four groups were eligible for the case study (low SES/low costs; low SES/
high costs; high SES/low costs and high SES/high costs), on the basis that these
households would contribute most to emerging theories in the original study. This list
was further refined based on fieldworkers’ estimation of which households would be
most likely to co-operate with the long-term study and complete follow up. The presence
or absence of chronic illness in the household was not used in selection. Case study
households were visited on at least five occasions by the same trained local fieldworker,
with specific topics explored at each visit (historical timeline; family tree and assets;
social resources; expenditure diaries; changes over follow-up period). Where
households had reported a chronic illness this was also discussed in detail. Consent
was sought for each household visit, with participants free to leave the study at any
point. 29 of the 31 households completed follow-up; no reason was given by the two
which withdrew consent during the study. Illness diagnoses were checked by the
fieldworker with patient-held health records when available. Detailed monthly
household expenditure data were noted by hand for February, March, May, June,
July and August 2004. Direct illness costs (expenditure on seeking and obtaining
treatment, including special food and transport) were recorded. Interviews were semi-
structured and conducted in the local language, with fieldworkers making detailed
handwritten notes in English following each visit. Interview notes and expenditure
summaries were later typed and stored electronically. The FGDs were also carried
out by trained fieldworkers, with six male-only and six female-only groups. The
initial FGDs were based around clinical vignettes, with participants asked how they
would react if members of their household developed specific symptoms. These
FGDs were followed by open-ended discussions addressing themes from the initial
FGDs in more detail, especially treatment-seeking behaviour and household coping
mechanisms.
Copyright # 2009 John Wiley & Sons, Ltd. J. Int. Dev. 21, 271–290 (2009)
DOI: 10.1002/jid

274 T. Porter et al.
2.2 Data Analysis for This Paper
This analysis was conducted at the KEMRI-Wellcome Trust Collaborative Programme,
Kilifi, between April and July 2007. Data generated through the urban household case
studies and FGDs were analysed.
Case study and FGD transcripts were read through in their entirety a number of times, to
identify initial coding categories, specifically concerning chronic illnesses and related
treatment-seeking behaviour. Manual coding of content suggested a number of emergent
themes, with analysis focusing in particular on perceived barriers to accessing treatment
and/or self-management of these conditions. As links between themes were explored a
conceptual framework was developed iteratively, based on these links. The same coding
schemawas used for both the case studies and FGD transcripts, with themes identified from
both sources. ‘Chronic illness’ was defined here as any which had been symptomatic for at
least 3months, or which had been diagnosed at least 3months prior. ‘Management’ of
chronic illness was taken to include any actions, opinions or feelings expressed by a
household member, acquaintance or health professional, concerning chronic illness.
Management was considered ‘successful’ if a condition was described as stable with
symptoms routinely controlled (through active monitoring if necessary) during the follow
up period.
Of the 29 households completing follow-up, 22 reported at least one chronic illness
during the follow-up period. If no expenditure was apparent on a reported chronic illness
during the six months analysed, the reasons for this were explored.
For each household total expenditure, total direct health expenditure, and chronic illness
expenditure were calculated for each of 6months during the follow-up period, along with
coefficients of variation to assess between-month fluctuation. In addition, expenditure data
were analysed to determine if any household’s total direct health expenditure or chronic
illness expenditure exceeded 10 per cent of its total expenditure in any month, one measure
of ‘catastrophic’ expenditure (Russell, 2004). At catastrophic levels, households are more
likely to sell assets, acquire debts and reduce consumption of necessities such as food.
3 FINDINGS
3.1 Household Characteristics and Illness Symptoms
A summary of the case study households is given in Table 1. Nearly two-thirds of
households (63.6 per cent, 14/22) had a household member educated to secondary school
level or above, a similar proportion to those in the original survey (65.0 per cent, 372/572).
The illness names given by householders usually directly matched a biomedical term,
although sometimes culturally-specific terms were used. The commonest chronic illnesses
were bone/joint pains, asthma and hypertension (Tables 1, 2).
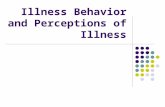
3.2 Conceptual framework for management of chronic illnesses (Figure 1)
A conceptual framework linking the themes identified in content analysis is presented in
Figure 1, which includes household responses to chronic illnesses, barriers to these
responses, outcomes and feedback mechanisms. The remaining findings are presented
according to this structure, with excerpts from fieldworker and FGD notes where relevant.
Copyright # 2009 John Wiley & Sons, Ltd. J. Int. Dev. 21, 271–290 (2009)
DOI: 10.1002/jid

Table 1. Case study household characteristics
Household (HH) HH members with chronic illness
HH code Number of
HH members
Highest
educational
level
Members with
chronic illness
Gender Age or age
range (years)
Chronic illnesses
A 6 College 2 F 6 Asthma
F 36 Stress/anxiety
B 8 Secondary 2 M 21 Asthma
F 2 Eye problem
C 6 College 2 F 35–50 Stomach ulcer, knee pain
F 50–80 Hypertension
D 10 Primary 1 F >60 ‘Chunu kuluma’ (waist ache)
E 7 Primary 1 F 50–80 Hypertension, ‘chunu kuluma’
F 7 Secondary 1 F 54 Diabetes mellitus, hypertension
G 8 Primary 2 M 75 Blind, diabetes mellitus,
hypertension, ‘chunu kuluma’
F 40 ‘Chunu kuluma’, ‘chala cha
mdudu’ (finger infection)
H 5 College 1 M 30 Epilepsy
I 7 Primary� 2 F 12 Meningitis complications
F 32 Stomach ulcers; breast lesion
J 3 College 1 M 35–50 Epilepsy
K 5 Secondary 1 M 57 Leg trauma
L 11 Secondary 2 M 46 Heart disease, stomach ulcers
M 26 Stress/anxiety
M 9 Secondary 2 M 23 Asthma
F 15 Gynaecological growth
N 13 Primary 1 M 18–35 Developmental delay
O 11 Primary� 1 F 30 Goitre
P 4 Secondary� 1 F 36 Tuberculosis
Q 6 Secondary 1 M 1 Asthma
R 6 Secondary 1 F 10–18 Down’s syndrome
S 5 Koran School 1 F 50–80 Mental illness
T 13 College 1 M 12 Asthma
U 12 Secondary 2 F >80 Hypertension, ’Maguu kuuma’
(leg pain)
M 20 Tuberculosis
V 13 Primary� 1 F 14 Epilepsy
Mean 8 1.4 36
�left before finishing.
Barriers to Managing Chronic Illness in Kenya 275
3.3 Household Responses (Box A, Figure 1)
Responses to chronic illness ranged from non-treatment to visiting multiple health
providers. Visiting a single, appropriately qualified, provider was unusual. Among those
not seeking treatment, some were delaying treatment as long as possible while others did
not intend to seek help.
Case study Household I: ‘The breast swelled and ached, and when she tried to
squeeze it some pus and blood come out. . . Since the problem started she has not seen
a doctor for medication because she has no money to go to hospital. Instead, when
she experiences the pain she boils water and sponges it. . .’
Copyright # 2009 John Wiley & Sons, Ltd. J. Int. Dev. 21, 271–290 (2009)
DOI: 10.1002/jid

Table 2. Frequency of chronic illnesses in case study households
Chronic illness Frequency
Bone/joint pains (including knee pain, ‘chunu kuluma’,
leg trauma, ‘maguu kuuma’)
7
Asthma 5
Hypertension 5
Epilepsy 3
Stomach ulcers 3
Diabetes mellitus 2
Eye problems (including non-specific eye problem and blindness) 2
Stress/anxiety 2
Tuberculosis 2
Other (breast lesion, ‘chala cha mdudu’, developmental delay,
Down’s syndrome, goitre, gynaecological growth, heart disease,
mental illness, neurological complications)
9
Total 40
276 T. Porter et al.
Individuals often visited a number of different providers for the same problem, e.g.
starting at a pharmacy then attending a private clinic, or seeking a second opinion after an
initial diagnosis. In other cases, private providers would be visited in the first instance, even
if they were more expensive than government facilities. Traditional healers were also
commonly attended, more so in the semi-rural areas of Mtwapa. The majority of visits to
health providers occurred once a patient had developed symptoms; it was rare for
preventive management to be sought.
Figure 1. Conceptual framework for management of chronic illnesses: household responses tochronic illness, barriers to household responses, outcomes and feedback mechanisms
Copyright # 2009 John Wiley & Sons, Ltd. J. Int. Dev. 21, 271–290 (2009)
DOI: 10.1002/jid

Barriers to Managing Chronic Illness in Kenya 277
3.4 Modifiers/Barriers to Household Responses (Box B, Figure 1)
A summary of how specific barriers contributed to household response is shown in Table 3,
with more detail below.
3.4.1 Anticipated cost
Cost was a very important factor underlying households’ responses, evidenced by 16/22
households which employed at least one cost-prevention or cost-reduction strategy. These
strategies were: not seeking medical advice (cost-prevention); seeking symptomatic
instead of preventive treatment, for example in asthma; not following or delaying advised
treatment; or attending a non-specialist facility (cost-reduction strategies). Cost-
management strategies (such as selling assets or going without food) were also widely
used. Since households usually made an estimate of treatment costs before seeking care,
the anticipated cost was often as important as the provider fee, and would take into account
transport and time off work. For tuberculosis (TB) and HIV/AIDS user fees were waived,
meaning patients were more likely to seek and receive treatment:
Case study Household P: ‘I thank God TB treatment is free, so I don’t spend much
on it’
Ironically, visiting multiple providers was often the result of cost-reduction strategies
(e.g. visiting a cheap provider but receiving inadequate treatment, necessitating further care;
or seeking a second opinion to obtain a diagnosis associated with less costly management).
3.4.2 Patient knowledge and beliefs
Varying levels of patient knowledge about diseases were found between FGD participants
and for different conditions.
FGDParticipant: ‘All the dust you inhaled went inside your lungs and this can bring
cough problems. That’s when people can say you have TB. And also smoking. . .Even a lady can get TB. Sometime back my cousin got TB and she used to cut Tano
(cutting or clearing the forests). . . And after about 4 years she suffered from TB and
all this was caused by the work and smoke (burning the cleared fields)’.
FGD Participant: ‘That man used to cough and is now serious. . . he needs to go tohospital for tests for TB (sputum). The doctor will know and treat’.
Some households seemed to be unaware that chronic illnesses can sometimes be
managed preventatively as well as acutely, indicating that avoiding preventive care could
result from a lack of knowledge as well as a deliberate cost-prevention strategy. A number
of households had strong traditional beliefs which caused them to seek healers or herbs for
certain illnesses, often regardless of cost.
Case study Household L: ‘Traditional healers are given first priority in the
household because he says experience has taught him that traditional medicine is
more effective than clinical medicine’.
Traditional beliefs were more pronounced among residents in the semi-rural areas of
Mtwapa, and there were suggestions from the FGDs that the use of healers was declining in
more urban areas.
Copyright # 2009 John Wiley & Sons, Ltd. J. Int. Dev. 21, 271–290 (2009)
DOI: 10.1002/jid

Table
3.
Specificeffectsofmodifiers/barriers(BoxB,Figure
1)onhousehold
responses(BoxA,Figure
1)
Household
response
Modifiers/barrierswhichmay
contribute
toresponse
Anticipated
cost
Patientknowledge
andbeliefs
Stigma
Provider
quality
Trust/perceived
quality
Longcare
pathway
Non-treatment
Notseekingmedical
adviceat
all
**
Delay
treatm
ent-seeking
*
Treatment-seeking
Visitmultiple
providers
**
**
*
Visitexpensiveprovider
only
**
*
Visittraditional
healer
**
**
Symptomatic
treatm
entonly
**
Attendingnon-specialistfacility
*
Visitsingle,appropriateprovider
*
Copyright # 2009 John Wiley & Sons, Ltd. J. Int. Dev. 21, 271–290 (2009
DOI: 10.1002/jid
278 T. Porter et al.
)

Barriers to Managing Chronic Illness in Kenya 279
3.4.3 Stigma
Individuals who thought they may have TB were sometimes deterred from visiting a health
facility for diagnosis because they feared being diagnosed with HIV/AIDS at the same
time. This fear seemed to result from a recognition that some of the symptoms of TB and
HIV can be similar and was demonstrated in an FGD and one of the case study households.
FGDFacilitator: ‘Now, why is it that the young people are afraid to visit the hospital
when they have TB’? Participant 2: ‘They are afraid depending on what one is
suffering from’. Participant 1: ‘For example if a man goes to the hospital with his
wife and has tests done, good if TB is found but if it’s the disease of nowadays
(AIDS) they become ashamed and that’s the reason they don’t visit the hospital’.
In household H there was also evidence of community stigma associated with epilepsy.
There was no evidence of stigma for other chronic illnesses in the study.
3.4.4 Provider quality
Households and FGD participants cited difficulties encountered with providers, including
long queues, unhelpful staff and slow service at government hospitals, and a lack of
common drugs at government dispensaries. Traditional healers could apparently
sometimes expose patients to additional risk:
FGD Participant: ‘Others also get [HIV] by bad luck - for example if one goes to a
mganga (local healer) and she uses a razor which she cuts on you and has been used
on another person, one can get infected’.
3.4.5 Trust/perceived quality
Trust seemed to influence householders’ choice of provider, reinforcing some relationships
and curtailing others. A lack of trust was suggested in some cases where individuals
visited multiple providers for a set of symptoms, only to be given the same diagnosis at
each:
Case study Household F: ‘Three years ago the spouse found herself at [a private
hospital]. She was suffering from high blood pressure and diabetes and she knew this
after undergoing some tests. . . She did not believe she had high blood pressure. Thismade her seek another doctor where she was also diagnosed with the same disease’.
Trust was also linked to patients’ previous clinical outcomes, reinforced after a positive
experience.
3.4.6 Long care pathways
For tuberculosis it was found that the official treatment pathway for patients wishing to use
government facilities was complex and required visiting three health facilities, often with
associated transport costs:
FGD Participant 1:‘One goes to the Coast General Hospital first for a picture (X-
ray) and then referred to Port Reitz’. Participant 2: ‘At Port Reitz you’ll get treated
then you’ll be referred to the nearest hospital near your home to get drugs. Like here
in Mtwapa one is referred to get them at Shimo la Tewa’
Copyright # 2009 John Wiley & Sons, Ltd. J. Int. Dev. 21, 271–290 (2009)
DOI: 10.1002/jid

280 T. Porter et al.
3.5 Outcomes (Box C, Figure 1)
3.5.1 Clinical
Following a single episode of treatment seeking, most patients’ symptoms were addressed
either temporarily, or not at all—few gained long-term control of their chronic illness. For
individuals who could not afford or delayed definitive treatment, disease progression was a
possibility.
Case study Household K: ‘November this year, it was very hard on me. I wouldn’t
walk, hold my stick or do anything. I was extremely sick. . .[then, following admission
to hospital for 3 days, shorter than advised]. . . I feared the bill would be too enormous
for the household to pay! And I come back home still very sick. . . [later in the year,
described by the fieldworker] Walking is now a serious problem. . . in fact this
problem is the main reason why the household head can’t/isn’t earning nowadays’
3.5.2 Costs of chronic illness
A summary of household expenditure (from expenditure diaries kept by the households),
including chronic illness expenditure, is given in Table 4. Chronic illnesses contributed, on
average, to just under one fifth (18.3 per cent, 104/569KSh) of total health expenditure in
households with chronic illness. Interestingly, whilst in 14 households total direct health
expenditure was catastrophic during at least one month in the study period, only in
4 households was this due to chronic illness alone. Pharmacies and private clinics were
responsible for the majority of chronic illness spending (34.7 and 34.2 per cent,
respectively), with little spent at government dispensaries (0.6 per cent) (data not shown).
There was also qualitative evidence of significant indirect illness costs associated with
chronic illness, such as time off work.
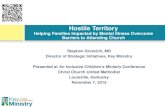
There was considerable month-by-month fluctuation in total expenditure, health
expenditure and chronic illness expenditure. Households broadly fell into four categories
with respect to the latter (Figure 2); interestingly only one household, U, showed a pattern
of regular chronic illness expenditure (category c). In households where no expenditure
was made during the formal diary period, the reasons for this were explored in the
interviews (Table 5); for example, in some cases, families related that chronic illness costs
had occurred, but outside the formal diary period.
3.5.3 Household vulnerability and resilience implications
Both direct and indirect costs associated with illness and treatment-seeking behaviour reduced
the resilience of households to face future illness episodes and other crises. For example, some
households were forced to sell assets or go without food in order to pay for treatment:
Case study Household F: ‘At the hospital she paid 800KSh from personal savings
because the husband works and from tenants. This affected the family financially
because. . .sometimes they were going without food’.
Others found difficulty working due to incapacitation. Social assets were often
diminished if debts taken to pay for treatment could not be paid back and illnesses were
sometimes responsible for breakdowns in family relationships:
Case study Household H: ‘The husband suffers from kifafa (epilepsy). During this
time he had no money to treat his illness and therefore after seeing the wife’s savings
Copyright # 2009 John Wiley & Sons, Ltd. J. Int. Dev. 21, 271–290 (2009)
DOI: 10.1002/jid

Table
4.
Financial
summaryofcase
studyhouseholdsFebruary–August
2004(excl
April)
Household
Totalexpenditure
Healthexpenditure
Chronic
illnessexpenditure
Catastrophic
costs�
Monthly
average
(KSh)
Coefficient
ofvariation
(%)
Monthly
average
(KSh)
Coefficient
ofvariation
(%)
%oftotal
expenditure
(mean)
Monthly
average
(KSh)
Coefficient
ofvariation
(%)
%oftotal
expenditure
(mean)
Allhealth
expenditure
Chronic
illness
only
A23638
70
452
159
4.8
3245
0.0
*
B33852
47
1426
140
4.1
314
122
0.7
*
C20853
12
403
144
2.0
382
156
1.9
D6754
42
170
119
2.3
0—
0.0
E7176
17
262
161
3.4
171
245
2.1
**
F10174
15
323
196
4.0
306
210
3.8
**
G5319
18
228
194
4.3
185
242
3.4
**
H15515
47
1136
83
9.2
205
124
1.4
*
I5192
53
19
40
0.4
0—
0.0
J11388
53
446
124
7.2
170
224
1.6
*
K6906
92
295
200
2.1
0—
0.0
L15801
36
266
168
1.2
40
224
0.3
M11435
64
2295
233
11.0
0—
0.0
*
N8803
39
71
160
0.8
0—
0.0
O12956
48
689
148
3.6
333
245
1.9
**
P19427
38
1553
111
7.4
0—
0.0
*
Q10461
26
374
167
3.0
44
239
0.3
*
R24618
65
475
179
4.4
0—
0.0
*
S4987
42
133
81
4.2
0—
0.0
*
T31319
65
1138
117
5.2
75
245
0.1
*
U12187
43
118
121
0.9
60
00.6
V16784
32
248
81
1.5
0—
0.0
Mean(allHH)
14343
44
569
142
4.0
104
194
0.8
Note:Exchangerate
£1¼144KShKenyan
Shillingson1March
2004(O
andA.com,2007).
� catastrophiccostsdefined
hereas
atleast1month
when
directhealthorchronicillnesscostsexceeded
10%
oftotalhousehold
expenditure
(notethiswillnotbeapparentfrom
the
Copyright # 2009 John Wiley & Sons, Ltd. J. Int. Dev. 21, 271–290 (20
DOI: 10.1002
Barriers to Managing Chronic Illness in Kenya 281
meanfigure
given
inthecolumnto
theleft).
09)
/jid

Figure 2. Household chronic illness expenditure by month, categorised by expenditure pattern
282 T. Porter et al.
in the house, he decided to use it and tell the wife when she came back. . .He thoughthewas doing the right thing to use the money to get treatment but it changed when the
wife returned. . . and found her money was missing. . . in the end she decided to
[leave]. . . ’
Furthermore, it was not always just the household of the ill individual which became
more vulnerable: it was common for relatives to be asked by the patient to help pay large
treatment bills at short notice.
Copyright # 2009 John Wiley & Sons, Ltd. J. Int. Dev. 21, 271–290 (2009)
DOI: 10.1002/jid

Table 5. Reasons for households (HH) reporting chronic illnesses but no associated expenditure
Household Treatment not sought or delayed
Treatment sought Treatment desiredby HH
Treatment not desiredby HH
Costs incurredoutside study
period
Freetreatment
Inabilityto pay
Fear ofrequestingcredit
Previoustreatmentfailure
No symptomsrequiringtreatment
D * *
I * * *
K *
M * *
N *
P *
R *
S * *
V * *
Barriers to Managing Chronic Illness in Kenya 283
3.6 Feedback Mechanisms (Box D, Figure 1)
There appeared to be a feedback loop between households’ illness responses and outcomes
and the barriers they faced to chronic illness management: in many cases barriers to
successfully managing future illness episodes increased. The cost of care sometimes
impacted on households’ resilience, reducing their ability to afford to pay for future
treatment; and where care was expensive (particularly if multiple providers were attended),
the anticipated cost of future episodes in some cases deterred a timely response. Finally,
clinical outcomes seemed to influence trust in providers in some households, with
increased or reduced trust following a positive or negative experience respectively.
4 DISCUSSION
4.1 Critique of Methods
The majority of studies examining household expenditure and treatment-seeking
behaviour are cross-sectional and more longitudinal studies such as this have been called
for to understand the relationship between treatment-seeking behaviour and long-term
household outcomes (Russell, 2004). Although the sample size was good for the
longitudinal qualitative data, the reliability of the quantitative expenditure data would
increase with a larger study. The generalisability of this latter dataset is also limited by the
selection procedure used for case study households.
The definition for ‘catastrophic’ expenditure used here (direct costs over 10 per cent of
total household expenditure) is widely accepted, although some poorer households would
experience catastrophic spending at levels below 10 per cent and less-poor households may
be able to cushion expenditure above this; an alternative measure may have been more
sensitive (indirect and direct costs over 40 per cent of non-food expenditure) (Xu et al.,
2003). Although only direct cost data were available to be analysed quantitatively here,
there was qualitative evidence of significant indirect costs captured in household
Copyright # 2009 John Wiley & Sons, Ltd. J. Int. Dev. 21, 271–290 (2009)
DOI: 10.1002/jid

284 T. Porter et al.
interviews, consistent with the literature that indirect costs in chronic illness can be large
(McIntyre et al., 2006), often higher than direct (Babu et al., 2002); quantitative analysis of
indirect costs would have been useful to confirm this. The observation that households’
expenditure patterns fell into distinct groups (Figure 2) could have been spurious. For
example, it is possible that most households face catastrophic chronic illness costs from
time to time, even if this was not picked up during the study.
Barriers were identified from the perspective of households and FGD members and as
such (except for cost) were ‘expressed’ or ‘felt’ barriers; this study did not explore whether
these were problems of perception rather than reality. It is also known that the frequency of
self-reported chronic illness often exceeds formally diagnosed illness, since many chronic
symptoms are never reported to health professionals (Bazargan et al., 2005). There are also
likely to be barriers in further areas, especially on the supply-side (e.g. healthcare
organisations), outside the scope of this primarily demand-side study. Compliance with
expenditure diaries was generally good (126/132¼ 95.4 per cent complete), with high
between-month variation unlikely to be the result of measurement error.
The use in some cases of culturally-specific illness labels (e.g. ‘chunu kuluma’) could
make comparisons with other studies and applicability to other settings difficult, but it was
felt that attempting to convert these labels to biomedical diagnoses may be misleading.
Although many of the same barriers to chronic illness care are likely to exist in resource-
poor settings elsewhere, the detail and relative significance of each probably vary between
countries and cultures, so local studies would be needed to assess these and identify
appropriate interventions in each context.
4.2 Cost is By Far the Most Important Barrier
The illness costs observed in this study fit broadly with the general literature on household
health expenditure, with mean total health expenditure of 4 per cent (Table 4) within the
2.5–7 per cent range seen in similar settings (Russell, 2004) and chronic illness costs
contributing to catastrophic expenditure (Su et al., 2006). Costs may escalate as a result of
particular household responses, with the behaviour contributing to this cycle documented
for acute care elsewhere in Kenya (Nyamongo, 2002).
The ICCC framework calls for protection from catastrophic health costs. In many
countries—including Kenya—costs have been found to be ‘regressive’, with the poor
paying a larger proportion of their income on health (Chuma et al., 2007). How easily
households can meet costs is determined in part by their ‘resilience’, a concept related to
‘vulnerability’, encompassing their financial, social and human assets (Russell, 1996). The
present study found that expenditure on chronic illness could affect the determinants of
household resilience, through an erosion of these assets. This implies that, in contrast to
most acute illnesses, the poor management of a chronic illness could potentially affect
resilience over a period of months or years.
4.3 Other Barriers Also Play A Significant Role
4.3.1 Patient knowledge and beliefs
The ICCC ideal of patients as ‘active participants in care’ was not observed in this setting.
A lack of awareness of preventive care for many chronic conditions has been found
elsewhere in sub-Saharan Africa (Berhanu et al., 2002), and in Ghana the use of traditional
healers was found to be one form of coping strategy if it was cheaper than biomedicine
Copyright # 2009 John Wiley & Sons, Ltd. J. Int. Dev. 21, 271–290 (2009)
DOI: 10.1002/jid

Barriers to Managing Chronic Illness in Kenya 285
(de-Graft Aikins, 2005), mirroring the responses of some Kenyan households. In Tanzania,
traditional healers were often preferred because they accepted payment ‘in kind’ and
costs for traditional treatment were more likely to be shared by the family (Muela et al.,
2000).
4.3.2 Stigma
HIV-related stigma in patients with suspected tuberculosis has also been seen in other low-
income settings (Ngamvithayapong et al., 2000; Godfrey-Faussett and Ayles, 2003), along
with stigma due to TB alone (Liefooghe et al., 1995), and may be responsible for delayed
presentation of individuals for tuberculosis investigation.
4.3.3 Provider quality and trust
There is circumstantial evidence from this study of under-performing health providers,
causing patients to seek second opinions or visit expensive providers at the outset. The
numbers of government hospitals, dispensaries and health centres in Coast Province are
below the Kenyan average for the population size (Gondi et al., 2006), suggesting this may
partly be due to a lack of capacity.
4.3.4 Long care pathways
Providing management is not delayed by patients visiting a number of different providers
(Pronyk, 2001), siting specialist facilities at a regional referral hospital may actually help
maintain quality of care, although transport costs can still be limiting for the very poor.
4.4 Addressing the Barriers
A recent strategy document, the NHSSP, has proposed widespread changes in the way the
Kenyan health system is organised and funded (Government of Kenya, 2005). Where
applicable, proposals in the NHSSP are discussed in relation to the findings presented here.
4.4.1 Cost
To make it easier for households with chronic illness to cope with the resulting costs, two
main approaches exist: reduce (or even out) the absolute cost of healthcare for chronic
illnesses; or reduce the relative cost of healthcare by increasing household resilience.
(Additionally, increasing access to acute care could have an effect on chronic illness
management—some of the illnesses reported here were likely to have been inadequately
treated acute diseases.)
In recent years user fees have been criticised as disadvantaging the poor, leading to calls
for their abolition (Palmer et al., 2004; McIntyre et al., 2006). In Kenya, user fees were
introduced through a ‘cost sharing’ initiative in 1989, but due to increasingly
heterogeneous costs at health facilities, consultation tariffs were fixed in 2004 at
10KSh and 20KSh at government dispensaries and health centres respectively (Oyaya and
Rifkin, 2003; Pearson, 2005). The results of the present analysis would support the
abolition of user fees for the poorest in society, although without extra funding this risks a
knock-on reduction in the quality or availability of other government health services. The
recent waiver of user fees for HIV/AIDS and TB in Kenya, and the plans set out in the
NHSSP for user fees to be replaced by compulsory National Social Health Insurance Fund
(NSHIF) payments which would be waived for the poorest members of society, are
Copyright # 2009 John Wiley & Sons, Ltd. J. Int. Dev. 21, 271–290 (2009)
DOI: 10.1002/jid

286 T. Porter et al.
encouraging developments. It is implied that chronic illness management would be funded
by the NSHIF for vulnerable members of society, although this is not categorically stated in
the NHSSP. Research into alternative funding mechanisms for healthcare has also been
called for (McIntyre et al., 2006), with health insurance and microeconomic loans
proposed to reduce the economic impact of illness (Sherer, 2004).
The cost of providing care might be reduced through the use of peer-support groups or
trained laypeople. New ‘community owned resource persons’ (CORPs) suggested in the
NHSSP may prove useful, so long as difficulties encountered with community health
worker and Primary Health Care initiatives elsewhere (mainly around adequacy of training
and support), are avoided (Berman et al., 1987; Stekelenburg et al., 2003). Encouraging
responsible self-management could also reduce this bill (WHO, 2002c; Newman et al.,
2004), and given the rapid uptake of mobile phones in Kenya and many other parts of sub-
Saharan Africa (Ovum, 2007), telephone consultations could also have a role in disease
monitoring (Piette et al., 2006), although this may decrease equity by favouring those who
own a mobile phone.
Addressing household resilience is the second approach. Measures to help households
increase or stabilise their income, promote savings, support social networks and increase
equity would have a positive effect on their ability to cope with chronic illness costs, over
the longer term. These measures would require concerted government-wide action; the
NHSSP proposes identifying and providing financial support for vulnerable groups at the
local level, although the details are vague. In Kenya most borrowing is through informal
contacts, such as neighbours or self-help groups, with only 6.5 per cent of borrowers using
banks (Daily Nation, 2007); recent work suggests that community-based organisations
could play a significant role in supporting households coping with illness costs (Molyneux
et al., 2007).
4.4.2 Patient knowledge and beliefs
Information asymmetry between patients and providers makes it difficult for patients to
accurately assess the quality of providers and self-manage their condition. Empowered,
knowledgeable patients are particularly important in chronic compared with acute
illnesses; the use of independent consumer education could help in this respect (Mills et al.,
2002). The NHSSP suggestion of regular health promotion is a start, but appears to be
restricted to the elderly and may not be ambitious enough to empower patients to manage
their own diseases. However, proposals to develop a network of CORPs managed at the
village level and the adoption of a ‘human rights’ approach to health are more encouraging,
although again much of the detail of these measures is to be decided. Registering and
regulating traditional healers and medicines may also help patients make a more informed
choice as well as increasing provider quality (see below) (WHO, 2002d).
4.4.3 Stigma
It has been suggested HIV-related stigma is best addressed through community
mobilisation and advocacy, encouraging the HIV-positive community to actively oppose
stigmatisation (WHO, 2002c; Parker and Aggleton, 2003), rather than by attempting to
directly increase tolerance among the general population (Brown et al., 2003).
4.4.4 Provider quality
Accreditation and regulation of providers could help improve quality, so long as excessive
or poorly targeted regulation was avoided (Soderlund and Tangcharoensathien, 2000);
Copyright # 2009 John Wiley & Sons, Ltd. J. Int. Dev. 21, 271–290 (2009)
DOI: 10.1002/jid

Barriers to Managing Chronic Illness in Kenya 287
NHSSP proposals for increased power to be handed to professional regulatory bodies, as
well as the development of quality assurance programmes for traditional medicine, are
useful if limited.
4.4.5 Trust
Trust between patient and provider may be increased by providing high quality services,
and ensuring staff adhere to professional and ethical codes. Visibly increasing the equity of
government services and ensuring probity and good management practice, may also
improve trust (Tibandebage and Mackintosh, 2005). Increasing trust may have other
benefits too, increasing system efficiency and providing therapeutic advantages for the
individual (Gilson, 2003; Tibandebage and Mackintosh, 2005).
4.5 Applying Chronic Illness Management Frameworks
The ICCC framework identifies ‘building blocks’ to promote chronic illness management
at three levels—micro (the patient and family and primary care/community professionals),
meso (healthcare organisations and the community), and macro (the policy environment)
(WHO, 2002c). None of the barriers identified in this analysis relate to just one ICCC level;
instead they transect all three. In general, the building blocks are useful reference points
with which to compare local healthcare provision, although some of the present findings
suggest that implementation of the framework in coastal Kenya could still be challenging,
such as integrating care pathways and empowering patients.
5 CONCLUSION
This analysis has provided evidence for some of the barriers faced when managing chronic
illnesses in resource-poor settings. In particular, treatment costs are punitive and
unpredictable and in concert with other barriers can adversely affect households’
resilience, further limiting their ability to cope.
The NHSSP is encouraging but ambitious and requires implementation through wide-
reaching legislation in the health, social and financial sectors. In particular, policies to
reduce chronic illness costs must be honoured if their management is to improve.
Further studies are needed to examine whether the barriers identified here expressed at
the household level are also present at the micro, meso and macro levels and in other
resource-poor settings. Operational research is needed to examine how best to implement
policy changes in local environments.
ACKNOWLEDGEMENTS
We would like to thank Isaac Charoh, Gladys Sanga and all the individuals who took part
in the case study and focus group discussions for their help and advice. Also thanks to
Dr Steve Russell for his helpful comments on drafts of this paper. Finally, Thomas Porter is
sincerely grateful to his wife for remaining patient while he was ‘in the field’!
Copyright # 2009 John Wiley & Sons, Ltd. J. Int. Dev. 21, 271–290 (2009)
DOI: 10.1002/jid

288 T. Porter et al.
REFERENCES
Adams SG, Smith PK, Allan PF, Anzueto A, Pugh JA, Cornell JE. 2007. Systematic review of the
chronic care model in chronic obstructive pulmonary disease prevention and management.
Archives of Internal Medicine 167: 551–561.
Babu BV, Nayak AN, Dhal K, Acharya AS, Jangid PK, Mallick G. 2002. The economic loss due to
treatment costs and work loss to individuals with chronic lymphatic filariasis in rural communities
of Orissa, India. Acta Tropica 82: 31–38.
Bazargan M, Bazargan-Hejazi S, Baker RS. 2005. Who is playing doctor?—The gap between self-
perceived versus professionally-diagnosed chronic conditions among the underserved minority.
Preventive Medicine 41: 883–886.
Berhanu S, Alemu S, Asmera J, Prevett M. 2002. Primary care treatment of epilepsy in rural Ethiopia.
Ethiopian Journal of Health Development 16: 235–240.
Berman PA, Gwatkin DR, Burger SE. 1987. Community-based health workers: head start or false
start towards health for all? Social Science & Medicine 25: 443–459.
Berman P, Kendall C, Bhattacharyya K. 1994. The household production of health: integrating social
science perspectives on micro-level health determinants. Social Science & Medicine 38: 205–215.
Birbeck GL. 2000. Barriers to care for patients with neurologic disease in rural Zambia. Archives of
Neurology 57: 414–417.
Bodenheimer T, Wagner EH, Grumbach K. 2002. Improving care for patients with chronic illness.
Journal of the American Medical Association 288: 1775–1779.
Brown L, Macintyre K, Trujillo L. 2003. Interventions to reduce HIV/AIDS stigma: what have we
learned? AIDS Education and Prevention 15: 49–69.
Chuma JM, Thiede M, Molyneux CS. 2006. Rethinking the economic costs of malaria at the
household level: evidence from applying a new analytical framework in rural Kenya. Malaria
Journal 5: 76.
Chuma J, Gilson L, Molyneux C. 2007. Treatment-seeking behaviour, cost burdens and coping
strategies among rural and urban households in Coastal Kenya: an equity analysis. Tropical
Medicine & International Health 12: 673–686.
Daily Nation. 2007. Many Kenyans borrow money from neighbours not banks. From: www.na-
tionmedia.com (accessed 27 April 2007).
de-Graft Aikins A. 2005. Healer shopping in Africa: new evidence from rural-urban qualitative study
of Ghanaian diabetes experiences. British Medical Journal 331: 737–743.
El Ansari W. 2006. Chronic conditions and the developing world: a contribution to the evidence base.
Chronic Illness 2: 159–160.
Furber AS, Hodgson IJ, Desclaux A, Mukasa DS. 2004. Barriers to better care for people with AIDS
in developing countries. British Medical Journal 329: 1281–1283.
Gilson L. 2003. Trust and the development of health care as a social institution. Social Science &
Medicine 56: 1453–1468.
Godfrey-Faussett P, Ayles H. 2003. Can we control tuberculosis in high HIV prevalence settings?
Tuberculosis 83: 68–76.
Gondi O, Otieno C, James J. 2006. Report on human resource mapping and verification
exercise. From: http://www.health.go.ke/planning1/HUMAN%20RESOURCE%20MAPPING%
20report.pdf (accessed 26 July 2007).
Government of Kenya, Ministry of Health. 2005. Reversing the trends: the second national health
sector strategic plan (NHSSP). From: http://www.drh.go.ke/documents/NHSSP%20II%202005-
2010 (accessed 11 August 2007).
Copyright # 2009 John Wiley & Sons, Ltd. J. Int. Dev. 21, 271–290 (2009)
DOI: 10.1002/jid

Barriers to Managing Chronic Illness in Kenya 289
Harpham T, Stephens C. 1991. Urbanization and health in developing countries. World Health
Statistics Quarterly 44: 62–69.
Liefooghe R, Michiles N, Habib S, Moran MB, de Muynck A. 1995. Perception and social
consequences of tuberculosis: a focus group study of tuberculosis patients in Sialkot, Pakistan.
Social Science & Medicine 41: 1685–1692.
McIntyre D, Thiede M, Dahlgren G, Whitehead M. 2006. What are the economic consequences for
households of illness and of paying for health care in low- and middle-income country contexts?
Social Science & Medicine 62: 858–865.
Mills A, Brugha R, Hanson K, McPake B. 2002. What can be done about the private health sector in
low-income countries? Bull WHO 80: 325–330.
Molyneux C, Hutchison B, Chuma J, Gilson L. 2007. The role of community-based organizations in
household ability to pay for health care in Kilifi District, Kenya. Health Policy and Planning 22:
381–392.
Muela SH, Mushi AK, Ribera JM. 2000. The paradox of the cost and affordability of traditional and
government health services in Tanzania. Health Policy and Planning 15: 296–302.
Mufunda J, Chatora R, Ndambakuwa Y, Nyarango P, Kosia A, Chifamba J, Filipe A, Usman A,
Sparks VA. 2006. Emerging non-communicable disease epidemic in Africa: preventive measures
from the WHO regional office for Africa. Ethnicity & Disease 16: 521–526.
Murray CJ, Lopez AD. 1997. Alternative projections of mortality and disability by cause 1990–2020 :
global burden of disease study. Lancet 349: 1498–1504.
Newman S, Steed L, Mulligan K. 2004. Self-management interventions for chronic illness. Lancet
364: 1523–1537.
Ngamvithayapong J, Winkvist A, Diwan V. 2000. High AIDS awareness may cause tuberculosis
patient delay: results from an HIV epidemic area, Thailand. AIDS 14: 1413–1419.
Nyamongo IK. 2002. Health care switching behaviour of malaria patients in a Kenyan rural
community. Social Science & Medicine 54: 377–386.
OandA.com. 2007. Historical currency exchange rates for 1 March. 2004. From: http://www.oan-
da.com/convert/fxhistory (accessed 10 August 2007).
Ovum. 2007. Africa passes 200 million connections in Q1 2007. From: http://www.ovum.com/go/
content/c,377,70918 (accessed 27 July 2007).
Oyaya CO, Rifkin SB. 2003. Health sector reforms in Kenya: an examination of district level
planning. Health Policy 64: 113–127.
Palmer N, Mueller DH, Gilson L, Mills A, Haines A. 2004. Health financing to promote access in
low-income settings—how much do we know? Lancet 364: 1365–1370.
Parker R, Aggleton P. 2003. HIV and AIDS-related stigma and discrimination: a conceptual
framework and implications for action. Social Science & Medicine 57: 13–24.
Pearson M. 2005. Abolishing user fees in Africa? It depends. . . HLSP Institute. From: http://
www.hlspinstitute.org/files/project/83490/abolishing_user_fees.pdf (accessed 26 July 2007).
Piette JD, Lange I, Issel M, Campos S, Bustamante C, Sapag J, Poblete F, Tugwell P, O’Connor AM.
2006. Use of telephone care in a cardiovascular disease management programme for type 2
diabetes patients in Santiago, Chile. Chronic Illness 2: 87–96.
Pronyk PM. 2001. Assessing health seeking behaviour among tuberculosis patients in rural South
Africa. International Journal of Tuberculosis and Lung Disease 5: 619–627.
Russell S. 1996. Ability to pay for health care: concepts and evidence. Health Policy and Planning
11: 219–237.
Russell S. 2004. The economic burden of illness for households in developing countries: a review of
studies focusing on malaria, tuberculosis, and human immunodeficiency virus/acquired immu-
nodeficiency syndrome. American Journal of Tropical Medicine and Hygiene 71(S2): 147–155.
Copyright # 2009 John Wiley & Sons, Ltd. J. Int. Dev. 21, 271–290 (2009)
DOI: 10.1002/jid

290 T. Porter et al.
Sherer RD. 2004. Microeconomic loans and health education to families in impoverished commu-
nities: implications for the HIV pandemic. Journal of the International Association of Physicians
in AIDS Care 3: 110–114.
Soderlund N, Tangcharoensathien V. 2000. Health sector regulation—understanding the range of
responses from government. Health Policy and Planning 15: 347–348.
Stekelenburg J, Kyanamina SS, Wolffers I. 2003. Poor performance of community health workers in
Kalabo District, Zambia. Health Policy 65: 109–118.
Strong K,Mathers C, Leeder S, Beaglehole R. 2005. Preventing chronic diseases: howmany lives can
we save? Lancet 366: 1578–1582.
Su TT, Kouyate B, Flessa S. 2006. Catastrophic household expenditure for health care in a low
income society: a study from Nouna District, Burkina Faso. Bull WHO 84: 21–27.
Tibandebage P, Mackintosh M. 2005. The market shaping of charges, trust and abuse: health care
transactions in Tanzania. Social Science & Medicine 61: 1385–1395.
Tsai AC, Morton SC, Mangione CM, Keeler EB. 2005. A meta-analysis of interventions to improve
care for chronic illnesses. American Journal of Managed Care 11: 478–488.
Unwin N, Setel P, Rashid S, Mugusi F, Mbanya J, Kitange H, Hayes L, Edwards R, Aspray T, Alberti
KG. 2001. Non-communicable diseases in sub-Saharan Africa: where do they feature in the health
research agenda? Bull WHO 79: 947–953.
Wagner EH, Austin BT, Korff MV. 1996. Organizing care for patients with chronic illness. The
Milbank Quarterly 74: 511–544.
Wagner EH. 1998. Chronic disease management: what will it take to improve care for chronic illness?
Effective Clinical Practice 1: 2–4.
Wang L, Kong L, Wu F, Bai Y, Burton R. 2005. Preventing chronic diseases in China. Lancet 366:
1821–1824.
World Health Organization. 2002a. Global Burden of Disease: DALYs by age, sex and
cause for 2002. From: http://www.who.int/entity/healthinfo/statistics/gbd1990regiondaly2002.xls
(accessed 22 July 2007).
World Health Organization. 2002b. Estimated total DALYs by cause and member state, 2002. From:
http://www.who.int/entity/healthinfo/statistics/bodgbddeathdalyestimates.xls (accessed 23 July
2007).
World Health Organization. 2002c. Innovative Care for Chronic Conditions: building blocks for
action. From: http://www.who.int/diabetesactiononline/about/icccreport/en/index.html (accessed
22 July 2007).
World Health Organization. 2002d. WHO Traditional Medicine Strategy 2002-2005. From. http://
whqlibdoc.who.int/hq/2002/WHO_EDM_TRM_2002.1.pdf (accessed 27 July 2007).
World Health Organization. 2005. Preventing chronic disease: a vital investment. From: http://
www.who.int/chp/chronic_disease_report/en/index.html (accessed 22 July 2007).
Xu K, Evans DB, Kawabata K, Zeramdini R, Klavus J, Murray CJ. 2003. Household catastrophic
expenditure: a multicountry analysis. Lancet 362: 111–117.
Copyright # 2009 John Wiley & Sons, Ltd. J. Int. Dev. 21, 271–290 (2009)
DOI: 10.1002/jid