Balloon Assisted Coiling in Ruptured Cerebral Aneurysms
40
BALLOON ASSISTED COILING IN RUPTURED CEREBRAL ANEURYSMS Vipul Gupta Neurointerventional Surgery Artemis Hospital, Gurgaon
-
Upload
dr-vipul-gupta -
Category
Health & Medicine
-
view
42 -
download
3
Transcript of Balloon Assisted Coiling in Ruptured Cerebral Aneurysms

BALLOON ASSISTED COILING IN RUPTURED CEREBRAL ANEURYSMS
Vipul GuptaNeurointerventional SurgeryArtemis Hospital, Gurgaon



Major changes Length of balloon Double lumen 14 wire, easy to
reshape, stability, exchange
Placement of stents Distal infusion
Historical One of the major issues for coiling – broad
neck Prof J Moret – “Remodeling technique”
Interventional Neuroradiology 1997

Uses of balloon
Broad neck aneurysm Remodelling – J Moret Packing density Control of rupture Test occlusion

Remodeling- broad neck

Balloon assisted coiling

Intra-operative rupture

Test occlusion

Remodeling technique for endovascular treatment of ruptured intracranial aneurysms had a higher rate of adequate postoperative occlusion than did conventional coil embolization with comparable safety.Pierot L Cognard C, Anxionnat R, Ricolfi F; CLARITY Investigators.
CONCLUSION –REMODELING TECH SAFE AND MORE EFFICACIOUS IN TERMS OF POSt OP OCCLUSION THAN THE CONVENTIONAL COILING TECH
Radiology. 2011 Feb;258(2):546-53.
POSTOP ANATOMICAL RESULTS
http://www.ncbi.nlm.nih.gov/pubmed/?term=Anxionnat%20R%5BAuthor%5D&cauthor=true&cauthor_uid=21131582

Technique Sidewall- compliant balloon, if overinflation
needed and aneurysm not large supercompliant
Bifurcation- Supercompliant Usually balloon with 014 wire Wire – usually choice, Synchro 6 F (.70) Guiding catheter , long sheath
(Raphe, Cook) Choose the right branch (even if takes time,
effort…)- more involved, lobule near neck

Usually check after first coil placement
Thereafter – multiple coils in single inflation – 5min (may be more)
Increase heparinization, BP maintenance
If unruptured- anti-platelet beforehand
Overall – 70-80% of cases (our practise- 90% ruptured, 80% small)- trend towards balloon coiling in all broad neck aneurysms

Choice of artery …



Placement angle….



A B C
STENT ASSISTED COILING TECH VS STAND ALONE COILING
ADVANTAGES – Scaffolding, haemodynamic effect, straightening of vessels
DRAWBACKS WITH SACT:
• looser aneurysm packing, lesser immmediate angiographic occlusions rate than the stand alone coiling
• DUAL ANTIPLATELET – RISK OF HEMORRHAGIC COMPLICATION
• MORE THROMBOEMBOLIC RISKS
AT FOLLOW UP COMPLETE OCCLUSION RATE WITH SACT INCREASED TO 73.4% IN SACT VS 54% IN SAC

MORBI-MORTALITY WITH STAND ALONE COILING OR BRT
MORBI-MORTALITY WITH STENT ASSISTED COILING
Nishido et al.(AJNR 2014) unruptured and ruptured aneurysms
5.6% 9.4%
Shapiro et al. (AJNR 2012) review, unruptured and ruptured aneurysms
NA 12.2%
GeyIk at al (AJNR 2013)
NA 6.4%
Stent assisted coiling .. Complication rateM Piotin et al , Frontiers in Neurology, 2014

Balloon – specific situations
Branch from aneurysm – overinflation tech.
Near the neck rupture – catheter reposition tech.
Unstable catheter coils- Single inflation
Circumferential involvement- end hole technique
Very small aneurysm – partial inflation tech
Displaced coil loop – balloon reposition
Balloon assisted MC placement

A B
Branch from aneurysm- Overinflation technique


Near the neck rupture

Multi-lobulated aneurysms-
Catheter reposition


Single inflation technique

Circumferential involvement-End hole

Follow-up

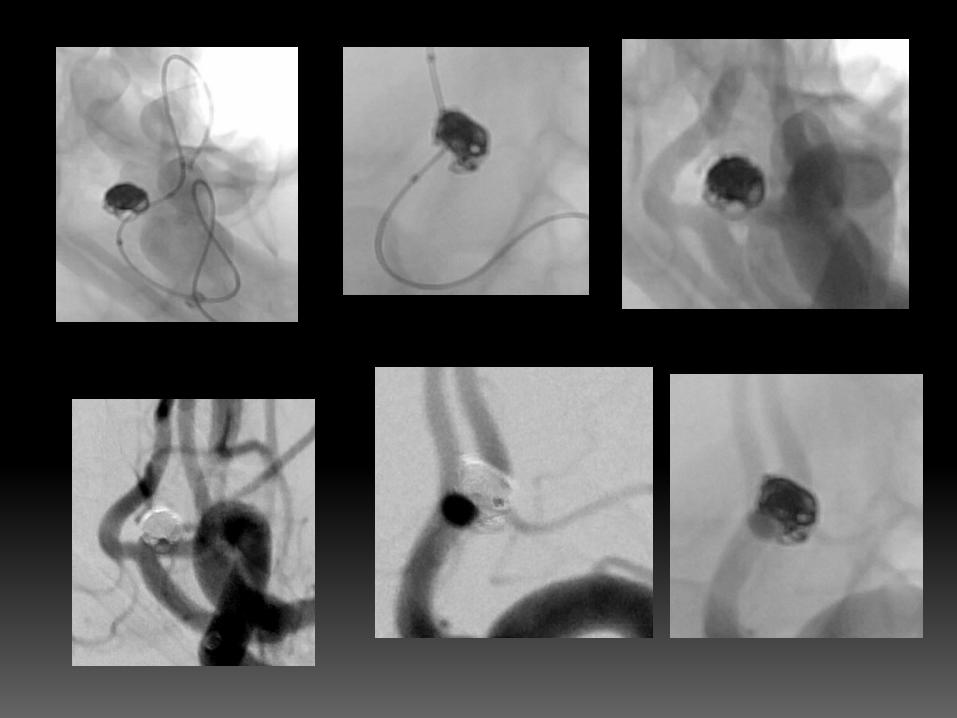

Very small aneurysm- partial inflation technique
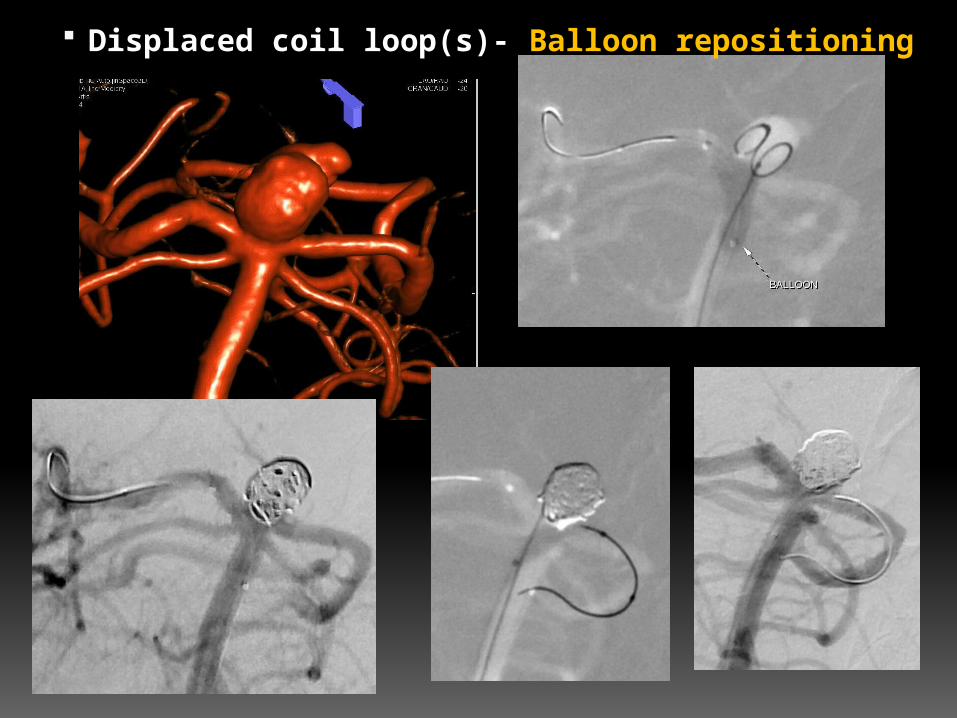
Displaced coil loop(s)- Balloon repositioning



Balloon assisted coiling Extremely versatile technique Almost essential in treating
difficult ruptured aneurysms Modern balloons – easier, better Overall doesn't increase
complication rate Stent when needed Personal balance

Complications
? Higher thromboembolism, rupture - van Rooij at al AJNR 2006
Review of literature Shapiro M et al, AJNR 2008
No significant difference in thrombo-embolism and rupture rate
Better occlusion rate Improvement in technology

Thank you ….
For more information on:STROKE & NEUROVASCULAR INTERVENTIONS:
URL:www.sanif.co.in
Facebook:https://www.facebook.com/strokeawarenessindiahttps://www.facebook.com/vipul.gupta.35175
Twitterhttps://twitter.com/drvipulgupta25
LinkedINhttps://in.linkedin.com/pub/dr-vipul-gupta/51/8a1/25a
YouTubeChannel: Stroke & Neurovascular Interventionswww.youtube.com/c/StrokeNeurovascularInterventionsfoundation
Dr Vipul Gupta