Balance Assessment in the Management of Sport-Related ... Assessment.… · Balance Assessment in...
14
Balance Assessment in the Management of Sport-Related Concussion Kevin M. Guskiewicz, PhD, ATC Over the past decade, there is probably no sports injury more discussed in the lay media than concussion or traumatic brain injury (TBI). There has also been a flood of publications into the peer-reviewed medical literature on the topic in recent years, and the medical community has a better understanding of concussive injury today than it did just 10 years ago. Clinicians, especially those responsible for the medical care of elite athletes, have been placed under the microscope and are being scruti- nized for their management of these potentially catastrophic injuries. Concussion often presents with varying symptomatology and most experts think it should be eval- uated using a multifactorial approach. 1–4 Yet many clinicians neglect the use of a comprehensive concussion assessment plan, 5 despite the complexity of this injury. Given that athletes may under-report concussions by nearly 50%, 6 significant atten- tion has been given to the validation of objective measures for managing concussion. Although neuropsychological testing has proven to be a valuable tool in concussion management, it is most useful when administered as part of a comprehensive assess- ment battery that includes grading of symptoms and clinical balance tests. 2,4,7,8 A thorough sideline and clinical examination by the certified athletic trainer and team physician is considered an important first step in the management of concussion. It is best if the clinician performing the examination knows the athlete well enough to detect changes in their disposition. The evaluation, whether on the field or in the clin- ical setting, should be conducted in a systematic manner. The evaluation should include obtaining a history for specific details about the injury (eg, mechanism, symp- tomatology, concussion history), followed by assessing neurocognitive function and balance, which is the focus of this article. The objective measures from balance testing The author has nothing to disclose. Matthew Alan Gfeller Sport-Related Traumatic Brain Injury Research Center, Department of Exercise and Sport Science, University of North Carolina at Chapel Hill, 209 Fetzer Hall, CB#8700, Chapel Hill, NC 27599-8700, USA E-mail address: [email protected] KEYWORDS Postural stability Equilibrium Clinical assessment Traumatic brain injury Clin Sports Med 30 (2011) 89–102 doi:10.1016/j.csm.2010.09.004 sportsmed.theclinics.com 0278-5919/11/$ – see front matter Ó 2011 Elsevier Inc. All rights reserved.
Transcript of Balance Assessment in the Management of Sport-Related ... Assessment.… · Balance Assessment in...

Balance Assessmentin the Managementof Sport-RelatedConcussion
Kevin M. Guskiewicz, PhD, ATC
KEYWORDS
� Postural stability � Equilibrium � Clinical assessment� Traumatic brain injury
Over the past decade, there is probably no sports injury more discussed in the laymedia than concussion or traumatic brain injury (TBI). There has also been a floodof publications into the peer-reviewed medical literature on the topic in recent years,and the medical community has a better understanding of concussive injury todaythan it did just 10 years ago. Clinicians, especially those responsible for the medicalcare of elite athletes, have been placed under the microscope and are being scruti-nized for their management of these potentially catastrophic injuries. Concussionoften presents with varying symptomatology and most experts think it should be eval-uated using a multifactorial approach.1–4 Yet many clinicians neglect the use ofa comprehensive concussion assessment plan,5 despite the complexity of this injury.Given that athletes may under-report concussions by nearly 50%,6 significant atten-tion has been given to the validation of objective measures for managing concussion.Although neuropsychological testing has proven to be a valuable tool in concussionmanagement, it is most useful when administered as part of a comprehensive assess-ment battery that includes grading of symptoms and clinical balance tests.2,4,7,8
A thorough sideline and clinical examination by the certified athletic trainer and teamphysician is considered an important first step in the management of concussion. It isbest if the clinician performing the examination knows the athlete well enough todetect changes in their disposition. The evaluation, whether on the field or in the clin-ical setting, should be conducted in a systematic manner. The evaluation shouldinclude obtaining a history for specific details about the injury (eg, mechanism, symp-tomatology, concussion history), followed by assessing neurocognitive function andbalance, which is the focus of this article. The objective measures from balance testing
The author has nothing to disclose.Matthew Alan Gfeller Sport-Related Traumatic Brain Injury Research Center, Department ofExercise and Sport Science, University of North Carolina at Chapel Hill, 209 Fetzer Hall,CB#8700, Chapel Hill, NC 27599-8700, USAE-mail address: [email protected]
Clin Sports Med 30 (2011) 89–102doi:10.1016/j.csm.2010.09.004 sportsmed.theclinics.com0278-5919/11/$ – see front matter � 2011 Elsevier Inc. All rights reserved.

Guskiewicz90
can provide clinicians with an additional piece of the concussion puzzle, remove someof the guesswork in uncovering less obvious symptoms, and assist in determiningreadiness to return safely to participation.For many years, neurologic examination in the athletic setting has included Rom-
berg’s tests of balance/postural stability. However, the standard Romberg test lacksobjectivity and sensitivity for evaluating concussion, especially in elite athletes whotend to normally excel with activities of coordination and agility. Recent technologicaldevelopments have provided the sports medicine community with more quantitativeand objective assessment tools for evaluating head injuries. A review of the balanceliterature indicates there are characteristic deficits following traumatic brain injury,even those classified as mild traumatic brain injury (mTBI) or cerebral concussion.
ROLE OF THE CENTRAL NERVOUS SYSTEM IN MAINTAINING POSTURAL EQUILIBRIUM
Understanding the central nervous system’s (CNS) feedback mechanism for maintain-ing postural equilibrium is the first step in building a case for objective balance testingin the management of sport concussion. Maintaining equilibrium requires the CNS toprocess and integrate afferent information from the visual, somatosensory (proprio-ceptive), and vestibular systems to execute appropriate and coordinated musculo-skeletal responses. Feedback, obtained from sensors housed within the 3 systems,sends commands to the muscles of the extremities, which then generate an appro-priate contraction to maintain postural stability.9–13
The primary purposes of the human vestibular system are to (1) maintain the eyesfixed on a stationary target in the presence of head and body movement and (2) main-tain balance in conjunction with additional information from visual and somatosensoryinputs. To accomplish the first, the semicircular canals of the vestibular labyrinth senseangular acceleration of the head, converting it to velocity information, and sending itthrough the vestibuloocular reflex pathways to the ocular muscles. Secondly, balanceis maintained by central integration of vestibular, visual, and somatosensory orienta-tion information. The vestibular system provides angular information from the semicir-cular canals and linear acceleration information (including gravity) from the utricles andsaccules of the inner ear and transmits it via the vestibulospinal spinal tract to thespinal and lower extremity muscles. Under normal conditions, visual and somatosen-sory information is adequate for maintenance of balance. However, in populations withknown vestibular deficits, the inner ear senses of balance are essential when visualand somatosensory inputs are disrupted or provide conflicting information.13,14
Balance Control
Balance plays a vital role in the maintenance of fluid, dynamic movement common insport, and is defined as the process of maintaining the center of gravity (COG) withinthe body’s base of support. Many factors enter into the task of controlling balancewithin this designated area. The system involves a complex network of neural connec-tions and centers that are related by peripheral and central feedback mechanisms. Ahierarchy integrating the cerebral cortex, cerebellum, basal ganglia, brainstem, andspinal cord is primarily responsible for controlling voluntary movements.14,15
The highest level of the hierarchy involves areas of the brain responsible for atten-tion, concentration, memory and emotion, as well as the association cortex forreceiving and correlating input from other brain structures. The middle level involvesthe sensorimotor cortex, cerebellum, parts of the basal ganglia, and some brainstemnuclei. The cerebellum is likely the most important structure for coordinating andcontrolling balance, as it receives information from the muscles, joints, skin, eyes,
Management of Sport-Related Concussion 91
ears, and even the viscera.14,15 The afferent pathways of the reflex arcs come from 3sources: the eyes, the vestibular apparatus, and the proprioceptors. Their collectiveactions are referred to as postural reflexes. The efferent pathways are the alpha motorneurons to the skeletal muscles, and the integrating centers are neuron networks inthe brainstem and spinal cord.11,14 The lowest level of the hierarchy involves the brain-stem and the spinal cord from which the motor neurons exit. These structures receiveinformation from the middle level via the descending pathways. Its function is tospecify the tension of particular muscles and the angle of joints necessary to carryout the programs transmitted from the middle level.
Isolation of Sensory Input
From our knowledge of the central nervous system’s involvement in maintainingupright posture, we can divide the processes into 2 components. The term sensoryorganization involves those processes that determine timing, direction, and amplitudeof corrective postural actions based upon information obtained from the vestibular,visual, and somatosensory inputs. This concept is important for understandingsome of the concussion assessment techniques described later, such as the SensoryOrganization Test (SOT; NeuroCom International, Inc, Clackamas, OR, USA). Despitethe availability of multiple sensory inputs, the central nervous system generally relieson only one sense at a time for orientation information. For healthy adults, thepreferred sense for balance control comes from somatosensory information (ie, feetin contact with the support surface).13
The second component, muscle coordination, describes processes that determinethe temporal sequencing and distribution of contractile activity among the musclesof the legs and trunk that generate supportive reactions for maintaining balance.Balance deficiencies in people with neurologic problems can result from inappropriateinteraction among the 3 sensory inputs that provide orientation information to thepostural control system. Patients may be inappropriately dependent on one sensefor situations presenting intersensory conflict.11,13,16
Several studies have attempted to isolate and clarify which sensory inputs are mostinvolved with regulating posture and how the interaction among these inputs affectspostural control.16–22 A technique described by Shumway-Cook and Horak11 andIngersoll and Armstrong23 called the Clinical Test of Sensory Interaction and Balance(CTSIB) was originally used to systematically remove or conflict sensory input from 1or more of the 3 senses. The technique used combinations of 3 visual and 2 support-surface conditions during assessment of postural sway to identify any reliance on 1 ormore of the 3 senses for postural control, which was thought to be present for certainpathologic conditions, including TBI.23
BALANCE DEFICITS FOLLOWING TBI
Disruption of static and dynamic balance in nonathletic populations has been identi-fied and described following pathologic conditions, such as moderate-severe trau-matic brain injury,23–31 hemiplegia and craniocerebral injury,32 cerebellar atrophyand ataxia,33 and whiplash.25,34 It is thought that communication between the 3sensory systems is lost in many of these individuals, causing moderate to severepostural instability in either the anterior-posterior direction, medial-lateral direction,or both. In most cases symptoms with visual, vestibular, or somatosensory orienta-tion, such as dizziness, vertigo, tinnitus, lightheadedness, blurred vision, or photo-phobia, are reported.23–34 These deficits may be either temporary or permanent,depending on the structures involved and the severity of the injury.

Guskiewicz92
The Genesis?
Occasionally, we witness the woozily looking football player or hockey player who hasjust been hit trying to find his way back to the huddle, sideline, or bench. More likely,however, we hear of the subtle and less obvious balance problems a concussedathlete might complain of during the follow-up clinic evaluation. The author’s 2000study of 1003 sport-related concussions, found that balance problems are present30% of the time following concussive injury, trailing only headache, dizziness, confu-sion, disorientation, and blurred vision in frequency of occurrence among a list of 18symptoms (Fig. 1).35 So what might explain this disruption in balance following TBI,be it mild, moderate, or severe? In the case of cerebral concussion and mTBI, weknow that the injury produces functional rather than structural neurophysiologicchanges in the cortex and brainstem’s reticular formation.36 The latter disturbancein particular is presumed to account for the autonomic, motor, and postural impair-ments that occur in many individuals following TBI.23,36 Subtle vestibular deficitscaused by sensory integration disruption identified in the nonathlete mTBI popula-tion25 also occurs in sport-related concussion (see later discussion).The transient nature of most cerebral concussion symptoms and impairments
suggests that like a headache, blurred vision, or memory problems, balance deficits(when they exists) should resolve quickly. Several longitudinal studies involving highschool and college athletes have demonstrated a typical pattern of recovery usingboth high-technology (computerized dynamic posturography) and low-technology(clinical balance) methods. In the sports medicine setting, similar balance deficitshave been identified, but fortunately have been shown to resolve within 3 to 10days after injury.4,7,37–43 High-technology and low-technology balance assessmenttools have been validated for assessing the initial deficits and tracking recoveryfollowing concussive injury.
HIGH-TECHNOLOGY BALANCE ASSESSMENT FOLLOWING SPORT-RELATEDCONCUSSION
Studies of postural stability and balance following concussion have used a variety ofmethodologies and metrics. For example, in one of the earliest studies assessingbalance deficits in concussed athletes, the author used a modified CTSIB on a forceplate to systematically remove or conflict sensory inputs.37 The author recorded
0102030405060708090
100
cadaeH
he
Dzziine
ss noisufnoCD
tatneirosi
ion
lBruer d V is
noi
evitisoP
grebmoR A
senmia niaP kceN
aFgitue
egatnecreP
Fig. 1. Percentage of total injured athletes experiencing signs and symptoms associatedwith concussion. Positive Romberg test represents balance problems. (Reprinted from Gus-kiewicz KM, Weaver NL, Padua DA, et al. Epidemiology of concussion in collegiate andhigh school football players. Am J Sports Med 2000;28(5):643–50; with permission.)

Management of Sport-Related Concussion 93
2 indices of center of pressure displacement about a fixed, central reference point toquantify impairments in postural stability in college and high school athletes with cere-bral concussion. Concussed subjects, matched to healthy comparison controls,demonstrated decreased postural stability compared with their own baseline scoresand to their matched controls during the initial 3 days after injury. The degree ofbalance impairment in the concussed subjects increased with increasing taskdemands, such as altering the visual, vestibular, or somatosensory feedback duringthe trial. The author attributed the overall balance deficits to a sensory interactionproblem (ie, difficulty using various combinations of somatosensory, visual, andvestibular information) for controlling upright posture during the first few daysfollowing concussion.More recently, the SOT has been used to assess balance following concus-
sion.7,38–44 The SOT technical force plate system is designed to systematically disruptthe sensory selection process by altering the orientation information available to thesomatosensory or visual inputs while at the same time measuring the patients’ abilityto maintain a quiet stance. Sway referencing is used throughout the test because themovement of the platform beneath the patients’ feet and the environmental surroundmove in response to the athlete’s anterior-posterior (A-P) sway. The SOT uses 6different conditions; each condition is performed 3 times to assess balance (Fig. 2).The test protocol consists of 3 20-second trials under 3 different visual conditions(eyes open, eyes closed, sway referenced) and 2 different surface conditions (fixed,sway referenced) (see Fig. 2). Patients are asked to stand as motionless as possiblefor each of the 20-second trials in a normal stance with the feet shoulder width apart.The term sway referencing involves the tilting of the support surface or visual surround
Fig. 2. Six testing conditions (1–6) for the Sensory Organization Test used with the Neuro-Com Smart Balance Master.

Guskiewicz94
to directly follow the athlete’s COG sway. During sway reference support surfaceconditions (4–6), the force plate tilts synchronously with the patients’ A-P COGsway. Similarly, during sway referenced visual surround conditions (3, 6), the visualsurround tilts synchronously with A-P COG sway. Sway referencing causes orientationof the support surface or surround to remain constant relative to body position. TheSOT can assess patients’ ability to ignore the inaccurate information from the swayreferenced senses.An overall composite equilibrium score describing a person’s overall level of perfor-
mance during all of the trials in the SOT is calculated, with higher scores being indic-ative of better balance performance. The composite score is the average of thefollowing 14 scores: the condition 1 average score, the condition 2 average score,and the 3 equilibrium scores from each of the trials in conditions 3 to 6. The equilibriumscores from each of the trials represent a nondimensional percentage comparing thepatients’ peak amplitude of anterior-posterior sway to the theoretical anterior-poste-rior limit of stability. Additionally, relative differences between the equilibrium scores ofvarious conditions are calculated using ratios to reveal specific information about eachof the sensory systems involved with maintaining balance. For example, a vestibularratio is computed by using scores attained in condition 5 (eyes closed, sway refer-enced platform) and condition 1 (eyes open, fixed platform). This ratio indicates therelative reduction in postural stability when visual and somatosensory inputs aresimultaneously disrupted. Condition 4:Condition 1 represents the visual ratio, andCondition 2:Condition 1 represents the somatosensory ratio. These ratios are usefulin identifying sensory integration problems.Results of several studies using the SOT in concussed athletes have identified
sensory interaction and balance deficits that typically resolve within 3 to 5 days afterinjury.7,38–41 Cavanaugh and colleagues,42,43 concluded that when applying approxi-mate entropy techniques to the SOT data, athletes balance deficits can be shown topersist longer than 3 to 4 days, even among athletes with no signs of unsteadiness onthe standard SOT analysis. The investigators concluded that approximate entropyprovides a theoretically distinct, valuable measurement alternative that appears toprovide unique insights and may prove useful for reducing uncertainty in the return-to-play decision.In general, these studies indicate that the regions of the brain responsible for coor-
dinating the sensory modalities (thalamus and its interconnective pathways to thecerebral cortex) may be initially disrupted following concussive injury. These studiesalso suggest that the sensory system most often affected following concussion isthe vestibular system (Fig. 3).7 If a person has difficulty balancing under conditionsin which sensory systems have been altered, it can be hypothesized that they areunable to ignore altered environmental conditions and therefore select a motorresponse based on the altered environmental cues, which could potentially predis-pose them to further injury should they return to participation while experiencingsensory interaction problems.There are 2 possible mechanisms for vestibular dysfunction following cerebral
concussion: (1) the peripheral receptors themselves may be damaged and provideinaccurate senses of motion or (2) the brain centers responsible for central integrationof vestibular, visual, and somatosensory information may be impaired. Mallinson andLongridge25 found evidence of central integration balance deficits and subtle periph-eral vestibular deficits when comparing SOT and electronystagmography results insubjects with mild head injury from an associated whiplash injury. These findingssuggest that various combinations of peripheral and central deficits may be the causeof balance deficits in athletes with concussion. An additional factor that surfaced from

SOT Composite Score
60
65
70
75
80
85
90
BL Day 1 Day 3 Day 5
Postinjury Day
er
oc
Se
ti
so
pm
oC
InjuredControl
*
+
* *
* Significant group difference+ Significant difference from baseline (p<.05)
SOT Vestibular Ratio
0.4
0.5
0.6
0.7
0.8
0.9
1
BL Day 1 Day 3 Day 5
Postinjury Day
oit
aR
InjuredControl
** *
+
* Significant group difference+ Significant difference from baseline (p<.05)
Fig. 3. Composite Score means (top) and vestibular ratio means (bottom) on the NeuroComSmart Balance Master for 36 concussed and 36 control subjects across test sessions(Preseason through day 5 after injury). Higher scores represent better performance. (FromGuskiewicz KM, Ross SE, Marshall SW. Postural stability and neuropsychological deficits afterconcussion in collegiate athletes. J Athl Train 2001;36:263–73; with permission.)
Management of Sport-Related Concussion 95
the author’s research is the possibility that concentration and attention impairmentsidentified on day 1 after injury could be a contributing factor to decreased posturalstability. Future research should focus on this potential relationship.Both the modified CTSIB and SOT require sophisticated force plate systems that
provide a way to challenge and alter information sent to the various sensory systems.Although the aforementioned studies suggest that force platform sway measuresprovide valuable information in making return to play decisions following concussion,there is still a question of practicality and accessibility for the sports medicine clinician.
LOW-TECHNOLOGY (CLINICAL) BALANCE ASSESSMENT FOLLOWING SPORT-RELATEDCONCUSSION
In an attempt to provide a more cost-effective, yet quantifiable method of assessingbalance in athletes, the Balance Error Scoring System (BESS) was developed byresearchers at the University of North Carolina at Chapel Hill. This clinical balancetest can be performed on the sideline, with the use of only a stopwatch and a pieceof medium-density foam (Power Systems Airex Balance Pad 81,000, Knoxville, TN,USA). Testing involves 3 different stances (double, single, and tandem) completedtwice, once while on a firm surface and once on the foam, for a total of 6 trials(Fig. 4). Athletes are asked to assume the required stance by placing their hands on

Fig. 4. Balance Error Scoring System performed on firm surface (A–C) and foam surface(D–F).
Guskiewicz96
the iliac crests and upon eye closure, the 20-second test begins. During the single legstances, subjects are asked to maintain the contralateral limb in 20� to 30� of hipflexion and 40� to 50� of knee flexion. Additionally, the athlete is asked to stand quietlyand as motionless as possible in the stance position, keeping their hands on the iliaccrests and eyes closed. The single-limb stance tests are performed on the nondomi-nant foot. This same foot is placed toward the rear on the tandem stances. Patients aretold that upon losing their balance, they are to make any necessary adjustments andreturn to the testing position as quickly as possible. Performance is scored by adding1 error point for each error committed (Box 1). Trials are considered to be incomplete ifthe athlete is unable to sustain the stance position for longer than 5 seconds during theentire 20-second testing period. These trials are assigned a standard maximum errorscore of 10.

Box 1
Balance error scoring system
Errors
Hands lifted off iliac crests
Opening eyes
Step, stumble, or fall
Moving hip into more than 30� of flexion or abduction
Lifting forefoot or heel
Remaining out of testing position for more than 5 seconds
The BESS score is calculated by adding 1 error point for each error committed during each ofthe 6 (20 seconds) trials.
Management of Sport-Related Concussion 97
The BESS, which has been described as a rapid, easy-to-administer, and inexpen-sive clinical balance test, has identified postconcussion deficits in severalstudies.2,4,7,40,45 McCrea and colleagues4 reported that BESS scores in concussedcollege football players changed from baseline on average by 5.7 points, whenmeasured immediately following the game or practice in which the injury occurred.Notably, however, at 1 day after injury, their average BESS score was only 2.7 pointsgreater than baseline. For most athletes, BESS performance returned to preseasonbaseline levels (average 12 errors) by 3 to 7 days after injury. In a large study of Amer-ican collegiate football players, impairment on the BESS was seen in 36% of injuredsubjects immediately following concussion, compared with 5% of the control group.A total of 24% of injured subjects remained impaired on the BESS at 2 days afterinjury, compared with 9% by day 7 after injury. Sensitivity values for the BESS werehighest at the time of injury (sensitivity 0.34). Specificity values for this instrumentranged from 0.91 to 0.96 across postinjury days 1 to 7.2
Significant correlations between the BESS and force platform sway measures withnormal subjects have been established for 4 static balance tests (single-leg stance/firm surface, tandem stance/firm surface, double-leg stance/foam surface, single-leg stance/foam surface, and tandem stance/foam surface), with inter-rater reliabilityintraclass correlation coefficients ranging from 0.78 to 0.96.46 Researchers havereported that BESS performance can be influenced by a number of factors, includingthe type of sport played,47 a history of ankle injuries and ankle instability,48 and exer-tion and fatigue.49,50 Healthy athletes typically demonstrate a subtle learning (ie, prac-tice) effect on the BESS when it is administered over brief retest intervals,51,52 whichshould be considered when interpreting postinjury results during serial testing, andfactoring in a practice effect if the test is being administered multiple times over a shortperiod of time.In comparison to the SOT scores on 36 concussed athletes previously mentioned
(see Fig. 3), the BESS revealed a similar recovery curve (Fig. 5) when administeredon the same day as the SOT.7 Furthermore, the BESS is sensitive to the effects ofconcussion with and without the use of other brief screening instruments, such asa graded symptom checklist and the Standardized Assessment of Concussion(SAC).2 However, when used in combination with a graded symptom checklist andthe SAC, the BESS is more sensitive and specific for accurately classifying injuredand noninjured athletes during the acute postinjury phase.2,4
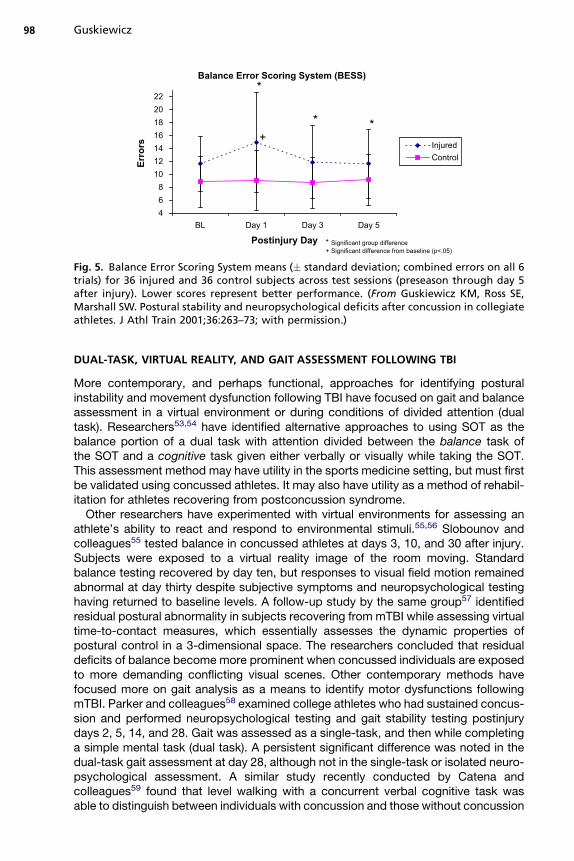
Balance Error Scoring System (BESS)
468
10121416182022
BL Day 1 Day 3 Day 5
Postinjury Day
sr
or
rE
InjuredControl
*
* *+
* Significant group difference+ Significant difference from baseline (p<.05)
Fig. 5. Balance Error Scoring System means (� standard deviation; combined errors on all 6trials) for 36 injured and 36 control subjects across test sessions (preseason through day 5after injury). Lower scores represent better performance. (From Guskiewicz KM, Ross SE,Marshall SW. Postural stability and neuropsychological deficits after concussion in collegiateathletes. J Athl Train 2001;36:263–73; with permission.)
Guskiewicz98
DUAL-TASK, VIRTUAL REALITY, AND GAIT ASSESSMENT FOLLOWING TBI
More contemporary, and perhaps functional, approaches for identifying posturalinstability and movement dysfunction following TBI have focused on gait and balanceassessment in a virtual environment or during conditions of divided attention (dualtask). Researchers53,54 have identified alternative approaches to using SOT as thebalance portion of a dual task with attention divided between the balance task ofthe SOT and a cognitive task given either verbally or visually while taking the SOT.This assessment method may have utility in the sports medicine setting, but must firstbe validated using concussed athletes. It may also have utility as a method of rehabil-itation for athletes recovering from postconcussion syndrome.Other researchers have experimented with virtual environments for assessing an
athlete’s ability to react and respond to environmental stimuli.55,56 Slobounov andcolleagues55 tested balance in concussed athletes at days 3, 10, and 30 after injury.Subjects were exposed to a virtual reality image of the room moving. Standardbalance testing recovered by day ten, but responses to visual field motion remainedabnormal at day thirty despite subjective symptoms and neuropsychological testinghaving returned to baseline levels. A follow-up study by the same group57 identifiedresidual postural abnormality in subjects recovering from mTBI while assessing virtualtime-to-contact measures, which essentially assesses the dynamic properties ofpostural control in a 3-dimensional space. The researchers concluded that residualdeficits of balance become more prominent when concussed individuals are exposedto more demanding conflicting visual scenes. Other contemporary methods havefocused more on gait analysis as a means to identify motor dysfunctions followingmTBI. Parker and colleagues58 examined college athletes who had sustained concus-sion and performed neuropsychological testing and gait stability testing postinjurydays 2, 5, 14, and 28. Gait was assessed as a single-task, and then while completinga simple mental task (dual task). A persistent significant difference was noted in thedual-task gait assessment at day 28, although not in the single-task or isolated neuro-psychological assessment. A similar study recently conducted by Catena andcolleagues59 found that level walking with a concurrent verbal cognitive task wasable to distinguish between individuals with concussion and those without concussion

Management of Sport-Related Concussion 99
immediately following concussive injury. The concussed individuals walked moreslowly and more conservatively (reduced sagittal plan movement of body’s centerof mass). By day 6 after injury, attention had recovered to the point at which thedivided task was no longer effective in perturbing balance in those with concussion,and it appeared that the concussed subjects had recovered. By day 14 after injury,a more conservative control of mediolateral center of mass was observed in the con-cussed group during a more challenging task involving obstacle crossing. The authorsconcluded that although this work was preliminary, the information someday couldlead to clinically executable dynamic balance control tests after concussion.In summary, preliminary findings involving contemporary assessment techniques
suggest that in challenging cases, difficult tasks combining divided attention andmotor challenges may be more sensitive for identifying deficits in otherwise healthyactive athletes. The clinical significance of altered response to virtual reality environ-ments or dual-task gait assessments is intriguing. However, their clinical utility hasyet to be established. These dual-task paradigms may also be useful in developingrehabilitation programs for athletes recovering from postconcussion syndrome.
SUMMARY
Balance assessment, whether through the use of a force plate or a clinical balancetest, such as the BESS, is useful in identifying neurologic impairment in athletesfollowing concussion. In many cases, this impairment lasts only a few days after injury;however, in a small number of cases in which there are lingering vestibular issues, thedeficits can last significantly longer. In such cases, balance/vestibular training may beindicated for assuring a full return to activity for the athlete. Clinicians should realizethat balance is only one small piece of a large puzzle in the assessment of concussionand may not be affected in every concussed athlete. With repeated testing, there isa subtle practice effect with both the BESS and SOT, so the absence of this improve-ment in concussed athletes should be considered in the interpretation.Many of the concussion management consensus statements used by sports medi-
cine clinicians recommend the inclusion of objective balance assessment as part ofa comprehensive injury evaluation and follow-up. The new “Zurich Guidelines,” whichresulted from the Third International Conference on Concussion in Sport,1 include, aspart of its standardized concussion assessment tool (SCAT2), a systematic balanceassessment similar to that of the BESS. The SCAT2 uses the first 3 trials (firm condi-tions) of the BESS, and errors are recorded in the same way. It is recommended thatwhenever possible, the BESS, in its entirety (including the foam conditions), becompleted for assessing clinical balance of concussed athletes. To ensure best useand interpretation of the BESS or any other metric of postural stability for clinicalmanagement of concussion, postinjury scores should be compared with a preseasonbaseline score. Finally, it is important to recognize that although symptom severity,neurocognitive function, and postural stability are often affected initially followingconcussion, they are not necessarily related or even affected to the same degree.Thus, a comprehensive concussion assessment plan includes assessment of all thesedomains.
REFERENCES
1. McCrory H, Meeuwisse W, Johnson K, et al. Consensus statement on concussionin sport: the 3rd international conference on concussion in sport held in Zurich,November 2008. Br J Sports Med 2009;43:76–84.

Guskiewicz100
2. McCrea M, Barr WB, Guskiewicz K, et al. Standard regression-based methods formeasuring recovery after sport-related concussion. J Int Neuropsychol Soc 2005;11:58–69.
3. Guskiewicz KM, Bruce SL, Cantu RC, et al. National athletic trainers’ associationposition statement: management of sport-related concussion. J Athl Train 2004;39:280–97.
4. McCrea M, Guskiewicz KM, Marshall SW, et al. Acute effects and recovery timefollowing concussion in collegiate football players: the NCAA concussion study.JAMA 2003;290:2556–63.
5. Notebaert AJ, Guskiewicz KM. Current trends in athletic training practice forconcussion assessment and management. J Athl Train 2005;40:320–5.
6. McCrea M, Hammeke T, Olsen G, et al. Unreported concussion in high schoolfootball players. Clin J Sport Med 2004;14(1):13–7.
7. Guskiewicz KM, Ross SE, Marshall SW. Postural stability and neuropsychologicaldeficits after concussion in collegiate athletes. J Athl Train 2001;36:263–73.
8. Guskiewicz KM. Postural stability assessment following concussion: one piece ofthe puzzle. Clin J Sport Med 2001;11:182–9.
9. Hellebrant F, Braun G. The influence of sex and age on the postural sway of man.Am J Phys Anthropol 1939;24:347–59.
10. Sugano H, Takeya T. Measurement of body movement and its clinical applica-tions. Jpn J Physiol 1970;20:296–308.
11. Shumway-Cook A, Horak F. Assessing the influence of sensory interaction onbalance. Phys Ther 1986;66:1548–50.
12. Jansen E, Larsen R, Mogens B. Quantitative romberg’s test: measurement &computer calculations of postural stability. Acta Neurol Scand 1982;66:93–9.
13. Nashner L. Adaptation of human movement to altered environments. Trends Neu-rosci 1982;5:358–61.
14. Guyton A. Textbook of medical physiology. Philadelphia: WB Saunders Co; 1986.p. 1610–5.
15. Vander A, Sherman J, Luciano D. Human physiology: the mechanisms of bodyfunction. 5th edition. New York: McGraw-Hill, Inc; 1990.
16. Nashner L, Black F, Wall C. Adaptation to altered support and visual conditionsduring stance: patients with vestibular deficits. J Neurosci 1982;2:536–44.
17. Horstmann G, Dietz V. The contribution of vestibular input to the stabilizationof human posture: a new experimental approach. Neurosci Lett 1988;95:179–84.
18. Dietz V, Horstmann G, Berger W. Significance of proprioceptive mechanisms inthe regulation of stance. Prog Brain Res 1989;80:419–23.
19. Dornan J, Fernie G, Holliday P. Visual input: it’s importance in the control ofpostural sway. Arch Phys Med Rehabil 1918;59:586–91.
20. Nashner L, Berthoz A. Visual contribution to rapid motor responses duringpostural control. Brain Res 1978;150:403–7.
21. Diener H, Dichgans J, Guschlbauer B, et al. The significance of proprioception onpostural stabilization as assessed by ischemia. Brain Res 1984;296:103–9.
22. Norre M. Sensory interaction testing in platform posturography. J Laryngol Otol1993;107:496–501.
23. Ingersoll C, Armstrong C. The effects of closed-head injury on postural sway.Med Sci Sports Exerc 1992;24:739–42.
24. Geurts AC, Ribbers GM, Knoop JA, et al. Identification of static and dynamicpostural instability following traumatic brain injury. Arch Phys Med Rehabil1996;77:639–44.

Management of Sport-Related Concussion 101
25. Mallinson AI, Longridge NS. Dizziness from whiplash and head injury: differencesbetween whiplash and head injury. Am J Otol 1998;19(6):814–8.
26. Wober C, Oder W, Kollegger H, et al. Posturographic measurement of body swayin survivors of severe closed head injury. Arch Phys Med Rehabil 1993;74:1151–6.
27. Greenwald BD, Cifu DX, Marwitz JH, et al. Factors associated with balance defi-cits on admission to rehabilitation after traumatic brain injury: a multicenter anal-ysis. J Head Trauma Rehabil 2001;16:238–52.
28. Rinne MB, Pasanen ME, Vartiainen MV, et al. Motor performance in physicallywell-recovered men with traumatic brain injury. J Rehabil Med 2006;38:224–9.
29. Kaufman KR, Brey RH, Chou LS, et al. Comparison of subjective and objectivemeasurements of balance disorders following traumatic brain injury. Med EngPhys 2006;28:234–9.
30. Campbell M, Parry A. Balance disorder and traumatic brain injury: preliminaryfindings of a multi-factorial observational study. Brain Inj 2005;19:1095–104.
31. Gagnon I, Forget R, Sullivan SJ, et al. Motor performance following a mild trau-matic brain injury in children: an exploratory study. Brain Inj 1998;12:843–53.
32. Arcan M, Brull M, Najenson T, et al. FGP assessment of postural disorders duringthe process of rehabilitation. Scand J Rehabil Med 1977;9:165–8.
33. Mauritz K, Dichgans J, Hufschmidt A. Quantitative analysis of stance in latecortical cerebellar atrophy of the anterior lobe and other forms of cerebellarataxia. Brain 1979;102:461–82.
34. Rubin AM, Woolley SM, Dailey VM, et al. Postural stability following mild head orwhiplash injuries. Am J Otol 1995;16:216–21.
35. Guskiewicz KM, Weaver NL, Padua DA, et al. Epidemiology of concussion incollegiate and high school football players. Am J Sports Med 2000;28(5):643–50.
36. Shaw N. The neurophysiology of concussion. Prog Neurobiol 2002;67(4):281.37. Guskiewicz KM, Perrin DH, Gansneder BM. Effect of mild head injury on postural
stability in athletes. J Athl Train 1996;31(4):300–6.38. GuskiewiczKM,RiemannBL,PerrinDH, et al. Alternative approaches to theassess-
ment of mild head injury in athletes. Med Sci Sports Exerc 1997;29(Suppl 7):S213–21.
39. Mrazik M, Ferrara MS, Peterson CL, et al. Injury severity and neuropsychologicaland balance outcomes of four college athletes. Brain Inj 2000;14(10):921–31.
40. Riemann BL, Guskiewicz KM. Effects of mild head injury on postural stability asmeasured through clinical balance testing. J Athl Train 2000;35:19–25.
41. Peterson CL, Ferrara MS, Mrazik M, et al. Evaluation of neuropsychologicaldomain scores and postural stability following cerebral concussion in sports.Clin J Sport Med 2003;13:230–7.
42. Cavanaugh JT, Guskiewicz KM, Giuliani C, et al. Detecting altered posturalcontrol after cerebral concussion in athletes without postural instability. Br JSports Med 2005;39(11):805–11.
43. Cavanaugh JT, Guskiewicz KM, Stergiou N. A nonlinear dynamic approach forevaluating postural control: new directions of the management of sport-relatedcerebral concussion. Sports Med 2005;35(11):935–50.
44. Register-Mihalik JK, Mihalik JP, Guskiewicz KM. Balance deficits after sports-related concussion in individuals reporting posttraumatic headache. Neurosur-gery 2008;63:76–80 [discussion: 80–2].
45. Broglio SP, Puetz TW. The effect of sport concussion on neurocognitive function,self-report symptoms and postural control: a meta-analysis. Sports Med 2008;38:53–67.

Guskiewicz102
46. Riemann BL, Guskiewicz KM, Shields EW. Relationship between clinical andforce plate measures of postural stability. J Sport Rehabil 1999;8:71–82.
47. Bressel E, Yonker JC, Kras J, et al. Comparison of static and dynamic balance infemale collegiate soccer, basketball, and gymnastics athletes. J Athl Train 2007;42:42–6.
48. Docherty CL, Valovich McLeod TC, Shultz SJ. Postural control deficits in partici-pants with functional ankle instability as measured by the balance error scoringsystem. Clin J Sport Med 2006;16:203–8.
49. Susco TM, Valovich McLeod TC, Gansneder BM, et al. Balance recovers within20 minutes after exertion as measured by the balance error scoring system.J Athl Train 2004;39:241–6.
50. Wilkins JC, Valovich McLeod TC, Perrin DH, et al. Performance on the balanceerror scoring system decreases after fatigue. J Athl Train 2004;39:156–61.
51. Valovich McLeod TC, Perrin DH, Guskiewicz KM, et al. Serial administration ofclinical concussion assessments and learning effects in healthy young athletes.Clin J Sport Med 2004;14:287–95.
52. Valovich TC, Perrin DH, Gansneder BM. Repeat administration elicits a practiceeffect with the balance error scoring system but not with the standardizedassessment of concussion in high school athletes. J Athl Train 2003;38:51–6.
53. Broglio SP, Tomporowski PD, Ferrara MS. Balance performance with a cognitivetask: a dual-task testing paradigm. Med Sci Sports Exerc 2005;37:689–95.
54. Ross LM, Register-Mihalik JK, Mihalik JP, et al. Effects of a single task vs. a dualtask paradigm on cognition and balance in healthy subjects: a feasibility and reli-ability study. J Sport Rehabil, in press.
55. Slobounov S, Tutwiler R, Sebastianelli W, et al. Alteration of postural responses tovisual field motion in mild traumatic brain injury. Neurosurgery 2006;59:134–9[discussion: 134–9].
56. Mihalik JP, Kohli L, Whitton MC. Do the physical characteristics of a virtual realitydevice contraindicate its use for balance assessment? J Sport Rehabil 2008;17(1):38–49.
57. Slobounov S, Cao C, Sebastianelli W, et al. Residual deficits from concussion asrevealed by virtual time-to-contact measures of postural stability. Clin Neurophy-siol 2008;119:281–9.
58. Parker TM, Osternig LR, van Donkelaar P, et al. Recovery of cognitive anddynamic motor function following concussion. Br J Sports Med 2007;41:868–73[discussion: 873].
59. Catena RD, van Donkelaar P, Chou L. Different gait tasks distinguish immediatevs. long-term effects of concussion on balance control. J Neuroeng Rehabil2009;6:25.