Back to Basics: Substance Use/Abuse/Withdrawal Melanie Willows B.Sc. C.C.F.P. C.A.S.A.M. C.C.S.A.M....
73
Back to Basics: Substance Use/Abuse/Withdrawal Melanie Willows B.Sc. C.C.F.P. C.A.S.A.M. C.C.S.A.M. Clinical Director Substance Use and Concurrent Disorders Program The Royal Assistant Professor University of Ottawa
-
Upload
kristin-higgins -
Category
Documents
-
view
212 -
download
0
Transcript of Back to Basics: Substance Use/Abuse/Withdrawal Melanie Willows B.Sc. C.C.F.P. C.A.S.A.M. C.C.S.A.M....

Back to Basics: Substance Use/Abuse/WithdrawalMelanie Willows B.Sc. C.C.F.P. C.A.S.A.M. C.C.S.A.M.
Clinical Director Substance Use and Concurrent Disorders Program
The RoyalAssistant Professor University of Ottawa

LMCC Objectives
• Key Objectives– Given a patient with an addiction or a substance abuse
problem, be able to identify the issue, potential consequences and the need to provide immediate and continuing support and intervention.
– Given a patient with suspected substance withdrawal, the candidate will diagnose the cause, severity and complications, and will initiate an appropriate management plan.

LMCC Objectives
• Objectives• List and interpret critical investigations including history,
physical exam, drug and alcohol screening, risk of withdrawal, critical laboratory investigations
• Determine an effective initial management plan which may include brief intervention, supportive measures, safe environment, pharmacological interventions, or referral to specialized services

Addiction
• Addiction may be to substances or may be a process (behavioral) addiction.– Depressants: Alcohol, Opioids, Benzodiazepines– Stimulants: Cocaine, Amphetamines– Hallucinogens: Marijuana
– Process (behavioural): Gambling• Sex, Food, Internet (not in the DSM IV)

Addiction
• Reward pathway involves the nucleus accumbens, ventral tegmental area (VTA) and the prefrontal cortex
• Drugs of abuse act on the reward centre resulting in dopamine flooding ....brain either produces less dopamine or downregulates dopamine receptors...net result is lower baseline dopamine...need to take more drug to increase dopamine

Causal Factors/Risk Factors
• Individual: Genetics, Mental Health
• Exposure to drug or experience (gambling)
• Environmental: trauma, poverty, peers

Case
• Mary is a 43 year old woman. Her mother and father both had alcohol problems. Her home life was filled with fighting and chaos. She was sexually abused by her uncle and grandfather. Mary started using drugs and alcohol when she was 13. She was diagnosed with schizophrenia at the age of 25.

Taking a History
• What is the purpose of taking a drug and alcohol history?
• Answer:– To make a Diagnosis – Medical and psychosocial history will influence
management

DSM IV Criteria for Substance Dependence
• 3 or more occurring over 12 months– tolerance– withdrawal– larger amounts or longer period of time– unsuccessful efforts to cut down or control– time spent obtaining, using, recovering– activities given up or reduced– continued use despite problems

DSM IV Criteria for Substance Abuse• A. A maladaptive pattern of substance use leading to
clinically significant impairment or distress, as manifested by one (or more) of the following occurring within a 12 month period:1. recurrent substance use resulting in a failure to fulfill major obligations at work, school, or home2. recurrent substance use in situations in which it is physically hazardous3. recurrent substance-related legal problems4. continued use despite persistent or recurrent social or interpersonal problems caused by or exacerbated by effects of a substance
B. The symptoms have never met the criteria for substance dependence for this class of substance.

Taking a Drug and Alcohol History
History of Substance Use
• Past substance abuse treatment history: type of program, ?completed, attendance at AA or NA.
• Substances used: alcohol, marijuana, cocaine, heroin, tobacco, prescription/OTC drugs (opiates, benzodiazepines, gravol), ecstasy, crystal meth
• For each substance used: first use, current use, pattern of use, route, and last use

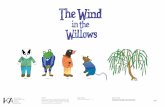
Quantifying Alcohol and Drug Use• Alcohol• One standard drink= 13.6 grams of alcohol
– 5 oz/142ml wine (12% alcohol)– 1.5 oz/43ml hard liquor (40% alcohol)– 12 oz/341 ml beer (5% alcohol)
• Hard Liquor: 1 bottle-13 oz. Mickey = 8 standard drinks-26 oz./750 ml = 17 standard drinks-40 oz./1.14L = 27 standard drinks
• Wine: 1 Bottle-26 oz./750ml = 5 standard drinks
• Beer: ask what size? 500ml, 710ml (=2 standard drinks)

One Standard Drink (equivalent to 13.6 grams of alcohol)
341 ml (12 oz.) bottle of 5% alcohol beer, cider or cooler
142 ml (5 oz.) glass of 12% alcohol wine
43 ml (1.5 oz.) serving of 40% distilled

Quantifying Alcohol and Drug Use
Marijuana• Measured in grams, 1 ounze equals 28 grams• How many grams? Pattern of use.
CocainePowder(snort or IV) or crack/freebase/rock form
(smoke)8 ball equals 3.5 grams; speedball is cocaine and
heroin

Quantifying Alcohol and Drug Use
Benzodiazepines• Total amount used per day, how many years taking
(assessing for risk of withdrawal)• Source of medication
OpioidsWhich opioid? Oxy, Dilaudid (hydromorph), Fentanyl,
morphine, codeine, heroinHow much? What route? (IV, smoked, snorted,
chewed, swallowed) How often?

Taking an Alcohol and Drug History
• Ask about blackouts, loss of control of use.• Withdrawal symptoms when stopping use: Alcohol
(shakes, seizures, DTs, hallucinations); Opioids ( nausea, vomiting, abdominal cramps, diarrhea, chills/hot flashes, myalgias/arthralgias, pilo-erection)
• Tolerance• Consequences of Using: health problems (physical,
mental), work or school problems, legal problems, involvement with CAS, effect on family/friends/children, financial problems.

Case 2
• Lisa started smoking marijuana and drinking alcohol when she was 13. She started using cocaine when she was 15. She currently smokes 2 grams of marijuana a day. Smokes crack cocaine 2-3 times per week usually a 40 piece. She drinks 6 tall beers (710ml) per day. Four years ago she was prescribed oxycodone for injuries she sustained when she was beaten up by a boyfriend. Within one month she was snorting 160mg daily and has now switched to smoking a 50ug fentanyl patch per day.

Taking a Drug and Alcohol History Family History• family history of alcohol or drug problems in blood relatives
(biggest risk factor for development of addiction)
Social History• marital status, current relationship, children• living arrangements, use of alcohol/drugs in the home• education level, current employment/disability• family of origin: marital status of parents, relationship with
parents and siblings, abusive environment
Legal History• past or current legal charges or convictions (DUI, assault,
theft, possession, trafficking etc.)

Taking a Drug and Alcohol History Past Psychiatric History• inpatient admissions, outpatient counseling, suicide
attempts• any diagnosis ever given: trauma, anxiety, depression • medications prescribed in past and present
Medical History• all medical problems and surgeries• HIV and Hepatitis C• accidents related to substance use
Medications• list of all current medications and dosing• ask about use/abuse of over the counter medication

Case 2
• Lisa is Hepatitis C positive. She lives in subsidized housing. She frequently uses with her next door neighbour who is addicted to crack cocaine. She has no family in town. She has two children who were taken from her care 15 years ago because of her drug use and mental health instability.

Screening Questionnaires
• CAGE• CRAFFT (adolescents)• AUDIT (Alcohol Use Disorders Identification Test)• DAST (The Drug Abuse Screening Test)

CAGE Questionnaire(Screening Questionnaire for Alcohol Disorders)
• Have you ever felt you should CUT DOWN on your drinking?
• Have people ANNOYED you by criticizing your drinking?
• Have you ever felt bad or GUILTY about your drinking?
• Have you ever had a drink first thing in the morning to steady your nerves or to get rid of a hangover (EYE-OPENER)
• Score of 2 or more indicates a problem• Sensitivity 75-85%

How do addiction issues present?
• Sometimes patients do not initially disclose that they have a substance problem
• It is sometimes only by reviewing their clinical presentation that we start to suspect they may have a substance problem

Potential Clinical Presentation of Alcohol and Drug Problems
• Cardiovascular: hypertension, cardiomyopathy• GI: fatty liver, hepatitis, cirrhosis, gastritis, pancreatitis,
dyspepsia, recurrent diarrhea• Neurological: ataxia, tremor, peripheral neuropathy,
cerebellar disease, dementia, Wernicke-Korsakoff’s syndrome
• Infections (injection drug use): cellulitis, abscess, Hepatitis C, endocarditis

Potential Clinical Presentation of Alcohol and Drug Problems
• Trauma: accidents, violence, suicide• Psychiatric: fatigue, insomnia, depression, anxiety,
psychosis• Behavioural: missed appointments, non-compliance,
drug-seeking• Social: deterioration in social functioning, spousal
abuse, violence, legal problems• Other: weight loss, loss of libido

Case 3
• John is a 53 year old man who has been drinking alcohol daily for 25 years. He is currently drinking 20 oz of hard liquor per day.
• He presents today with uncontrolled hypertension, complaints of insomnia, abdominal pain, diarrhea, anxiety, and depression.

Physical Examination in Cases of Suspected Alcohol or Drug Abuse/Dependence
• BP, heart rate, pupils• Level of consciousness, Mental Status Exam• Signs of liver disease (hepatomegaly, spider nevae,
jaundice, ascites)• Signs of withdrawal/intoxication• Injection marks and bruising in arms, wrists, legs,
ankles, neck, inguinal region• Long history of alcohol use (10+ years): hypertension,
cardiomyopathy, dementia, gait (cerebellar dysfunction), distal polyneuropathy

Case 3
• John comes to see you three years later after a recent hospitalization. You barely recognize him as he walks into your office with a walker. He is jaundiced, his face is very thin and his abdomen is distended.

Laboratory Investigations in Cases of Suspected Alcohol or Drug Abuse or Dependency
• CBC (increased MCV, decreased platelets), GGT (to detect heavy alcohol consumption)
• AST, ALT (to detect alcoholic or viral hepatitis)• Cirrhosis: INR, albumin, bilirubin• Urine drug screen• Hepatitis B, C, and HIV (ask permission first)

Case
• John has been diagnosed with cirrhosis and continues to drink. His MCV is elevated at 103(80-97). His platelets are depressed at 70(145-450). GGT is 342(<60). AST is 370(<37) and ALT is 240(<46).
• His INR is increased to 1.3, albumin is decreased at 24 (34-48) and her bilirubin is increased at 35(<23).

Urine Drug Testing Methods
• Immunoassay: Based on the principle of competitive binding. An antibody reacts to a portion of a drug or its metabolite. – Point of care testing possible– Not as specific
• Gas Chromotography with mass spectroscopy (GC/MS): couples the separation potential of gas chromatography with the precise detection and identification capability of mass spectroscopy.– More expensive– Gold Standard

Drug Minimum detection (hours) Maximum detection
Ethanol 0 to 4 <=6-12 hours
Benzodiazepines 2 to 7 Infrequent User- 3 daysChronic User- 4-6 weeks
Marijuana metabolite 6 to 18 Infrequent User – up to 10 daysChronic User – 30 days or longer
Cocaine metabolite 1 to 4 2 to 4 days
Amphetamines 2 to 7 2 to 4 days
Methamphatamine 1 to 3 2 to 4 days
MDMA (Ecstasy) 1 2 to 3 days
Opiates (codeine, morphine, heroin) 2 2 to 3 days
Oxycodone 1 1 to 2 days
Methadone 2 2 to 6 days


Treatment for Substance Use or Abuse
• Advise of concern and in the case of alcohol advise of low risk drinking guidelines
• Motivational interviewing to determine and set goals to reduce harm
• Follow up and monitoring for any progression to substance dependence (addiction)

Canada’s Low-Risk Alcohol Drinking Guidelines
• Women ≤ 10 drinks/week (≤ 2 drinks/day most days)• Men ≤ 15 drinks/week (≤ 3 drinks/day most days)
• In one sitting:• Women, no more than 3 drinks• Men, no more than 4 drinks
– Plan a few non drinking days each week to avoid developing a habit

PrecontemplationIncrease awareness of need to change
ContemplationMotivate and increase confidence
in ability to change
ActionReaffirm commitment
and follow-up
Termination
Stages of Change Model (Prochaska & Diclemente)
RelapseAssist in Coping
MaintenanceEncourage activeproblem-solving
PreparationNegotiate a plan

Motivational Interviewing
• Four General Principles1. Express Empathy
• Acceptance facilitates change 2. Develop Discrepancy
• Between behaviour and personal goals3. Roll with resistance
• Patient primary source for solutions 4. Support self-efficacy
• Patient responsible for choosing and carrying out change

FRAMES brief intervention interviewing technique• Feedback: specifically address concerns about use (i.e. I am
concerned about how alcohol is affecting your liver)• Responsibility: Emphasize that change is up to the patient.
(Only you can decide to make your life better)• Advice: Give specific goals you have for the patient (I want
you to be evaluated at a treatment center)• Menu: Offer alternatives to advice (You could alternatively go
to an AA meeting)• Empathy: I know you find talking about this difficult• Self-efficacy: you deserve better – you can be better with help

Treatment Decision Tree for Substance Dependence (Addiction)
Want to stop?
Is it safe to stop?
Can they
stop?
Yes
Yes
Motivational interviewing
No
Medically supervised detox Inpatient or outpatient
No
Community withdrawalOrResidential WithdrawalManagement level 2
No
Explore addiction treatment options
Yes

Case
• 54 year old man presents with diagnosis of alcohol dependence. Patient desperately wants to stop drinking but is afraid of the withdrawal. Patient has experienced 2 previous withdrawal seizures. Patient has hypertension, and coronary artery disease and has had 2 previous MI’s. Patient is drinking 26 oz. of alcohol per day, usually having his first drink at 5a.m. to take away the shakes.

Withdrawal Assessment Tools• Alcohol: CIWA (Nausea & Vomiting, Tactile
Disturbances, Tremor, Auditory Disturbances, Paroxysmal Sweating, Visual Disturbances, Anxiety, Headache/Fullness in the Head, Agitation, Orientation and Clouding of Sensorium
• Opioids: COWS: (Resting Heart Rate, Sweating, Restlessness, Pupil Size, Bone or Joint Aches, Nose Running or Tearing, GI upset, Tremor, Yawning, Anxiety or Irritability, Gooseflesh Skin)

Treatment of Withdrawal
• Alcohol
• Benzodiazepines
• Opioids
• Cannabis
• Amphetamines/Cocaine
• May be life-threatening• May require benzodiazepines• Inpatient or outpatient• Vitamin B1 (Thiamine)
• Requires tapering (weeks to months)
• Inpatient or outpatient
• Withdrawal not life-threatening but very distressing
• Likely will require supportive medications +/- opioids
• No medications required
• No medications required• Suicide Risk Assessment

Pharmacological Interventions
• Alcohol– Thiamine (B1) 100mg IM then po to prevent Wernicke-
Korsakoff– Diazepam, Chlorodiazepoxide: long acting for management
of withdrawal and prevention of seizures, DT’s– Lorazepam: short acting, used if respiratory or hepatic
compromised

Pharmacological Interventions• Antabuse (Disulfiram):
• binds irreversibly to aldehyde dehydrogenase • Daily dose of 250mg to 500mg• Must not drink alcohol within 7 days of taking• Common effects with drinking include: flushed face,
vomiting, headache, chest pain, palpitations. • Serious effects include: seizures, hypotension, vagally
induced dysrhythmias. • Contra-indications: unstable angina, recent MI,
schizophrenia and other psychotic states, pregnancy, severe cirrhosis of the liver
• Liver enzymes monitored at quarterly intervals, monitored for visual changes and symptoms of peripheral neuropathy

Pharmacological Interventions• Naltrexone (Revia)
– Competitive opioid antagonist– Usual dose 50mg po daily
• Indications: – alcohol dependence (reduce craving and intensity and frequency of
alcohol binges) and for– Opioid dependence(for those who wish to remain abstinent from all
opioids)• Side effects: nausea, GI symptoms, headache, dizziness, light-
headedness, weakness• Contra-indications: acute hepatitis, liver failure, opioids
should be discontinued 10 days prior to starting naltrexone, naltrexone should be discontinued 3 days prior to elective surgery
• Monitor ALT, AST and bilirubin

Pharmacological Interventions
• Campral (Acamprosate): – amino acid derivative that increases GABA and has
complex effects on excitatory amino acid (i.e. Glutamate) neurotransmission
– Positive and negative studies– Dosing 2 333mg tablets TID– Side effects: GI (diarrhea, bloating), pruritis– Excreted unmetabolized thorugh the kidney’s, must
evaluate renal function prior to initiations

Pharmacological Interventions
• Opioids– Dimenhydrinate (vomiting, nausea), Immodium (diarrhea),
ibuprofen (aches and pain), meds for insomnia– Clonidine: Alpha 2 Adrenergic agonist
• 0.05-0.2mg po TID prn • Most effective in suppressing autonomic signs and symptoms of
opioid withdrawal • warn of sedation and orthostatic hypotension • BP must be greater than 90/60 to take

Pharmacological Interventions
• Opioids– Methadone: long-acting (>24 hours) synthetic opioid
agonist, require methadone exemption to prescribe– Buprenorphine/Naloxone (Suboxone): long acting
synthetic partial opioid agonist, naloxone component present to prevent IV abuse
– Naloxone: opioid antagonist, used in opioid overdose kits

Pharmacological Interventions
• Nicotine– NRT (patch, gum, lozenge, inhaler)– Zyban (Wellbutrin, Bupropion)- not if seizure d/o– Champix (Varenicycline)-monitor for psych symptoms

Types of Treatment Options• Mutual Help Groups: Alcoholics Anonymous, Narcotics
Anonymous, Women for Sobriety, SMART recovery• Withdrawal Management• Outpatient Treatment (once weekly, daily)• Residential Treatment programs (ranging from 21 days to
9 months+)• Medically Supervised Treatment programs• Individual Counseling • Opioid Substitution Therapy• Harm Reduction approaches

References
• DSM IV Diagnostic & Statistical Manual of Mental Disorders 4th Ed. Test Revision 2000
• Substance Abuse: A Comprehensive Textbook 4th Ed. Lewinson et al. 2005
• Management of Alcohol, Tobacco, & Other Drug Problems, Edited by Bruno Brands Phd. Addiction Research Foundation 2000
• Principles of Addiction Medicine 4th ed. , American Society of Addiction Medicine. 2009

References
• NIDA National Institute on Drug Abuse• NIAAA National Institute on Alcohol Abuse and Alcoholism• Butt, P., Beirness, D., Cesa, F., Gliksman, L., Paradis, C., &
Stockwell, T. (2011). Alcohol and health in Canada: A summary of evidence and guidelines for low-risk drinking. Ottawa, ON: Canadian Centre on Substance Abuse.

Differentiating between substance dependence and substance abuseCriteria for substance abuse does not include
tolerance, withdrawal, or a pattern of compulsive use
Although not listed as a criterion item, CRAVING (a strong subjective drive to use the substance) is likely to be experienced by most individuals with substance dependence
High blood levels of the substance coupled with little evidence of intoxication suggests tolerance is likely

Differentiating between substance dependence and substance abuseCriteria for substance abuse does not include
tolerance, withdrawal, or a pattern of compulsive use
Although not listed as a criterion item, CRAVING (a strong subjective drive to use the substance) is likely to be experienced by most individuals with substance dependence
High blood levels of the substance coupled with little evidence of intoxication suggests tolerance is likely

Canadian Guidelines for Low Risk Drinking
1.Reduce your long-term health risks by drinking no more than:10 drinks a week for women, with no more than 2 drinks
a day most days15 drinks a week for men, with no more than 3 drinks a
day most days
Plan non-drinking days every week to avoid developing a habit.
2. Reduce your risk of injury and harm by drinking no more than 3 drinks (for women) and 4 drinks (for men) on any single occasion.

Canadian Guidelines for Low Risk Drinking
3. Do not drink when you are:• driving a vehicle or using machinery and tools• taking medicine or other drugs that interact with
alcohol• doing any kind of dangerous physical activity• living with mental or physical health problems• living with alcohol dependence• pregnant or planning to be pregnant• responsible for the safety of others• making important decisions

Canadian Guidelines for Low Risk Drinking
• 4. If you are pregnant, planning to become pregnant, or before breastfeeding, the safest choice is to drink no alcohol at all.
• 5. If you are a child or youth, you should delay drinking until your late teens. Talk with your parents about drinking. Alcohol can harm the way your brain and body develop. If you are drinking, plan ahead, follow local alcohol laws and stay within the limits outlined in Guideline 1.

Clinical Institute Withdrawal Assessment of Alcohol Scale, Revised (CIWA-Ar)
• Patient:__________________________ Date: ________________ Time: _______________ (24 hour clock, midnight = 00:00)
• Pulse or heart rate, taken for one minute:_________________________ Blood pressure:______
• NAUSEA AND VOMITING -- Ask "Do you feel sick to your• stomach? Have you vomited?" Observation.• 0 no nausea and no vomiting• 1 mild nausea with no vomiting• 2• 3• 4 intermittent nausea with dry heaves• 5• 6• 7 constant nausea, frequent dry heaves and vomiting

Clinical Institute Withdrawal Assessment of Alcohol Scale, Revised (CIWA-Ar)
• TACTILE DISTURBANCES -- Ask "Have you any itching, pins and• needles sensations, any burning, any numbness, or do you feel bugs• crawling on or under your skin?" Observation.• 0 none• 1 very mild itching, pins and needles, burning or numbness• 2 mild itching, pins and needles, burning or numbness• 3 moderate itching, pins and needles, burning or numbness• 4 moderately severe hallucinations• 5 severe hallucinations• 6 extremely severe hallucinations• 7 continuous hallucinations

Clinical Institute Withdrawal Assessment of Alcohol Scale, Revised (CIWA-Ar)
• TREMOR -- Arms extended and fingers spread apart.• Observation.• 0 no tremor• 1 not visible, but can be felt fingertip to fingertip• 2• 3• 4 moderate, with patient's arms extended• 5• 6• 7 severe, even with arms not extended

Clinical Institute Withdrawal Assessment of Alcohol Scale, Revised (CIWA-Ar)
• AUDITORY DISTURBANCES -- Ask "Are you more aware of• sounds around you? Are they harsh? Do they frighten you? Are you• hearing anything that is disturbing to you? Are you hearing things you• know are not there?" Observation.• 0 not present• 1 very mild harshness or ability to frighten• 2 mild harshness or ability to frighten• 3 moderate harshness or ability to frighten• 4 moderately severe hallucinations• 5 severe hallucinations• 6 extremely severe hallucinations• 7 continuous hallucinations

Clinical Institute Withdrawal Assessment of Alcohol Scale, Revised (CIWA-Ar)
• PAROXYSMAL SWEATS -- Observation.• 0 no sweat visible• 1 barely perceptible sweating, palms moist• 2• 3• 4 beads of sweat obvious on forehead• 5• 6• 7 drenching sweats

Clinical Institute Withdrawal Assessment of Alcohol Scale, Revised (CIWA-Ar)
• VISUAL DISTURBANCES - Ask "Does the light appear to be too• bright? Is its color different? Does it hurt your eyes? Are you seeing• anything that is disturbing to you? Are you seeing things you know are• not there?" Observation.• 0 not present• 1 very mild sensitivity• 2 mild sensitivity• 3 moderate sensitivity• 4 moderately severe hallucinations• 5 severe hallucinations• 6 extremely severe hallucinations• 7 continuous hallucinations

Clinical Institute Withdrawal Assessment of Alcohol Scale, Revised (CIWA-Ar)
• ANXIETY -- Ask "Do you feel nervous?" Observation.• 0 no anxiety, at ease• 1 mild anxious• 2• 3• 4 moderately anxious, or guarded, so anxiety is inferred• 5• 6• 7 equivalent to acute panic states as seen in severe delirium or• acute schizophrenic reactions

Clinical Institute Withdrawal Assessment of Alcohol Scale, Revised (CIWA-Ar)
• HEADACHE, FULLNESS IN HEAD -- Ask "Does your head feel• different? Does it feel like there is a band around your head?" Do not• rate for dizziness or lightheadedness. Otherwise, rate severity.• 0 not present• 1 very mild• 2 mild• 3 moderate• 4 moderately severe• 5 severe• 6 very severe• 7 extremely severe

Clinical Institute Withdrawal Assessment of Alcohol Scale, Revised (CIWA-Ar)• AGITATION -- Observation.• 0 normal activity• 1 somewhat more than normal activity• 2• 3• 4 moderately fidgety and restless• 5• 6• 7 paces back and forth during most of the interview, or constantly• thrashes about

Clinical Institute Withdrawal Assessment of Alcohol Scale, Revised (CIWA-Ar)
• ORIENTATION AND CLOUDING OF SENSORIUM -- Ask• "What day is this? Where are you? Who am I?"• 0 oriented and can do serial additions• 1 cannot do serial additions or is uncertain about date• 2 disoriented for date by no more than 2 calendar days• 3 disoriented for date by more than 2 calendar days• 4 disoriented for place/or person• Total CIWA-Ar Score ______• Rater's Initials ______• Maximum Possible Score 67
The CIWA-Ar is not copyrighted and may be reproduced freely. This assessment for monitoring withdrawal symptoms requires approximately 5 minutes to administer. The maximum score is 67 (see instrument). Patients scoring less than 10 do not usually need additional medication for withdrawal.

COWS (Clinical Opioid Withdrawal Scale)• Resting Pulse Rate: _________beats/minute• Measured after patient is sitting or lying for one minute • 0 pulse rate 80 or below• 1 pulse rate 81-100• 2 pulse rate 101-120• 4 pulse rate greater than 120
• Sweating: over past ½ hour not accounted for by room temperature or patient activity.• 0 no report of chills or flushing• 1 subjective report of chills or flushing• 2 flushed or observable moistness on face• 3 beads of sweat on brow or face• 4 sweat streaming off face
• Restlessness Observation during assessment• 0 able to sit still• 1 reports difficulty sitting still, but is able to do so• 3 frequent shifting or extraneous movements of legs/arms• 5 Unable to sit still for more than a few seconds

COWS (Clinical Opioid Withdrawal Scale)• Pupil size• 0 pupils pinned or normal size for room light• 1 pupils possibly larger than normal for room light• 2 pupils moderately dilated• 5 pupils so dilated that only the rim of the iris is visible
• Bone or Joint aches If patient was having pain previously, only the additional component attributed to opiates withdrawal is scored
• 0 not present• 1 mild diffuse discomfort• 2 patient reports severe diffuse aching of joints/ muscles• 4 patient is rubbing joints or muscles and is unable to sit still because of discomfort
• Runny nose or tearing Not accounted for by cold symptoms or allergies• 0 not present• 1 nasal stuffiness or unusually moist eyes• 2 nose running or tearing• 4 nose constantly running or tears streaming down cheeks

COWS (Clinical Opioid Withdrawal Scale)
• GI Upset: over last ½ hour• 0 no GI symptoms• 1 stomach cramps• 2 nausea or loose stool• 3 vomiting or diarrhea• 5 Multiple episodes of diarrhea or vomiting
• Tremor observation of outstretched hands• 0 No tremor• 1 tremor can be felt, but not observed• 2 slight tremor observable• 4 gross tremor or muscle twitching
• Yawning Observation during assessment• 0 no yawning• 1 yawning once or twice during assessment• 2 yawning three or more times during assessment• 4 yawning several times/minute

COWS (Clinical Opioid Withdrawal Scale)
• Anxiety or Irritability• 0 none• 1 patient reports increasing irritability or anxiousness• 2 patient obviously irritable anxious• 4 patient so irritable or anxious that participation in the assessment is difficult
• Gooseflesh skin• 0 skin is smooth• 3 piloerrection of skin can be felt or hairs standing up on arms• 5 prominent piloerrection
• Total Score ________• The total score is the sum of all 11 items• Initials of person
completing Assessment: ______________• Score: 5-12 = mild; 13-24 = moderate; 25-36 = moderately severe; more than 36 = severe
withdrawal

Pathological Gambling• Persistent and recurrent maladaptive gambling behaviour as indicated by five (or
more) of the following:• 1. is preoccupied with gambling (e.g. preoccupied with reliving past gambling
experiences, handicapping or planning the next venture, or thinking of ways to get money with which to gamble)
• 2. Needs to gamble with increasing amounts of money in order to achieve the desired excitement.
• 3. Has repeated unsuccessful efforts to control, cut back or stop gambling• 4. is restless or irritable when attempting to cut down or stop gambling• 5. gambles as a way of escaping from problems or of relieving a dysphoric mood (e.g.
feelings of helplessness, guilt, anxiety, depression)• 6. after losing money gambling, often returns another day to get even (“chasing one’s
losses”)• 7. Lies to family members, therapist or others to conceal the extent of involvement
with gambling• 8.Has committed illegal acts such as forgery, fraud, theft or embezzlement to finance
gambling• 9. Has jeopardized or lost a significant relationship, job, or educational or career
opportunity because of gambling• 10 relies on others to provide money to relieve a desperate financial situation caused
by gambling
• B. The gambling behaviour is not better accounted for by a Manic Episode.

Drug Testing - Opioids
Immunoassay: detects morphine, does not differentiate between opioids and has poor sensitivity for oxycodone and meperidine; 3-4 day detection period
Chromotography required to identify specific opioids, but only 1-2 day detection period
Heroin: metabolite 6-monoacetylmorphine detected by chromatography for <12 hours
Methadone: chromatography required detection for 1-4 days