
BACE 2014 10-1-14... · Dr. Schaie’s “Seattle Study ... •A Policy approach can be effective &...
62
For the fitness for duty attendees: Please go to www.pollev.com/vortex
Transcript of BACE 2014 10-1-14... · Dr. Schaie’s “Seattle Study ... •A Policy approach can be effective &...

For the fitness for duty attendees: Please go to
www.pollev.com/vortex

Would You Fly With This Pilot? Assessing Fitness For Duty
Strategies for Safety
NBAA Safety Committee
Fitness for Duty Working Group
Quay Snyder, MD (Team Lead) – AMAS
Peter Agur – VanAllen Group
Paulo Alves, MD – MedAire

Fitness For Duty Working Group
• Quay Snyder (Lead)
• Gene Benson
• Dan Dominguez
• Debbi Laux
• Ed Thayres
• Jay White
• Leigh White
• Mark Larsen (NBAA)
• Peter Agur
• Paulo Alves
• Francois Lassale
• NBAA Safety Committee Leadership Team

Fitness For Duty
• NBAA Safety Focus Area – 2014 www.nbaa.org/ops/safety/top-safety-focus-areas/
• 3 Year Project
– Year 1 – Build Awareness / Needs Assessment
– Year 2 – Data Gathering / Refine Deliverables
– Year 3 – Field Industry Resources





Do We Have a Problem?

Evaluation Barriers- Cockpit
Protection of fellow pilots / long time friends

Evaluation Barriers- Cockpit
Potential Loss of Career / Income / Friendship
$$$

Evaluation Barriers- Cockpit
Needed for mission demands

Evaluation Barriers- Cockpit
“Not Bad Enough” … “I can cover for him/her”
“I can cover.”

Evaluation Barriers- Cockpit
Denial – personal or other pilots

Evaluation Barriers- Cockpit
Rationalization – “Just having a rough spell”
Sorry I missed all those radio
calls today.
“He’s OK – just having a rough spell.”

Evaluation Barriers- Cockpit
FAA medical certification fears
That condition is
disqualifying.

Evaluation Barriers- Cockpit
Fear to be involved

Evaluation Barriers - Management
• Legal / HR - Discrimination Suit
• Privacy concerns
• No Written Policy / Procedure
• Operational Demands
• Lack of Insurance / Disability Coverage
• Internal medical staff not trained for pilots
• Absence of Independent Expert evaluators
• Someone else’s responsibility

Bottom Line
Critical Threats & Risks to Safety
– Cockpit workload
– National Airspace System safety
– Puts Principals at risk
– Reputation of Aviation Department

Bottom Line
Critical Personal Health Issue
– Treatable conditions missed
– Physical / Psychological / Cognitive well being

Why Evaluate?
• SAFETY! SAFETY!! SAFETY!!!
• Staffing decisions
• Training Effectiveness / CRM
• Improved Health / Longevity
• Career Protection
• Financial Protection – Pilot – Insurance / Disability
– Company – Maximize Resources, Minimize Liability

Fatigue
NBAA Duty – Rest Guidelines
See Presentation by NBAA Fatigue Working
Group led by Leigh White
Wednesday 22 Oct 1330 Room S320H

Potential Causes - Medical
• Sleep Apnea / Sleep Disorders / Fatigue
• Medication Side Effects – NTSB-SS-14/01 (Includes OTC, Prescriptions, Illicit & Supplements)
• Acute Medical Condition (GI, ENT, Infection, etc.)
• Heart / Lung Disease
• Endocrine (diabetes, thyroid, adrenal)
• Hearing / Vision Deterioration
• Cancer
• Neurological disease

Potential Causes - Psychological
• Life Events (family, financial, legal, work)
• Post-Traumatic Stress Disorder – PTSD
• Depression
• Substance Abuse
• Anxiety Disorders
• Personality Traits
• Loss of Desire to Fly / Work

Potential Causes - Cognitive
• Mild Cognitive Impairment
• Alzheimer’s
• Substance dependence
• Surgery
• Brain injury / Bleed / Tumor
• Drug Use Trends in Aviation: Assessing the Risk of Pilot Impairment – NTSB-SS-14/01

Acute Medical Problems
Paulo Alves, MD, MSC, FASMA
Global Medical Director, Aviation Health
MedAire

Case 1
• 60 years old male
• LIMC-KCHS (Malpensa – Charleston) – Hawker 800
• Severe back pain and nausea
• Advil® (ibuprofen) 500 mg taken twice 45 minutes prior to contact
• Recommended diphenhydramine (Benadryl®) to relief nausea

Case 2
• 22 years old male co-pilot
• Shaking both hands, racing heart, difficulty breathing
• Van Nuys to Tapachula, Mexico
• Reports taking coffee and Rockstar® prior to the flight

Case 3
• 35 years old male
• G-650, EDDG-KBDL (return flight home)
• 5 hours to destination, 1 hour to EINN
• Vomiting, diarrhea initiated 3 days prior, now diarrhea with blood
• Tired and weak, severe stomach cramping

MedAire Experience 29 Months
• 89 cases Flight Deck-In Flight Medical Events were retrieved out of 59,143 total in-flight cases
• In 50 (60.9%) cases a medication was recommended or taken before contacting Ground Based Medical Support.
• NTSB – Study on Drug Use Trends in Assessing Risk of Pilot Incapacitation

Flight Deck Medical Categories
Source: MedAire

Level of Impairment
• Loss of consciousness occurred in 10 cases (8 syncope and 2 seizures).
• In 29/82 (35.4%) cases treatment was deemed to interfere with cognitive function
Source: MedAire

Medical Incapacitation Categories
Loss of consciousness,
9, 31%
Gastro, 6, 21%
Neurological, 6, 21%
Cardiac, 5, 17%
Urologic, 3, 10%
Source: FAA

Summary
• Acute medical problems may cause various levels of impairment/incapacitation
• Gastrointestinal and neurologic events are responsible for more than 50% in-flight medical situations
• Prevention of acute cases requires applying I’M SAFE (Illness, Medication, Stress, Alcohol, Fatigue, Eating)

Aging Pilots’ Fitness for Duty
Pete Agur, MBA
Chairman
The VanAllen Group

Aging Pilots’ Fitness for Duty
Are Aging Pilots a Threat?
The data says, “Yes.”
• US Census data
• Dr. Schaie’s “Seattle Study”
• NAMI Study
• FSF BASS attendees

Aging Pilots Fitness for Duty US Census Auto Accidents by Age
0%
20%
40%
60%
80%
100%
120%
140%
160%
20 - 24 25 - 34 35 - 44 45 - 54 55 - 64 65 - 74 75+

Aging Pilots Fitness for Duty Dr. Schaie’s “Seattle Study”
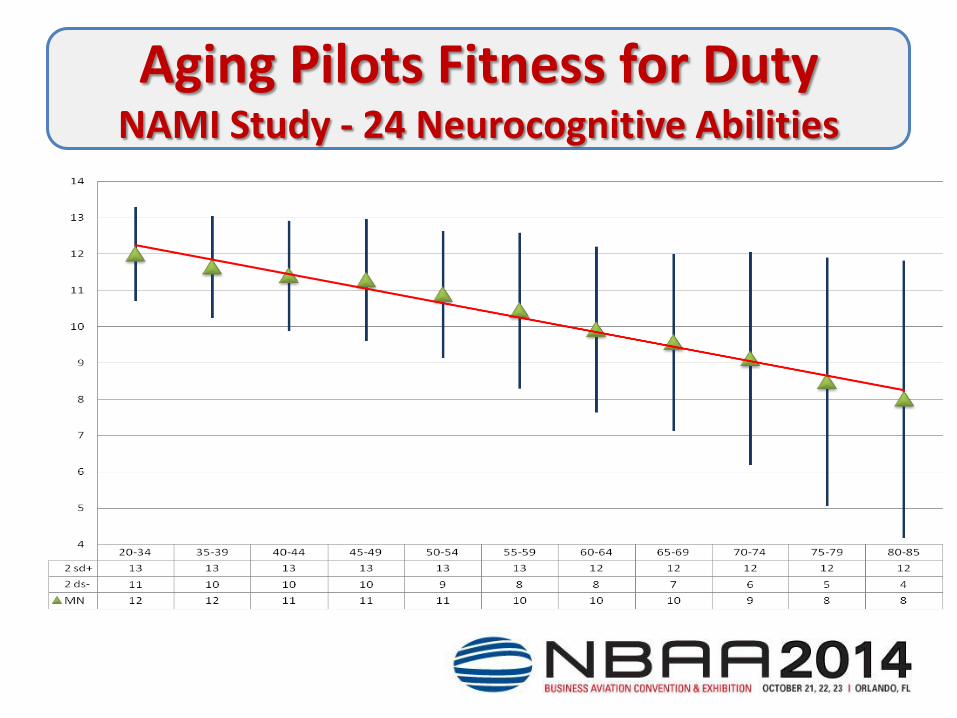
Aging Pilots Fitness for Duty NAMI Study - 24 Neurocognitive Abilities

Aging Pilots Fitness for Duty
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
None Low Moderate High
1%
17%
58%
24%
How significant are Aging Pilot risks?
Source: BASS 2014 Responses

Aging Pilots Fitness for Duty
0%
20%
40%
60%
80%
100%
Yes No
6%
94%
Do FARs address Aging Pilot risks?
Source: BASS 2014 Responses

Aging Pilots Fitness for Duty
0%
20%
40%
60%
80%
100%
No Some Yes
64%
18% 18%
Do you have Aging Pilot Policies?
Source: BASS 2014 Responses

Aging Pilots Fitness for Duty
Four Cases of Aging Pilots
• 57 years old Failing Eyesight
• 57 years old and 300 pounds
• 57 years old and Alzheimer's
• 85 years old and kicking ***

Aging Pilots’ Fitness for Duty
Why self-reporting / FARs are inadequate:
• FAR 61.53 – Honor System
• Sense of Self – I fly, therefore I am.
• Career – If I cannot fly, what will I do?
• Economic – My IRA has not recovered.
• Social – She/he married me for better or for worse, but not for lunch.

Aging Pilots’ Fitness for Duty
A “Policy” Approach:
• Include HR & Legal – Fair & defensible.
• Set an Age Limit – 65? 70?
• Set a Retirement Date – 12/31/XX. Celebrate!
• Physical Assurance – Approved AMEs only.
• Cognitive Assurance – Testing / observing?

Aging Pilots Fitness for Duty
Summary
• Aging Pilots are a “Threat”
• FARs are inadequate for Business Aviation
• We must address ALL “Threats,” even if it means it creates a career risk for some pilots
• A Policy approach can be effective & elegant





Fitness For Duty Evaluations
Quay Snyder, MD, MSPH
President/ CEO
Aviation Medicine Advisory Service a division of
Virtual Flight Surgeons, Inc.

What Have We Seen?
Business Aviation Community
• 32 FFD evaluations in 3 years
• 3 pilots evaluated but not entered into FFD program
• 3 pilots retired immediately after entry
Well Defined Process Exists
• Approval by Company and Pilot Group
• FAA Buy-In and Support
• Medical Providers Aeromedical / Safety Focus

Medical Causes Diagnoses Cases Pending* Grounded Flying
Sleep Apnea & Restless Legs 5 3 0 2
Medication Side Effects 2 1 0 1
Eyes 2 2 0 0
Hearing Loss 2 0 0 2
Heart Disease 3 1 1 1
Lung Disease 2 2 0 0
Anemia 1 1 0 0
Neurological Disorder 1 0 1 0
Cancer 1 0 0 1
Diabetes* (3 others not related) 3 2 1 0
Heavy Metal Toxicity 1 0 0 1
Total 23 12 3 8

Psychological Causes
Diagnoses Cases Pending Grounded Flying
Family Issues / Counseling 4* 1 0 3*
Post Traumatic Stress Disorder 3* 0 0 3*
Depression requiring Meds 2 1 0 1
Personality Issues 3 2 1 0
Total 11 4 1 6

Cognitive Causes
Diagnoses Cases Pending Grounded Flying
Alzheimer’s Disease - Probable 4 1 3 0
Mild Cognitive Impairment 11 5 1 1 retired
4
Note : All pilots had potential medical causes
of MCI treated before evaluation / treatment

Solutions
• Ethical – Fair to All
• Optimize Health
• Reduce Liability
• Reduce Costs
• Integral to Flight Department
Bottom Line:
Reduces Risk, Reduces Threats &
Enhances Safety

Key Elements - Company
• Leadership –understanding & support
• Process – clearly defined with timeline
• Legal – negligible liability profile – 3rd party
• HR – regular communication, benefits adequate
• Aviation Director – pilot availability estimate
• SAFETY PROGRAM – Principals, Pilots, Public

Key Elements – Pilots
• Confidentiality / Dignity / Respect
• Benefit Protection – Disability, Loss of License
• Evaluation – Comprehensive for Health
• Aeromedical Context & Expertise
• FAA Medical Certification Advocacy
• Health Safety Career

Results
• Ethical Program – unlike status quo
• Policy Emphasis, Not Regulatory
• Return to Optimum Health
• Financial Protections for All
• Graceful Exit, if necessary
• Safety Priority – Balances many factors


Fitness For Duty
• ENHANCING SAFETY
• OPTIMIZING HEALTH
• PRESERVING CAREERS
• SAVING LIVES

Questions
• Public – Now
• Private – Cards on Table
• NBAA Floor Exhibit – Safety Committee Counter 1100 – 1300 22 October – Booth 297
• BASS, IOC, S&D, BACE 2015, others
• [email protected] – Dr. Snyder
• [email protected] – Pete Agur
• [email protected] – Dr. Alves


















