Awareness with recall during general anesthesia
101
Department of Anaesthesia and Intensive Care Medicine University of Helsinki, Finland Awareness with recall during general anesthesia Seppo Ranta Academic Dissertation To be publicly discussed by permission of the Medical Faculty of the University of Helsinki, in Auditorium 2, Biomedicum Helsinki, Haartmaninkatu 8, on September 21, 2002, at 12 o’clock noon Helsinki 2002
Transcript of Awareness with recall during general anesthesia

Department of Anaesthesia and Intensive Care Medicine
University of Helsinki, Finland
Awareness with recall duringgeneral anesthesia
Seppo Ranta
Academic Dissertation
To be publicly discussed by permission of the Medical Faculty of theUniversity of Helsinki, in Auditorium 2, Biomedicum Helsinki,Haartmaninkatu 8, on September 21, 2002, at 12 o’clock noon
Helsinki 2002

Supervised by:
Docent Markku Hynynen, MD
Department of Anaesthesia and Intensive Care Medicine,
Helsinki University Central Hospital, Jorvi Hospital, Espoo, Finland
Reviewed by:
Professor Harry Scheinin, MD
Turku PET Centre, Turku University Hospital
Turku, Finland
Docent Arvi Yli-Hankala, MD
Department of Anaesthesia, Tampere University Hospital
Tampere, Finland
Official opponent:
Professor Rolf Sandin, MD
The Karolinska Institute, Stockholm,
and Department for Anesthesia and Intensive Care,
Länssjukhuset, Kalmar, Sweden
ISBN 952-91-4981-6 (nid.)ISBN 952-10-0642-0 (PDF)
Hakapaino OyHelsinki 2002
http://ethesis.helsinki.fi/


Contents
Abstract .............................................................................................. 7
List of original publications ................................................................ 9
Abbreviations .................................................................................... 10
1. Introduction ................................................................................. 11
2. Review of the literature ................................................................. 12
2.1. Definitions ............................................................................... 122.1.1. General anesthesia ..............................................................................122.1.2. Consciousness ....................................................................................122.1.3. Awareness ...........................................................................................122.1.4. Memory and Recall ............................................................................132.1.5. Awareness with recall during general anesthesia ..................................13
2.2. The nature of the experience of awareness during general anesthe-sia ................................................................................................... 14
2.3. Methods of detecting awareness during general anesthesia ........ 14
2.4. Incidence of awareness and recall during general anesthesia ...... 152.4.1. General surgery ..................................................................................152.4.2. Cardiac surgery ..................................................................................182.4.3. Other types of surgery ........................................................................18
2.5. Reasons for awareness with recall during general anesthesia ...... 222.5.1. General considerations .......................................................................222.5.2. Anesthetics .........................................................................................23
2.5.2.1. The concepts of minimum alveolar concentration and effective concentration . 23
2.5.2.2. Potent volatile anesthetic agents ........................................................................ 232.5.2.3. Intravenous anesthetics ..................................................................................... 242.5.2.4. Opioids ............................................................................................................. 242.5.2.5. Benzodiazepines ................................................................................................ 242.5.2.6. Nitrous oxide .................................................................................................... 252.5.2.7. Neuromuscular blocking agents ........................................................................ 25
2.6. Prevention of awareness with recall ........................................... 252.6.1. General recommendations ..................................................................252.6.2. Methods of monitoring consciousness during general anesthesia ........26
2.6.2.1. Clinical signs ..................................................................................................... 262.6.2.2. The isolated forearm technique ......................................................................... 262.6.2.3. Electroencephalography .................................................................................... 27
2.7. After-effects of awareness with recall during general anesthesia . 282.7.1. Mental after-effects .............................................................................282.7.2. Medico-legal after-effects ....................................................................29
3. Aims of the study.......................................................................... 30
4. Patients and methods.................................................................... 31
4.1. Patients .................................................................................... 31
4.2. Interviews and classification ..................................................... 33
4.3. Medications ............................................................................. 33
4.4. Artificial neural networks ......................................................... 34
4.5. Feedback information .............................................................. 364.6. Psychiatric interview and testing............................................... 37
4.7. Statistical methods ................................................................... 37
5. Results .......................................................................................... 38
5.1. The nature of the experience of awareness during general anesthe-sia ................................................................................................... 38
5.2. Incidence of awareness with recall during general surgery ......... 38
5.3. Incidence of awareness with recall during open heart surgery .... 38
5.4. Differences in anesthetic drug dosing between patients with andwithout awareness ........................................................................... 39
5.5. Conventional statistical methods and artificial neural networks indetecting awareness from monitored physiologic variables ............... 39

5.6. The possibility of reducing the incidence of awareness by givingfeedback information to the anesthesiologists .................................. 40
5.7. Psychiatric consequences of awareness during anesthesia ........... 41
5.8. Medico-legal consequences of awareness with recall in Finland . 42
6. Discussion .................................................................................... 46
6.1. Patients’ experiences during the episode of intra-anesthetic aware-ness ................................................................................................. 46
6.2. Methods used in the present studies ......................................... 46
6.2.1. Interviews ............................................................................. 46
6.2.2. Anesthetic records ................................................................. 47
6.3. Incidence of awareness with recall during general surgery ......... 476.4. Incidence of awareness with recall during cardiac surgery ......... 48
6.5. Differences in anesthetic drug dosing between patients with andwithout awareness ........................................................................... 49
6.6. Conventional statistical methods and artificial neural networks indetecting awareness from monitored physiologic parameters............ 49
6.7. The possibility of reducing the incidence of awareness by givingfeedback information to the anesthesiologists .................................. 50
6.8. Psychiatric consequences of awareness during anesthesia ........... 51
6.9. Medico-legal consequences of awareness with recall in Finland . 52
7. Conclusions .................................................................................. 53
8. Practical considerations ................................................................ 55
9. Future implications ....................................................................... 57
Acknowledgements ........................................................................... 58
References ......................................................................................... 60
Appendix .......................................................................................... 65
7
Awareness with recall is a rare but serious com-plication of general anesthesia with potentiallyvery disabling psychiatric consequences. Pre-requisites for the phenomenon of awarenessand recall are (1) consciousness with the abil-ity to receive and process sensory information,(2) storage of the processed information inmemory, and (3) recollection of the storedinformation at some later time.
The present study examines incidence ofawareness with recall during general anesthe-sia, the effects of anesthetic agents on it, meth-ods of detecting and preventing it, and its psy-chiatric and medico-legal after-effects. A totalof 3,868 cases (1,485 male and 2,383 female)were included in this study. Structured inter-views were conducted after general anesthesiafor cardiac or general surgery to find patientswho had experienced awareness during anes-thesia and were able later to recall their expe-rience. Additional cases were identified frominsurance claims based on awareness with re-call filed with the Patient Insurance Associa-tion in Finland. Psychiatric interview and test-ing were used to evaluate after-effects ofawareness and recall. Feedback informationwas given to cardiac anesthesiologists in orderto study the possibility of reducing incidenceof awareness with recall by educational means.Artificial neural networks were used to evalu-ate the likelihood of detecting intraoperativeawareness on the basis of conventional moni-toring information.
Abstract
In the present studies, the incidence ofundisputed intraoperative awareness was 0.2-0.4 % of all general anesthetics given for gen-eral surgery procedures, while the incidencewas about 0.3 % during cardiac anesthesia.Both incidences are 6 to 7 fold higher if casesof possible awareness and recall are included.Lower doses of primary anesthetic agents weregiven to patients with awareness and recallwhen compared to controls (isoflurane 0.42Fi% vs. 0.65 Fi% [p<0.005] and propofol 73µg/kg/min vs. 228 µg/kg/min [p<0.05], dur-ing general surgery respectively; midazolam0.8 µg/kg/min vs. 1.1 µg/kg/min [p<0.05]during cardiac surgery respectively). Standardphysiologic monitoring used during generalanesthesia did not reliably detect inadequatedepth of anesthesia, even when analyzed withcomputer-based artificial intelligence. Infor-mation given to anesthesiologists about in-traoperative awareness lead to a decreasingtrend in its incidence with simultaneous in-crease in the use of anesthetics and decreasein the use of muscle relaxants.
The psychiatric studies revealed anxiety inone patient after awareness and recall. In ad-dition, a case of pre-existing depression wasexacerbated after an episode of awareness andrecall. Awareness during general anesthesia hastriggered a small number of Patient Insuranceclaims in Finland (about 1 % of anesthesia-related claims). Seventy percent of the patientswho filed insurance claims received compen-

8
sations for pain; the average amount of com-pensation was EUR 1,000.
Awareness with recall is a rare complica-tion of general anesthesia and its incidence ison the decline. Insufficient dosing of generalanesthetics contributes significantly to thepresent incidence and it is likely that inform-ing anesthesiologists about this complication
would decrease it further Awareness cannotbe detected by standard monitoring; bettermonitoring tools need to be developed. Theincidence of psychiatric after-effects of intra-operative awareness is not known. In Finland,a small number of Patient Insurance claimshas been the only medico-legal after-effect ofthis complication.

9
1. Ranta S., Laurila R., Saario J., Ali-Melkkilä T., Hynynen M.: Awareness with recall duringgeneral anesthesia - Incidence and risk factors. Anesth Analg 86: 1084-1089, 1998.
2. Ranta S., Jussila J., Hynynen M.: Recall of awareness during cardiac anaesthesia: influenceof feedback information to the anaesthesiologist. Acta Anaesthesiol Scand 40:554-560, 1996.
3. Ranta S., Herranen P, Hynynen M.: Patients’ conscious recollections from cardiac anesthe-sia. J Cardiothorac Vasc Anesth 16:426-430, 2002.
4. Ranta S., Hynynen M., Räsänen J: Application of artificial neural networks as an indicatorof awareness with recall during general anaesthesia. J Clin Monit Comput 17:53-60, 2002.
5. Ranta S., Ranta V., Aromaa U.: The claims of compensation for awareness with recallduring general anaesthesia in Finland. Acta Anaesthesiol Scand 41:356-359, 1997.
List of original publications

10
AA Anesthetic agentAEP Auditory evoked potentialAER Auditory evoked responseANOVA Analysis of varianceASA American Society of AnesthesiologistsBIS Bispectral indexBP Blood pressureCABG Coronary artery bypass graftingCI Confidence intervalCO
2Carbon dioxide
D&C Dilatation and curettageDSM-III Diagnostic and Statistical Manual of Mental Disorders, 3rd editionDSM-IV Diagnostic and Statistical Manual of Mental Disorders, 4th editionEBT Endobronchial tubeEC
50Effective concentration in 50 percent of the subjects
ECG ElectrocardiogramEEG ElectroencephalogramET End-tidalETAGC End-tidal anesthetic gas concentrationETT Endotracheal tubeEUR EuroFi Inspiratory fractionFIM Finnish MarkGBP Pound sterlingi.v. IntravenousICU Intensive care unitIFT Isolated forearm techniqueMAC Minimum alveolar concentrationMLAEP Mid-latency auditory evoked potentialMVR Mitral valve replacementN.A. Not assessedN
2O Nitrous oxide
NMB Neuro-muscular blockerns. non-significantPACU Post-anesthesia care unitPIA Patient Insurance AssociationP
kPrediction probability
PTSD Post-traumatic stress disorderSaO
2Arterial blood oxygen saturation
SE Standard errorTx TransplantationUSD United States Dollar
Abbreviations

11
Conscious awareness with recall as a compli-cation of general anesthesia has existed for aslong as general anesthesia itself. In 1846,William Morton gave the first anesthetic toGilbert Abbott in a demonstration at theMassachusetts General Hospital in Boston.Gilbert Abbott told later that he was awareduring the anesthetic but felt no pain. Only asmall number of further reports of awarenessduring anesthesia were published in the nine-teenth and in the early twentieth century(Ghoneim, 2001). In the early days of anes-thesia, the practice of using a single generalanesthetic agent in relatively high concentra-tions to produce all components of generalanesthesia – unconsciousness, relief from pain,absence of reflexes, and muscle relaxation –apparently protected the patients from trau-matic awareness. Moreover, neuromuscularblocking agents (NMB) were not available,and patients were, therefore, able to signalawareness by movement. When NMBs wereintroduced into anesthetic practice to improveoperative conditions and to reduce the toxic-ity of general anesthetic agents, traumaticawareness became possible.
The first case report of traumatic consciousawareness with later recall during general an-esthesia was described in 1950(Winterbottom, 1950). Perhaps describing the
1. Introduction
attitude of some members of the medical pro-fession towards this complication, the surgeonwho operated on the patient reported byWinterbottom, later published a letter wherehe wrote that “the anaesthetic as a whole couldonly be described as excellent” (Wells, 1950).Studies of the incidence of awareness with re-call began in the 1960s. Generally, the pos-sible traumatic psychologic sequelae of thiscomplication were not acknowledged in themedical literature until the 1970s. However,despite several decades of attention to thisproblem, patient groups and, especially, indi-vidual patients at risk have not been clearlyidentified, the definition of this complicationis not entirely clear, its prevention has not beenstudied in detail, and the nature and incidenceof possible after-effects of awareness duringgeneral anesthesia are not known. Further-more, this complication is one of the mostfrequent fears of our patients. In a preopera-tive interview study, 54 % of patients wereanxious about not being asleep during theoperation (McCleane, and Cooper, 1990).
This thesis focuses solely on awareness withexplicit recall during general anesthesia. Thepossibility of subconscious learning andmemory during general anesthesia, or its pos-sible sequelae are not discussed.

12
2. Review of the literature
2.1. Definitions
2.1.1. General anesthesia
General anesthesia is a state characterized byunconsciousness, analgesia, muscle relaxation,and depression of reflexes (Willenkin, 1990)or, the administration of chemical agents toproduce reversible unconsciousness and de-pression of reflex response to afferent stimuli(Critchley, 1978). However, there are alsodefinitions of anesthesia where loss of con-sciousness, an all-or-none phenomenon, de-fines the beginning and ending of the anes-thetic state (Prys-Roberts, 1987). Thus,analgesia, muscle relaxation, and suppressionof autonomic activity, are not components ofanesthesia, but rather, should be consideredas desirable supplements to the state of anes-thesia (Prys-Roberts, 1987). Other authors,however, consider that the state of generalanesthesia includes different, smoothly chang-ing states of consciousness (Jones, andKonieczko, 1986). As the present thesis fo-cuses on awareness during general anesthesiawith explicit recall occurring afterwards, theterm ‘unconsciousness’ becomes the most im-portant component of general anesthesia. Itshould be clear that by preventing conscious-ness during general anesthesia there shouldbe no recall of it.
2.1.2. Consciousness
The term ‘consciousness’ is explained as “thestate of being conscious; awareness of one’sown existence, sensations, thoughts, surround-ings, etc.” (Anonymous, 1989). Conscious-ness involves four functions: stimulus uptake(perception), stimulus processing (mnemonicrepresentation), stimulus evaluation (emo-tion), and stimulus response (volition). Theseprocesses are integrated by complex neuronalsystems to achieve regional linking within onemodality, temporal, and semantic binding ofinformation. (Pöppel, and Schwender, 1993).
2.1.3. Awareness
The term ‘awareness’ is explained as “havingknowledge, conscious, cognizant” (Anony-mous, 1989). The term represents the state ofmind at a certain moment of time irrespec-tive of whether that state is later recalled ornot (Ghoneim, and Mewaldt, 1990). How-ever, Jones and Konieczko have claimed, thatthere would be different stages of “consciousawareness” and that also “unconscious aware-ness” would be possible (Jones, and Konieczko,1986).
In medical terminology, the term “aware-ness” has sometimes been regarded as mean-ing only consciousness during general anes-thesia (Critchley, 1978). This usage is differentfrom both the general meaning of the termand its meaning in the context of psychologi-

13
cal research. Therefore, the ‘medicalization’ ofthe term “awareness” is best avoided.
In this thesis, the terms “awareness” and“consciousness” are used interchangeably, assuggested by Ghoneim and Block (Ghoneim,and Block, 1997). As general anesthesia isdefined as a state of unconsciousness, it wouldlogically follow that a patient under generalanesthesia cannot be aware, and the converse.The term “awareness during general anesthe-sia” is, however, almost universally acceptedby both medical and legal circles, and its mean-ing is well understood. Therefore, this term isused in this thesis, and in other papers, as thereis no simple substitute (Payne, 1994).
2.1.4. Memory and Recall
Memory is essential for the recall of intraop-erative perception. As a cognitive function,memory has been divided to a variety of sub-systems (Andrade, and Baddeley, 1993). Theseinclude a working memory comprising a ‘pho-nological loop’ for linguistic memory and‘visuospatial sketchpad’ for visual and spatialinformation processing, and a ‘central execu-tive’ which organizes the process. The pro-cessed ideas are then transferred from work-ing memory to long term memory for storage,and possible retrieval. Forgetting is possiblein both the working memory and long termmemory. Responding to ideas retrieved fromlong term memory requires that these ideasare processed again in the working memory.(Baddeley, 1990; Andrade, and Baddeley,1993; Bailey, and Jones, 1997)
The anatomical representation of the work-ing memory in the human brain is the pre-frontal cortex. The long term memory is scat-tered in the medial temporal lobe, thehippocampus, and the posterior neocortex(Bailey, and Jones, 1997).
The retrieval from memory can be either aconscious or subconscious process. Theformer, explicit memory retrieval, includes thespatio-temporal context in which the recalled
event occurred, and the latter, implicit memoryretrieval, is revealed by a change in task per-formance (Kihlstrom, and Schacter, 1990).Explicit memory is also called declarative andimplicit memory non-declarative (Bailey, andJones, 1997). Declarative memory is furtherdivided into episodic, or autobiographicalmemory, and semantic, or factual memory(Bailey, and Jones, 1997). Explicit memoryrequires effortful recall (Bailey, and Jones,1997). Examples of explicit memory are re-membering meeting a person, or recallinghaving seen an accident. Examples of implicitmemory are subconscious processes like walk-ing, or riding a bicycle. It is likely that thelearning mechanisms involved in implicit andexplicit memory are different (Griffiths, andJones, 1990).
Memory is tested with direct and indirecttests; the former are used to test explicit re-call, the latter test implicit recall. In directmemory tests the subject is asked whether heor she remembers the stimulus such as hear-ing a word. Of primary importance is not,which words the subject knows but, rather,the specific process of hearing a word in a cer-tain situation. Indirect tests assess the changein the performance of the subject. For example,prior exposure to a certain word increases thelikelihood of that word being chosen from alist of words. (Ghoneim, and Block, 1992;Andrade, and Baddeley, 1993)
2.1.5. Awareness with recall duringgeneral anesthesia
The experience of awareness with recall dur-ing general anesthesia requires general anes-thesia and awareness being present in the pa-tient simultaneously. Furthermore, it isrequired that the patient later recalls this inci-dent.
It is claimed that anesthetic agents preventthe occurrence of awareness with recall by threemechanisms: 1. by interfering with the devel-opment of neuronal adequacy for signal pro-

14
cessing, 2. by interfering with the establish-ment of the time marker for the sensory expe-rience thus distorting the experience, and 3.by interfering with recall of the conscious ex-perience (Jessop, and Jones, 1991).
We rely on memory for evidence of whathas been perceived during general anesthesia.This evidence, when negative, will always besomewhat equivocal (Kihlstrom, and Schacter,1990). Accordingly, it is not unequivocallypossible to discriminate between patients whohave or have not been ‘aware’ or ‘conscious’during general anesthesia. The term ‘wakeful-ness’ has been used to describe patients whoare able to react meaningfully to stimuli dur-ing general anesthesia but are not able to re-call either the stimuli or their reactions post-operatively (Tunstall, 1977). There is evidencethat a large number of such patients exist(Tunstall, 1977, 1979; Russell, 1985, 1986,1993; Russell, and Wang, 1997). There alsois some evidence that wakefulness withoutexplicit recall might be detrimental for thepatient (Wang, 2001) but this has not beendefinitely proven (Ghoneim, and Block,1997).
In the present thesis, only awareness withexplicit recall is studied. This means that, in apost-operative interview, the patient can re-call having had perceptions of some kind dur-ing the time-context of general anesthesia.This is called ‘awareness with recall’ or, forbrevity, ‘awareness’ in this study.
2.2. The nature of the experienceof awareness during generalanesthesiaThe primary characteristics of awareness varybetween published reports. In a study of 26patients with intraoperative awareness basedon voluntary referral by anesthesiologistsMoerman et al. (1993) found that the mostcommon form of recall was hearing sounds,reported by 89 % of the patients. Paralysiswas the second most common feeling, recalled
by 85 % of the study population, while painwas reported by 39 % of those included inthe study
Cobcroft, and Forsdick (1993) recruitedpatients by advertising in popular magazines,and found pain to be the most common rec-ollection reported by 39 % of those respond-ing to the survey. Recollection of sounds wasreported by 31 % of this study population.
Schwender et al., (1998) recruited patientsboth with advertisements in newspapers andon the internet, and by referral from col-leagues. They confirmed auditory perceptionsto be the most common sensory modalityduring intraoperative awareness (100 % ofpatients). The next most common were tac-tile perceptions (64 %), and paralysis (60 %);24 % of the patients felt pain. In a closedclaims analysis, auditory perception was re-called by 30 % of the study population, tac-tile perceptions by 25 %, pain by 21 %, andparalysis by 20 % of the patients (Domino etal., 1999).
2.3. Methods of detectingawareness during generalanesthesiaObviously, detection of learning and explicitmemory during general anesthesia, requiresinterviewing the patient postoperatively(Kihlstrom, and Schacter, 1990; Ghoneim,and Block, 1992). In principal, either a post-operative interview for intraoperative events,or recall or recognition of stimuli presentedduring anesthesia can be used (Ghoneim, andBlock, 1992). Both types require consciousrecollection of specific learning episodes(Wolters, and Phaf, 1990).
The postoperative interview should bestructured (Ghoneim, and Block, 1992), oth-erwise a lower incidence of awareness and re-call is likely to be found (Jelicic, and Bonke,1989). A structured interview presents a stan-dard set of questions to all interviewed sub-jects. Brice et al. (1970) have designed five

15
simple questions for detecting explicit aware-ness in a postoperative interview (Table 1).
Some authors, however, have used simplersets of questions (Lyons, and Macdonald,1991; Sandin, and Nordström, 1993), and apostoperative interview under hypnosis hasbeen used by others (Goldmann et al., 1987).The value of hypnosis as a tool for studyingawareness, learning, or memory during gen-eral anesthesia has, however, been questioned(Ghoneim, and Block, 1992).
Typical positive responses indicating aware-ness are factual memories of discussions,noises, tactile sensations, or episodes of painor distress that can be traced back to the in-traoperative period. Feeling of muscle paraly-sis has also been considered typical of intra-operative awareness (Bailey, and Jones, 1997).Dreams that are either associated with anes-thesia or are altered states of awareness char-acterized by vivid thoughts and images areconsidered to be due to inadequate depth ofanesthesia (Ghoneim, and Block, 1992).
The timing of the interview has raisedmuch discussion. There is evidence that as-sessment of learning during anesthesia is moresuccessful later rather than sooner after expo-sure to inhalational agents (Bennett, 1986).However, there are case reports of patients whoremembered an experience of awareness in anearly interview but not any more in a laterinterview (Brice et al., 1970; Harris et al.,
1971; Dutton et al., 1995). In a well-con-ducted study, there was no correlation betweengeneral memory performance of intraopera-tive events and the time-interval between sur-gery and memory test (Lubke et al., 1999).Recently, it has been shown by Sandin andco-workers that more than one interview overa time period of at least two weeks increasesthe number of detected cases of awareness(Sandin et al., 2000).
It was noted very early that, in the inter-views, it is difficult to know what, if anything,is actually being remembered (Parkhouse,1960). Some authors have called for betterscrutiny of the reported cases by psychiatricinterview and hypnosis (Aldrete, and Wright,1985). The reporting of the recollections ofthe study patients varies between studies.
There are many ways of studying the im-plicit memory by indirect testing. These arereviewed, e.g., by Ghoneim, and Block (1992);Bailey, and Jones (1997); and Ghoneim, andBlock (1997).
2.4. Incidence of awareness andrecall during general anesthesia
2.4.1. General surgery
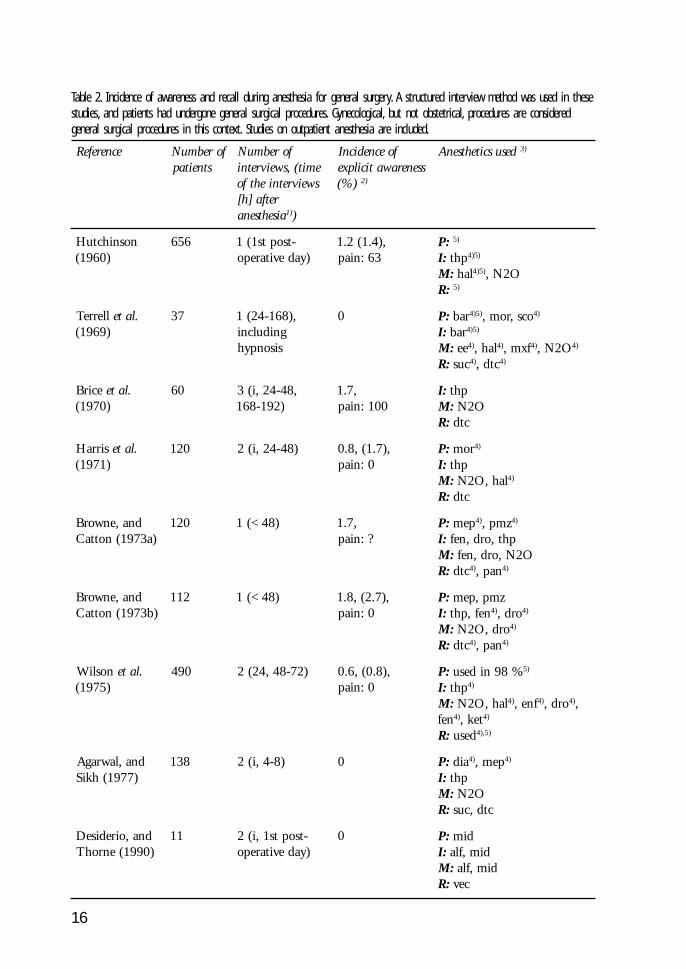
A large number of studies on the incidence ofintraoperative awareness and recall have beenpublished since Winterbottom’s original re-port of this intraoperative complication in1950 (Winterbottom, 1950). The publishedstudies using postoperative structured inter-view method are summarized in Table 2
Pedersen, and Johansen (1989) found andincidence of 0.1 % for intraoperative aware-ness in a study of 7,306 anesthetics conductedwithout structured interviews. Myles et al.(2000) used interviews, although not neces-sarily structured ones, in another large study,and identified 12 patients with awareness froma group of 10,811 interviewed patients, giv-ing an incidence of awareness of 0.11 %.
In general, the incidence has been on the
Table 1. Questions asked during the interviews.
1. What is the last thing you rememberbefore going to sleep for the operation?
2. What is the first thing you rememberafter waking after the operation?
3. Do you remember anything in between?
4. Did you have any dreams?
5. What was the most unpleasant thingyou remember from your operation andanesthesia?
16
Table 2. Incidence of awareness and recall during anesthesia for general surgery. A structured interview method was used in thesestudies, and patients had undergone general surgical procedures. Gynecological, but not obstetrical, procedures are consideredgeneral surgical procedures in this context. Studies on outpatient anesthesia are included.
ecnerefeR forebmuNstneitap
forebmuNemit(,sweivretnisweivretniehtfo
retfa]h[aisehtsena )1 )
foecnedicnIssenerawaticilpxe
)%( )2
desuscitehtsenA )3
nosnihctuH)0691(
656 -tsopts1(1)yadevitarepo
,)4.1(2.136:niap
:P )5
:I pht )5)4
:M lah )5)4 O2N,:R )5
llerreT .late)9691(
73 ,)861-42(1gnidulcnisisonpyh
0 :P rab )5)4 ocs,rom, )4
:I rab )5)4
:M ee )4 lah, )4 fxm, )4 O2N, )4
:R cus )4 ctd, )4
ecirB .late)0791(
06 ,84-42,i(3)291-861
,7.1001:niap
:I pht:M O2N
:R ctd
sirraH .late)1791(
021 )84-42,i(2 ,)7.1(,8.00:niap
:P rom )4
:I pht:M lah,O2N )4
:R ctd
dna,enworB)a3791(nottaC
021 )84<(1 ,7.1?:niap
:P pem )4 zmp, )4
:I pht,ord,nef:M O2N,ord,nef
:R ctd )4 nap, )4
dna,enworB)b3791(nottaC
211 )84<(1 ,)7.2(,8.10:niap
:P zmp,pem:I nef,pht )4 ord, )4
:M ord,O2N )4
:R ctd )4 nap, )4
nosliW .late)5791(
094 )27-84,42(2 ,)8.0(,6.00:niap
:P %89nidesu )5
:I pht )4
:M lah,O2N )4 fne, )4 ord, )4 ,nef )4 tek, )4
:R desu )5,)4
dna,lawragA)7791(hkiS
831 )8-4,i(2 0 :P aid )4 pem, )4
:I pht:M O2N
:R ctd,cus
dna,oirediseD)0991(enrohT
11 -tsopts1,i(2)yadevitarepo
0 :P dim:I dim,fla:M dim,fla
:R cev

17
1) i = immediately after emergence from the anesthesia
2) Incidence of clear awareness is given first, incidence of clear and doubtful awareness is given second (in parenthesis) if thatcan be estimated by the data given in the publication, and incidence of painful awareness (as a percentage of the total cases ofclear awareness) is given third.
3) Abbreviations of anesthetics used:
P = Premedication, I = Induction, M = Maintenance, R = Muscle relaxation,
alf = alfentanil, atr = atracurium, bar = barbiturate, bzd = benzodiazepine, dia = diazepam, dix = dixyrazine, dro=droperidol,dtc = d-tubocurarine, ee = ethyl ether, enf = enflurane, fen = fentanyl, hal = halothane, iso = isoflurane, ket = ketamine, kbe =ketobemidone, mep = meperidine, mhx = methohexital, mid = midazolam, mor = morphine, mxf = methoxyflurane, ndr =non-depolarizing muscle relaxant, N
2O = nitrous oxide, o = opioid; pan = pancurone, pro = propofol, pmz = promethazine,
Table 2. Continued.
ecnerefeR forebmuNstneitap
forebmuNemit(,sweivretnisweivretniehtfo
retfa]h[aisehtsena )1 )
foecnedicnIssenerawaticilpxe
)%( )2
desuscitehtsenA )3
uiL .late)1991(
000,1 )53-02(1 2.0 :P dzb )5)4 ocs, )4 ,citemeitna )5)4 rehto,
sevitades )5)4 o, )5)4
:I ?:M ?
:R cus )4
dna,nidnaSmörtsdroN
)3991(
005,2 )6 ehtrof2,)i(17271tsal
no,i(stneitapUCAPgnivael )7 )
,2.004:niap
:P ebk,xid:I orp,fla:M orp,fla
:R cev
relliM .late)6991(
09 )84-42(1 7.6 :P -:I dim,orp,fla )4
:M orp,fla:R rta
mörtsdroN te.la )7991(
000,1 ,18-21,i(3)293,1-27 )8
,)3.0(,2.005:niap
:P xid )4 dim, )4 o, )5)4
:I orp,fla:M orp,fla
:R stneitapllanidesu )5
nidnaS .late)0002(
587,11 ,63-42,i(3)633-861
,50.0:etinifeD,60.0:elbaborP
.30.0:elbissoP:sisylarapekawA
.esaceno61.0:llA
ybdetroperniaPsesacllafo%73
ssenerawafo
:P ,)%1.79(o)%.7.71(dzb
:I ,)%9.45(orp,)%13.0(ves,)%5.44(pht
)%42.0(tek:M ,)%6.39(O2N
,)%3.33(osi,)%7.66(ves)%8.2(orp
:R ,)%7.8(cusrdn )5 )%8.56(

18
decline in recent decades (Liu et al., 1991;Moerman et al., 1995; Table 2) but the vastmajority of studies continue to report a mea-surable incidence of this complication. Thedecline of incidence has been explained by thetendency to use progressively deeper levels ofanesthesia (Cormack, 1993). A higher inci-dence is often cited to be associated with cer-tain types of procedures, especially cardiacsurgery, obstetrics, and trauma surgery(Ghoneim, and Block, 1992; Ghoneim, andBlock, 1997). The incidence of explicit intra-operative awareness during different types ofprocedures is reviewed below.
Another source reflecting the frequency ofawareness during general anesthesia, are thecomplication databases. In the Australian In-cident Monitoring Study of 2,000 reportedcomplications, awareness during anesthesiawas the reason for reporting in 16 cases (0.8%) (Osborne et al., 1993). In a study usingthe closed claims database from the U.S.A.,claims concerning awareness during generalanesthesia resulted in 79 of the 4,183 claims(1.9%) (Domino et al., 1999).
2.4.2. Cardiac surgery
There are several studies on the incidence ofawareness and recall during cardiac anesthe-sia. The incidence figures are given in Table3. One has to note, that in one study inter-views during hypnosis were used (Goldmannet al., 1987). Therefore, the results of thatstudy are not directly comparable with otherstudies, which have used standard post-op-erative interview methods.
2.4.3. Other types of surgery
The studies on the incidence of awareness withrecall during operative obstetrics are summa-rized in Table 4.
The study by Crawford is one of the veryfew studies with a reasonable number of pa-tients comparing different anesthetic proto-cols in relation to awareness and recall(Crawford, 1988). The incidence of aware-ness and recall during elective caesarean sec-tion was 3.7 % in a group receiving thiopen-tal induction and maintenance of anesthesiawith 67 % nitrous oxide (N
2O). In a group
that received similar anesthesia with the addi-tion of 0.1 % methoxyflurane after the deliv-ery, the incidence of awareness was 0 %,p<0.045. Similarly, in the group of all opera-tive obstetric cases (elective and emergencysection plus vaginal deliveries) the incidenceof awareness was 3.1 vs. 0.3, p<0.003.
An incidence of awareness and recall dur-ing caesarean section of 2.8 % has been re-ported in a study group of 777 patients(Crawford et al., 1985) However, a structuredinterview method was probably not used inthis study.
In the most recent large study, the incidenceof awareness with recall during cesarean sec-tion during the years 1982 through 1989 wasfollowed. The mean incidence of awarenessand recall among the 3.076 patients was 0.9%. Until and including 1985, the incidenceof awareness and recall was 1.3 % and it de-creased to 0.4 % thereafter. The anestheticprotocol was changed during 1986: The in-duction dose of thiopental was increased from
sco = scopolamine, sev = sevoflurane, suc = succinylcholine, thp = thiopental, vec = vecuronium
4) An anesthetic received by some of the patients in the study.
5) Exact drug(s) not given in the published data.
6) Numbers are approximate.
7) PACU = Post anesthesia care unit.
8) Third interview was accomplished with a questionnaire, and 500 patients anesthetized last in the study series were included.
Table 2. Continued.

19
Table 3. Incidence of awareness and recall during cardiac anesthesia.
1) Incidence of clear awareness is given first, incidence of clear and doubtful awareness is given second (in parenthesis) if thatcan be estimated by the data given in the publication, and incidence of painful awareness (as a percentage of the total cases ofclear awareness) is given third.
2) Abbreviations of anesthetics used:
P = Premedication, I = Induction, M = Maintenance, R = Muscle relaxation,
anh=antihistamine, bar=barbiturate, dia = diazepam, dro=droperidol, fen = fentanyl, hal = halothane, hxz = hydroxyzine,iso = isoflurane, lor = lorazepam, mid = midazolam, mor = morphine, N2O = nitrous oxide, pan = pancurone,pap = papaveretum, pro = propofol, scb = secobarbital, sco = scopolamine, thp = thiopental
3) A drug received by some of the patients in the study.
4) Interviewed under hypnosis.
ecnerefeR forebmuNstneitap
forebmuNemit(,sweivretnisweivretniehtfo
retfa]h[)aisehtsena
foecnedicnIssenerawaticilpxe
)%( )1
desuscitehtsenA )2
aleskunuaM)7791(
931 -tsopts1(1)keewevitarepo
8.5 :P rab+hna:I ord )3 nef, )3 lah, )3 O2N, )3 ,pht )3
:M ord )3 lah, )3 O2N, )3
:R nap
)8791(miK 65 )17-42(1 ,)9.8(,6.305:niap
:P bcs,zxh:I pht,nef,ord:M nef )3 pht, )3 O2N, )3 lah, )3
:R nap
namdloG .late)7891(
03 )042-861(1 3.32(,7.6 )4 ,)0:niap
:P pap )3 ocs, )3 rol, )3
:I nef )3 lah, )3 O2N, )3
:M nef )3 lah, )3 O2N, )3
:R ?
spillihP .late)3991(
007 )021-69(1 ,)1.1(,6.005:niap
:P ?:I pht,nef,dimroaid )3
:M dim,nef )3 aid, )3 rol, )3
:R nap
dwoD .late)8991(
806 retfasruoh81(1)noitabutxe
3.0 :P aid )3 rol, )3 rom, )3
:I pht,nef )3
:M .dim,osissapyberofebosi,orpssapybgniruD )3 ,
orpssapybretfa:R nap
anesthetic was allowed after the delivery(Lyons, and Macdonald, 1991).
In a study of the incidence of awareness
5 to 7 mg/kg, the maintenance volatile anes-thetic was changed from halothane toisoflurane, and the use of a potent inhaled

20
Table 4. Incidence of awareness and recall during general anesthesia for operative obstetrics. A structured interview method isused in these studies.
ecnerefeR forebmuNstneitap
forebmuNemit(,sweivretnisweivretniehtfo
retfa]h[))1aisehtsena
foecnedicnIssenerawaticilpxe
)%( )2
desuscitehtsenA )3
dna,mörtsgreBnietsnreB
)8691(
71 )i(1 ,)3.53(,8.1105:niap
:P ocs )4
:I zxh,O2N )4
:M zxh,O2N:R cus
dna,nosliW)9691(renruT
051 )h63<,i(2 )576:niap,0.2 :P ?:I pht )4
:M O2N
drofwarC)1791(
088 )6 -tsopts1(1)yadevitarepo
6.1 )7 :P zdc )4 pem, )4 zrp, )4
:I pht,ocs:M pem,O2N )4 fxm, )4
:R cus
dna,gNmahtaburuG
)4791(
831 -tsopts1(1)yadevitarepo
76:niap,2.2 )8 detropertoN
dna,hsieluobA)6791(rolyaT
86 )63-42(1 0:niap,5.1 :P ?:I ait:M rom,aid,O2N
:R cus,nap,ctd
htrowsnraF)8791(
08 -tsopts1(1)yadevitarepo
0.5 :P ?:I pht:M fne,O2N )4
:R ctd,cus )4
sutetluhcS .late)6891(
63 -tsopts1,i(2)yadevitarepo
0:niap,3.8 :P ?:I tek )4 pht, )4
:M nef,O2N:R cus
akaraB .late)9891(
05 -tsopts1,i(2)yadevitarepo
4 :P -:I tek )4 pht, )4
:M lah )4 O2N, )4
:R cus
dogoB .late)0991(
47 )42(1 2.21(,7.2 )9 ,)05:niap
:P -:I pht:M O2N,fne
:R rta )4 cev, )4

21
with recall during surgery for major trauma,51 operated patients were divided into twogroups: to those who received anesthetics forthe intubation and for maintenance of anes-thesia during surgery, and to those who didnot receive any anesthetic for the intubationand / or did not receive anesthetics for at leasttwenty minutes during surgery because ofunstable hemodynamic condition or becauseof unconsciousness on arrival at the emergencyroom. The incidence of awareness with recall,
found in two consecutive structured inter-views, was 11 % in the former group, and 43% in the latter (Bogetz, and Katz, 1984). In arecent study, these findings were not con-firmed, but rather, the investigators were notable to find any convincing evidence of ex-plicit memories in a series of 96 trauma pa-tients. These patients were anesthetized accord-ing to a standardized protocol consisting ofetomidate, fentanyl, and isoflurane (Lubke etal., 1999).
Table 4. Continued.
ecnerefeR forebmuNstneitap
forebmuNemit(,sweivretnisweivretniehtfo
retfa]h[))1aisehtsena
foecnedicnIssenerawaticilpxe
)%( )2
desuscitehtsenA )3
dna,snoyLdlanodcaM
)1991(
670,3 1 )01 9.0 )11 :P ?:I pht:M lah )4 osi, )4 pap,O2N,
:R rdn,cus )21
1) i = immediately after emergence from the anesthesia
2) Incidence of clear awareness is given first, incidence of clear and doubtful awareness is given second (in parenthesis) if thatcan be estimated from the data, and incidence of painful awareness (as a percentage of the total cases of clear awareness) isgiven third.
3) Abbreviations of anesthetics used:
P = Premedication, I = Induction, M = Maintenance, R = Muscle relaxation,
alf = alfentanil, atr = atracurium, cdz = chlordiazepoxide, dia = diazepam, dtc = d-tubocurarine, enf = enflurane,fen = fentanyl, hal = halothane, hxz = hexobarbitone, iso = isoflurane, ket = ketamine, mep = meperidine, mor = morphine,mxf = methoxyflurane, ndr = non-depolarizing muscle relaxant, N2O = nitrous oxide, pan = pancurone, pap = papaveretum,prz = promazine, sco = scopolamine, suc = succinylcholine, thp = thiopental, tia = thiamylal, vec = vecuronium
4) A drug received by some of the patients in the study.
5) In addition to three patients classified as having experienced awareness, there were 23 (15.3 %) patients with unpleasantdreams and seven of these patients also experienced intraoperative pain.
6) Includes 218 patients undergoing postpartum sterilization
7) Different incidences of awareness for the two study groups, see text for details.
8) In addition to three patients classified as having experienced awareness, there were nine (6.5 %) patients with unpleasantdreams and seven of these patients also experienced intraoperative pain.
9) Includes patients reported to have “had dreams or heard voices”.
10) Time of postoperative interview not specified.
11) Study reported awareness and recall during eight years (1982-1989). Incidence differed over time, see text for details.
12) Exact drug(s) not given in the published data.

22
Moerman et al. (1995) studied the inci-dence of awareness with recall duringcardioverter defibrillator implantation: thepatients received diazepam premedication;induction with etomidate and alfentanil, andmaintenance with a propofol infusion; anatracurium infusion was used for muscle re-laxation. Two of the 33 (6.1 %) patients re-called the defibrillation shocks delivered dur-ing the cardioverter implantation. The authorssuggest that awareness was due to extravasa-tion of the anesthetic through a hole in thesubclavian vein created for the central lead ofthe defibrillator.
In a study trying to find out the incidenceof awareness and recall during intubation 160patients were interviewed; three (1.9 %) re-ported intraoperative awareness. However,only two were able to remember the intuba-tion while the third patient recalled paralysis(McKenna, and Wilton, 1973). In a more re-cent study, 30 patients were anesthetized withdifferent doses of etomidate (0.2–0.4 mg/kg)and fentanyl. The patients’ consciousness wasmonitored during intubation by the isolatedforearm technique (IFT). Positive IFT re-sponse was found in 80, 70, and 20 % of thepatients receiving 0.2, 0.3, and 0.4 mg/kgetomidate, respectively. One of the patientswith positive IFT response recalled awarenessin a postoperative interview, giving an inci-dence of awareness with recall of 3.3 % dur-ing intubation in this study (St Pierre et al.,2000).
An incidence of awareness and recall of 4.0% has been reported in patients anesthetizedwith thiopental for broncho- or laryngoscopy.(Barr, and Wong, 1973). In another study thatinvestigated awareness during bronchoscopythe incidence of awareness with recall was 6.7% in a group of 104 patients. The anestheticconsisted of thiopental 0.4-1.9 mg/kg/min,and succinylcholine for relaxation (Moore, andSeymour, 1987).
2.5. Reasons for awareness withrecall during general anesthesia
2.5.1. General considerations
The causes of awareness with recall have beenestimated from cases reported to the BritishMedical Defence Union (Hargrove, 1987;Table 5). Cases of faulty anesthetic techniqueinclude reliance on N
2O only in maintaining
anesthesia, and cases where the anesthesiolo-gist considered light anesthesia justified with-out apparent reasons. Failure to check appa-ratus includes cases in which a correctable faultin the anesthetic apparatus caused awareness.The authors considered that if a patient wasin danger of dying on the operating table, theuse of light anesthesia was justified.
The anesthetic care was defined substan-dard in 54 % of cases of awareness in a reportof closed claims analysis in the United States(Domino et al., 1999).
There are few case reports where toleranceto anesthetic agents has been implemented asa reason for recall (Walder, 1995). In general,these cases form a very small minority of thereported cases of awareness with recall. How-ever, it seems that consumption of alcohol,tobacco, or coffee is associated with increasedfentanyl requirement during induction ofhigh-dose fentanyl anesthesia (Stanley, and DeLange, 1984).
The majority of cases of awareness and re-
Table 5. Causes of awareness with recall reported to the BritishMedical Defence Union between 1982 and 1986 (Hargrove,1987).
Causes Percentage of cases
Faulty anesthetic technique 70
Failure to check apparatus 20
Genuine apparatus failure 5
Spurious claims 2.5
Justified risks / unknown cause 2.5

23
call seem to be due to preventable problemsin the anesthetic apparatus and administra-tion of anesthesia. A smaller fraction of pa-tients seem to suffer from this complicationbecause of individual differences in pharma-cokinetics and pharmacodynamics of anes-thetic agents. Important differences are knownto exist in the distribution of drugs and intheir entry into the effector site. The differ-ences between drug concentration and effectare, however, smaller than differences betweendrug dose and effect (Scheinin, 1999). Asmany anesthetic drugs are used in standarddoses it is likely that the complication of aware-ness will continue to exist unless the drug ef-fect can be titrated against a specific monitorof consciousness.
2.5.2. Anesthetics
A very large number of studies have comparedthe effect of different doses of anesthetic agentson learning and memory.
2.5.2.1.2.5.2.1.2.5.2.1.2.5.2.1.2.5.2.1. The concepts of minimum alveolarThe concepts of minimum alveolarThe concepts of minimum alveolarThe concepts of minimum alveolarThe concepts of minimum alveolarconcentrconcentrconcentrconcentrconcentration and effation and effation and effation and effation and effective concentrective concentrective concentrective concentrective concentrationationationationation
Movement as a response to a noxious stimu-lus has been used as a measure of the relativepotency of volatile anesthetics. Originally,movement as a response variable was chosenbecause it is an easily observable, categoricalvariable, and no other simple and unequivo-cal response variables existed (Eger, 2002). Theminimum alveolar concentration (MAC) isthe concentration of a volatile anesthetic nec-essary to eliminate movement in response tosurgical stimulation, usually skin incision, in50 % of subjects (Eger et al., 1965). MACvalues of several anesthetic agents are consid-ered to be additive (Eger, 1989). The MACconcept, however, only relates to movement,a response probably mediated by lower, spi-nal centers of the central nervous system(Rampil, 1994). A concept of MAC-awakehas been proposed to describe the concentra-tion needed to abolish consciousness in 50 %
of the subjects (Stoelting et al., 1970). MACis useful in comparing the potencies of differ-ent volatile anesthetics (Jones, 2000), how-ever, MAC is based on population studies, andby definition, 50 % of patients are still con-scious at MAC
awake value. Furthermore, sev-
eral individual factors like hypothermia, hy-potension, hypercarbia, acidosis, andelectrolyte disturbances affect MAC. Usually,the effector site (central nervous system) con-centration may be estimated by the end-tidalexpiratory gas concentration after a reason-able equilibration period. However, ventila-tion-perfusion mismatch may cause a variabledifference between the end-tidal and arterialblood gas concentration (Quasha et al., 1980).These factors render MAC alone unsuitablefor monitoring unconsciousness or depth ofanesthesia in an individual patient.
An analogous value for intravenous (i.v.)anesthetics, EC
50 (effective concentration) has
been defined as the blood concentration nec-essary to prevent movement in response tosurgical stimulation in 50 % of subjects(Scheinin, 1999; Jones, 2000). Significantinterindividual differences exist in drug dis-tribution and entry into the effector site(Scheinin, 1999). This, in addition to theobvious difficulties in obtaining the concen-tration values in a clinical situation, makeseven EC
50-values unsuitable for monitoring
an individual patient.
2.5.2.2.2.5.2.2.2.5.2.2.2.5.2.2.2.5.2.2. P P P P Potent volatile anesthetic agentsotent volatile anesthetic agentsotent volatile anesthetic agentsotent volatile anesthetic agentsotent volatile anesthetic agents
MACawake
values for desflurane, isoflurane, andsevoflurane are roughly 33-35 % of the MAC
skin incision value of the anesthetic. MAC
awake val-
ues of halothane and N2O are 52-58 % of
their MAC skin incision
values. Therefore,desflurane, isoflurane, and sevoflurane may beconsidered more potent amnestic anestheticsthan halothane (Eger, 2001).
A MACawake
of 2.6 % has been estimatedfor desflurane based on a volunteer study(Chortkoff et al., 1995). Desflurane has been

24
found to suppress both implicit and explicitmemory formation at a concentration of 0.6MAC
skin incision (Gonsowski et al., 1995).
Conscious memory was suppressed by ad-ministration of 0.45 MAC
skin incision of
isoflurane to a population of 17 volunteers.The EC
50 for isoflurane for preventing con-
scious memories was 0.20 MAC skin incision
inthe study (Dwyer et al., 1992). Isoflurane hasalso been reported to suppress both implicitand explicit memory formation at a concen-tration of 0.6 MAC
skin incision (Gonsowski et
al., 1995).A low concentration of sevoflurane (0.3 %
and 0.6 %, end-tidal) produced a greater de-gree of amnesia, psychomotor impairment anddrowsiness than 15 % and 30 % end-tidalN
2O, which was equipotent with the
sevoflurane concentration in terms of MAC(Galinkin et al., 1997). Based on mid-latencyauditory evoked potential (MLAEP) studies,end-expiratory concentrations of sevofluranegreater than 1.5 % should suppress auditoryperception, memory formation and implicitand explicit recall (Schwender et al., 1996).
2.5.2.3.2.5.2.3.2.5.2.3.2.5.2.3.2.5.2.3. Intr Intr Intr Intr Intravenous anestheticsavenous anestheticsavenous anestheticsavenous anestheticsavenous anesthetics
EC50awake
values for propofol (measured asblood concentration) follow the same patternas for volatile anesthetics, EC
50awake being 40
% of the EC50skin incicision
of propofol (Jones,2000). A case of awareness with recall has beenreported, where propofol was used as a soleanesthetic in a microlaryngeal procedure. Theinduction dose of propofol was 2.1 mg/kg andthe maintenance dose was 200 µg/kg/min(Kelly, and Roy, 1992).
Thiopental increases the latency and de-creases the amplitude of the MLAEPs. Thechange is comparable to that seen with e.g.propofol and potent inhalational anesthetics(Schwender, Klasing et al., 1994). Wilder-Smith et al. (1995) compared EEG arousalreactions during intubation in patients ran-domized to have anesthetic induction with
either thiopental 6 mg/kg or propofol 3 mg/kg. The degree of cortical EEG depression wassimilar in both groups, but the degree of EEGarousal reactions was significantly lower in thepropofol group.
In a study by Baraka et al. (1989), induc-tion of anesthesia for an elective caesarean sec-tion with ketamine 1.5 mg/kg produced sig-nificantly lower incidence of reactions in theisolated forearm (70 % vs. 13 %, p<0.05) thanthiopental 4 mg/kg. There was, however, nodifference between the groups in recall ofawareness in the postoperative interview.
Ketamine does not seem to producechanges in MLAEP amplitudes or latencies(Schwilden, 1994). This seems to imply thatthe primary processing of the auditory sen-sory information remains intact, but that thereis disruption of sensory processing at a higherlevel reflected by EEG changes (Schwilden,1994). Ketamine also has been shown to dis-rupt the memory retrieval process unlike manyother drugs (Ghoneim, and Block, 1992).
2.5.2.4. Opioids2.5.2.4. Opioids2.5.2.4. Opioids2.5.2.4. Opioids2.5.2.4. Opioids
There are case reports of awareness duringgeneral anesthesia with very high doses of fen-tanyl (72-96 µg/kg) (Mummaneni et al., 1980;Hilgenberg, 1981; Mark, and Greenberg,1983), and it may therefore be regarded thatopioids alone cannot guarantee surgical anes-thesia (Wong, 1983).
2.5.2.5.2.5.2.5.2.5.2.5.2.5.2.5.2.5.2.5. Benzodiaz Benzodiaz Benzodiaz Benzodiaz Benzodiazepinesepinesepinesepinesepines
Benzodiazepines (diazepam, midazolam, andlorazepam) have been used for the mainte-nance of anesthesia in cardiac surgical patients.The dose of benzodiazepines, or opioids, didnot differ between patients with and withoutawareness and recall (Phillips et al., 1993).
In a study of the frequency of awarenesswith recall during arthroscopy, patients re-ceived either placebo or midazolam 15, 30, or45 µg/kg i.v. in the operating room beforethe induction of anesthesia. Anesthesia was
25
induced and maintained with propofol whichwas titrated to maintain heart rate and sys-tolic blood pressure within ± 20 % of preop-erative values. There were four patients withawareness (19.1 %) in the group of 21 pa-tients receiving placebo ), while the incidenceof awareness was 2/69 (2.9 %) in the groupsreceiving midazolam (p < 0.04) (Miller et al.,1996).
A group of cardiac surgical patients receivedflunitrazepam 0.01 mg/kg for the inductionand 1.2 mg/h for maintenance of anesthesia.There was only a slight increase in the latencyor decrease in amplitude of MLAEPs. Thesepatients also reacted to loud sound (the soundof the sternotomy saw) with an increase inheart rate, arterial pressure, and pulmonarycapillary wedge pressure. These changes wherenot noticed in two groups of patients whoseanesthesia was induced with etomidate, andmaintained with isoflurane, or propofol, re-spectively (Schwender, Haessler et al., 1994).
2.5.2.6.2.5.2.6.2.5.2.6.2.5.2.6.2.5.2.6. Nitrous o Nitrous o Nitrous o Nitrous o Nitrous oxidexidexidexidexide
Conscious memories were not totally abol-ished by 0.6 MAC of N
2O in a population of
17 volunteers. The EC50
for N2O in prevent-
ing conscious memories was estimated to be0.50 MAC
skin incision (Dwyer et al., 1992). Simi-
larly, it has been shown that cortical auditoryevoked potentials (AEP) were suppressed sig-nificantly less by N
2O at 0.6 MAC
skin incision
than by isoflurane at 0.6 MAC skin incision
(New-ton et al., 1989). There is evidence that N
2O
may even antagonize the suppression of learn-ing induced by isoflurane (Chortkoff et al.,1993), as well as EEG depression caused byisoflurane (Yli-Hankala et al., 1993).
In a study by Russell, the incidence of wake-fulness as assessed by the isolated forearmmethod was 44 % in the group receiving 66% N
2O in oxygen for the maintenance of
anesthesia. The incidence of wakefulness was7 % in the group receiving etomidate 10 µg/kg/min. The incidence of awareness with re-
call was 4 % in the group receiving N2O for
maintenance, and zero in the etomidate group(Russell, 1986). A conclusion was reached ina recent study that an anesthetic consisting ofN
2O and bolus dosing of an opioid carries an
unacceptably high risk of awareness and re-call. The incidence of awareness with recall inthe group of patients receiving 70 % N
2O
supplemented with fentanyl boluses was sixpercent (Ghoneim et al., 2000).
There is, however, a study of 138 patientsnone of whom reported awareness with recallafter thiopental 7 mg/kg for induction fol-lowed by 66 % N
2O. The patients underwent
various abdominal procedures with a meanduration of anesthesia of 80 minutes. Recallwas tested with three consecutive structuredinterviews immediately after awakening andat 30-45 min and 3-4 h later(Agarwal, andSikh, 1977).
The effect of N2O, which is, at room tem-
perature, a gas, is dependent on its partial pres-sure. Therefore, the effect of N
2O is reduced
at high altitudes. Considering the earth’s sur-face, a vast population lives, and is anaesthe-tized, at high altitudes (James, 1994).
2.5.2.7.2.5.2.7.2.5.2.7.2.5.2.7.2.5.2.7. Neuromuscular b Neuromuscular b Neuromuscular b Neuromuscular b Neuromuscular blocking agentslocking agentslocking agentslocking agentslocking agents
Most cases of awareness are recorded duringso-called balanced anesthesia which includesthe use of NMBs. Therefore, it is often rec-ommended that NMBs be used as sparinglyas possible (Mainzer, 1979; Ponte, 1995).There are, however, a small number of casereports of awareness in patients who receivedno NMBs at all (Saucier et al., 1983; Osborneet al., 1993; Cundy, 1995; Sandin et al., 2000).
2.6. Prevention of awareness withrecall
2.6.1. General recommendations
Several authors have expressed as a goal theprevention of awareness with recall duringgeneral anesthesia by all possible means

26
(Anonymous, 1976, 1980)Several recommendations have been pub-
lished on avoiding awareness with recall. Theseusually include avoiding or limiting musclerelaxant use (Hug, 1990; Lunn, and Rosen,1990; Ghoneim, 2000), defining therapeuticwindows for anesthetics, and also, definingfactors modifying those windows (Hug,1990).
There are recommendations not to relysolely on N
2O, but to supplement it with a
volatile agent concentration of at least 0.6 %MAC
skin incision (Lunn, and Rosen, 1990;
Ghoneim, 2000), to administer at least 0.8-1MAC
skin incision when volatile anesthetics are
used alone, and to use drugs that produceamnesia when only light anesthesia is toler-ated (Ghoneim, 2000).
2.6.2. Methods of monitoringconsciousness during general anesthesia
Many methods have been used to monitor theanesthetic state, especially to detect an insuf-ficient depth of general anesthesia. Thesemethods do not measure learning or possibil-ity for later recall, but consciousness. There isa thorough review of the methodology byHeier and Steen (1996), and an update in-cluding the most recent methods byDrummond (2000).
2.6.2.1. Clinical signs2.6.2.1. Clinical signs2.6.2.1. Clinical signs2.6.2.1. Clinical signs2.6.2.1. Clinical signs
When anesthesia becomes too light, the pa-tient may move or show signs of sympatheticactivity. Movement is obviously not possibleif large doses of NMBs have been used. More-over, not all patients with intraoperative aware-ness move during the procedure (Saucier etal., 1983; Cundy, 1995).
Signs of sympathetic activity: tachycardia,hypertension, sweating, pupillary dilatation,lacrimation and sweating are often used asclinical signs of an inadequate level of anes-thesia. However, the signs of increased auto-nomic activity may be absent during treat-
ment with many drugs: opioids, cholinergicand beta-adrenergic antagonists, vasodilators,and antihypertensive agents (Ghoneim, andBlock, 1992). Epidural anesthesia may alsoobtund the sympathetic responses (Schwender,Faber-Zullig et al., 1994). Furthermore, itseems that not all patients with intraoperativeawareness, even with pain, show signs of in-creased sympathetic activity. In one study,propofol infusion was controlled to keep heartrate and systolic blood pressure within ± 20% of the patient’s preoperative values. How-ever, a 19 % incidence of awareness and recallof was found in one of the study groups (Milleret al., 1996).
Scoring methods have been developed formeasuring the anesthetic state based on sym-pathetic activity (Evans, and Davies, 1984).However, the correlation of these scores withother measures of the anesthetic depth hasbeen poor (Russell, 1993). Neither was agroup of experienced anesthesiologists able todiscriminate between patients with and with-out awareness in a study by Moerman andcolleagues (Moerman et al., 1993).
2.6.2.2.2.6.2.2.2.6.2.2.2.6.2.2.2.6.2.2. The isolated fThe isolated fThe isolated fThe isolated fThe isolated forearorearorearorearorearm techniquem techniquem techniquem techniquem technique
The technique of isolating one forearm fromcirculation before giving NMBs is describedby Tunstall in 1977 (Tunstall, 1977). Afterinduction of general anesthesia by anestheticdrugs but before giving NMBs, a blood pres-sure cuff is inflated on one arm to isolate thatforearm from the circulation. The forearmremains isolated from the effects of NMBsonce these drugs are administered, and there-fore, the patient may use the isolated forearme.g. for signaling. The method is limited bythe ischemia produced by the inflated bloodpressure cuff. However, the tourniquet maybe pressurized several times consecutively ifone assures that the concentration of NMBsis low at the time of deflation. The patientmay respond by voluntary movement of theisolated forearm to questions posed by the

27
investigator. Most of the patients respondingby intraoperative forearm movement have norecall afterwards. IFT has been reported to bean unhelpful indicator of patients with aware-ness and postoperative recall (Bogod, 1990).Indeed, it has been shown that the responsesof the isolated forearm, though representingcomplex responses to verbal commands, maynot necessarily represent a conscious response(Thornton, and Jones, 1993). Some authorshave found the method impossible to use be-cause it interferes with the surgical activity(Breckenridge, and Aitkenhead, 1981).
2.6.2.3.2.6.2.3.2.6.2.3.2.6.2.3.2.6.2.3. Electroencephalogr Electroencephalogr Electroencephalogr Electroencephalogr Electroencephalographyaphyaphyaphyaphy
The electroencephalogram (EEG) is the sum-mary result of the activity of the cortical neu-rons (Bailey, and Jones, 1997). In general,there is a decrease of the fast activity and anincrease in the high-amplitude, slow-frequencycomponents in the EEG during anesthesia(Bailey, and Jones, 1997). However, the mag-nitude of change and exact patterns vary be-tween anesthetic agents (Clark, and Rosner,1973). Furthermore, there is considerable in-terference in the EEG recording caused bydifferent electrical devices present in the oper-ating room environment (Rampil, 1998).Therefore, raw EEG is not very suitable forassessing anesthetic state, at least in inexperi-enced hands.
Many forms of processed EEG signal havealso been evaluated for the monitoring ofdepth of anesthesia. At least the followingmethods have been used: spectral array, pe-riod-amplitude analysis, spectral edge fre-quency, median frequency, and aperiodicanalysis (Rampil, 1998). None of these meth-ods have proven to be of practical value inmonitoring the anesthetic state produced byanesthetic drug combinations (Ghoneim, andBlock, 1992; Bailey, and Jones, 1997).
The bispectral index (BIS) is an empiri-cally derived algorithm that reflects the stateof the brain in relation to sedation (Sigl, and
Chamoun, 1994; Rosow, and Manberg,1998). It was developed by a statistical analy-sis of a large number of EEG samples on sub-jects whose level of sedation was known. BISincorporates power spectral analysis of theEEG, components of the EEG that are due tophase relationships, and the degree of burstsuppression (Rampil, 1998; Drummond,2000; Kerssens, and Sebel, 2001).
The BIS seems to function well as a practi-cal clinical on-line trend monitor of the levelof sedation. The correlation of conscious re-sponses and memory function at a popula-tion level is good, but there are considerableinterindividual differences in these parameters,particularly at the lower end of the scale(Drummond, 2000; Kerssens, and Sebel,2001).
The principle of auditory evoked responses(AER) is that the subject listens to ‘click’-stimuli while his EEG is recorded, and anaverage response, the AER, is extracted fromthe background EEG that, in this context, isconsidered noise (Thornton, and Sharpe,2001). The mid-latency auditory evoked po-tentials (MLAEP) are recorded 15-100 msafter the stimulus, and represent the primarynon-cognitive cortical processing of auditoryimpulses (Heier, and Steen, 1996). All vola-tile anesthetics, propofol and thiopental re-duce the amplitudes of MLAEPs and increasetheir latency in a dose-dependent fashion(Heier, and Steen, 1996; Yli-Hankala, 2000).
A correlation between short latencies of theauditory evoked signal and signaling of aware-ness by the isolated forearm method has beenshown (Thornton et al., 1989).
It has been shown that when the early cor-tical potentials of MLAEPs are preserved dur-ing general anesthesia, auditory informationmay be processed and remembered postop-eratively (Schwender, Kaiser et al., 1994).However, AER does not predict movement tonoxious stimulation during 1 MAC
skin incision
concentration of isoflurane and N2O (Kochs

28
et al., 1999). Thus, AER reflects the consciousstate of the patient in relation to anesthesiaand surgical stimulation and not solely in re-lation to anesthetic depth.
2.7. After-effects of awarenesswith recall during generalanesthesia
2.7.1. Mental after-effects
The potential for mental consequences afterneuromuscular paralysis was first described byMeyer and Blacher in 1961 in cardiac surgerypatients (Meyer, and Blacher, 1961). The mainfeatures of the patients were anxiety, irritabil-ity, and repetitive nightmares. However, thepatients did not have clear recollection of in-tra-operative awareness, and they were uncer-tain of the cause of their symptoms.
Mental after-effects are due to the verystressful experience of awareness during gen-eral anesthesia. It is, however, difficult for thepatient to distinguish between periods imme-diately before and after anesthesia and theanesthesia itself. Patients have been describedwho claim to have been aware during anes-thesia, even though only sedation or localanesthesia had been used. After-effects havebeen similar to those after awareness duringintended general anesthesia (Moerman et al.,1993; Cundy, 1995). This also applies toawareness and recall during waking up froman anesthesia: the time scale of the patient isdistorted, and a patient may have serious psy-chiatric sequelae after recalling waking up in-tubated and during transport, even thoughhe is no longer anesthetized from the stand-point of the anesthesiologist (Ho, 2001). Ithas also been claimed that awareness per se isnot the important issue but rather, the senseof passively experiencing something overwhich one has no control, where the feeling isthat things are not going as expected, and yet,they cannot be corrected by calling for help(Blacher, 1984). Muscle relaxation (Wang,2000), pain and fear of dying (Cundy, and
Dasey, 1996) have been cited as worst stres-sors causing the after-effects. Furthermore, ithas been suggested that patients who havebeen forewarned of the possibility of beingaware during surgery, and of the reasons forit, may not develop psychiatric after-effects(Holt, and Yate, 1993). In patient satisfac-tion studies, dissatisfaction scores are typicallyextremely high in cases of awareness with re-call during general anesthesia (Myles et al.,2000).
Typical symptoms after an experience ofawareness during general anesthesia are irri-tability, insomnia, repetitive nightmares, anxi-ety, depression, and preoccupation with death.There may also be morbid fear of hospitals ordoctors, and of the need for future surgery(Blacher, 1975, 1984; Payne, 1994). The pa-tients also typically find it difficult to discusstheir experience of awareness (Blacher, 1975).This may be made worse by the medical andnursing staff if it is suggested that the experi-ence had been imagined, or, even worse, thepatient is blamed for it because of e.g. over-weight (Payne, 1994). When a patient re-ported an experience of awareness during an-esthesia to the hospital staff 37 % of thepersonnel responded with disbelief, ignorance,or anger. An additional 14 % of patients weretold that their experience was “just a baddream”, “all in your imagination”, or that they“were mad or hallucinating”, or “had a sev-enth sense” (Cobcroft, and Forsdick, 1993).
In the study of Moerman et al. (1993),70 % of patients who had experienced aware-ness during general anesthesia had unpleas-ant after-effects; 6 % of patients had neededpsychotherapeutic help. In the study byShwender and co-workers 48.9 % of the pa-tients had after-effects, anxiety (55.0 %) andnightmares (52.4 %) being the most commonones. Post-traumatic stress disorder (PTSD)was found in 14.3 % (Schwender et al., 1998).Both studies recruited patients by advertisingor via referral from colleagues.
Of the long term after-effects, the most

29
important is PTSD. PTSD is characterized bythree symptom clusters: 1) re-experiencing, 2)avoidance and numbing, and 3) increasedarousal which follows a traumatic event(Osterman, and Van Der Kolk, 1998). PTSDis chronic or recurring in a high proportionof those in whom it develops (Osterman, andVan Der Kolk, 1998). In a prospective study,four out of six patients had mental reactionsafter a year of the precipitating anesthesia(Bergström, and Bernstein, 1968), and inanother study 56.3 % of the subjects withintraoperative awareness had PTSD after amean of 17.9 postoperative years (Ostermanet al., 2001). In a prospective follow-up study,all eight patients with intraoperative aware-ness experienced fear when falling asleep fromtime to time. All had anxiety concerning fu-ture anesthetics (Jordening, and Pedersen,1991). A recent study (Lennmarken et al.,2002) tried to evaluate all patients with pre-viously experienced awareness and recall foundin another large study (Sandin et al., 2000).The investigators were able to interview nineof the 18 original patients. Four of the nineinterviewed patients fulfilled all DSM-IV cri-teria for PTSD median of 27 months afterthe unsuccessful anesthesia. Three other pa-tients had some PTSD symptoms, but did notfulfill the diagnostic criteria. Six of the origi-nal 18 patients refused the interview, whichthe authors partly interpret as avoidance be-havior typical of PTSD (Lennmarken et al.,2002).
Recommendations for treating a patientwho has just experienced awareness with re-call have been published. The anesthesiolo-gist should always visit the patient complain-ing awareness with recall and acknowledgepatient’s account of events as real. The anes-thesiologist should apologize to the patient andassure that the event will be recorded in thehospital notes. A possible error that has leadto the event of awareness with recall should
be admitted (Aitkenhead, 1990; Ghoneim,2000). It is also suggested that a patient withintraoperative awareness needs to feel a senseof safety and connection to the surgical andanesthesia teams (Osterman, and Van DerKolk, 1998). Care should be taken not to as-cribe blame on the patient. However, it is theopinion of some authors that explanation andsimple reassurance are not adequate measuresfor preventing serious psychiatric complica-tions of awareness with recall (Macleod, andMaycock, 1992). Indeed, based on the possi-bly large incidence of PTSD after, at least,painful awareness (Osterman et al., 2001), andthe chronic nature of PTSD, a psychiatricconsultation is usually warranted in these cases(Osterman, and Van Der Kolk, 1998;Lennmarken et al., 2002).
2.7.2. Medico-legal after-effects
Very large compensations, GBP 20,000 to100,000, have been awarded for awarenessduring general anesthesia in Great Britain(Payne, 1994). In one of the cases, the com-pensation was particularly large, in part, be-cause the anesthesiologists refused to see thepatient after surgery even though she com-plained about her awareness (Payne, 1994).In the malpractice claims involving awarenessduring general anesthesia in the United States,the cost of settlement or jury awards haveranged from USD 1,000 to 600,000 (Dominoet al., 1999). In this analysis, factors associ-ated with claims for recall during general an-esthesia compared to other general anesthesiaclaims were: no volatile anesthetic agent used,female gender, obstetric or gynecologic pro-cedure, intraoperative opioid, and intraopera-tive muscle relaxant (Domino et al., 1999).
No precedent based on a case of intraop-erative awareness and recall has been issuedby the Finnish Supreme Court according tothe Finlex database kept by the Ministry ofJustice of Finland (Anonymous, 2002).

30
3. Aims of the study
1. To study the incidence of awareness withrecall during anesthesia for general surgery.(Study1)
2. To study the incidence of awareness withrecall during anesthesia for cardiac surgery.(Studies 1 and 2)
3. To find out possible differences in anestheticdrug dosing between patients with andwithout awareness and recall (Studies 1 and3)
4. To study whether or not it is possible todetect awareness with recall by analyzingchanges in variables commonly monitored
during general anesthesia with conventionalstatistical methods or artificial intelligenceneural networks. (Study 4)
5. To evaluate the utility of giving feedbackinformation to the anesthesiologists in low-ering the incidence of awareness. (Study 2)
6. To study the psychiatric consequences ofawareness with recall. (Studies 1,2,3 and5)
7. To study the medico-legal consequences ofawareness with recall in Finland in the formof patient insurance claims. (Study 5)

31
4. Patients and methods
4.1. PatientsThese studies were carried out at the Päijät-Häme Central Hospital, Lahti, Finland (Study1), and the Meilahti Hospital Department ofSurgery, Helsinki University Central Hospi-tal, Helsinki, Finland (Studies 2 and 3). Inaddition, patient records were obtainedthrough the Patient Insurance Association(PIA) of Finland and through advertisementsin the Journal of the Finnish Society ofAnaesthesiologists (Finnanest 1997: 30: 38).The total number of enrolled patient cases was3,868 (1,485 male and 2,383 female). Tak-ing into account the fact that some patientshad been operated more than once, the totalnumber of individuals included in these stud-ies is 3,739 (1,463 male, 2,276 female). Per-missions of local ethical committees were ob-tained for the studies. The number of cases inthe individual Studies is shown in Figure 1.
In Study 1 all elective general surgery pa-tients over 12 years of age operated betweenAugust 1994 and August 1995 in the Päijät-Häme Central Hospital, Lahti, Finland wereincluded in the study. A total of 4,818 (1,215male, 3,603 female) such patients were oper-ated on during the study period, and 2612(54.2 %, 608 male, 2,004 female) of themwere interviewed. 121 of the included patientswere operated more than once, and hence,interviewed more than once. Therefore, thetotal number of different patients included is
2,484 (586 male and 1,898 female). Failureto enter all elective patients into the study re-sulted from time constraints imposed by otherduties on the anesthesia nurses who did thescreening interviews.
In Study 2, a random sample of 99 (74male, 25 female) patients who underwent openheart surgery between June, 1992 and Sep-tember, 1992 was selected first. The secondpart of study included all open heart surgerypatients operated on between September, 22and November, 23, 1993, altogether 236 pa-tients. Thirty two patients were excluded, leav-ing 204 (86%; 147 male, 57 female) for theanalysis. Excluded were those transferred toother hospitals before the screening interviews,patients with Intensive care unit (ICU) staysover ten days, patients with neurological com-plications making the screening interviewimpossible, and patients who did not surviveuntil the interview. The total number of pa-tients in Study 2 was 303 (221 male, 82 fe-male).
In Study 3, all open heart surgery patientsoperated on between January 13, 1995 andJanuary 13, 1996 were evaluated for enroll-ment. There were 1,218 (870 male, 348 fe-male) such patients, and 929 (76%; 653 male,276 female) of those were included in thestudy. The reasons for exclusion were: 148patients could not be reached before they leftthe ward after the operation, 62 stayed in the

32
Figure 1. Number and flow of patients in the studies. Operated and actually interviewed cases (interview percentage) are shownfor the interview studies 1, 2, and 3. Use of patient cases from these and other sources for the artificial intelligence study (4) areshown by arrows.

33
ICU for more than 5 days, 38 died before theinterview, 25 developed neurological symp-toms preventing the screening interview, 6 didnot speak Finnish, 2 had psychiatric syn-dromes preventing interview, and 7 had vari-ous other reasons preventing interview.
In Study 4, patients with awareness andrecall were recruited from Study 1 (n = 9, 2male, 7 female), Study 5 (n = 4, 2 male, 2female), from claims filed in the PIA (n = 5,all female), and from information receivedfrom colleague anesthesiologists (n = 15, 1male, 13 female, one of whom had experi-enced awareness twice). The total number ofpatients with awareness and recall was, there-fore, 33 (5 male, 28 female). The control pa-tients (n = 510, 137 male, 373 female) wererandomly gathered from the patients withoutconscious awareness and recall in Study 1 (n= 501, 133 male, 368 female) and from pa-tients interviewed after general surgery inMeilahti Hospital (n = 9, 4 male, 5 female).Altogether, in Study 4, there were 543 (142male, 401 female) patient cases, and 542 in-dividuals (142 males, 400 females).
In Study 5, there were 4 patient recordscollected from the claims of compensation filedin the PIA between May 1, 1987 and Decem-ber 31, 1993. Two of these patients were maleand two female.
4.2. Interviews and classificationThe screening interviews used questions de-scribed earlier (Brice et al., 1970, Table 1) andthe patients were interviewed only once. InStudy 1, the interviews were conducted byrecovery room nurses before the patient leftthe recovery room. The nurses notified theinvestigators immediately of clear cases of in-traoperative awareness. After the completionof the studies, the interview forms completedby the nurses were analyzed by the investiga-tors. The cardiac surgery patients in studies 2and 3 were interviewed in the postoperativewards by the investigators.
When interpreting the answers to the struc-
tured interview questions, importance wasplaced on the subjective feeling of the patientregarding awareness during anesthesia. Theanswers were also graded to three groups ac-cording to objective memories that could betraced back to the time of anesthesia, and theduration of awareness (Table 6).
Table 6. Grouping of structured interview answers.
Group Definition
Group 1 Patients with unclear memories ordreams, which could be of intra-operative origin.
Group 2 Patients with short periods ofawareness occurring eitherintraoperatively or during theperiod of awakening fromanesthesia.
Group 3 Patients with long-lasting, clear,and undisputed recall of theintraoperative period.
4.3. MedicationsAnesthesia records were used as a source ofinformation regarding the anesthetic medica-tions used during the studies. In Studies 1, 2,and 3 the total dose of medications given i.v.was recorded. The dose of the inhaled anes-thetics was calculated from the anestheticrecords as follows: The inspired concentrationof the anesthetic was multiplied by the time(in minutes) that this concentration was used;the concentration-time products were thenadded to a grand total. The anesthetic timewas recorded, and a mean dose of both i.v.and inhaled anesthetic agents was calculated.Furthermore, continuous or intermittent an-esthetic delivery was also noted. Continuousadministration of an anesthetic was definedas an inhaled or i.v. anesthetic started within15 minutes after induction and continueduntil the end of surgery without interruptionslasting longer than 15 min.
In Study 1, the doses of anesthetics used

34
for general anesthesia were estimated fromrandom samples collected as follows: First, asample of 103 anesthetic records was collectedfrom the three-month period immediatelypreceding the interview period. We assumethat this period represents the standard prac-tice of the anesthesiologists in the hospital.During each four three-month interview pe-riods, a sample of 108 anesthetic records wascollected. Thus, we had a database of 535 ran-dom anesthetic records, which allowed detec-tion of possible change in the doses of anes-thetics over time, and comparison betweendoses received by patients with or withoutawareness. This database was also used forPoisson regression analysis. When comparingthe doses of anesthetics received by the pa-tients with or without awareness, the recordsof patients not interviewed for some reasonwere excluded. After this exclusion, 247records were left for analysis.
In Study 2, the anesthetic records of allinterviewed patients were included in theanalysis.
In Study 3, a random sample of 308 anes-thetic records was selected from the group of
interviewed patients. Later, the anestheticrecords of 16 patients with awareness and fivepatients with unpleasant dreams were in-cluded. Thus the total number of anestheticrecords used for the analysis of medicationswas 329.
In Study 5, the anesthetic records of all fourpatients were analyzed.
4.4. Artificial neural networksArtificial neural networks are a form of artifi-cial intelligence with the ability to discovernon-linear dependencies between input andoutput patterns even when they are difficultor impossible to detect with conventional sta-tistical methods. In practice, an artificial neu-ral network is simulated in a computer pro-gram and is configured and trained to performa specific task. A network is trained by pre-senting examples of input records with cor-rect output from a training data set. The net-work ‘learns’ to associate a given input withcorrect output by altering its internal weights.A successfully trained network can correctlyclassify input patterns that are similar, but notnecessarily identical to the training patterns
Figure 2. General representation of an artificial neural network neuron consisting of aprocessing node and synaptic input and output connections.

35
(Veselis et al., 1991; Zurada, 1992; Cross etal., 1995).
There are many different types of artificialneural models that use different configurationsand learning rules (Zurada, 1992). A sche-matic representation of an artificial neuron isshown in Figure 2.
The neuron output signal is given by thefollowing general rule:
o = f (w t x) (1)or
(the delta learning rule; Zurada, 1992; Anony-mous, 1998):
(4)
o f w xi ii
n
=
=∑
1
(2)
where w is the weight vector and x is theinput vector. All vectors defined here are col-umn vectors, and superscript t denotes a trans-position. The function f (w t x) is called theactivation function (Zurada, 1992).
In this thesis, the hidden and output neu-rons of the neural models follow continuousnonlinear activation functions of the type:
∑+
=+−
ijiji wowj
e
oθ
1
1 (3)
where o denotes output of a neuron, wji
denote connection weights, oi denotes the out-
put of a neuron in the previous layer, wjθ de-notes the adjustable threshold for the neuron,i denotes the number of inputs to the neuronfrom the previous layer and j denotes the cur-rent neuron (Anonymous, 1998).
Training of the network in this study fol-lowed the delta learning rule, and first involvedinitializing the connection weights to smallrandom numbers. The network then calcu-lated its own output value from the first in-put record and compared this to the targetvalue presented to the output neuron. Thedifference was the error signal. If there was noerror then no learning took place. Otherwise,the interconnecting weights were changed toreduce the error by an amount proportionalto the product of the error signal and the firstderivative of the nonlinear activation function
Neural networks have been used in vari-ous applications in clinical medicine. Ex-amples are diagnostic problems (appendicitis,myocardial infarction, pulmonary embolism),image analysis, waveform analysis (ECG,EEG), and outcome prediction. Best artifi-cial neural models have performed as well, orbetter, than experienced clinicians (Baxt,1995).
In Study 4, artificial neural models wereused for analyzing the physiologic data in thefollowing fashion: All individual data pointsfor heart rate, systolic and diastolic blood pres-sure, end-tidal carbon dioxide (PetCO
2) con-
centration, and arterial blood oxygen satura-tion (SpO
2) throughout the duration of each
anesthetic were entered manually from theanesthesia records into a database, along withage, gender, weight and height. Maximum,minimum and mean values of these variableswere calculated for each patient. The use ofanticholinergic or sympathetic agonist medi-cation may influence the measured physiologicparameters. Therefore, the dose (mg/kg) ofatropine, ethilephrine, or ephedrine given topatients with or without awareness was ana-lyzed and compared with Mann-Whitney test.
The artificial neural networks were config-ured using commercially available neural net-work software (NNModel32®, Neural Fusion,New York, NY) running on a desktop com-puter. The variables used in the analysis, werefirst normalized using the NORMDIST func-tion in Microsoft Excel 5.0 spreadsheet(Microsoft Corporation, Redmond, WA) andsubsequently divided to training and testingdata sets in a random fashion. The trainingdata set consisted of 412 patients withoutawareness and 20 patients with awareness. Thecomplete data of the 20 patients with aware-ness were multiplied fivefold resulting in a

36
training database of 100 records with aware-ness, and 412 without awareness. Theserecords were presented to the neural networkprogram in a random order. The remainingdata of 13 patients with awareness and 98patients without awareness were reserved forthe testing of the trained network.
We used a three-level back-error propaga-tion neural network model, fully intercon-nected between layers (Zurada, 1992; Crosset al., 1995). The summary functions of thephysiologic and demographic parameters indifferent combinations formed the input val-ues to the network, and the outcome was re-ported by a single continuous-function out-put neuron designating target 1 = awarenessand 0 = no awareness. The number of neu-rons in the intermediate (hidden) layer of thenetwork was changed between three and ten.A learning rate of 0.75 and a momentum con-stant a = 0.8 were used for all neural models(Haykin, 1999). The training data matrix waspresented to the network 1,000 times or untilerror tolerance of ±5 % of the total error wasreached, whichever came first. The resultingmodels were analyzed by feeding the test datamatrix values into the network.
The success of randomization of patientsinto training and testing groups was evalu-ated by comparing these groups with chi-squared and Student’s t-tests. The goodnessof the neural models in indicating awarenesswith recall in the testing data set were esti-mated by calculating the sensitivity and speci-ficity of any given model. Subsequently, thelikelihood ratio was calculated as
(5)
The positive and negative predictive val-ues of the test were calculated using the Bayes’theorem (Altman, 1991). The prevalence ofthe condition of interest necessary for this cal-culation was assumed to be 0.5%. Also, pre-diction probability (P
k) as suggested by Smith
et al. (1996) was calculated for the neuralmodels.
The training of the neural models includesreduction of error. The success of this processmay be estimated by calculating the root-meansquare normalized error:
The best neural models were chosen usingthe likelihood ratio as the criterion. The mod-els generated by the study were compared withthe Mann-Whitney test.
where P is the number of training patterns,K is the number of outputs, d is the desired(target) output, and o is the observed output(Zurada, 1992).
Classifying networks, like those in thepresent study, may further be evaluated in theclassifying task by calculating the decision er-ror of the network:
PK
NE err
d = (7)
where N
err is the total number of bit errors
resulting at K thresholded outputs over thecomplete training cycle (Zurada, 1992).
4.5. Feedback informationIn Study 2, feedback information for the car-diac anesthesiologists was used to examine theeffect of that information as a possible way ofreducing the incidence of awareness with re-call. The feedback consisted of general infor-mation of possibilities to reduce consciousawareness during general anesthesia. Writteninformation of the same matter was also in-cluded in the education files of the clinic wherethe study was performed. This informationrecommends continuous use of either inhala-tion or i.v. anesthetic agents, monitoring of
∑∑= =
−=P
p
K
kpkpkrms od
PKE
1 1
2)(1
(6)

37
end-tidal concentrations of inhalation anes-thetic agents, minimizing neuromuscularblockade, and encourages noticing clinicalsigns of light anesthesia. Also specific sugges-tions of dosages for some anesthetic agentscommonly used in cardiac anesthesia weregiven.
4.6. Psychiatric interview andtestingIn Study 1, the patients with awareness wererecruited to a psychiatric interview, testing,and follow-up. Simultaneously matched con-trol patients were included in similar psychi-atric scrutiny. The matching was made for thefollowing factors: age ± 5 years, sex, weight ±5 kg, body mass index ± 3 %, type of surgery,date of surgery ± 3 weeks, and ASA physicalstatus.
If the patients with the experience of aware-ness and the matched control patients wereable and willing to give informed consent, theywere interviewed by a psychiatrist immediatelyafter the operation. If the patient had alreadyleft the hospital, the first interview was doneover the telephone and the first face-to-faceinterview within two weeks after the opera-tion. The patients were re-interviewed 2 and6 months after the operation.
The interviewer was blinded to the pres-ence of absence of awareness during the op-eration. All diagnoses were made accordingto strict DSM-III-criteria by using the Struc-tured Clinical Interview for DSM-III-R NonPatient edition (SCID-NP) (Spitzer et al.,1990a) and Structured Clinical Interview forDSM-III-R-Personality Disorders (SCID-II)(Spitzer et al., 1990b).
Patients completed the Symptom-Check-list-90-Revised (SCL-90-R), a measure of psy-chological distress (Degoratis et al., 1973).SCL-90-R was used to make the diagnosticstructured interview complete. Patients werealso asked to fill out the Impact of Event Scale
(IES), a measure which indexes symptoms thatcharacterize PTSD (Horowitz et al., 1979).
4.7. Statistical methodsDifferences in frequencies were compared withthe chi-squared test (with Yate’s continuitycorrection, as appropriate), except in Study 2where Fisher’s exact test also was used. Forother paired comparisons, Student’s t-test orthe Mann-Whitney U-test was used, accord-ing to the distribution of the data. Analysis ofvariance (ANOVA) was used to detect statis-tical significance of changes in the use of medi-cations over time (Study 1). Post-hoc compari-sons were performed with Tukey’s honestlysignificant test.
The Poisson regression model, a conven-tional statistical technique which allows anadjustment for a rare event such as awarenesswith recall, was used in Studies 1, 3 and 4. Inthe Poisson regression, the relationship be-tween an observed count and a set of explana-tory variables is analyzed with a Poisson dis-tribution. For large n and small p, e.g.,awareness with recall during general anesthe-sia, binomial probabilities are approximatedby the Poisson distribution. The outcome(awareness or no awareness) formed the de-pendent factor in these regression models.Possible factors explaining intraoperativeawareness were entered in the regression asindependent factors. For significant explana-tory factors, relative risk for one unit changeof the explaining factor was calculated.
For some categorical comparisons of twogroups with respect to the risk of awarenessand recall, relative risk estimation was also used(Altman, 1991). 95 % CI based on the Nor-mal distribution or the Poisson distribution,according to the distribution of the data, werealso calculated.
For all statistical tests, a p-value less than0.05 was considered statistically significant.

38
5. Results
5.1. The nature of the experienceof awareness during generalanesthesiaThe patients with awareness and recall fromall the Studies 1-5 are summarized in the Ap-pendix. There were seventy patients who suf-fered from awareness and recall during gen-eral anesthesia. The anesthetics for thesepatients were administered between 1976 and1998 with a median of 1994. Forty (57 %) ofthe patients were female, and thirty (43 %)male. The experience of these patients during
the episode of awareness is summarized inTable 7.
5.2. Incidence of awareness withrecall during general surgeryThe incidence of awareness with recall duringnon-cardiac surgery procedures requiring gen-eral anesthesia is shown in Table 8
5.3. Incidence of awareness withrecall during open heart surgeryThe incidence of awareness with recall during
Table 7. Experiences during episode of awareness. Numbers of patients and percentages of those who responded to the questionare shown.
noitcelloceR
yrotiduA lausiV elitcaT niaP otdeirTevom
otelbAevom
etaidemmIgnidnatsrednu
etaidemmIyteixna
tsomehtsassenerawAecneirepxetnasaelpnu
noitarepognirud
seY24
)7.26(21
)9.71(34
)2.46(22
)9.13(82
)4.28(6
)0.02(35
)8.28(92
)7.16(7
)7.61(
oN52
)3.73(55
)1.28(42
)8.53(74
)1.86(6
)6.71(42
)0.08(11
)2.71(81
)3.83(53
)3.38(
rebmuNdednopser
76 76 76 96 43 03 46 74 24
oNesnopser
3 3 3 1 63 04 6 32 82
latoT 07 07 07 07 07 07 07 07 07

39
open heart surgery is shown in Table 9.
5.4. Differences in anesthetic drugdosing between patients with andwithout awarenessPossible differences in anesthetic agent dos-ing were studied using Poisson regressionmodels. There were differences in the dosingof isoflurane and propofol during anesthesiafor general surgery (Study 1), and midazolamduring cardiac surgery (Study 3) as summa-rized in Tables 10 and 11, respectively.
5.5. Conventional statisticalmethods and artificial neuralnetworks in detecting awarenessfrom monitored physiologicvariablesArtificial neural models and conventional sta-
tistical methods (Poisson regression) were com-pared in Study 4 in relation to their ability todiscriminate between patients with and with-out intraoperative awareness. A total of 52different neural models were tested. The twobest neural models by their ability to identifypatients with awareness in the test data setboth had a likelihood ratio of 11.3. Their sen-sitivity and specificity in the discriminatingtask were 23 % and 98 %, respectively (Fig-ure 3).
Both models had 20 input values: mean,minimum, maximum and number of recordedmeasurements for end-tidal carbon dioxideconcentration, arterial blood oxygen satura-tion, systolic and diastolic blood pressure, andheart rate. The models had 7 and 8 interme-diate layer neurons, and output ranges from -0.299 to 1.176 and from -0.331 to 1.090 in
Table 8. Incidence of awareness during non-cardiac procedures requiring general anesthesia (Study 1).
Awareness Group Awareness / Number of interviews Percentage (95 % CI)
Group 1 9 / 2,612 0.34 (0.16-0.65)
Group 2 6 / 2,612 0.23 (0.08-0.50)
Group 3 4 / 2,612 0.15 (0.04-0.39)
Groups 2-3 10 / 2,612 0.38 (0.18-0.70)
Total 19 / 2,612 0.73 (0.44-1.14)
Table 9. The incidence of awareness during open heat surgery.
Study Awareness Group Awareness / Number of interviews Percentage (95 % CI)
Study 2, Group 3 4 / 99 4.0 (1.1-10.3)year 1992
Study 2. Group 2 1 / 204 0.49 (0.01-2.73)year 1993 Group 3 2 / 204 0.98 (0.12-3.54)
Total 3 / 204 1.5 (0.3-4.3)
Study 3, Group 1 16 / 929 1.72 (0.98-2.80)Year 1995 Group 2 4 / 929 0.43 (0.12-1.10)
Group 3 1 / 929 0.11 (0.003-0.60)Groups 2-3 5 / 929 0.54 (0.17-1.26)
Total 21 / 929 2.26 (1.40-3.46)

40
the test data set, respectively. The root-mean-square normalized errors for these models were0.967 and 0.922, respectively. Decision errorsin the training data set were 0 and 0.0098,respectively. In the test data set, the valuesindicated by the neural models were not dif-ferent between groups of patients with andwithout awareness by Mann-Whitney test.The prediction probabilities P
k (SE) for the
best neural models were 0.66 (0.08) and 0.60(0.10), respectively. If we assume that the in-cidence of awareness with recall is 0.5 %, wecan calculate a negative predictive value of 99.6% for the artificial neural models.
The prognostic significance of the measuredvariables as analyzed with the Poisson regres-
sion are given in Table 12. In this analysis,high systolic blood pressure, high minimumdiastolic blood pressure, and high mean andmaximum heart rate were significant predic-tors of intraoperative awareness with recall.
5.6. The possibility of reducing theincidence of awareness by givingfeedback information to theanesthesiologistsIn study 2, the incidence of awareness fell(from 4 % to 1.5 %, ns.) after the cardiacanesthesiologists received general and feedbackinformation about awareness during anesthe-sia. The relative risk of awareness and recall(95 % CI) in 1992 was 275 % (range 63 -
Table 10. Dose of anesthetic agents given to patients with awareness and recall (groups 1-3) and control patients during generalsurgery. The probability of the Poisson regression model as well as the relative risk derived from the model is also given.
1) The inspiratory concentration that would have been delivered had the total dose of the volatile anesthetic agent beendivided equally to the whole duration of anesthesia.
ssenerawahtiwstneitaP ssenerawatuohtiwstneitaP
esoD esoD
citehtsenA n naideM egnaR n naideM egnaR nossioP(p)ledomnoisserger
enorofksirevitaleResodniegnahctinu
latnepoihT)gk/gm(
8 0.6 3.8-2.4 031 6.5 9.8-2.2 95.0 .A.N
lofoporP)nim/gk/gµ(
01 37 753-32 09 2.822 067-22 30.0 99.0
enarulfosInim/%AAiF( )1 )
21 24.0 57.0-21.0 811 56.0 17.1-50.0 300.0 07.0
enarulfnEnim/%AAiF( )1 )
2 96.0 11.1-62.0 23 85.0 01.1-82.0 .A.N .A.N
lynatneF)nim/gk/gn(
61 14 99-32 361 6.24 032-81 28.0 .A.N
linatneflA)nim/gk/gµ(
3 2.1 8.1-6.0 75 45.1 0.4-2.0 A.N .A.N
muirucartA)nim/gk/gµ(
31 3.9 4.21-4.4 941 1.8 3.76-4.2 27.0 .A.N
samapezaiDnoitacidemerp
)gk/gm(
6 41.0 91.0-70.0 131 51.0 920-70.0 A.N .A.N

41
1204 %) of the risk in 1993. Simultaneously,the use of continuous infusions, or the use ofa combination of an anesthetic infusion andinhalation, increased significantly, from 14 %of the anesthetics to 36 % (p<0.001) and 19% to 56 % (p<0.001), respectively. Also, thedoses of diazepam, fentanyl, and enfluraneincreased while doses of pancuronium de-creased (Table 13).
In Study 1, there was an increase in thedosing of isoflurane over time during the
Table 11. Dose of anesthetic drugs during cardiac surgery given to patients with and without awareness and recall.
ssenerawahtiwstneitaP ssenerawatuohtiwstneitaP
esoD esoD
citehtsenA n naideM egnaR n naideM egnaR nossioP(Pnoisserger
)ledom
enorofksirevitaleResodniegnahctinu
mapezaiD)nim/gk/gµ(
11 74.0 69.0-42.0 311 06.0 10.2-11.0 941.0 .A.N
mapezaroL)nim/gk/gµ(
2 41.0 81.0-01.0 33 71.0 35.0-80.0 194.0 .A.N
malozadiM)nim/gk/gµ(
01 88.0 49.1-64.0 751 41.1 81.3-92.0 740.0 31.0
lofoporP)nim/gk/gµ(
2 5.62 6.84-5.4 42 4.4 2.88-4.0 356.0 .A.N
latnepoihT)nim/gk/gµ(
2 4.11 0.81-8.4 56 7.9 7.94-4.2 317.0 .A.N
linatneflA)nim/gk/gµ(
1 10.1 53 54.1 99.3-92.0 913.0 .A.N
lynatneF)nim/gk/gµ(
31 22.0 23.0-11.0 981 22.0 54.6-20.0 148.0 .A.N
linatnefuS)nim/gk/gµ(
7 40.0 50.0-20.0 97 40.0 81.0-10.0 117.0 .A.N
muinorucnaP)nim/gk/gµ(
02 25.0 28.0-53.0 792 65.0 00.1-60.0 772.0 .A.N
enarulfnEnim/%AAiF( )1 )
7 21.0 36.0-90.0 19 73.0 78.0-40.0 601.0 .A.N
enarulfosInim/%AAiF( )1 )
31 43.0 06.0-41.0 502 33.0 59.0-20.0 987.0 .A.N
1) The inspiratory concentration that would have been delivered had the total dose of the volatile anesthetic been divided
equally to the whole duration of anesthesia.
course of the study. Simultaneously, a decreas-ing trend in awareness was noted. There were,however, no significant changes in the inci-dence of awareness over time during the study(Table 14).
5.7. Psychiatric consequences ofawareness during anesthesiaIn Study 1, seven patients with awareness andrecall were evaluated for psychiatric interviewand follow-up. Two patients had to be ex-

42
cluded from the interview, one because he wasin very poor physical condition and did notremember the experience of awareness, andthe other because she was too incoherent tofollow the structured psychiatric interview.One of the five remaining patients felt intensefear during the experience of awareness andhad some sleep disturbances afterwards. How-ever, she did not meet the criteria of PTSD.None of the other patients followed-up expe-rienced any after-effects. Three of five patientswith awareness had a history of major depres-sion, and preoperative symptoms of depres-sion and anxiety. None of the control grouppatients had any preoperative psychiatric dis-orders. The mental state of the two depressive
patients did not significantly change after theoperation, but one patient was treated withantidepressant medication and recovered.
5.8. Medico-legal consequences ofawareness with recall in FinlandFour insurance claims concerning awarenessduring anesthesia were filed in the PIA be-tween May 1, 1987 and December 31, 1993(Study 5). This represents 0.02 % of all Pa-tient Insurance claims (n = 23,363) filed dur-ing that period. Further cases were collectedfor Study 4: between Jan 1, 1994 and June15, 1997 another seven claims, concerningawareness at least as a part of the complaint,were filed. The details of all these 11 cases with
Figure 3. The values indicated by the two best neural model for each case of the test data set.Each individual bar in the graphs represents the value given by the neural model to eachpatient in the test data set. Patients with awareness are shown by black bars and patientswithout awareness are shown in gray. Value close to 1 indicates awareness with recall whilevalue close to 0 indicates no awareness. The decision threshold (K) between awareness and noawareness is shown as a straight line.

43
Table 12. Demographic and monitored parameters for patients with awareness and recall and those without. Number of patientsanalyzed, median (ranges), and results of the Poisson regression model are given.
ssenerawahtiwstneitaP ssenerawatuohtiwstneitaP noissergernossioP
n )egnar(naidem n )egnar(naidem p enorofksirevitaleRehtniesaercnitinuelbairavehtfoeulav
)sraey(egA 33 )28-32(73 015 )09-21(34 02.0
)m/f(xeS 5/82 731/373 61.0
)mc(thgieH 13 )081-051(861 705 )491-541(761 37.0
)gk(thgieW 23 )211-5.82(07 905 )241-04(86 49.0
xednIssaMydoB 13 )9.73-4.61(5.42 705 )9.24-4.51(4.42 47.0
)%(naem2OCTE 82 )0.6-7.3(7.4 814 )2.6-6.3(7.4 55.0
muminim2OCTE)%(
82 )0.6-4.3(5.4 814 )2.6-2.3(4.4 06.0
mumixam2OCTE)%(
82 )8.7-7.3(9.4 814 )8.6-7.3(0.5 24.0
)%(naem2OaS 62 )001-29(89 794 )001-28(89 33.0
)%(muminim2OaS 52 )001-09(79 694 )001-06(79 09.0
)%(mumixam2OaS 62 )001-69(99 794 )001-49(99 57.0
naemPBcilotsyS)gHmm(
33 )102-57(921 805 )602-08(811 5000.0 30.1
muminimPBcilotsyS)gHmm(
33 )081-55(801 605 )571-55(001 2200.0 30.1
mumixamPBcilotsyS)gHmm(
33 )332-001(051 805 )852-58(541 3800.0 20.1
naemPBcilotsaiD)gHmm(
92 )321-24(77 014 )041-84(57 11.0
PBcilotsaiD)gHmm(muminim
92 )211-43(06 014 )501-53(06 5930.0 30.1
PBcilotsaiD)gHmm(mumixam
92 )251-65(29 014 )541-55(59 3658.0
naemetartraeH)nim/(
33 )711-85(77 805 )021-05(47 8820.0 30.1
muminimetartraeH)nim/(
33 )501-34(66 705 )501-04(56 1252.0
mumixametartraeH)nim/(
33 )051-07(59 805 )061-55(09 2000.0 30.1
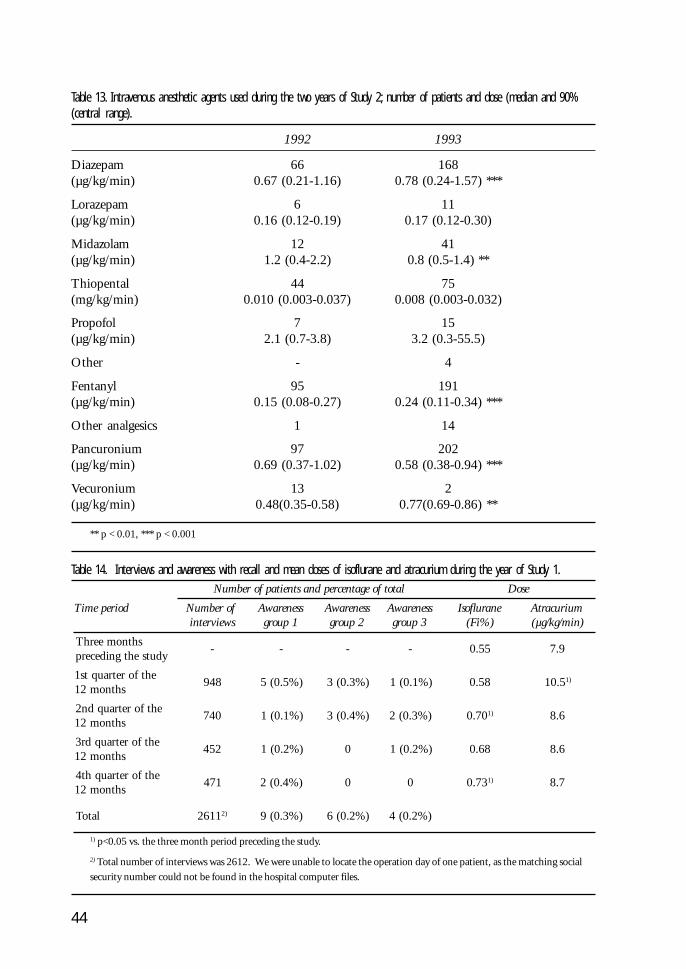
44
Table 13. Intravenous anesthetic agents used during the two years of Study 2; number of patients and dose (median and 90%(central range).
1992 1993
Diazepam 66 168(µg/kg/min) 0.67 (0.21-1.16) 0.78 (0.24-1.57) ***
Lorazepam 6 11(µg/kg/min) 0.16 (0.12-0.19) 0.17 (0.12-0.30)
Midazolam 12 41(µg/kg/min) 1.2 (0.4-2.2) 0.8 (0.5-1.4) **
Thiopental 44 75(mg/kg/min) 0.010 (0.003-0.037) 0.008 (0.003-0.032)
Propofol 7 15(µg/kg/min) 2.1 (0.7-3.8) 3.2 (0.3-55.5)
Other - 4
Fentanyl 95 191(µg/kg/min) 0.15 (0.08-0.27) 0.24 (0.11-0.34) ***
Other analgesics 1 14
Pancuronium 97 202(µg/kg/min) 0.69 (0.37-1.02) 0.58 (0.38-0.94) ***
Vecuronium 13 2(µg/kg/min) 0.48(0.35-0.58) 0.77(0.69-0.86) **
** p < 0.01, *** p < 0.001
Table 14. Interviews and awareness with recall and mean doses of isoflurane and atracurium during the year of Study 1.latotfoegatnecrepdnastneitapforebmuN esoD
doirepemiT forebmuNsweivretni
ssenerawA1puorg
ssenerawA2puorg
ssenerawA3puorg
enarulfosI)%iF(
muirucartA)nim/gk/gµ(
shtnomeerhTydutsehtgnidecerp
- - - - 55.0 9.7
ehtforetrauqts1shtnom21
849 )%5.0(5 )%3.0(3 )%1.0(1 85.0 5.01 )1
ehtforetrauqdn2shtnom21
047 )%1.0(1 )%4.0(3 )%3.0(2 07.0 )1 6.8
ehtforetrauqdr3shtnom21
254 )%2.0(1 0 )%2.0(1 86.0 6.8
ehtforetrauqht4shtnom21
174 )%4.0(2 0 0 37.0 )1 7.8
latoT 1162 )2 )%3.0(9 )%2.0(6 )%2.0(4
1) p<0.05 vs. the three month period preceding the study.
2) Total number of interviews was 2612. We were unable to locate the operation day of one patient, as the matching social
security number could not be found in the hospital computer files.

45
Table 15. The patient claims filed because of awareness during general anesthesia, and the compensations granted.
egA)sry(
xeS)f/m(
ecneirepxE noitarepO noitasnepmoC)MIF(
35 m ymotocarohtafosliateD.niap,noitarepo
ymotocarohT 000,4
72 m ,sliatednoitarepo,noitabutnIniap
ymotcedneppA 006,9
14 f .evomotytilibissopmi,niaP lanimodbafonoitaucavEamotameh
000,5
63 f .evomotytilibani,niaP noitaziliretscipocsorapaL 000,7
73 f .snoissucsiddraeh,niaP ymotcellisnoT 005,4
04 m ssenerawalangisotytilibani,niaP ymotocarohT enoN
54 m dewollofnoitabutxelatnediccAgnitca-gnolgnisunoitabutnieryb
tahtretfA.stnaxalerelcsumfossentrohs,evomotytilibani
rotalitnevnoelihwhtaerb,noitadesroaisehtsenatuohtiw
yteixnaemertxe
ehtnitnemtaertpo-tsoPretfamooryrevocer
ymotorapalafonoitarutuserdnuow
enoN
52 f evitarepofonoitresni,noitabutnIniap,stnemurtsni
ymotcetsycelohccipocsorapaL enoN
74 f htaerbroevomotytilibanI dnalgyrammamafonoisicxEsedonhpmylyrallixadna
005,4
62 f ebutlaehcart,sisylarapfognileeFfonoitresni,taorhtehtni
,niap,stnemurtsnievitareposnoissucsiddraeh
ymotcetsycelohccipocsorapaL 000,8
65 f ssenerawalangisotytilibani,niaPniapdna
ssecsbatoofafonoisicnI 000,5
the compensation granted, if any, is shown inTable 15. The mean age of the 11 cases was39.4 years; four patients were male and sevenfemale. The mean compensation paid was
FIM 4,327 (EUR 727), or FIM 5,950 (EUR1,001) if the patients who were not compen-sated are excluded. The compensation wastechnically granted because of pain.

46
6. Discussion
6.1. Patients’ experiences duringthe episode of intra-anestheticawarenessSeventy patients with awareness during gen-eral anesthesia were analyzed in the presentthesis. Tactile perceptions (recalled by 64 %of patients) were the most common sensorymodality during the episode of awareness. Thiswas followed by pain (32 %) and visual recol-lections (18 %) (Table 7). Paralysis was re-called by 80 % of the thirty patients who re-sponded to this question. These figures aresimilar to those reported previously (Moermanet al., 1993; Schwender et al., 1998; Sandin etal., 2000). Lower incidence of painful aware-ness or sensory perceptions have also been re-ported (Domino et al., 1999). However, basedon the present thesis and other recent studies(Sandin, and Nordström, 1993; Nordströmet al., 1997; Sandin et al., 2000) the incidenceof painful awareness is likely to be higher thanpreviously suggested (Jones, 1994). The ma-jority (83 %) of patients understood immedi-ately that they are aware of the operation anddid not consider their situation as a dream orhallucination. Immediate anxiety over whatis going on was felt by 62 % of the patientsbut, perhaps astonishingly, only 17 % of thepatients with awareness considered the epi-sode of awareness as the worst perioperativeexperience in the early post-operative inter-view.
6.2. Methods used in the presentstudies
6.2.1. Interviews
Structured post-operative interview was usedin Studies 1-3 to detect patients with aware-ness and recall. Interviews are obviously theonly currently available method to find outexperiences and recollections of another per-son. However, the results of an interview, ifnegative, always leave some doubt (Kihlstrom,and Schacter, 1990). The results of an inter-view are not always easy to interpret, and thecontents of a post-operative interview rangefrom no memories through vague, dream-likerecollections to exact verbatim descriptions ofthe occurrences in the operating room. How-ever, the patient’s interpretation of his or hermemories is of importance, and consequently,if the patient interprets a vague memory mean-ing intraoperative awareness, mental after-ef-fects may follow. To complicate things further,it has been shown that recollections immedi-ately after a very traumatizing incident con-tain little or no narrative component, and thepatient may react to the post-operative inter-view only with crying, for example (Van DerKolk, and Osterman, 2000). It has also beenshown by Sandin and co-workers that morethan one interview several weeks apart isneeded as new cases of patients with aware-ness and recall could be found in each inter-

47
view (Sandin et al., 2000). All these problemsaccompanied by the low incidence of aware-ness, and consequently, large samples needed,make the interviews both laborious and time-consuming.
In Study 1, interviews were performed byPACU nurses. Two problems arose from thisarrangement: first, a large number of patientswere not interviewed because the nurses wereengaged in other activities, and second, somecases suggestive of awareness and recall werenot always immediately identified but werenoted only after screening of interview sheetsby the investigators. The problem of low in-terview-rates is not rare in large interview stud-ies (Kapur, 1994), and the investigators wereconvinced that the sample in the Study 1 wasrepresentative of the whole surgical popula-tion. The second problem prevented the re-cruitment all possible cases of awareness,which were eventually found, to the psychiat-ric interviews. This was a major draw-backsince we were not able to describe the patternof possible psychiatric after-effects in a pro-spective manner.
Still another problem is that very sick pa-tients that were treated in the ICU were ex-cluded form the study. It may be that thesepatients do not receive as much anesthetic asother patients because of the severity of theirdisease. Therefore, they may be predisposedto awareness. On the other hand, interview-ing these patients after the ICU is difficult,because the ICU period itself likely producesconfusing recollections (Aitkenhead, 1989;Fu-Jin et al., 1997).
As usual during the time of the studies,only one screening interview was used in Stud-ies 1-3 and, therefore, we probably did notidentify all cases of awareness and recall.
6.2.2. Anesthetic records
Manual anesthetic charts were used for calcu-lating the anesthetic drug doses (Studies 1-3)and values of the measured physiologic vari-
ables (Study 4). It has been shown in manystudies that manual anesthetic charts tend toinclude errors, particularly in the measuredvariables (Junger et al., 1999; Sado, 1999). Itis, therefore, likely that using computer baseddata would have been superior to manualrecords. However, computerized charting wasnot available at the time of these studies.
Some of the cases with awareness and re-call in Study 4 dated from the 1970s. Theremay be systematic changes in the practice ofanesthesiology between those days and the1990s when the control patients’ data wererecorded. However, the study concentrated onphysiologic reactions to intraoperative aware-ness which are not likely to change over thistime span. Furthermore, there were no differ-ences in anticholinergic or sympathomimeticdrug dosing between the patients with andwithout awareness, and the median date ofgeneral anesthesia for the patients studied was1994. Therefore, it is unlikely that the timeof the anesthesia during which awareness oc-curred would have had large effect on thestudy.
6.3. Incidence of awareness withrecall during general surgeryIn Study 1, an overall incidence of awarenesswith recall during general anesthesia was foundto be 0.73 % (Table 8). The incidence ofawareness when counting only patients withsome form of objective memories was 0.38%. However, even these cases included manywhich probably would not be considered torepresent awareness during general anesthe-sia, as they include patients recalling extuba-tion (Patients # 2, 9, 11, 16, 19 in Appen-dix). If all these patients are dropped, we areleft with an incidence of 0.19 %.
Certain difficulties exist in comparing in-cidence figures of awareness with recall dur-ing general anesthesia between different stud-ies. Firstly, to evaluate recall, one needs to relyon the story of the patient. In terms of objec-

48
tive, verifiable facts recalled, different gradesof memories exist, and consequently, classify-ing patients’ memories becomes more or lesssubjective and obscure. Secondly, authors ofthe studies define the time of wakeup fromgeneral anesthesia differently. Some feel thatextubation or residual relaxation and associ-ated breathing difficulties are not awarenessduring anesthesia. We did include these cases,because from a patient’s point of view, there isoften no difference between the intraopera-tive and the immediate postoperative periods(Ho, 2001). Thirdly, very sick patients oftenare excluded from the studies, many times forpractical reasons. These patients are cared forin the ICU, postoperative ventilator therapyand sedation may be needed for variablelengths of time. All this poses considerabledifficulties for the postoperative interviews.Furthermore, the sickest patients may receiveless anesthetics than other patients, and there-fore, may be prone to awareness during anes-thesia. Fourthly, the methodology of assess-ing awareness and recall varies between studies:structured interview is the most popularmethod, but non-structured interviews andinterviews during hypnosis also have beenused. Fifthly, the timing and number of in-terviews used to detect awareness vary betweenstudies.
In Study 1, the incidence of clear, intraop-erative, long-lasting awareness (Grade 3) was0.15 %. This is very similar to the incidencereported by the most recent large study, whichreported an incidence of 0.16 % (Sandin etal., 2000). The criteria behind these figuresseem to be somewhat similar, although the19 patients reported in the study by Sandinand co-workers were further classified intodefinite, probable, and possible categories.These incidence figures are also of the sameorder of magnitude as those published by Liuet al. in 1991 (0.2 %). Earlier large studieshave usually reported slightly higher inci-dences (Table 2).
Sandin and co-workers interviewed theirpatients three times, and found that only sixof 18 patients recalled awareness in the firstinterview in the PACU, 12/18 patients recalledawareness in the second interview 1-3 daysafter anesthesia, and 17/18 in the third inter-view 7-14 days after anesthesia. Based on thesefigures it is likely that in the present Study 1(patients interviewed in the PACU only), andin the studies by Liu et al. (one interview 20-36 hours postoperatively) and by Pedersen andJohansen (1989) (one interview on first post-operative day), the observed incidence ofawareness underestimates the true incidence.It seems, therefore, that the incidence of aware-ness and recall is declining.
In the present Study 1, there were five pa-tients (0.2 %) with recollections related tounpleasant extubation or breathing difficul-ties on awakening. Some of these patients maybe in danger of developing post-operative psy-chiatric complications similar to those withdefinite intraoperative awareness.
6.4. Incidence of awareness withrecall during cardiac surgeryIn Study 2, we report an incidence of aware-ness of 4 % in 1992, and 1.5 % in 1993. Inthis study, grading of memories was not usedbut all of the reported patients recollectedmemories likely of intraoperative origin. Later,one patient (Patient # 24 in Appendix) in thesecond half of Study 2, was considered a short-lasting case of awareness and graduated toGroup 2.
In Study 3, an overall incidence of aware-ness with recall during general anesthesia wasfound to be 2.3 % (Table 9). These patientsalmost certainly include some whose memo-ries originate in the ICU while patients them-selves interpret the memories as intraopera-tive. The incidence of awareness whencounting only patients with some form ofobjective memories was 0.54 %. In this casetoo, there were two patients (Patients # 28

49
and 29 in Appendix) with memories prob-ably originating during transport fromangioplasty into an emergency CABG opera-tion (# 28) and from ICU to the operatingroom for emergency re-sternotomy because ofbleeding (# 29). If these patients are omitted,the incidence of patients with likely intraop-erative awareness was 0.3 %.
Interpreting the results of studies on aware-ness during cardiac anesthesia is influencedby the same factors as the studies on generalsurgery. In addition, all patients are treated inthe ICU for a variable period of time and pa-tients’ interpretation of their recollections canbe different from the interpretation of thehospital or study personnel. The longer thepostoperative intensive care lasts, the morecomplicated matters become. We have there-fore decided not to include patients with post-operative ICU stay over five days.
The incidence found in Study 3 is similarto that found by Dowd et al. (1998) (0.3 %)if only likely cases of true intraoperative aware-ness are counted. It also seems that incidenceof awareness during cardiac surgery has di-minished over the years and is of similar or-der of magnitude, or only slightly higher, thanduring general surgery (Table 3).
6.5. Differences in anesthetic drugdosing between patients with andwithout awarenessThere are few other studies (Phillips et al.,1993) except those presented in this thesis thathave compared the doses of primary anestheticdrugs between patients with and withoutawareness. We noted differences in the dos-ing of isoflurane and propofol in Study 1, andin the dosing of midazolam during cardiacsurgery in Study 3. The mean doses of anes-thetics are smaller in patients with awareness,and therefore a major contribution to the ex-istence of this complication is that not enoughanesthetics are administered to every patient.
One must interpret the results of Studies 1and 3 cautiously in this respect. Firstly, the
same problems apply as for assessing aware-ness: if not all patients with awareness arefound and if patients without awareness areincluded in the wrong groups, the results willbe biased. Secondly, calculating doses of singleanesthetics may not be appropriate as generalanesthesia is not usually the result of a singledrug but a combination of drugs. Therefore,one should be able to create a summary mea-sure of the anesthetic effect of a combinationof i.v. and volatile anesthetics, which is ofcourse, not currently possible. A third prob-lem is that in these studies, awareness and re-call are treated as one phenomenon. In real-ity, we are dealing with two linkedphenomena: awareness during general anes-thesia, and later recall. It seems thatmidazolam, and probably all benzodiazepines,induce profound amnesia but, based on thestudies using IFT, not unconsciousness(Russell, 1993).
6.6. Conventional statisticalmethods and artificial neuralnetworks in detecting awarenessfrom monitored physiologicparametersThe conclusion from the literature is that stan-dard physiologic monitoring is not helpful indetecting awareness during general anesthe-sia. In current anesthesiology practice, how-ever, physiologic monitoring of heart rate,blood pressure, arterial blood oxygen satura-tion, and ventilatory gas composition com-prise the standard monitoring (Rosenberg etal., 1992). Neurophysiologic monitoring, evenif becoming increasingly common, is muchless often used. Even the current Nordic stan-dards suggest that “state of consciousnessshould be clinically observed” (Rosenberg etal., 1992). The concept of following “clinicalsigns” in monitoring consciousness is also con-stantly brought to consideration when discuss-ing awareness during general anesthesia(Gilston, 2000).
Artificial neural models have worked well

50
in detecting complex combination patterns inimaging, waveform analysis, and diagnostics(Baxt, 1995). We therefore wanted to studythe feasibility of this type of artificial intelli-gence in the analysis of data obtained fromstandard physiologic monitors. For a compari-son, conventional statistical methods (Poissonregression) were used as well. The best neuralmodels, picked by the likelihood ratio, had ahigh specificity (98 %) but a low sensitivity(23 %). In the Poisson regression analysis,patients with awareness had higher blood pres-sures and heart rates than patients withoutawareness. Together these findings seem toimply that some patients react to awarenessby change of autonomic monitored param-eters, and that these patients can be picked bythe artificial neural model, while no patternof constant in the group of patients withawareness emerges that can be used to detectthem as a group. This further confirms thatmonitoring of heart rate, blood pressure, andother standard variables is not valuable inmonitoring consciousness. However, aware-ness must be considered as one possible ex-planation for a tachycardia or high blood pres-sure during general anesthesia.
Our studies are limited by the fact that wewere unable to retrospectively pinpoint theexact time of inadequate anesthesia in thepatients who reported recall. Therefore, we hadto use statistical summary functions, such asmean, minimum and maximum, of the ac-tual data. If one knew the timing of aware-ness, actual values measured during that timecould be used for training the neural networkmodels. This could increase the informationvalue of the data. Furthermore, manual datarecords were used in these studies, as not manycomputerized records of patients with aware-ness and recall were available to us. Manualrecords contain errors; for example, true mea-sured highest and lowest values tend to bemissing in manual recordings (Edsall et al.,1993).
6.7. The possibility of reducing theincidence of awareness by givingfeedback information to theanesthesiologistsEducation of practitioners in the field of an-esthesiology is a way to try to reduce aware-ness during general anesthesia (Ghoneim,2001). We had noticed a fairly high incidenceof awareness during cardiac anesthesia in ourunit in 1992. Therefore, information aboutthis anesthesia complication and about itsavoidance was increased in the education filesof the unit. We also decided to estimate theeffect of this increased information and re-peated the structured interview in 1993 (Study2).
Incidence of awareness decreased from 4% to 1.5 % between the study periods, andthe relative risk for awareness in 1992 was 275% (95 % CI 63-1204 %) of the risk in 1993in our unit. Simultaneously, the use constantinfusion of anesthetics or constant use of avolatile anesthetics increased, consumption ofprimary anesthetic agents increased and con-sumption pancuronium (the primary musclerelaxant used in cardiac anesthesia at that time)decreased, all changes proposed in the educa-tional materials.
The change in the incidence of awarenessbetween the years 1992 and 1993 is not sta-tistically significant. However, there seems tobe a decreasing trend in awareness during car-diac surgery starting in 1992 (Table 9). Itseems likely that informing the anesthesiolo-gists about the possibility of awareness andrecall during cardiac anesthesia is one reasonfor the decreasing incidence of this complica-tion.
There are always many reasons for thechange of behavior in anesthesiologists, as wellas other human beings. Therefore, we cannotbe sure that changes in the use of anestheticdrugs and concurrent decrease in the incidenceof awareness were due to the information givento the anesthesiologists. However, there areno other obvious explanations for the change

51
in practice during that particular time. Ourstudy seems to put forth further evidence infavor of the value of education in reducingawareness during anesthesia.
These findings are further supported byfindings during anesthesia for general surgeryin Study 1. In this study, the anesthesiologistswere informed about the nature of the studybut no specific suggestions were given. Themean dosing of isoflurane increased duringthe study compared to the three-month pe-riod immediately preceding the study. Simul-taneously, a decreasing trend in the incidenceof awareness was noted, which, however, wasnot statistically significant at the 95 % level.The anesthesiologists likely changed their wayof anesthetizing patients because they knewthey were being observed in conjunction withan ongoing study.
Another possible conclusion drawn fromthese two studies may be that the studies them-selves and not the information changed thebehavior of the anesthesiologists. The effectof the measurement procedure on the mea-sured variable (Hawthorne effect) is an inher-ent cause of bias in all empirical studies. It isvery difficult to try to eliminate the Hawthorneeffect by blinding the anesthesiologists to alarge ongoing interview study. A possibilityto quantify this bias might be estimating an-esthetic drug dosing before, during, and aftera study of this kind.
6.8. Psychiatric consequences ofawareness during anesthesiaThere is one recent small prospective studyon the incidence of psychiatric complicationsafter awareness with recall during general an-esthesia. In this study, 22 % of patients withprevious awareness and recall had PTSD aftera median of 20 months. The incidence ofPTSD may be even higher because the inves-tigators state that they have reasons to believethat the unwillingness of some patients toparticipate in the study constituted avoidancebehavior, a typical symptom of PTSD. Fur-
thermore, 11 % of the patients with previousawareness experienced some symptoms ofPTSD in the follow-up, although they did notfulfill all criteria of PTSD (Lennmarken et al.,2002).
The studies that have used some form ofadvertising, or complication databases, togather patients who have suffered from aware-ness during anesthesia, tend to have a highnumber of patients suffering PTSD, or otherserious psychiatric after-effects (Cobcroft, andForsdick, 1993; Moerman et al., 1993;Schwender et al., 1998; Domino et al., 1999).In addition, it is likely that the most severelytraumatized patients are not likely to be ableto respond to the advertisements, and controlgroups are lacking in these studies (Wang,2001).
In the study by Bergström and Bernstein,the incidence of psychiatric after-effects wasvery high: four out of six patients were suffer-ing from after-effects a year after the anesthe-sia, and one was in psychiatric care (Bergström,and Bernstein, 1968). In this study, all pa-tients anesthetized by two different methodswere followed.
We found that none of the five patientswith awareness (Study 1), who were recruitedfor psychiatric interview and testing, devel-oped any serious after-effects. One patient hadintense fear that subsided spontaneously. Threeof the five patients had suffered from depres-sion in the past, and one of the three neededantidepressant medication after the awarenessperiod. It seems that the experiences recalledby these patients were not very traumatizingand that serious psychiatric after-effects are notvery common. On the other hand, none ofthe control patients in our Study 1 had anypsychiatric after-effects. Therefore, even if se-rious psychiatric after-effects of awareness areunlikely, sequelae of some sort may be muchmore common.
The number of patients included in thepsychiatric interviews and testing, is howeverquite small, which makes definite conclusions

52
impossible. We were not able to recruit allpatients with possible awareness into the psy-chiatric interview and testing because thesepatients were only found in the retrospectivescrutiny of the interview records. It has alsobeen shown that very traumatic memories tendto be primarily implicit memories with sen-sorimotor or affective nature but little narra-tive component. Patients with traumatizingmemories are able to speak coherently abouttheir traumatic recollections only after vari-able time span (Van Der Kolk, and Osterman,2000). Therefore, it is possible that severelytraumatized patients are missed in the presentStudy 1. This has also been found to be thecase as patients may initially seem to be doingwell after an awareness episode, but later dodevelop psychiatric problems (Lennmarken etal., 2002).
In conclusion, we do not know the currentincidence of psychiatric after effects of intra-operative awareness. It is likely that the inci-dence of severe psychiatric consequences isrelatively high (probably 20-30 %), but also,that some patients will not develop any psy-chiatric after-effects. The scope of psychiatricafter-effects ranges from nil to very trauma-tizing PTSD that may completely ruin the lifeof the patient for many years. Informationabout this possibility should probably be givento surgeons and primary care physicians whoare more likely than anesthesiologists to meetthe patient when the problems become mani-fest.
6.9. Medico-legal consequences ofawareness with recall in FinlandTo my knowledge, there have been no casesof litigation and trial resulting from intraop-erative awareness in Finland. The Patient In-jury Act, effective since May 1, 1987 in Fin-land, states that compensation for patientinjury is payable after injury from medicaltreatment. The PIA handles all the claims,makes the decisions and pays the compensa-tions. The basic principle of the no fault
scheme is that the patient does not sue throughthe courts, but submits an insurance claimwhich will bring compensation if the insurersare satisfied that the injury was caused by thetreatment. Consideration will, however, begiven to unavoidable consequences of therapyand to necessary risk-taking by health careproviders. This insurance scheme allows pa-tients to be compensated for injuries arisingfrom medical treatment without the need toprove fault and causation through adversariallitigation.
In Study 5, we studied insurance claimssubmitted to PIA between May 1, 1987 andDecember 31, 1993. Four claims because ofawareness during general anesthesia had beenfiled representing one insurance claim forabout 350,000 general anesthetics. During thesame time period, 391 claims had been filedfor anesthesia care, giving for awareness dur-ing general anesthesia a 1 % share of claimsagainst the anesthetic practice.
Between January 1, 1994 and June 15,1997 another seven insurance claims result-ing from anesthetic awareness were filed (Study4). One insurance claim every twenty monthswas filed from 1987 to 1993, and one everysix months from 1994 to 1997. Compensa-tion was granted in 73 % of the cases; theaverage award was EUR 1,001.
Of the 4,183 claims in the ASA ClosedClaims Project database (Domino et al., 1999)79 (1.9 %) were filed because of awarenessduring anesthesia. Compensations rangedfrom USD 1,000 to 600,000. High compen-sation (GBP 13,000) for awareness duringanesthesia has also been reported in the U.K(Domino, and Aitkenhead, 2001).
In conclusion, the medicolegal conse-quences of awareness during general anesthe-sia in Finland have been relatively rare, al-though there may be a slightly increasingtrend. Compensations granted for pain andawareness during anesthesia have been smallaccording to the policy of the PIA to keepcompensations for immaterial loss low.

53
7. Conclusions
1. The incidence of awareness during generalanesthesia for general surgery seems to bein slow, constant decline. The current inci-dence of undisputed intraoperative aware-ness is about 0.1-0.2 % of all general anes-thetics. If cases of unpleasant awakeningare counted, the incidence is about 0.4 %,and if cases with possible awareness are in-cluded, the incidence is 0.7 %.
2. The incidence of awareness during anes-thesia for cardiac surgery is also in decline.Current estimate of the incidence of un-disputed intraoperative awareness is 0.3 %of all cases of cardiac anesthesia. If all pos-sible cases of awareness are counted, theincidence is 2.3 %. Incidence of awarenessduring cardiac surgery was previously muchhigher than during general surgery but ithas come down to a level almost similar tothe incidence during general surgery.
3. Lower doses of anesthetics were used forpatients with awareness than for those with-out, during anesthesia for general surgery:isoflurane 0.42 Fi% vs. 0.65 Fi% andpropofol 73 µg/kg/min vs. 228 µg/kg/min,respectively (Study 1).Lower dose of midazolam was used duringcardiac surgery: 0.8 µg/kg/min vs. 1.1 µg/kg/min (Study 3).A principal factor for the existing measur-
able incidence of awareness during anes-thesia is the use of an insufficient concen-tration of anesthetic for the patient’s need.
4. Standard physiologic monitoring is not re-liable for monitoring consciousness duringgeneral anesthesia. Even with computer-based artificial intelligence, it is currentlynot possible to create systems able to reli-ably distinguish between patients with andwithout awareness. However, patients withawareness as a group tend to have higherblood pressure and heart rate than patientswithout awareness.
5. Information about awareness during gen-eral anesthesia, and means of preventing itlead to a lowering trend of its incidence.Concurrently, there was increase in the con-sumption of primary anesthetics and de-crease in the consumption of pancuroniumduring cardiac surgery. All these changeswere suggested in the information given.It is likely that information given to anes-thesiologists leads into a change in theirpractice of anesthetizing patients.
6. Psychiatric after-effects of awareness dur-ing general anesthesia range from no ef-fects to invalidating chronic PTSD. Cur-rent incidence of serious psychiatricafter-effects is not known, but it is likely

54
that a significant number (possibly 20-30%) of patients suffer from serious psychi-atric consequences.
7. Awareness during general anesthesia hastriggered a small number of Patient Insur-
ance claims in Finland (about 1 % of anes-thesia-related claims). Seventy percent ofthe patients who have submitted insuranceclaims have received compensations forpain, the mean amount of compensationbeing EUR 1,000.

55
8. Practical considerations
A practical goal for an anesthesiologist is asafe general anesthesia without awareness and,certainly, without post-operative recall. Thereis currently no evidence that any kind of pre-medication, or withholding premedication forthat matter, would affect the incidence ofawareness and recall. Therefore, the choice ofpremedication should be based on other con-siderations of patient safety, comfort, and re-quirements of surgery. There is currently noconsensus on whether the patients should beforewarned about the possibility of awarenessduring general anesthesia. Some have, how-ever, suggested that this might give the pa-tient better chances of coping with possibleawareness and that mental after-effects wouldbe more unlikely (Holt, and Yate, 1993). Cer-tainly, discussing this matter is wise if the an-esthesiologist foresees a need for very lightanesthesia for some reason.
General anesthesia may be induced withany inhaled or i.v. anesthetic drugs. The doseof the chosen drug should be large enough tocover the stimulus of possible endotrachealintubation. If prolonged laryngoscopy is re-quired, one should not forget to maintaingeneral anesthesia with supplemental doses ofthe induction agent or with a potent inhala-tional anesthetic. During the operation, an-esthesia should be maintained with continu-ous administration of an anesthetic, whetherthat be i.v. or inhaled. Anesthetics should be
administered in such amounts that uncon-sciousness is maintained until the patient’strachea is extubated and muscle strength hasrecovered to sufficient amount to sustain nor-mal breathing. A technique relying on N
2O,
whether supplemented with an opioid or not,to maintain general anesthesia, is not accept-able. There is some evidence that desflurane,isoflurane, and sevoflurane cause unconscious-ness and amnesia in lower concentration rela-tive to their MAC
skin incision than halothane
(Eger, 2001). Therefore, the use of these in-haled anesthetics would be wise if hemody-namic instability is encountered. The main-tenance of anesthesia with large doses ofbenzodiazepines, with or without opioidsupplementation, would probably cause am-nesia but not unconsciousness. Therefore, thistechnique is not as good as using potent in-haled or i.v. general anesthetics. However,there is currently no evidence that awarenesswithout later recall is detrimental to the pa-tient, and in critical hemodynamic situationusing benzodiazepines instead of general an-esthetics may be acceptable. NMBs should beused as sparingly as possible unless indicatedfor surgery or intubation.
There is currently no evidence that aware-ness and recall could be prevented by moni-toring consciousness with sophisticated meth-ods, such as AEP or BIS. However, any clinicalsigns are much more unreliable in this respect

56
and, certainly, it would be wise to use EEG-based monitoring if a patient has a history ofawareness and recall under anesthesia. Someof these patients have abnormal pharmacoki-netic or –dynamic profiles, and monitoringthe effect of the anesthetic drugs on the effec-tor site (brain) should be used.
If a patient after all has suffered form aware-ness and recalls this postoperatively, psychiat-ric consultation and follow-up is recom-mended. Quality control programs, such aspostoperative interviews or surveys, shouldincorporate questions revealing possible casesof intraoperative awareness.

57
9. Future implications
It seems that prospective, multi-center stud-ies would be needed to establish after-effectsof awareness and recall during anesthesia, aswell as, the after-effects of awareness, or wake-fulness, without recall. There is evidence, pre-sented in this thesis, too, that awareness andrecall may be followed by detrimental after-effects, but less evidence exists about the pos-sibility of negative after-effects after wakeful-ness without later recall. An associatedquestion is the effect of drugs that have effecton memory but are not likely to be anesthet-ics in the sense of being able to suppress con-sciousness and prevent wakefulness duringgeneral anesthesia. Benzodiazepines are themost notorious example of such drugs. Thesedrugs are also often used as component ofmodern general anesthesia.
The question of monitoring consciousnessduring general anesthesia is also important.Monitoring the central nervous system func-tion with currently available methods is fairlyexpensive. It is suggested, but not shown, thatawareness and recall may be prevented by thesemodes of monitoring (Kelly et al., 2000). Aparticular problem of all the methods (BISand AEP) available today is that they are ret-rospective in the sense that the result displayedby the monitoring systems represents time 10-30 seconds past the present. If the patient isconscious at the present time, it will only bedisplayed a minute later (Rosow, and
Manberg, 1998). It is not established, whetheractions taken a few minutes after the occur-rence of consciousness during general anes-thesia are able to prevent all negative after-effects.
The problem of all studies on awarenesswith and without recall is the large amount ofpatients needed (O’Connor et al., 2001).Multi-center studies are obviously necessaryto overcome these problems. In addition, theamount of labor needed, for example, to showa 50 % fall in the incidence of awareness andrecall from the current level using a hypotheti-cal new technique, would require three to fiveyears of labor only to complete the structuredinterviews. Even though we are dealing witha very basic dilemma of anesthesiology – con-sciousness – it is questionable whether or notsuch an investment of time and money wouldbe worthwhile.
There are no studies on the incidence ofawareness and recall in children. The generalanesthetics during childhood, however, maybe somewhat different from that used inadults. The fact that the ability to conductstructured interviews diminishes as the age ofthe target group decreases, makes collectionof accurate data in children with current meth-odology difficult if not impossible. A tech-nique suitable for evaluating awareness andrecall in children would be most welcome.

58
Acknowledgements
These studies were carried out at the Depart-ment of Anaesthesiology and Intensive CareMedicine, Helsinki University Central Hos-pital and at the Department of Anesthesiol-ogy, Päijät-Häme Central Hospital, Lahti.Patient cases were also recruited from the ar-chives of the Patient Insurance Association ofFinland.
I express my sincere gratitude to the headof the Department of Anaesthesiology andIntensive Care Medicine, Helsinki UniversityCentral Hospital, Professor Per Rosenberg,MD, PhD. Professor Rosenberg has in manyways, both mentoring and financing, encour-aged the process of creating this thesis. I willalso wish to thank Professor Emeritus TapaniTammisto, MD, PhD, the former head of theDepartment of Anaesthesiology in theHelsinki University Central Hospital, for hisgreat interest and support of my studies.
I am grateful to the head of the Depart-ment of Anesthesiology, Päijät-Häme CentralHospital, Lahti, Dr. Timo Ali-Melkkilä, MD,PhD. He has co-authored one of the studiesand made it possible to study the patients ofhis department.
Docent Markku Hynynen, MD, PhD hassupervised this thesis. He introduced me withthe subject of awareness during anesthesia; hehas thought me basic ideas of scientific think-ing and hard work. Markku has always beenpromptly available despite of his many activi-
ties when help has been needed. I owe himmy sincere gratitude.
I wish to thank Professor Harry Scheinin,MD, PhD and Docent Arvi Yli-Hankala,MD, PhD for the thorough and constructivecriticism of this thesis.
I am grateful to Professor Jukka Räsänen,MD, PhD, for teaching me ideas of clinicalscience and basics of artificial intelligence. Iwill also thank Jukka for the language revi-sion of this thesis.
I thank Docent Ulla Aromaa, MD, PhD,for an opportunity to do clinical and scien-tific work under her supervision. Ulla has alsobeen an invaluable contact between me andthe Patient Insurance Association.
I thank Ms Johanna Saario, RN, and MsPirkko Herranen, RN, for their great help inmanaging the patient interviews. The comple-tion of this thesis would not have been pos-sible without their contribution.
I am indebted to Dr. Riitta Laurila, MD,for performing the psychiatric interviews andtesting Also, I wish to thank Dr. Janne Jussila,MD, for his contribution in the study ofawareness during cardiac anesthesia.
I am grateful to Professor Seppo Sarna, PhDfor his advice with the statistical problems. Ithank Mr Arttu Laine, MSc, and Ms HannaTolonen, MSc, for performing the Poisson re-gressions of these studies.
I wish to thank all the nursing staff of the

59
Department of Anesthesiology of the Päijät-Häme Central Hospital, Lahti, for their in-valuable contribution to the patient interviews.I also thank all of my colleagues in Helsinkiand Lahti for their support.
I am most grateful to my parents, Eila andVeikko Ranta, for the best possible upbring-ing, creating an atmosphere of love in mychildhood home, and for their never-endingsupport in all fields of life. I also thank mymother-in-law, Anna-Liisa Lahti, and my sis-
ters and sisters and brothers-in-law for theirinterest and support.
The greatest gratitude of all I owe to mywife Dr. Varpu Ranta, MD, PhD, and to ourchildren Henrik and Kirsti.
This study was financially supported by theFinnish Medical Foundation, the FinnishMedical Society Duodecim, the Finnish-Nor-wegian Medical Foundation, and the Instru-mentarium Foundation of Science, which aregratefully acknowledged.

60
References
AnonymousAnonymousAnonymousAnonymousAnonymous. Awareness during anaesthesia. BMJ 1: 977, 1976.
AnonymousAnonymousAnonymousAnonymousAnonymous. Awareness in general anaesthesia. BMJ 280: 811, 1980.
AnonymousAnonymousAnonymousAnonymousAnonymous. Webster’s encyclopedic unabridged dictionary ofthe English language. New York: Portland House, 1989.
AnonymousAnonymousAnonymousAnonymousAnonymous. NNModel32 Version 1.0 User’s manual. New York,NY: Neural Fusion, 1998.
AnonymousAnonymousAnonymousAnonymousAnonymous. Precedents of the Finnish Supreme Court. http://www.finlex.fi/oikeus/index.html. Accessed: 4.1.2002.
Abouleish E, TAbouleish E, TAbouleish E, TAbouleish E, TAbouleish E, Taylor FHaylor FHaylor FHaylor FHaylor FH. Effect of morphine-diazepam on signs ofanesthesia, awareness, and dreams of patients under N2O for ce-sarean section. Anesth Analg 55: 702-5, 1976.
Agarwal G, Sikh SSAgarwal G, Sikh SSAgarwal G, Sikh SSAgarwal G, Sikh SSAgarwal G, Sikh SS. Awareness during anaesthesia. A prospectivestudy. Br J Anaesth 49: 835-8, 1977.
Aitkenhead ARAitkenhead ARAitkenhead ARAitkenhead ARAitkenhead AR. Analgesia and sedation in intensive care. Br JAnaesth 63: 196-206, 1989.
Aitkenhead ARAitkenhead ARAitkenhead ARAitkenhead ARAitkenhead AR. Awareness during anaesthesia: what should thepatient be told? Anaesthesia 45: 351-2, 1990.
Aldrete JA, WAldrete JA, WAldrete JA, WAldrete JA, WAldrete JA, Wright AJright AJright AJright AJright AJ. Concerning the acceptability of awarenessduring surgery. Anesthesiology 63: 460-1, 1985.
Altman DGAltman DGAltman DGAltman DGAltman DG. Practical statistcs for medical research. London:Chapman & Hall, 1991.
Andrade J, Baddeley AAndrade J, Baddeley AAndrade J, Baddeley AAndrade J, Baddeley AAndrade J, Baddeley A. Human memory and anesthesia. Int AnesthClin 31: 39-51, 1993.
Baddeley ABaddeley ABaddeley ABaddeley ABaddeley A. Human memory, theory and practice. Hove:Lawrence Erlbaum Associates, 1990.
Bailey AR, Jones JGBailey AR, Jones JGBailey AR, Jones JGBailey AR, Jones JGBailey AR, Jones JG. Patients’ memories of events during generalanaesthesia. Anaesthesia 52: 460-76, 1997.
Baraka A, Louis FBaraka A, Louis FBaraka A, Louis FBaraka A, Louis FBaraka A, Louis F, Noueihid R, Diab M, Dabbous A, Sibai A, Noueihid R, Diab M, Dabbous A, Sibai A, Noueihid R, Diab M, Dabbous A, Sibai A, Noueihid R, Diab M, Dabbous A, Sibai A, Noueihid R, Diab M, Dabbous A, Sibai A.Awareness following different techniques of general anaesthesia forcaesarean section. Br J Anaesth 62: 645-8, 1989.
Barr AM, WBarr AM, WBarr AM, WBarr AM, WBarr AM, Wong RMong RMong RMong RMong RM. Awareness during general anaesthesia forbronchoscopy and laryngoscopy using the apnoeic oxygenationtechnique. Br J Anaesth 45: 894-900, 1973.
Baxt WGBaxt WGBaxt WGBaxt WGBaxt WG. Application of artificial neural networks to clinical med-icine. Lancet 346: 1135-8, 1995.
Bennett HBennett HBennett HBennett HBennett H. Response to intraoperative converation, in response.Br J Anaesth 58: 134-5, 1986.
Bergström H, Bernstein KBergström H, Bernstein KBergström H, Bernstein KBergström H, Bernstein KBergström H, Bernstein K. Psychic reactions after analgesia withnitrous oxide for caesarean section. Lancet 2: 541-2, 1968.
Blacher RSBlacher RSBlacher RSBlacher RSBlacher RS. On awakening paralyzed during surgery. A syndromeof traumatic neurosis. JAMA 234: 67-8, 1975.
Blacher RSBlacher RSBlacher RSBlacher RSBlacher RS. Awareness during surgery. Anesthesiology 61: 1-2,1984.
Bogetz MS, Katz JABogetz MS, Katz JABogetz MS, Katz JABogetz MS, Katz JABogetz MS, Katz JA. Recall of surgery for major trauma. Anesthe-siology 61: 6-9, 1984.
Bogod DGBogod DGBogod DGBogod DGBogod DG. Detecting awareness during general anaesthesia. An-aesthesia 45: 590, 1990.
Bogod DG, Orton JK, YBogod DG, Orton JK, YBogod DG, Orton JK, YBogod DG, Orton JK, YBogod DG, Orton JK, Yau HM, Oh TEau HM, Oh TEau HM, Oh TEau HM, Oh TEau HM, Oh TE. Detecting awareness dur-ing general anaesthetic caesarean section. An evaluation of twomethods. Anaesthesia 45: 279-84, 1990.
Breckenridge J, Aitkenhead ARBreckenridge J, Aitkenhead ARBreckenridge J, Aitkenhead ARBreckenridge J, Aitkenhead ARBreckenridge J, Aitkenhead AR. Isolated forearm technique fordetection of wakefulness during general anaesthesia. Br J Anaesth52: 665P, 1981.
Brice DD, Hetherington RR, Utting JEBrice DD, Hetherington RR, Utting JEBrice DD, Hetherington RR, Utting JEBrice DD, Hetherington RR, Utting JEBrice DD, Hetherington RR, Utting JE. A simple study of aware-ness and dreaming during anaesthesia. Br J Anaesth 42: 535-42,1970.
Browne RA, Catton DVBrowne RA, Catton DVBrowne RA, Catton DVBrowne RA, Catton DVBrowne RA, Catton DV. A study of awareness during anesthesia.Anesth Analg 52: 128-32, 1973a.
Browne RA, Catton DVBrowne RA, Catton DVBrowne RA, Catton DVBrowne RA, Catton DVBrowne RA, Catton DV. . . . . Awareness during anaesthesia: A compar-ison of anaesthesia with nitrous oxide – oxygen and nitrous oxide– oxygen with Innovar®. Canad Anaesth Soc J 20: 763-8, 1973b.
Chortkoff BS, Bennett HL, Eger EIIChortkoff BS, Bennett HL, Eger EIIChortkoff BS, Bennett HL, Eger EIIChortkoff BS, Bennett HL, Eger EIIChortkoff BS, Bennett HL, Eger EII. Does nitrous oxide antago-nize isoflurane-induced suppression of learning? Anesthesiology79: 724-32, 1993.
Chortkoff BS, Eger EII, Crankshaw DPChortkoff BS, Eger EII, Crankshaw DPChortkoff BS, Eger EII, Crankshaw DPChortkoff BS, Eger EII, Crankshaw DPChortkoff BS, Eger EII, Crankshaw DP, Gonsowski CT, Gonsowski CT, Gonsowski CT, Gonsowski CT, Gonsowski CT, Dutton, Dutton, Dutton, Dutton, DuttonRC, Ionescu PRC, Ionescu PRC, Ionescu PRC, Ionescu PRC, Ionescu P. Concentrations of desflurane and propofol thatsuppress response to command in humans. Anesth Analg 81: 737-43, 1995.
Clark DL, Rosner BSClark DL, Rosner BSClark DL, Rosner BSClark DL, Rosner BSClark DL, Rosner BS. Neurophysiologic effects of general anes-thetics: I . The electroencephalogram and sensory evoked respons-

61
es in man. Anesthesiology 38: 564-82, 1973.
Cobcroft MD, Forsdick CCobcroft MD, Forsdick CCobcroft MD, Forsdick CCobcroft MD, Forsdick CCobcroft MD, Forsdick C. Awareness under anaesthesia: the pa-tients’ point of view. Anaesth Intensive Care 21: 837-43, 1993.
Cormack RSCormack RSCormack RSCormack RSCormack RS. Conscious levels during anaesthesia. Br J Anaesth71: 469-71, 1993.
Crawford JSCrawford JSCrawford JSCrawford JSCrawford JS. Awareness during operative obstetrics under generalanaesthesia. Br J Anaesth 43: 179-82, 1971.
Crawford JS, Lewis M, Davies PCrawford JS, Lewis M, Davies PCrawford JS, Lewis M, Davies PCrawford JS, Lewis M, Davies PCrawford JS, Lewis M, Davies P. Maternal and neonatal respons-es related to the volatile agent used to maintain anaesthesia at cae-sarean section. Br J Anaesth 57: 482-7, 1985.
Crawford JSCrawford JSCrawford JSCrawford JSCrawford JS. Fetal well-being and maternal awareness. Br J An-aesth 61: 247-9, 1988.
Critchley MCritchley MCritchley MCritchley MCritchley M. Butterworths Medical Dictionary (2 ed.). London:Butterworth & Co (Publishers) Ltd, 1978, p. 1942.
Cross SS, Harrison RFCross SS, Harrison RFCross SS, Harrison RFCross SS, Harrison RFCross SS, Harrison RF, Kennedy RL, Kennedy RL, Kennedy RL, Kennedy RL, Kennedy RL. Introduction to neural net-works. Lancet 346: 1075-9, 1995.
Cundy JMCundy JMCundy JMCundy JMCundy JM. Post traumatic stress disorders. Br J Anaesth 75: 501-2,1995.
Cundy JM, Dasey NCundy JM, Dasey NCundy JM, Dasey NCundy JM, Dasey NCundy JM, Dasey N. An audit of stress disorders related to anaes-thesia. In: Memory and awareness in anaesthesia III, Bonke B,Bovill JG, Moerman N, eds. Assen: Van Gorcum, 1996: 143-50.
Degoratis LR, Lipman RS, Covi LDegoratis LR, Lipman RS, Covi LDegoratis LR, Lipman RS, Covi LDegoratis LR, Lipman RS, Covi LDegoratis LR, Lipman RS, Covi L. An out-patient rating scale:preliminary report. Psychophramacol Bull 9: 13-28, 1973.
Desiderio DPDesiderio DPDesiderio DPDesiderio DPDesiderio DP, Thorne AC, Thorne AC, Thorne AC, Thorne AC, Thorne AC. Awareness and general anaesthesia. ActaAnaesthesiol Scand Suppl 92: 48-50, 1990.
Domino KB, Posner KL, Caplan RA, Cheney FWDomino KB, Posner KL, Caplan RA, Cheney FWDomino KB, Posner KL, Caplan RA, Cheney FWDomino KB, Posner KL, Caplan RA, Cheney FWDomino KB, Posner KL, Caplan RA, Cheney FW. Awareness dur-ing anesthesia: a closed claims analysis. Anesthesiology 90: 1053-61, 1999.
Domino KB, Aitkenhead ARDomino KB, Aitkenhead ARDomino KB, Aitkenhead ARDomino KB, Aitkenhead ARDomino KB, Aitkenhead AR. Medicolegal consequences of aware-ness during anesthesia. In: Awareness during anesthesia, Gho-neim MM, ed. Oxford: Butterworth-Heinemann, 2001: 155-72.
Dowd NPDowd NPDowd NPDowd NPDowd NP, Cheng DC, Karski JM, W, Cheng DC, Karski JM, W, Cheng DC, Karski JM, W, Cheng DC, Karski JM, W, Cheng DC, Karski JM, Wong DTong DTong DTong DTong DT, Munro JAC, Sandler, Munro JAC, Sandler, Munro JAC, Sandler, Munro JAC, Sandler, Munro JAC, SandlerANANANANAN. Intraoperative awareness in fast-track cardiac anesthesia. An-esthesiology 89: 1068-73, 1998.
Drummond JCDrummond JCDrummond JCDrummond JCDrummond JC. Monitoring depth of anesthesia: with emphasis onthe application of the bispectral index and the middle latency au-ditory evoked response to the prevention of recall. Anesthesiology93: 876-82, 2000.
Dutton RC, Smith WD, Smith NTDutton RC, Smith WD, Smith NTDutton RC, Smith WD, Smith NTDutton RC, Smith WD, Smith NTDutton RC, Smith WD, Smith NT. Wakeful response to commandindicates memory potential during emergence from general anes-thesia. J Clin Monit 11: 35-40, 1995.
Dwyer R, Bennett HL, Eger EId, Heilbron DDwyer R, Bennett HL, Eger EId, Heilbron DDwyer R, Bennett HL, Eger EId, Heilbron DDwyer R, Bennett HL, Eger EId, Heilbron DDwyer R, Bennett HL, Eger EId, Heilbron D. Effects of isofluraneand nitrous oxide in subanesthetic concentrations on memory andresponsiveness in volunteers. Anesthesiology 77: 888-98, 1992.
Edsall DWEdsall DWEdsall DWEdsall DWEdsall DW, Deshane P, Deshane P, Deshane P, Deshane P, Deshane P, Giles C, Dick D, Sloan B, Farrow J, Giles C, Dick D, Sloan B, Farrow J, Giles C, Dick D, Sloan B, Farrow J, Giles C, Dick D, Sloan B, Farrow J, Giles C, Dick D, Sloan B, Farrow J. Com-puterized patient anesthesia records: less time and better qualitythan manually produced anesthesia records. J Clin Anesth 5: 275-83, 1993.
Eger EI, Saidman LJ, Brandstater BEger EI, Saidman LJ, Brandstater BEger EI, Saidman LJ, Brandstater BEger EI, Saidman LJ, Brandstater BEger EI, Saidman LJ, Brandstater B. Minimum alveolar concen-tration: A standard of anesthetic potency. Anesthesiology 26: 756-
63, 1965.
Eger EIEger EIEger EIEger EIEger EI. Does 1 + 1 = 2? Anesth Analg 68: 551-2, 1989.
Eger EIEger EIEger EIEger EIEger EI. Age, minimum alveolar anesthetic concentration, andminimum alveolar anesthetic concentration-awake. Anesth Analg93: 947-53, 2001.
Eger EIEger EIEger EIEger EIEger EI. A brief history of the origin of minimum alveolar concen-tration (MAC). Anesthesiology 96: 238-9, 2002.
Evans JM, Davies WLEvans JM, Davies WLEvans JM, Davies WLEvans JM, Davies WLEvans JM, Davies WL. Monitoring anaesthesia. Clin Anasthesiol2: 243-62, 1984.
Farnsworth GMFarnsworth GMFarnsworth GMFarnsworth GMFarnsworth GM. Enflurane and the incidence of awareness inCaesarean section. Anaesthesia 33: 553, 1978.
Fu-Jin S, Shu-Hsun C, Po-Jui YFu-Jin S, Shu-Hsun C, Po-Jui YFu-Jin S, Shu-Hsun C, Po-Jui YFu-Jin S, Shu-Hsun C, Po-Jui YFu-Jin S, Shu-Hsun C, Po-Jui Y, W, W, W, W, Wen-Yen-Yen-Yen-Yen-Yu H, Guey-Shiun Hu H, Guey-Shiun Hu H, Guey-Shiun Hu H, Guey-Shiun Hu H, Guey-Shiun H. Turn-ing points of recovery from cardiac surgery during the intensivecare unit transition. Heart Lung 26: 99-108, 1997.
Galinkin JL, Janiszewski D, YGalinkin JL, Janiszewski D, YGalinkin JL, Janiszewski D, YGalinkin JL, Janiszewski D, YGalinkin JL, Janiszewski D, Young CJ, Klafta JM, Klock Poung CJ, Klafta JM, Klock Poung CJ, Klafta JM, Klock Poung CJ, Klafta JM, Klock Poung CJ, Klafta JM, Klock PA, Coal-A, Coal-A, Coal-A, Coal-A, Coal-son DWson DWson DWson DWson DW, Apfelbaum JL, Zacny JP, Apfelbaum JL, Zacny JP, Apfelbaum JL, Zacny JP, Apfelbaum JL, Zacny JP, Apfelbaum JL, Zacny JP. Subjective, psychomotor, cogni-tive, and analgesic effects of subanesthetic concentrations of sevof-lurane and nitrous oxide. Anesthesiology 87: 1082-8, 1997.
Ghoneim MM, Mewaldt SPGhoneim MM, Mewaldt SPGhoneim MM, Mewaldt SPGhoneim MM, Mewaldt SPGhoneim MM, Mewaldt SP. Benzodiazepines and human memo-ry: a review. Anesthesiology 72: 926-38, 1990.
Ghoneim MM, Block RIGhoneim MM, Block RIGhoneim MM, Block RIGhoneim MM, Block RIGhoneim MM, Block RI. Learning and consciousness during gen-eral anesthesia. Anesthesiology 76: 279-305, 1992.
Ghoneim MM, Block RIGhoneim MM, Block RIGhoneim MM, Block RIGhoneim MM, Block RIGhoneim MM, Block RI. Learning and memory during generalanesthesia: an update. Anesthesiology 87: 387-410, 1997.
Ghoneim MMGhoneim MMGhoneim MMGhoneim MMGhoneim MM. Awareness during anesthesia. Anesthesiology 92:597-602, 2000.
Ghoneim MM, Block RI, Dhanaraj VJ, TGhoneim MM, Block RI, Dhanaraj VJ, TGhoneim MM, Block RI, Dhanaraj VJ, TGhoneim MM, Block RI, Dhanaraj VJ, TGhoneim MM, Block RI, Dhanaraj VJ, Todd MM, Choi WWodd MM, Choi WWodd MM, Choi WWodd MM, Choi WWodd MM, Choi WW,,,,,Brown CKBrown CKBrown CKBrown CKBrown CK. Auditory evoked responses and learning and aware-ness during general anesthesia. Acta Anaesthesiol Scand 44: 133-43, 2000.
Ghoneim MMGhoneim MMGhoneim MMGhoneim MMGhoneim MM. Awareness during anesthesia. In: Awareness dur-ing anesthesia, Ghoneim MM, ed. Oxford: Butterworth-Heinemann,2001: 1-22.
Gilston AGilston AGilston AGilston AGilston A. Awareness during anaesthesia. Lancet 355: 1722, 2000.
Goldmann L, Shah MVGoldmann L, Shah MVGoldmann L, Shah MVGoldmann L, Shah MVGoldmann L, Shah MV, Hebden MW, Hebden MW, Hebden MW, Hebden MW, Hebden MW. Memory of cardiac anaes-thesia. Psychological sequelae in cardiac patients of intra-opera-tive suggestion and operating room conversation. Anaesthesia 42:596-603, 1987.
Gonsowski CTGonsowski CTGonsowski CTGonsowski CTGonsowski CT, Chortkoff BS, Eger EII, Bennett HL, W, Chortkoff BS, Eger EII, Bennett HL, W, Chortkoff BS, Eger EII, Bennett HL, W, Chortkoff BS, Eger EII, Bennett HL, W, Chortkoff BS, Eger EII, Bennett HL, WeiskopfeiskopfeiskopfeiskopfeiskopfRBRBRBRBRB. Subanesthetic concentrations of desflurane and isofluranesuppress explicit and implicit learning. Anesth Analg 80: 568-72,1995.
Griffiths D, Jones JGGriffiths D, Jones JGGriffiths D, Jones JGGriffiths D, Jones JGGriffiths D, Jones JG. Awareness and memory in anaesthetizedpatients. Br J Anaesth 65: 603-6, 1990.
Hargrove RLHargrove RLHargrove RLHargrove RLHargrove RL. Awareness under anaesthesia. J Med Def Union 9:9-11, 1987.
Harris TJB, Brice DD, Hetherington RR, Utting JEHarris TJB, Brice DD, Hetherington RR, Utting JEHarris TJB, Brice DD, Hetherington RR, Utting JEHarris TJB, Brice DD, Hetherington RR, Utting JEHarris TJB, Brice DD, Hetherington RR, Utting JE. Dreamingassociated with anaesthesia: the influence of morphine premedi-cation and two volatile adjuvants. Br J Anaesth 43: 172-8, 1971.

62
Haykin SSHaykin SSHaykin SSHaykin SSHaykin SS. Neural networks: a comprehensive foundation.Upper Saddle River, New Jersey: Prentice Hall, 1999.
Heier THeier THeier THeier THeier T, Steen P, Steen P, Steen P, Steen P, Steen PAAAAA. Assessment of anaesthesia depth. Acta Anaes-thesiol Scand 40: 1087-100, 1996.
Hilgenberg JCHilgenberg JCHilgenberg JCHilgenberg JCHilgenberg JC. Intraoperative awareness during high-dose fenta-nyl-oxygen anesthesia. Anesthesiology 54: 341-3, 1981.
Ho AMHo AMHo AMHo AMHo AM. ‘Awareness’ and ‘recall’ during emergence from generalanaesthesia. Eur J Anaesthesiol 18: 623-5, 2001.
Holt GM, YHolt GM, YHolt GM, YHolt GM, YHolt GM, Yate PMate PMate PMate PMate PM. Psychological responses to anaesthesia. In:Hazards and complications of anaesthesia (2. ed.), Taylor TH,Major E, eds. Edinburgh: Churchill Livingstone, 1993: 447-57.
Horowitz M, Wilner N, Alvarez WHorowitz M, Wilner N, Alvarez WHorowitz M, Wilner N, Alvarez WHorowitz M, Wilner N, Alvarez WHorowitz M, Wilner N, Alvarez W. Impact of event scale: a mea-sure of subjective stress. Psychosomatic Medicine 41: 3, 1979.
Hug CCHug CCHug CCHug CCHug CC. Does opioid “anesthesia” exist? Anesthesiology 73: 1-4,1990.
Hutchinson RHutchinson RHutchinson RHutchinson RHutchinson R. Awareness during surgery. Br J Anaesth 33: 463-9,1960.
James MFMJames MFMJames MFMJames MFMJames MFM. Conscious levels during anaesthesia. Br J Anaesth72: 496, 1994.
Jelicic M, Bonke BJelicic M, Bonke BJelicic M, Bonke BJelicic M, Bonke BJelicic M, Bonke B. The incidence of awareness during anaesthe-sia. Anaesthesia 44: 1004-5, 1989.
Jessop J, Jones JGJessop J, Jones JGJessop J, Jones JGJessop J, Jones JGJessop J, Jones JG. Conscious awareness during general anaesthe-sia-what are we attempting to monitor? Br J Anaesth 66: 635-7,1991.
Jones JG, Konieczko KJones JG, Konieczko KJones JG, Konieczko KJones JG, Konieczko KJones JG, Konieczko K. Hearing and memory in anaesthetisedpatients. BMJ 292: 1291-3, 1986.
Jones JGJones JGJones JGJones JGJones JG. Awareness during general anaesthesia - what are wemonitoring. In: Memory and awareness in anaesthesia IV, Jor-dan C, Vaughan DJA, Newton DEF, eds. London: Imperial CollegePress, 2000: 3-40.
Jordening H, Pedersen TJordening H, Pedersen TJordening H, Pedersen TJordening H, Pedersen TJordening H, Pedersen T. The incidence of conscious awarenessin a general population of anesthetized patients. Anesthesiology75: A1055, 1991.
Junger A, Benson M, Quinzio L, Jost A, VJunger A, Benson M, Quinzio L, Jost A, VJunger A, Benson M, Quinzio L, Jost A, VJunger A, Benson M, Quinzio L, Jost A, VJunger A, Benson M, Quinzio L, Jost A, Veit C, Klöss Teit C, Klöss Teit C, Klöss Teit C, Klöss Teit C, Klöss T, Hempel-, Hempel-, Hempel-, Hempel-, Hempel-mann Gmann Gmann Gmann Gmann G. Qualitätsdokumentation mit einem Anästhesie-Informa-tions-Management-System (AIMS). Anaesthetist 48: 523-32, 1999.
Kapur PKapur PKapur PKapur PKapur PAAAAA. Multicenter study versus nausea outcomes: the value oflarge numbers and the limitations. Anesth Analg 78: 5-6, 1994.
Kelly JS, Roy RCKelly JS, Roy RCKelly JS, Roy RCKelly JS, Roy RCKelly JS, Roy RC. Intraoperative awareness with propofol-oxygentotal intravenous anesthesia for microlaryngeal surgery. Anesthe-siology 77: 207-9, 1992.
Kelly SJ, Myles PS, Bain D, Rosow C, Ramsay JKelly SJ, Myles PS, Bain D, Rosow C, Ramsay JKelly SJ, Myles PS, Bain D, Rosow C, Ramsay JKelly SJ, Myles PS, Bain D, Rosow C, Ramsay JKelly SJ, Myles PS, Bain D, Rosow C, Ramsay J. Case 8-2000.Intraoperative bispectral index monitoring and early extubationafter cardiac surgery in patients with a history of awareness underanesthesia. J Cardiothorac Vasc Anesth 14: 726-30, 2000.
Kerssens C, Sebel PSKerssens C, Sebel PSKerssens C, Sebel PSKerssens C, Sebel PSKerssens C, Sebel PS. BIS and memory during anesthesia. In:Awareness during anesthesia (1. ed.), Ghoneim MM, ed. Oxford:Butterworth-Heinemann, 2001: 103-16.
Kihlstrom JFKihlstrom JFKihlstrom JFKihlstrom JFKihlstrom JF, Schacter DL, Schacter DL, Schacter DL, Schacter DL, Schacter DL. Anaesthesia, amnesia, and the cogni-tive unconscious. In: Memory and Awareness in Anaesthesia,
Bonke B, Fitch W, Millar K, eds. Amsterdam: Swets & ZeitlingerPublishers, 1990: 21-44.
Kim CLKim CLKim CLKim CLKim CL. Awareness during cardiopulmonary bypass. AANA-J 46:373-83, 1978.
Kochs E, Kalkman CJ, Thornton C, Newton D, Bischoff PKochs E, Kalkman CJ, Thornton C, Newton D, Bischoff PKochs E, Kalkman CJ, Thornton C, Newton D, Bischoff PKochs E, Kalkman CJ, Thornton C, Newton D, Bischoff PKochs E, Kalkman CJ, Thornton C, Newton D, Bischoff P, Kuppe, Kuppe, Kuppe, Kuppe, KuppeH, Abke J, Konecny E, Nahm WH, Abke J, Konecny E, Nahm WH, Abke J, Konecny E, Nahm WH, Abke J, Konecny E, Nahm WH, Abke J, Konecny E, Nahm W, Stockmanns G, Stockmanns G, Stockmanns G, Stockmanns G, Stockmanns G. Middle latencyauditory evoked responses and electroencephalographic derivedvariables do not predict movement to noxious stimulation during1 minimum alveolar anesthetic concentration isoflurane/nitrousoxide anesthesia. Anesth Analg 88: 1412-7, 1999.
Lennmarken C, Bildfors K, Enlund G, Samuelsson PLennmarken C, Bildfors K, Enlund G, Samuelsson PLennmarken C, Bildfors K, Enlund G, Samuelsson PLennmarken C, Bildfors K, Enlund G, Samuelsson PLennmarken C, Bildfors K, Enlund G, Samuelsson P, Sandin, Sandin, Sandin, Sandin, SandinRHRHRHRHRH. Victims of awareness. Acta Anaesthesiol Scand 46: 229-31,2002.
Liu WH, Thorp TLiu WH, Thorp TLiu WH, Thorp TLiu WH, Thorp TLiu WH, Thorp TA, Graham SG, Aitkenhead ARA, Graham SG, Aitkenhead ARA, Graham SG, Aitkenhead ARA, Graham SG, Aitkenhead ARA, Graham SG, Aitkenhead AR. Incidence ofawareness with recall during general anaesthesia. Anaesthesia 46:435-7, 1991.
Lubke GH, Kerssens C, Phaf H, Sebel PSLubke GH, Kerssens C, Phaf H, Sebel PSLubke GH, Kerssens C, Phaf H, Sebel PSLubke GH, Kerssens C, Phaf H, Sebel PSLubke GH, Kerssens C, Phaf H, Sebel PS. Dependence of explicitand implicit memory on hypnotic state in trauma patients. Anes-thesiology 90: 670-80, 1999.
Lunn JN, Rosen MLunn JN, Rosen MLunn JN, Rosen MLunn JN, Rosen MLunn JN, Rosen M. Anaesthetic awareness. BMJ 300: 938, 1990.
LLLLLyons G, Macdonald Ryons G, Macdonald Ryons G, Macdonald Ryons G, Macdonald Ryons G, Macdonald R. Awareness during caesarean section. An-aesthesia 46: 62-4, 1991.
Macleod AD, Maycock EMacleod AD, Maycock EMacleod AD, Maycock EMacleod AD, Maycock EMacleod AD, Maycock E. Awareness during anaesthesia and posttraumatic stress disorder. Anaesth Intensive Care 20: 378-82, 1992.
Mainzer J, JrMainzer J, JrMainzer J, JrMainzer J, JrMainzer J, Jr..... Awareness, muscle relaxants and balanced anaes-thesia. Can Anaesth Soc J 26: 386-93, 1979.
Mark JB, Greenberg LMMark JB, Greenberg LMMark JB, Greenberg LMMark JB, Greenberg LMMark JB, Greenberg LM. Intraoperative awareness and hyperten-sive crisis during high-dose fentanyl-diazepam-oxygen anesthe-sia. Anesth Analg 62: 698-700, 1983.
Maunuksela E-LMaunuksela E-LMaunuksela E-LMaunuksela E-LMaunuksela E-L. Hemodynamic response to different anestheticsduring open-heart surgery. Acta Anaesthesiol Scand Suppl. 65,1977.
McCleane GJ, Cooper RMcCleane GJ, Cooper RMcCleane GJ, Cooper RMcCleane GJ, Cooper RMcCleane GJ, Cooper R. The nature of pre-operative anxiety. An-aesthesia 45: 153-5 issn: 0003-2409, 1990.
McKenna TMcKenna TMcKenna TMcKenna TMcKenna T, Wilton TNP, Wilton TNP, Wilton TNP, Wilton TNP, Wilton TNP. Awareness during endotracheal intuba-tion. Anaesthesia 28: 599-602, 1973.
Meyer BC, Blacher RSMeyer BC, Blacher RSMeyer BC, Blacher RSMeyer BC, Blacher RSMeyer BC, Blacher RS. A traumatic neurotic reaction induced bysuccinylcholine chloride. N Y State J Med 61: 1255-61, 1961.
Miller DR, Blew PG, Martineau RJ, Hull KAMiller DR, Blew PG, Martineau RJ, Hull KAMiller DR, Blew PG, Martineau RJ, Hull KAMiller DR, Blew PG, Martineau RJ, Hull KAMiller DR, Blew PG, Martineau RJ, Hull KA. Midazolam andawareness with recall during total intravenous anaesthesia. Can JAnaesth 43: 946-53, 1996.
Moerman A, Herregods L, Foubert L, Poelaert J, Jordaens L, LMoerman A, Herregods L, Foubert L, Poelaert J, Jordaens L, LMoerman A, Herregods L, Foubert L, Poelaert J, Jordaens L, LMoerman A, Herregods L, Foubert L, Poelaert J, Jordaens L, LMoerman A, Herregods L, Foubert L, Poelaert J, Jordaens L, LDH, Rolly GDH, Rolly GDH, Rolly GDH, Rolly GDH, Rolly G. Awareness during anaesthesia for implantable car-dioverter defibrillator implantation. Recall of defibrillation shocks.Anaesthesia 50: 733-5, 1995.
Moerman N, Bonke B, Oosting JMoerman N, Bonke B, Oosting JMoerman N, Bonke B, Oosting JMoerman N, Bonke B, Oosting JMoerman N, Bonke B, Oosting J. Awareness and recall duringgeneral anesthesia. Facts and feelings. Anesthesiology 79: 454-64,1993.
Moore JK, Seymour AHMoore JK, Seymour AHMoore JK, Seymour AHMoore JK, Seymour AHMoore JK, Seymour AH. Awareness during bronchoscopy. Ann RColl Surg Engl 69: 45-7, 1987.

63
Mummaneni N, Rao TL, Montoya AMummaneni N, Rao TL, Montoya AMummaneni N, Rao TL, Montoya AMummaneni N, Rao TL, Montoya AMummaneni N, Rao TL, Montoya A. Awareness and recall withhigh-dose fentanyl-oxygen anesthesia. Anesth Analg 59: 948-9,1980.
Myles PS, Williams DL, Hendrata M, Anderson H, WMyles PS, Williams DL, Hendrata M, Anderson H, WMyles PS, Williams DL, Hendrata M, Anderson H, WMyles PS, Williams DL, Hendrata M, Anderson H, WMyles PS, Williams DL, Hendrata M, Anderson H, Weeks AMeeks AMeeks AMeeks AMeeks AM.Patient satisfaction after anaesthesia and surgery: results of a pro-spective survey of 10 811 patients. Br J Anaesth 84: 6-10, 2000.
Newton DEFNewton DEFNewton DEFNewton DEFNewton DEF, Thornton C, Creagh-Barry P, Thornton C, Creagh-Barry P, Thornton C, Creagh-Barry P, Thornton C, Creagh-Barry P, Thornton C, Creagh-Barry P, Doré J, Doré J, Doré J, Doré J, Doré J. Early corticalauditory evoked response in anaesthesia: comparison of the effectsof nitrous oxide and isoflurane. Br J Anaesth 62: 61-5, 1989.
Ng KH, Gurubatham AINg KH, Gurubatham AINg KH, Gurubatham AINg KH, Gurubatham AINg KH, Gurubatham AI. Awareness during caesarean sectionunder general anaesthesia. Med J Aust 2: 774-6, 1974.
Nordström O, Engström S, Persson S, Sandin RNordström O, Engström S, Persson S, Sandin RNordström O, Engström S, Persson S, Sandin RNordström O, Engström S, Persson S, Sandin RNordström O, Engström S, Persson S, Sandin R. Incidence ofawareness in total i.v. anaesthesia based on propofol, alfentanil andneuromuscular blockade. Acta Anaesthesiol Scand 41: 978-84,1997.
O’Connor MFO’Connor MFO’Connor MFO’Connor MFO’Connor MF, Daves SM, T, Daves SM, T, Daves SM, T, Daves SM, T, Daves SM, Tung A, Cook RI, Thisted R, Apfel-ung A, Cook RI, Thisted R, Apfel-ung A, Cook RI, Thisted R, Apfel-ung A, Cook RI, Thisted R, Apfel-ung A, Cook RI, Thisted R, Apfel-baum Jbaum Jbaum Jbaum Jbaum J. BIS monitoring to prevent awareness during general an-esthesia. Anesthesiology 94: 520-2, 2001.
Osborne GA, WOsborne GA, WOsborne GA, WOsborne GA, WOsborne GA, Webb RK, Runciman WBebb RK, Runciman WBebb RK, Runciman WBebb RK, Runciman WBebb RK, Runciman WB. The Australian IncidentMonitoring Study. Patient awareness during anaesthesia: an anal-ysis of 2000 incident reports. Anaesth Intensive Care 21: 653-4,1993.
Osterman JE, van der Kolk BAOsterman JE, van der Kolk BAOsterman JE, van der Kolk BAOsterman JE, van der Kolk BAOsterman JE, van der Kolk BA. Awareness during anesthesia andposttraumatic stress disorder. Gen Hosp Psychiatry 20: 274-81,1998.
Osterman JE, Hopper J, Heran WJ, Keane TM, van der Kolk BAOsterman JE, Hopper J, Heran WJ, Keane TM, van der Kolk BAOsterman JE, Hopper J, Heran WJ, Keane TM, van der Kolk BAOsterman JE, Hopper J, Heran WJ, Keane TM, van der Kolk BAOsterman JE, Hopper J, Heran WJ, Keane TM, van der Kolk BA.Awareness under anesthesia and the development of posttraumat-ic stress disorder. Gen Hosp Psychiatry 23: 198-204, 2001.
Parkhouse JParkhouse JParkhouse JParkhouse JParkhouse J. Awareness during surgery. Postgrad Med J 36: 674-7, 1960.
Payne JPPayne JPPayne JPPayne JPPayne JP. Awareness and its medicolegal implications. Br J An-aesth 73: 38-45, 1994.
Pedersen TPedersen TPedersen TPedersen TPedersen T, Johansen SH, Johansen SH, Johansen SH, Johansen SH, Johansen SH. Serious morbidity attributable to ana-esthesia. Considerations for prevention. Anaesthesia 44: 504-8,1989.
Phillips AA, McLean RFPhillips AA, McLean RFPhillips AA, McLean RFPhillips AA, McLean RFPhillips AA, McLean RF, Devitt JH, Harrington EM, Devitt JH, Harrington EM, Devitt JH, Harrington EM, Devitt JH, Harrington EM, Devitt JH, Harrington EM. Recall of in-traoperative events after general anaesthesia and cardiopulmonarybypass. Can J Anaesth 40: 922-6, 1993.
Ponte JPonte JPonte JPonte JPonte J. Neuromuscular blockers during general anaesthesia - lessmay be better. BMJ 310: 1218-9, 1995.
Prys-Roberts CPrys-Roberts CPrys-Roberts CPrys-Roberts CPrys-Roberts C. Anaesthesia: A practical or impractical construct?Br J Anaesth 59: 1341-45, 1987.
Pöppel E, Schwender DPöppel E, Schwender DPöppel E, Schwender DPöppel E, Schwender DPöppel E, Schwender D. Temporal mechanisms of consciousness.Int Anesth Clin 31: 27-38, 1993.
Quasha AL, Eger EI, TQuasha AL, Eger EI, TQuasha AL, Eger EI, TQuasha AL, Eger EI, TQuasha AL, Eger EI, Tinker JHinker JHinker JHinker JHinker JH. Determination and applicationsof MAC. Anesthesiology 53: 315-34, 1980.
Rampil IJRampil IJRampil IJRampil IJRampil IJ. Anesthetic potency is not altered after hypothermic spi-nal cord transection in rats. Anesthesiology 80: 606-10, 1994.
Rampil IJRampil IJRampil IJRampil IJRampil IJ. A primer for EEG signal processing in anesthesia. An-esthesiology 89: 980-1002, 1998.
Rosenberg PRosenberg PRosenberg PRosenberg PRosenberg P, Gisvold SE, Flaatten H, Nuutinen L, Stenqvist O,, Gisvold SE, Flaatten H, Nuutinen L, Stenqvist O,, Gisvold SE, Flaatten H, Nuutinen L, Stenqvist O,, Gisvold SE, Flaatten H, Nuutinen L, Stenqvist O,, Gisvold SE, Flaatten H, Nuutinen L, Stenqvist O,TTTTTryggvason B, Vryggvason B, Vryggvason B, Vryggvason B, Vryggvason B, Viby-Mogensen Jiby-Mogensen Jiby-Mogensen Jiby-Mogensen Jiby-Mogensen J. Guidelines for anaesthesia carein the Nordic countries. Acta Anaesthesiol Scand 36: 741-4, 1992.
Rosow C, Manberg PJRosow C, Manberg PJRosow C, Manberg PJRosow C, Manberg PJRosow C, Manberg PJ. Bispectral index monitoring. Anesth ClinNorth Am 2: 89-107, 1998.
Russell IFRussell IFRussell IFRussell IFRussell IF. Balanced anesthesia: does it anesthetize? Anesth Analg64: 941-2, 1985.
Russell IFRussell IFRussell IFRussell IFRussell IF. Comparison of wakefulness with two anaesthetic regi-mens. Total i.v. v. balanced anaesthesia. Br J Anaesth 58: 965-8,1986.
Russell IFRussell IFRussell IFRussell IFRussell IF. Midazolam-alfentanil: an anaesthetic? An investiga-tion using the isolated forearm technique. Br J Anaesth 70: 42-6,1993.
Russell IFRussell IFRussell IFRussell IFRussell IF, W, W, W, W, Wang Mang Mang Mang Mang M. Absence of memory for intraoperative infor-mation during surgery under adequate general anaesthesia. Br JAnaesth 78: 3-9, 1997.
Sado ASSado ASSado ASSado ASSado AS. Electronic medical record in the intensive care unit. CritCare Clin 15: 499-522, 1999.
Sandin R, Nordström OSandin R, Nordström OSandin R, Nordström OSandin R, Nordström OSandin R, Nordström O. Awareness during total i.v. anaesthesia.Br J Anaesth 71: 782-7, 1993.
Sandin RH, Enlund G, Samuelsson PSandin RH, Enlund G, Samuelsson PSandin RH, Enlund G, Samuelsson PSandin RH, Enlund G, Samuelsson PSandin RH, Enlund G, Samuelsson P, Lennmarken C, Lennmarken C, Lennmarken C, Lennmarken C, Lennmarken C. Aware-ness during anaesthesia: a prospective case study. Lancet 355: 707-11, 2000.
Saucier N, WSaucier N, WSaucier N, WSaucier N, WSaucier N, Walts LFalts LFalts LFalts LFalts LF, Moreland JR, Moreland JR, Moreland JR, Moreland JR, Moreland JR. Patient awareness during ni-trous oxide, oxygen, and halothane anesthesia. Anesth Analg 62:239-40, 1983.
Scheinin HScheinin HScheinin HScheinin HScheinin H. Lääkkeen pitoisuuden ja vaikutuksen korrelaatio.Duodecim 115: 2275-83, 1999.
Schultetus RR, Hill CR, Dharamraj CM, Banner TE, BermanSchultetus RR, Hill CR, Dharamraj CM, Banner TE, BermanSchultetus RR, Hill CR, Dharamraj CM, Banner TE, BermanSchultetus RR, Hill CR, Dharamraj CM, Banner TE, BermanSchultetus RR, Hill CR, Dharamraj CM, Banner TE, BermanLSLSLSLSLS. Wakefulness during cesarean section after anesthetic induc-tion with ketamine, thiopental, or ketamine and thiopental com-bined. Anesth Analg 65: 723-8, 1986.
Schwender D, FaberSchwender D, FaberSchwender D, FaberSchwender D, FaberSchwender D, Faber-Zullig E, Klasing S, Poppel E, Peter K-Zullig E, Klasing S, Poppel E, Peter K-Zullig E, Klasing S, Poppel E, Peter K-Zullig E, Klasing S, Poppel E, Peter K-Zullig E, Klasing S, Poppel E, Peter K.Motor signs of wakefulness during general anaesthesia with pro-pofol, isoflurane and flunitrazepam/fentanyl and midlatency au-ditory evoked potentials. Anaesthesia 49: 476-84, 1994.
Schwender D, Haessler R, Klasing S, Madler C, Pöppel E, PeterSchwender D, Haessler R, Klasing S, Madler C, Pöppel E, PeterSchwender D, Haessler R, Klasing S, Madler C, Pöppel E, PeterSchwender D, Haessler R, Klasing S, Madler C, Pöppel E, PeterSchwender D, Haessler R, Klasing S, Madler C, Pöppel E, PeterKKKKK. Mid-latency auditory evoked potentials and circulatory responseto loud sounds. Br J Anaesth 72: 307-14, 1994.
Schwender D, Kaiser A, Klasing S, Peter K, Poppel ESchwender D, Kaiser A, Klasing S, Peter K, Poppel ESchwender D, Kaiser A, Klasing S, Peter K, Poppel ESchwender D, Kaiser A, Klasing S, Peter K, Poppel ESchwender D, Kaiser A, Klasing S, Peter K, Poppel E. Midlaten-cy auditory evoked potentials and explicit and implicit memory inpatients undergoing cardiac surgery. Anesthesiology 80: 493-501,1994.
Schwender D, Klasing S, Madler C, Pöppel E, Peter KSchwender D, Klasing S, Madler C, Pöppel E, Peter KSchwender D, Klasing S, Madler C, Pöppel E, Peter KSchwender D, Klasing S, Madler C, Pöppel E, Peter KSchwender D, Klasing S, Madler C, Pöppel E, Peter K. Midlaten-cy auditory evoked potentials and purposeful movements after thi-opentone bolus injection. Anaesthesia 49: 99-104, 1994.
Schwender D, Klasing S, Conzen PSchwender D, Klasing S, Conzen PSchwender D, Klasing S, Conzen PSchwender D, Klasing S, Conzen PSchwender D, Klasing S, Conzen P, Finsterer U, Poppel E, Pe-, Finsterer U, Poppel E, Pe-, Finsterer U, Poppel E, Pe-, Finsterer U, Poppel E, Pe-, Finsterer U, Poppel E, Pe-ter Kter Kter Kter Kter K. Midlatency auditory evoked potentials during anaesthesiawith increasing endexpiratory concentrations of desflurane. ActaAnaesthesiol Scand 40: 171-6, 1996.

64
Schwender D, Kunze-Kronawitter H, Dietrich PSchwender D, Kunze-Kronawitter H, Dietrich PSchwender D, Kunze-Kronawitter H, Dietrich PSchwender D, Kunze-Kronawitter H, Dietrich PSchwender D, Kunze-Kronawitter H, Dietrich P, Klasing S, Forst, Klasing S, Forst, Klasing S, Forst, Klasing S, Forst, Klasing S, ForstH, Madler CH, Madler CH, Madler CH, Madler CH, Madler C. Conscious awareness during general anaesthesia:patients’ perceptions, emotions, cognition and reactions. Br J An-aesth 80: 133-9, 1998.
Schwilden HSchwilden HSchwilden HSchwilden HSchwilden H. Neuropharmacology of anaesthetics. Curr OpinAnaesthesiol 7: 326-9, 1994.
Sigl JC, Chamoun NGSigl JC, Chamoun NGSigl JC, Chamoun NGSigl JC, Chamoun NGSigl JC, Chamoun NG. An introduction to bispectral analysis forthe electroencephalogram. J Clin Monit 10: 392-404, 1994.
Smith WD, Dutton RC, Smith NTSmith WD, Dutton RC, Smith NTSmith WD, Dutton RC, Smith NTSmith WD, Dutton RC, Smith NTSmith WD, Dutton RC, Smith NT. Measuring the performance ofanesthetic depth indicators. Anesthesiology 84: 38-51, 1996.
Spitzer RL, Williams JBWSpitzer RL, Williams JBWSpitzer RL, Williams JBWSpitzer RL, Williams JBWSpitzer RL, Williams JBW, Gibbon M, First MB, Gibbon M, First MB, Gibbon M, First MB, Gibbon M, First MB, Gibbon M, First MB. Structured clin-ical interview for DSM-III-R non patient version (SCID-NP).Washington D.C.: American Psychiatric Press, 1990a.
Spitzer RL, Williams JBWSpitzer RL, Williams JBWSpitzer RL, Williams JBWSpitzer RL, Williams JBWSpitzer RL, Williams JBW, Gibbon M, First MB, Gibbon M, First MB, Gibbon M, First MB, Gibbon M, First MB, Gibbon M, First MB. Structured clin-ical interview for DSM-III-R personality disorder (SCID-II, ver-sion 1.0). Washington D.C.: American Psychiatric Press, 1990b.
St Pierre M, Landsleitner B, Schwilden H, Schuettler JSt Pierre M, Landsleitner B, Schwilden H, Schuettler JSt Pierre M, Landsleitner B, Schwilden H, Schuettler JSt Pierre M, Landsleitner B, Schwilden H, Schuettler JSt Pierre M, Landsleitner B, Schwilden H, Schuettler J. Aware-ness during laryngoscopy and intubation: quantitating incidencefollowing induction of balanced anesthesia with etomidate and ci-satracurium as detected with the isolated forearm technique. J ClinAnesth 12: 104-8, 2000.
Stanley TH, de Lange SStanley TH, de Lange SStanley TH, de Lange SStanley TH, de Lange SStanley TH, de Lange S. The effect of population habits on sideeffects and narcotic requirements during high-dose fentanyl ana-esthesia. Can Anaesth Soc J 31: 368-76, 1984.
Stoelting RK, Longnecker DE, Eger EI. Stoelting RK, Longnecker DE, Eger EI. Stoelting RK, Longnecker DE, Eger EI. Stoelting RK, Longnecker DE, Eger EI. Stoelting RK, Longnecker DE, Eger EI. Minimum alveolar con-centrations in man on awakening from methoxyflurane, halothane,ether and fluroxene anesthesia: MAC Awake. Anesthesiology 33: 5-9, 1970.
TTTTTerrell RK, Sweet WO, Gladfelter JH, Stephen CRerrell RK, Sweet WO, Gladfelter JH, Stephen CRerrell RK, Sweet WO, Gladfelter JH, Stephen CRerrell RK, Sweet WO, Gladfelter JH, Stephen CRerrell RK, Sweet WO, Gladfelter JH, Stephen CR. Study of recallduring anesthesia. Anesth Analg 48: 86-90, 1969.
Thornton C, Barrowcliffe MPThornton C, Barrowcliffe MPThornton C, Barrowcliffe MPThornton C, Barrowcliffe MPThornton C, Barrowcliffe MP, Konieczko KM, V, Konieczko KM, V, Konieczko KM, V, Konieczko KM, V, Konieczko KM, Ventham Pentham Pentham Pentham Pentham P, Dore, Dore, Dore, Dore, DoreCJ, Newton DE, Jones JGCJ, Newton DE, Jones JGCJ, Newton DE, Jones JGCJ, Newton DE, Jones JGCJ, Newton DE, Jones JG. The auditory evoked response as an in-dicator of awareness. Br J Anaesth 63: 113-5, 1989.
Thornton C, Jones JGThornton C, Jones JGThornton C, Jones JGThornton C, Jones JGThornton C, Jones JG. Evaluating depth of anesthesia: review ofmethods. Int Anesthesiol Clin 31: 67-88, 1993.
Thornton C, Sharpe RMThornton C, Sharpe RMThornton C, Sharpe RMThornton C, Sharpe RMThornton C, Sharpe RM. The auditory evoked responses andmemory during anesthesia. In: Awareness during anesthesia,Ghoneim MM, ed. Oxford: Butterworth-Heinemann, 2001: 117-27.
TTTTTunstall MEunstall MEunstall MEunstall MEunstall ME. Detecting wakefulness during general anaesthesiafor caesarean section. BMJ 1: 1321, 1977.
TTTTTunstall MEunstall MEunstall MEunstall MEunstall ME. The reduction of amnesic wakefulness during Cae-sarean section. Anaesthesia 34: 316-9, 1979.
WWWWWalder ADalder ADalder ADalder ADalder AD. Failure of anaesthesia with etomidate. Eur J Anaes-thesiol 12: 325-7, 1995.
van der Kolk BA, Osterman JEvan der Kolk BA, Osterman JEvan der Kolk BA, Osterman JEvan der Kolk BA, Osterman JEvan der Kolk BA, Osterman JE. The effects of trauma on memory:implications for awareness under anaesthesia. In: Memory andawareness in anaesthesia IV, Jordan C, Vaughan DJA, Newton DEF,eds. London: Imperial College Press, 2000: 193-202.
WWWWWang Mang Mang Mang Mang M. The psychological consequences fo awareness duringsurgery. In: Memory and awareness in anaesthesia IV, Jordan C,Vaughan DJA, Newton DEF, eds. London: Imperial College Press,2000: 315-24.
WWWWWang Mang Mang Mang Mang M. The psychological consequences fo explicit and implicitmemories of events during surgery. In: Awareness during anes-thesia, Ghoneim MM, ed. Oxford: Butterworth-Heinemann, 2001:145-53.
WWWWWells Cells Cells Cells Cells C. Insufficient anaesthesia. BMJ 1: 610, 1950.
VVVVVeselis RA, Reinsel R, Sommer S, Carlon Geselis RA, Reinsel R, Sommer S, Carlon Geselis RA, Reinsel R, Sommer S, Carlon Geselis RA, Reinsel R, Sommer S, Carlon Geselis RA, Reinsel R, Sommer S, Carlon G. Use of neural net-work analysis to classify electroencephalographic patterns againstdepth of midazolam sedation in intensive care unit patients. J ClinMonit 7: 259-67, 1991.
WilderWilderWilderWilderWilder-Smith OHG, Hagon O, T-Smith OHG, Hagon O, T-Smith OHG, Hagon O, T-Smith OHG, Hagon O, T-Smith OHG, Hagon O, Tassonyi Eassonyi Eassonyi Eassonyi Eassonyi E. EEG arousal duringlaryngoscopy and intubation: comparison of thiopentone or pro-pofol supplemented with nitrous oxide. Br J Anaesth 75: 441-6,1995.
Willenkin RLWillenkin RLWillenkin RLWillenkin RLWillenkin RL. Management of general anesthesia. In: Anesthesia(3. ed.), Miller RR, ed. New York: Churchill Livingstone, 1990: 1335-46.
Wilson J, TWilson J, TWilson J, TWilson J, TWilson J, Turner DJurner DJurner DJurner DJurner DJ. Awareness during caesarean section undergeneral anaesthesia. BMJ 1: 280-3, 1969.
Wilson SL, VWilson SL, VWilson SL, VWilson SL, VWilson SL, Vaughan Raughan Raughan Raughan Raughan RWWWWW, Stephen CR, Stephen CR, Stephen CR, Stephen CR, Stephen CR. Awareness, dreams, andhallucinations associated with general anesthesia. Anesth Analg54: 609-17, 1975.
Winterbottom EHWinterbottom EHWinterbottom EHWinterbottom EHWinterbottom EH. Insufficient anaesthesia. BMJ 1: 247-8, 1950.
WWWWWolters G, Phaf RHolters G, Phaf RHolters G, Phaf RHolters G, Phaf RHolters G, Phaf RH. Explicit and implicit measures of memory:evidence for two learning mechanisms. In: Memory and Aware-ness in Anaesthesia, Bonke B, Fitch W, Millar K, eds. Amsterdam:Swets & Zeitlinger Publishers, 1990: 57-63.
WWWWWong KCong KCong KCong KCong KC. Narcotics are not expected to produce unconsciousnessand amnesia. Anesth Analg 62: 625-6, 1983.
Yli-Hankala A, Lindgren L, Porkkala TYli-Hankala A, Lindgren L, Porkkala TYli-Hankala A, Lindgren L, Porkkala TYli-Hankala A, Lindgren L, Porkkala TYli-Hankala A, Lindgren L, Porkkala T, Jäntti V, Jäntti V, Jäntti V, Jäntti V, Jäntti V. Nitrous oxide-mediated activation of the EEG during isoflurane anaesthesia inpatients. Br J Anaesth 70: 54-7, 1993.
Yli-Hankala AYli-Hankala AYli-Hankala AYli-Hankala AYli-Hankala A. Operating theatre-the patient is listening. ActaAnaesthesiol Scand 44: 131-2, 2000.
Zurada JMZurada JMZurada JMZurada JMZurada JM. Introduction to artificial neural systems. Boston, MA:PWS Publishing Company, 1992.

Appendix 65
Appendix
Details of the patient cases with awareness and recall during general anesthesia. Patientdemographics, recalled experience, surgery and anesthesia details, details of the recalledexperience, and after-effects are given. Comments refer to the author’s commentson certain experiences.
Abbreviations usedAEP Auditory evoked potentialCABG Coronary artery bypass graftingD & C Dilatation and curettageEBT Endobronchial tubeETAGC End-tidal anesthetic gas concentrationETT Endotracheal tubeF FemaleICU Intensive care unitM MaleMVR Mitral valve replacementN2O Nitrous oxideNMB Neuromuscular blockerOR Operating roomTx cordis Heart transplantation
Awareness groups:1. Patients with unclear memories or dreams, which could be of intraoperative origin.2. Patients with short periods of awareness occurring either intraoperative or during the period
of awakening from anesthesia.3. Patients with long-lasting, clear, and undisputed recall of the intraoperative period.

66 Appendix
tneitaP
tneitaP ydutS foraeYaisehtsena
egA)sraey(
xeS thgieW)gk(
thgieH)mc(
yregruS
1 4,1 4991 03 F 08 271 ypocsorapallacigolocenyG
2 4,1 4991 56 M 27 081 ycnangilamrofymotorapaL
3 1 4991 74 F 5.87 061 ymotorapallacigolocenyG
4 4,1 5991 13 F 07 061 noitasinoC
5 4,1 5991 28 F 85 051 ymotcetsycelohC
6 4,1 4991 26 M 211 271 ypocsognyralorciM
7 1 5991 46 F 56 161 nodnetsutanipsarpusfonoitcurtsnoceR
8 1 5991 74 M 07 471 amonalemsuoenatucfonoisicxE
9 4,1 5991 35 F 08 361 gelthgirnisnodnetfonoitisopsnarT
01 4,1 5991 63 F 29 861 ypocsorapallacigolocenyG
11 4,1 5991 32 F 07 761 ypocsorhtraeenK
21 1 4991 02 F 75 171 ymotcedneppA
31 1 4991 94 F 46 961 C&D
41 1 4991 83 F 06 451 ymotcetsycelohccipocsorapaL

Appendix 67
sliatedcitehtsenA
tneitaP ecneirepxedellaceR ssenerawApuorg
fonoitaruDaisehtsena
)nim(
noitacidemerP
1 noitabutxedna,noitcudnicitehtsenaehtsrebmemerylraelCdnaseciovnamuhraelcdraeh,neewtebnI.aehcartrehfo
.ezilacolotelbatonsawehshcihwniaptlef
3 361 enoN
2 dnataorhtehtniebutnoitabutnihtiwgnikawstcelloceRtuphcihwsnoitacidemeromnevig,dnuoraelpoepynam
niagapeelsamih
2 071 enipezaidozneB
3 dnamoorgnitarepoehtfosthgilfomaerdastcelloceRrehnognitarepodnuoraelpoeplareves
1 911 enipezaidozneB
4 sesiondraeH.noitcudnitayteixnadnahtaerbfossentrohStleFrehhcuotydobemostlefdnaeciovelamadnatahtdeveileB.raefesnetniemitemasehttadnanoitabutxe
.gniydsawehs
2 63 enoN
5 tlef,)seciovelamefdnaelamhtob(snoissucsiddraeHdoolbfoerusserpgnirrucer;hcamotsrehnienodgnihtemos
niapon;rotalitnevehtdraeh,mrarehnoffucerusserp
3 97 enoN
6 tahttlefdnataorhtsihniebutnoitabutniehttleF,snoissucsiddraeh,serugifnamuhdnathgilwas,gnitaesuansgnidaererusserpdoolbhgihetouqydobemossrebmemer
)droceraisehtsenaehtybdemrifnocebdluoc(
3 74 dioipO
7 sihtfi,wonkflesrehtonseod;snoissucsiddnaseciovdraeHlaerromaerdsaw
1 56 enipezaidozneB
8 gnimocekiltlefgninekawagnirud;seiromemdenifednUthgifamorf
1 76 enipezaidozneB
9 taorhtrehniebutnoitabutniehttlefgninekawatA 2 24 enoN
01 ehtniniap;noitalupinamlanigavtlefdna,snoissucsiddraeHylevitarepotsopro-artnirehtie,nemodba
3 53 enoN
11 taorhtrehniebutnoitabutniehttlefgninekawatA 2 05 enipezaidozneB
21 noitarepoehtgnirud”gnileeftnasaelpnu“deificepsnU 1 77 dioipO
31 cisumdraeH 1 31 enoN
41 gninekawatayteixnadeificepsnU 1 371 enipezaidozneB

68 Appendix
Anesthetic details
Patient Co-induction Induction Maintenance N2O ETAGCmonitoring
1 Fentanyl Propofol Propofol (bolus dosing),enflurane (non-continuous)
Yes Not recorded
2 Fentanyl Thiopental Isoflurane Yes Not recorded
3 Fentanyl Thiopental Thiopental (bolus dosing),isoflurane (non-continuous)
Yes Not recorded
4 Fentanyl Propofol Isoflurane Yes Not recorded
5 Fentanyl Thiopental Isoflurane No Not recorded
6 Fentanyl Propofol Propofol (bolus dosing) Yes No
7 Fentanyl Thiopental Isoflurane Yes Not recorded
8 Fentanyl Thiopental Isoflurane Yes Not recorded
9 Fentanyl Propofol Isoflurane Yes Not recorded
10 Fentanyl Propofol Propofol (bolus dosing) Yes No
11 Fentanyl Propofol Isoflurane Yes Not recorded
12 Benzodiazepine,Fentanyl
Ketamine Isoflurane (non-continuous) Yes Not recorded
13 Alfentanil Propofol Propofol (bolus dosing) Yes No
14 Fentanyl Thiopental Enflurane No Not recorded

Appendix 69
Anesthetic details Details of recollection and after-effects
Patient NMB Airway Pain Auditory Visual Tactile Tried tomove
Able tomove
Immediateunderstanding
1 Atracurium ETT Yes Yes No No Yes
2 Atracurium ETT No Yes Yes
3 Vecuronium ETT No No Yes No Yes
4 Atracurium ETT No Yes Yes Yes Yes Yes
5 Atracurium ETT No Yes No Yes Yes Yes Yes
6 Succinylcholine ETT No Yes Yes Yes Yes Yes
7 Atracurium ETT No Yes No No No
8 Atracurium ETT No No No No No
9 Atracurium ETT No No No Yes Yes
10 Atracurium ETT Yes Yes No Yes No
11 Atracurium ETT No No No Yes Yes
12 Atracurium ETT No No No No No
13 None Mask No Yes No No
14 Vecuronium ETT No No No No No

70 Appendix
Details of recollection and after-effects
Patient Immediateanxiety
Duration ofawareness asestimated by thepatient
Awareness as themost unpleasant
experienceduring operation
After effects
1 No Minutes No
2
3 No Short (seconds) No
4 Yes Long (minutes) Yes Sleep disturbances, but did not meet the criteriafor post traumatic stress disorder (PTSD)
5 No Long No
6 No Not very long Yes Treated with anti-depressant medication afterthe experience, recovered.
7 No Long
8 Long
9 No
10
11 No
12 No
13 No
14 Yes

Appendix 71
Patient Comments
1
2 Recollection at the immediate post-operative interview only. Did not remember anything the next day.
3 Experience could also have been a dream or hallucination.
4
5 Did not find the experience of awareness at all unpleasant. Recalls having thought: "Now, the doctorsare working and I will lie down here"
6
7
8 Experience mixed with very unpleasant dreams.
9
10
11
12
13
14

72 Appendix
Patient
Patient Study Year ofanesthesia
Age(years)
Sex Weight(kg)
Height(cm)
Surgery
15 1 1994 47 F 70 160 D & Cc
16 1,4 1994 29 F 44 164 Gynecological laparoscopy
17 1 1995 50 F 107 163 D & Cc
18 1 1995 71 F 70 158 Spinal laminectomy
19 1 1994 69 F 71 165 Laparotomy due to malignancy
20 2 1992 49 M 84 167 CABG
21 2 1992 49 M 63 176 CABG
22 2 1992 45 F 48 144 CABG
23 2 1992 44 M 123 175 CABG
24 2 1993 44 M 72 174 CABG
25 2 1993 51 M 87,5 178 Tx cordis
26 2 1993 59 F 49 159 MVR

Appendix 73
Anesthetic details
Patient Recalled experience Awarenessgroup
Duration ofanesthesia
(min)
Premedication
15 Unspecified intraoperative memories 1 10 None
16 Could not breathe at awakening 2 46 None
17 Unspecified “powerful feelings” during the operation 1 15 None
18 Heard noises and somebody moving around her. 1 75 Benzodiazepine
19 Felt difficult to breathe at awakening and felt somethingtaken out of her throat
2 58 Opioid
20 Felt tearing sensation in his chest, "Like horses were tearingme in pieces." This was not painful, though. He also heard"diffuse speech."
3 205 Scopolamine +opioid
21 Felt the opening of his sternum starting from the upper end.There was no pain. He also heard women voices but couldnot recall what was said. He did not feel this unpleasantand felt confident in his doctors all the time. He also dreamtof cartoons.
3 254 Scopolamine +opioid
22 Felt the opening of her chest, but this was not painful. Shealso heard her doctor saying, "This won't take long." Afterthis, she had no recall of operation.
3 212 Benzodiazepine
23 Heard somebody call, "Now there's a hurry!" He feltsomething done in his chest but felt no pain. He wasalarmed, frightened and anxious and in vain tried to signalhis consciousness. Then he felt an "electric shock" afterwhich he became unconscious again.
3 375 Scopolamine +opioid
24 Felt a scraping sensation on his chest twice. This sensationpersisted only for few seconds, and the patient thought that,apparently, the operation has begun. He felt no pain, didnot consider this sensation alarming.
2 320 Scopolamine +opioid
25 He heard some discussion and thought, "The doctors don'tknow that I'm not asleep yet." He tried to say he was notasleep but felt paralyzed. Then he felt something pushed inhis mouth and throat. After this he rapidly became unaware.
3 283 Benzodiazepine
26 She had had a mitral valve commisurotomy made twice inthe past. During the general anesthesia, she heard adiscussion where a male voice said, "Shall we cut out the oldscar?" Another voice replied, "Of cause we shall." Thenshe felt something pushed down her throat and further feltpressure and pain in her chest. She tried to wave her armbut could not. According to the patient, this all took aboutone minute.
3 276 Scopolamine +opioid
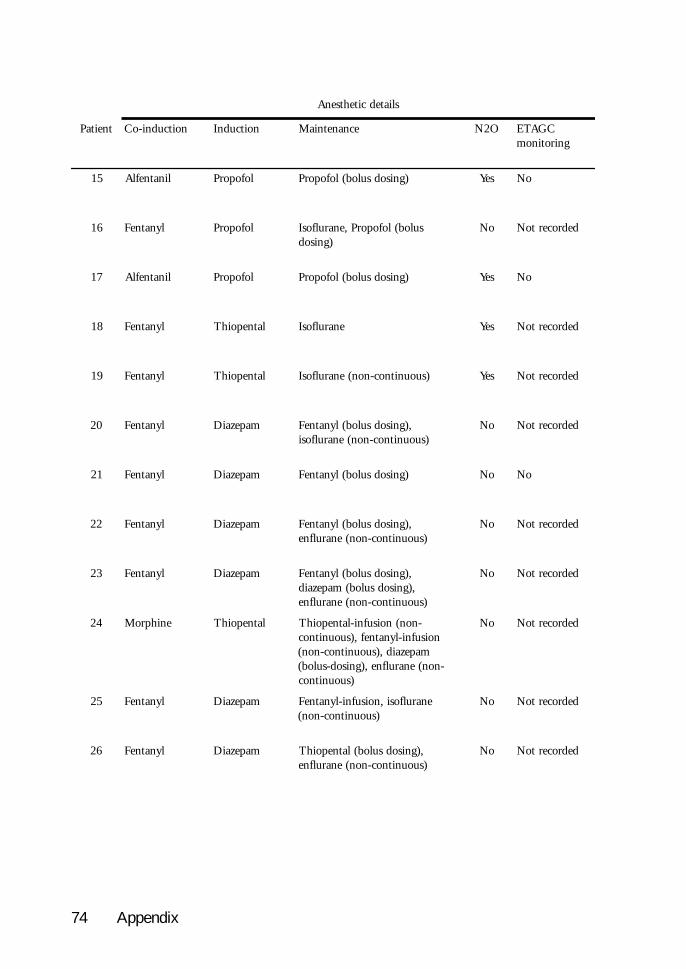
74 Appendix
sliatedcitehtsenA
tneitaP noitcudni-oC noitcudnI ecnanetniaM O2N CGATEgnirotinom
51 linatneflA lofoporP )gnisodsulob(lofoporP seY oN
61 lynatneF lofoporP sulob(lofoporP,enarulfosI)gnisod
oN dedrocertoN
71 linatneflA lofoporP )gnisodsulob(lofoporP seY oN
81 lynatneF latnepoihT enarulfosI seY dedrocertoN
91 lynatneF latnepoihT )suounitnoc-non(enarulfosI seY dedrocertoN
02 lynatneF mapezaiD ,)gnisodsulob(lynatneF)suounitnoc-non(enarulfosi
oN dedrocertoN
12 lynatneF mapezaiD )gnisodsulob(lynatneF oN oN
22 lynatneF mapezaiD ,)gnisodsulob(lynatneF)suounitnoc-non(enarulfne
oN dedrocertoN
32 lynatneF mapezaiD ,)gnisodsulob(lynatneF,)gnisodsulob(mapezaid
)suounitnoc-non(enarulfne
oN dedrocertoN
42 enihproM latnepoihT -non(noisufni-latnepoihTnoisufni-lynatnef,)suounitnoc
mapezaid,)suounitnoc-non(-non(enarulfne,)gnisod-sulob(
)suounitnoc
oN dedrocertoN
52 lynatneF mapezaiD enarulfosi,noisufni-lynatneF)suounitnoc-non(
oN dedrocertoN
62 lynatneF mapezaiD ,)gnisodsulob(latnepoihT)suounitnoc-non(enarulfne
oN dedrocertoN

Appendix 75
sliatedcitehtsenA stceffe-retfadnanoitcellocerfosliateD
tneitaP BMN yawriA niaP yrotiduA lausiV elitcaT otdeirTevom
otelbAevom
etaidemmIgnidnatsrednu
51 enoN ksaM oN oN oN oN oN
61 muirucartA TTE oN oN oN oN seY
71 enoN ksaM oN oN oN oN
81 muirucartA TTE oN seY oN oN
91 muirucartA TTE oN oN oN seY seY
02 muinorucnaP TTE oN seY oN seY seY
12 muinorucnaP TTE oN seY oN seY seY
22 muinorucnaP TTE oN seY oN seY seY
32 muinorucnaP TTE oN seY oN seY seY oN seY
42 muinorucnaP TTE oN oN oN seY seY
52 muinorucnaP TTE oN seY oN seY seY oN seY
62 muinorucnaP TTE seY seY oN seY seY oN seY

76 Appendix
Details of recollection and after-effects
Patient Immediateanxiety
Duration ofawareness asestimated by thepatient
Awareness as themost unpleasant
experienceduring operation
After effects
15 No
16 No
17 No
18
19 Yes Yes
20 No No
21 No No
22 No No
23 Yes Yes Post-operative nightmares, flashbacks
24 No Seconds No
25 Yes 1-2 minutes Yes
26 Yes Minutes No
Appendix 77
Patient Comments
15
16
17
18
19
20
21
22
23
24
25
26

78 Appendix
Patient
Patient Study Year ofanesthesia
Age(years)
Sex Weight(kg)
Height(cm)
Surgery
27 3 1995 54 M 82 170 CABG
28 3 1995 68 M 83 170 CABG
29 3 1995 47 M 97 180 CABG
30 3 1995 53 M 99 177 CABG
31 3 1995 71 M 80 171 CABG
32 3 1995 72 M 90 176 CABG
33 3 1995 70 M 71,5 168 CABG
34 3 1995 53 M 90 186 CABG+MVR
35 3 1995 60 M 75 176 CABG
36 3 1996 69 M 73 174 CABG
37 3 1995 82 M 62 172 CABG

Appendix 79
Anesthetic details
Patient Recalled experience Awarenessgroup
Duration ofanesthesia
(min)
Premedication
27 Suffered from ser ious mental depression before theoperation, and antidepressive medication was started a weekbefore the operation. Recollects waking with much pain inhis chest “like the chest was opened with a saw”. Saw peoplemoving around him and heard women laughing. Felt alsopain his neck. Thinks that he was aware of what is goingon around him for 2 to 3 hours.
3 252 Benzodiazepine
28 Thi s pat ient underwent an unsucce ss fu l coronaryangioplasty and was immediately transferred to the OR forsurgical CABG. The patient recollects discussions, pain inhis neck and a tracheal tube in his throat.
2 325 None
29 The patient underwent a second operation because of post-operative bleeding six hours after the primary operation.The patient recollects being unable to open his eyes,shortness of breath and utmost anxiety. Then remembersfalling asleep again.
2 239 min,reoperation5,75 h later,reoperation
105 min
Scopolamine +opioid
30 Recollects the intubation. 2 265 Benzodiazepine
31 Recollects hearing a rattling noise which the patientattributes to sawing of the sternum. Recollects thinking thatone should not hear this.
2 184 Benzodiazepine
32 Pain which the patient attributes to the time of awakening 1 265 Benzodiazepine
33 Heard male voices; the patient attributes this to thepreoperative period in the OR
1 294 Benzodiazepine
34 Memories of movement. The patient can’t attribute therecollection to a specified time.
1 514 Scopolamine +opioid
35 Remembers a discussion about reoperation. The patientunderwent a reoperation because of inadequate hemostasis6½ hours after the primary operation. Recollections arelikely to have occurred during the interval between theoperations.
1 240min,reoperation6,75 hours
later,reoperation
49 min
Scopolamine +opioid
36 Opened his eyes during the operation. Doesn’t, however,remember this. On the other hand recollects loud male andfemale voices, “like in a noisy restaurant”. The patientattributes this to the postoperative period in the ICU.
1 229 Scopolamine +opioid
37 Unpleasant feeling coupled with nausea. The patientattributes this to the intraoperative period.
1 314 Opioid

80 Appendix
sliatedcitehtsenA
tneitaP noitcudni-oC noitcudnI ecnanetniaM O2N CGATEgnirotinom
72 linatnefuS malozadiM -malozadim,noisufni-linatnefuS-non(enarulfosi,noisufni
)suounitnoc
oN seY
82 linatnefuS mapezaiD enarulfosi,noisufni-linatnefuSlatnepoiht,)suounitnoc-non(
)gnisodsulob(
oN seY
92 linatnefuS mapezaiD enarulfne,noisufni-linatnefuS oN dedrocertoN
03 lynatneF malozadiM -malozadim,noisufni-lynatneF-non(enarulfosi,noisufni
)suounitnoc
oN dedrocertoN
13 linatnefuS mapezaiD enarulfne,noisufni-linatnefuS oN seY
23 lynatneF mapezaiD -lofoporp,noisufni-lynatneFnoisufni
oN dedrocertoN
33 linatnefuS mapezaiD enarulfne,noisufni-linatnefuSenarulfosi,)suounitnoc-non(
)suounitnoc-non(
oN dedrocertoN
43 lynatneF malozadiM -malozadim,noisufni-lynatneF-non(enarulfosi,noisufni
)suounitnoc
oN seY
53 lynatneF mapezaiD -malozadim,noisufni-lynatneF-non(enarulfosi,noisufni
)suounitnoc
oN seY
63 lynatneF mapezaiD enarulfne,noisufni-lynatneF)suounitnoc-non(
oN seY
73 lynatneF ,malozadiMlatnepoiht
-malozadim,noisufni-lynatneF-non(enarulfosi,noisufni
)suounitnoc
oN seY

Appendix 81
sliatedcitehtsenA stceffe-retfadnanoitcellocerfosliateD
tneitaP BMN yawriA niaP yrotiduA lausiV elitcaT otdeirTevom
otelbAevom
etaidemmIgnidnatsrednu
72 muinorucnaP TTE seY seY seY seY oN seY
82 muinorucnaP TTE seY seY oN seY seY
92 muinorucnaP TTE oN seY oN oN seY oN seY
03 muinorucnaP TTE oN oN oN seY oN seY
13 muinorucnaP TTE oN seY oN oN oN seY
23 muinorucnaP TTE seY oN oN
33 muinorucnaP TTE oN seY oN oN seY
43 muinorucnaP TTE oN oN oN oN
53 muinorucnaP TTE oN seY oN oN oN seY seY
63 muinorucnaP TTE oN seY oN oN oN seY seY
73 muinorucnaP TTE oN oN oN oN oN

82 Appendix
Details of recollection and after-effects
Patient Immediateanxiety
Duration ofawareness asestimated by thepatient
Awareness as themost unpleasant
experienceduring operation
After effects
27 Yes 2-3 hours No
28 No
29 Yes Yes
30 No No
31 No Seconds No
32 No
33 No No
34 No
35 No 30 seconds No
36 No Not long No
37 No

Appendix 83
Patient Comments
27
28 Coronary angioplasty and emergency CABG. Recollections may originate between these operations.
29
30
31
32 Possible post-operative recollection from the ICU
33
34
35 Reoperation anesthesia: diazepam, fentanyl and non-continuous isoflurane. Recollections possibly fromthe time between the operations.
36
37

84 Appendix
tneitaP
tneitaP ydutS foraeYaisehtsena
egA)sraey(
xeS thgieW)gk(
thgieH)mc(
yregruS
83 3 5991 16 M 17 861 GBAC
93 3 5991 35 M 18 871 GBAC
04 3 5991 25 M 18 471 GBAC
14 3 5991 35 F 18 761 GBAC
24 3 5991 28 M 87 571 GBAC
34 3 5991 55 M 28 771 GBAC
44 3 5991 86 M 5,08 571 GBAC
54 3 5991 75 M 57 671 GBAC
64 3 5991 05 M 96 671 GBAC
74 3 5991 47 F 86 551 GBAC
84 5,4 7891 35 M 57 171 ymotocarohT

Appendix 85
sliatedcitehtsenA
tneitaP ecneirepxedellaceR ssenerawApuorg
fonoitaruDaisehtsena
)nim(
noitacidemerP
83 sawsihT.tsehcsihfotuodelluperewsebuttahtstcelloceRsihtsetubirttatneitapehT.niapthgilshtiwdeinapmoccadesusawgnirotinomPEA.noitarepoehtfoesahptsalehtotyranomlupoidracehtretfatontubnoitareposihtgnirud
.doirepssapyb
1 013 enipezaidozneB
93 gnileeftnasaelpnunA.mihotgniklatenoemossrebmemeRaotsnoitcellocerehtetubirttatonnaC.taorhtsihni
.emitdeificeps
1 522 enipezaidozneB
04 .rehtonaotecalpenomrofdetropsnartgniebstcelloceR 1 733 +enimalopocSdioipo
14 .sthgilemosneesgnivahstcelloceR 1 102 enipezaidozneB
24 daedsaflesmihderedisnoc,dabyrevgnileefsrebmemeR 1 062 enipezaidozneB
34 ehtgnixiftuobamihotgniklatelpoepwefstcelloceR.ebutnoitabutni
1 042 enipezaidozneB
44 .sniarddnasebutgnieesstcelloceR 1 262 enipezaidozneB
54 dnatsehcehtniniaptlefnehT.peelsagnillafstcelloceRgnivomereraew“gniyasydobemosdraehylsuoenatlumissetubirttatneitapehT.”niapleefyamuoydnagnihtemosdlotsawtneitapehttahT.doirepevitarepoerpehtotsihterasnoitcellocerehttahtstseggus”niapleefyamuoy“taht
.evitarepoartniton
1 372 +enimalopocSdioipo
64 foesuacebnoitarepodnocesatnewrednutneitapehTyramirpehtretfasruohruofgnideelbevitarepotsopdenrecnocahtiwnoissucsidagniraehstcelloceR.noitarepoelddimehtnillitssiehtahtthguohtemittahtgniruD.enot
.noitareponafo
1 ,nim382noitarepoer
sruoh4,retal
noitarepoernim94
enipezaidozneB
74 nipeehsgnirethgualsydobemostuobagnimaerdstcelloceRehT.taorhtrehnignihtemostlefylsuoenatlumiS.cittana
.gninethgirfyrevsawgnileef
1 072 dioipO
84 ,noisicniniks,ymotocarohtrofgninoitisopstcelloceRlatsocretnifogninepo,slessevsuoenatucbusfoymrehtaidffucerusserpdoolB.ymrehtaidgnittuchtiwselcsum
.eciovelamanonoissucsiD.mraehtgnizeeuqs
3 49 enipezaidozneB

86 Appendix
Anesthetic details
Patient Co-induction Induction Maintenance N2O ETAGCmonitoring
38 Fentanyl Lorazepam Fentanyl-infusion, enflurane No Yes
39 Sufentanil Midazolam Sufentanil-infusion, midazolam-infusion, isoflurane (non-continuous)
No Yes
40 Fentanyl Diazepam Fentanyl-infusion, isoflurane(non-continuous)
No Yes
41 Fentanyl Midazolam Fentanyl-infusion, midazolam-infusion, isoflurane (non-continuous)
No Not recorded
42 Fentanyl Midazolam Fentanyl-infusion, midazolam-infusion, isoflurane (non-continuous)
No Not recorded
43 Sufentanil Diazepam Sufentanil-infusion, isoflurane No Yes
44 Alfentanil Midazolam,propofol
Alfentanil-infusion, midazolam-infusion, isoflurane (non-continuous)
No Yes
45 Fentanyl Diazepam Fentanyl-infusion, midazolam-infusion, enflurane (non-continuous)
No Yes
46 Fentanyl Lorazepam Fentanyl-infusion, enflurane No Yes
47 Fentanyl Diazepam Fentanyl (bolus dosing),diazepam (bolus dosing),isoflurane (non-continuous)
No Yes
48 Fentanyl Thiopental Isoflurane Yes Not recorded

Appendix 87
Anesthetic details Details of recollection and after-effects
Patient NMB Airway Pain Auditory Visual Tactile Tried tomove
Able tomove
Immediateunderstanding
38 Pancuronium ETT Yes No No Yes No Yes Yes
39 Pancuronium ETT Yes Yes No Yes No
40 Pancuronium ETT No No No No Yes
41 Pancuronium ETT No No Yes No Yes
42 Pancuronium ETT No No No No Yes
43 Pancuronium ETT No Yes No No No
44 Atracurium ETT No No Yes Yes
45 Pancuronium ETT Yes Yes No Yes Yes Yes
46 Pancuronium ETT No Yes No No Yes
47 Pancuronium ETT No Yes No No Yes No No
48 Succinylcholine,pancuronium
EBT Yes Yes No Yes Yes No Yes

88 Appendix
Details of recollection and after-effects
Patient Immediateanxiety
Duration ofawareness asestimated by thepatient
Awareness as themost unpleasant
experienceduring operation
After effects
38 No Seconds No
39 No
40 No
41 No
42 Yes No
43 No No
44 No
45 No
46 No
47 Yes Yes
48 Yes

Appendix 89
Patient Comments
38 Feeling of pulling drains out of chest suggests this to be post-operative recollection from the ICU
39 Possible post-operative recollection from the ICU
40
41 Possible post-operative recollection from the ICU
42
43 Possible post-operative recollection from the ICU
44 Possible post-operative recollection from the ICU
45 Possible post-operative recollection from the ICU
46 Reoperation anesthesia: diazepam, fentanyl and non-continuous isoflurane. Recollections possibly fromthe time between the operations.
47
48

90 Appendix
Patient
Patient Study Year ofanesthesia
Age(years)
Sex Weight(kg)
Height(cm)
Surgery
49 4,5 1989 27 M 70 180 Appendectomy
50 4,5 1990 41 F 65 163 Explorative laparotomy
51 4,5 1992 36 F 80 173 Laparoscopic sterilization
52 4 1992 37 F 97 169 Tonsillectomy
53 4 1994 25 F 55 169 Laparoscopic cholecystectomy
54 4 1992 47 F Mastectomy with axillary lymph nodedissection
55 4 1995 26 F 64 162,5 Laparoscopic cholecystectomy later convertedto laparotomy
56 4 1996 56 F 80 163 Incision of plantar abscess
57 4 1994 38 M 81 176 Thyreoidectomy
58 4 1994 33 F 61 162 Thyroid resection
59 4 1991 68 F 67 168 Cholecystectomy

Appendix 91
Anesthetic details
Patient Recalled experience Awarenessgroup
Duration ofanesthesia
(min)
Premedication
49 Fell asleep, then felt that something was pushed in to hismouth and throat. Heard somebody saying: "it is gone".Interpreted this meaning that he will die. Felt skin incisionin his abdomen, tried to move but was not able.
3 127 Opioid
50 During the course of the operation she gradually started tofeel agonizing pain. She tried to scream or move, but wasable to move her eyes only. Delusions mixed with pain, andshe thought that her family is tearing her abdomen.
3 114 Opioid
51 Stated that she was awake during the operation, and withterrible pain and fear of death. She also stated that herdoctors deny the possibility of awareness. The patient hadseen a general practitioner few days after the operationbecause of inability to sleep and preoccupation with death.According to the general practitioner's notes, the patient hadregained consciousness during the operation and had beenunable to move.
3 23 Benzodiazepine
52 Felt pain, and operation in her mouth. Heard discussionswhere a doctor suspected that the patient is not adequatelyanesthetized, while another doctor replied that: yes, she is.
3 57 Benzodiazepineand opioid
53 Felt something put her mouth, heard discussions, felt theentry of laparoscopic instruments.
3 100 Benzodiazepine
54 Woke in the middle of the operation, unable to move,shortness of breath, unable to breathe, then fell asleep again.
3 123 Benzodiazepine
55 Woke early after induction, was unable to move but felt theintubation tube. Felt four sticking wounds done on herabdomen and after that excruciating pain. Heard theoperator say: "there is no other solution but to open theabdomen". Felt somebody dry tears on her cheeks and say"is she asleep at all". Saw silver colored instruments and abrownish lump taken out of her abdomen.
3 90 Benzodiazepine
56 Excruciating pain, inability to move. 3 58 Benzodiazepine
57 Fell asleep, then heard discussions: a male voice speakingabout the teeth, also women voices but cannot recall thediscussions. Then felt something pushed in his throat, thisfelt unpleasant but not painful. Tried to move but wasunable to.
2 223 Opioid
58 Felt onion taste in her mouth, then something was pushedin her mouth and throat. Tried to move but was unable.
2 124 Opioid
59 Fell asleep, then heard discussions that she cannot recall,then felt excruciating pain in the abdomen, felt themanipulation of abdominal organs.
3 78 Antihistamine

92 Appendix
Anesthetic details
Patient Co-induction Induction Maintenance N2O ETAGCmonitoring
49 Fentanyl Thiopental Enflurane (part time) Yes Not recorded
50 Fentanyl Propofol Propofol (bolus dosing) Yes No
51 Alfentanil Propofol Isoflurane No Not recorded
52 Fentanyl Thiopental None Yes No
53 Fentanyl Thiopental Propofol-infusion, enflurane No Not recorded
54 Fentanyl Thiopental Enflurane Yes Not recorded
55 Fentanyl Thiopental Enflurane Yes Not recorded
56 Fentanyl Thiopental Enflurane Notrecorded
Not recorded
57 Fentanyl Thiopental Enflurane Yes Not recorded
58 Fentanyl Thiopental Enflurane Yes Not recorded
59 Droperidol,fentanyl
Thiopental Enflurane Yes Not recorded

Appendix 93
Anesthetic details Details of recollection and after-effects
Patient NMB Airway Pain Auditory Visual Tactile Tried tomove
Able tomove
Immediateunderstanding
49 Succinylcholine,vecuronium
ETT Yes Yes No Yes Yes No Yes
50 Succinylcholine,vecuronium
ETT Yes No No Yes Yes No Yes
51 Atracurium ETT Yes Yes No Yes
52 Vecuronium ETT Yes Yes No Yes Yes No Yes
53 Vecuronium ETT Yes Yes No Yes Yes
54 Vecuronium ETT Yes Yes No Yes
55 Vecuronium ETT Yes Yes Yes Yes Yes No Yes
56 Vecuronium ETT Yes No No Yes Yes No Yes
57 Vecuronium ETT No Yes No Yes Yes No Yes
58 Vecuronium ETT No no no Yes Yes No Yes
59 Succinylcholine,pancuronium
ETT Yes Yes No Yes Yes

94 Appendix
Details of recollection and after-effects
Patient Immediateanxiety
Duration ofawareness asestimated by thepatient
Awareness as themost unpleasant
experienceduring operation
After effects
49 Yes Flashbacks when falling asleep, unable to sleep,fear of another operation.
50 Yes Nightmares, flashbacks of the operation.
51 Yes Fear of death and fear of falling asleep during athree-week period after anesthesia. Neededsedative medication during that time.
52 Yes Depression, sleep disturbances, on diazepammedication for a week after the anesthesia. Fourmonths after the anesthesia receiving psychiatrictreatment. Fear of further operations.
53 Yes Anxiety.
54 Yes Six months after the anesthesia receivedpsychiatric treatment for post-traumatic stressdisorder.
55 Yes At two months after anesthesia extreme anxiety,unable to leave her apartment because of fearand anxiety. Unable to return to her work.
56 Yes
57 Yes One minute None
58 No Seconds No
59

Appendix 95
Patient Comments
49
50
51
52
53
54
55
56
57
58
59

96 Appendix
Patient
Patient Study Year ofanesthesia
Age(years)
Sex Weight(kg)
Height(cm)
Surgery
60 4 1987 41 F 56 164 Insertion of breast implant
61 4 1976 25 F 55 171,5 Bronchography
62 4 1996 22 F 70 173 Oophorectomy
63 4 1995 23 F 28,5 Revision of gluteal ulcer
64 4 1997 40 F 70 173 Sterilization
65 4 1994 70 F 80 172 Excision of coecal adenoma
66 4 1976 35 F 86 165 Caesarean section, sterilization
67 4 1993 40 F 64 168 Laparoscopic cholecystectomy
68 4 1993 38 F 60 160 Salpingo-oophorectomy
69 4 1991 24 F 69 169 Laparotomy for endometriosis
70 4 1979 41 F 80 163 Extirpation of intervertebral disc prolapse.

Appendix 97
Anesthetic details
Patient Recalled experience Awarenessgroup
Duration ofanesthesia
(min)
Premedication
60 Woke in the middle of the operation, heard discussions,he ard th e a nes th e s io lo g i s t c omment h er rh ythmdisturbances. Felt that something is in her mouth andthroat. Thought that she is dying, unable to move, extremeanxiety.
3 152 Opioid
61 Awareness during two bronchographies two days apart. Fellasleep, then woke and saw a long catheter being pushed inher mouth. Herd discussions (on the second occasion agroup of medical students trained intubation)
2 15 Opioid
62 Pain and manipulation in the abdomen. 2 94 None
63 Woke in the middle of the operation, saw people dressed inwhite around her, felt the endotracheal tube in her mouth,was unable to move, no pain.
3 99 None
64 Felt the scrubbing and positioning during the preparationof operation, heard discussions the content of which shedoesn't recall..
3 30 None
65 Feels that did not fall asleep at all but felt intubation tubebeing pushed in her mouth. Tried to move and signalawareness but was unable. Then felt skin incision, deeperopening of the abdominal wall, manipulation of abdominalorgans. Worst pain when the intestines were pushed back toabdominal cavity. Recalls discussions, recalls that someoneopened her eye twice.
3 84 Opioid
66 Recalls having thought: "why you are putting that tube intomy mouth", noises, shortness of breath.
2 46 None
67 Heard noises, saw lights, felt the scrubbing, tried to signalawareness but could not.
2 135 None
68 Discussions, pain and manipulation in the abdomen,inability to move or breathe.
3 80 Benzodiazepine
69 Shortness of breath before intubation, extreme anxiety, fearof dying.
2 38 Benzodiazepine
70 Shooting pain in the back 3-4 times, between episodes ofpain was in a light sleep. Tried to move but could not. Feltsomething in her mouth.
3 112 Opioid

98 Appendix
Anesthetic details
Patient Co-induction Induction Maintenance N2O ETAGCmonitoring
60 Fentanyl Thiopental Enflurane Yes Not recorded
61 None Thiopental None No No
62 Remifentanil Propofol Propofol-infusion, remifentanil-infusion
No No
63 Fentanyl Thiopental Thiopental (bolus dosing),isoflurane (non-continuous)
No Not recorded
64 Fentanyl Propofol Propofol (bolus dosing),isoflurane
No Not recorded
65 Fentanyl Thiopental Enflurane No Not recorded
66 Meperidine Thiopental Thiopental (bolus dosing) Yes No
67 Alfentanil Propofol Propofol-infusion, isoflurane No Not recorded
68 Fentanyl Propofol Enflurane Yes Not recorded
69 Fentanyl Propofol Propofol-infusion Yes No
70 Meperidine Thiopental None Yes No

Appendix 99
Anesthetic details Details of recollection and after-effects
Patient NMB Airway Pain Auditory Visual Tactile Tried tomove
Able tomove
Immediateunderstanding
60 Vecuronium ETT No Yes No Yes Yes No Yes
61 Succinylcholine Mask No Yes Yes Yes Yes Yes Yes
62 Atracurium ETT Yes No No Yes
63 Atracurium ETT No Yes Yes Yes Yes No Yes
64 Atracurium ETT No Yes No Yes Yes No Yes
65 Vecuronium ETT Yes Yes Yes Yes Yes No Yes
66 Succinylcholine ETT No Yes No Yes Yes No Yes
67 Vecuronium ETT No Yes Yes Yes Yes No Yes
68 Pancuronium ETT Yes Yes No Yes Yes No Yes
69 Succinylcholine,vecuronium
ETT No Yes No Yes Yes No Yes
70 Allopherine ETT Yes No No Yes Yes No Yes

100 Appendix
Details of recollection and after-effects
Patient Immediateanxiety
Duration ofawareness asestimated by thepatient
Awareness as themost unpleasant
experienceduring operation
After effects
60 Yes Minutes Considers the experience as the worst one in herlife. Nine years after the operation fears allfurther operations and suffers from nightmaresand sleep disturbances
61 Yes Eighteen years after anesthesia wakes sometimesfrom a nightmare that she is in the middle ofthe operation. The incidence of nightmares hasdiminished over the years.
62
63 Yes Several minutes Three years after the anesthesia nightmares ofthe operation sometimes wake her from sleep.
64 No Less than 5minutes
65 Yes Very long Told of her experience immediately in therecovery room. Discussions with theanesthesiologist, nurses, and a clinicalpsychologist were immediately organized.According to the psychologist, the debriefingwas effective. Four years after the experience,the patient does not suffer form obvious after-effects.
66 Yes Not long In a subsequent cholecystectomy was veryfrightened of anesthesia.
67 Yes 1-2 minutes No
68 Yes Several minutes Frightened of subsequent operations.
69 Yes Not long
70 Yes Not long, butrecurred 3-4times.
Bad nightmares and sleep disturbances for overten years. Not able to return to work.

Appendix 101
Patient Comments
60
61
62
63
64
65
66
67
68
69
70