Awareness of Illness in Schizophrenia
20
VOL. 17, NO. 1, 1991 Awareness of Illness in Schizophrenia 113 by Xavier F. Amador, David H. Strauss, Scott A. Yale, and Jack M. Gorman Abstract This article reviews the literature on "poor insight" or unawareness of ill- ness in schizophrenia. A large body of knowledge representing several different perspectives on insight has developed. This work can be divided into three broad categories, suggest- ing an important role for insight in the phenomenology, pathophysiol- ogy, and treatment of schizophrenia. The argument is made here that many of the self-awareness deficits observed in schizophrenia are of di- agnostic significance, are neurally based, and are indispensable in guid- ing treatment decisions. In addition, this article proposes guidelines for assessing unawareness of illness in schizophrenia and discusses the rele- vance of such deficits to the diagno- sis of schizophrenia. Individuals with schizophrenia have often been observed to ignore the deficits caused by their illness and the effect their illness has on their lives. This lack of awareness, typi- cally described as "poor insight," is believed to contribute to noncompli- ance with treatment. The relationship between schizophrenia and poor in- sight was identified when the disor- der was first named by Bleuler (Bertschinger 1916; Mayer-Gross 1920, as cited in Wciorka 1988). Al- though the concept of insight is widely used in psychiatry, it has ac- quired a variety of meanings (Green- feld et al. 1989). In recent years, an impressive body of knowledge repre- senting several different perspectives on insight has developed. This work can be divided into three broad cate- gories, suggesting an important role for insight in the phenomenology, pathophysiology, and treatment of schizophrenia. This article reviews the literature on unawareness of illness in schizo- phrenia. We will begin by focusing on the relevance of insight to diagno- sis and classification in schizo- phrenia. Next, we will discuss re- search on unawareness of deficits; this work coming largely from the neurological literature, bears on is- sues of etiology and pathophysiology in schizophrenia. Finally, we will review studies that assess insight as a predictor of treatment compliance and outcome. We will argue throughout that many of the self- awareness deficits observed in schizo- phrenia are of diagnostic signifi- cance, are neurally based, and are indispensable in guiding treatment decisions. In addition, we will pro- pose guidelines for ascribing unawareness of illness in schizo- phrenia and will make recommenda- tions for its measurement. Before any review of the literature, a discussion of terminology and mea- surement is in order. Terminology A variety of terms have been applied to the observed unawareness of ill- ness in schizophrenia, including "poor insight," "sealing over," "de- fensive denial," "attitudes about illness," "indifference reaction," "evasion," and "external attributions" (McGlashan et al. 1975; Wciorka 1988; Greenfeld et al. 1989; David 1990). These different terms reflect important underlying conceptual dif- ferences. On one end of the spec- Reprint requests should be sent to Dr. X.F. Amador, Dept. of Clinical Psychobi- ology, Schizophrenia Research Unit, Box 2, New York State Psychiatric Institute, 722 West 168th Street, New York, NY 10032. by guest on June 24, 2015 http://schizophreniabulletin.oxfordjournals.org/ Downloaded from
Transcript of Awareness of Illness in Schizophrenia

VOL. 17, NO. 1, 1991 Awareness of Illness inSchizophrenia
113
by Xavier F. Amador, David H.Strauss, Scott A. Yale, andJack M. Gorman
Abstract
This article reviews the literature on"poor insight" or unawareness of ill-ness in schizophrenia. A large bodyof knowledge representing severaldifferent perspectives on insight hasdeveloped. This work can be dividedinto three broad categories, suggest-ing an important role for insight inthe phenomenology, pathophysiol-ogy, and treatment of schizophrenia.The argument is made here thatmany of the self-awareness deficitsobserved in schizophrenia are of di-agnostic significance, are neurallybased, and are indispensable in guid-ing treatment decisions. In addition,this article proposes guidelines forassessing unawareness of illness inschizophrenia and discusses the rele-vance of such deficits to the diagno-sis of schizophrenia.
Individuals with schizophrenia haveoften been observed to ignore thedeficits caused by their illness andthe effect their illness has on theirlives. This lack of awareness, typi-cally described as "poor insight," isbelieved to contribute to noncompli-ance with treatment. The relationshipbetween schizophrenia and poor in-sight was identified when the disor-der was first named by Bleuler(Bertschinger 1916; Mayer-Gross1920, as cited in Wciorka 1988). Al-though the concept of insight iswidely used in psychiatry, it has ac-quired a variety of meanings (Green-feld et al. 1989). In recent years, animpressive body of knowledge repre-senting several different perspectiveson insight has developed. This workcan be divided into three broad cate-gories, suggesting an important rolefor insight in the phenomenology,pathophysiology, and treatment ofschizophrenia.
This article reviews the literatureon unawareness of illness in schizo-phrenia. We will begin by focusingon the relevance of insight to diagno-sis and classification in schizo-phrenia. Next, we will discuss re-search on unawareness of deficits;this work coming largely from theneurological literature, bears on is-sues of etiology and pathophysiologyin schizophrenia. Finally, we willreview studies that assess insight as apredictor of treatment complianceand outcome. We will arguethroughout that many of the self-awareness deficits observed in schizo-phrenia are of diagnostic signifi-cance, are neurally based, and areindispensable in guiding treatmentdecisions. In addition, we will pro-pose guidelines for ascribingunawareness of illness in schizo-phrenia and will make recommenda-tions for its measurement.
Before any review of the literature,a discussion of terminology and mea-surement is in order.
Terminology
A variety of terms have been appliedto the observed unawareness of ill-ness in schizophrenia, including"poor insight," "sealing over," "de-fensive denial," "attitudes aboutillness," "indifference reaction,""evasion," and "external attributions"(McGlashan et al. 1975; Wciorka1988; Greenfeld et al. 1989; David1990). These different terms reflectimportant underlying conceptual dif-ferences. On one end of the spec-
Reprint requests should be sent to Dr.X.F. Amador, Dept. of Clinical Psychobi-ology, Schizophrenia Research Unit, Box2, New York State Psychiatric Institute,722 West 168th Street, New York, NY10032.
by guest on June 24, 2015http://schizophreniabulletin.oxfordjournals.org/
Dow
nloaded from

114 SCHIZOPHRENIA BULLETIN
trum, poor insight is understood as apsychological defense mechanism; atthe other extreme, it denotes a theo-retical position implicating cognitivedeficit. In between lies a quagmire ofrelated constructs that vary with theorientations of their authors. For ex-ample, from researchers grounded incognitive psychology have comestudies examining the "external attri-butions about illness" of schizo-phrenic patients (Wciorka 1988).Psychodynamically oriented explana-tions of poor insight have also beengiven (e.g., denial as a defense mech-anism) and include a subdivision ofemotional versus intellectual insight(Richfield 1954). Most of these differ-ing constructs signify a particularetiology for poor insight.
Furthermore, the poor insight de-scribed in schizophrenia is not a uni-tary construct. For example, Wciorka(1988) and others (Greenfeld et al.1989; David 1990) have argued thatinsight comprises a variety of phe-nomena. It has subtypes (e.g., retro-spective and current insight), and, bydefinition, it forces presumptionsabout the nature of reality (David1990). However, whatever the natureof reality, the phenomenon of inter-est here is one in which an individ-ual's perception of himself is grosslyat odds with that of his communityand culture. Indeed, it is at oddseven with the views of similarly af-fected psychiatric patients (Wing etal. 1964).
At the most fundamental level,then, what has been described inschizophrenia is a seeming lack ofawareness of the deficits, the conse-quences of the disorder, and the needfor treatment. We will use the term"unawareness of illness" in thisbroadest sense. However, we agreewith those authors who propose thatinsight is best conceptualized as amultidimensional construct. In keep-
ing with this perspective, and to al-low for more precise comparisonsbetween studies, we will comment onour view of the specific phenomenacomprising the dependent variablesassessed.
The Measurement ofSelf-Awareness Deficits
The measurement of insight inschizophrenia has received little criti-cal attention in the literature. Vari-ous methods for measuring insighthave been reported. Thosecommonly used can be broadly di-vided into five categories: (1) clinicaldescriptions of free responses (i.e.,spontaneous patient behaviors), (2)clinical descriptions of free responsesto a controlled stimulus, (3) system-atized scoring of free responses, (4)systematized scoring of response to astandard stimulus, and (5) multiplechoice. These categories have previ-ously been identified in a method-ological critique of studies of schizo-phrenic language (Chapman andChapman 1973). In this section, wewill briefly review the various meth-ods, discuss the advantages and dis-advantages of each, and present rec-ommendations for future work.
Clinical Descriptions of FreeResponses. The majority of the earlystudies on insight in schizophreniafall into the category of clinical de-scriptions of free responses. Most ofthese studies are based on case mate-rials describing patients' beliefs aboutwhether or not they are mentally ill(e.g., Bertschinger 1916;Mayer-Gross 1920; Martin 1952;Richfield 1954; Tolor and Reznikoff1960; Sacks et al. 1974). Using thismethod, the investigator places norestrictions on the patients'responses, nor are restrictions neces-
sarily placed on the investigator'sown categories for describing the re-sponses. The investigator simplynotes the spontaneous behavior ofschizophrenic patients, speaks withthe patients, or examines their writ-ings. The advantage to this methodis that it does not restrict observa-tions or hypothesis making, and itmaximizes the chances of observingnew phenomena. A conspicuousdrawback to this technique is theextreme variability of the elicitingstimuli and responses, making gener-alizability and replication extremelydifficult.
Clinical Descriptions of FreeResponses to a Controlled Stimulus.One method of reducing the variabil-ity mentioned above is to control thesituation that elicits the response.With the implementation of a con-trolled stimulus, some ambiguity canbe reduced. Any structured psychiat-ric interview, when interpreted with-out standardized scoring, would alsofall under this category of data col-lection. The most widely used clini-cal test of insight that falls into thiscategory is the Mental Status Exam(MSE; Talbott et al. 1988). Insight,as generally assessed in the MSE, isconsidered present "if the patient re-alizes that he is ill and the problemis in his own mind" (MacKinnon andYudofsky 1986, p. 76). Several stud-ies, particularly those reliant onchart review for their dependentmeasures, have used the MSE to cat-egorize patients along the insight di-mension (e.g., Eskey 1958; Caracci etal. 1990). Clinical descriptions of pa-tients' responses to semistructuredinterviews have also been used (e.g.,McGlashan et al. 1975; Greenfeld etal. 1989).
This method is useful for lesseningthe ambiguity as to what elicits the
by guest on June 24, 2015http://schizophreniabulletin.oxfordjournals.org/
Dow
nloaded from

VOL. 17, NO. 1, 1991 115
patients' responses; moreover, it af-fords the possibility of direct com-parison between schizophrenic pa-tients and other groups. If twogroups are given the same standard-ized stimuli, their responses can becompared less ambiguously thanwould be the case if their everydaybehavior were simply observed andthen compared. The disadvantage tothis method is the subjectivity in theclinical observation of the patients'responses.
Systematized Scoring of FreeResponses. The method of system-atized scoring of free responses issimilar to the first method discussed;however, the interpretation of thedata is more systematic. A system isdevised to categorize patients' re-sponses, making comparisons be-tween studies easier. Taken to itsextreme, this method includes the useof continuous variables within eachcategory. For example, Wciorka(1988) tape-recorded patients'thoughts about how they definedtheir illness. He subsequently ratedthe tapes based on six categories ofattitude about illness and used a 5-point scale to quantify responses as-signed to each category. Others haveemployed similar techniques in theirmeasurement of insight (WorldHealth Organization 1973; Carpenteret al. 1976; Van Putten et al. 1976;Lin et al. 1979; Rosen et al. 1982;Heinrichs et al. 1985; Wilson et al.1986; Bartko et al. 1988).
The benefit of this method is thatit allows for the quantification of thedependent measure, permitting statis-tical analyses. Additionally, it pro-vides the opportunity for several ex-perimental controls not available inthe first two methods; for example,raters can be blind to experimentalhypotheses, subject identity, etc. Re-
liability can be established betweenraters, and the replicability of thestudy is increased. The main limita-tion to this approach is that someresponses may not fit neatly into thecategories created and, consequently,information is lost.
Systematized Scoring of Response toa Standard Stimulus. Anothermethod involves the use of a stand-ardized stimulus to elicit responses.The subject can respond in a varietyof ways; however, the response isscored in terms of predetermined cat-egories. Several semistructured inter-views and questionnaires have beenreported in the literature (Thurm andHaefner 1987; Greenfeld et al. 1989;McEvoy et al. 1989fc). We (X.F.A.,D.H.S.) have developed a semistruc-tured interview and scale to assessUnawareness of Mental Disorder(SUMD). The SUMD allows for theindependent assessment of patients'current and retrospective awarenessof having a mental disorder. Otherdimensions assessed include patients'awareness of various signs andsymptoms, of benefit fromtreatment, and of the psychosocialconsequences of mental disorder. At-tributional patterns in each of theseareas are also assessed, as patientsare questioned in each area, andtheir responses are rated on 5-pointscales. We are currently conducting areliability and construct validitystudy in a large sample of patientswith schizophrenia and other psy-chotic disorders.
The value of the method discussedabove is that the eliciting stimuli areconsistent from subject to subject,and the criteria by which one catego-rizes responses can be carefully de-fined. The probability of replicatingthe procedure and results is fargreater than is the case with clinical
interpretation of the same data. Theobvious disadvantage is that manyresponses cannot be scored meaning-fully using scoring schemes. If allresponses to a test must be forced tofit into a limited set of preconceivedcategories, there will undoubtedly beinstances when some responses arearbitrarily placed into those catego-
Multiple Choice. In the multiplechoice method, the patient is pre-sented with a standardized stimulusand given the choice between two ormore alternative responses. For ex-ample, Soskis and Bowers (1969) de-veloped a 55-item questionnaire forpatients. For each item, patients wereasked to indicate whether the state-ment applied to them. Statementssuggestive of an insight-positive atti-tude included "It always helps to sitdown and think things through," and"When I feel strange or bad, I like tostop and try to figure out what iscausing it. ' Insight-negative state-ments included "There are certain ofmy problems that I would rather for-get about," and "When I feel strangeor bad, the best thing to do is tokeep busy and hope it will go away"(Soskis and Bowers 1969, p. 446).Overall insight score was tabulatedby subtracting the number of nega-tive statements endorsed from thenumber of positive statements en-dorsed. A few studies have used sim-ilar techniques (e.g., Lin et al. 1979;McGlashan and Carpenter 1981).
The use of multiple choice ques-tionnaires provides an easy methodfor obtaining multiple sources of in-formation. For example, we havedeveloped a SUMD questionnaire forrelatives to complete about their psy-chiatrically ill family member. Thecollection of confirming evidencefrom multiple sources is essential to
by guest on June 24, 2015http://schizophreniabulletin.oxfordjournals.org/
Dow
nloaded from

116 SCHIZOPHRENIA BULLETIN
the issue of construct validity, whichwill be considered below.
In summary, these five generalstrategies for measuring insight haverelative strengths and weaknesses. Inlarge part, the choice of any particu-lar method over another requires anassessment of the goals of the inves-tigation. If the aim is to perform anexploratory, hypothesis-generatingstudy, the first two methodsdescribed above seem appropriate. Ifthe aim is to generate replicable re-search, the last three methods aremore appropriate. We also recom-mend that future work in this areafocus more on the issue of constructvalidity. We will argue below thatseveral studies, under the pretense ofstudying insight, have in fact meas-ured multiple constructs simultane-ously. To increase construct validity,future investigations in this areashould seek to assess multiple inde-pendent measures of the same phe-nomenon.
Diagnostic Relevance
Is Poor Insight a Sign ofSchizophrenia? The identification ofa schizophrenia syndrome(s) basedon signs and symptoms has been acomplex task. In large part, this isdue to the heterogeneity of the disor-der and the overlap of symptomsamong the traditional subtypes. Inthe past decade, there has been aresurgence of interest in subtypingschizophrenia (e.g., Andreasen 1982).As shall be seen, the literature onunawareness of illness in schizo-phrenia is relevant to the task of de-veloping more meaningful subtypes.
In an attempt to better identifymore distinct subtypes of schizo-phrenia, Carpenter and his associates(1976) employed cluster analytictechniques on quantified sign and
symptom data. This study, based ondata collected from the InternationalPilot Study of Schizophrenia (IPSS;World Health Organization 1973),provided a unique opportunity todetermine whether subtype diagnosesdefine groups of patients similarlyacross cultures. From the results ofthis study, Carpenter et al. (1976)observed that poor insight was aprevalent feature of schizophreniaand that level of insight was an im-portant discriminating factor in mak-ing subtype diagnoses. Of 811 sub-jects studied, 680 were initiallyassigned to one of the following sixschizophrenia subtypes: simple, hebe-phrenic, catatonic, paranoid, acute,and schizoaffective. The scores onthe 27 dimensions assessed on thePresent State Examination (PSE;Wing et al. 1974) (table 1) were thensubmitted to a profile analysis ofvariance, which revealed that thesubtypes were not readilydistinguishable from one another.Carpenter and his associates suggestthat, as generally employed, thesesubtypes may be of limited value.They add that their findings, if repli-cated, challenge the use of the tradi-tional signs and symptoms to definethese subtypes. Largely due to theirunreliability, these subtypes as origi-nally described are no longer used incurrent diagnostic criteria (Black etal. 1988). However, the traditionalsigns and symptoms continue to beused in most nosological schemes.
Having found little symptomaticdiscrimination between traditionalsubtypes. Carpenter et al. (1976) sub-mitted data from the same 27 dimen-sions to a cluster analysis and identi-fied four distinct and mathematicallydefined clusters (total n = 573).These were viewed as potentiallymeaningful subtypes of schizophreniaby the authors, who labeled them"typical," "flagrant," "insightful,"
and "hypochondriacal." As can beseen in figure 1, typical schizo-phrenia was characterized by poorinsight, persecutory and passivitydelusions, auditory hallucinations,social withdrawal, and restricted af-fect. The second cluster, flagrantschizophrenia, "was distinguished byaberrant, agitated, or bizarre behav-ior, incomprehensibility, unkemptappearance, incongruent or restrictedaffect, and absence of anxiety or de-pression" (Carpenter et al. 1976,p. 515). Insightful schizophreniashared many of the features of typi-cal schizophrenia, but it had goodrather than poor insight. The fourthcluster, hypochondriacal schizo-phrenia, was characterized by inter-mediate insight and distinguished byincreased somatic concerns and vi-sual hallucinations. The authors raiseseveral methodological issues havingto do with their use—which wasnovel at the time—of cluster analytictechniques to define diagnosticgroups. They caution that their re-sults should be considered prelimi-nary pending replication and validitystudies.
In a more recent multinationalstudy entitled Classification ofChronic Hospitalized Schizophrenics(CCHS), the 12 signs and symptomsof the Flexible System Criteria (Car-penter et al. 1973) were assessed in asample of 768 patients (Wilson et al.1986). The results of this study repli-cated the IPSS finding of high ratesof poor insight in schizophrenia. Pa-tients were included if they receiveda hospital diagnosis of schizophreniaby ICD-9 (World Health Organiza-tion 1978) criteria that was independ-ently confirmed by one of the re-searchers. In addition, patients hadto evidence at least five of the symp-toms from the Flexible System Crite-ria. Wilson and colleagues contrasted
by guest on June 24, 2015http://schizophreniabulletin.oxfordjournals.org/
Dow
nloaded from

VOL 17, NO. 1, 1991 117
Table 1. Psychopathologic dimensions1
Dimension
1. Depression2. Anxiety3. Restlessness4. Psychomotor retardation5. Hypomania/mania6. Somatic concerns7. Belligerence8. Obsessions9. Unkempt appearance
10. Disorientation11. Lack of insight12. Depersonalization/derealization13. Paranoid delusions14. Grandiose delusions15. Delusions of passivity16. Depressive and nihilistic
delusions17. Other delusions18. Visual hallucinations19. Auditory hallucinations20. Other hallucinations21. Bizarre behavior22. Withdrawal23. Incomprehensibility24. Nonsocial speech25. Restricted affect26. Labile affect27. Incongruous affect
Interclassreliability
0.920.840.740.890.920.780.860.780.590.330.790.860.930.930.920.85
0.840.820.920.920.810.820.830.760.650.590.66
No. of PSE2
items
2446915143111
1017577
3135166164311
'Reprinted, with permission, from Carpenter etMedical Association, 1976.2Present State Examination.
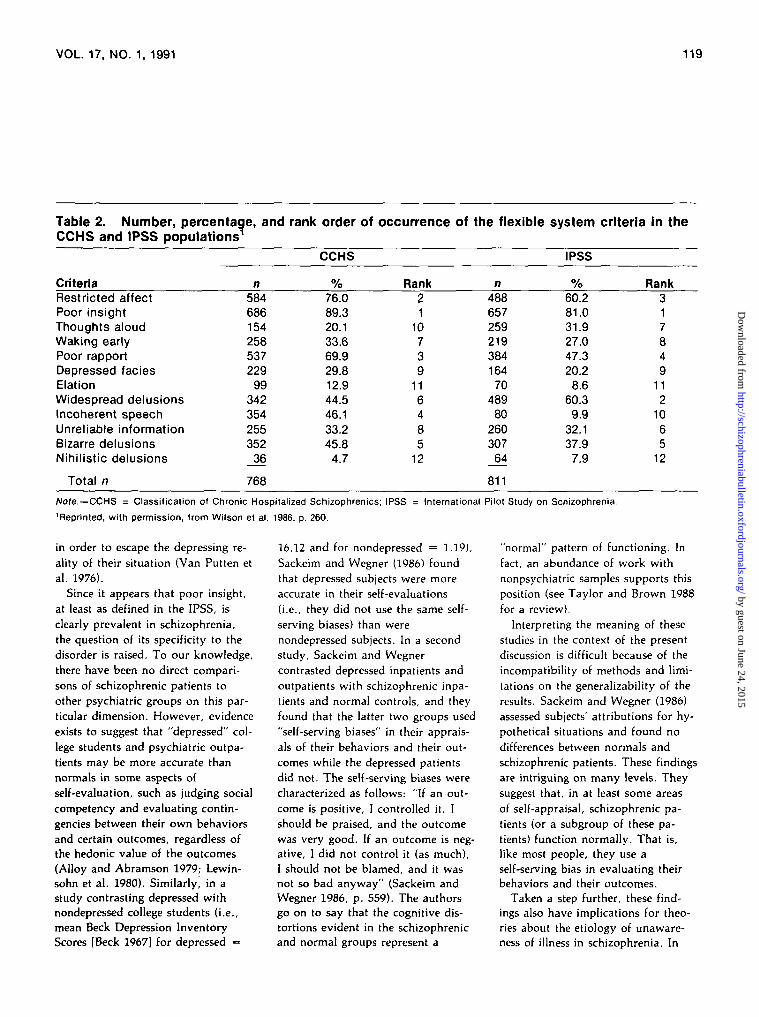
the sign and symptom data from thischronic sample to the relatively moreacute IPSS sample (n = 811). Thedata contrasted were the numbers,percents, and rank order of the 12signs and symptoms. As can be seenin table 2, poor insight occurredmore often across both samples thandid any other dimension. Interest-ingly, when they calculated a rankorder correlation coefficient to assessthe relations between these two sam-ples, they found a strong similarityin the rank order of occurrence of all12 items (r's = +0.76). The items
al. (1976, p. 511). Copyright © American
that differed the most between sam-ples were incoherent speech, wide-spread delusions, and thoughtsaloud. Next, using the same data,Wilson et al. (1986) categorized theCCHS sample by ICD-9 subtypesand compared those groups. Most ofthe patients were diagnosed as hav-ing hebephrenic (n = 240) or para-noid (n = 238) schizophrenia; therest received diagnoses of simple (n= 53), catatonic (n = 46), or schi-zoaffective (n = 24) schizophrenia,or did not fit into any of these cate-gories (n = 167). The authors found
that widespread delusions, wakingearly, and depressed facies showedthe greatest variability betweensubtypes, while poor insight,restricted affect, and nihilistic delu-sions showed the least. They con-clude that these comparisons suggesta shift in chronic schizophrenia to-ward more negative features. What isparticularly noteworthy for this dis-cussion is the authors' independentreplication, in a second large multi-national sample, of the finding ofboth the prevalence of poor insight(as defined in the IPSS) and its orderof occurrence relative to other signsand symptoms.
In both studies reviewed(Carpenter et al. 1976; Wilson et al.1986), insight was defined as present"if there was some awareness ofemotional illness" and absent if thepatient "vigorously denied he wasdisturbed" (World Health Organiza-tion 1973). Such a definition of in-sight is conservative: it requires onlythat the patient evidence someawareness of emotional illness. In theIPSS, awareness need not be accom-panied by correct attribution for spe-cific signs and symptoms (i.e.,awareness of specific symptoms andaccurate identification of these as aconsequence of mental illness) to becalled insight. Similarly, the IPSSgeneral definition of insight does notrequire that the patient express rec-ognition of the need for treatment.This definition of insight approxi-mates that used by most clinicians intheir implementation of the MSE. Onthe other hand, the IPSS definitionof absence of insight is narrow andmay identify something other than alack of awareness. For example, theargument can be made that patientswho "vigorously" deny the existenceof a mental illness may be respond-ing defensively to a recognition ofthe very deficits they are disavowing
by guest on June 24, 2015http://schizophreniabulletin.oxfordjournals.org/
Dow
nloaded from

118 SCHIZOPHRENIA BULLETIN
Figure 1. Dimension scores on the 27 items of the Present State Examination (PSE) for four clus-ters: Typical, flagrant, insightful, and hypochondriacal schizophrenia1
Psychopathologic Dimensions
Note:—Profile clutter 1 (n = 439). typical schizophrenia.
I9 20 31 22 n 24 2S 2t 27
Psychopathologic Dimensions
Note:—Profile clutter 3 (n = 29). Irtilghttul tchlzophrenla.
17 IS 19 20 21 22 23 24 25 M 27
Psychopathologic Dimensions
Note:—Profile clutter 2 (n = 25). flagrant schizophrenia.
- S
s5
-J I L t I I 1 I I
Psychopathologic Dimensions
-Profile duster 4 (n = 80). hypochondriacal tchlzophrenla.
I 20 21 22 23 24 25 2S 27
Note.—See table 1 for the 27 PSE dimensions.
'Reprinted, with permission, from Carpenter et al. (1976, pp. 512-514). Copyright @ American Medical Association, 1976.
by guest on June 24, 2015http://schizophreniabulletin.oxfordjournals.org/
Dow
nloaded from
VOL. 17, NO. 1, 1991 119
Table 2. Number, percentage, andCCHS and IPSS populations1
CriteriaRestricted affectPoor insightThoughts aloudWaking earlyPoor rapportDepressed faciesElationWidespread delusionsIncoherent speechUnreliable informationBizarre delusionsNihilistic delusions
Total n
n584686154258537229
99342354255352
36
768
rank order of
CCHS
%76.089.320.133.669.929.812.944.546.133.245.8
4.7
occurrence
Rank21
10739
116485
12
of the flexible
n48865725921938416470
48980
26030764
811
system
IPSS
%60.281.031.927.047.320.2
8.660.39.9
32.137.9
7.9
criteria in the
Rank317849
112
1065
12
Note.—CCHS = Classification of Chronic Hospitalized Schizophrenics; IPSS = International Pilot Study on Schizophrenia.
'Reprinted, with permission, from Wilson et al. 1986, p. 260.
in order to escape the depressing re-ality of their situation (Van Putten etal. 1976).
Since it appears that poor insight,at least as defined in the IPSS, isclearly prevalent in schizophrenia,the question of its specificity to thedisorder is raised. To our knowledge,there have been no direct compari-sons of schizophrenic patients toother psychiatric groups on this par-ticular dimension. However, evidenceexists to suggest that "depressed" col-lege students and psychiatric outpa-tients may be more accurate thannormals in some aspects ofself-evaluation, such as judging socialcompetency and evaluating contin-gencies between their own behaviorsand certain outcomes, regardless ofthe hedonic value of the outcomes(Alloy and Abramson 1979; Lewin-sohn et al. 1980). Similarly, in astudy contrasting depressed withnondepressed college students (i.e.,mean Beck Depression InventoryScores [Beck 1967] for depressed =
16.12 and for nondepressed = 1.19),Sackeim and Wegner (1986) foundthat depressed subjects were moreaccurate in their self-evaluations(i.e., they did not use the same self-serving biases) than werenondepressed subjects. In a secondstudy, Sackeim and Wegnercontrasted depressed inpatients andoutpatients with schizophrenic inpa-tients and normal controls, and theyfound that the latter two groups used"self-serving biases" in their apprais-als of their behaviors and their out-comes while the depressed patientsdid not. The self-serving biases werecharacterized as follows: "If an out-come is positive, I controlled it, Ishould be praised, and the outcomewas very good. If an outcome is neg-ative, I did not control it (as much),I should not be blamed, and it wasnot so bad anyway" (Sackeim andWegner 1986, p. 559). The authorsgo on to say that the cognitive dis-tortions evident in the schizophrenicand normal groups represent a
"normal" pattern of functioning. Infact, an abundance of work withnonpsychiatric samples supports thisposition (see Taylor and Brown 1988for a review).
Interpreting the meaning of thesestudies in the context of the presentdiscussion is difficult because of theincompatibility of methods and limi-tations on the generalizability of theresults. Sackeim and Wegner (1986)assessed subjects' attributions for hy-pothetical situations and found nodifferences between normals andschizophrenic patients. These findingsare intriguing on many levels. Theysuggest that, in at least some areasof self-appraisal, schizophrenic pa-tients (or a subgroup of these pa-tients) function normally. That is,like most people, they use aself-serving bias in evaluating theirbehaviors and their outcomes.
Taken a step further, these find-ings also have implications for theo-ries about the etiology of unaware-ness of illness in schizophrenia. In
by guest on June 24, 2015http://schizophreniabulletin.oxfordjournals.org/
Dow
nloaded from

120 SCHIZOPHRENIA BULLETIN
anticipation of our discussion of theneuropsychology of unawareness def-icits, it is important to make a dis-tinction that is made in neurologybetween dysfunctions that result insystem breakdown and those thatrelease a system so that its manifes-tations stand in greater relief. In thiscontext, the gross unawareness ofillness observed in schizophreniacould be explained as a result of thedisinhibition of normally adaptivecognitive biases rather than as a defi-cit state per se. Meanwhile, the moreaccurate self-appraisals identified indepressives can be understood as afailure of these cognitive biases toaffect their normal inhibitory effecton dysphoric mood. In other words,the self-awareness deficits evident inschizophrenia may result from over-use of normally adaptive cognitivebiases whereas depressives fail tomake use of such protective mecha-nisms. Indeed, Sackeim (1983) hasproposed that self-deception (or de-nial) is adaptive and essential to theregulation of euthymic mood states.Interestingly, a report on insight andmedication compliance from VanPutten et al. (1976) seems to supportthis view: they found a significantinverse relation between grandiosityand insight, leading them to hypoth-esize that drug refusers may prefer agrandiose psychotic state (i.e., anextreme, self-serving cognitive bias)to the more normal state induced bypsychotropic medicine.
From the literature reviewed thusfar, it remains unclear if unawarenessof illness is specific to schizophreniaamong psychiatric disorders or ifself-awareness deficits observed inother disorders is of a different type.This uncertainty is due to the lack ofcomparability between methods andthe dearth of work on unawarenessof illness as such in psychiatric disor-ders other than schizophrenia. Future
work could address these issues byusing a standardized assessment ofunawareness in large samples of psy-chiatric patients across diagnosticgroups. We are currently pursuingsuch a study.
The studies of poor insightreviewed above bear on the persist-ent problem of the validity of thediagnosis of schizophrenia. Some re-searchers have argued that signs andsymptoms may not be the best dif-ferentiating criteria for distinguishingschizophrenia from other disorders(Carpenter et al. 1976; Carpenter andKirkpatrick 1988; Meehl 1989).Given the burgeoning literature onputative genetic and the diagnosticmarkers such as smooth pursuit eye-tracking dysfunction, and given indi-cations that some of these markersmay have value as risk indicators,this strategy may indeed be useful.Unawareness of illness inschizophrenia may also prove valu-able in such an approach as an alter-native sign. The data from studiesreviewed in this section are consist-ent with a conceptualization of un-awareness of illness in schizophreniaas an expression of the disorder,much as are hallucinations or delu-sions. Indeed, as shall be discussed inthe section on etiology, some evi-dence exists that can be interpretedas supporting the idea that at leastsome forms of unawareness of illnessin schizophrenia may stem from thesubtle neurological deficits associatedwith the disorder.
Relation to Severity of Illness. Therelationship between unawareness ofillness and severity of psychopathol-ogy in schizophrenia remains un-clear. Some early studies examiningthis relationship have found thesedimensions to be both inversely cor-related (Small et al. 1965) and posi-
tively correlated (Whitman and Duf-fey 1961). More recent reportsindicate that they are independent ofeach other (Bartko et al. 1988;McEvoy et al. 1989c).
The finding by Small andcolleagues that insight improves withclinical status is based on a study of154 psychiatric patients from differ-ent diagnostic groups, includingschizophrenia (Small et al. 1965).Since the authors do not report in-sight scores by diagnosis, it is un-clear if insight improved as symp-toms remitted in the schizophrenicpatients studied.
Bartko et al. (1988) studied 58schizophrenic patients diagnosed ac-cording to Research Diagnostic Crite-ria (RDC; Spitzer et al. 1978), andrated them using the Brief PsychiatricRating Scale (BPRS; Overall andGorham 1962) and the Global As-sessment Scale (GAS; Endicott et al.1976). Patients were divided into twogroups: medication compliant (n =26) and noncompliant (n = 32). Thenoncompliant group evidenced signif-icantly more "lack of insight intoillness" (p < 0.05) and "lack of feel-ing of illness" (p < 0.01), as meas-ured by Zerssen's Clinical Self-RatingScale (Zerssen and Koeller 1976, ascited by Bartko et al. 1988), and wasmore grandiose (p < 0.05). How-ever, these two groups did not differon the GAS or on any BPRS itemsother than grandiosity.
McEvoy and associates (1989b)assessed the relations between insightand psychopathology in 52 acutelypsychotic schizophrenic patients diag-nosed according to DSM-III (Amer-ican Psychiatric Association 1980)criteria. Patients were assessed withthe BPRS and the Insight and Treat-ment Attitudes Questionnaire (ITAQ)developed by McEvoy et al. (1989b).While patients displayed significant
by guest on June 24, 2015http://schizophreniabulletin.oxfordjournals.org/
Dow
nloaded from

VOL 17, NO. 1, 1991 121
improvement in symptomatologyduring the hospitalization (mean ini-tial BPRS score, 42.9 ± 8.1; lastBPRS score, 33.3 ± 9.6), the level ofinsight remained stable, leading theauthors to conclude that the mecha-nisms responsible for insight andpositive symptoms of schizophreniaare independent.
In a subsequent article, McEvoy etal. (1989a) found that while degreeof psychopathology diminished dur-ing hospitalization for both volun-tary and involuntary patients, onlythe voluntary patients' insight ratingsimproved over the course of hospi-talization. This finding is of particu-lar importance to the distinction be-tween poor insight and delusionalbeliefs. Increased insight into thefalseness of delusional beliefs is anindicator of improvement in the se-verity of delusions. The dissociationbetween insight and improvement insymptoms of psychosis overall inMcEvoy et al.'s data suggests thatimprovement in insight cannot beexplained by treatment of delusionsalone.
In summary, the lack of compara-bility between studies in their defini-tions and methods of measuring in-sight and psychopathology probablyaccounts for conflicting results in theliterature. The methodologicallymore sophisticated studies reviewedindicate that insight and severity ofsymptoms of psychosis are independ-ent. Further standardization of meas-ures of insight, psychopathology,and patient samples will determinethe generalizability of these results.
Relations to Outcome and Compli-ance. One would expect that patientswith schizophrenia who believe theyare ill and can benefit from treat-ment would likely be more compliantwith treatment and have better out-
come. Although some studies havefailed to find any relationship be-tween insight and outcome (Eskey1958; Wing et al. 1964; Van Puttenet al. 1976), the majority of studiesindicate that higher levels of aware-ness of having an illness and of ben-efiting from treatment augur well forpositive clinical outcome and compli-ance with treatment (Lin et al. 1979;McGlashan and Carpenter 1981;Heinrichs et al. 1985; Bartko et al.1988; McEvoy et al. 1989£>). Lin andcolleagues (1979) examined 100 read-mitted patients meeting 5 of Carpen-ter and colleagues' (1974) 12 differen-tial symptoms of schizophrenia.Insight was judged to be present ifpatients responded positively to anyone of the following threequestions: "Do you think you needto be in the hospital?" "Do youthink you had to see a psychiatrist?""Do you think you had to see adoctor?" Perceived benefit of medica-tion was judged to be present if pa-tients stated that the medication hadsome positive effect. Lin et al. (1979)found that those patients who hadinsight, those who perceived benefitsfrom medication, and, most impor-tant, those who perceived a relationbetween the two were more likely tocomply with medication, as deter-mined by self-report and corrobora-tion by the outpatient therapist. Ofthe 69 patients without insight, only12 adhered to their regimen, whereas14 of 31 (45%) insightful patientsadhered to theirs. Compliance wasbest for those patients who under-stood that medication was treating amental illness.
Bartko et al. (1988) contrasted agroup of 32 RDC-diagnosed schizo-phrenic patients who were medica-tion noncompliant to a compliantgroup (n = 26) and found that non-compliant patients had significantly
poorer insight (for two measures ofinsight, both p's < 0.05).
McEvoy and colleagues (1989b)examined the longitudinal relation-ship between insight as measured bythe ITAQ and medication compli-ance in a group of 52 hospitalizedDSM-///-diagnosed schizophrenicpatients. These patients were admit-ted during acute exacerbations re-lated to medication noncompliance.Compliance was assessed on admis-sion to the study, at day 14, and atdischarge from the hospital. Ratingswere made on a 4-point scale, withactive compliance (1) at one end andovert refusal (4) at the other. Theauthors found a moderate inversecorrelation between insight and com-pliance with medication regimen atinitial assessment (r = - 0.35, p =0.006) and at day 14 (r = -0.36,p = 0.005). That is, patients withhigher insight ratings were morecompliant than those with lower in-sight ratings. Although this relationdid not hold up at the final assess-ment (r = 0.16, p = 0.12), the au-thors suggest that this was probablydue to the reduced range of scoresproduced by the high rate of compli-ance evident in the sample at dis-charge. They conclude that, overall,insight predicted better compliance intheir sample. However, having ob-served good compliance in some pa-tients who did not believe they wereill or needed medication, the authorssuggest that socialization of patientsto expected behaviors may also ac-count for cooperation with medica-tion regimens. They add that com-pliance itself is not a good measureof insight, particularly for hospital-ized patients.
Some investigators have examinedthe relations between poor insightand various measures of outcomeand psychosocial functioning. Forexample, Heinrichs et al. (1985)
by guest on June 24, 2015http://schizophreniabulletin.oxfordjournals.org/
Dow
nloaded from

122 SCHIZOPHRENIA BULLETIN
found that relapse rates were signifi-cantly higher in noninsightful pa-tients. Subjects were 39 outpatients,of whom 33 were diagnosed asschizophrenic and 6 as schizoaffec-tive by RDC. The treating clinician'sprogress note on the day the clini-cian judged that a relapse had begunwas extracted, and a judgment wasmade as to whether the patient dis-played insight. Of the 24 patientsjudged to have had "early" insight,only 2 required rehospitalization af-ter discharge, in contrast to 7 of the14 patients without insight (p =0.006, Fischer's exact t test). The au-thors do not indicate at what pointin time relapse was assessed, so wecannot tell from their results if morepatients from the insightful groupswould have required hospitalizationlater on. Heinrichs et al. conclude,however, that early insight is an im-portant patient attribute predictive ofcourse.
McGlashan and Carpenter (1981)found that insight correlated posi-tively with frequency of social con-tacts and that poor insight correlatednegatively with quality of usefulwork. Similarly, in a longitudinalstudy of 32 schizophrenic patients,Soskis and Bowers (1969) found thatfrom 3 to 7 years after the index epi-sode, patients who ignored or deniedillness evidenced poorer psychosocialfunctioning (e.g., less employment,poorer socialization, greater numberof hospitalizations) than patientswho had insight.
Some studies have not found in-sight to be related to length of hospi-talization, compliance, and posthos-pitalization functioning. Eskey (1958)reviewed the MSEs of 300 psychoticpatients and classified each patientinto one of three groups: those withmarked insight, those with partialinsight, and those with no insight.The three groups did not differ in
length of hospitalization. Van Puttenet al. (1976) found that insight, asdefined in the IPSS, was not signifi-cantly related to medication compli-ance. Wing et al. (1964) followed asample of 128 male schizophrenicpatients (by hospital diagnosis) for 1year after discharge from the hospitaland assessed attitudes about illnessbefore hospital discharge. Specifi-cally, they asked patients if theythought they were ill, whether thedelusions and hallucinations they hadwere a sign of illness, and whetherthe patients viewed other similarlyaffected individuals as ill. None ofthese attitudes was found to be re-lated to several measures of posthos-pital psychosocial functioning.
To summarize, the investigationsreviewed used widely differingmeasures of insight, compliance, andoutcome, which makes comparisonsbetween studies difficult. Nonethe-less, the bulk of the evidencereviewed supports the general notionthat displaying an awareness of ill-ness in schizophrenia is associatedwith better medication complianceand clinical outcome. Of the studiesfinding no such relations, severalmethodological flaws in diagnosticand assessment procedures may ac-count for the nonsignificant results.For example, these studies did notuse well-specified patient groups(e.g., "hospital diagnosis of schizo-phrenia," "psychotic patients"),which suggests that other nonschizo-phrenic patients may have been in-cluded in the samples. If the self-awareness deficits described areschizophrenia-specific, the inclusionof other diagnoses will mask the re-lations to variables such as outcome.Future work in this area is needed todetermine if particular dimensions ofinsight are related to measures ofoutcome and compliance.
Etiology
Neuropsychology of Unawareness ofIllness. Unawareness of illness inneurological disorders (i.e.,anosognosia), first described by Ba-binski (1914), bears a striking resem-blance to poor insight in schizo-phrenia. Babinski described the ano-sognostic patient as displaying a lackof knowledge, awareness, or recogni-tion of disease. This has most fre-quently been observed in patientssuffering from hemiplegia and hemia-nopia following stroke. Gerstmannoffers the following description:
The hemiplegia is usually on theleft side of the body. The patientbehaves as though he knew noth-ing about his hemiplegia, asthough it had not existed, asthough his paralysed limbs werenormal, and insists that he canmove them and walk as well as hedid before. (Gerstmann 1942,pp. 891-892]
As in schizophrenia, unawareness ofillness in neurological disorders islargely intractable to direct confron-tation. For example, when such apatient is shown the affected limb,he or she will be indifferent to it(Gerstmann 1942). In other instances,the patient will reveal delusionalideas (insisting, e.g., that the limb issomeone else's), presumably to ex-plain the dissociation between his orher experience of self and his or herperceptions. To our knowledge, therehave been no studies of the neuro-logical substrates of unawareness ofillness in schizophrenia, althoughthere has been a plethora of suchwork in neurological disorders. Thiswork will be discussed briefly below,as we believe it provides a usefulmodel for schizophrenia.
As with unawareness of illness inschizophrenia, anosognosia has beenunderstood in various ways. It is
by guest on June 24, 2015http://schizophreniabulletin.oxfordjournals.org/
Dow
nloaded from

VOL 17, NO. 1, 1991 123
most often distinguished from moti-vated denial (psychological defense)in that anosognosia is thought tostem from a neuropsychological defi-cit that leaves a patient unable tobecome aware of the signs of theirillness (McGlynn and Schacter 1989).Various terms have been used besidesanosognosia, including "lack ofinsight," "imperception of disease,""denial of illness," and "organic re-pression." McGlynn and Schacter(1989) provide an extensive review ofthis literature and discuss the theoret-ical implications of the variousterms. Regardless of the etiology,one thing is certain: anosognosia inneurological disorders arises directlyfollowing injury to the brain. On theother hand, denial of illness has beenobserved in physical disorders suchas cardiac disease and cancer, butwith widely varying reports of itsfrequency (Strauss et al. 1990).
In neurological disorders, neuro-anatomically based theories of ano-sognosia can be broadly divided intothose that attribute this deficit to fo-cal brain lesions and those that at-tribute it to diffuse brain damage(McGlynn and Schacter 1989). Re-searchers subscribing to the focal le-sion viewpoint generally attributeanosognosia to right hemisphere le-sions of the parietal area and its con-nections (Von Hagen and Ives 1939;Gerstmann 1942; Critchley 1953;Warrington 1962; Geschwind 1965;Stuss and Benson 1986). Althoughthere are some reports of anosogno-sia following left hemisphere insult,these are less convincing due tomethodological problems (e.g., hemi-spheric dominance was not ascer-tained), and the bulk of evidence isfrom right hemisphere lesions (Stussand Benson 1986; McGlynn andSchacter 1989). The findings impli-cating right hemisphere involvementin self-awareness deficits have led to
several theories suggesting that ano-sognosia may stem from the isolationof cortical speech areas (Geschwind1965), a disconnection from aware-ness of body scheme or image repre-sentation (Schilder 1935; Gerstmann1942), or a neurologically based af-fective disturbance (Bear 1982).
The frontal lobes have also beenimplicated in anosognosia. Stuss andBenson (1986) review a wide rangeof unawareness deficits, and theysuggest that these deficits have incommon an inability to beself-monitoring or to self-correct andthat self-awareness demands intactprefrontal function. They note thesimilarities between different formsof anosognosia—Capgras syndrome,reduplicative paramnesia, and con-fabulations frequently seen in Korsa-koff syndrome. Specifically, Stussand Benson suggest that these deficitsinvolve a disorder of self-awarenessand the ability to be self-corrective,resulting in a general deficiency inreality testing. They suggest that al-though frontal structural damage hasnot been demonstrated in most re-ported disorders of awareness, anargument can be made that a func-tional disturbance exists. They cite alarge body of literature implicatingprefrontal function as necessary forthe capacity of self-awareness.
Stuss and Benson offer a generalmodel for the neurological underpin-nings of the wide range of self-awareness disorders they review:
Inattention (most often unilateral)apparently occurs with pathologyinvolving a number of anatomicalsites, one being the frontal eyefield area. If there is a neural cir-cuit underlying attention as sug-gested, the frontal cortex . . . ap-pears to be important. Greaterdegrees of unawareness, such asunconcern, anosognosia, reduplica-tion, confabulation, etc., probably
demand simultaneous malfunctionof several cerebral areas with dif-ferent degrees and combinationsproducing different syndromes.The specific behavioral abnormal-ity . . . may be dependent on aspecific combination of brain ab-normalities. [Stuss and Benson1986, p. 120]
As shall be discussed shortly, thisview has important implications forthe self-awareness deficits observedin schizophrenia.
Anosognosia has also been ob-served in patients who have had dif-fuse brain damage, usually followinga stroke (Sandifer 1946; Ullman1962; Cole et al. 1968). In these pa-tients, self-awareness deficits aremost often understood as stemmingfrom an overall decline in cognitivefunction. This seems unlikely, how-ever, since anosognosia has been ob-served in patients without generalintellectual impairment (Babinski1914; Gerstmann 1942; Cutting 1978)and in patients with unawareness ofspecific dysfunctions coinciding withintact awareness of other decifits(Von Hagen and Ives 1939). If ano-sognosia stemmed from general intel-lectual impairments, we would ex-pect awareness deficits for multiplerather than for specific defects.
Of interest is the finding of do-main specificity for anosognosia(e.g., Von Hagen and Ives 1939; Bisi-ach et al. 1986). For example, a casedescribed by Von Hagen and Ives(1939) involved a 76-year-old patientwho denied paralysis of the left legand yet was aware of the paralysisof the left upper limb and of severememory impairment. Such observa-tions have led some investigators topostulate that these deficits involve"modality-specific disorders ofthought" that arise from a dysfunc-tion of a modular central processingsystem rather than of a single higher
by guest on June 24, 2015http://schizophreniabulletin.oxfordjournals.org/
Dow
nloaded from

124 SCHIZOPHRENIA BULLETIN
order system responsible forself-awareness. Schacter (in press)disagrees with this view and offers adescriptive model for unawarenessphenomena referred to as dissociableinteractions and conscious experience(DICE). This model involves a cen-tralized conscious awareness system(CAS), which interacts with modularsystems concerned with language,memory, perception, etc. In orderfor unawareness to occur in a partic-ular domain, the input to the CASfrom the relevant module wouldneed to drop to a sufficiently lowlevel of activation that it becomesfunctionally disconnected fromawareness.
The literature on unawareness oftardive dyskinesia in schizophreniasuggests that self-awareness deficitsin schizophrenia may also be domainspecific. Rosen and his associates(1982) found that of 70 schizophrenicpatients with tardive dyskinesia, 47(67%) were unaware of the deficitsproduced by the movement disorder.Similarly, Caracci et al. (1990) foundthat 15 of 20 (75%) schizophrenicpatients with tardive dyskinesia wereunaware of their movement disorder.Interestingly, verbal and visual feed-back resulted in a short-term increasein awareness; however, this was notsustained for longer than 2 weeks.Moreover, when the relation betweenawareness of tardive dyskinesia and"awareness of psychiatric disorder"was examined, Caracci et al.observed that 13 patients were un-aware of psychiatric disorder, indi-cating that although the two meas-ures strongly correlated, there wasnot complete overlap.
If the self-awareness deficits ob-served in schizophrenia areneuropsychologically based and canvary for different signs and symp-toms (e.g., hallucinations, tardivedyskinesia, flat affect, etc.) and for
other consequences of the disorder,the models proposed by Stuss andBenson (1986) and McGlynn andSchacter (1989) may have relevanceto schizophrenia.
From the literature reviewed, cer-tain parallels between unawarenessphenomena described in neurologicaldisorders and schizophrenia can bedrawn. Phenomenologically, self-awareness deficits in their extreme,as described in these two literatures,share common features that distin-guish both from the less severedisturbances that result from psycho-logical defense mechanisms. Theo-etically, neuroanatomically basedmodels have been outlined in ano-sognosia, which may have relevanceto schizophrenia. For example, thereare numerous reports of the presenceof neurological soft signs and neu-ropsychological deficits in schizo-phrenic patients (e.g., Kolakowska etal. 1985; Heinrichs and Buchanan1988). A model developed to explainthe familial data on schizophreniaand eye-tracking dysfunction is di-rectly applicable to these findings.Matthysse et al. (1986) propose thatschizophrenia and eye-tracking dys-function are independent expressionsof an underlying "latent" trait, somenervous system disease process thataffects different regions and systemsof the brain independently. Thismodel is consistent with the explana-tions for anosognosia offered byStuss and Benson (1986) andMcGlynn and Schacter (1989). Thatis, schizophrenia in all its variedforms may result from deficits inmultiple brain regions leading to dis-orders of thought, perception, atten-tion, affect, eye movement, and/orself-awareness.
The etiology of unawareness phe-nomena in schizophrenia is poorlyunderstood. An argument has been
made that at least some forms ofself-awareness deficits may stemfrom neuropsychological dysfunc-tion. Future work in this area couldaddress this issue more directly byassessing the relations between self-awareness deficits in schizophreniaand measures of abnormal brainstructure (e.g., magnetic resonanceimaging) and function.
Denial of Illness: Psychological Cop-ing Mechanism or Defense. Histori-cally, self-awareness deficits inschizophrenia have most often beenunderstood as stemming from psy-chological defenses or adaptive cop-ing strategies (Mayer-Gross 1920;Searles 1965; Semrad 1966; Levy etal. 1975; McGlashan and Carpenter1976; Van Putten et al. 1976; Lally1989). Several investigators have sug-gested that schizophrenic patientshave distinct recovery styles follow-ing psychotic episodes (Sacks et al.1974; McGlashan et al. 1975; Mc-Glashan and Carpenter 1981; Strausset al. 1987; Thurm and Haefner1987; Greenfeld et al. 1989). We willreview literature representative ofthis view below.
Based on case history material,Mayer-Gross (1920) classified the de-fensive strategies of schizophrenicpatients into four categories: denialof the future, creation of a new lifeafter the illness, denial of the psy-chotic experience, and melting of thepsychotic experience into a new setof life experiences. These four cate-gories were thought to compose acontinuum of defenses that serve tohelp the patients adapt to their ab-normal experiences. In two of thesesteps, different types of self-awareness deficits were observed. Inthe "denial of the future" category,patients were observed to deny thepossibility of positive future events
by guest on June 24, 2015http://schizophreniabulletin.oxfordjournals.org/
Dow
nloaded from

VOL 17, NO. 1, 1991 125
(i.e., they displayed "despair") evenwhen such events were of high likeli-hood. Meanwhile, in the "denial ofthe psychotic experience" category,patients were typically unaware ofthe signs and symptoms of the ill-ness. This latter stage is of direct rel-evance to the present discussion,whereas the former combines un-awareness phenomena (e.g., denial ofrelevant data for making predictionsabout the future) with attributionalprocesses. Essentially, Mayer-Grossidentified various domains for whichschizophrenic patients displayedawareness deficits and interpretedthis finding as evidence for distinctcategories of psychological defense.In addition, he proposed that thedegree of denial (i.e., defense)changes over the course of recovery.This view has its origins in psycho-analytic theory. As shall be seen, theresults of several other studies havebeen interpreted similarly.
In their review of the literature onpostpsychotic depression (PPD), Mc-Glashan and Carpenter (1976) iden-tify its relation to denial in schizo-phrenia. They cite several authorswho have identified PPD as markinga stage of recovery from psychosisthat either follows a more "prim-itive" defensive state characterized bydenial (Semrad 1966; Kayton 1973,as cited in McGlashan and Carpenter1976) or precedes the reinstatementof psychotic denial (Donlon andBlacker 1973). Despite their differ-ences, the authors who McGlashanand Carpenter review all share theview that PPD arises from a lessen-ing of defensive denial, which resultsin the patients becoming aware ofthe tragic circumstances of their ill-ness. McGlashan and Carpenter re-port that the results of numerousstudies (mostly case histories) havebeen interpreted by most authors assupporting the psychoanalytic con-
ception of PPD in schizophrenia. Inshort, this view can be described asfollows: "Patients who try to inte-grate information from their psycho-sis (rather than use extensive denial)may be more prone to react depres-sively to new insight" (McGlashanand Carpenter 1976, p. 235 [empha-sis added]). Implicit in this view ofPPD is the concept that denial inschizophrenia serves a defensivefunction.
In other work, McGlashan and hisassociates (1975) have suggested thatthere exists a continuum of recoverystyles: on one end lies "integration,"and on the other, "sealing over."Fourteen neuroleptic-withdrawn,"generally nonpsychotic" schizo-hrenic patients diagnosed accordingto DSM-II (American PsychiatricAssociation 1968) criteria were inter-viewed 12 months following an acutepsychotic episode. Patient responsesduring a taped, structured interviewwere reliably categorized (kappa =0.46, z = 4.3, p < 0.001) into eitherthe integration or sealing-over cate-gories. The raters used the followingcriteria for making this distinction:
(1) Some patients prefer not tothink about their psychotic experi-ence during recovery and adopt anattitude of "the less said thebetter." They would be referred toas sealing over patients. (2) Somepatients manifest an interest intheir psychotic experiences duringrecovery and are willing to discusstheir experiences in an effort tolearn more about themselves.These patients would be consid-ered integrators. [McGlashan et al.1975, p. 1270].
Responses from each group wereevaluated and led the authors to con-clude that integrators displayed anawareness of the continuity of theirpersonality before, during, and after
their psychotic episode. They "tookresponsibility" for their psychoticsymptoms and were flexible in theirthoughts about them. Meanwhile,patients who sealed over tended toisolate their psychotic experience.That is, they resisted thinking aboutthe experience and, when confrontedwith it by others, were unaware of(or "encapsulated") aspects of it. Inaddition, they viewed the psychosisas alien, caused by some force out-side themselves.
In the study just reviewed, Mc-Glashan et al. (1975) describe vary-ing patterns of retrospective aware-ness, flexibility of beliefs, andattributional style, and interpretthese as representing distinct styles ofrecovery from psychosis. They sug-gest that, at one end of a continuum,patients cope with schizophrenia byactively keeping from awarenessfacts about their illness, while at theother extreme, patients are aware ofthese facts and are active in expand-ing this knowledge. The differencesin awareness they describe are forpast events (i.e., retrospective aware-ness) and are interpreted as reflectingcoping strategies applicable to otherstressful life events besides havingschizophrenia.
The results from several otherstudies of patients' attitudes abouttheir illness (Eskey 1958; Soskis andBowers 1969; Levy et al. 1975; Co-hen and Berk 1985; Wciorka 1988;Greenfeld et al. 1989) have been in-terpreted similarly—that is, thatvarying levels of insight stem fromeither psychological defense mecha-nisms per se or from coping strate-gies. The frequent finding that poorinsight is positively correlated withelated mood and grandiosity (VanPutten et al. 1976; Roback andAbramowitz 1979; Heinrichs et al.1985; Bartko et al. 1988) has alsobeen interpreted as evidence that
by guest on June 24, 2015http://schizophreniabulletin.oxfordjournals.org/
Dow
nloaded from

126 SCHIZOPHRENIA BULLETIN
poor insight serves a defensive func-tion.
To say whether unawareness ofillness in schizophrenia reflects a psy-chological defense mechanism, onemust test the question directly. Ofrelevance to this issue is the work byGur and Sackeim (1979) onself-deception. Hilgard (1949) claimedthat all defense mechanisms share themechanism of self-deception. Gurand Sackeim offer operationalizedcriteria for ascribing self-deception:"(1) The individual holds two contra-dictory beliefs. (2) These two contra-dictory beliefs are held simultaneous-ly. (3) The individual is not aware ofholding one of the beliefs. (4) Theact that determines which belief isand which belief is not subject toawareness is a motivated act"(p. 149). Citing an extensive litera-ture indicating that people with nega-tive attitudes about themselves findself-confrontation aversive, Gur andSackeim identified a group of suchindividuals using personality ques-tionnaires, and they presented thesesubjects with their own taped voice(self-confrontation) and the voices ofothers. Subjects were asked to decidewhether the voice they werepresented with was their own orsomeone else's. Gur and Sackeimwere interested in answering thequestion of whether avoidance ofself-confrontation (i.e., misidentify-ing the self as others, a false nega-tive) and unmindful self-confron-tation (i.e., misidentifying others asself, a false positive) were instancesof self-deception as defined by theircriteria. To demonstrate that subjectsheld two contradictory beliefs simul-taneously (criterion 2), they neededto employ other indices of knowl-edge besides the subjects' response tothe question. To accomplish this,they measured electrodermalresponses (EDRs) to the presentations
and reaction times (RTs) for thevoice identifications. Interestingly,they found that both EDR reactivityand RT latency were significantlyhigher when subjects were presentedwith their own voice than when sub-jects were presented with the voicesof others. The authors interpretedthis pattern of results in subjects whomade errors (i.e., false negatives andfalse positives) as an indication thatthese subjects had knowledge as tothe true source of the voices butwere apparently unaware of this, asindicated by their choices (criterion3). Moreover, these errors were be-lieved to be motivated. To addressthe issue of motivation (criterion 4),Gur and Sackeim performed a sec-ond experiment wherein they intro-duced two pretest manipulations de-signed either to increase or to lowerself-esteem. As they expected, sub-jects who underwent the pretreat-ment to lower self-esteem made moreerrors in identifying their own voice(i.e., they avoided self-confronta-tion), while those in the conditiondesigned to increase self-esteem mademany more true and false-positiveresponses (i.e., they sought out self-confrontation). The authors suggestthat since such errors should nor-mally occur by chance, the patternof results indicates that motivationalfactors influenced self-deception.
The studies discussed earlier in thissection all share the presumption thatpoor insight (or unawareness of ill-ness) in schizophrenia is an impor-tant psychological coping or defensemechanism. However, these studiesdid not directly test the question ofwhether poor insight is a defensivestrategy. Instead, they describe un-awareness of current psychosis, ret-rospective unawareness for past epi-sodes, rigidly held beliefs about lackof illness, and external attributionsfor events associated with schizo-
phrenia, and they interpret these asstemming from psychological defenseor coping strategies. Up to this time,experimental paradigms such as thatreported by Gur and Sackeim (1979)have not been used in the study ofunawareness of illness in schizo-phrenia. The use of such procedurescould shed light on the question ofwhether such phenomena areinstances of self-deception for thepurposes of psychological defense.
Insight Is a Multidimensional Con-struct. From the literature reviewedthus far, certain distinctions can bemade regarding the different compo-nents of insight in schizophrenia. Inour view, the concept of insight intoillness appears to consist of at leastfour distinct dimensions: (1) aware-ness of the signs, symptoms, andconsequences of illness; (2) generalattributions about illness and specificattributions about symptoms andtheir consequences; (3) self-conceptformation; and (4) psychological de-fensiveness. We believe that thesefour dimensions are identifiable inmost published investigations of in-sight.
Other distinctions have been madethat may be more accurately reclassi-fied by our scheme. Based on astudy involving 21 psychoticpatients, Greenfeld et al. (1989) de-fine five components of insight inpsychotic disorders. They label thesecomponents "symptomatology," "ex-istence of illness," "etiology," "vul-nerability to relapse," and "the valueof treatment." Citing patientresponses, the authors suggest thatinsight is a multidimensional con-struct with independent components.That is, patients appear to have dif-ferent levels of insight into distinctlydifferent and largely independent ar-eas related to their illness.
by guest on June 24, 2015http://schizophreniabulletin.oxfordjournals.org/
Dow
nloaded from

VOL 17, NO. 1, 1991 127
Wciorka (1988) proposes a typol-ogy of "attitudes" schizophrenic pa-tients have about their illness. Hesuggests that insight may have sev-eral dimensions and features bywhich several different subtypes ofpatients can be classified. A sampleof 100 ICD-9-diagnosed schizo-phrenic patients in relative symptomremission underwent an extensiveclinical interview. Patients were en-couraged to talk about their subjec-tive definitions of their illness, andtheir responses were taped. Based onthese tapes and on suggestions fromthe literature, Wciorka identified six"features of attitudes toward illness."For each, Wciorka created a 5-pointrating scale (from total nonendorse-ment of the idea (I) to full endorse-ment (5]). The six features ratedwere patients' (1) sense of their ill-ness belonging to them, (2) sense ofinfluence over their illness, (3) senseof the location of cause of their ill-ness, (4) evaluation of their illness,(5) readiness to discuss the facts oftheir illness, and (6) effort to developa concept of their illness. These fea-tures were then aggregated into threedimension scales based on positivecorrelations between items: (1) iden-tification of the illness with them-selves, (2) evaluation of their illness,and (3) willingness to be reflectiveabout their illness. The dimensionswere interpreted as reflecting cogni-tive, evaluative, and reactive compo-nents of attitude toward illness.
In our terms, we would describethese same dimensions as reflecting(1) general attributions about illnessand self-concepts, (2) specific attribu-tions regarding symptoms, and (3)defensiveness. The value of using theclassifications we have proposed isthat the categories reflect more dis-tinct processes that have been studiedextensively in different contexts. Forexample, the literature contains re-
ports of many investigations of attri-butional styles in psychiatric patientsthat are not directly aimed at theissue of insight in schizophrenia andyet are relevant. Empirical studies ofself-concept and the related personal-ity construct of self-esteem abound(Winters and Neale 1985; Link 1987),as do investigations of psychologicaldefense mechanisms. Finally, the cog-nitive psychology literature on spe-cific self-awareness deficits is broad,spanning many disorders and patientgroups. Using the categories we haveproposed will make comparisons be-tween studies easier and will make itpossible to specify the unique contri-bution each of these processes makesto what is commonly labeled "poorinsight" in schizophrenia.
Attempts at Improving PoorInsight
The psychiatric literature largely failsto examine directly the relationshipbetween specific interventions andchanges in insight. The question ofwhether poor insight can beimproved remains unresolved. Be-low, we will briefly review studies inwhich improvement in insight,broadly defined, is examined in rela-tion to efforts to improve complianceand outcome. Since, to our knowl-edge, very little work has been re-ported on this issue in schizophrenia,we will begin by briefly discussingattempts to treat problems of self-awareness reported in the neurologi-cal literature, as we believe thisserves as a useful model.
McGlynn and Schacter (1989), in acomprehensive review of unaware-ness of neuropsychological symp-toms, note that there is a virtual ab-sence of literature on "awarenesstraining" in neurological disorders inwhich anosognosia is a prominent
feature. They state that in severeforms of anosognosia, even repeatedattempts to demonstrate deficits tothe patient are ineffective, and thatother currently employed trainingattempts may be inadequate. CitingGlisky and Schacter's (1987) worktraining brain-damaged patients withmemory impairments, they suggestthat extremes of repetition are neces-sary. Importantly, they note that alltoo often, psychogenic and neurogen-ic contributions to poor awarenessare not distinguished, and that theserequire different therapies. Alongwith making distinctions betweendifferent types of unawareness, dis-tinguishing between anosognosia sec-ondary to different kinds of braindamage is also important in planninginterventions. Prigatano and Fordyce(1986), in a large-scale rehabilitationprogram in which cognitive retrain-ing is used to address awareness defi-cits, found that "self-appraisal" isoften compromised after headtrauma, but when the basis is frontallobe disfunction (with resultant inat-tentiveness, concrete thinking, andmisinterpretation of higher levels ofinformation), patients can be signifi-cantly helped to improveself-perception. In contrast, in pa-tients who present with temporallobe and deep-brain structural abnor-malities, such therapies are ineffec-tive. The implications of such workfor schizophrenia, in which bothfrontal and temporal lobe lesions arepostulated, may be valuable in guid-ing classification according to levelof insight and in studying interven-tions across patient groups.
The research on attempts to ame-liorate awareness deficits in schizo-phrenia is less direct than the reportsjust discussed. Partially successfulattempts to modify delusional beliefs(Watts et al. 1973; Milton et al.1978) and at patient education (Lin
by guest on June 24, 2015http://schizophreniabulletin.oxfordjournals.org/
Dow
nloaded from

128 SCHIZOPHRENIA BULLETIN
et al. 1979; Brown et al. 1987) offerindirect evidence that some forms ofknowledge about their illness can bemodified in patients withschizophrenia. For example, Seltzerand colleagues (1980), in a studywith significant shortcomings (50%patient dropout rate and mixed diag-nostic samplings), lectured 67 inpa-tients about the "nature of their dis-order" and its pharmacologicalmanagement. These patients and agroup of matched controls weretested on a 14-point scale to assessmedication knowledge. Medicationcompliance in-hospital and at5-month outpatient followup wasassessed by urine levels and pillcount. An outpatient noncompliancerate of 9 percent (2 of 23) in the "ed-ucated" sample was significantly dif-ferent from the 67 percent (6 of 9) ofthose in the control group. Becausepretreatment level of knowledge (orawareness) was not assessed and sev-eral patient groups were included inthe sample, it is not possible fromthe data presented to draw conclu-sions about the impact of educationon unawareness of illness in schizo-phrenia.
From a psychoanalytic perspective,some researchers (e.g., Searles 1965)have suggested that unawareness ofillness (i.e., psychotic denial) can bemodified through psychotherapy.However, to our knowledge, empiri-cal studies of this position in schizo-phrenia do not exist.
From the studies discussed above,it is evident that an important lacunaexists in the empirical literature re-garding interventions with awarenessdeficits in schizophrenia. Here again,the neuropsychological literature onimproving awareness of deficits inpatients with anosognosia serves as auseful model for psychiatric researchin schizophrenia. Since it appearsthat schizophrenic patients with poor
insight do more poorly on severalmeasures of outcome and compliancethan do those patients with good in-sight, improving awareness of illnessin this disorder should be among theprimary goals of any good clinicalstrategy.
Summary
From the literature reviewed, wehave suggested that at least someforms of unawareness of illness inschizophrenia may stem directlyfrom the pathophysiology of the dis-order. Given this, the study of thesephenomena offers important oppor-tunities for improving the meaning-fulness of diagnoses, understandingthe neuropsychology, and enhancingthe treatment of schizophrenia.Nonetheless, a comprehensive exami-nation of the meaning, treatment,etiology, and pathophysiology ofunawareness of illness in schizo-phrenia has been difficult due to con-ceptual ambiguities. For this reason,we propose the following terminol-ogy and guidelines in the interest ofincreasing comparability betweenstudies: (1) for "unawareness of defi-cit," patients should communicate alack of knowledge about a specificdeficit when confronted with it bythe examiner; and (2) for "incorrectattributions about illness," patientsshould communicate the belief thateither specific deficits or conse-quences of illness are unrelated tohaving a mental disorder. Both crite-ria are necessary for ascribing "un-awareness of illness." In other words,to display unawareness of illness,patients should communicate bothunawareness of deficits and incorrectattributions simultaneously. Forsymptoms that are generally assessedon the basis of subjective report
(e.g., hallucinations), the concept ofunawareness of deficit cannot easilyapply. In these instances, unaware-ness of illness relates only to attribu-tional deficits.
The question of the etiology ofunawareness of illness remains unan-swered although much indirect evi-dence is available. Unawareness ofillness appears stable over time insome samples of patients and is notjust associated with acute exacerba-tions of psychosis. Given the obser-vations of poor insight in studies be-fore the advent of neuroleptics, infirst-break schizophrenic patients,and in patients who have been neu-roleptic withdrawn, it is unlikely thatpoor insight is due to treatment withneuroleptics. Also, from the studiesreviewed we can say that unaware-ness of illness in schizophrenia occursindependent of specific cultural ef-fects or gender differences.
Future studies could directly an-swer the question of whetherunawareness of illness in schizo-phrenia is trait related by examininga sample of patients longitudinally,both on and off neuroleptics. Thespecificity to schizophrenia couldalso be determined by direct compar-isons with other psychiatric disordersand psychotic controls. To test thehypothesis that some forms of un-awareness are neurologically based,future investigations could contrastpatients with and without awarenessof illness on measures of brain func-tion and structure. Alternatively, in-stances of unawareness of illnessstemming from psychological defensemechanisms could be more convinc-ingly identified by employing thecriteria for self-deception and associ-ated experimental paradigms pro-posed by Gur and Sackeim (1979). Inconclusion, future work on unaware-ness of illness in schizophrenia willneed to address its multidimensional
by guest on June 24, 2015http://schizophreniabulletin.oxfordjournals.org/
Dow
nloaded from

VOL. 17, NO. 1, 1991 129
nature and use more reliable andvalid measures to better answer thequestions raised in this review.
The reappraisal of unawareness ofillnesss may be particularly impor-tant to current efforts to expand andredefine the diagnosis of schizo-phrenia. Relative to DSM-II1 andDSM-IU-R (American PsychiatricAssociation 1987), broader defini-tions of schizophrenia have been pro-posed for DSM-IV, for example,briefer duration criteria and moreemphasis on negative symptoms (An-dreasen 1990). Unawareness of illnessappears to be as prevalent in schizo-phrenia as are many of theDSM-IU-R and proposed DSM-IVcriterion symptoms. In conjunctionwith the DSM-IV field trial,unawareness of illness will beassessed in a large geographicallydiverse sample of patients with psy-chotic and negative symptoms. Thisstudy will shed light on the relationof awareness deficits to other symp-toms, subtypes, and course variables.With other data emerging as to thespecificity, trait stability, and neuro-biological basis of unawareness ofillness, perhaps there will be furthersupport for the suggestion that un-awareness of illness is an importantcore symptom of the syndrome andan indispensable means of subtypingpatients with schizophrenia.
References
Alloy, L.B., and Abramson, L.Y.Judgment of contingency indepressed and nondepressed students:Sadder but wiser? Journal of Experi-mental Psychology, 108:441-485,1979.
American Psychiatric Association.DSM-II: Diagnostic and StatisticalManual of Mental Disorders. 2nd ed.
Washington, DC: The Association,1968.
American Psychiatric Association.DSM-III: Diagnostic and StatisticalManual of Mental Disorders. 3rd ed.Washington, DC: The Association,1980.
American Psychiatric Association.DSM-IU-R: Diagnostic and Statisti-cal Manual of Mental Disorders. 3rded., revised. Washington, DC: TheAssociation, 1987.
Andreasen, N.C. Negative symptomsin schizophrenia: Definition and reli-ability. Archives of General Psychia-try, 39:784-788, 1982.
Andreasen, N.C. Schizophrenia.DSM-IV Update. Washington, DC:American Psychiatric Press, 1990.
Babinski, M.J. Contribution a l'etudedes troubles mentaux dans l'hemiple-gieorganique cerebale (Agnosognosie).Revue Neurologique, 12:845-888,1914.
Bartko, G.; Herczog, I.; and Zador,G. Clinical symptomatology anddrug compliance in schizophrenicpatients. Acta Psychiatrica Scandina-vica, 77:74-76, 1988.
Bear, D.M. Hemispheric specializa-tion and neurology of emotion. Ar-chives of Neurology, 40:195-202,1982.
Beck, A.T. Depression: Clinical, Ex-perimental and Theoretical Aspects.New York: Hoeber Medical Divi-sion, Harper & Row, 1967.
Bertschinger, H. Processes of recov-ery in schizophrenics. PsychoanalysisReview. 3:176-188, 1916.
Bisiach, C; Valler, G.; Periani, D.;Papogano, C ; and Berti, J.Unawareness of disease followinglesions of the right hemisphere: Ano-sognosia for hemiplegia and ano-
sognosia for hemianopia. Neuropsy-chologia, 24:471-482, 1986.
Black, D.W.; Yates, W.R.; and An-dreasen, N.C. Schizophrenia,schizophreniform disorder, and delu-sional (paranoid) disorders. In: Tal-bott, J.A.; Hales, R.E.; andYudofsky, S.C., eds. Textbook ofPsychiatry. Washington, DC: Amer-ican Psychiatric Press, 1988. pp.357-402.
Brown, C.S.; Wright, R.G.; andChristensen, D.B. Association be-tween type of medication instructionand patient's knowledge, side effects,and compliance. Hospital and Com-munity Psychiatry, 38:55-60, 1987.
Caracci, G.; Muhkerjee, S.; Roth,S.; and Decina, P. Subjective aware-ness of abnormal involuntary move-ments in chronic schizophrenic pa-tients. American Journal ofPsychiatry, 147:295-298, 1990.
Carpenter, W.T., Jr.; Bartko, J.J.;Carpenter, C.L.; and Strauss, J.S.Another view of schizophreniasubtypes. Archives of General Psy-chiatry, 33:508-516, 1976.
Carpenter, W.T., Jr., and Kirkpa-trick, B. The heterogeneity of thelong-term course of schizophrenia.Schizophrenia Bulletin, 14:645-651,1988.Carpenter, W.T., Jr.; Strauss, J.S.;and Bartko, J.J. Flexible system forthe diagnosis of schizophrenia. Re-port from the World Health Organi-zation International Pilot Study ofSchizophrenia. Science, 182:1275-1278, 1973.
Carpenter, W.T., Jr.; Strauss, J.S.;and Bartko, J.J., The diagnosis andunderstanding of schizophrenia. PartI. Use of signs and symptoms for theidentification of schizophrenic pa-tients. Schizophrenia Bulletin, (Exper-imental issue No. 11), 1:37-49, 1974.
by guest on June 24, 2015http://schizophreniabulletin.oxfordjournals.org/
Dow
nloaded from

130 SCHIZOPHRENIA BULLETIN
Chapman, L.J., and Chapman, J.P.Disordered Thought in Schizo-phrenia. New York: Appleton-Century-Crofts, 1973.
Cohen, C.I., and Berk, L.A. Per-sonal coping styles of schizophrenicoutpatients. Hospital and Commu-nity Psychiatry, 36:407-410, 1985.
Cole, M.; Saexinger, H.G.; andHard, A. Anosognosia: Studies usingregional intravenous anesthesia. Neu-ropsychologia, 6:365-371, 1968.
Critchley, M. The Parietal Lobes.New York: Hafner Publishing Cor-poration, 1953.
Cutting, J. Study of anosognosia.Journal of Neurology, Neurosurgeryand Psychiatry, 41:548-555, 1978.
David, A.S. On insight and psycho-sis: Discussion paper. Journal of theRoyal Society of Medicine,83:325-329, 1990.
Donlon, P.T., and Blacker, K.H.Stages of schizophrenic decompensa-tion and reintegration. Journal ofNervous and Mental Disease,157:200-209, 1973.
Endicott, J.; Spitzer, R.L.; Fleiss,J.L.; and Cohen, J. The Global As-sessment Scale: A procedure formeasuring overall severity of psychi-atric disturbance. Archives of Gen-eral Psychiatry, 33:766-771, 1976.
Eskey, A. Insight and prognosis.Journal of Clinical Psychology,14:426-429, 1958.
Gerstmann, J. Problem of impercep-tion of disease and of impaired bodyterritories with organic lesions. Rela-tion to body scheme and its disor-ders. Archives of Neurology andPsychiatry, 48:890-913, 1942.
Geschwind, N. Disconnection syn-dromes in animals and man. Brain,88:237-294, 585-644, 1965.
Glisky, E.L., and Schacter, D.L. Ac-quisition of domain-specific knowl-edge in organic amnesia: Trainingfor computer related work.Neuropsychologia, 25:893-906, 1987.
Greenfeld, D.; Strauss, J.S.; Bowers,M.B.; and Mandelkern, M. Insightand interpretation of illness in recov-ery from psychosis. SchizophreniaBulletin, 15:245-252, 1989.
Gur, R.C., and Sackeim, H.A. Self-deception: A concept in search of aphenomenon. Personality and SocialPsychology, 37:142-169, 1979.
Heinrichs, D.W., and Buchanan,R.W. Significance and meaning ofneurological signs in schizophrenia.American Journal of Psychiatry,145:11-18, 1988.Heinrichs, D.W.; Cohen, B.P.; andCarpenter, W.T., Jr. Early insightand the management of schizo-phrenic decompensation. Journal ofNervous and Mental Disease,173:133-138, 1985.
Hilgard, E.R. Human motives andthe concept of the self. AmericanPsychologist, 4:374-382, 1949.
Kayton, L. Good outcome in youngadult schizophrenia. Archives ofGeneral Psychiatry, 29:103-110,1973.
Kolakowska, K.; Williams, A.O.;and Ardern, M. Schizophrenia withgood and poor outcome: III. Neuro-logical "soft" signs, cognitive impair-ment, and their clinical significance.British Journal of Psychiatry,146:348-357, 1985.
Lally, S.J. "Does being in here meanthere is something wrong with me?"Schizophrenia Bulletin, 15:253-265,1989.
Levy, S.T.; McGlashan, T.H.; andCarpenter, W.T., Jr. Integration andsealing-over as recovery styles fromacute psychosis. Journal of Nervous
and Mental Disease, 161:307-312,1975.Lewinsohn, P.M.; Mischel, W.;Chaplain, W.; and Barton, R. Socialcompetence and depression: The roleof illusory self-perceptions. Journalof Abnormal Psychology,89:203-212, 1980.
Lin, I.F.; Spiga, R.; and Fortsch, W.Insight and adherence to medicationin chronic schizophrenics. Journal ofClinical Psychiatry, 40:430-432,1979.
Link, B.G. Understanding labelingeffects in the area of mental disor-ders: An assessment of the expecta-tions of rejection. American Socio-logical Review, 52:96-112, 1987.
MacKinnon, R.A., and Yudofsky,S.C. The Psychiatric Evaluation inClinical Practice. Philadelphia: J.B.Lippincott Company, 1986.Martin, A.R. The dynamics of in-sight. American Journal of Psycho-analysis, 12:24-38, 1952.
Matthysse, S.; Holzman, P.S.; andLange, K. The genetic transmissionof schizophrenia: Application ofMendelian latent structure analysis toeye tracking dysfunctions in schizo-phrenia and affective disorder. Jour-nal of Psychiatric Research,20:57-67, 1986.Mayer-Gross, W. Uber die stellung-nahme zur abgelaufenen akuten psy-chose. Zeitschrifte fur die GesmateNeurologie und Psychiatrie,60:160-212, 1920.
McEvoy, J.P.; Appelbaum, P.S.;Geller, J.L.; and Freter, S. Why mustsome schizophrenic patients be invol-untarily committed? The role of in-sight. Comprehensive Psychiatry,30:13-17, 1989a.
McEvoy, J.P.; Apperson, L.J.; Ap-pelbaum, P.S.; Ortlip, P.; Brecosky,J.; and Hammill, K. Insight in schizo-
by guest on June 24, 2015http://schizophreniabulletin.oxfordjournals.org/
Dow
nloaded from

VOL. 17, NO. 1, 1991 131
phrenia: Its relationship to acute psy-chopathology. Journal of Nervousand Mental Disease, 177:43-47,1989b.
McEvoy, J.P.; Freter, S.; Everett, G.;Geller, J.L.; Appelbaum, P.; Apper-son, L.J.; and Roth, L. Insight andthe clinical outcome of schizophren-ics. Journal of Nervous and MentalDisease, 177:48-51, 1989c.
McGlashan, T.H., and Carpenter,W.T., Jr. Postpsychotic depression inschizophrenia. Archives of GeneralPsychiatry, 33:231-239, 1976.
McGlashan, T.H., and Carpenter,W.T., Jr. Does attitude toward psy-chosis relate to outcome? AmericanJournal of Psychiatry, 138:797-801,1981.
McGlashan, T.H.; Levy, S.T.; andCarpenter, W.T., Jr. Integration andsealing over: Clinically distinct re-covery styles from schizophrenia.Archives of General Psychiatry,32:1269-1272, 1975.
McGlynn, S.M., and Schacter, D.L.Unawareness of deficits in neuropsy-chological syndromes. Journal ofClinical and Experimental Neuropsy-chology, 11:143-205, 1989.
Meehl, P.E. Schizotaxia revisited.Archives of General Psychiatry,45:935-944, 1989.
Milton, F.; Patwa, V.K.; andHafner, RJ. Confrontational vs. be-lief modification in persistently de-luded patients. British Journal ofMedical Psychology, 51:127-130,1978.
Overall, J.E., and Gorham, D.R. TheBrief Psychiatric Rating Scale. Psy-chological Reports, 10:799-812, 1962.
Prigatano, G.P., and Fordyce, D.J.The Neuropsychological Rehabilita-tion Program at Presbyterian Hospi-
tal, Oklahoma City. In: Prigatano,G.; Fordyce, D.J.; Zeiner, H.K.;Roueche, J.R.; Pepping, M.; andWood, B.C., eds. Neuropsycholo-gical Rehabilitation After Brain In-jury. Baltimore: Johns HopkinsPress, 1986. pp. 96-118.
Richfield, J. An analysis of the con-cept of insight. Psychoanalytic Quar-terly, 23:390-409, 1954.
Roback, H.B., and Abramowitz, S.I.Insight and hospital adjustment.Canadian Journal of Psychiatry,24:233-236, 1979.
Rosen, A.M.; Mukherjee, S.; Olarte,S.; Varia, V.; and Cardenas, C. Per-ception of tardive dyskinesia in out-patients receiving maintenance neuro-leptics. American Journal ofPsychiatry, 139:372-373, 1982.
Sackeim, H.A. Self-deception, de-pression, and self-esteem: The adapt-ive value of lying to oneself.In: Masling, ]., ed. Empirical Studiesof Psychoanalytic Theory. Hillsdale,NJ: Lawrence Erlbaum, 1983.pp. 101-157.
Sackeim, H.A., and Wegner, A.Z.Attributional patterns in depressionand euthymia. Archives of GeneralPsychiatry, 43:553-560, 1986.
Sacks, M.H.; Carpenter, W.T., Jr.;and Strauss, J.S. Recovery from de-lusions: Three phases documented bypatient's interpretation of researchprocedures. Archives of General Psy-chiatry, 30:117-120, 1974.
Sandifer, P.H. Anosognosia and dis-orders of body scheme. Brain,69:122-137, 1946.
Schacter, D.L. On the relation be-tween memory and consciousness.In: Roediger, H., and Craik, F., eds.Varieties of Memory and Conscious-
ness. Hillsdale, NJ: Lawrence Erl-baum, in press.
Schilder, P. The Image and Appear-ance of Human Body. London: Ke-gan Paul, Trench, Trubner & Co.,1935.
Searles, H.F. Collected Papers onSchizophrenia and Related Subjects.New York: New York InternationalUniversity Press, 1965.
Seltzer, A.; Roncari, I.; and Gar-finkel, P. Effect of patient educationon medication compliance. CanadianJournal of Psychiatry, 25:638-645,1980.
Semrad, E.V. Longterm therapy ofschizophrenia. In: Usdin, G., ed.Psychoneuroses and Schizophrenia.Philadelphia: J.B. Lippincott Co.,1966. pp. 155-173.
Small, I.F.; Small, J.G.; and Gonza-lez, R. The clinical correlates of atti-tudinal change during psychiatrictreatment. American Journal of Psy-chotherapy, 19:66-74, 1965.
Soskis, D.A., and Bowers, M.B. Theschizophrenic experience: A follow-up study of attitude and post hospi-tal adjustment. Journal of Nervousand Mental Disease, 149:443-449,1969.
Spitzer, R.L.; Endicott, J.; and Rob-ins, E. Research Diagnostic Criteria:Rationale and reliability. Archives ofGeneral Psychiatry, 35:773-782,1978.
Strauss, D.H.; Spitzer, R.L.; andMuskin, P.R. Maladaptive denial ofphysical illness: A proposal forDSM-IV. American Journal of Psy-chiatry, 147:1168-1172, 1990.
Strauss, J.S.; Harding, C M . ; Hafez,H.; and Lieberman, P. The role ofthe patient in recovery from psycho-sis. In: Strauss, J.S.; Boker, W.; andBrenner, H., eds. Psychosocial Treat-ment of Schizophrenia. Toronto:
by guest on June 24, 2015http://schizophreniabulletin.oxfordjournals.org/
Dow
nloaded from

132 SCHIZOPHRENIA BULLETIN
Hans Huber Publishers, 1987. pp.160-166.Stuss, D.T., and Benson, D.F. TheFrontal Lobes. New York: RavenPress, 1986.
Talbott, J.A.; Hales, R.E.; and Yu-dofsky, S.C. Textbook of Psychia-try. Washington, DC: AmericanPsychiatric Press, 1988.Taylor, E.T., and Brown, J.D. Illu-sion and well-being: A social psy-chological perspective on mentalhealth. Psychological Bulletin,103:193-210, 1988.
Thurm, I., and Haefner, H.Perceived vulnerability, relapse risk,and coping in schizophrenia. Euro-pean Archives of Psychiatry andNeurological Sciences, 237:46-53,1987.
Tolor, A., and Reznikoff, M. A newapproach to insight: A preliminaryreport. Journal of Nervous and Men-tal Disease, 130:286-296, 1960.Ullman, M. Behavioral Changes inPatients Following Strokes. Spring-field, IL: Charles C Thomas, 1962.
Van Putten, T.; Crumpton, E.; andYale, C. Drug refusal in schizo-phrenia and the wish to be crazy.Archives of General Psychiatry,33:1443-1446, 1976.
Von Hagen, K.O., and Ives, E.R.Two autopsied cases of anosognosia.Bulletin of the Los Angeles Neurolog-ical Society, 4:41-44, 1939.
Warrington, E.K. The completion ofvisual forms across hemianopic de-fects. Journal of Neurology, Neuro-surgery and Psychiatry, 25:208-217,1962.
Watts, F.N.; Powell, G.E.; and Aus-tin, S.V. The modification of abnor-mal beliefs. British Journal of Medi-cal Psychology, 46:359-363, 1973.
Wciorka, J. A clinical typology ofschizophrenic patients' attitudes to-wards their illness. Psychopathology,21:259-266, 1988.
Whitman, J.R., and Duffey, R.F. Therelationship between type of therapyreceived and a patient's perception ofhis illness. Journal of Nervous andMental Disease, 133:288-292, 1961.
Wilson, W.H.; Ban, T.A.; and Guy,W. Flexible system criteria in chronicschizophrenia. Comprehensive Psy-chiatry, 27:259-265, 1986.
Wing, J.K.; Cooper, J.E.; and Sarto-rius, N. The Description and Classifi-cation of Psychiatric Symptoms: AnInstruction Manual for PSE and Ca-tego System. London: CambridgeUniversity Press, 1974.
Wing, J.K.; Monck, E.; Brown,G.W.; and Carstairs, G.M. Morbid-ity in the community of schizo-phrenic patients discharged fromLondon mental hospitals in 1959.British Journal of Psychiatry,110:10-21, 1964.
Winters, K.C., and Neale, J.M. Ma-nia and low self esteem. Journal ofAbnormal Psychology, 94:282-290,1985.
World Health Organization. Reportof the International Pilot Study ofSchizophrenia. Geneva: The Organi-zation, 1973.World Health Organization. MentalDisorders: Glossary and Guide toTheir Classification in AccordanceWith the Ninth Revision of the Inter-national Classification of Disease.Geneva: The Organization, 1978.
Zerssen, D.V., and Koeller, D.M.Klinische Seblstbeurn lungsskalen ausdem Miinchner Psychiatrischen In-fomtionsystem. Manuale. Weinheim:Beltz, 1976.
Acknowledgments
This research was supported in partby a National Alliance for Researchin Schizophrenia and Affective Dis-orders Young Investigator Award(Amador) and by a Columbia Uni-versity Schizophrenia ResearchAward (Amador). The authors thankJean Endicott, Ph.D., Charles Kauf-man, M.D., and Dolores Malaspina,M.D., for their comments on earlierversions of this manuscript.
The Authors
Xavier F. Amador, Ph.D., isResearch and Diagnostic Coordina-tor, Schizophrenia Research Unit,New York State Psychiatric Institute,and Instructor in Clinical Psychol-ogy, College of Physicians and Sur-geons, Columbia University, NewYork, NY. David H. Strauss, M.D.,is Assistant Unit Chief, Schizo-phrenia Research Unit, New YorkState Psychiatric Institute, and In-structor in Psychiatry, College ofPhysicians and Surgeons, ColumbiaUniversity, New York, NY. Scott A.Yale, M.S.W., is Data Manager,Schizophrenia Research Unit, NewYork State Psychiatric Institute, andStaff Research Associate, Departmentof Psychiatry, College of Physiciansand Surgeons, Columbia University,New York, NY. Jack M. Gorman,M.D., is Director, Department ofClinical Psychobiology, and theSchizophrenia Research Unit, NewYork State Psychiatric Institute, andAssociate Professor of Psychiatry,College of Physicians and Surgeons,Columbia University, New York,NY.
by guest on June 24, 2015http://schizophreniabulletin.oxfordjournals.org/
Dow
nloaded from