Avoiding Diabetic Complications GPCME, Rotorua- 2015 North/1401 fri room 1 Khanolkar -...
48
Avoiding Diabetic Complications GPCME, Rotorua- 2015 Dr Manish Khanolkar, MD, MRCP, FRACP Consultant Physician & Diabetologist, ADHB Senior Lecturer in Medicine, University of Auckland Tutor, University of Leicester, Online Diploma Diabetes course (BMJ group)
-
Upload
nguyenkhuong -
Category
Documents
-
view
218 -
download
2
Transcript of Avoiding Diabetic Complications GPCME, Rotorua- 2015 North/1401 fri room 1 Khanolkar -...
Avoiding Diabetic ComplicationsGPCME, Rotorua- 2015
Dr Manish Khanolkar, MD, MRCP, FRACP
Consultant Physician & Diabetologist, ADHB
Senior Lecturer in Medicine, University of Auckland
Tutor, University of Leicester, Online Diploma Diabetes course (BMJ group)
What I will cover….
• The micro and macrovascular complications of diabetes
• Case scenarios
• Tips on what can be done to delay/ halt complications
• Some medication related issues
• Diabetic foot problems
• Briefly- hypoglycaemia
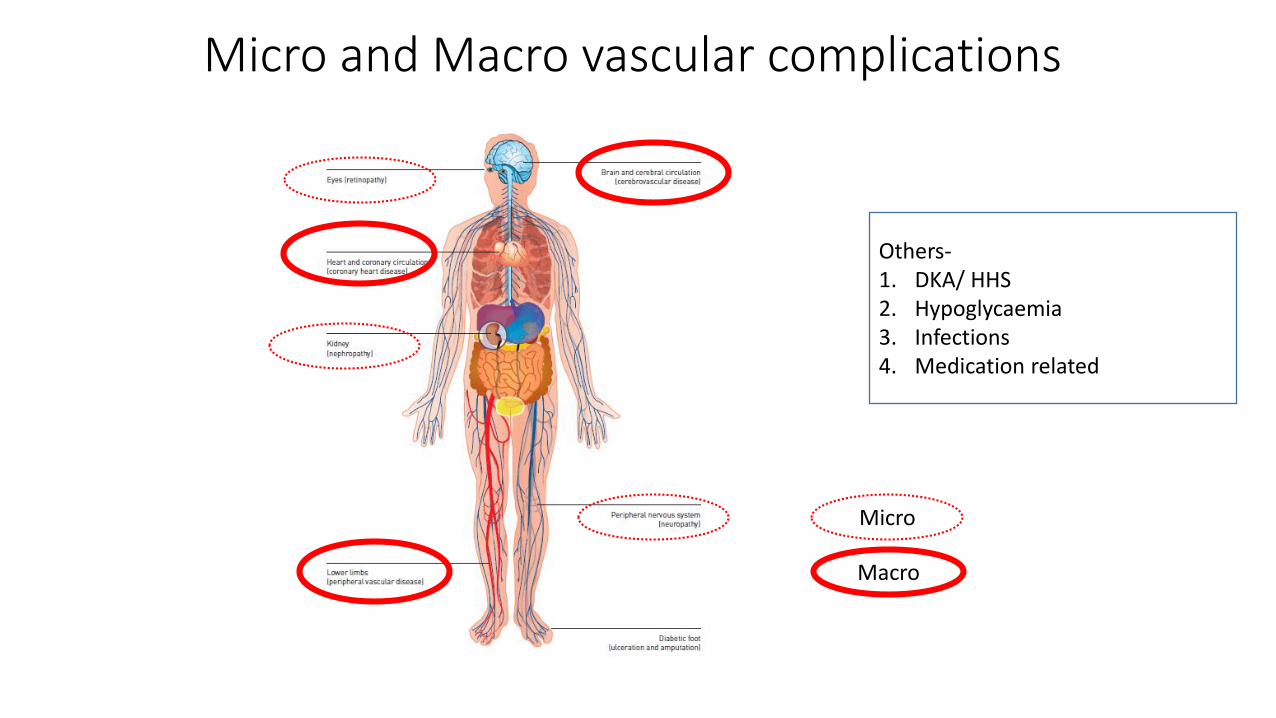
Micro and Macro vascular complications
Micro
Macro
Others-1. DKA/ HHS2. Hypoglycaemia3. Infections4. Medication related
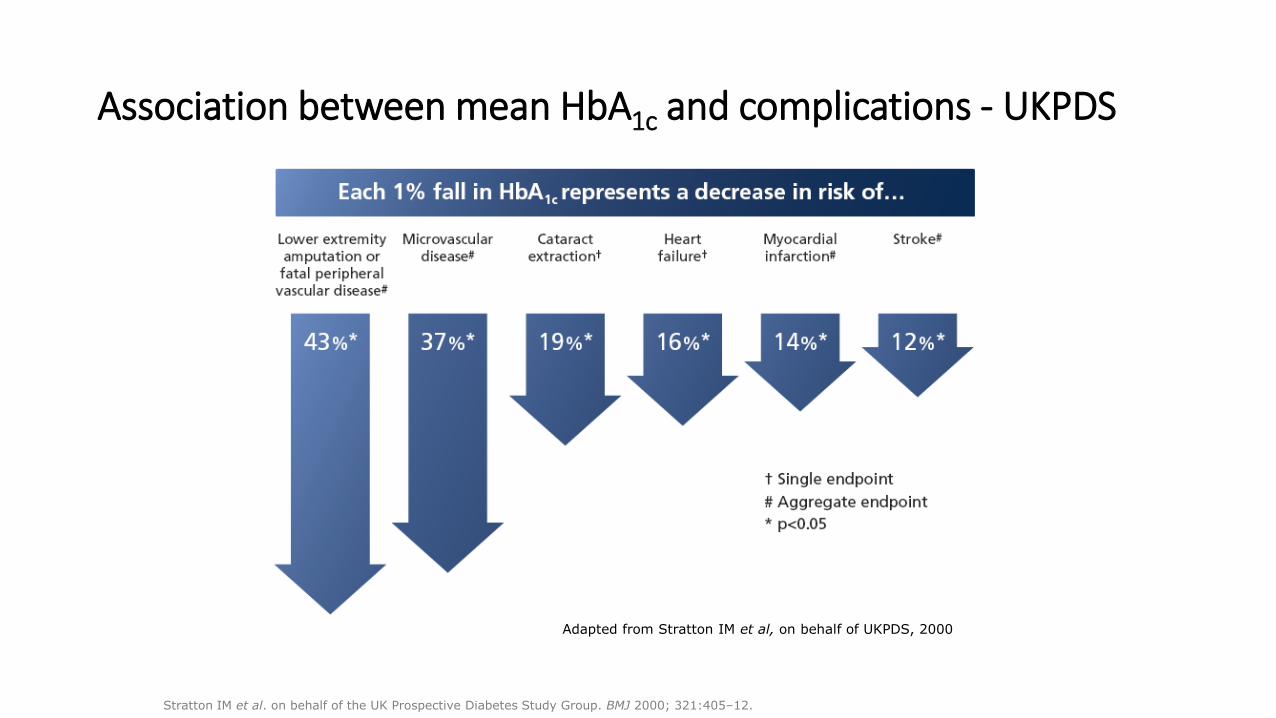
Association between mean HbA1c and complications - UKPDS
Adapted from Stratton IM et al, on behalf of UKPDS, 2000
Stratton IM et al. on behalf of the UK Prospective Diabetes Study Group. BMJ 2000; 321:405–12.
3 case scenarios…
Case C
50 years, male, T2d for last 5 years
Peripheral neuropathy
Similar BP/ lipids etc
Case B
50 years, male, T2d for last 5 years
Nephropathy
Similar BP/ lipids etc
Case A
50 years, male, T2d for last 5 years
Retinopathy
Similar BP/ lipids etc
1. Retinopathy
2. Peripheral neuropathy
3. Nephropathy
4. All contribute equally
Which diabetes complication correlates the most with cardiovascular risk?
Diabetic Nephropathy
• Irreversible
• Why treat?- slow/stop progression and also REDUCE CV RISK
• Low eGFR and proteinuria- both independent and powerful predictors of CVD/ mortality
• Refer all <75 years and eGFR<45 (stage 3b)/ many when eGFR <60
• Sudden big jump in creatinine or proteinuria always needs to be worked up soon
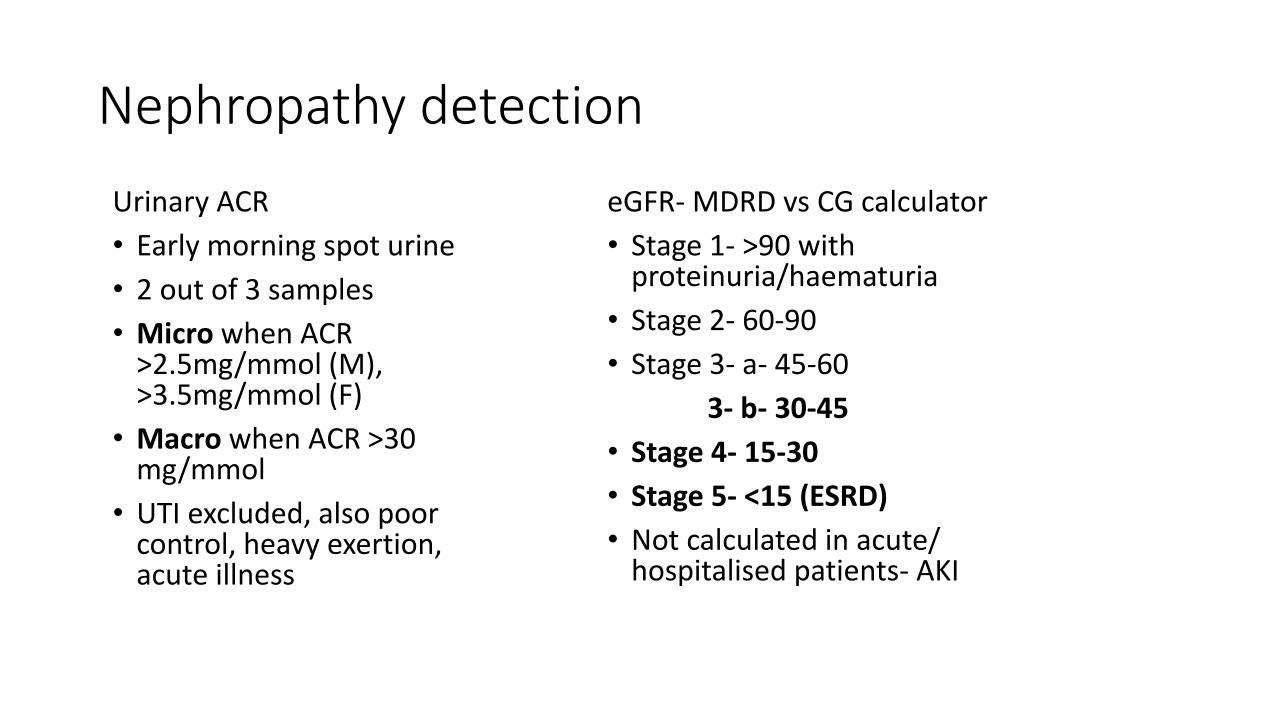
Nephropathy detection
Urinary ACR
• Early morning spot urine
• 2 out of 3 samples
• Micro when ACR >2.5mg/mmol (M), >3.5mg/mmol (F)
• Macro when ACR >30 mg/mmol
• UTI excluded, also poor control, heavy exertion, acute illness
eGFR- MDRD vs CG calculator
• Stage 1- >90 with proteinuria/haematuria
• Stage 2- 60-90
• Stage 3- a- 45-60
3- b- 30-45
• Stage 4- 15-30
• Stage 5- <15 (ESRD)
• Not calculated in acute/ hospitalised patients- AKI
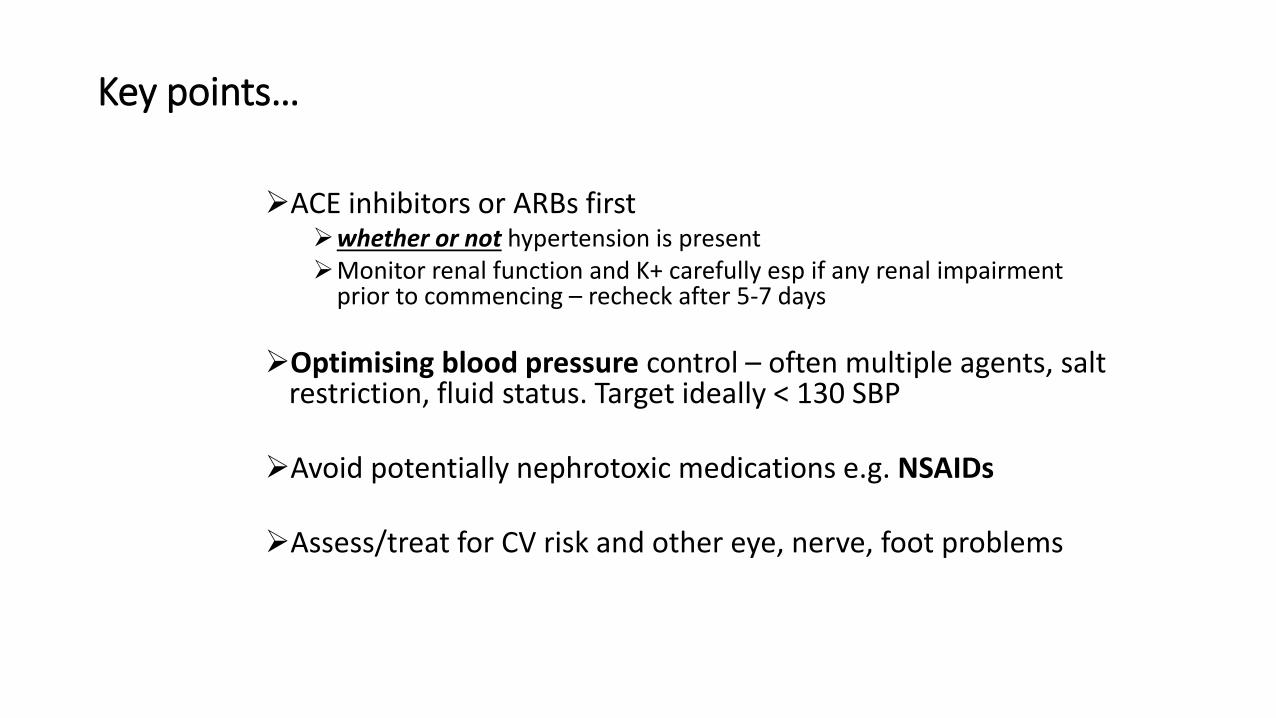
Key points…
ACE inhibitors or ARBs firstwhether or not hypertension is presentMonitor renal function and K+ carefully esp if any renal impairment
prior to commencing – recheck after 5-7 days
Optimising blood pressure control – often multiple agents, salt restriction, fluid status. Target ideally < 130 SBP
Avoid potentially nephrotoxic medications e.g. NSAIDs
Assess/treat for CV risk and other eye, nerve, foot problems
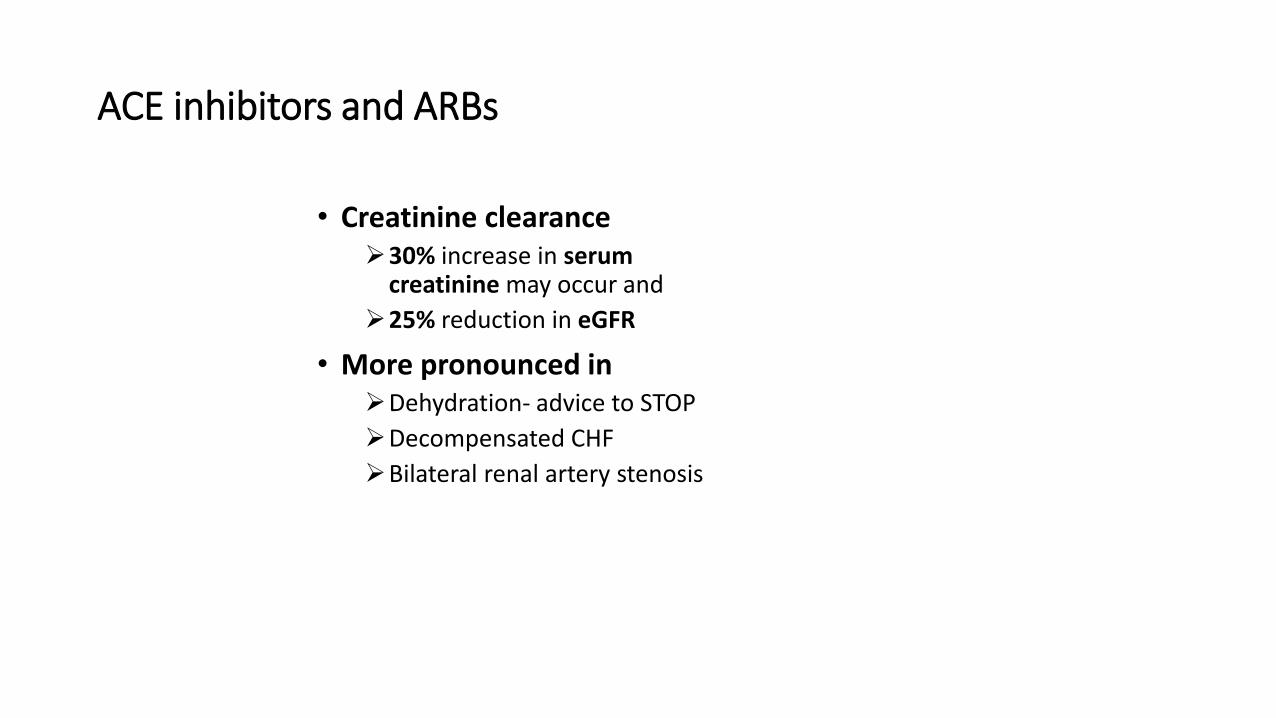
ACE inhibitors and ARBs
• Creatinine clearance30% increase in serum
creatinine may occur and
25% reduction in eGFR
• More pronounced inDehydration- advice to STOP
Decompensated CHF
Bilateral renal artery stenosis
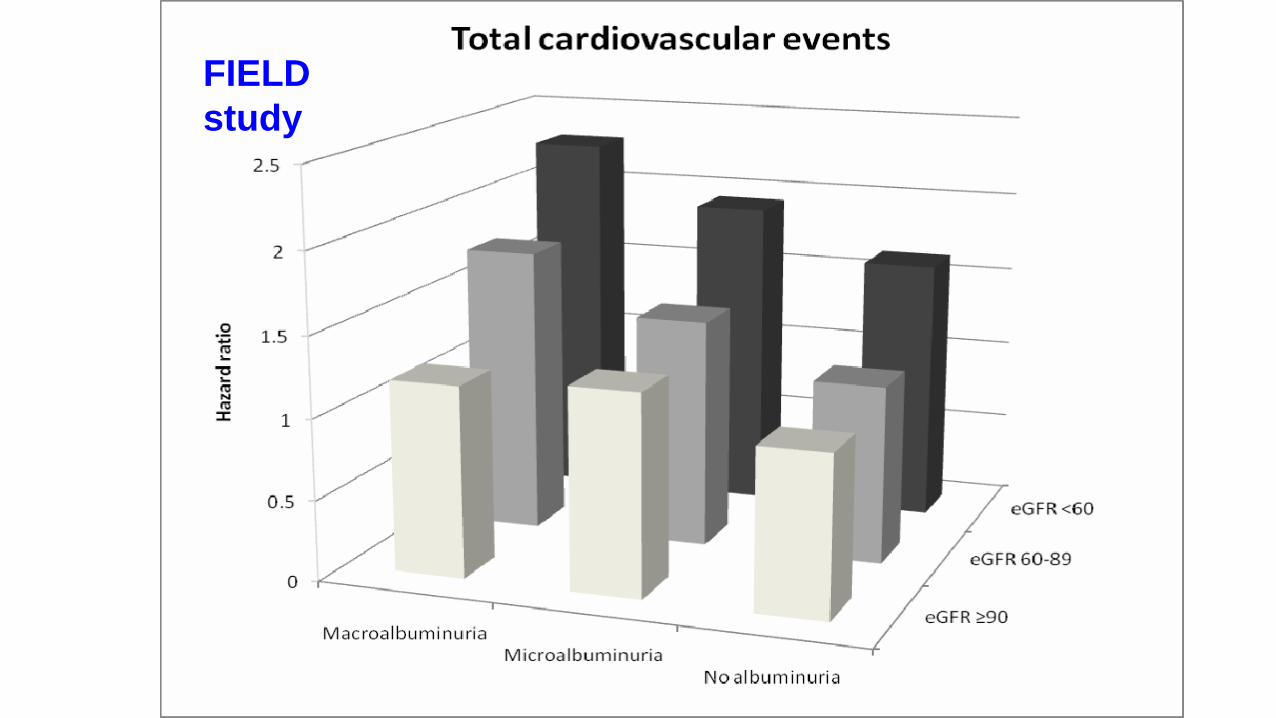
FIELD
study
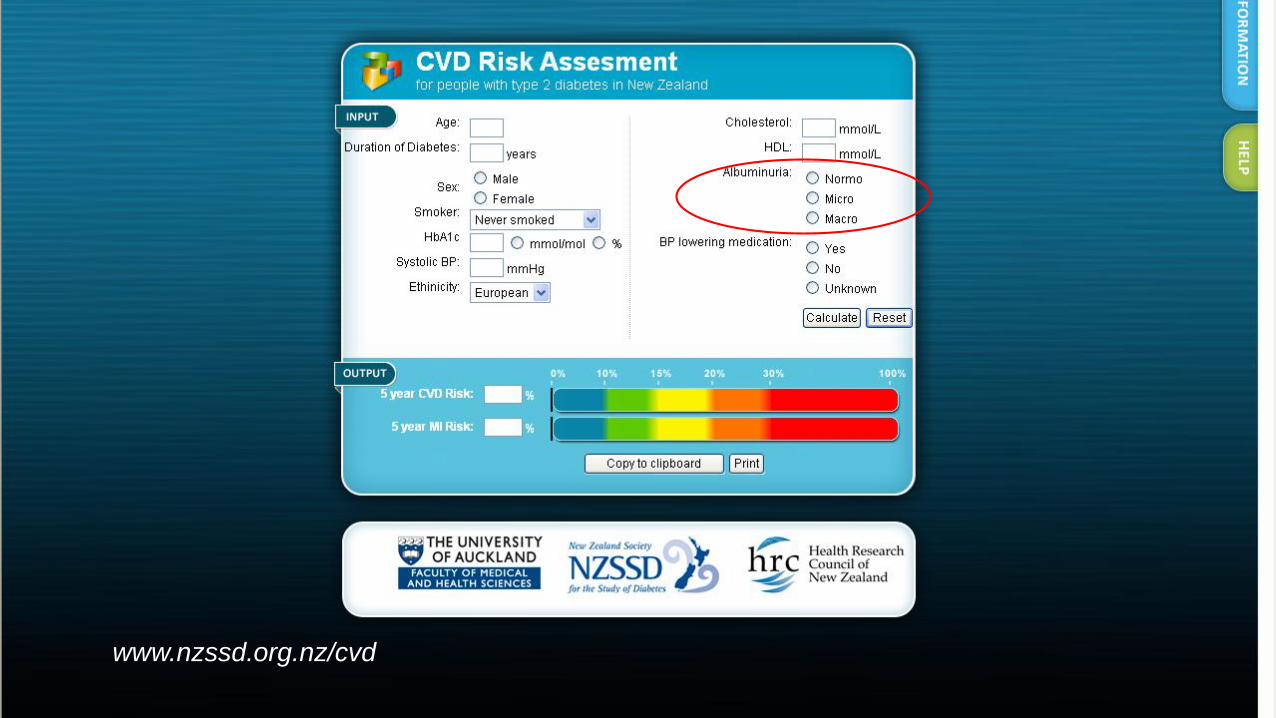
www.nzssd.org.nz/cvd
Case study….
49 yrs, Man, T2D for over 5 years
Longstanding poor glycaemia- HbA1c consistently >100 mmol/molfor over 2 years
On Protaphane insulin 30 units bd and metformin 1 g bd
Suddenly gets compliant with diet/ exercise/ insulins etc- HbA1c drops to 61 mmol/mol from 105 mmol/mol 2 months ago
But now feels more miserable- suddenly has developed severe tingling and pain in both feet
Diagnosis- insulin neuritis
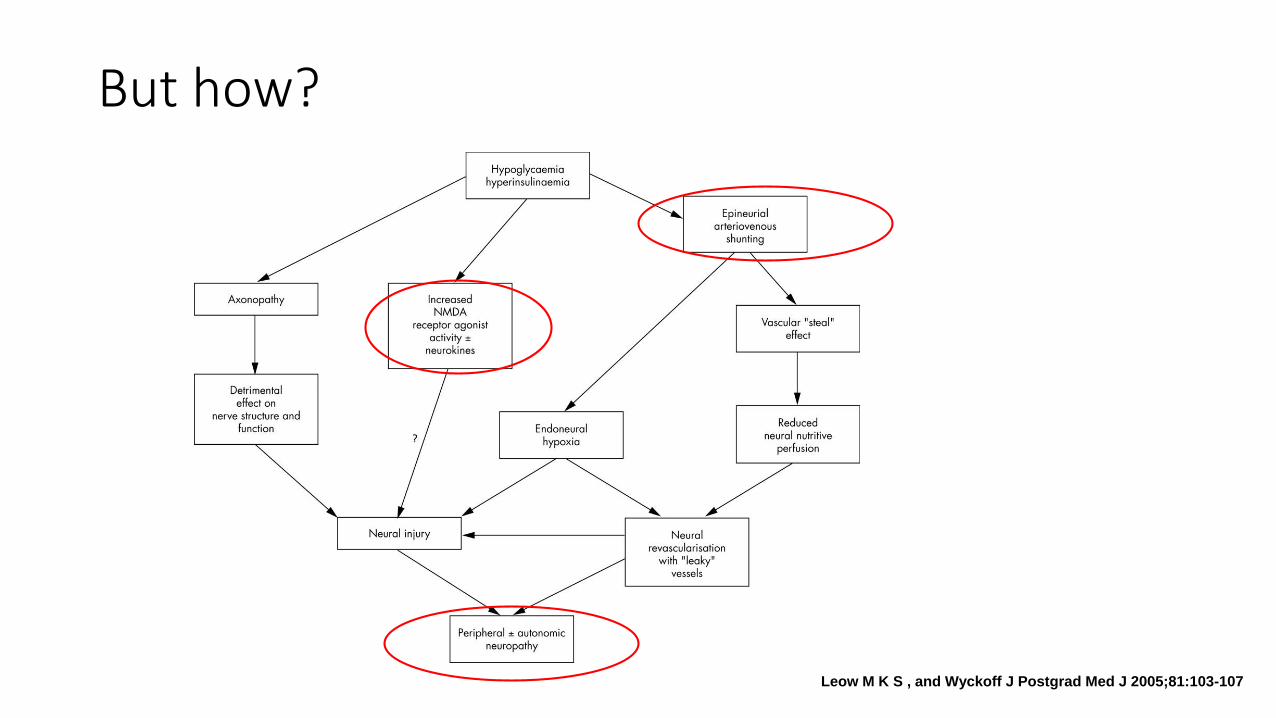
But how?
Leow M K S , and Wyckoff J Postgrad Med J 2005;81:103-107
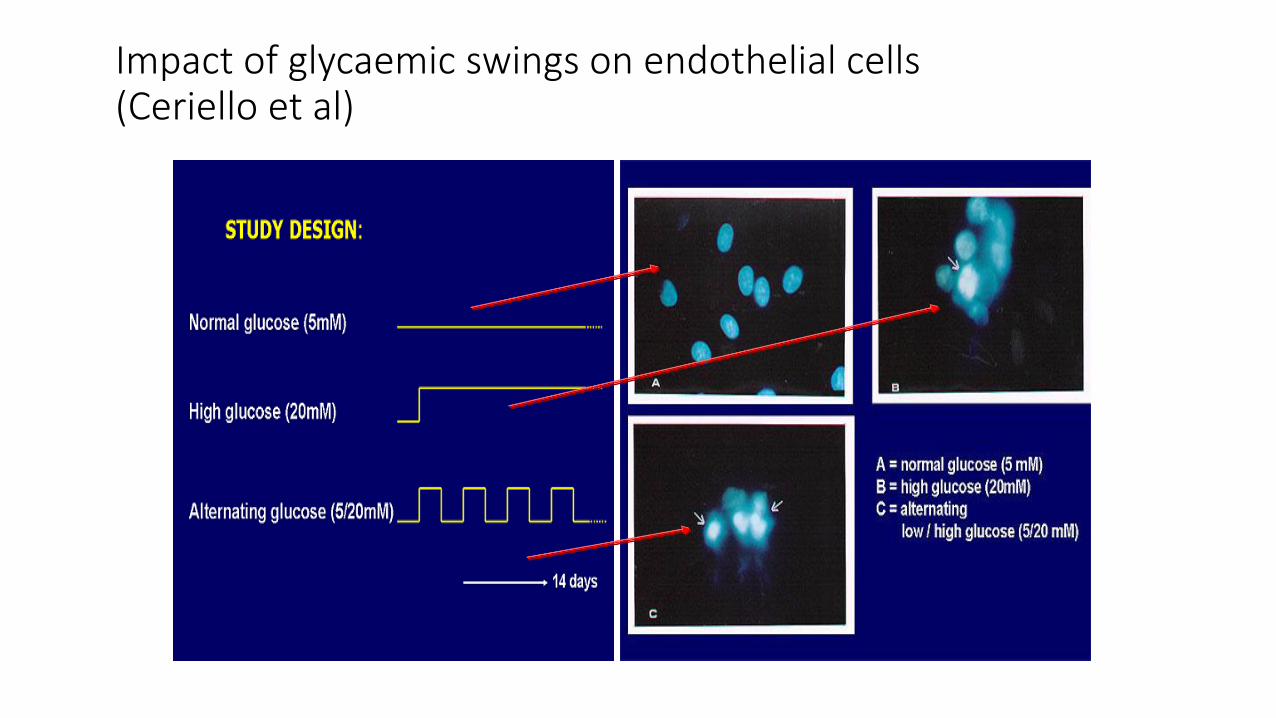
Impact of glycaemic swings on endothelial cells(Ceriello et al)
Management
• Aim for gradual glycaemic improvement
• Exclude other causes- ETOH, Vit B12 def- pernicious/ vegan/ on metformin
• Usually self limiting
• On occasions- tricyclics/ gabapentin/ opiates if significant pain
And remember….
• Similar situation may arise with retinopathy
• Classic scenario- Referred to eye clinic from retinal screening- the penny drops- glycaemia suddenly improves- retinopathy worsens!
• Retina screened regularly during pregnancy …..
AccordThe Action to Control Cardiovascular Risk in Diabetes Study Group
• N=10,000• 1/3 already on insulin/ 1/3 prevalent CVD events
• Age 62/ Diabetes for 10 years
• HbA1c 8.3
Strategy of (ultra) intensive glycaemic control aiming for HbA1c 6 (achieved 6.3)
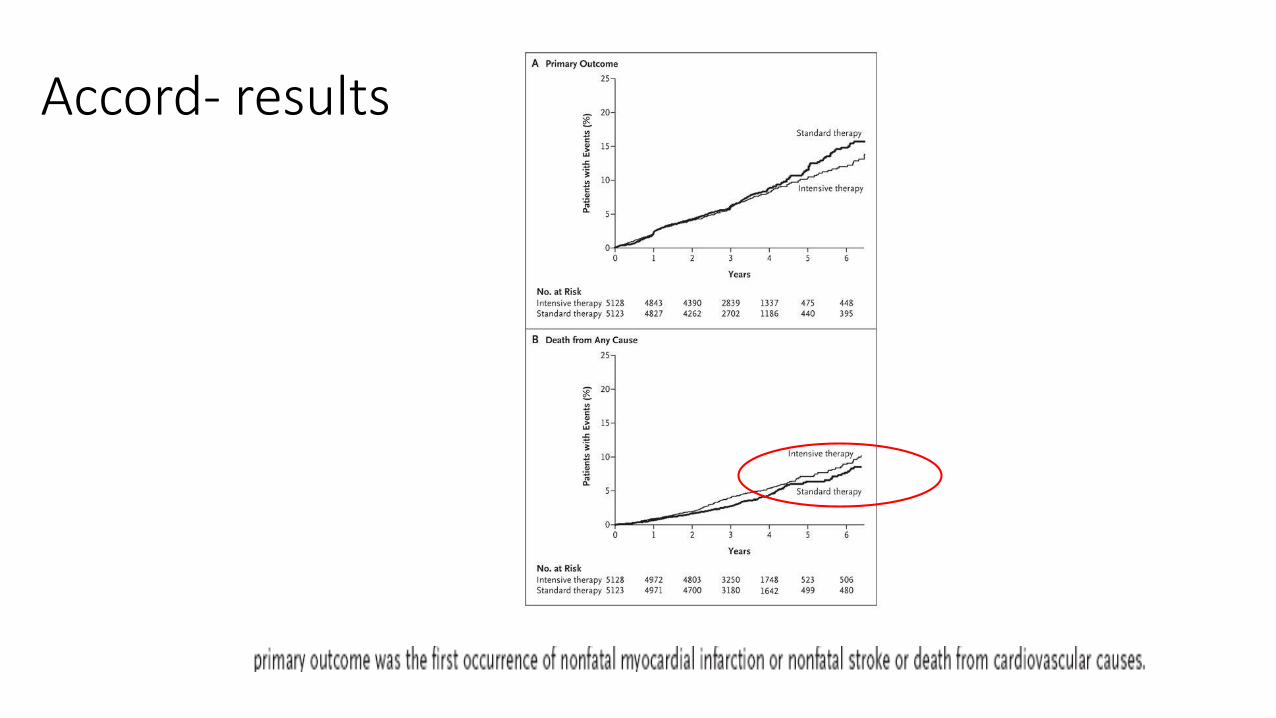
Accord- results
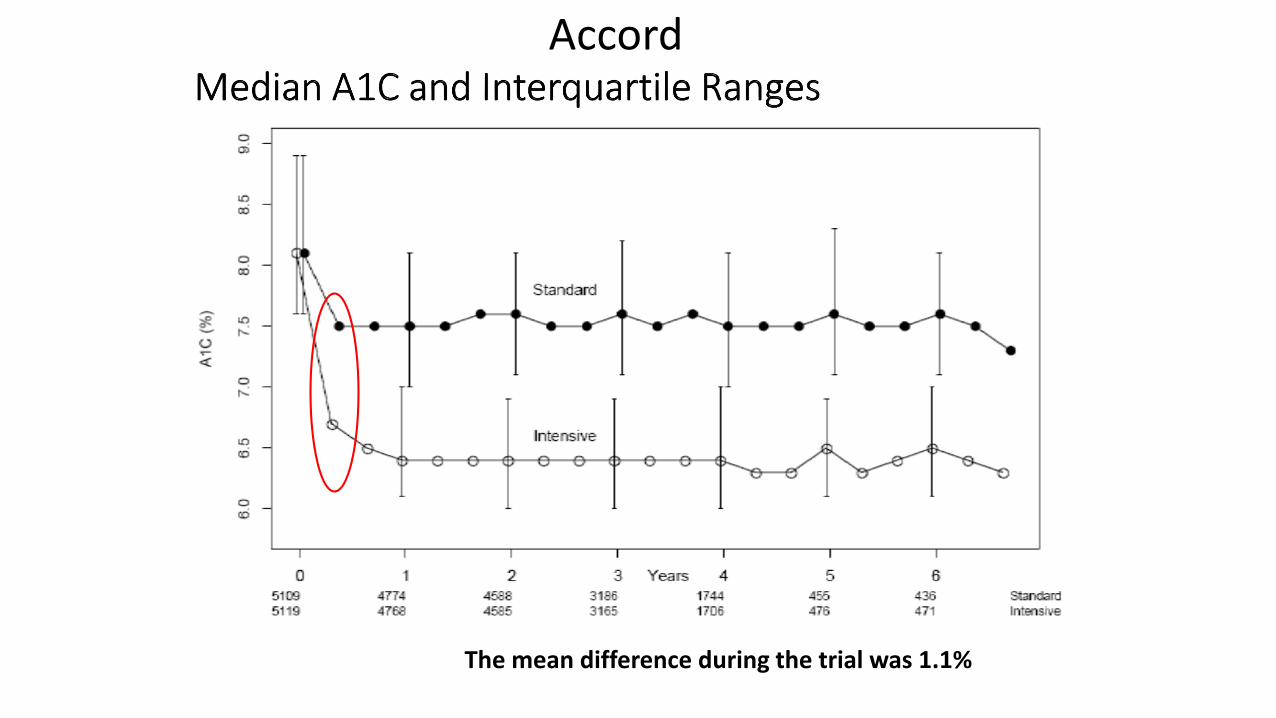
The mean difference during the trial was 1.1%
Accord
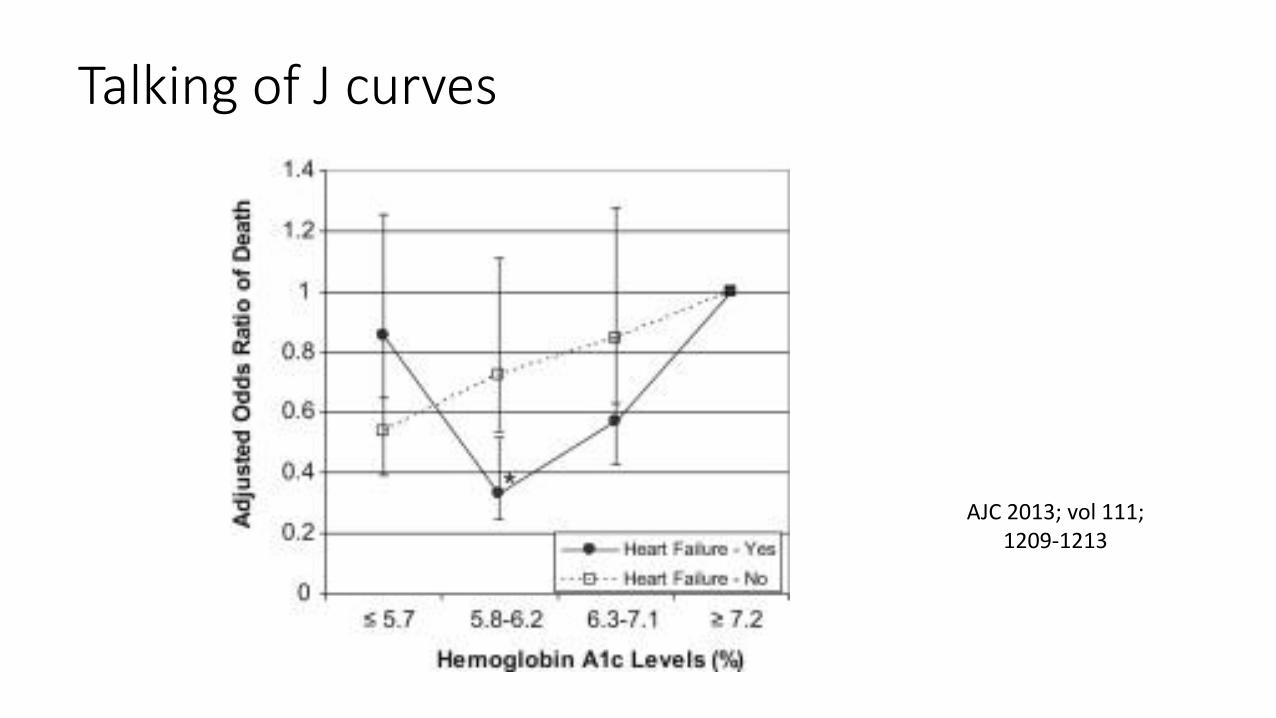
Talking of J curves
AJC 2013; vol 111; 1209-1213
Learning points…
• Cautious with too much intense glycaemic control- esp elderly/ premorbidities
• Go slow and steady….
Mr LK, 48 years
• Married with 3 young children
• Heavy Goods Vehicle driver
• T2D- 7 years
• Bilateral preproliferative retinopathy/ Macular oedema awaiting macular grid laser/ microalb/ Feet normal sensations
• BP 126/76 mmHg, BMI 36 kg/m2
Current Medications
• Metformin 1 g bd
• Gliclazide 160 mg bd
• Cilazapril 5 mg od
• Simvastatin 20 mg od
Current hbA1c 68 mmol/mol (8.4%)
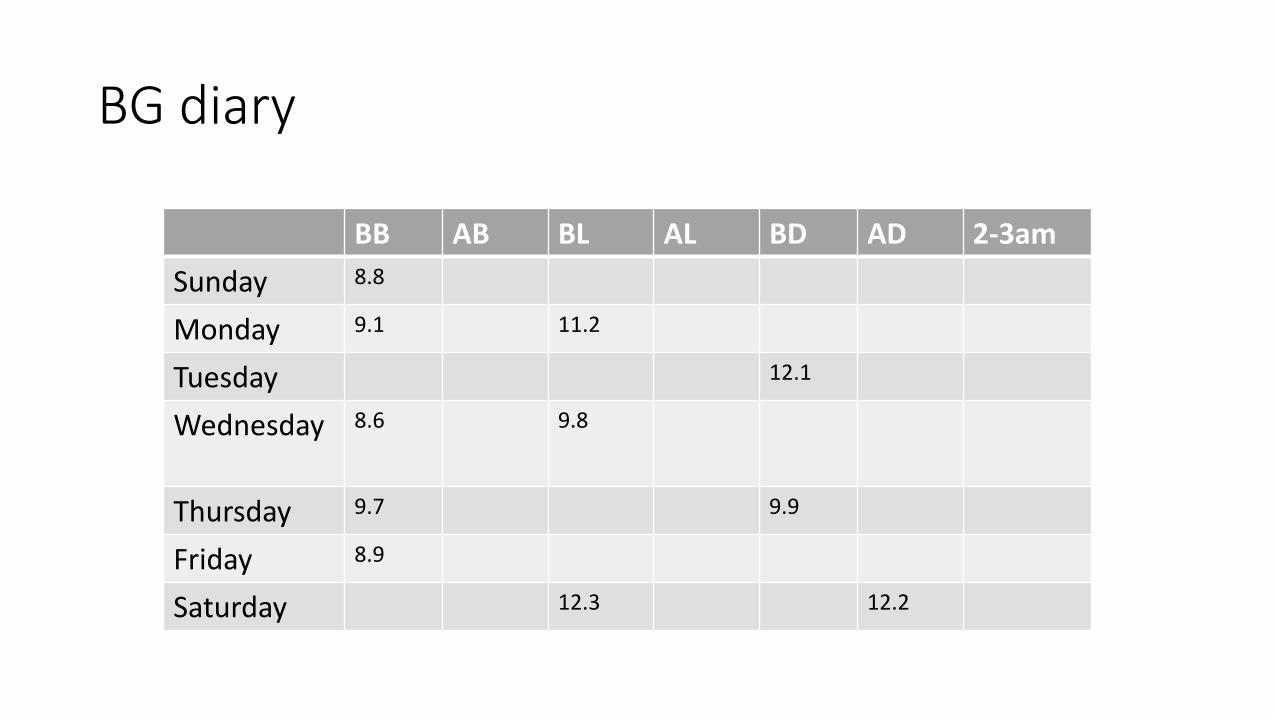
BG diary
BB AB BL AL BD AD 2-3am
Sunday 8.8
Monday 9.1 11.2
Tuesday 12.1
Wednesday 8.6 9.8
Thursday 9.7 9.9
Friday 8.9
Saturday 12.3 12.2
Will not consider insulin- what are his options…..
Pioglitazone AVOID- significant macular oedema
Insulin sensitizer/ moves visceral fat to subcutaneous sites- valuable in some patients
Use slowly declining- fluid retaining properties- heart failure, pedal oedema
Osteoporosis especially females
Bladder tumours- especially after prolonged use/ higher dose- review use after 2-3 years
What other options….
GLP-1 agonists (Exenatide) or DPP4 inhibitors (gliptins)- not yet funded by pharmac
SGLT2 inhibitors- Forxiga (dapagliflozin)- not funded yet/ polyuria may be unappealing
What else apart from individualised glycaemic management…• BP is to target
• Lipid profile on simvastatin-
T Cholesterol- 3.8 mmol/l, LDL-C- 2.2 mmol/l, HDL-C- 0.8 mmol/l
Triglycerides- 2.6 mmol/l (fasting)- consistent with metabolic syndrome
Any role for adding in a fibrate?
FIELD study
• Fenofibrate Intervention and Event Lowering in Diabetes
• Multinational study- NZ, Australia, Finland
• Around 10,000 T2D subjects/ age 50-75 years
• Fenofibrate 200 mg a day versus placebo
• Laser treatment for retinopathy- prespecified tertiary endpoint
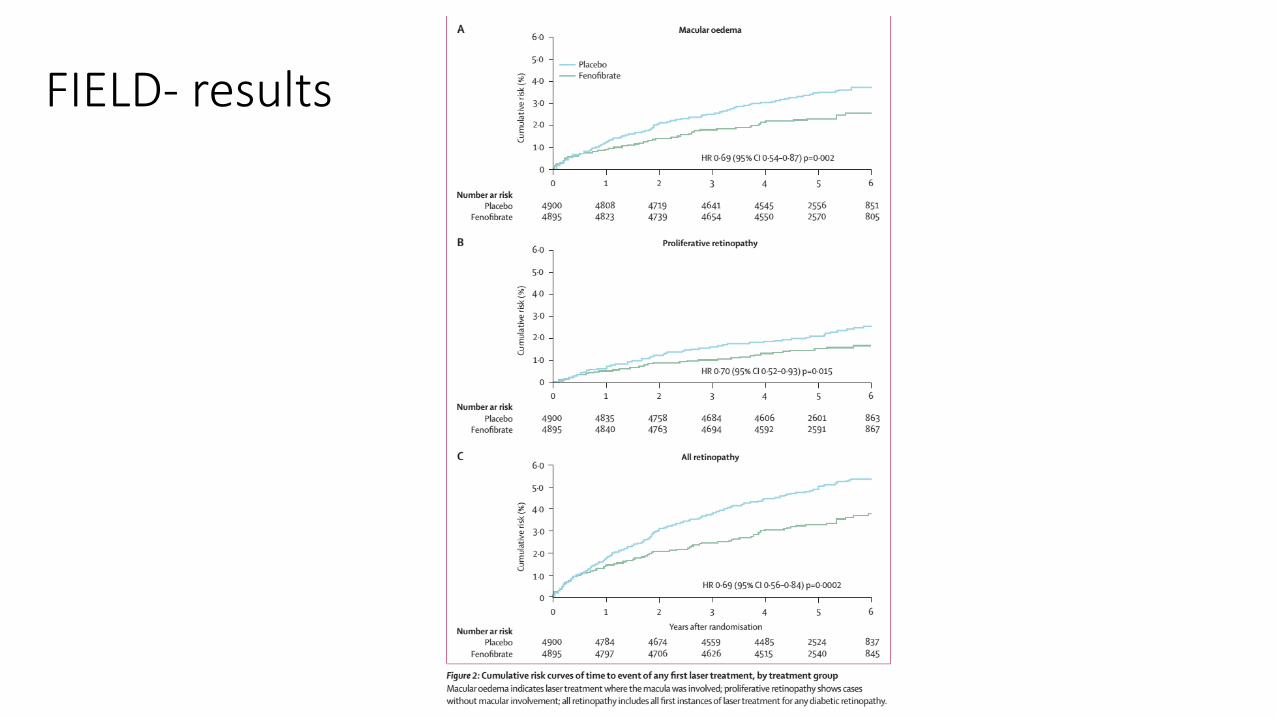
FIELD- results
Fenofibrate use in T2D
• In those with preexisting retinopathy- Reduced 2 step progression of retinopathy/ less need for laser treatment
• Independent of lipid effects- possibly by inhibiting VEGF/ reduced endothelial cell apoptosis/ reduced inflammation
• Benefit within 8 months of treatment/ benefits additive to better glycaemia/ BP control
• BUT….. Not subsidised- hopefully there is a class effect
Learning points…
• Caution with using glitazones in setting of heart failure/ macular oedema
• Review longer term use of glitazones- bladder tumours/ osteoporosis especially in females
• Consider fibrate therapy in T2D patients with established retinopathy-? Role of bezafibrate
Mr MD, 67 years
• T1D for over 30 years
• HbA1c consistently in 70s for last many years
• Bilateral mod-severe retinopathy/ Neuropathy/ no evident nephropathy
• Previous marathoner

Presents with swollen, red, painful left foot-no obvious trigger….
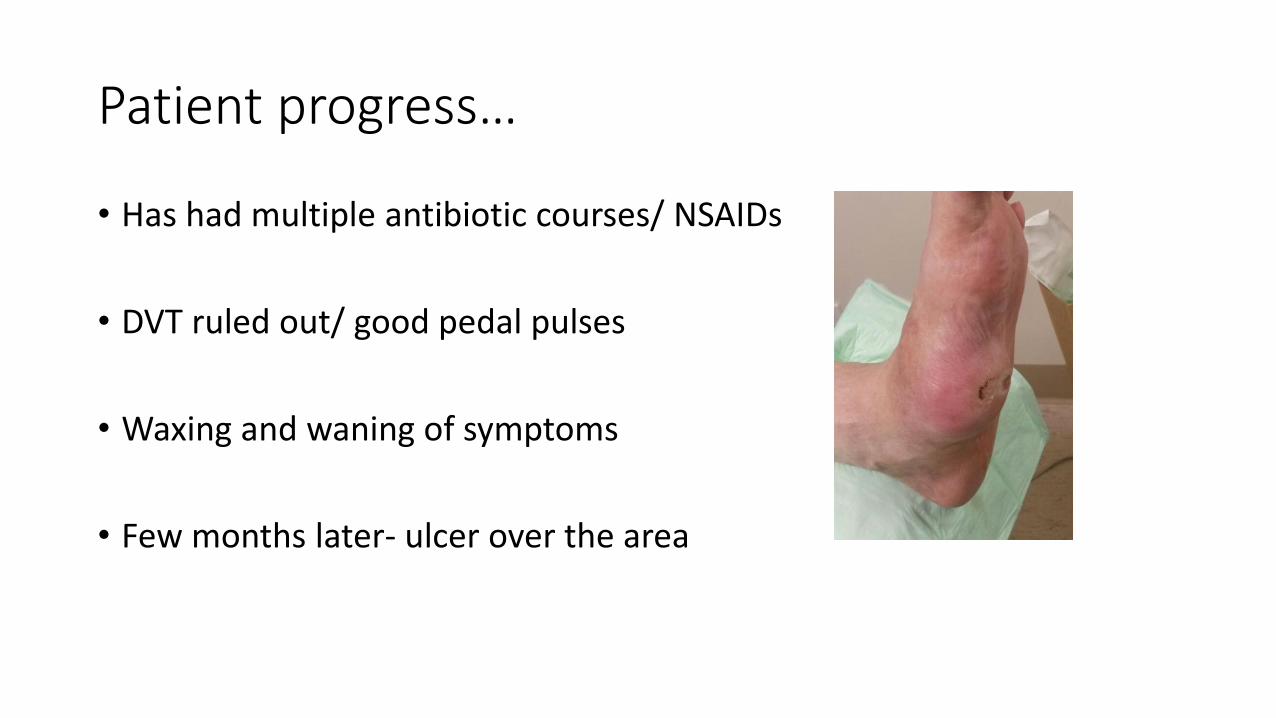
Patient progress…
• Has had multiple antibiotic courses/ NSAIDs
• DVT ruled out/ good pedal pulses
• Waxing and waning of symptoms
• Few months later- ulcer over the area
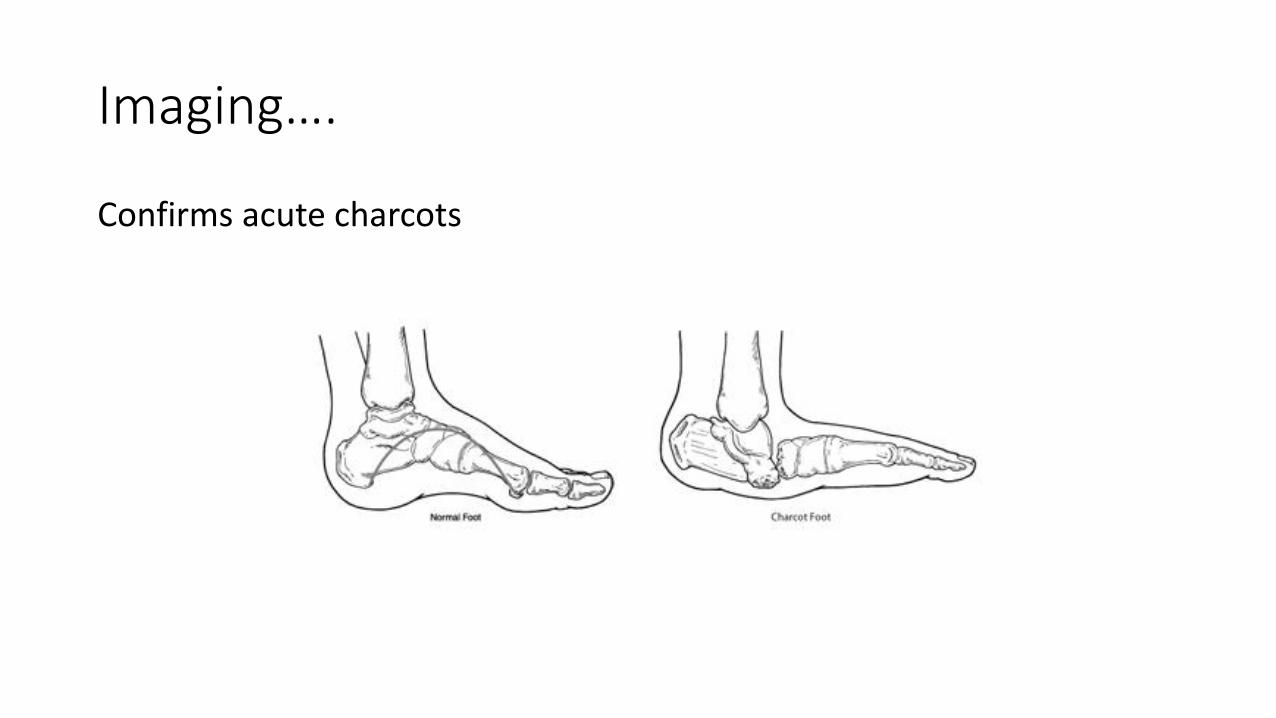
Imaging….
Confirms acute charcots
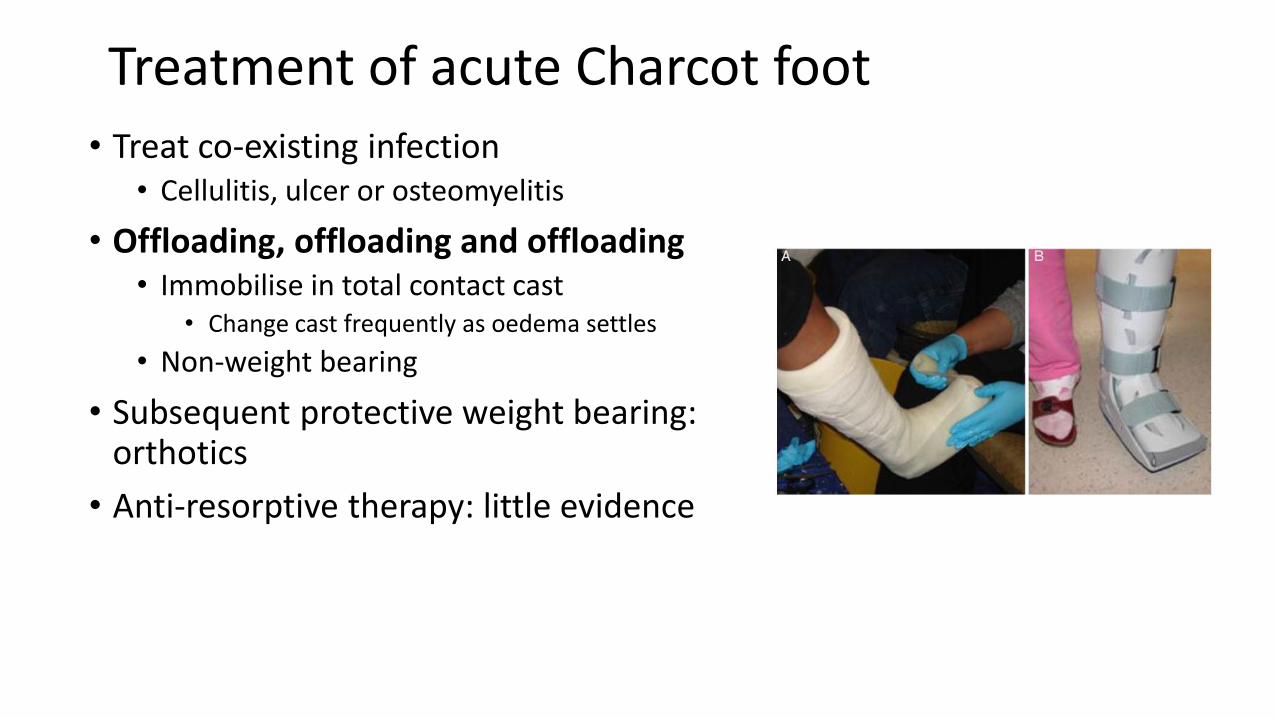
Treatment of acute Charcot foot• Treat co-existing infection
• Cellulitis, ulcer or osteomyelitis
• Offloading, offloading and offloading• Immobilise in total contact cast
• Change cast frequently as oedema settles
• Non-weight bearing
• Subsequent protective weight bearing: orthotics
• Anti-resorptive therapy: little evidence
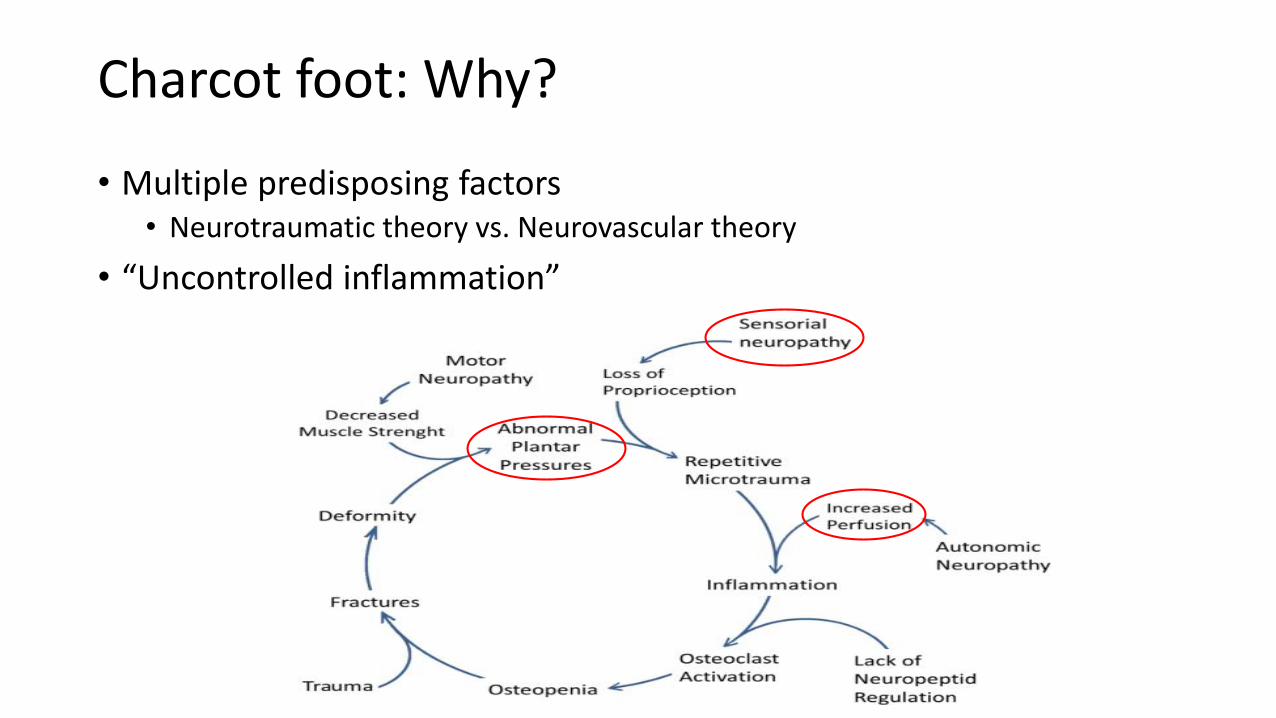
Charcot foot: Why?
• Multiple predisposing factors• Neurotraumatic theory vs. Neurovascular theory
• “Uncontrolled inflammation”
“The goal in the treatment of CN is to achieve a
plantigrade, stable foot that is able to fit into a shoe and to
also prevent a recurrent ulceration”
Talking of diabetic foot ulcers (DFU)…
• Annual incidence of DFU 1-4% with a lifetime risk of 15-25%
• Risk of recurrence 50-70% over 5 years
• 15% of DFU result in LE amputation
• After initial amputation, risk of contralateral amputation- 25-68% in next 3-5 years
• 85% of nontraumatic LE amputations attributed to DM
Alavi et al, J Am Acad Dermatol, 2014
Learning points…..
• Hot/ swollen/ painful foot- think Charcots- long DM history, neuropathy
• Attention to the other foot
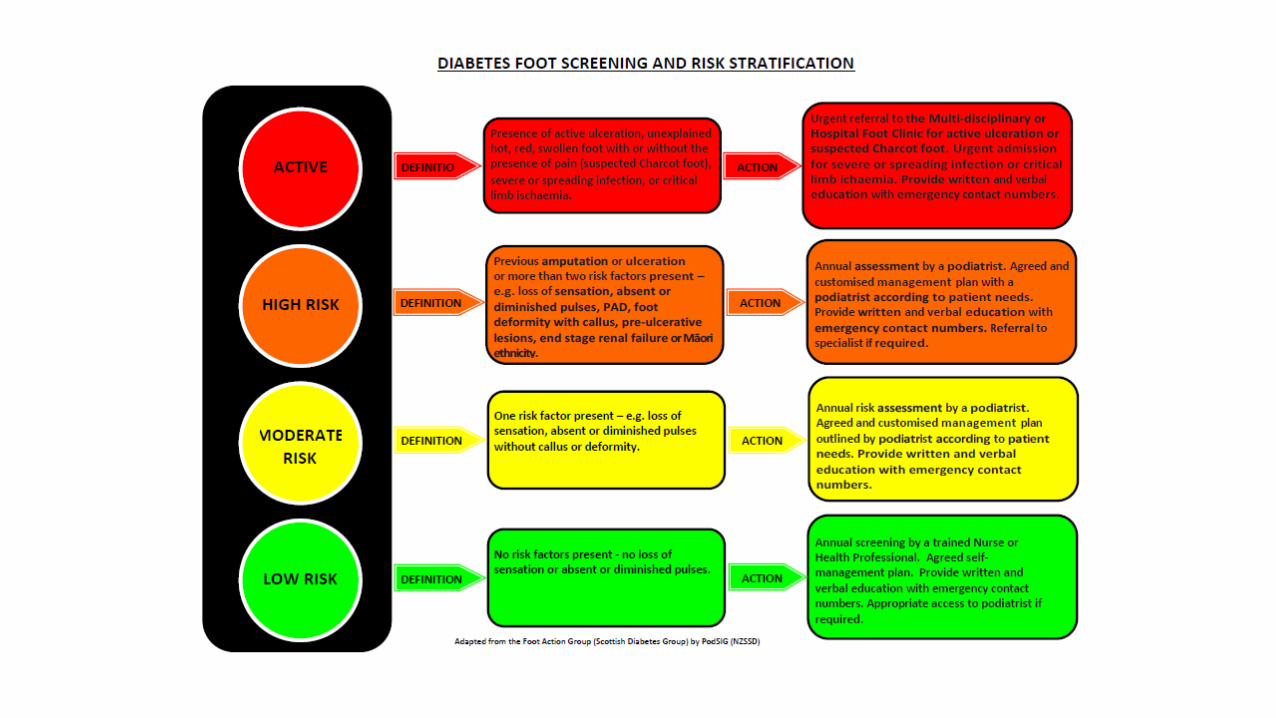
• Risk stratify feet- Low risk/ high risk foot/ active foot
• Education is key
• Clear pathways/ access
Mr TH, 75 yrs
• 4 am- Daughter found him collapsed in bathroom/ confused/ slurred speech/rt facial droop/ right sided weakness.
• Bilateral LL pain/ redness for 1/52- not seen GP as concerned would need amputation.
• May have taken extra Glibenclamide previous night (normally takes 1 tab mane).
• Previous IHD/ Emphysema/ No h/o ETOH
Impression- ?Cerebrovascular event
• BG paramedics- 2.3 mmol/l
• Weakness/ confusion improved with hypoglycaemia treatment
• Can hypoglycaemia cause focal neurological deficits- YES
• Does this person need hospital admission- YES
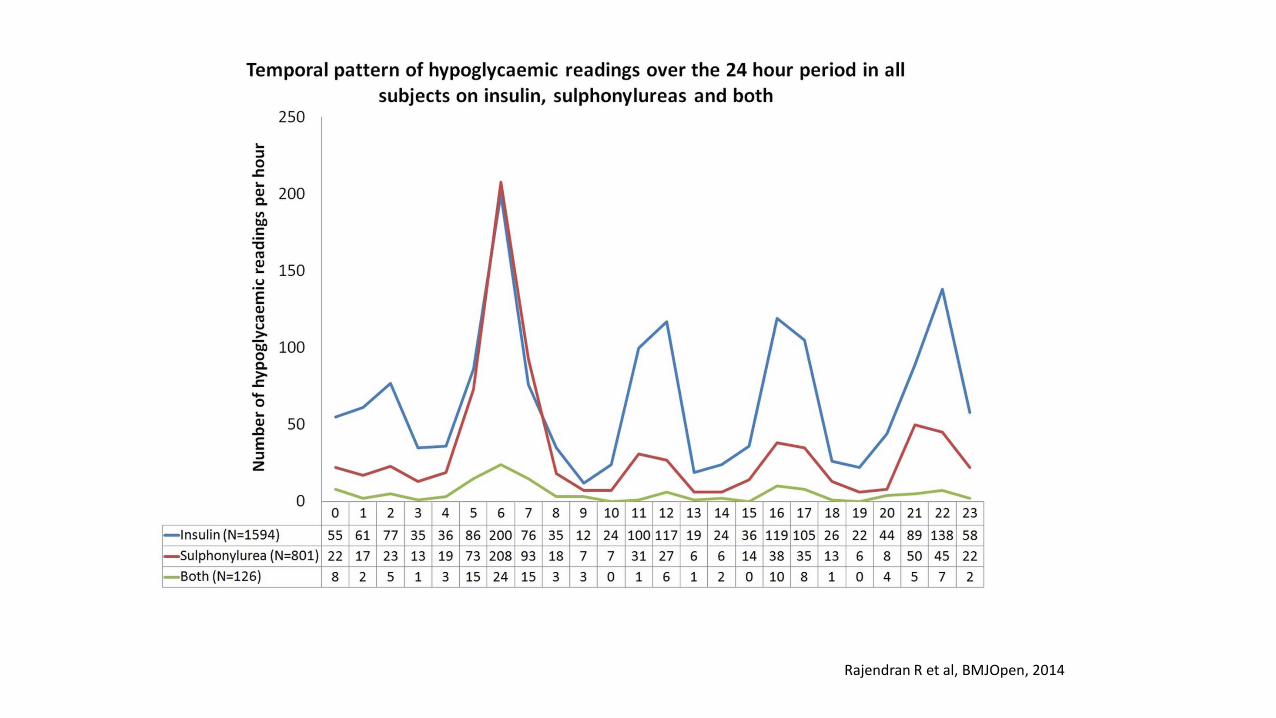
Rajendran R et al, BMJOpen, 2014
Learning points…..
• Hypoglycaemia may present like a TIA
• Caution with sulphonylureas especially in elderly
• Avoid glibenclamide (longer halflife) wherever possible/ switch if necessary
• May need hospital admission especially if severe episode/ cannot monitor and treat oneself- some patients may need octreotide (anti-dote)