
Autonomia abitativa Relazioni interpersonali Attività del ... · Meta-analisi di 50 studi...
32
Obiettivo del trattamento della schizofrenia: RECOVERY FUNZIONALE • Autonomia abitativa • Relazioni interpersonali • Attività del tempo libero • Lavoro/scuola • … Symptom remission alone is inadequate for a definition of recovery ... Dimensions of improved psychosocial functioning must also be integral to a definition of recovery... these dimensions include work, school, family life, friends, recreation, and independent living. Liberman & Kopelowicz, Psychiatr Serv 2005
Transcript of Autonomia abitativa Relazioni interpersonali Attività del ... · Meta-analisi di 50 studi...

Obiettivo del trattamento della schizofrenia:
RECOVERY FUNZIONALE
• Autonomia abitativa
• Relazioni interpersonali
• Attività del tempo libero
• Lavoro/scuola
• …
Symptom remission alone is inadequate for a definition
of recovery ...
Dimensions of improved psychosocial functioning must
also be integral to a definition of recovery... these
dimensions include work, school, family life, friends,
recreation, and independent living.
Liberman & Kopelowicz, Psychiatr Serv 2005
Schizofrenia e Recovery
A proportion of schizophrenia patients have a favourable prognosis and have a good clinical and functional outcomes
Systematic review of available data showed that 13.5% of patients met recovery criteria
Meta-analisi di 50 studi
Recovery:
• La persona deve mostrare un recupero sia sul piano clinico
che su quello psicosociale.
• In almeno uno di questi piani il recupero deve avere una
durata di almeno 2 anni.
Jääskeläinen et al. Schizophr Bull 2013
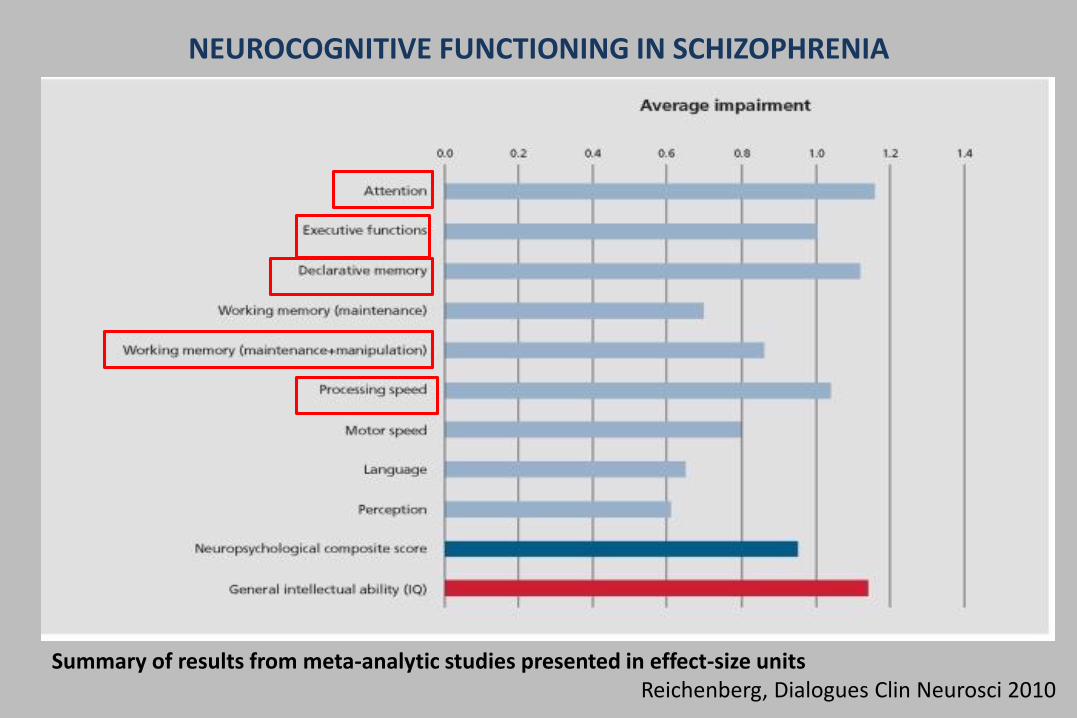
NEUROCOGNITIVE FUNCTIONING IN SCHIZOPHRENIA
Summary of results from meta-analytic studies presented in effect-size unitsReichenberg, Dialogues Clin Neurosci 2010

Meta-analysis of cognitive performance in drug-naïve patients with schizophreniaVerbal Memory
Speed of Processing Attention
Working Memory
Verbal memory, speed of processing and workingmemory were three of the domains with thegreatest impairments
The pattern of results is in line with previousmeta-analytic findings in antipsychotic treatedpatients
The present meta-analysis confirms the existence of significant cognitive impairments at the early stage of the illness in the absence of antipsychotic medication Fatouros-Bergman et al, Schizophr Res 2014

The Italian Network for Research on Psychoses StudyDegree of cognitive impairment in individual subjects with
schizophrenia (N=921)
0-0.5 SD below norms
1-1.5 SD below norms in at least 2 domains
2-2.5 SD below norms in at least 2 domains
2.5-3 SD below norms in at least 2 domains
Mucci et al, 2017


VELOCITÀ DI PROCESSAZIONE
ATTENZIONE
MEMORIA VERBALE
SINTOMI NEGATIVI
FUNZIONAMENTO
GLOBALE
PSICOSOCIALE
(Milev et al., Am J Psychiatry, 2005)
Baseline Follow-Up 7 anni

Neuropsychopharmacology: The Fifth Generation of Progress 2002
Neurocognitive constructs and functional outcome
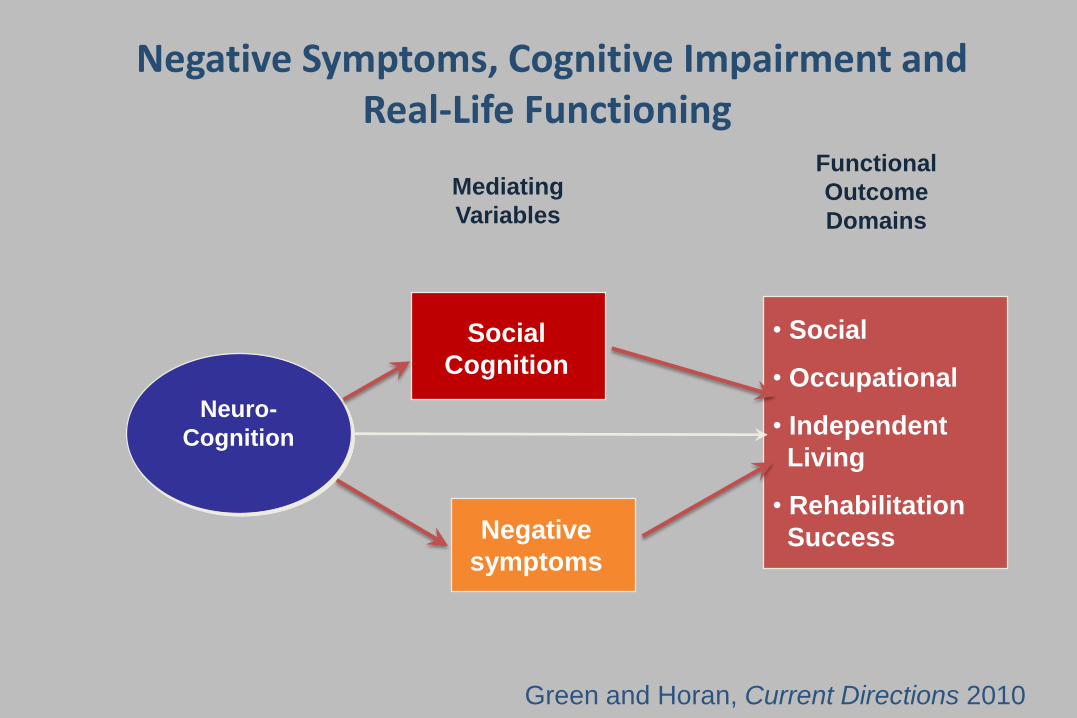
• Social
• Occupational
• Independent
Living
• Rehabilitation
Success
Mediating
Variables
Neuro-
Cognition
Functional
Outcome
Domains
Social
Cognition
Negative
symptoms
Green and Horan, Current Directions 2010
Negative Symptoms, Cognitive Impairment and Real-Life Functioning

Negative symptoms of schizophrenia: Clinical characteristics, pathophysiological
substrates, experimental models and prospects for improved treatment
NS may, to a certain extent, channel the deleterious influence of other symptoms into poor functional
outcome with which NS are strongly correlated




SEM - Modello Finale

VARIABLES SHOWING SIGNIFICANT ASSOCIATION WITH FUNCTIONING
TOTAL(direct+indirect)
NEUROCOGNITIVE FUNCTIONING 0.30
PANSS DISORGANIZATION -0.26
BNSS AVOLITION -0.25
FUNCTIONAL CAPACITY 0.24
ENGAGEMENT WITH MENTAL HEALTH SERVICES -0.18
SOCIAL COGNITION 0.17
PANSS POSITIVE -0.15
INCENTIVES -0.14
RESILIENCE 0.11
INTERNALIZED STIGMA -0.06
The Italian Network for Research in Psychoses
Galderisi et al, World Psychiatry 2014

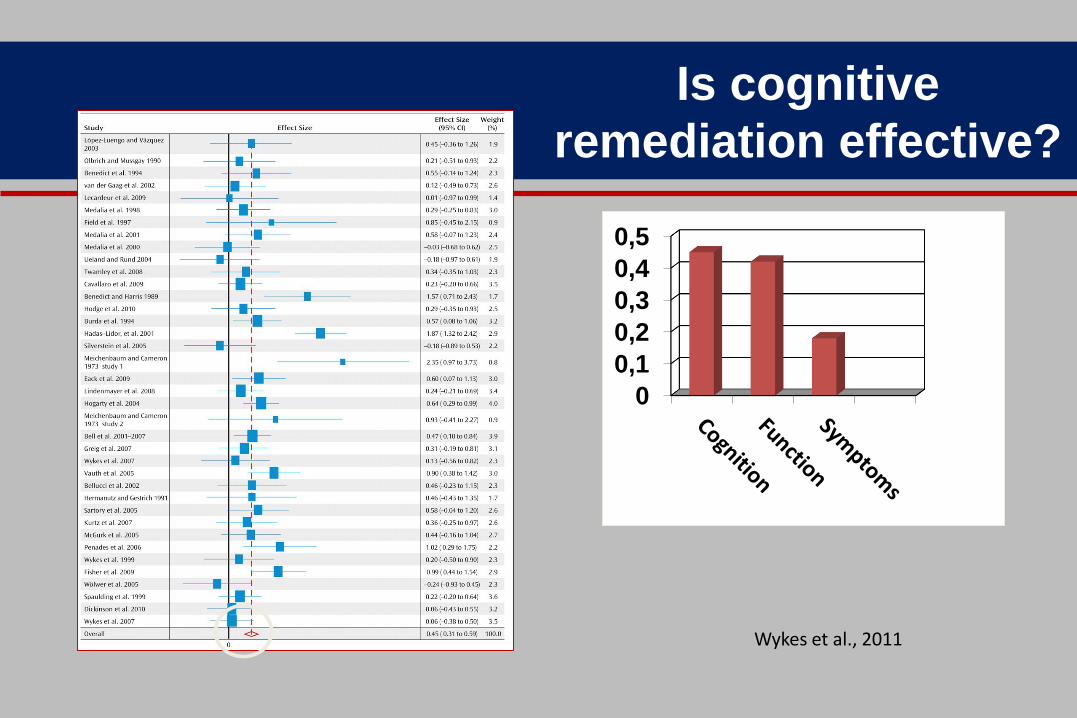
Is cognitive
remediation effective?
1982 participantsEffect size 0.45
Wykes et al., 2011
0
0,1
0,2
0,3
0,4
0,5


What differences really matter?
• Strategic approach produced a higher functional effect
– DP=0.34 (95% CI -0.11, 0.78); SC+=0.47 (95% CI 0.22, 0.73)
• Adjunctive psychiatric rehabilitation increases functional gains
– Rehab=0.59 (95% CI 0.30, 0.88);CRT only=0.28(95% CI -0.02, 0.58)
0
0,1
0,2
0,3
0,4
0,5
0,6
0,7
0,8
0,9
1
SC+
Rehab
DP+
Rehab
Effect sizes when rehab provided



Continuous treatment
Schizophrenia Research, 2017
• Cognition stable over time in both groupsBUT• CRT/SRT + only produced stable functional improvement (Time by
treatment effect F=11.48, p<0.001)
DesignCRT/SRT for 6 monthsCRT/SRT + post-therapy SRT
Follow-up after 5 years


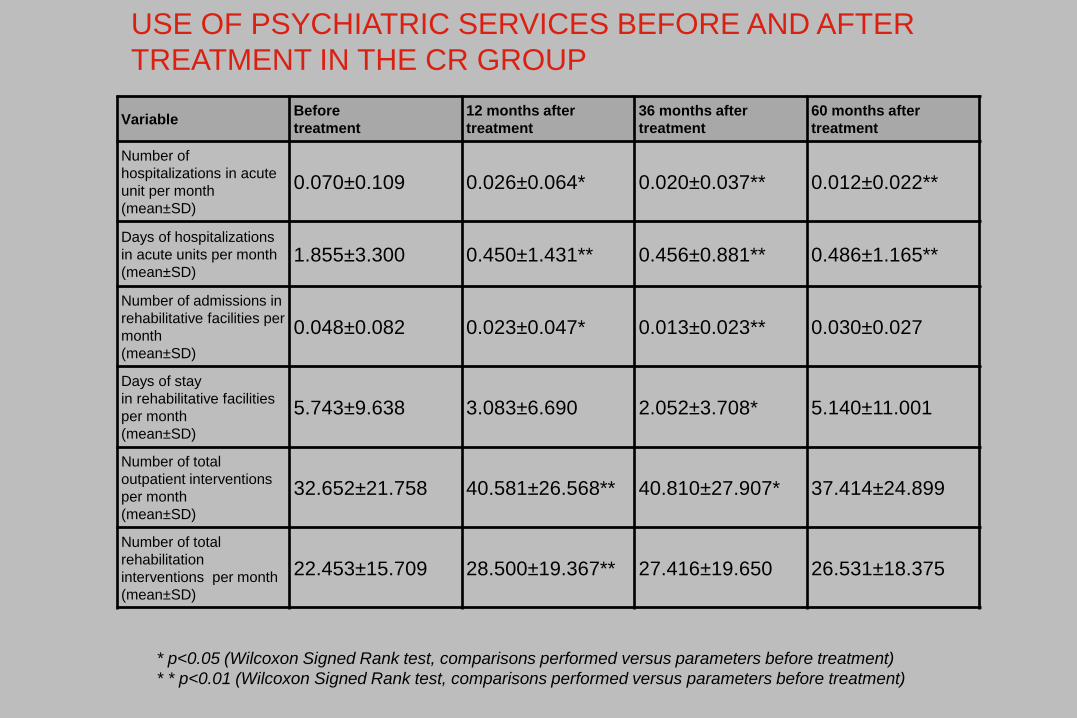
VariableBefore
treatment
12 months after
treatment
36 months after
treatment
60 months after
treatment
Number of
hospitalizations in acute
unit per month
(mean±SD)
0.070±0.109 0.026±0.064* 0.020±0.037** 0.012±0.022**
Days of hospitalizations
in acute units per month
(mean±SD)1.855±3.300 0.450±1.431** 0.456±0.881** 0.486±1.165**
Number of admissions in
rehabilitative facilities per
month
(mean±SD)
0.048±0.082 0.023±0.047* 0.013±0.023** 0.030±0.027
Days of stay
in rehabilitative facilities
per month
(mean±SD)
5.743±9.638 3.083±6.690 2.052±3.708* 5.140±11.001
Number of total
outpatient interventions
per month
(mean±SD)
32.652±21.758 40.581±26.568** 40.810±27.907* 37.414±24.899
Number of total
rehabilitation
interventions per month
(mean±SD)
22.453±15.709 28.500±19.367** 27.416±19.650 26.531±18.375
USE OF PSYCHIATRIC SERVICES BEFORE AND AFTER
TREATMENT IN THE CR GROUP
* p<0.05 (Wilcoxon Signed Rank test, comparisons performed versus parameters before treatment)
* * p<0.01 (Wilcoxon Signed Rank test, comparisons performed versus parameters before treatment)


Sintomi, funzionicognitive, social
cognition
Funzionamento
sociale
Lavoro/Scuola
Relazioniinterpersonali
Addestramentoalle abilità
sociali
Rimediocognitivo
Inserimentolavorativo
Psicoeducazione
Farmacoterapia(efficace, tollerata, continuativa)
Cura di sé
Recoveryfunzionale
Interventipsicosociali
Qualitàdella vita
Autonomia
Benesseresoggettivo
Motivazioneestrinseca e intrinseca
MODELLO DI INTERVENTO INTEGRATO NELLA SCHIZOFRENIA

Vita et al., 2016
DEPRESSION AND COGNITION

Meta-analysis of cognitive deficits in 1st-episode
MDD: pooled effect sizes by cognitive domain
Cognitive flexibility
Verbal fluency
Attentional switching
Visual learning and memory
Verbal learning and memory
Working memory
Attention
Psychomotor speed
-2 -1 0 1 2
Patients performing worseControls performing worse
Std mean differenceIV, random, 95% CI
Co
gnit
ive
do
mai
n
0.48 [0.21, 0.75]
0.36 [0.13, 0.59]
0.16 [-0.20, 0.51]
0.13 [-0.18, 0.45]
0.53 [-0.05, 1.11]
0.22 [0.00, 0.44]
0.59 [0.10, 1.07]
0.53 [0.23, 0.83]
Std mean differenceIV, random, 95% CI
Lee RS et al. J Affect Disord 2012;140:113-24
MDD, major depressive disorder; CI, confidence interval

Conradi HJ et al. Psychol Med 2011;41:1165-74
Cognitive symptoms are common in
depression
94%
Proportion of time spent without cognitive symptoms
Cognitive symptoms during
depressive episodes
Proportion of time spent with
cognitive symptomsa
Proportion of time spent without cognitive
symptoms
Residual cognitive symptoms in between depressive episodes
44%
aAccording to Diagnostic and Statistical Manual of Mental Disorders 4th Edition: diminished ability to think or concentrate, or indecisivenessProspective study (n=267) assessed 12 times over 3 years
Proportion of time spent with
cognitive symptomsa



















