Autoimmune blistering diseases Pemphigus Pemphigoid Dermatitis herpetiformis (Duhring) Dr. Kejian...
50
Autoimmune blistering diseases Pemphigus Pemphigoid Dermatitis herpetiformis (Duhring) Dr. Kejian Zhu Sir Run Run Shaw Hospital http:www.srrsh.com
-
Upload
milton-rogers -
Category
Documents
-
view
234 -
download
3
Transcript of Autoimmune blistering diseases Pemphigus Pemphigoid Dermatitis herpetiformis (Duhring) Dr. Kejian...

Autoimmune blistering diseases
PemphigusPemphigoid
Dermatitis herpetiformis (Duhring)
Dr. Kejian ZhuSir Run Run Shaw Hospital
http:www.srrsh.com

Blister---classification
Intraepithelial vesicles: Acantholytic vesicles: the break down of specialized attachments (desmosomes)
Nonacantholytic vesicles: the death or the rupture of the group of cells, usually seen in viral infections
Subepithelial vesicles:
Autoimmune blistering diseases
Diseases with intraepidermal blistering (pemphigus-group)
Pemphigus vulgaris Pemphigus vegetans Pemphigus foliaceus
Pemphigus erythematosus Paraneoplastic pemphigus Drug-induced pemphigus
Neonatal pemphigus Intercellular IgA dermatosis
Brazilian pemphigus

Autoimmune blistering diseases
Diseases with subepidermal blistering (pemphigoid group)
Bullous pemphigoid (BP)
Herpes gestationis
Cicatricial pemphigoid
Epidermolysis bullosa acquisita
Dermatitis herpetiformis (Duhring)
Linear IgA bullous dermatosis (LAD)
Bullous SLE

Diseases with intraepidermal blistering (pemphigus-group)
Pemphigus vulgaris Pemphigus vegetans Pemphigus foliaceus
Pemphigus erythematosus

Outline
Middle-aged and elderly people are most commonly affected Flaccid blisters Two main groups: vulgaris & foliaceus Nikolsky’s sign and Tzanck test are positive Autoimmune diseases Acantholytic intraepidermal blistering is produced by
autoantibodies against desmoglein Anti-desmoglein antibodies are detected by ELISA In vivo IgG deposition and IgG antibodies are observed by
immunofluorescence Oral steroids & immunosuppressants are mainly administered.

Adhesion of keratinocytes
Keratinocytes are firmly adhered by desmosomes.
Transmembrane adhesion molecules in the cadherin superfamily, such as desmoglein 1 (Dsg 1), Dsg3, and desmocolin cadherin (DC), are important to intercellular adhesion.
In pemphigus, autoantibodies are produced against Dsg1 and Dsg3, some of whose molecular functions are disturbed. This causes acantholysis.

Acantholysis
Acantholysis: dissociation of intercellular connections in the epidermis.
As dissociation progresses, epidermal cleavage and blistering occurs.
Acantholytic cells: deformed keratinocytes become spherical from loss of intercellular connection within the blisters.

Tzanck test
Tzanck test is a kind of cytological diagnosis method.
It is induced by applying a slide glass to the bottom of a broken blister and staining the adhered cellular components in Giemsa for observation under a light microscope.
Tzanck cells are acantholytic cells observed in pemphigus.
Tzanck cells can also be observed in blisters of herpes simplex and herpes zoster, ballooning cells produced by viral infection.
Nikolsky’s sign
Nikolsky's sign: blistering or exfoliation of the skin’s outmost layer produced by slight rubbing of the normal-looking skin
It is positive in pemphigus, epidermolysis bullosa, staphylococcal scalded-skin syndrome (SSSS), and toxic epidermal necrolysis (TEN).
Nikolsky's sign is useful in differentiating between pemphigus vulgaris (where it is present or positive) and bullous pemphigoid (where it is absent)
Pemphigus vulgarisPemphigus vegetansPemphigus foliaceus
Pemphigus erythematosus
Outline
The most common variety of pemphigus The disease most frequently occurs in the middle-aged
and elderly. The disease is caused by autoantibodies against
desmoglein 3, which is a desmosomal adhesion factor in keratinocytes.
Acantholytic blisters form immediately above epidermal basal cells。
It tends to manifest as oral enanthema. Nikolsky’s sign is positive. Oral steroids and immunosuppressants are the first-line
treatment.

Clinical features
Most frequently affects the middle-aged and elderly Erosions and ulcers develop acutely in the oral
mucosa in 70-80% of cases Blisters of various sizes occur on normal skin, easily
rupture to form erosions and crusts Painful, esp. when touched Anywhere on the body, esp. at sites of pressure and
friction (back, buttocks and feet) Nikolsky’s sign When widespread, electrolyte abnormalities due to
loss of body fluid or hypoprotein Be fatal when there is secondary infection

Workup
Pathology: acantholysis, intraepidermal blistering, leaving one basal layer at the bottom
Immunofluorescence: intercellular in vivo IgG deposition
ELISA: anti-Dsg3 IgG Ab, sometimes also anti-Dsg1 IgG Ab

Diagnosis
Clinical features Pathology Immunofluorescence ELISA DDx: bullous pemphigoid, impetigo, bullous
drug eruption, dermatitis herpetiformis,
erythema multiforme,
Stevens-Johnson syndrome, etc.

Treatment
Systemic application of steroids is the first-line treatment (0.5-1.0mg/kg/d).
Taper off to a maintenance dose or until it can be discontinued.
Immunosuppressants (mycophenolate mofetil, CTX, AZT, MTX, cyclosporine) may be used.
In intractable cases, plasma exchange therapy and IVIG can be performed.
Antibiotics, fluid transfusion, nutrition management are conducted supplementarily.

Pemphigus vulgarisPemphigus vegetansPemphigus foliaceus
Pemphigus erythematosus

Clinical features
A subtype of pemphigus vulgaris, the most uncommon variety of pemphigus
Characterized by the formation of vesicles and erosions that do not re-epithelialize but gradually proliferate and elevate
Frequently occurs on areas of friction (axillary fossa, umbilical fossa, periphery of the oculonasal and perioral regions) and exposure (face, neck, scalp)
Oral mucosa is often involved
Strong odor

Workup
Pathology: suprabasal cell acantholysis, downward proliferation of rete ridges
Immunofluoscence: intercellular deposition of IgG and C3
Culture: bacteria and/or candida

Diagnosis
Vesicles and erosions
Areas of friction, exposure
Proliferate and elevate
Suprabasal cell acantholysis
DDx: chronic pyoderma and fungal granuloma,
Hailey-Hailey disease, condyloma
acuminatum, etc.

Treatment
The same as for pemphigus vulgaris Treat local infections Consider topical and systemic antibiotics
Consider antifungal agents for candida Surgical excision of large vegetative
growths
Better prognosis than pemphigus vulgaris

Pemphigus vulgarisPemphigus vegetansPemphigus foliaceus
Pemphigus erythematosus

Outline
Autoantibodies are produced exclusively against Dsg 1
Acantholysis and blistering are seen in the superficial
epidermis (in the granular cell layer)
Fragile blisters, scaling and erosion, accompanied by
crusts
Lesions are not/occasionally produced in the mucosa
Examinations and treatments are the same as for
pemphigus vulgaris. The steroid dosage is usually less
than for pemphigus vulgaris
Clinical features
Most commonly affects the middle-aged and elderly Extremely fragile flaccid vesicles Some of the blisters dry to become leafy and to
exfoliate successively The face, head, back and chest are most commonly
affected When spreads over the whole body, it resembles
exfoliative erythroderma Mucosa is not or occasionally involved Nikolsky’s sign is positive
Workup
Pathology: acantholytic blistering is found in the epidermal upper layer.
Immunofluorescence: intercellular in vivo IgG deposition is observed
ELISA: anti-desmoglein 1 antibodies

Diagnosis
Clinical features Pathology Immunofluorescence ELISA DDx: pemphigus vulgaris, pemphigus erythematosus, drug-induced bullous disease, paraneoplastic pemphigus, etc.

Treatment
The same as for pemphigus vulgaris Oral steroid dosage may be less than
that for pemphigus vulgaris In limited involvement cases, topical
steroid are sufficient

Pemphigus vulgarisPemphigus vegetansPemphigus foliaceus
Pemphigus erythematosus
Clinical features
A subtype of pemphigus foliaceus Occurs most commonly in the middle-
aged and elderly Frequently affects the seborrheic
zones (head, face, chest and back) The mucosa is not involved Involvement of SLE is seen in some
cases

Workup
Pathology: intraepidermal superficial bullae within the granular layer or just below it. Acantholysis may occur in the blister floor or roof.
Immunofluorescence: linear deposits of IgG and C3 in the intercellular space of the epidermis
May have lab abnormalities of SLE

Diagnosis
Clinical features Pathology Immunofluorescence DDx: paraneoplastic pemphigus,
seborrheic dermatitis, lupus
erythematosus, pemphigus
foliaceus, etc.

Treatment
The same as for pemphigus foliaceus
Diseases with subepidermal blstering (pemphigoid group)
Bullous pemphigoid (BP)
Dermatitis herpetiformis (Duhring)

Outline
Subepidermal blistering occurs as a result of autoantibody action against epidermal basement membrane structural proteins
Blisters are tense and do not rupture easily Divided into pemphigoid, linear IgA bullous
dermatosis, epidermolysis bullosa acquisita, dermatitis herpetiformis, herpes gestations, etc.
Immunofluorescence is useful for diagnosis Steroids and dapsone are applied
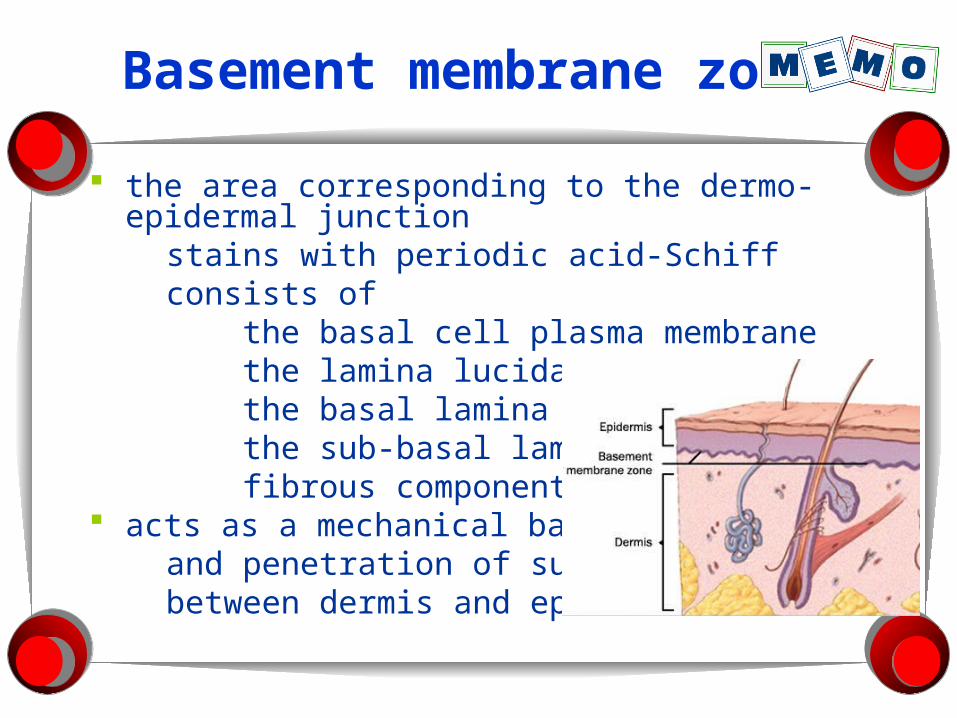
Basement membrane zone
the area corresponding to the dermo-epidermal junction
stains with periodic acid-Schiff consists of the basal cell plasma membrane the lamina lucida the basal lamina the sub-basal lamina fibrous components acts as a mechanical barrier and penetration of substance between dermis and epidermis
Bullous pemphigoid (BP)Dermatitis herpetiformis

pathogenesis
Autoantibodies are produced against hemidesmosome, type XVII collagen (BP180) and BP230 in the epidermal basement membranes, which leads to blistering.
Autoantibodies against BP180 play a major role.

Outline
Autoantibodies against hemidesmosomes The major pathogenic antigen is type XVII
collagen (BP180). The roof of the blister has the full thickness
of the epidermis Elderly people account for the majority of
cases Characterized by subepidermal blisters Blisters do not rupture easily Oral steroids are effective

Clinical features
The elderly are more commonly affected Multiple relatively large and severe tense
blisters form immediately Often accompanied by edematous erythema Much less invasively to the mucous
membranes (20% involved) The general condition is favourable May be complicated by malignant tumors

Workup
Pathology: subepidermal blistering, accompanied by eosinophilic infiltration
Immunofluorescence: linear IgG and C3 deposition in the basement membranes
ELISA: autoantibodies against type XVII collagen (BP180) proteins
High IgE values and elevated levels of eosinophils in peripheral blood

Diagnosis
Clinical features Pathology Immunofluorescence ELISA DDx: drug-induced bullous disorders, epidermolysis bullosa, epidermolysis bullosa acquisita, erythema multiforme, dermatitis herpetifomis, linear IgA dermatosis, etc.

Treatment
Oral steroids (0.5mg/kg/d) Gradually reduced Combination therapy of Immunosuppressants
(CTX), DDS, tetracyclines and nicotinic-acid amide are also useful
Avoid secondary infections Nutrition management is important for elderly Topical steroid application may be sufficient in mild
cases Plasma exchange therapy and IVIG may also be
used in severe cases

Bullous pemphigoid (BP)Dermatitis herpetiformis

Outline
Characterized by extremely intense itching and irritation, chronically recurrent erythema and vesicles
Vesicles tend to form circular patterns Common in Caucasians, rare in Asians Granular IgA deposition in the dermal
papillary Gluten-induced enteropathy develops as a
complication Oral dapsone is effective
Gluten
composed of the sticky, storage proteins found in wheat
exist conjoined with starch in the same grass-related grains, notably wheat, rye and barley

Pathogenesis
IgA antibodies against tissue transglutaminase
The granular IgA deposition in the skin is an immuno-complex
Clinical features
Extremely intense itching Erythema and urticarial lesions Vesicles in a ring-shaped pattern Scratch and resulted crusts Heal with abnormal pigmentation or
depigmentation Appear symmetrically on the entire body,
esp. on the elbows, knees and buttocks Gluten-induce enteropathy is found in more
than 90% of cases

Workup
Pathology: subepidermal blistering, micro-abscesses of neutrophils in dermal papillary
Immunofluorescence: granular IgA deposition in the dermal papillary

Diagnosis
Clinical features Pathology Immunofluorescence DDx: linear IgA bullous dermatosis,
bullous pemphigoid,
herpes gestationis,
erythema multiforme, ect.

Treatment
Dapsone is effective Gluten-free diet antihistamines